Status Epilepticusin Children
67
Status Epilepticus in Children 儿童癫痫的连续状态 -2010 update 林口长庚 儿童加护科 林建志医师 2010-7-21 PDF created with pdfFactory trial version www.pdffactory.com
Transcript of Status Epilepticusin Children

Status Epilepticus in Children儿童癫痫的连续状态
-2010 update
林口长庚儿童加护科
林建志医师
2010-7-21
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Outline - Status Epilepticus• Case Presentation• Definitions• Epidemiology• Clinical Features• Causes / Outcomes• Pathophysiology• Management *
– General– Drugs
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Outline - Status Epilepticus• Case Presentation• Definitions• Epidemiology• Clinical Features• Causes / Outcomes• Pathophysiology• Management *
– General– Drugs
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Seizure movies
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Clinical senario
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
现病史
• 3 years and 8 months Female• ED visit time: 2010/3/20 23:37
• CC: Seizure for 20 minutes
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

现病史
• 22:00 cough, vomit once• 22:10 seizure attack with staring gaze,
generalized tonic-clonic seizure, drooling, lip cyanosisè sent to LMD, seizure stopped 20
minutes later• 23:37 sent to our ED due to still
unconsciousness
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Triage & Vital sign at our ER
• T 38.0 P 120 R 26, BP?, SpO2 98%• GCS: E2V2M4• BW 15kg
• 体格检查• Consciousness: drowsy,E2V2M4• Pupil: 3mm/3mm; Light reflex: +/+• Neck: supple, no lymphadenopathy; • Brudzinski sign : negative,Kernig sign:
negative
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

现病史– continued (2)
• However, seizure attack again without conscious recovery between the seizure episode.
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

儿童癫痫的连续状态
诊断
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Outline - Status Epilepticus• Case Presentation• Definitions• Epidemiology• Clinical Features• Causes / Outcomes• Pathophysiology• Management *
– General– Drugs
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Q1: The definition of following disease
Impending Status Epilepticus
Convulsive SEConvulsive SE
Subtle SESubtle SE
NonconvulsiveNonconvulsiveSESE
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Definition of Status Epilepticus
• 癫痫持续状态是指持续、频繁的癫痫发作,发作时间持续30分钟以上或连续多次发作,发作间期意识不恢复。 ”
• Clinical or electrographic seizures lastingmorethan 30 minor withoutfull recovery of consciousness between seizures– “no recovery between attacks”– “20-30 min” --> risk of injury to CNS neurons
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Impending Status Epilepticus
• Continuous or intermittent seizures lasting more than 5 min without full recovery of consciousness between seizures– more practical definition: since isolated tonic - clonic
seizures rarely last > few minutes ... consider Status if sz > 5 min or 2 discrete sz with no regaining of consciousness between
• Treat as aggressively as confirmed status epilepticus
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Subtle Status Epilepticus• The first description by Dr. David Treiman (1984). • It is defined subtle status epilepticus as
consisting of “nystagmus, eye blinking, and/or mild motor movements…with marked impairment of consciousness and continuous or nearly continuous, usually bilateral, ictalpatterns on the EEG.”
• Both the motor and EEG expression of seizures become less florid, however prognosis and therapeutic implications remain the same
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
Nonconvulsion status epilepticus
• Nonconvulsive status epilepticus (NCSE) is an important status epilepticus (SE) type and is defined as a mental status changes from baseline of at least 30 to 60 minutes duration associated with continuous or near continuous ictaldischarges on EEG.
Kaplan PW. Nonconvulsive status epilepticus. Seminars in Neurology 1996;16:33-40.
