
STEMI System Hospital Orientation Self Studycchealth.org/ems/pdf/stemi_hosp_orient_selfstudy.pdf ·...
41
Contra Costa County Emergency Medical Services STEMI System Hospital Orientation Self Study June 2008
-
Upload
vuongkhanh -
Category
Documents
-
view
223 -
download
0
Transcript of STEMI System Hospital Orientation Self Studycchealth.org/ems/pdf/stemi_hosp_orient_selfstudy.pdf ·...

Contra Costa CountyEmergency Medical
Services
STEMI System Hospital Orientation
Self Study
June 2008

Contra Costa County STEMI Hospital Training
LESSON PLAN
COURSE: “STEMI System Hospital Orientation”
Overview of STEMI Center designation/destination for Contra Costa County.
Audience: Emergency department and STEMI program support personnel including physicians, nurses, cardiac cath lab personnel. This program may be adapted and is designed as a tool for use at all emergency departments in Contra Costa County.
TOPIC: STEMI System Orientation Educational Approach: This training may be accomplished using a variety of
strategies. Traditional lecture presentation or adapted to self study. If adapted to self study it is recommended that post-test questions be developed specific to the facility.
OBJECTIVES: At the completion of the training session, the student will be
able to:
1. Identify why STEMI Centers are necessary. 2. Identify requirements for a STEMI Center.
3. Identify triage and destination goals for patients with chest
pain in Contra Costa County.
4. Identify how your Emergency Department patient intake changes in a STEMI system.
5. Describe how EMS providers identify STEMI patients in the
field.
6. Describe EMS communication to be included in a radio and hospital report of a patient with a STEMI.
7. Identify appropriate hand off of 12-lead ECG to hospital
personnel.
8. Accurately describe Emergency Department personnel role in facilitating triage of EMS STEMI-Alert patients.
9. Describe the benefits and challenges of STEMI systems.
MATERIALS NEEDED: Projection Screen
LCD Projector Laptop/Computer with PowerPoint Presentation: "STEMI System Hospital Orientation" Handouts -
PowerPoint Presentation - "STEMI System Hospital Orientation” CCC EMS Policy #25 – “STEMI Triage and Destination” CCC EMS Policy #26- “STEMI Receiving Center Designation” Contra Costa County STEMI Hospital Training Post-test and annotated answer key
References: All educational resources are available at our EMS website at : www.cccems.orgSTEMI Contra Costa County Health Services Prehospital Care Manual Contra Costa County Health Services EMS Policies and Procedures Please contact EMS if you have questions about this training.

1
STEMI STEMI SYSTEMSYSTEM
HOSPITALHOSPITALORIENTATIONORIENTATION
June 2008June 2008
Contra Costa Emergency Medical ServicesContra Costa Emergency Medical Services
•This powerpoint provides a basic introduction to Contra Costa County STEMI System to be implemented in the Fall of 2008•For questions contact Contra Costa EMS Medical Director Joe Barger MD or QI Coordinator and STEMI Project Manager Pat Frost RN, MS, PNP•Definitions:•STEMI stands for ST Elevation Myocardial Infarction. A particular type of Acute Myocardial Infarction (AMI) that can be quickly diagnosed by 12 lead ECG machine in the field by EMS providers. •STEMI Systems refer to a network of prehospital, emergency departments and cardiac intervention resources that are created to “fast track” patients having “STEMIs” to definitive care.•STEMI Receiving Centers are hospitals designated by Contra Costa County EMS with cardiac capabilities, (cardiac catheterization, laboratory and/or cardiovascular surgery), designed to provide rapid intervention for STEMI patients 24/7/365 days a year.
2
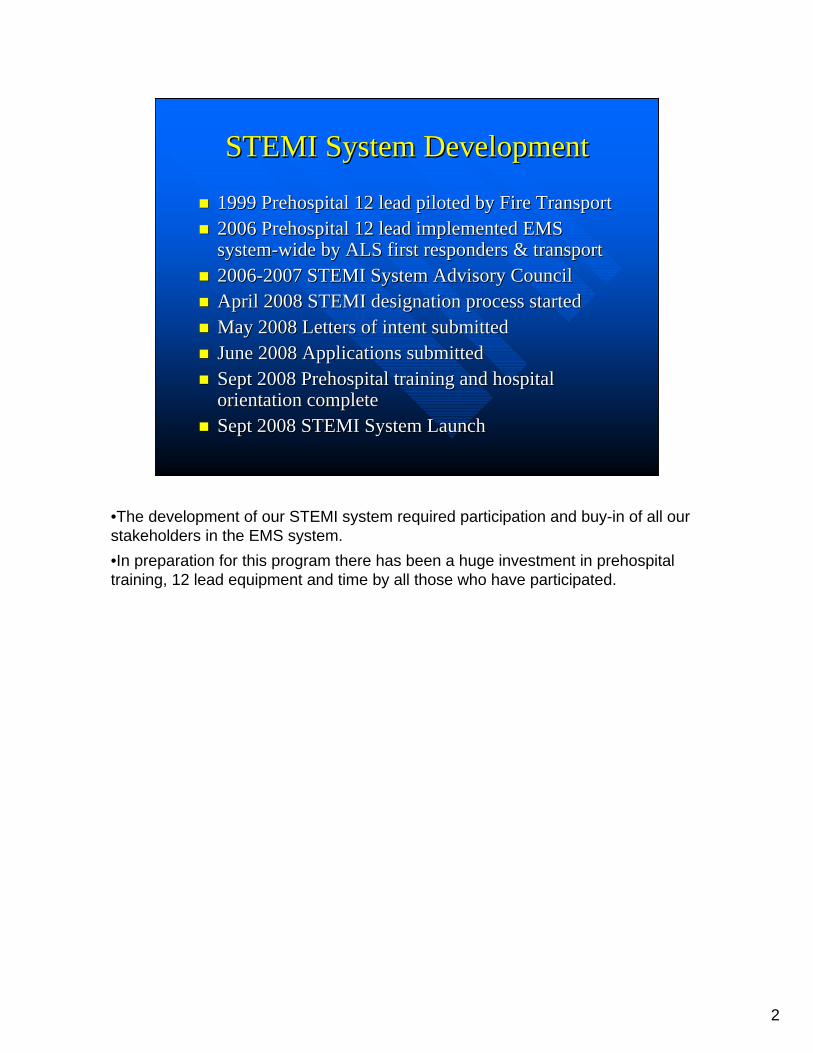
STEMI System DevelopmentSTEMI System Development
1999 Prehospital 12 lead piloted by Fire Transport1999 Prehospital 12 lead piloted by Fire Transport2006 Prehospital 12 lead implemented EMS 2006 Prehospital 12 lead implemented EMS systemsystem--wide by ALS first responders & transportwide by ALS first responders & transport20062006--2007 STEMI System Advisory Council2007 STEMI System Advisory CouncilApril 2008 STEMI designation process startedApril 2008 STEMI designation process startedMay 2008 Letters of intent submittedMay 2008 Letters of intent submittedJune 2008 Applications submittedJune 2008 Applications submittedSept 2008 Prehospital training and hospital Sept 2008 Prehospital training and hospital orientation completeorientation completeSept 2008 STEMI System LaunchSept 2008 STEMI System Launch
•The development of our STEMI system required participation and buy-in of all our stakeholders in the EMS system.•In preparation for this program there has been a huge investment in prehospital training, 12 lead equipment and time by all those who have participated.

