![Focal hemodynamic patterns of status epilepticus detected ... · epilepticus or subtle status epilepticus [4]. Electroenceph-alogram (EEG), the diagnostic gold standard, may not be](https://static.fdocuments.us/doc/165x107/6074493ed430437ef144c30f/focal-hemodynamic-patterns-of-status-epilepticus-detected-epilepticus-or-subtle.jpg)
Status epilepticus in the neonate: different diagnoses and ...
56
Status epilepticus in the neonate: different diagnoses and different treatments
Transcript of Status epilepticus in the neonate: different diagnoses and ...

Status epilepticus in the neonate:
different diagnoses and different treatments

Toward a patient-tailored approach and
targeted treatment
Maria Roberta Cilio, MD, PhD Professor, Neurology & Pediatrics
University of California, San Francisco

THE CHALLENGE OF DIAGNOSIS
acute seizures versus
neonatal-onset epilepsies

Treatment ■ Phenobarbital ■ Phenytoin ■ Levetiracetam ■ Benzodiazepines



43 45
0
20
40
60
80
100
Phenobarbital PhenytoinPainter et al, NEJM 1999
Effica
cy (%)

Cochrane Review ■ There is little evidence to support the use of any of the
AEDs currently used in the neonatal period ■ Heterogeneity of seizure definition: clinical vs EEG
■ No data on whether controlling neonatal seizures has any measurable impact on the most important outcomes: ◆ Mortality ◆ Neurodevelopmental impairment Booth and Evans, 2004
■ Trend in reduction in total seizure duration and reduction in the severity of MRI injury when both clinical and subclinical seizures were rapidly treated (Van Rooij et al, 2010)
Booth and Evans, 2014

■ Barbiturates and benzodiazepines GABA agonists.
■ They are effective in the older brain, but have limited efficacy in the neonate (Jensen et al, 1999)
■ In the immature brain, PHT and PB may produce apoptosis of
neurons (Bittigau et al, 2002)

Scott and Holmes, Nature Medicine, 2012
EXPLORING NEW THERAPIES

■ Levetiracetam ◆ Ongoing prospective, randomized –PI Richard Haas, UC San
Diego ◆ First-line i.v. compared with Phenobarbital for acute seizures in
term infants ■ Topiramate ■ Bumetanide + Phenobarbital
◆ NEMO study (Pressler et al. Lancet, May 2015) ✦ Trial stopped earlier because of serious
adverse events and limited evidence for seizure reduction
◆ US trial
EXPLORING NEW THERAPIES

u High cognitive and behavioral side effects in studies undertaken in developed countries but not in those sited in the developing world – The China Project (Wang et al., 2003, 2006, 2008)
u It is arguable that Phenobarbital’s negative reputation comes from its lack of commercial sponsors rather than from a critical analysis of the available literature (Kale & Perrucca, 2004)

■ Phenobarbital remains the drug of first choice for seizures in the neonate and it should be made readily available in all settings
■ Before the guidelines of World Health Organization that made PB an essential drug, governments in Africa did not feel that making access to the drug everywhere was essential

Treating seizures in neonates with HIE:
The role of hypothermia

Seizures were diagnosed with EEG in 34% of the patients
Nash et al, Neurology 2011
Scher, Neurology 2014
Seizures in non-cooled babies 61%

THE CHALLENGE OF TREATMENT
DOES ONE SIZE FIT ALL?

DOUBLE TROUBLE:
SEIZURES IN TWINS

DOUBLE TROUBLE: SEIZURES IN TWINS
■ Seizures were stereotyped and quite similar in each twin.
■ The twins were having more than 20 episodes per day.
■ Neurological examination in between attacks was normal in both infants

DOUBLE TROUBLE: SEIZURES IN TWINS
■ MRI scan, CSF examination, organic acids,electrolytes, CBC, NH3, and liver function tests: normal
■ Very frequent seizures occurred despite PB levels > 40 µg/mL, clonazepam, and intermittent diazepam therapy.
■ Oral CBZ was added and there was a total cessation of seizures