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Spectrum of Disease
Impending Status Epilepticus
Convulsive SEConvulsive SE
Subtle SESubtle SE
NonconvulsiveNonconvulsiveSESE
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Outline - Status Epilepticus• Case Presentation• Definitions• Epidemiology• Clinical Features• Causes / Outcomes• Pathophysiology• Management *
– General– Drugs
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
Epidemiology - SE
• Life threatening• USA: -102,000 -152,000 cases / year
(Adult) - 52,000 deaths / year• Of new cases of epilepsy, 12 -30%
present in Status• Generalized Status is most common
form
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Outline - Status Epilepticus• Case Presentation• Definitions• Epidemiology• Clinical Features• Causes / Outcomes• Pathophysiology• Management *
– General– Drugs
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Clinical - Generalized SE• At onset - usually obvious tonic / clonic• As continues often subtle - slight twitch of
face / extremities, nystagmoid eye movements
• May be NO observable motor sz ***still risk for CNS injury - assume still seizing if SE pt not waking
• need EEG to definitely dx - not uncommon in comatose hospital inpatients
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
Outline - Status Epilepticus• Case Presentation• Definitions• Epidemiology• Clinical Features• Causes / Outcomes• Pathophysiology• Management *
– General– Drugs
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Cause of SESE in children can be classified broadly into one of
three categories based on etiology:1. Reactive
-Status is caused most commonly by fever ("Febrile seizures".)
2. Symptomatic, acute or remote- Acute symptomatic causes include infection, hypoxia, glucose and electrolyte imbalance, trauma, and hemorrhage or stroke. - Remote symptomatic refers to seizures caused by an insult earlier in life, such as perinatal hypoxic-ischemic injury, trauma, infection, or a congenital brain malformation.
3. Idiopathic or cryptogenic— No known or identifiable cause.
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
Cause of SE
• Chronic (Remote symptomatic) causes - usually better response to Rx– known epilepsy - breakthrough sz +/- low
anticonvulsant levels– remote CNS process (eg brain surgery / CVA
/ trauma) --> SE after long latent period
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Outcome of SE
• Overall adult mortality 20% (>80 yr : 50%)• Children - better outcomes - mortality 2.5 %
• Worse outcome if prolonged / severephysiologic disturbance
• Outcome depends on cause
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Pediatr Neurol 2009;41:413-418.
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Lin K-L, Lin J-J. Analysis of convulsive status epilepticus in children of Taiwan. Pediatr Neurol 2009;41:413-418
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Outcome of SE
• Overall adult mortality 20% (>80 yr : 50%)• Children - better outcomes - mortality 2.5 %
• Worse outcome if prolonged / severephysiologic disturbance