3
What’s New…What’s New…STEMI Centers Are Almost Here!STEMI Centers Are Almost Here!
STEMI Triage and Destination Policy begins– Sufficient STEMI
center approval– Anticipate Fall 2008
STEMI patients to STEMI Centers
•The good news….STEMI Centers Are Almost Here!•STEMI Triage and Destination Policy will begin when Centers are approved and ready to go – anticipate September 2008. We have a tentative launch date of Sept 8, 2008 but this could be delayed due to the time it takes contracts to be completed.•If we have at least 3 hospitals through the designation process we will be launching the system on target. If not then we will push back our start date until we do.•Will begin to transport STEMI patients specifically to STEMI Centers

4
STEMI CentersSTEMI Centers
Hospitals requirements– Personnel, Policy,
Equipment Requirements
– Contract with EMS
24/7/365 cath lab capability– No STEMI diversion
process
•Hospitals must meet requirements and enter into contract with EMS•Personnel, Policy, Equipment Requirements
•Will provide 24/7/365 cath lab capability -- - no diversion process
5
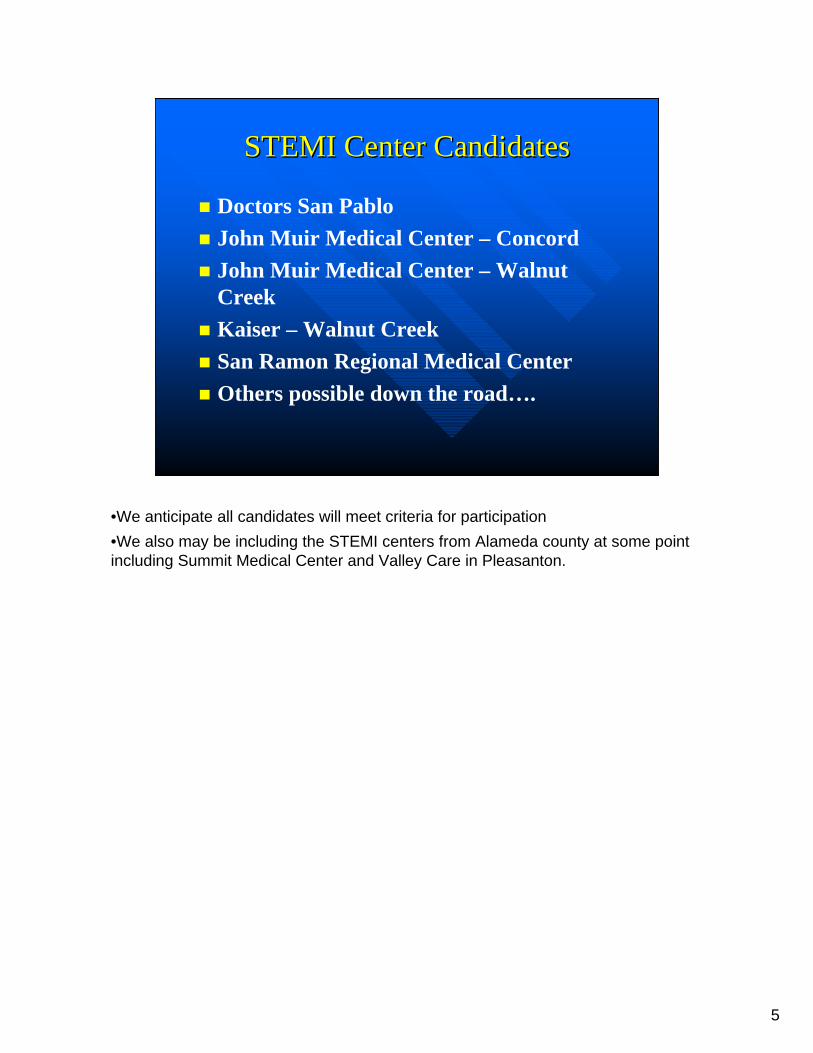
STEMI Center CandidatesSTEMI Center Candidates
Doctors San PabloJohn Muir Medical Center – ConcordJohn Muir Medical Center – Walnut CreekKaiser – Walnut CreekSan Ramon Regional Medical CenterOthers possible down the road….
•We anticipate all candidates will meet criteria for participation•We also may be including the STEMI centers from Alameda county at some point including Summit Medical Center and Valley Care in Pleasanton.

