Statement.pdf · North Carolina 2000 17. North Dakota 2004 ... probation, monitoring of the ......
60
2.0 MEMORANDUM To: Board Members Ohio Board of Nursing From: Betsy Houchen Executive Director Subject: Compact Licensure Background Information Date: March 27, 2017 At the Retreat, the Board reviews multi-state licensure, also known as Compact licensure, or the National Licensure Compact (NLC). The Board reviews multi-state licensure annually to consider the benefits and risks to the citizens of Ohio in relation to the Board’s mission of public protection. Background of Multi-State Licensure Multi-state licensure was established in 1998 when the NCSBN Delegate Assembly adopted the NLC model legislation. Under the “old” Compact, 25 states are NLC members (Attachment A). In 2005, the Board examined issues and learned about the experience of some Compact states participating in the NLC. Although the Board recognized that multi-state nurse licensure could be advantageous for occupational health nurses, traveling nurses, or employers, the Board discussed that potential risks of harm to the public outweigh the potential benefits. With multi-state licensure, nurses could be practicing in Ohio when they have not been held to the same standards of safe practice that Ohio has deemed important for public safety. For example, Ohio requires criminal records checks for licensure, but not all Compact states have the same requirement. In addition, the Ohio statute specifies absolute bars to licensure. If an applicant has been convicted of certain crimes such as Murder and Rape, among others, the applicant cannot be considered for licensure in Ohio. The majority of Compact states either do not bar violent felonies, or they impose time-limited bars, rather than absolute bars to licensure. Since 2005, the Board has been an active participant in NLC discussions with other states and NCSBN in order to clearly identify the Board’s concerns. The Board adopted a statement regarding multi-state nurse licensure in 2005, and each year thereafter, the Board has reviewed NLC information and re-affirmed its position. 1
-
Upload
phungthuan -
Category
Documents
-
view
213 -
download
0
Transcript of Statement.pdf · North Carolina 2000 17. North Dakota 2004 ... probation, monitoring of the ......

2.0
MEMORANDUM
To: Board Members Ohio Board of Nursing From: Betsy Houchen Executive Director
Subject: Compact Licensure Background Information Date: March 27, 2017 At the Retreat, the Board reviews multi-state licensure, also known as Compact licensure, or the National Licensure Compact (NLC). The Board reviews multi-state licensure annually to consider the benefits and risks to the citizens of Ohio in relation to the Board’s mission of public protection. Background of Multi-State Licensure Multi-state licensure was established in 1998 when the NCSBN Delegate Assembly adopted the NLC model legislation. Under the “old” Compact, 25 states are NLC members (Attachment A). In 2005, the Board examined issues and learned about the experience of some Compact states participating in the NLC. Although the Board recognized that multi-state nurse licensure could be advantageous for occupational health nurses, traveling nurses, or employers, the Board discussed that potential risks of harm to the public outweigh the potential benefits. With multi-state licensure, nurses could be practicing in Ohio when they have not been held to the same standards of safe practice that Ohio has deemed important for public safety. For example, Ohio requires criminal records checks for licensure, but not all Compact states have the same requirement. In addition, the Ohio statute specifies absolute bars to licensure. If an applicant has been convicted of certain crimes such as Murder and Rape, among others, the applicant cannot be considered for licensure in Ohio. The majority of Compact states either do not bar violent felonies, or they impose time-limited bars, rather than absolute bars to licensure. Since 2005, the Board has been an active participant in NLC discussions with other states and NCSBN in order to clearly identify the Board’s concerns. The Board adopted a statement regarding multi-state nurse licensure in 2005, and each year thereafter, the Board has reviewed NLC information and re-affirmed its position.
1