• Outcome depends on cause
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Outline - Status Epilepticus• Case Presentation• Definitions• Epidemiology• Clinical Features• Causes / Outcomes• Pathophysiology• Management *
– General– Drugs
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Basic Mechanism of SE
• Appears that SE can become self‐sustaining(自我持续的)
• Animal models (chemical or electrical) of SE• Human observations (no real “proof”)
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Self‐Sustaining(自我持续的)SESeconds to minutes-Receptor trafficking• Existing receptors move from synaptic
membrane to endosomes• Can move from storage to synaptic membranesMinutes to hours• Increase inproconvulsive neuropeptides• Depletion ofinhibitory neuropeptidesHours to days• Change in gene expression• Neuronal death
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
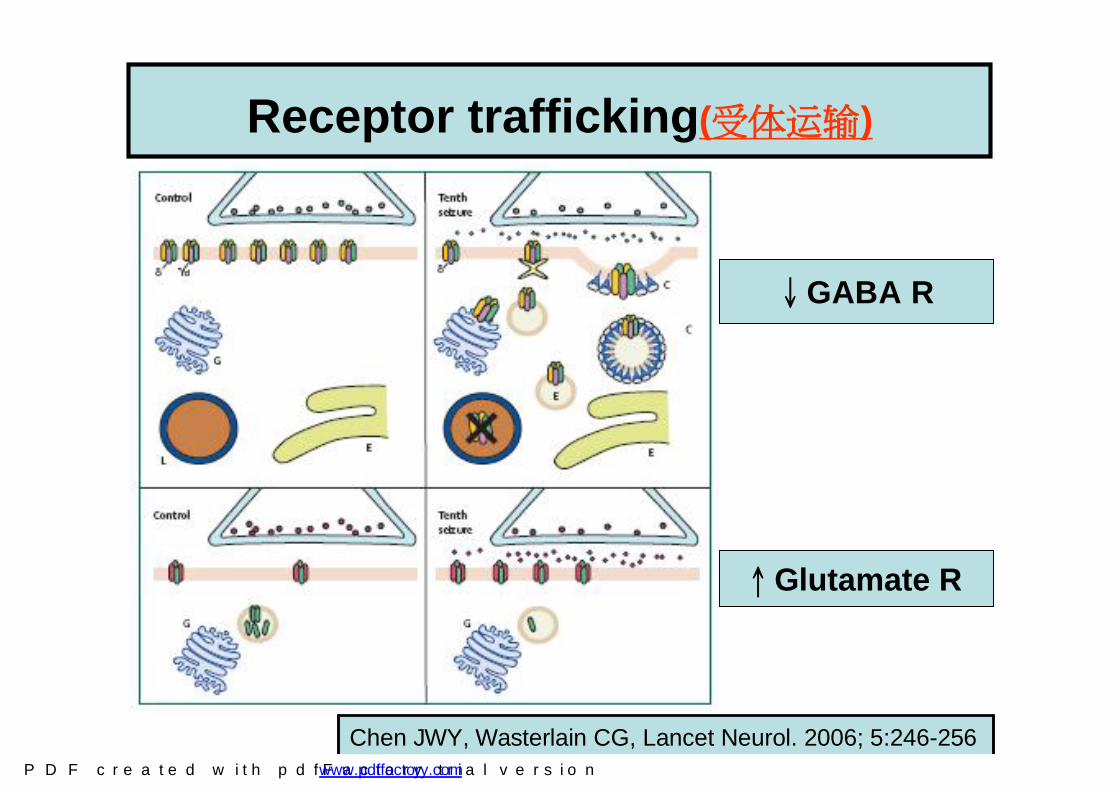
Chen JWY, Wasterlain CG, Lancet Neurol. 2006; 5:246-256
Receptor trafficking(受体运输)
↓GABA R
↑Glutamate R
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Self‐sustaining SE (自我持续的SE)
• Easily stopped only by drugs that directly or indirectlyinhibit glutamatergicneurotransmission
• GABAergic and barbituates loose potency
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Pharmaco-resistance(药物抗药性)
• Time‐dependant resistanceto benzodiazepines (GABA-R) and others well documented in animal models
• In humans –early treatment more effectiveimplying resistance is one possible explanation
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Outline - Status Epilepticus• Case Presentation• Definitions• Epidemiology• Clinical Features• Causes / Outcomes• Pathophysiology• Management *
– General– Drugs
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

OUTLINE - Management of SE
• General approach• Anti - Epileptic Drugs
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
Management of SE-Clinical senario
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Management of SE
• ABC’s (+ monitor / O2 / large IV’s)• Search and treat underlying causes
• START PHARMACOTHERAPY ASAP
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Management of SE continued
• History & Physical - do once Rx initiated
• Hx: events, trauma, meds, sz hx, infx• P/E: Neuro - look for focal signs vs.
generalized tonic-clonic– look for signs of underlying causes -
trauma, infection, etc
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Is neuroimage needed to arrange ???
• Neuroimaging is generally deferred until the patient is stabilized.
• However, if LP is considered, computed tomography (CT) may be recommended beforehand to exclude a mass lesion, especially in a patient with focal neurologic signs.
• Later, a magnetic resonance imaging study (MRI) is recommended if the etiology of SE is unknown.
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Brain CT
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

OUTLINE - Management of SE
• General approach• Anti - Epileptic Drugs
Whic drug do you want to choice?