6
STEMI Triage and DestinationSTEMI Triage and DestinationNew EMS Destination policyApplies only to STEMIs identified by 12 lead.Other messages– Do not qualify as
STEMI– Do not merit
transport to STEMI Center
(Zoll) ** * ACUTE MI * ** (Zoll) ** * ACUTE MI * **
(LP(LP--12)***ACUTE MI SUSPECTED*** 12)***ACUTE MI SUSPECTED***
•New EMS Policy. (Distribute policy and review at the time of training)•Applies only to STEMIs identified by 12 lead.•Prehospital uses Zoll 12 lead and LP-12 (physiocontrol monitor) that “diagnoses rhythm”. Prehospital providers do not make the 12 lead interpretation decision. Machine generated.•Other messages – e.g., possible MI, possible ischemia, MI age undetermined do not qualify as STEMI and do not merit transport to STEMI Center

7
STEMI Triage and DestinationSTEMI Triage and Destination
1212--lead needs to be rapidly obtained lead needs to be rapidly obtained –– Acceptable quality Acceptable quality
»» good QRS in all 12 leads good QRS in all 12 leads »» no significant artifactno significant artifact
STEMI determined by 12 leadSTEMI determined by 12 lead–– Determine destination Determine destination –– Contact of STEMI center ASAP Contact of STEMI center ASAP –– Do not wait Do not wait
STEMI Report needs to give critical STEMI Report needs to give critical information to hospitalinformation to hospital
•This is what we want to happen in the field. However we know that there are no perfect circles and this may not happen everytime so that is why there is a STEMI QI review process involved. At the hospital all STEMI issues should go through the STEMI RN project manager for your facility if you are a STEMI center and if you are not be sent to EMS through your nurse manager using EMS event reporting (patient safety reporting system). Forms are available at cccems.org under EMS Event Reporting.•.•12-lead needs to be rapidly obtained
•Must be of acceptable quality with good QRS complexes in all 12 leads and no significant artifact•Once obtained destination needs to be determined and contact of STEMI center should happen as soon as possible (do not wait until ready for transport or after departure)•STEMI Report needs to give critical information to hospital
8
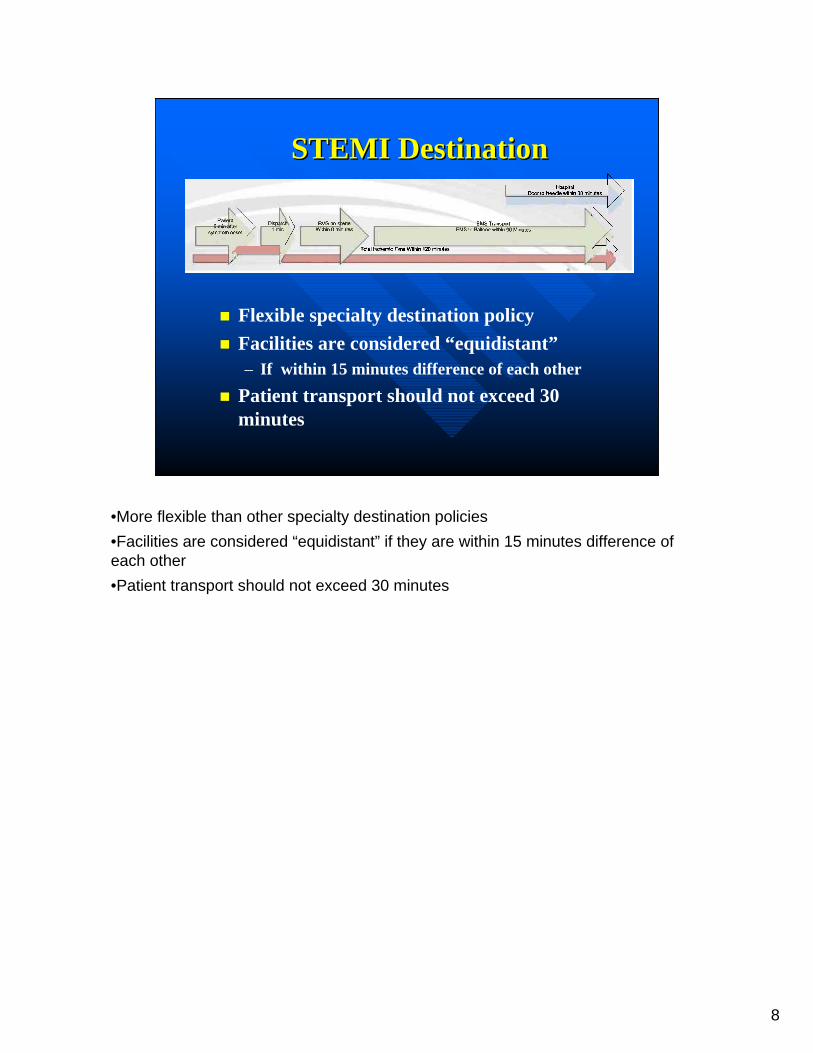
STEMI DestinationSTEMI Destination
Flexible specialty destination policyFacilities are considered “equidistant” – If within 15 minutes difference of each other
Patient transport should not exceed 30 minutes
•More flexible than other specialty destination policies•Facilities are considered “equidistant” if they are within 15 minutes difference of each other•Patient transport should not exceed 30 minutes

