
Step 1: Initial Assessment for NIV€¦ · CXR – exclude pneumothorax / pneumonia ARTERIAL blood...
10
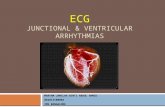
Acute Non-Invasive Ventilation Pathway 1 BSUH Acute Non Invasive Ventilation Pathway - 2020 v3.2 – NIV steering group. SH, KD. All steps in this pathway must be completed prior to starting NIV. Step 1: Initial Assessment for NIV Contraindications for ward NIV: Patient Name: …….…………… Trust ID: …….………………… DoB: ………..………………… (Attach patient sticker) Baseline Investigations: (tick) CXR – exclude pneumothorax / pneumonia ARTERIAL blood gas 12 lead ECG – cardiac monitor if arrhythmia, HR>120 or known cardiomyopathy Bloods – do not delay NIV to await results Respiratory Acidosis? pH < 7.35 pCO2 > 6.5 RR > 23 STOP! Consider alternative diagnosis/ management Consider NIV - Use NIV decision tree & complete pathway. YES NO NIV is not indicated for pneumonia or life threatening asthma - refer to ITU for consideration of intubation if pCO 2 >6.5 and pH <7.35 or worsening respiratory distress. NIV is not indicated for treatment of metabolic acidosis (or metabolic part of acidosis), check BASE EXCESS and consider alternative diagnosis/management. Absolute NIV contraindications: Pneumonia Asthma Severe facial deformity Facial or upper airway burns Fixed upper airway obstruction Relative NIV contraindications: Untreated pneumothorax Recent upper GI or craniofacial surgery Vomiting / aspiration risk Bowel obstruction (consider NGT) pH ≤7.15 (or <7.25 and additional adverse features) GCS ≤ 8, confusion/ agitation, cognitive impairment Suspected COVID19 – see BSUH NIV COVID pathway Indications for ICU input: Acute Hypercapnic Respiratory Failure with impending arrest IV sedation Close monitoring Suspected difficult intubation e.g. Obesity, NMD Suspected COVID19 Patients with contraindications for ward NIV, or where indication for ICU input is identified: STOP! Seek senior /ICU advice and/or consider alternative management. RSCH Med SpR:bleep 8521 PRH Med SpR:bleep 6044 ICU RSCH:bleep 8413 ICU PRH:bleep 6010
Transcript of Step 1: Initial Assessment for NIV€¦ · CXR – exclude pneumothorax / pneumonia ARTERIAL blood...

Acute Non-Invasive Ventilation Pathway
1
BSUH Acute Non Invasive Ventilation Pathway - 2020 v3.2 – NIV steering group. SH, KD.
All steps in this pathway must be completed prior to starting NIV.
Step 1: Initial Assessment for NIV
Contraindications for ward NIV:
Patient Name: …….……………
Trust ID: …….…………………
DoB: ………..…………………
(Attach patient sticker)
Baseline Investigations: (tick)
CXR – exclude pneumothorax / pneumonia ARTERIAL blood gas 12 lead ECG – cardiac monitor if arrhythmia,
HR>120 or known cardiomyopathy Bloods – do not delay NIV to await results
Respiratory Acidosis?
pH < 7.35
pCO2 > 6.5 RR > 23
STOP! Consider alternative
diagnosis/ management
Consider NIV - Use NIV decision tree & complete
pathway.
YES
NO
NIV is not indicated for pneumonia or life threatening asthma - refer to ITU for consideration of intubation if pCO2 >6.5 and pH <7.35 or worsening respiratory distress.
NIV is not indicated for treatment of metabolic acidosis (or metabolic part of acidosis), check BASE EXCESS and consider alternative diagnosis/management.
Absolute NIV contraindications:
Pneumonia
Asthma
Severe facial deformity
Facial or upper airway burns
Fixed upper airway obstruction
Relative NIV contraindications:
Untreated pneumothorax
Recent upper GI or craniofacial surgery
Vomiting / aspiration risk
Bowel obstruction (consider NGT)
pH ≤7.15 (or <7.25 and additional adverse features)
GCS ≤ 8, confusion/ agitation, cognitive impairment
Suspected COVID19 – see BSUH NIV COVID pathway
Indications for ICU input:
Acute Hypercapnic Respiratory Failure with impending arrest
IV sedation
Close monitoring
Suspected difficult intubation e.g. Obesity, NMD
Suspected COVID19
Patients with contraindications for ward NIV, or where indication for ICU input is identified:
STOP! Seek senior /ICU advice and/or consider alternative management.
RSCH Med SpR:bleep 8521 PRH Med SpR:bleep 6044 ICU RSCH:bleep 8413 ICU PRH:bleep 6010