2.0 The New/Enhanced Compact Model for Multi-State Licensure In 2013, the Executive Officers requested NCSBN convene a meeting to discuss the future of licensure models for several reasons: lack of consensus regarding the NLC; discussions about a national model of licensure for telehealth; and implementation of the Affordable Care Act. NCSBN convened several Executive Officer Forums for the purpose of resolving the differences in nurse licensure. As a result, the current NLC model was modified and on May 4, 2015, at a special NCSBN Delegate Assembly, the new Compact model was adopted (Attachment B). NCSBN provided an outline of key provisions and FAQs for legislators and policy makers (Attachments C and D). In addition, the APRN Compact was modified to mirror the enhanced Compact language and was also adopted at the May 4, 2015 special NCSBN Delegate Assembly. The APRN Compact language is not included for this discussion because Ohio does not authorize APRN independent practice and therefore, Ohio would not be eligible to join the APRN compact. Status of Adoption of the Enhanced NLC NCSBN reports that fourteen states have enacted the enhanced NLC: Arkansas; Arizona; Florida; Idaho; Kentucky; New Hampshire; Mississippi; Missouri; Oklahoma; South Dakota: Tennessee; Utah; Virginia; Wyoming. Other states with bills in various legislative stages: Colorado; Georgia; Illinois; Iowa; Maine; Maryland; Massachusetts; Montana; Nebraska; Nevada; New Jersey North Dakota; South Carolina; West Virginia NCSBN published their Leader-To-Leader publication for nursing educators about the enhanced compact and a document, “Anticipated Process for Rulemaking by the Commission” (Attachment E and F). Various Points of View Regarding Compact Licensure Some states do not plan to introduce legislation and/or there is opposition in their state to its introduction. The Board reviewed a Wall Street Journal article, “Occupational Licensing Doesn’t Seem to Restrict Nurses; Mobility” at the September 2016 meeting (Attachments G through I). Board Statement The enhanced NLC model was reviewed by the Board at the 2016 Retreat and the Board discussed areas of concern (Attachment J). At that time, the Board decided not to proceed with the enhanced NLC. This year at the Retreat, the Board is asked to review the materials and consider the Board statement (Attachment K).
2

Attachment A: Nurse Licensure Compact (NLC) States “Old” Compact
April 2017
T ILEMENTATION DATE 1. Arizona 2002
2. Arkansas 2000
3. Colorado 2007
4. Delaware 2000
5. Idaho 2001
6. Iowa 2000
7. Kentucky 2007
8. Maine 2001
9. Maryland 1999
10. Mississippi 2001
11. Missouri 2010
12. Montana 2015
13. Nebraska 2001
14. New Hampshire 2006
15. New Mexico 2004
16. North Carolina 2000
17. North Dakota 2004
18. Rhode Island 2008
19. South Carolina 2006
20. South Dakota 2001
21. Tennessee 2003
22. Texas 2000
23. Utah 2000
24. Virginia 2005
25. Wisconsin 2000
3

Nurse Licensure Compact March 17, 2015
ARTICLE I
Findings and Declaration of Purpose
a. The party states find that:
1. The health and safety of the public are affected by the degree of compliance with and the
effectiveness of enforcement activities related to state nurse licensure laws;
2. Violations of nurse licensure and other laws regulating the practice of nursing may result in injury
or harm to the public;
3. The expanded mobility of nurses and the use of advanced communication technologies as part of
our nation’s health care delivery system require greater coordination and cooperation among
states in the areas of nurse licensure and regulation;
4. New practice modalities and technology make compliance with individual state nurse licensure
laws difficult and complex;
5. The current system of duplicative licensure for nurses practicing in multiple states is cumbersome
and redundant for both nurses and states; and
6. Uniformity of nurse licensure requirements throughout the states promotes public safety and
public health benefits.
b. The general purposes of this Compact are to:
1. Facilitate the states’ responsibility to protect the public’s health and safety;
2. Ensure and encourage the cooperation of party states in the areas of nurse licensure and
regulation;
3. Facilitate the exchange of information between party states in the areas of nurse regulation,
investigation and adverse actions;
4. Promote compliance with the laws governing the practice of nursing in each jurisdiction;
5. Invest all party states with the authority to hold a nurse accountable for meeting all state practice
laws in the state in which the patient is located at the time care is rendered through the mutual
recognition of party state licenses;
1
4