Weckhuysen et al, Ann Neurol 2012
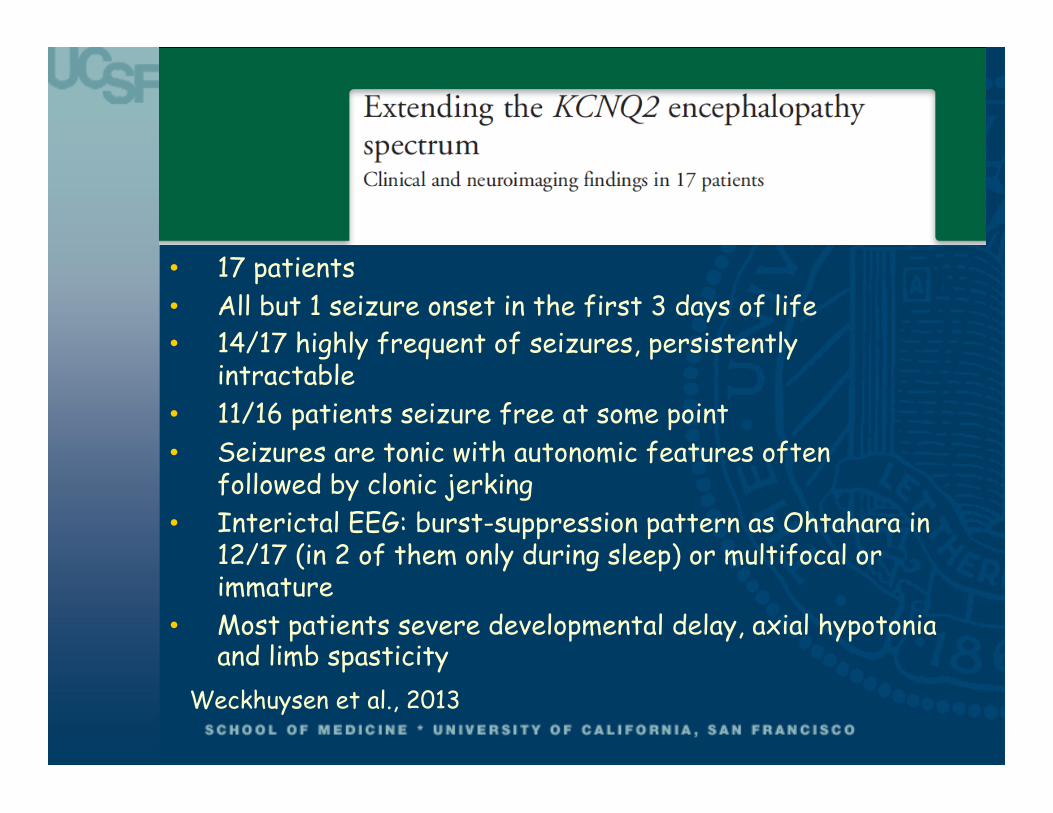
Weckhuysen et al., 2013
• 17 patients • All but 1 seizure onset in the first 3 days of life • 14/17 highly frequent of seizures, persistently
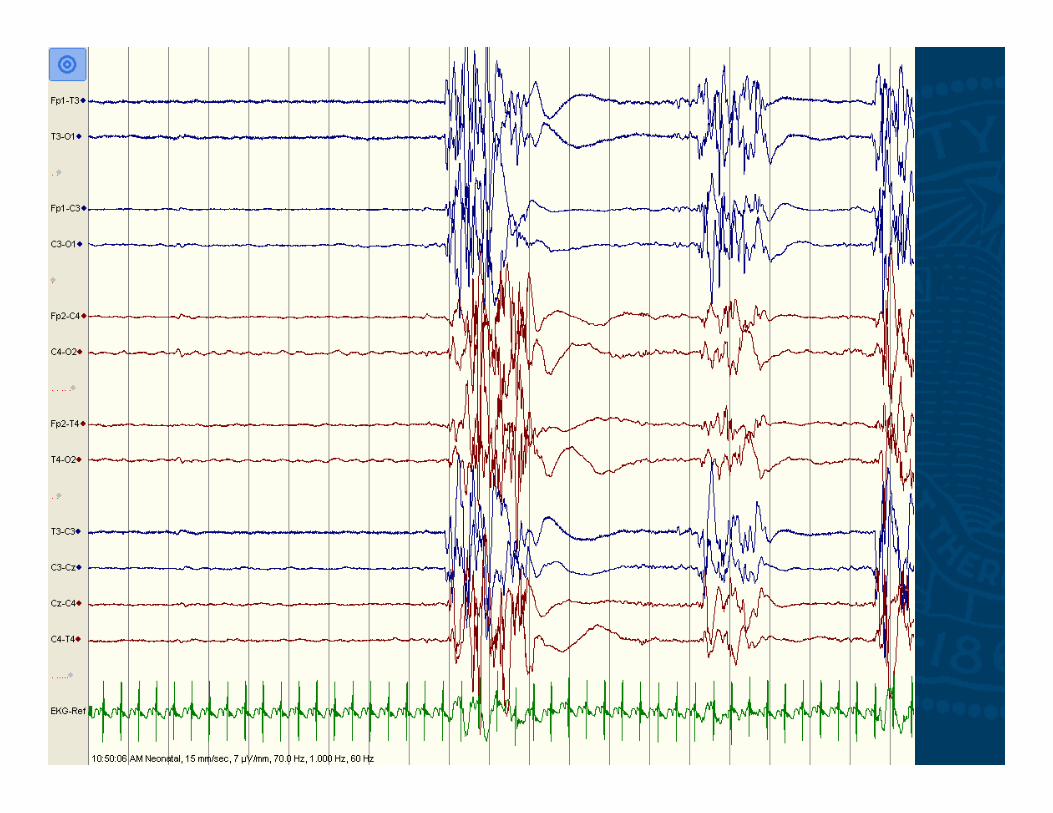
intractable • 11/16 patients seizure free at some point • Seizures are tonic with autonomic features often
followed by clonic jerking • Interictal EEG: burst-suppression pattern as Ohtahara in
12/17 (in 2 of them only during sleep) or multifocal or immature
• Most patients severe developmental delay, axial hypotonia and limb spasticity