Acute Non-Invasive Ventilation Pathway
2
BSUH Acute Non Invasive Ventilation Pathway - 2020 v3.2 – NIV steering group. SH, KD.
Maximum Medical Therapy COPD / bronchiectasis:
Controlled O2 venturi / humidified
Salbutamol nebs 2.5mg QDS
Ipratropium nebs 500mcg QDS
Steroids
If appropriate: Antibiotics
IV broncho-dilators.
Patient Name: …….……………
Trust ID: …….…………………
DoB: ………..…………………
(Attach patient sticker)
for > 1 hour

Acute Non-Invasive Ventilation Pathway
3
BSUH Acute Non Invasive Ventilation Pathway - 2020 v3.2 – NIV steering group. SH, KD.
Step 2: Consent and Escalation planning
Step 3: Referrals
Patient Name: …….……………
Trust ID: …….…………………
DoB: ………..…………………
(Attach patient sticker)
Capacity assessment and best interest decision (if lacking capacity) must be clearly documented in the patient’s health records.
Make and document escalation plan appropriate
for patient in case NIV fails
Refer patient to on call Medical SpR/Consultant
RSCH MedSpR bl 8521 PRH MedSpR bl 6044
Name of senior physician discussed with:
……………………………………………………
Escalation plan:
For intubation/ICU (Level 3 care) For HDU (Level 2 care) For ward-based care For resuscitation Not for resuscitation (DNACPR) Document discussions and use BSUH TEP pro forma All patients suitable for
ICU/HDU commencing NIV should be discussed with
ICU SpR/consultant. RSCH bleep:8413 PRH bleep 6010
Discussed with ICU Document in notes if not accepted for ICU/HDU
Respiratory team referral for all NIV patients in
daytime hours
RSCH bleep:8064 PRH bleep:6048 RSCH resp consultant 8am -5pm 65021
Date/time CCOT contacted:
……………………………………………………
Critical Care Outreach Team referral for ALL
patients starting NIV (24/7)
RSCH bleep:8495 PRH bleep:6331
Date/time respiratory team informed:
……………………………………………………
For ALL motor neurone disease patients starting NIV, please contact NIV consultant Dr Hippolyte during admission. Email: [email protected]
Doctor completing initiation of NIV pathway:
Signature: ……………………………Print Name: ……………………………Date: ……………..
This is required for all patients starting NIV and confirms no contraindications to NIV.

Acute Non-Invasive Ventilation Pathway
4
BSUH Acute Non Invasive Ventilation Pathway - 2020 v3.2 – NIV steering group. SH, KD.
Step 4: Setting up NIV
1. Sit patient up. Prepare patient and explain procedure
2. Set up tubing with bacterial filter and expiratory port (see below)- filter may be alternatively placed between patient mask and expiratory port if risk of cross-infection from expired gases.
3. Choose correct mask size for patient – measure using mask sizing tool
4. Protect nasal bridge with dressing
5. Check all settings and alarms BEFORE connecting patient
6. See troubleshooting guide for all settings and alarms, use S/T mode for BiPAP
7. Connect mask to patient. Aim for leak 25-40, Aim for tidal volume (TV) 400-500ml.
8. Increase IPAP in 1 - 2 cmH2O increments within the first 10-30 mins to achieve target IPAP e.g 20.
9. Monitor SpO2 continuously; titrate FiO2 to achieve SpO2 88-92%
Trilogy 202 BiPAP
Bacterial Filter Expiratory
port
Attach to patient mask
BiPAP
tubing
Patient Name: …….……………
Trust ID: …….…………………
DoB: ………..…………………
(Attach patient sticker)