6. Decrease redundancies in the consideration and issuance of nurse licenses; and
7. Provide opportunities for interstate practice by nurses who meet uniform licensure requirements.
ARTICLE II
Definitions
As used in this Compact:
a. “Adverse action” means any administrative, civil, equitable or criminal action permitted by a state’s
laws which is imposed by a licensing board or other authority against a nurse, including actions
against an individual’s license or multistate licensure privilege such as revocation, suspension,
probation, monitoring of the licensee, limitation on the licensee’s practice, or any other encumbrance
on licensure affecting a nurse’s authorization to practice, including issuance of a cease and desist
action.
b. “Alternative program” means a non-disciplinary monitoring program approved by a licensing board.
c. “Coordinated licensure information system” means an integrated process for collecting, storing and
sharing information on nurse licensure and enforcement activities related to nurse licensure laws that
is administered by a nonprofit organization composed of and controlled by licensing boards.
d. “Current significant investigative information” means:
1. Investigative information that a licensing board, after a preliminary inquiry that includes
notification and an opportunity for the nurse to respond, if required by state law, has reason to
believe is not groundless and, if proved true, would indicate more than a minor infraction; or
2. Investigative information that indicates that the nurse represents an immediate threat to public
health and safety regardless of whether the nurse has been notified and had an opportunity to
respond.
e. “Encumbrance” means a revocation or suspension of, or any limitation on, the full and unrestricted
practice of nursing imposed by a licensing board.
f. “Home state” means the party state which is the nurse’s primary state of residence.
g. “Licensing board” means a party state’s regulatory body responsible for issuing nurse licenses.
2
5
h. “Multistate license” means a license to practice as a registered or a licensed practical/vocational
nurse (LPN/VN) issued by a home state licensing board that authorizes the licensed nurse to practice
in all party states under a multistate licensure privilege.
i. “Multistate licensure privilege” means a legal authorization associated with a multistate license
permitting the practice of nursing as either a registered nurse (RN) or LPN/VN in a remote state.
j. “Nurse” means RN or LPN/VN, as those terms are defined by each party state’s practice laws.
k. “Party state” means any state that has adopted this Compact.
l. “Remote state” means a party state, other than the home state.
m. “Single-state license” means a nurse license issued by a party state that authorizes practice only
within the issuing state and does not include a multistate licensure privilege to practice in any other
party state.
n. “State” means a state, territory or possession of the United States and the District of Columbia.
o. “State practice laws” means a party state’s laws, rules and regulations that govern the practice of
nursing, define the scope of nursing practice, and create the methods and grounds for imposing
discipline. “State practice laws” do not include requirements necessary to obtain and retain a license,
except for qualifications or requirements of the home state.
ARTICLE III
General Provisions and Jurisdiction
a. A multistate license to practice registered or licensed practical/vocational nursing issued by a home
state to a resident in that state will be recognized by each party state as authorizing a nurse to
practice as a registered nurse (RN) or as a licensed practical/vocational nurse (LPN/VN), under a
multistate licensure privilege, in each party state.
b. A state must implement procedures for considering the criminal history records of applicants for initial
multistate license or licensure by endorsement. Such procedures shall include the submission of
fingerprints or other biometric-based information by applicants for the purpose of obtaining an
applicant’s criminal history record information from the Federal Bureau of Investigation and the
agency responsible for retaining that state’s criminal records.
3
6

c. Each party state shall require the following for an applicant to obtain or retain a multistate license in
the home state:
1. Meets the home state’s qualifications for licensure or renewal of licensure, as well as, all other
applicable state laws;
2. i. Has graduated or is eligible to graduate from a licensing board-approved RN or LPN/VN
prelicensure education program; or
ii. Has graduated from a foreign RN or LPN/VN prelicensure education program that (a) has been
approved by the authorized accrediting body in the applicable country and (b) has been verified
by an independent credentials review agency to be comparable to a licensing board-approved
prelicensure education program;
3. Has, if a graduate of a foreign prelicensure education program not taught in English or if English
is not the individual’s native language, successfully passed an English proficiency examination
that includes the components of reading, speaking, writing and listening;
4. Has successfully passed an NCLEX-RN® or NCLEX-PN® Examination or recognized
predecessor, as applicable;
5. Is eligible for or holds an active, unencumbered license;
6. Has submitted, in connection with an application for initial licensure or licensure by endorsement,
fingerprints or other biometric data for the purpose of obtaining criminal history record information
from the Federal Bureau of Investigation and the agency responsible for retaining that state’s
criminal records;
7. Has not been convicted or found guilty, or has entered into an agreed disposition, of a felony
offense under applicable state or federal criminal law;
8. Has not been convicted or found guilty, or has entered into an agreed disposition, of a
misdemeanor offense related to the practice of nursing as determined on a case-by-case basis;
9. Is not currently enrolled in an alternative program;
10. Is subject to self-disclosure requirements regarding current participation in an alternative
program; and
11. Has a valid United States Social Security number.
4
7