Hos
pita
lD
oor t
o N
eedl
e w
ithin
30
min
utes
Ons
et o
f sy
mpt
oms
of S
TEM
I
9-1-
1 E
MS
D
ispa
tch
EM
S o
n-sc
ene
12-L
ead
EC
Gs
STE
MI A
lert
Not
PC
I Cap
able
Hos
pita
l
PC
I Cap
able
S
TEM
I Rec
eivi
ng
Cen
ter
EM
S
Tria
ge
Pla
n
Inte
r-Hos
pita
l Tr
ansf
er
Cal
l 9-1
-1C
all F
ast
Tota
l Isc
hem
ic T
ime
With
in 1
20 m
inut
es
Pat
ient
5 m
in a
fter
sym
ptom
ons
et
Dis
patc
h1
min
EM
S o
n sc
ene
With
in 8
min
utes
EM
S T
rans
p ort
EM
S to
Bal
l oon
with
in 9
0 M
inu t
es
Ada
pted
from
: Ant
aman
, et.
al. “
Man
agem
ent o
f Pat
ient
s w
ith S
TEM
I: E
xecu
tive
Sum
mar
y” C
ircul
atio
n, O
ct. 2
007
at
http
://ci
rc.a
hajo
urna
ls.o
rg/c
gi/c
onte
nt/fu
ll/11
0/5/
588

9
STEMI STEMI DestinationDestination
When no STEMI Center within 30 minutes, (e.g. far east county) patient should be transported to closest basic ED facility
Patients retain right to choose destination, whether it is a STEMI Center or not
Patients without preference should go to closest STEMI Center
•When no STEMI Center within 30 minutes, (e.g. far east county) patient should be transported to closest basic ED facility
•Patients retain right to choose destination, whether it is a STEMI Center or not.
•Patients without preference should go to closest STEMI Center
10
STEMI DestinationSTEMI DestinationReason for Flexibility on DestinationReason for Flexibility on Destination
Gets patient to their desired facility and physicianCath lab startup is most time-consuming step ED arrival delay does not impact final time to cath lab or intervention
•Reason for flexibility on destination:•Get patient to their desired facility and physician•Cath lab startup is most time-consuming step and if it takes a while to get to the ED the delay does not impact final time to cath lab or intervention as the cath lab takes awhile to get set up
11
Example: East Contra Costa CountyExample: East Contra Costa County
Page 1
STEM I DESTINATIO N CHO ICES EAST CO UNTYTuesday , M ay 27, 2008
STEM I PATIEN T
W ITHIN 30 M IN U TES O F
STEM I CEN TER ?
C H O IC ESJO H N M U IR M EDIC AL C EN TER -CO N CO R D
KAISER -W ALN U T C R EEKJO HN M U IR M ED IC AL C EN TER -W ALN UT
CR EEKYES
CHO ICESK AISE R ANTIO CH
S UTTER D ELTA
NO
C O M M EN TSFor Patients w ith in 30 m inutes o f STEM I Center: John M uir Concord is the c losest, but if patient requests one of the others and transport is w ithin 30 m inutes those options are availab le . The W alnut C reek hospita ls m ay not be appropria te in heavy tra ffic tim es , and would be m ore applicable from closer vic inities (e .g . Bay Point, P ittsburg). Patients m ay request local non -STEM I facilities , but the param edic should exp lain rationale for transport to STEM I center and a llow forpatient decision and docum ent .
For Patients greater than 30 m inutes from STEM I Center: C losest fac ility by transport tim e is best but if reasonably equal in transport tim e allow ing choice is appropriate (as we would norm ally do ). Som e patients m ay insist on a particular destination . In those cases docum ent patient dec ision .
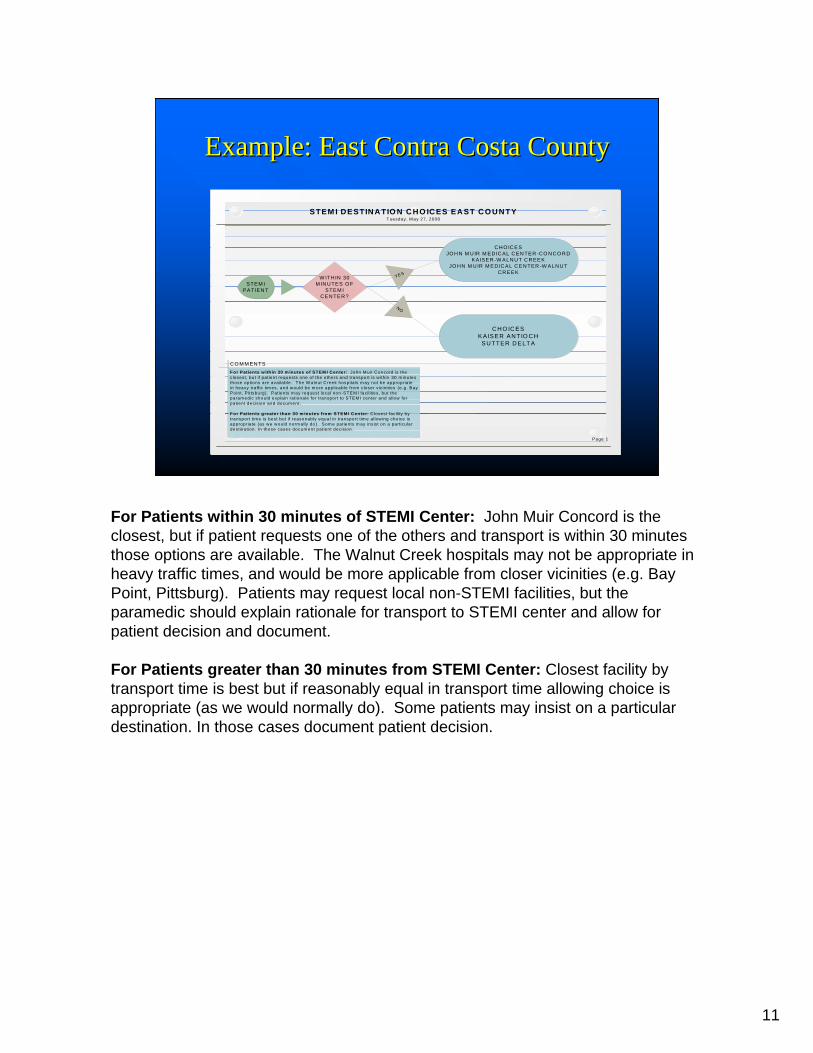
For Patients within 30 minutes of STEMI Center: John Muir Concord is the closest, but if patient requests one of the others and transport is within 30 minutes those options are available. The Walnut Creek hospitals may not be appropriate in heavy traffic times, and would be more applicable from closer vicinities (e.g. Bay Point, Pittsburg). Patients may request local non-STEMI facilities, but the paramedic should explain rationale for transport to STEMI center and allow for patient decision and document.
For Patients greater than 30 minutes from STEMI Center: Closest facility by transport time is best but if reasonably equal in transport time allowing choice is appropriate (as we would normally do). Some patients may insist on a particular destination. In those cases document patient decision.