Acute Non-Invasive Ventilation Pathway
5
BSUH Acute Non Invasive Ventilation Pathway - 2020 v3.2 – NIV steering group. SH, KD.
Blood gas trends (Arterial / Capillary)
Baseline 1 hr post NIV set up
Subsequent trends, consider using capillary blood gases.
ABG/CBG ABG ABG
Date
Time
pH
PaCO2
PaO2
HCO3 (std)
Base Excess(B)
Oxygen Setting %
SpO2
IPAP
EPAP
Resp Rate
Frequency of documented observations on initiation of NIV:
NIV observation frequency
BP, HR, Temperature, RR, SpO2 should be recorded on the BSUH NEWS2 chart / Patient Track. First hour – every 15 minutes 1- 4 hours – every 30 minutes 4- 12 hours – hourly (or more frequently if indicated by NEWS).
Patients require continuous cardiac monitoring if they have HR >120, arrhythmias or known cardiomyopathy. Also note chest wall movement, ventilator synchrony, accessory muscle use, new confusion/distress and patient comfort – if any concerns escalate for help.
Patient Name: …….……………
Trust ID: …….…………………
DoB: ………..…………………
(Attach patient sticker)
If frequent ABGs required consider capillary blood gas samples or HDU referral for arterial line.

Acute Non-Invasive Ventilation Pathway
6
BSUH Acute Non Invasive Ventilation Pathway - 2020 v3.2 – NIV steering group. SH, KD.
Step 5: Assessing response and weaning of NIV *Avoid changing EPAP without senior advice.
After 1 hour NIV at target settings / if acute changes Review patient and check ABG
Is the pCO2 improving?
Are there any red flags or features of instability?
pH<7.25 on optimal NIV settings
RR persisting > 25
New onset of confusion /distress
Requiring EPAP > 6 *
Timed breaths (patient not spontaneously breathing)
Check mask fit/leak, synchronisation, exhalation port present & not blocked.
Consider further broncho-dilators, anxiolytics.
Chest physio
Check ABG
Increase IPAP in 1-2 cmH2O increments (seek senior help if
IPAP >26).
Continue current settings.
Review ABG in 2-4 hours if patient stable
If simple measures are not helping:
Escalate to senior and consider ITU review
Re-check ABG after 1hr if patient stable
NO
Once pH resolved Further ABGs not routinely required
Consider weaning
(see below).
Seek senior support if pCO2 and pH not
improving.
YES
NIV weaning guide
Patients should be encouraged to use NIV continuously in the first 24 hours (allowing for small breaks for drinks if tolerated e.g. 5 -10 minutes). As blood gases improve, time on NIV during the daytime may be reduced. During initial weaning the patient should have NIV continuously overnight. E.g. Day 0: Continuous NIV with short breaks for drinks. Day 1: 1 hour off (am); 2 hrs off (pm), on at night, Day 2: 3- 4 hours off (am) and 4 hours off (pm), Day 3: off all day, on at night. If the patient requires oxygen whilst off NIV this should be administered via nasal specs or controlled venturi /humidified O2 according to target saturations.
If frequent ABGs required consider capillary blood gas samples or HDU referral for arterial line.
Patient Name: …….……………
Trust ID: …….…………………
DoB: ………..…………………
(Attach patient sticker)

Acute Non-Invasive Ventilation Pathway
7
BSUH Acute Non Invasive Ventilation Pathway - 2020 v3.2 – NIV steering group. SH, KD.
Monitoring and weaning of NIV therapy:
Day 0: Date……………………. Medical review and plan:
Time Nursing evaluation of NIV therapy
Time BiPAP initiated …..:…. Increase settings over 10-30mins as per NIV pathway or individual SpR/consultant plan. ABG due after 1 hour of BiPAP @ …..:…. Document observations on NEWS2 chart; 15 mins for first hour, 30mins for next 3 hours, then hourly.
Action Nurse to Sign & date/time every time
BiPAP applied
Visually inspect circuit
Check settings
Check alarms
BiPAP prescribed
Time 24 hr clock
00:0
0
01:0
0
02:0
0
03:0
0
04:0
0
05:0
0
06:0
0
07:0
0
08:0
0
09:0
0
10:0
0
11:0
0
12:0
0
13:0
0
14:0
0
15:0
0
16:0
0
17:0
0
18:0
0
19:0
0
20:0
0
21:0
0
22:0
0
23:0
0
IPAP
EPAP
Oxygen %
RR
MV (est)
TV (est)
Back up rate
Leak
Rise time
NIV Break
Oral care
Patient Name: …….……………
Trust ID: …….…………………
DoB: ………..…………………
(Attach patient sticker)