d. All party states shall be authorized, in accordance with existing state due process law, to take
adverse action against a nurse’s multistate licensure privilege such as revocation, suspension,
probation or any other action that affects a nurse’s authorization to practice under a multistate
licensure privilege, including cease and desist actions. If a party state takes such action, it shall
promptly notify the administrator of the coordinated licensure information system. The administrator
of the coordinated licensure information system shall promptly notify the home state of any such
actions by remote states.
e. A nurse practicing in a party state must comply with the state practice laws of the state in which the
client is located at the time service is provided. The practice of nursing is not limited to patient care,
but shall include all nursing practice as defined by the state practice laws of the party state in which
the client is located. The practice of nursing in a party state under a multistate licensure privilege will
subject a nurse to the jurisdiction of the licensing board, the courts and the laws of the party state in
which the client is located at the time service is provided.
f. Individuals not residing in a party state shall continue to be able to apply for a party state’s single-
state license as provided under the laws of each party state. However, the single-state license
granted to these individuals will not be recognized as granting the privilege to practice nursing in any
other party state. Nothing in this Compact shall affect the requirements established by a party state
for the issuance of a single-state license.
g. Any nurse holding a home state multistate license, on the effective date of this Compact, may retain
and renew the multistate license issued by the nurse’s then-current home state, provided that:
1. A nurse, who changes primary state of residence after this Compact’s effective date, must meet
all applicable Article III.c. requirements to obtain a multistate license from a new home state.
2. A nurse who fails to satisfy the multistate licensure requirements in Article III.c. due to a
disqualifying event occurring after this Compact’s effective date shall be ineligible to retain or
renew a multistate license, and the nurse’s multistate license shall be revoked or deactivated in
accordance with applicable rules adopted by the Interstate Commission of Nurse Licensure
Compact Administrators (“Commission”).
5
8

ARTICLE IV
Applications for Licensure in a Party State
a. Upon application for a multistate license, the licensing board in the issuing party state shall ascertain,
through the coordinated licensure information system, whether the applicant has ever held, or is the
holder of, a license issued by any other state, whether there are any encumbrances on any license or
multistate licensure privilege held by the applicant, whether any adverse action has been taken
against any license or multistate licensure privilege held by the applicant and whether the applicant is
currently participating in an alternative program.
b. A nurse may hold a multistate license, issued by the home state, in only one party state at a time.
c. If a nurse changes primary state of residence by moving between two party states, the nurse must
apply for licensure in the new home state, and the multistate license issued by the prior home state
will be deactivated in accordance with applicable rules adopted by the Commission.
1. The nurse may apply for licensure in advance of a change in primary state of residence.
2. A multistate license shall not be issued by the new home state until the nurse provides
satisfactory evidence of a change in primary state of residence to the new home state and
satisfies all applicable requirements to obtain a multistate license from the new home state.
d. If a nurse changes primary state of residence by moving from a party state to a non-party state, the
multistate license issued by the prior home state will convert to a single-state license, valid only in the
former home state.
ARTICLE V
Additional Authorities Invested in Party State Licensing Boards
a. In addition to the other powers conferred by state law, a licensing board shall have the authority to:
1. Take adverse action against a nurse’s multistate licensure privilege to practice within that party
state.
i. Only the home state shall have the power to take adverse action against a nurse’s license
issued by the home state.
ii. For purposes of taking adverse action, the home state licensing board shall give the same
priority and effect to reported conduct received from a remote state as it would if such
6
9

conduct had occurred within the home state. In so doing, the home state shall apply its own
state laws to determine appropriate action.
2. Issue cease and desist orders or impose an encumbrance on a nurse’s authority to practice
within that party state.
3. Complete any pending investigations of a nurse who changes primary state of residence during
the course of such investigations. The licensing board shall also have the authority to take
appropriate action(s) and shall promptly report the conclusions of such investigations to the
administrator of the coordinated licensure information system. The administrator of the
coordinated licensure information system shall promptly notify the new home state of any such
actions.
4. Issue subpoenas for both hearings and investigations that require the attendance and testimony
of witnesses, as well as, the production of evidence. Subpoenas issued by a licensing board in a
party state for the attendance and testimony of witnesses or the production of evidence from
another party state shall be enforced in the latter state by any court of competent jurisdiction,
according to the practice and procedure of that court applicable to subpoenas issued in
proceedings pending before it. The issuing authority shall pay any witness fees, travel expenses,
mileage and other fees required by the service statutes of the state in which the witnesses or
evidence are located.
5. Obtain and submit, for each nurse licensure applicant, fingerprint or other biometric-based
information to the Federal Bureau of Investigation for criminal background checks, receive the
results of the Federal Bureau of Investigation record search on criminal background checks and
use the results in making licensure decisions.
6. If otherwise permitted by state law, recover from the affected nurse the costs of investigations
and disposition of cases resulting from any adverse action taken against that nurse.
7. Take adverse action based on the factual findings of the remote state, provided that the licensing
board follows its own procedures for taking such adverse action.
b. If adverse action is taken by the home state against a nurse’s multistate license, the nurse’s
multistate licensure privilege to practice in all other party states shall be deactivated until all
7
10