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Drug Rx of SE
• Starting Rx ASAP has been correlated with a better response rate to drug Rx, and lower morbidity– Lowenstein DH, Alldredge BK
Neurology 1993 (43): 483-8• < 30 min - 80% stopped• > 120 min - < 40% stopped
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

OUTLINE - Management of SE
• General approach• Anti - Epileptic Drugs:
– Benzodiazepines– Phenytoin / Fosphenytoin– Barbiturates– Propofol– others / new possibilities
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
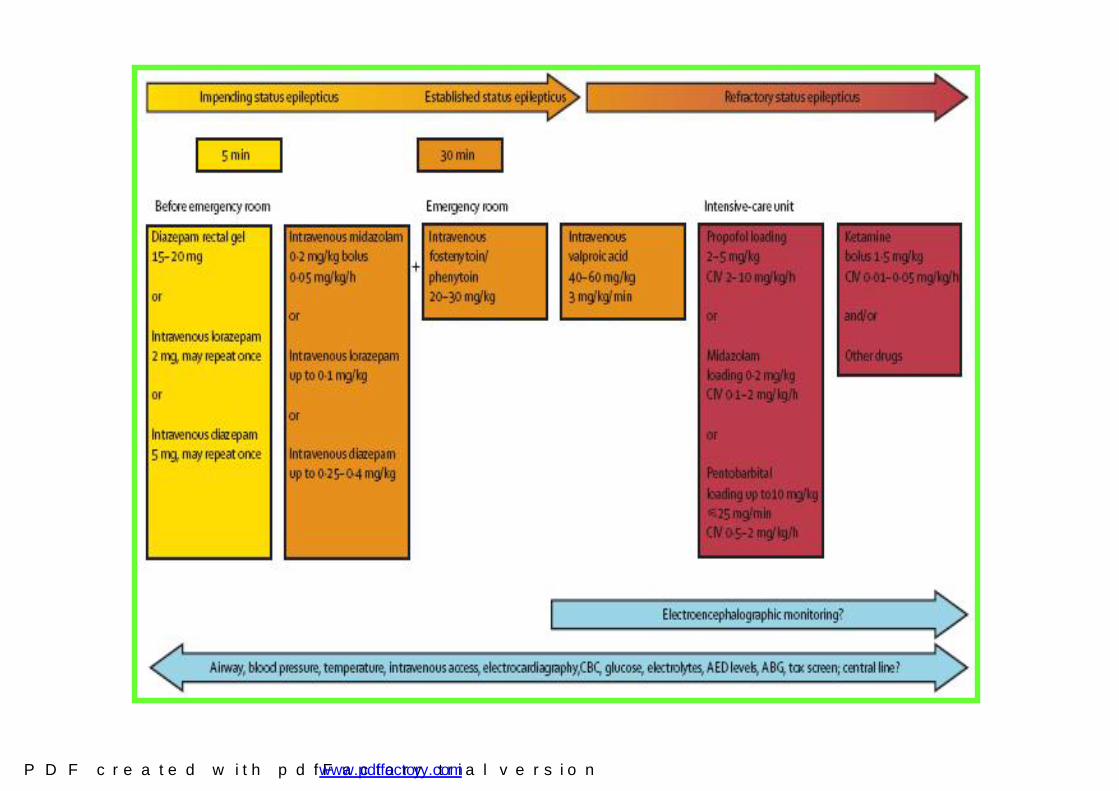
Lancet Neurol 2006; 5: 252
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Which drug do you want to choice first ?