STEM
I DES
TIN
ATI
ON
CH
OIC
ES E
AST
CO
UN
TYW
edne
sday
, May
07,
200
8
STE
MI
PA
TIE
NT
WIT
HIN
30
MIN
UTE
S O
F S
TEM
I C
EN
TER
?
CH
OIC
ES
JOH
N M
UIR
ME
DIC
AL
CE
NTE
R-C
ON
CO
RD
KA
ISE
R-W
ALN
UT
CR
EE
KJO
HN
MU
IR M
ED
ICA
L C
EN
TER
-WA
LNU
T C
RE
EK
YES
CH
OIC
ES
KA
ISE
R A
NTI
OC
HS
UTT
ER
DE
LTA
NO
CO
MM
EN
TSFo
r Pat
ient
s w
ithin
30
min
utes
of S
TEM
I Cen
ter:
Joh
n M
uir C
onco
rd is
the
clos
est,
but i
f pat
ient
requ
ests
one
of t
he o
ther
s an
d tra
nspo
rt is
with
in 3
0 m
inut
es
thos
e op
tions
are
ava
ilabl
e. T
he W
alnu
t Cre
ek h
ospi
tals
may
not
be
appr
opria
te
in h
eavy
traf
fic ti
mes
, and
wou
ld b
e m
ore
appl
icab
le fr
om c
lose
r vic
initi
es (e
.g. B
ay
Poi
nt, P
ittsb
urg)
. P
atie
nts
may
requ
est l
ocal
non
-STE
MI f
acilit
ies,
but
the
para
med
ic s
houl
d ex
plai
n ra
tiona
le fo
r tra
nspo
rt to
STE
MI c
ente
r and
allo
w fo
rpa
tient
dec
isio
n an
d do
cum
ent.
For P
atie
nts
grea
ter t
han
30 m
inut
es fr
om S
TEM
I Cen
ter:
Clo
sest
faci
lity
by
trans
port
time
is b
est b
ut if
reas
onab
ly e
qual
in tr
ansp
ort t
ime
allo
win
g ch
oice
is
appr
opria
te (a
s w
e w
ould
nor
mal
ly d
o).
Som
e pa
tient
s m
ay in
sist
on
a pa
rticu
lar
dest
inat
ion.
In th
ose
case
s do
cum
ent p
atie
nt d
ecis
ion.

12
What happens to patients who do not What happens to patients who do not go directly to a STEMI Center?go directly to a STEMI Center?
First line treatment First line treatment for MI.for MI.Rapid triage to Rapid triage to STEMI CenterSTEMI CenterInterfacility Interfacility critical critical care transportcare transport
•Patients may enter the STEMI system through a non-STEMI center in a number of ways:•First the patient always has a choice although they are advised of what resources we have available in our STEMI system. That choice has to be respected. •Second due to our current system limitations they may be too far away from a STEMI center such as in East County at certain times of the day. Eventually EMS hopes that STEMI Center resources will also open up in those areas but those decisions are up to the hospitals in those areas.•Third patients may walk into a non-STEMI center. All STEMI Centers are required to accept patients from non-STEMI centers and work with those facilities to create effective mechanisms for rapid transport.•Finally the non-STEMI centers are capable of administering first line therapy totreat MI’s as they do and have done for many years prior to triaging the patient to a STEMI center.

13
Radio Report Radio Report -- SBARSBARSSituationituation– “STEMI Alert” confirmed by 12 lead
» ** ACUTE MI** (ZOLL)» ***ACUTE MI SUSPECTED*** (LP-12)
– ETA– Patient Age and Gender
•We have chosen to use SBAR a best practice reporting system to assure effective communication during radio and bedside report. •SBAR has been adapted to meet the field needs of prehospital but is essentially the same as what you do in the hospital. •It brings urgent essential information to the forefront to assure things do not get missed.•SBAR is a new concept to EMS and it will take time for prehospital providers to “get it down”. •Please support them with constructive feedback.

14
Radio Report Radio Report -- SBARSBARBBackgroundackground– Presenting Complaint– Past Cardiac History– History of pacemaker
•Pacemakers are included since pacer spikes can interfere with the reliability of the machine interpretation. •A variable we have to deal with as part of the system.