encumbrances have been removed from the multistate license. All home state disciplinary orders
that impose adverse action against a nurse’s multistate license shall include a statement that the
nurse’s multistate licensure privilege is deactivated in all party states during the pendency of the
order.
c. Nothing in this Compact shall override a party state’s decision that participation in an alternative
program may be used in lieu of adverse action. The home state licensing board shall deactivate the
multistate licensure privilege under the multistate license of any nurse for the duration of the nurse’s
participation in an alternative program.
ARTICLE VI
Coordinated Licensure Information System and Exchange of Information
a. All party states shall participate in a coordinated licensure information system of all licensed
registered nurses (RNs) and licensed practical/vocational nurses (LPNs/VNs). This system will
include information on the licensure and disciplinary history of each nurse, as submitted by party
states, to assist in the coordination of nurse licensure and enforcement efforts.
b. The Commission, in consultation with the administrator of the coordinated licensure information
system, shall formulate necessary and proper procedures for the identification, collection and
exchange of information under this Compact.
c. All licensing boards shall promptly report to the coordinated licensure information system any adverse
action, any current significant investigative information, denials of applications (with the reasons for
such denials) and nurse participation in alternative programs known to the licensing board regardless
of whether such participation is deemed nonpublic or confidential under state law.
d. Current significant investigative information and participation in nonpublic or confidential alternative
programs shall be transmitted through the coordinated licensure information system only to party
state licensing boards.
e. Notwithstanding any other provision of law, all party state licensing boards contributing information to
the coordinated licensure information system may designate information that may not be shared with
non-party states or disclosed to other entities or individuals without the express permission of the
contributing state.
8
11

f. Any personally identifiable information obtained from the coordinated licensure information system by
a party state licensing board shall not be shared with non-party states or disclosed to other entities or
individuals except to the extent permitted by the laws of the party state contributing the information.
g. Any information contributed to the coordinated licensure information system that is subsequently
required to be expunged by the laws of the party state contributing that information shall also be
expunged from the coordinated licensure information system.
h. The Compact administrator of each party state shall furnish a uniform data set to the Compact
administrator of each other party state, which shall include, at a minimum:
1. Identifying information;
2. Licensure data;
3. Information related to alternative program participation; and
4. Other information that may facilitate the administration of this Compact, as determined by
Commission rules.
i. The Compact administrator of a party state shall provide all investigative documents and information
requested by another party state.
ARTICLE VII
Establishment of the Interstate Commission of Nurse Licensure Compact Administrators
a. The party states hereby create and establish a joint public entity known as the Interstate Commission
of Nurse Licensure Compact Administrators.
1. The Commission is an instrumentality of the party states.
2. Venue is proper, and judicial proceedings by or against the Commission shall be brought solely
and exclusively, in a court of competent jurisdiction where the principal office of the Commission
is located. The Commission may waive venue and jurisdictional defenses to the extent it adopts
or consents to participate in alternative dispute resolution proceedings.
3. Nothing in this Compact shall be construed to be a waiver of sovereign immunity.
b. Membership, Voting and Meetings
1. Each party state shall have and be limited to one administrator. The head of the state licensing
board or designee shall be the administrator of this Compact for each party state. Any
9
12

