STEMI Management in Belgium -...
24
STEMI Management in Belgium Belgian STEMI registry 2007-2011 Prof dr M Claeys University Hospital Antwerp Belgian Working Group of Acute cardiology
Transcript of STEMI Management in Belgium -...

STEMI Management in Belgium
Belgian STEMI registry
2007-2011
Prof dr M Claeys
University Hospital
Antwerp
Belgian Working Group of Acute cardiology

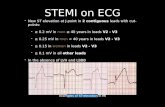
Age-standardized mortality from ischaemic heart
disease in European regions
(men; 45–74 years;
year 2000)
European Heart Journal (2008) 29, 1316–1326

Minimal Data Base
Patient characteristics
(TIMI risk score)
Reperfusion strategy
In Hospital Outcome
Electronic CRF

Enrolment STEMI patients 1/1/2007 – 31/12/2011
2847
553
631
76
843
2186
1435
13701526
n= 11468
110 hospitals
75 hospitals with
>10 pts/y
0
1000
2000
3000
20072008200920102011

Regional data on baseline characteristics
4.3
4,3
4.2
3.3
3.8
4.2
3,9
4.24,4
TIMI risk score
0
2
4
6
8
10
12
14
16
18
Perc
ent
0 1 2 3 4 5 6 7 8 9 >9
TIMI >>9
Histogram
4,2 +/- 2,9
3,6
3,8
4
4,2
4,4
2007 2008 2009 2010 2011

Time Evolution TIMI risk factors
5958
59
6364
54565860626466
20072008200920102011
Tot ischemic time<4h
11 119 8 8
0
5
10
15
20072008200920102011
Peripheral Artery Disease
46
44 4443
41
38
40
42
44
46
48
20072008200920102011
Arterial Hypertension
25 24 22 20 18
0
10
20
30
20072008200920102011
Killip class >1

Regional data on Reperfusion therapy
84
88
93
26
82
90
71
8684
Primary PCI
6
84
3 26
0
10
20
30
40
50
60
70
80
90
thromb. PPCI ResPCI facPCI no rep
reperfusion therapy
78 81 87 90 94
0
50
100

Evolution reperfusion therapy
12 11 9 7 4
3625
15 105
5365
7683
91
0
20
40
60
80
100
2007 2008 2009 2010 2011
no reperf
TT
PCI
4 4 4 3,5 35 3 2 1,5 1
90 93 94 95 96
0
20
40
60
80
100
120
2007 2008 2009 2010 2011
no reperf
TT
PCI
PCI center
No-PCI center

Regional data on in hospital mortality
8.8
6
6.3
6.5
3.8
7.0
4.5
6.87
Average:
6,8%
Mortality
30d mortility (n=4697)
5.4 % (vs 4.7% in hospital)
6,47,6 7,6
5,9 6,2
0
2
4
6
8
2007 2008 2009 2010 2011

Regional data on duration of hospital stay
8.1
6.8
6.8
5.5
6.2
7.1
5.4
9.88.1
Average:
7 +/- 8 d
>7d: 21%
Duration
N=2842 (alive)
86,5
0
5
10
2010 2011

Hospital duration and TIMI risk score
0
5
10
15
20
25
30
0 1 2 3 4 5 6 7 8 9 >9
IQ75%
median
N=2638 living patients (without CPR)
Risk factors for long hospital stay: age, female, PAD, Killip>1, no reperfusion, PCI center

Global Analyis: mortality data
• Mortality versus reperfusion strategy
• Mortality versus door to balloon/needle time
• Mortality versus cardiac care program
• Mortality and gender/age
• Mortality: independent predictors

Mortality versus Reperfusion strategy
0
5
10
15
20
25
30
Perc
ent
0 1 2 3 4 5 6 7 8 9 >9
TIMI risk score
N= 11467
TrombolysisN=665
Rescue PCIN=299
PCIN= 9617
Faciliated PCIN=250
No Reperfus.636
0
2
4
6
8
10
12
14
16
18
Perc
ent
0 1 2 3 4 5 6 7 8 9 >9
TIMI risk score
0
2
4
6
8
10
12
14
16
Perc
ent
0 1 2 3 4 5 6 7 8 9 >9
TIMI risk score
3.9
N = 954 ( 8%)* N=9867(86%) N= 636 (6%)
4.1 5.9
MORTALITY
6.0 %6,7% 19%
*Elective Invasive evaluation:502+299=801( 84%)

Mortality benefit PCI over TT is dependent
on baseline risk profile
0
5
10
15
20
25
30
35
40
45
50
0 1 2 3 4 5 6 7 8 >8
PCI thrombolysis
PCI vs TT : P=0.02
InTIME II