15
Radio Report Radio Report -- SBARSBARAAssessmentssessment– Stable or unstableIf unstable If unstable –– whywhy– Vital Signs– Shock; SOB; ALOC– Uncontrolled Pain
•The medic should provide you with this information.
16
Radio Report Radio Report -- SBARSBAR
RRx & x & RRecapecap– Treatments Given – Patient Response
•This is where the SBAR report is a little different for prehospital providers than how it is used in the hospital. •For EMS the R in SBAR stands for RX which means treatment and Recap of patient response. In the hospital it means Recommendation.

17
Report at Hospital Report at Hospital –– SBAR should include:SBAR should include:
SSituationituation repeated including patient identification repeated including patient identification with urgent concerns up front.with urgent concerns up front.
BBackgroundackground repeated including past history if repeated including past history if known (e.g. history of MI, clot busters, cath, or known (e.g. history of MI, clot busters, cath, or surgery, cardiologist). High risk medications surgery, cardiologist). High risk medications (especially anticoagulants, insulin, erectile (especially anticoagulants, insulin, erectile dysfunction drugs), allergies, advanced directivesdysfunction drugs), allergies, advanced directives
AAssessment ssessment repeated pertinent VS, ALOC Pain levelrepeated pertinent VS, ALOC Pain levelRRx/Recapx/Recap PrehopsitalPrehopsital treatments given and patient treatments given and patient
response. Concerns repeated and questions response. Concerns repeated and questions addressedaddressed
•SBAR should also be used during patient handoff report at the bedside. •Some of the information may not be known to the medic but if it is they will tell you. Example: the name of cardiologist.•Although this might look a little different from your hospital SBAR report in print, since the SBAR report flows like a conversation you should not notice a big difference between how prehospital uses SBAR and how you use it.

18
1212--Lead ECGLead ECGFirst responders doing 12-lead– Provide 2 copies for transport
» Hospital» Transport Agency Pt Record
Provide copy of 12-lead to ED– Include multiple if done
Hand directly to nurse caring for patient
•We direct the prehospital providers to give the ED the following….but we know that in the excitement of getting the patient to the cath lab patient care records and 12 leads get lost. We need your help to assure these documents stay with the patient and get into the patients record. This part is hard because it really depends on each individual double checking. The STEMI hospital coordinators and EMS will have QI processes in place to track down 12 leads after the fact but that defeats the purpose of having the 12 lead available at the time the patient needs it.•A copy of 12-lead must be left at ED (if multiple valid tracings are done, all should be left)•First responders doing 12-lead should provide 2 copies for transport (one for hospital and one for transport agency)•The field personnel giving report to the hospital on arrival should hand the 12 lead directly to the nurse caring for patient•Copy of 12-lead should be submitted to your agency if not uploaded into record

19
DocumentationDocumentationAll electronic PCR systems have documentation specifically for 12-lead performance and readingePCR documentation is very important whether STEMI or notCan’t evaluate STEMI system performance without this!
•EMS has a very strong emphasis on documentation of these events in the field.•All electronic PCR systems have documentation specifically for 12-lead performance and reading.•But documentation depends on people being conscientious and complete.•Documentation can still be omitted in some cases and we will be working with our prehospital providers to consistently improve this.•Why? Because it is a very important issue to document for overall system review whether STEMI or not.

20
1212--Lead Experience with STEMILead Experience with STEMI
3-4% of ECG’s show STEMIMany tremendous casesDoor-to-balloon (intervention) has been reduced to under 60 minutes in many casesE2B (911 call time to intervention) has been under 90 minutes on occasion
•Share STEMI newsletter “STEMI NEWS” here. •Goal is to publish twice a year and audience is all our stakeholders to keep them informed of our STEMi program process.•Why? Because when we all understand our roles and responsibilities excellence in patient care is supported.

21
1212--Lead Experience with STEMILead Experience with STEMI
Several instances where initial ECG is abnormal but second ECG confirms MI
Leaving leads on and repeating ECG is appropriate
•These are some of the issues we do know about and are educating our prehospital providers on.

22
1212--Lead Lessons LearnedLead Lessons Learned
Skin Prep remains the single most important issue in getting good tracing
Another example of what we emphasize during training of our prehospital providers.

23
1212--Lead Lessons LearnedLead Lessons Learned
Quality of ECG’s has markedly increased since startupStill have occasional issues with artifact or incomplete ECG or incorrect lead placementAll 12 leads must have readable complexes with stable baseline
•Important to know that if the Lifepak 12 (type of ECG machine) is left on the patient it will continue to assess the patient and print out another 12 lead if there is a change in the ECG reading.•We have 2 different types of ECG machines currently being used by different EMS agencies.•The average false positive rate for prehospital 12 leads is about 20% when looking at STEMI systems that are established.

24
1212--Lead Lessons LearnedLead Lessons Learned
Scene Times– STEMIs < chest
pain – Average 13-14 min
Some cases >20 min– Want to minimize
•Scene Times in STEMI cases are shorter than chest pain overall – average 13-14 minutes•Still some cases over have scene times >20 minutes – want to minimize this •QI program coordinators in each of our EMS provider agencies, our STEMI RN program managers and EMS will be working together to capture this information and work to shorten our times and do our best to eliminate delays. •We need your cooperation to getting information to the appropriate parties and working cooperatively giving positive and constructive feedback so we can improve.