Acute Non-Invasive Ventilation Pathway
8
BSUH Acute Non Invasive Ventilation Pathway - 2020 v3.2 – NIV steering group. SH, KD.
Monitoring and weaning of NIV therapy: Day 1: Date……………………. Medical review and plan:
Time Nursing evaluation of NIV therapy
Document observations on NEWS2 chart
Action Nurse to Sign & date/time every time
BiPAP applied
Visually inspect circuit
Check settings
Check alarms
BiPAP prescribed
Time 24 hr clock
00:0
0
01:0
0
02:0
0
03:0
0
04:0
0
05:0
0
06:0
0
07:0
0
08:0
0
09:0
0
10:0
0
11:0
0
12:0
0
13:0
0
14:0
0
15:0
0
16:0
0
17:0
0
18:0
0
19:0
0
20:0
0
21:0
0
22:0
0
23:0
0
IPAP
EPAP
Oxygen %
RR
MV (est)
TV (est)
Back up rate
Leak
Rise time
NIV Break
Oral care
Patient Name: …….……………
Trust ID: …….…………………
DoB: ………..…………………
(Attach patient sticker)

Acute Non-Invasive Ventilation Pathway
9
BSUH Acute Non Invasive Ventilation Pathway - 2020 v3.2 – NIV steering group. SH, KD.
Monitoring and weaning of NIV therapy:
Day 2: Date……………………. Medical review and plan:
Time Nursing evaluation of NIV therapy
Document observations on NEWS2 chart
Action Nurse to Sign & date/time every time
BiPAP applied
Visually inspect circuit
Check settings
Check alarms
BiPAP prescribed
Time 24 hr clock
00:0
0
01:0
0
02:0
0
03:0
0
04:0
0
05:0
0
06:0
0
07:0
0
08:0
0
09:0
0
10:0
0
11:0
0
12:0
0
13:0
0
14:0
0
15:0
0
16:0
0
17:0
0
18:0
0
19:0
0
20:0
0
21:0
0
22:0
0
23:0
0
IPAP
EPAP
Oxygen %
RR
MV (est)
TV (est)
Back up rate
Leak
Rise time
NIV Break
Oral care
Patient Name: …….……………
Trust ID: …….…………………
DoB: ………..…………………
(Attach patient sticker)

Acute Non-Invasive Ventilation Pathway
10
BSUH Acute Non Invasive Ventilation Pathway - 2020 v3.2 – NIV steering group. SH, KD.
Monitoring and weaning of NIV therapy:
Day 3: Date……………………. Medical review and plan:
Time Nursing evaluation of NIV therapy
Document observations on NEWS2 chart
Use additional pages as required.
Action Nurse to Sign & date/time every time
BiPAP applied
Visually inspect circuit
Check settings
Check alarms
BiPAP prescribed
Time 24 hr clock
00:0
0
01:0
0
02:0
0
03:0
0
04:0
0
05:0
0
06:0
0
07:0
0
08:0
0
09:0
0
10:0
0
11:0
0
12:0
0
13:0
0
14:0
0
15:0
0
16:0
0
17:0
0
18:0
0
19:0
0
20:0
0
21:0
0
22:0
0
23:0
0
IPAP
EPAP
Oxygen %
RR
MV (est)
TV (est)
Back up rate
Leak
Rise time
NIV Break
Oral care
Patient Name: …….……………
Trust ID: …….…………………
DoB: ………..…………………
(Attach patient sticker)















![arXiv:2001.08817v1 [cs.LG] 23 Jan 2020 · three different critical findings (pneumothorax, pneumonia, and pulmonary edema) from three different CXR datasets. Index Terms— chest](https://static.fdocuments.us/doc/165x107/5fb3fa175cfeae2d5f16acdc/arxiv200108817v1-cslg-23-jan-2020-three-different-critical-indings-pneumothorax.jpg)