administrator may be removed or suspended from office as provided by the law of the state from
which the Administrator is appointed. Any vacancy occurring in the Commission shall be filled in
accordance with the laws of the party state in which the vacancy exists.
2. Each administrator shall be entitled to one (1) vote with regard to the promulgation of rules and
creation of bylaws and shall otherwise have an opportunity to participate in the business and
affairs of the Commission. An administrator shall vote in person or by such other means as
provided in the bylaws. The bylaws may provide for an administrator’s participation in meetings
by telephone or other means of communication.
3. The Commission shall meet at least once during each calendar year. Additional meetings shall
be held as set forth in the bylaws or rules of the commission.
4. All meetings shall be open to the public, and public notice of meetings shall be given in the same
manner as required under the rulemaking provisions in Article VIII.
5. The Commission may convene in a closed, nonpublic meeting if the Commission must discuss:
i. Noncompliance of a party state with its obligations under this Compact;
ii. The employment, compensation, discipline or other personnel matters, practices or
procedures related to specific employees or other matters related to the Commission’s
internal personnel practices and procedures;
iii. Current, threatened or reasonably anticipated litigation;
iv. Negotiation of contracts for the purchase or sale of goods, services or real estate;
v. Accusing any person of a crime or formally censuring any person;
vi. Disclosure of trade secrets or commercial or financial information that is privileged or
confidential;
vii. Disclosure of information of a personal nature where disclosure would constitute a clearly
unwarranted invasion of personal privacy;
viii. Disclosure of investigatory records compiled for law enforcement purposes;
ix. Disclosure of information related to any reports prepared by or on behalf of the Commission
for the purpose of investigation of compliance with this Compact; or
x. Matters specifically exempted from disclosure by federal or state statute.
10
13

6. If a meeting, or portion of a meeting, is closed pursuant to this provision, the Commission’s legal
counsel or designee shall certify that the meeting may be closed and shall reference each
relevant exempting provision. The Commission shall keep minutes that fully and clearly describe
all matters discussed in a meeting and shall provide a full and accurate summary of actions
taken, and the reasons therefor, including a description of the views expressed. All documents
considered in connection with an action shall be identified in such minutes. All minutes and
documents of a closed meeting shall remain under seal, subject to release by a majority vote of
the Commission or order of a court of competent jurisdiction.
c. The Commission shall, by a majority vote of the administrators, prescribe bylaws or rules to govern its
conduct as may be necessary or appropriate to carry out the purposes and exercise the powers of
this Compact, including but not limited to:
1. Establishing the fiscal year of the Commission;
2. Providing reasonable standards and procedures:
i. For the establishment and meetings of other committees; and
ii. Governing any general or specific delegation of any authority or function of the Commission;
3. Providing reasonable procedures for calling and conducting meetings of the Commission,
ensuring reasonable advance notice of all meetings and providing an opportunity for attendance
of such meetings by interested parties, with enumerated exceptions designed to protect the
public’s interest, the privacy of individuals, and proprietary information, including trade secrets.
The Commission may meet in closed session only after a majority of the administrators vote to
close a meeting in whole or in part. As soon as practicable, the Commission must make public a
copy of the vote to close the meeting revealing the vote of each administrator, with no proxy votes
allowed;
4. Establishing the titles, duties and authority and reasonable procedures for the election of the
officers of the Commission;
5. Providing reasonable standards and procedures for the establishment of the personnel policies
and programs of the Commission. Notwithstanding any civil service or other similar laws of any
11
14

party state, the bylaws shall exclusively govern the personnel policies and programs of the
Commission; and
6. Providing a mechanism for winding up the operations of the Commission and the equitable
disposition of any surplus funds that may exist after the termination of this Compact after the
payment or reserving of all of its debts and obligations;
d. The Commission shall publish its bylaws and rules, and any amendments thereto, in a convenient
form on the website of the Commission.
e. The Commission shall maintain its financial records in accordance with the bylaws.
f. The Commission shall meet and take such actions as are consistent with the provisions of this
Compact and the bylaws.
g. The Commission shall have the following powers:
1. To promulgate uniform rules to facilitate and coordinate implementation and administration of this
Compact. The rules shall have the force and effect of law and shall be binding in all party states;
2. To bring and prosecute legal proceedings or actions in the name of the Commission, provided
that the standing of any licensing board to sue or be sued under applicable law shall not be
affected;
3. To purchase and maintain insurance and bonds;
4. To borrow, accept or contract for services of personnel, including, but not limited to, employees of
a party state or nonprofit organizations;
5. To cooperate with other organizations that administer state compacts related to the regulation of
nursing, including but not limited to sharing administrative or staff expenses, office space or other
resources;
6. To hire employees, elect or appoint officers, fix compensation, define duties, grant such
individuals appropriate authority to carry out the purposes of this Compact, and to establish the
Commission’s personnel policies and programs relating to conflicts of interest, qualifications of
personnel and other related personnel matters;
12
15
7. To accept any and all appropriate donations, grants and gifts of money, equipment, supplies,
materials and services, and to receive, utilize and dispose of the same; provided that at all times
the Commission shall avoid any appearance of impropriety or conflict of interest;
8. To lease, purchase, accept appropriate gifts or donations of, or otherwise to own, hold, improve
or use, any property, whether real, personal or mixed; provided that at all times the Commission
shall avoid any appearance of impropriety;
9. To sell, convey, mortgage, pledge, lease, exchange, abandon or otherwise dispose of any
property, whether real, personal or mixed;
10. To establish a budget and make expenditures;
11. To borrow money;
12. To appoint committees, including advisory committees comprised of administrators, state nursing
regulators, state legislators or their representatives, and consumer representatives, and other
such interested persons;
13. To provide and receive information from, and to cooperate with, law enforcement agencies;
14. To adopt and use an official seal; and
15. To perform such other functions as may be necessary or appropriate to achieve the purposes of
this Compact consistent with the state regulation of nurse licensure and practice.
h. Financing of the Commission
1. The Commission shall pay, or provide for the payment of, the reasonable expenses of its
establishment, organization and ongoing activities.
2. The Commission may also levy on and collect an annual assessment from each party state to
cover the cost of its operations, activities and staff in its annual budget as approved each year.
The aggregate annual assessment amount, if any, shall be allocated based upon a formula to be
determined by the Commission, which shall promulgate a rule that is binding upon all party
states.
3. The Commission shall not incur obligations of any kind prior to securing the funds adequate to
meet the same; nor shall the Commission pledge the credit of any of the party states, except by,
and with the authority of, such party state.
13
16