• KCNQ2 missense mutations in 12/239 patients with early onset epileptic encephalopathy with age at onset < 1 • 10/12 Ohtahara • 2/12 unclassified • 11/12 seizure onset within the first week of life • Daily/hourly tonic seizures • Treated mainly with phenobarbital • 8/12 seizure-free with different drugs/combination • Moderate to profound developmental delay













Ohtahara phenotype? ■ Differently from Ohtahara syndrome these babies
do not have tonic spasms neither at presentation nor during several months of follow-up and their EEG lacks the invariable and regular periodicity of the suppression-burst pattern of Ohtahara syndrome.
■ Role of PB loads in EEG discontinuity
■ Patients often became seizure-free after the first years of life and evolution into West syndrome is rare.

KCNQ2 encephalopathy 1 Seizures resistant to PB, Benzodiazepines,
Levetiracetam, Topiramate, ketogenic diet, Vigabatrin,…
2 Response to Carbamazepine
3 Influence on developmental outcome?
Numis et al. Neurology 2014


■ 15 patients ■ Seizure onset between 1 and 4 days of age ■ 6/15 has status epilepticus ■ All were trialed with several AEDs ■ 11/15 responded to carbamazepine or
phenytoin with seizure-freedom within days ■ Seizure-freedom was sustained ■ Most patients had severe developmental
delay at follow-up ■ The two patients who achieved seizure-
freedom within a few days after onset had a slightly better developmental outcome

■ Drugs targeting sodium channels block the movement of sodium ions through the channels during propagation of the action potential and thus block and prevent the development of seizure activity
■ Seemingly disparate, voltage-gated sodium channels and KCNQ potassium channels co-localize and are bound at critical locations of the neuronal membrane
■ Modulation of one channel may significantly impact the function of the channel-complex
Pan Z et al, J Neuroscience 2006

■ Two mutations affecting the same residue in the S4 domain of KCNQ2 (R213W and R213Q) associated with either benign (R213W) or severe phenothype.
Both mutations destabilized the open state of the channel with decreased channel voltage sensitivity and increased cell firing frequency, with the R213Q prompting more dramatic functional changes compared with R213W

R144Q R201C R201H

■ In addition to dramatic functional deficits, de novo mutations found in patients with KCNQ2 encephalopathy can enhance Kv7.2/3 channel
■ Changes in network interactions rather than in intrinsic cell properties may be responsible for the neuronal excitability by these gain-of-function mutation
Miceli et al, J Neuroscience 2015

Epilepsy of Infancy with Migrating Focal Seizures
■ Newly recognized epilepsy syndrome – Epilepsy of infancy with migrating focal seizure – ILAE 2010
■ Described by Coppola and Dulac in 1995 ■ Onset in the first 6 months ■ In one half of cases onset in the first
month/first days of life

■ Conventional AEDs have been proven ineffective as well as various vitamines and ketogenic diet
■ Some seizure control reported with potassium bromide (Okuda et al.2000) and levetiracetam (Hmaimess et al. 2006, Cilio et al. 2009)

EIMFS is a channelopathy

Electrophysiological studies of EIMFS-associated mutations
■ Gain-of-function ■ Constitutive activation of the channel ■ Enhanced K+ current ■ KCNT1 has not solely a pore function ■ Its C terminal region is involved in protein-
protein interaction with several partners including FMRP (Fragile-X Mental Retardation Protein)
Bhattacharjee & Kaczmarek 2005; Brown MR et al. 2008; Ruffin VA, et al. 2008

■ KCNT1 is not affected by any conventional AEDs ■ It is a known target of several cardiac drugs ■ Antiarrhythmic drug Quinidine operates as a pore
blocker Annals of Neurology, 2014

Significant group difference in gain of function between mutations associated with Autosomal-Dominant Nocturnal Frontal Lobe Epilepsy and those associated with Epilepsy of Infancy with Migrating Focal Seizures
Milligan et al. Annals of Neurology 2015

Quinidine as targeted treatment for KCNT1-associated epilepsies
Exposure to Quinidine, a drug approved for the treatment of cardiac arrhythmias, significantly reduced the gain of function in all mutation studied
Milligan et al, Annals of Neurology 2014


25-‐month patient with EIMFS associated with KCNT1 missense mutation (c.1283G>A; p.Arg428Gln

Quinidine ■ Extensive metabolized in the liver by the
cytochrome-P450 enzyme system
■ Many drug-drug interaction including inhibition of metabolism of many AEDs
■ QT prolongation is a common adverse effect
■ Should be used with caution in combination with other medication that may prolong QT interval
■ Close EKG monitoring should be considered

■ One size does not fit all! ■ Accurate phenotyping ■ Early diagnosis is essential for early
treatment ■ Determining mutation pathogenicity and
mechanisms of disease ■ Collaboration is key ■ Early treatment of seizures may lead to
better outcome by reducing the effects of frequent seizures in the neonatal brain
■ Targeted treatment may drastically change prognosis

We seek the truth as scientists, we heal the sick as clinicians, and we teach others
to do the same as mentors