Mortality versus door to balloon/needle time
Ealry PCI: < 60 min
Interm PCI: 60-120
Late PCI: > 120 min
Early TT: <30 min
Interm T: 30-60 min
Late T: > 60 min
Claeys et al, Arch of Inter Med.2011;171:544-549

0
2
4
6
8
10
12
14
16
18
Perc
ent
0 1 2 3 4 5 6 7 8 9 >9
TIMI risk score
0
2
4
6
8
10
12
14
16
18
20
Perc
ent
0 1 2 3 4 5 6 7 8 9 >9
TIMI risk score
Mortality versus Acute cardiac care program
4.2 4.1MORTALITY
6.7%
PCI centreN=7024(60%)
trombolysis: 2%
Rescue PCI: 1%
Prim –facilat PCI: 93%
No reperfusion: 4 %
No-PCI centreN=4443 (40%)
trombolysis: 15%
Rescue PCI: 5%
Prim –facilat PCI:75%
No reperfusion: 8 %
6.9%
EHJ-ACC 2012, in press

Mortality versus gender
Men
N=8594
Female
N=2873(25%)
age
DM
Time to T<4h
shock
PCI/throm/no
61
14%
63 %
7%
87/9/5
68 *
19% *
53% *
11 % *
83/8/9 *
Mortality 6% 11 % *
* p<0.0001

Indepedent predictors of mortality
P value 0R (95%CI)
Killip > 1 <.0001 5 (4 - 7)
CPR <.0001 5 ( 4-6)
age <.0001 1.04 (1.03-1.05)
PCI vs TT
No reperf
0.01
<0,0001
1.5 ( 1.1 – 2.7)
2,3 (1,7-3,1)
Ischemia>4h 0.0001 1.5 (1.3-2.0)
PAD <0.0001 1,8 (1.4-2.4)
Female
Anterior infarct
0.04
0.001
1.3 (1. 1-2.0)
1.4 (1.1-1.6)

Conclusions
• The Belgian STEMI registry is the first prospectiveregistry enroling patients from both PCI and no-PCIcentres.
• The overall in hospital mortality is 6.9 % and compares well with current European ACS surveys.
• In the setting of STEMI networking with low threshold for invasive evaluation , the mortality of STEMI in PCI and no-PCI centers is identical.
• Participation to the STEMI registry increasesadherence to guidelines as was evidenced by a significant gradual increase in primary PCI particularly in non-PCI centers.

Steering committee of STEMI database
• Prof dr P Sinnaeve, UZ Leuven
• Prof dr P Evrard , UCL Mont-Godinne
• Dr C Convens, ZNA Antwerpen
• Dr P Dubois, CHU Charleroi
• Dr J Boland, CHR Citadelle Liège
• Dr P Vranckx, Virga Jesse Hasselt
• Dr S Gevaert, UZ Gent
• Dr A de Meester, Hôpital Jolimont
• Dr P Coussement , AZ Brugge
• Dr De Raedt, OLV Ziekenhuis Aalst
• Prof C Beauloye, UCL Louvain
• Prof M Renard, ULB Brussels

Conclusions
• Mortality benefit of PPCI over trombolysis (6.0 versus 6.7) is smaller than in previously reportedrandomised clinical trials. This is related, at leastpartly, to the selective use of trombolytic therapymainly in low risk patients and to better outcome of thrombolytic therapy (related the high rate of subsequent invasive evaluation in Belgium. )
• In the setting of STEMI networking with low threshold for invasive evaluation , the mortality of STEMI in PCI and no-PCI centers is identical.
• Participation to the STEMI registry increasesadherence to guidelines as was evidenced by a significant gradual increase in primary PCI particularly in non-PCI centers.

STEMI in octogenerians (12%)
05
10152025303540
<80 years ≥80 years KC = I
≥80 years KC >1
5.1
31.6
4.8
34.6
17.9
8.5
36.3
in-hosp mort TL (%) in-hosp mort PCI (%) in-hosp mort no-reperfusion (%)
12
5.7
Killip class>1 :
40%vs20%
Shock: 12% vs 7%
Ischemic time>4h
53% vs 38%
PCI : 76% vs 84
Conservative
14% vs 5%
Abstract presentation ESC 2011 E Vandecasteele et al

AUDIT STEMI REGISTRY:2007-2010
Centre Source doc. Correct item
2007-2008 (16)
2008-2009 (15)
2009-2010 (14)
2007-2010 (45)
2468/3255= 76%
2541/2877= 88%
2445/2793= 88%
7454/8925= 84%
2356/2468=95%
2460/2541=97%
2349/2445=96%
7165/7454=96%

TIMI risk score (automatically calculated)
Circulation: 2000;102:2031