4. The Commission shall keep accurate accounts of all receipts and disbursements. The receipts
and disbursements of the Commission shall be subject to the audit and accounting procedures
established under its bylaws. However, all receipts and disbursements of funds handled by the
Commission shall be audited yearly by a certified or licensed public accountant, and the report of
the audit shall be included in and become part of the annual report of the Commission.
i. Qualified Immunity, Defense and Indemnification
1. The administrators, officers, executive director, employees and representatives of the
Commission shall be immune from suit and liability, either personally or in their official capacity,
for any claim for damage to or loss of property or personal injury or other civil liability caused by
or arising out of any actual or alleged act, error or omission that occurred, or that the person
against whom the claim is made had a reasonable basis for believing occurred, within the scope
of Commission employment, duties or responsibilities; provided that nothing in this paragraph
shall be construed to protect any such person from suit or liability for any damage, loss, injury or
liability caused by the intentional, willful or wanton misconduct of that person.
2. The Commission shall defend any administrator, officer, executive director, employee or
representative of the Commission in any civil action seeking to impose liability arising out of any
actual or alleged act, error or omission that occurred within the scope of Commission
employment, duties or responsibilities, or that the person against whom the claim is made had a
reasonable basis for believing occurred within the scope of Commission employment, duties or
responsibilities; provided that nothing herein shall be construed to prohibit that person from
retaining his or her own counsel; and provided further that the actual or alleged act, error or
omission did not result from that person’s intentional, willful or wanton misconduct.
3. The Commission shall indemnify and hold harmless any administrator, officer, executive director,
employee or representative of the Commission for the amount of any settlement or judgment
obtained against that person arising out of any actual or alleged act, error or omission that
occurred within the scope of Commission employment, duties or responsibilities, or that such
person had a reasonable basis for believing occurred within the scope of Commission
14
17

