
Stop…let Me A-”cyst” You A Case Study about Cystinuria by Amy Albright.
14
Stop…let Me A-”cyst” Stop…let Me A-”cyst” You You A Case Study about Cystinuria by Amy Albright
-
Upload
kelsie-batson -
Category
Documents
-
view
219 -
download
0
Transcript of Stop…let Me A-”cyst” You A Case Study about Cystinuria by Amy Albright.
Stop…let Me A-”cyst” YouStop…let Me A-”cyst” You
A Case Study about Cystinuria by Amy Albright

Patient History
• 57 year old woman with history of renal problems
• Patient hospitalized upon urgent referral from doctor’s office
• Urinalysis was performed
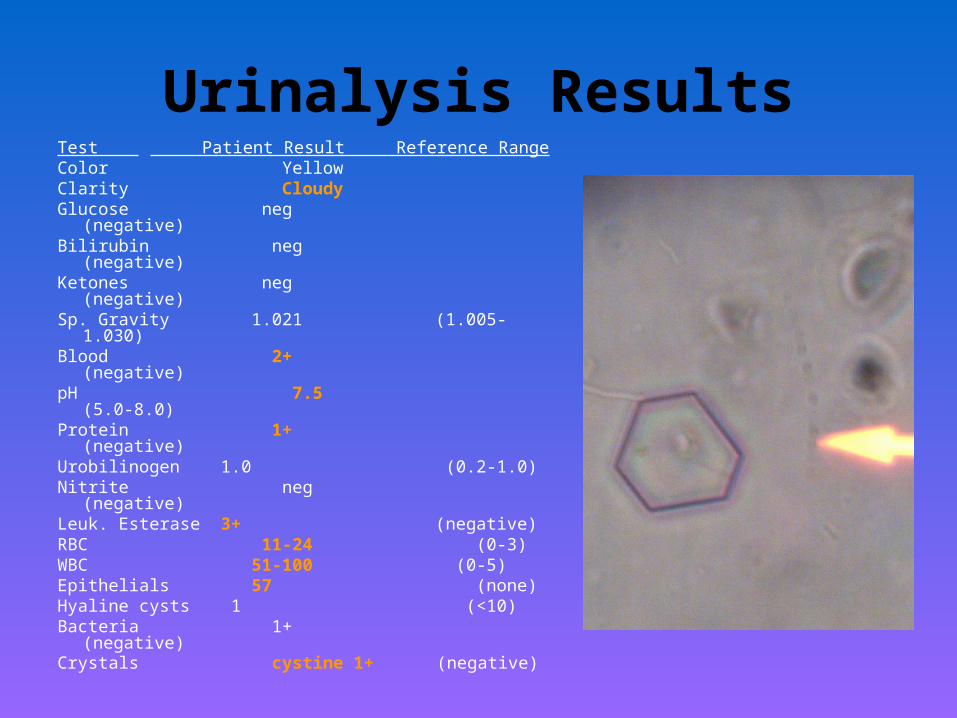
Urinalysis ResultsTest Patient Result Reference RangeColor YellowClarity CloudyGlucose neg (negative)Bilirubin neg (negative)Ketones neg (negative)Sp. Gravity 1.021 (1.005-1.030)Blood 2+ (negative)pH 7.5 (5.0-8.0)Protein 1+ (negative)Urobilinogen 1.0 (0.2-1.0)Nitrite neg (negative)Leuk. Esterase 3+ (negative)RBC 11-24 (0-3)WBC 51-100 (0-5)Epithelials 57 (none)Hyaline cysts 1 (<10)Bacteria 1+ (negative)Crystals cystine 1+ (negative)
Past Patient History
• Diagnosed with cystinuria as a child
• Left side nephrectomy as a child secondary to damage by cystine stones
• Recurrent kidney stones in the remaining right kidney
• Nephrostomy tube placed into
remaining kidney