25
1212--Lead Lessons LearnedLead Lessons LearnedFalse positive rate around 20% Issue: ECG says **Acute MI** but is NOTREASON: – Baseline artifact most
common cause– Tachycardia may fool
machine– Paced rhythms
•False positive readings around 20% •ECG says **Acute MI** but is NOT
•Baseline artifact most common cause•Tachycardia may fool machine•Paced rhythms
•Show false positive cases. Occasionally computer reading is just wrong despite no artifact or other finding (rare)

26
1212--Lead Lessons LearnedLead Lessons Learned
Most younger 12-lead patients with STEMI’s have presented with chest pain
Atypical presentations seen occasionally in older patients, diabetics and women.
•Atypical presentations have been weakness, syncope, SOB

27
AtypicalAtypical PresentationsPresentationsWho is at risk?Who is at risk?–– Diabetics….Women…..ElderlyDiabetics….Women…..Elderly
Chest pain may not be their chief complaintChest pain may not be their chief complaint–– Shortness of BreathShortness of Breath–– Nausea & Abdominal discomfort Nausea & Abdominal discomfort –– Weakness or SyncopeWeakness or Syncope–– Neck, jaw, shoulder or upper back pain.Neck, jaw, shoulder or upper back pain.–– IndigestionIndigestion–– Unexplained FatigueUnexplained Fatigue
•Diabetics and the Elderly experience pain differently and may not report “classic symptoms” of Acute Coronary Syndrome (ACS).•Women also present frequently with atypical symptoms. •These symptoms can occur in combination or be isolated. •Sometimes atypical patients are difficult to pick up in the field. •Be alert for these patients if they are brought to you from EMS and were not assessed as a potential ACS. •Not all STEMI’s are picked up in the field!

28
Overall ExperienceOverall ExperienceEven without a STEMI system in place we have had good success Prehospital has made a difference in decreasing time to intervention in many cases.We look forward to doing even more !
•Over the last two years we have had an informal STEMI program in place. •EMS has helped many hospitals decrease time to intervention in many cases and with the STEMI system in place we can do even more. •You will be an active part of that program and because of this we will save even more lives throughout our community!

29
But we need your help….But we need your help….An effective STEMI system relies on good communication!Make sure ECG’s get into the patient’s chart.Give constructive timely feedback.Report issues
•Issues should be reported to your STEMI Program Coordinator & ED Manager.
30
For more information on
Contra Costa EMS STEMI System
visit www.cccems.org
•We look forward to working with you on this important community program.

STEMI References
ACC/AHA, Management of Patients with ST-Elevation Myocardial Infarction, ACC/AHA Pocket Guideline. July 2004. Rokos, I.C., et. al. “Rationale for establishing regional ST-elevation myocardial infarction receiving center (SRC) networks” American Heart Journal, Oct 2006, Vol. 152, Number 4, pp 661-667 Bradley, E. H., et. al. “Strategies for Reducing the Door-to-Balloon Time in Acute Myocardial Infarction.” N Engl J Med, Nov 13, 20006. 355, pp 2308-2320. Moscucci, M. & Eagle, K.A., “Reducing the Door-to-Balloon Time for Myocardial Infarction with ST-Segment Elevation” N Engl J Med, Nov 30, 20006. 355:22, pp 2364-2365. Kostis, W. J., et. al. “Weekend versus Weekday Admission and Mortality from Myocardial Infarction” N Engl J Med, Mar 15, 20007. 356:11, pp 1099-1109. Contra Costa Emergency Medical Services STEMI System Program Information is available on our website at www.cccems.org.

C o n t r a C o s t a E m e r g e n c y M e d i c a l S e r v i c e s
STEMI NEWS Spring 2008
STEMI System Development… We Are Almost There! Contra Costa EMS, in collaboration with all our receiving facilities and EMS providers, has been working diligently over the last year to bring up our STEMI System. We are pleased to report that the process of designating STEMI receiving hospitals is well underway and letters of intent to participate have already been received.
The STEMI Receiving Center designation process and criteria are fully described on our EMS website at www.cccems.org. As letters of intent and applications are received site visits to the facilities will be scheduled. We will be asking each site to include a mock STEMI activation to help us fully appreciate the receiving facilities STEMI system program.
Meetings will soon be scheduled with the RN STEMI program managers for all prospective STEMI Receiving Centers. At these meet-ings we will further define the data and communication workflows that will be so critical to our ability to evaluate the STEMI system. On the prehospital side STEMI System training,including 12 lead review, radio contact and patient handoff guidelines and destination decision making has already begun. That training module is available on our website. Training modules for our emergency departments are also planned. EMS will be working with our hospitals to provide these training modules for both for Non-STEMI and STEMI designated facilities. Our goal is to have everyone on the same page when the system goes live in the Fall. At this point the launch date to bring the system up is September 2008. Delays could occur due to contractual requirements but at this time it appears we are on target!
The STEMI Advisory Committee and EMS looked at STEMI systems across the country and sought the advice of STEMI System experts throughout California to create our STEMI destination policy. The draft policy is available on our website. In our system, STEMI destination is designed to be more flexible than other specialty destination policies and STEMI Receiving Facilities will be considered “equidistant” if the difference between travel times is less than 15 minutes. This concept allows us to meet the national standards of EMS transport times of 30 minutes or less and 9-1-1 to needle/balloon times of less than 90 minutes.
The reason for the flexibility on destination is to get the patient to his/her desired facility and physician. After reviewing our current system and evaluating what we learned from other STEMI systems we believe these differences should not impact the final time to cath lab intervention.
In cases where there is no STEMI Center within 30 minutes, patients should be transported to the closest basic ED facility. Patients retain the right to choose destination in our EMS system….whether it is a STEMI Center or not. Patients without a preference should go to the closest STEMI Center. Once our STEMI Center designation process is finalized, destination patterns will be more clear. At this time we anticipate at least four STEMI Centers participating in our program and there could be more down the road.
Contra Costa Emergency Medical Services Agency www.cccems.org
Contra Costa STEMI Center Candidates As of May 1, 2008 the following facilities have filed a letter of intent to become STEMI Centers: • Doctor’s San Pablo Medical Center • John Muir Medical Center-Concord • John Muir Medical Center-Walnut Creek • Kaiser Medical Center-Walnut Creek • San Ramon Regional Medical Center
STEMI Destination: How It Will Work….