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Benzodiazepines
• Diazepam:地西泮 (安定) enters CNS in 10 sec, lasts 20-30 min; rectal gel (10mg) effective in 75-90% of cases
• Lorazepam:劳拉西泮(氯羟安定): enters CNS in 2-3 mins; lasts 2-3 hours
• Midazolam:咪唑安定 0.15 mg/kg load then drip @1-18 mic/kg/min iv, im, sl
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
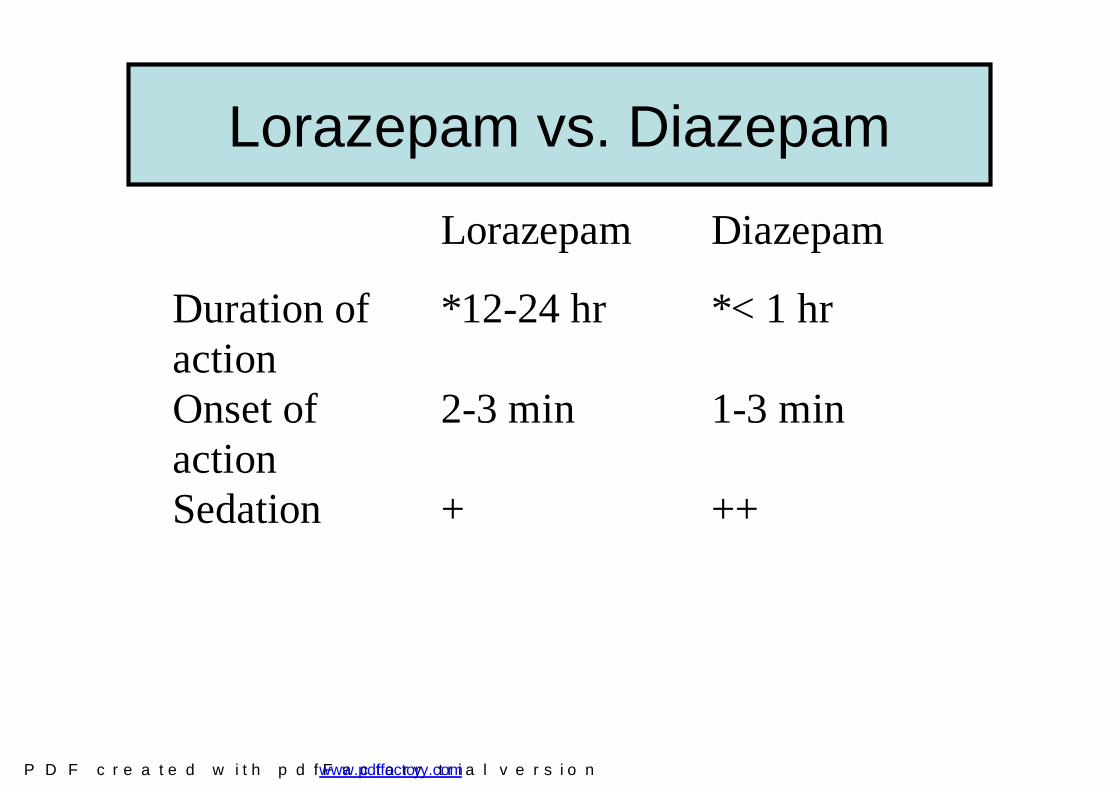
Lorazepam vs. Diazepam
Lorazepam Diazepam
Duration of action
*12-24 hr *< 1 hr
Onset of action
2-3 min 1-3 min
Sedation + ++
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Which Benzo Do I Use?
• Lorazepam is preferred due to long activity• In the absence of intravenous access,
Diazepam can be given via rectal route until access is established
• Midazolam is generally reserved for refractory status epelipticus
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Which drug do you want to use as 2nd line choice ?