Questions to be Considered:
1.) How does the patient’s current renal problems relate to the cystine crystals found?
2.) What laboratory tests are performed to confirm the presence of cystine crystals in the urine?
3.) What are the long term effects of cystine crystal formation?
4.) Are there treatments available for patients with cystinuria?
Pathogenesis of Cystinuria
• Autosomal recessive disorder• Involves a defect in the renal transport of cystine
by the tubules • Defect results in lack of cystine reabsorbtion of
the kidney• Homozygous patients usually the only ones to
present with problems• Heterozygotes have a milder form of cystinuria
(cystine crystals found in urine during analysis but don’t usually form stones)
Solubility within the Kidney• Normal excretion of amino acids such as cystine into
the urine is about 100 mg/day• Heterozygous excrete around 100-300 mg/day• Homozygous excrete around 500-1000 mg/day• Solubility limit is around 300-400 mg/day• Stones composed of cystine form when the
concentration of cystine exceeds the normal solubility levels and the excess cannot go into solution (cystine crystals favor the existing free cystine and will compound it to form the stone)
Cystine Confirmation
• Initially found during a microscopic urinalysis– crystals are found in neutral to acidic pH and are flat
hexagonal shapes
• Confirmation test for cystine once crystals are found microscopically is a cyanide-nitroprusside test– involves mixing the urine with sodium cyanide and
then sodium nitroprusside which will chemically react to produce a red-purple color indicative of presence of cystine crystals in the urine
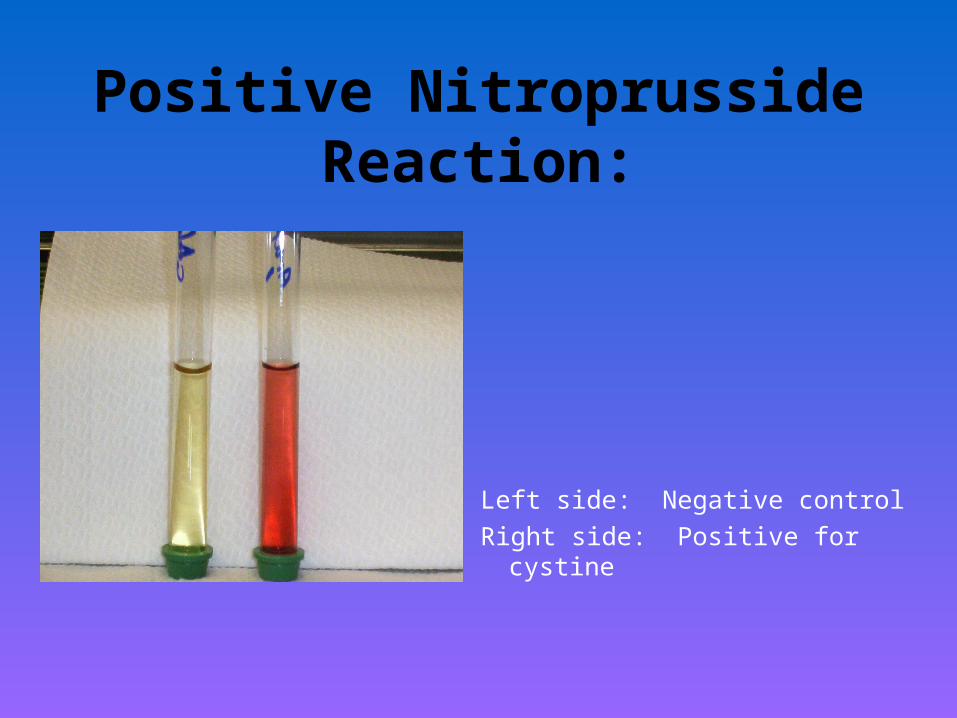
Positive Nitroprusside Reaction:
Left side: Negative control
Right side: Positive for cystine

Long Term Effects of Cystinuria
• Recurrent stone formation as seen with this patient
• Possible nephrectomy due to renal failure
• Pain associated with stone formation and passage
Treatments
• Focus is on management
• Relief of symptoms (pain medications)
• Prevention of further stones (drinking large amounts of water to dilute the urine)
Treatments - continued…..
• Watching diet ( avoiding methionine rich foods)• Alkanization of the urine (use of sodium
bicarbonate or sodium citrate to more readily dissolve the cystine)
• Lithotripsy (non-invasive, shock waves to break up the stone to where it can be passed)
• Invasive procedures for stone removal

Summary
• 57 year old women with presence of cystine crystals in the urine
• Confirmatory nitroprusside test was positive for cystine
• History revealed many renal problems associated with cystinuria
• Treatments are unpredictable
Credits
This case study was prepared by
Amy Albright, MT(ASCP) while she was a
Medical Technology student in
the 2004 MT Class at William Beaumont
Hospital, Royal Oak, MI.


