Contra Costa Emergency Medical Services Agency www.cccems.org
STEMI NEWS Prehospital 12 lead Program poised for STEMI System Implementation Bringing up a STEMI System is not a small task. The planning and preparation is enormous. Our prehospital first responders and transport providers have worked hard to fully implement our prehospital 12 lead program and have many responsibilities in making the STEMI system work. Their hard work has positioned our EMS system to effectively implement this new program and allowed us to understand and better anticipate what will happen when we bring our EMS system up. STEMI Facts • Scene times in STEMI are shorter than chest
pain overall & average 13-14 minutes. • There are rare cases of >20 minute scene
times and we are working with our prehospital providers to eliminate these cases.
• 3-4% of 12 lead ECG’s show STEMI. • False positives run about 20% where the ECG
says ***Acute MI*** . A 20% false positive rate is typical for most STEMI systems.
• False positives are most commonly caused by baseline artifact.
• Skin prep remains the single most important issue in getting a good tracing.
• Paced rhythms and some tachycardias can fool the diagnostics of the 12 lead ECG machine but this is rare.
• Many tremendous cases where door to balloon time has been reduced to under 60 minutes.
• Occasional cases of 911 call time to intervention under 90 minutes! Our prehospital providers are all committed to making the system work and will continue to be actively involved in improving the process as we move forward. In the upcoming STEMI system the EMS partnership between field and hospital will allow us to accomplish even more.
Communication Critical to Upcoming STEMI System Success
A great STEMI system with great outcomes is dependent on effective communication. The research is clear. The sooner you identify a STEMI and communicate that information to the STEMI Center the better the outcome for the patient. That is why our STEMI Radio Report will be based on a communication model called SBAR (Situation, Background, Assessment, Rx/Recap). SBAR is an evidence based safety communication model that was developed by the military and widely used in many industries make sure the right information gets to the right people in the shortest timeframe. It is what STEMI systems are all about. This model will be used for radio reporting STEMI activations from the field and as part of patient handoff at the STEMI Center. It builds on what people already do and puts urgent patient concerns up front and center. An added plus for our system is that this communication model is being widely used in all of our hospitals throughout the county for patient handoff and critical communications. We are adapting SBAR to make it “work best” for prehospital and are confident it will be effective. The radio report format is below.
Situation •Identify the call as a “STEMI Alert”. •Give ETA, patient age & gender. •State ECG findings & any urgent concerns.
Background •Presenting complaints/symptoms. •Past cardiac history including pacemaker.
Assessment •General impression. •Pertinent vital signs & physical exam. •Pain level.
RX & Recap
•Prehospital treatment given. •Patient response.
STEMI HOSPITAL TRAINING
Contra Costa County Emergency Medical Services
STEMI Hospital Training Post-test
Building a STEMI System is a process and your active participation is invited.
1. Development of a STEMI system requires participation and support of all
stakeholders in the EMS community. a. True b. False
2. The purpose of developing STEMI systems is to: a. Triage patients with ST elevation rapidly to definitive care. b. Limit total ischemic time to less than 120 minutes from onset of symptoms
to intervention. c. Answer a and b
3. STEMI Receiving Center Designation requires: a. 24/7-365 day a week STEMI coverage b. Performance Improvement (QI) plan c. Rapid transfer plan if surgical services are unavailable d. All of the above
4. STEMI Receiving Centers will have a diversion process if their cardiac catheterization lab is down.
a. True b. False
5. STEMI patients are identified by EMS in the field by a. 12-Lead ECG that “diagnoses” the rhythm b. ***ACUTE MI*** or ***ACUTE MI SUSPECTED*** c. ***POSSIBLE MI*** d. Answer a and b e. Answer a and c

6. The false positive rate of 20% is typical in experienced STEMI systems a. True b. False
7. STEMI patient destination is determined at the scene after the 12 lead ECG meets the appropriate criteria by the EMS provider.
a. True b. False
8. Factors that influence prehospital destination decisions in a STEMI system
include: a. Number and location of STEMI Receiving Centers b. Patient Family Preference c. If facilities are with 15 minutes difference of each other (equidistant) d. If a STEMI Receiving Center is NOT within 30 minutes e. All of the above
9. Contra Costa County STEMI destination protocol is designed to be flexible and honors the patient’s right to choose.
a. True b. False
10. Radio contact of a STEMI patient should include the following a. Situation: “STEMI ALERT” confirmed by 12 lead, ETA and patient age
and gender b. Background: Presenting complaint, past cardiac history, history of
pacemaker c. Assessment: Patient stable or unstable. If unstable why d. RX and Recap: Treatments given and patient response. e. All of the above
11. Handoff of the patient at the hospital should include
a. Patient report: i. Patient identification
ii. Recap of radio report with any updates iii. Allergies and medications iv. Other pertinent past medical history v. Name of patient cardiologist-if known
b. Hardcopies of all prehospital 12 leads c. Draft or completed patient care record. d. Answer a, b, c
12. An effective STEMI system relies on good communication and effective problem-solving.
a. True b. False

13. Hospital providers can support the STEMI system in the following ways a. Making sure ECG’s get into the patient’s chart. b. Reporting issues when they occur to STEMI Program Manager or ED
Manager. c. Giving constructive solution focused feedback. d. Being respectful in your communications. e. All of the above.


