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Drug, Routine, Dosage and Maximum dose
• Dilantin苯妥英钠 (250mg/5ml/amp) IV• Loading dose:20 mg/kg/dose, Max: 700-
750mg/dose• Maintain: 2mg/kg/dose Q8H (6mg/kg/day)
• Luminal 苯巴比妥 (100mg/ml/amp) IV • Loading dose:20 mg/kg/dose, max: 700mg/dose• Maintain : 2mg/kg/dose Q8H (6mg/kg/day)
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
Drug Rx of SE
• Existing agents - adverse effects: – Benzos / Bbts - decrease LOC / respiration– Dilantin / (Fosphenytoin) - infusion rate-
related hypotension / dysrhythmias– Dilantin / Bbts / (Fosphen) - slow onset d/t
limited rate of administration
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Drug Rx - Refractory SE• Anesthetic doses of:
- Valproic acid(1-2.5mg/kg/hr drip)– Midazolam (IV infusion 2 - 20 mcg/kg/min )– Propofol (1-2 mg/kg)– Barbiturates (Thiopental, high dose
Phenobarbital, Pentobarbital)– Inhalational anesthetics (Isoflurane)
1. ACEP Clinical Policies Committee and the Clinical Policies Subcommittee on Seizures. Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department With Seizures. Ann Emerg Med. 2004;43:605-625.
2. Chen, Wasterlain. Status epilepticus: pathophysiology and management in adults. Lancet Neurol 2006; 5: 246–56.
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Possible new drugs for Status
• Lidocaine 利多卡因- some positive trials• Topomax• Gabapentin / Vigabatrin / Lamotrigine• Felbamate - blocks NMDA receptors• Ketamine - blocks NMDA receptors
– Ketamine (only if CT head is negative for mass or hydocephalous)
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Drug Rx of SE
• 1st - Benzodiazepines– *Lorazepam, Diazepam
• 2nd - > 1 y/o Phenytoin, Fosphenytoin• < 1 y/o Phenobarbital• 3nd – Valproic acid 丙戊酸钠 (德巴金)• Loading:15mg/kg/doseà 100mg/kg/dose• Max: 800mg/dose• Maintain: 10-20mg/kg/dose Q8H• (30-60mg/kg/day)
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Drugs-reference • Standard Protocol• Lorazepam 0.1 mg/kg (max 4
mg)• Diazepam 0.3 mg/kg (max 10
mg)• Midazolam 0.2 mg/kg (max 10
mg)• Phenytoin or Fosphenytoin
15‐20mg/kg (up to 30 mg/kg) (I start ½ dose immediately)
• Propofol 1‐2 mg/kg load then 2‐10mg/kg/hr (ranges as high as 2‐5mg/kg load have been used) (not forkids)
• Pentobarbital 10‐15 mg/kg bolus then 0.5‐1 mg/kg/hr
• Midazolam drip 0.05‐2.0 mg/kg/hr
• Others• Valproic Acid 20‐30 mg/kg (in
Europe up to (40‐60 mg/kg) at 3mg/kg/min (faster rates fro SE). It is approved for SE in (Norway and Germany ??? Others now) . Avoid if severe liver disease or mitochondria disease.
• Levetiracetam (Keppra) dose not standard but up 2‐4 grams over 15 minutes administered to volunteers.
• Not approved for SE but may have advantages for critically ill liver disease patient (renal metabolism)
• Lidocaine really old school but Japan
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

CGMH Website: http://www.cgmh.org.tw/chldhos/intr/c4a00/bigwig/bulletin/neuro/03.htm
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

CGMH Website: http://www.cgmh.org.tw/chldhos/intr/c4a00/newworkbook/15.pdf
Page 41
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com

Take-Home points - Status• Better outcome if seizure stopped earlier• Consider/ correct underlying disease• AED Drug treatment
1st - Benzodiazepines– * Lorazepam, Diazepam
2nd - >1y/o Phenytoin, Fosphenytoin-Fosphenytoin - surpasses Phenytoin for SE,
and for any patient with altered mental status who would otherwise need IV Phenytoin - hopefully more available soon< 1y/o Phenobarbital
• Transfer Patients to ICU if refractory SE
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com
Thank you for your attention
The end
P D F c r e a t e d w i t h p d f F a c t o r y t r i a l v e r s i o n www.pdffactory.com