employment, duties or responsibilities, provided that the actual or alleged act, error or omission
did not result from the intentional, willful or wanton misconduct of that person.
ARTICLE VIII
Rulemaking
a. The Commission shall exercise its rulemaking powers pursuant to the criteria set forth in this Article
and the rules adopted thereunder. Rules and amendments shall become binding as of the date
specified in each rule or amendment and shall have the same force and effect as provisions of this
Compact.
b. Rules or amendments to the rules shall be adopted at a regular or special meeting of the
Commission.
c. Prior to promulgation and adoption of a final rule or rules by the Commission, and at least sixty (60)
days in advance of the meeting at which the rule will be considered and voted upon, the Commission
shall file a notice of proposed rulemaking:
1. On the website of the Commission; and
2. On the website of each licensing board or the publication in which each state would otherwise
publish proposed rules.
d. The notice of proposed rulemaking shall include:
1. The proposed time, date and location of the meeting in which the rule will be considered and
voted upon;
2. The text of the proposed rule or amendment, and the reason for the proposed rule;
3. A request for comments on the proposed rule from any interested person; and
4. The manner in which interested persons may submit notice to the Commission of their intention to
attend the public hearing and any written comments.
e. Prior to adoption of a proposed rule, the Commission shall allow persons to submit written data, facts,
opinions and arguments, which shall be made available to the public.
f. The Commission shall grant an opportunity for a public hearing before it adopts a rule or amendment.
15
18
g. The Commission shall publish the place, time and date of the scheduled public hearing.
1. Hearings shall be conducted in a manner providing each person who wishes to comment a fair
and reasonable opportunity to comment orally or in writing. All hearings will be recorded, and a
copy will be made available upon request.
2. Nothing in this section shall be construed as requiring a separate hearing on each rule. Rules
may be grouped for the convenience of the Commission at hearings required by this section.
h. If no one appears at the public hearing, the Commission may proceed with promulgation of the
proposed rule.
i. Following the scheduled hearing date, or by the close of business on the scheduled hearing date if
the hearing was not held, the Commission shall consider all written and oral comments received.
j. The Commission shall, by majority vote of all administrators, take final action on the proposed rule
and shall determine the effective date of the rule, if any, based on the rulemaking record and the full
text of the rule.
k. Upon determination that an emergency exists, the Commission may consider and adopt an
emergency rule without prior notice, opportunity for comment or hearing, provided that the usual
rulemaking procedures provided in this Compact and in this section shall be retroactively applied to
the rule as soon as reasonably possible, in no event later than ninety (90) days after the effective
date of the rule. For the purposes of this provision, an emergency rule is one that must be adopted
immediately in order to:
1. Meet an imminent threat to public health, safety or welfare;
2. Prevent a loss of Commission or party state funds; or
3. Meet a deadline for the promulgation of an administrative rule that is required by federal law or
rule.
l. The Commission may direct revisions to a previously adopted rule or amendment for purposes of
correcting typographical errors, errors in format, errors in consistency or grammatical errors. Public
notice of any revisions shall be posted on the website of the Commission. The revision shall be
subject to challenge by any person for a period of thirty (30) days after posting. The revision may be
challenged only on grounds that the revision results in a material change to a rule. A challenge shall
16
19

be made in writing, and delivered to the Commission, prior to the end of the notice period. If no
challenge is made, the revision will take effect without further action. If the revision is challenged, the
revision may not take effect without the approval of the Commission.
ARTICLE IX
Oversight, Dispute Resolution and Enforcement
a. Oversight
1. Each party state shall enforce this Compact and take all actions necessary and appropriate to
effectuate this Compact’s purposes and intent.
2. The Commission shall be entitled to receive service of process in any proceeding that may affect
the powers, responsibilities or actions of the Commission, and shall have standing to intervene in
such a proceeding for all purposes. Failure to provide service of process in such proceeding to
the Commission shall render a judgment or order void as to the Commission, this Compact or
promulgated rules.
b. Default, Technical Assistance and Termination
1. If the Commission determines that a party state has defaulted in the performance of its
obligations or responsibilities under this Compact or the promulgated rules, the Commission shall:
i. Provide written notice to the defaulting state and other party states of the nature of the
default, the proposed means of curing the default or any other action to be taken by the
Commission; and
ii. Provide remedial training and specific technical assistance regarding the default.
2. If a state in default fails to cure the default, the defaulting state’s membership in this Compact
may be terminated upon an affirmative vote of a majority of the administrators, and all rights,
privileges and benefits conferred by this Compact may be terminated on the effective date of
termination. A cure of the default does not relieve the offending state of obligations or liabilities
incurred during the period of default.
3. Termination of membership in this Compact shall be imposed only after all other means of
securing compliance have been exhausted. Notice of intent to suspend or terminate shall be
17
20

given by the Commission to the governor of the defaulting state and to the executive officer of the
defaulting state’s licensing board and each of the party states.
4. A state whose membership in this Compact has been terminated is responsible for all
assessments, obligations and liabilities incurred through the effective date of termination,
including obligations that extend beyond the effective date of termination.
5. The Commission shall not bear any costs related to a state that is found to be in default or whose
membership in this Compact has been terminated unless agreed upon in writing between the
Commission and the defaulting state.
6. The defaulting state may appeal the action of the Commission by petitioning the U.S. District
Court for the District of Columbia or the federal district in which the Commission has its principal
offices. The prevailing party shall be awarded all costs of such litigation, including reasonable
attorneys’ fees.
c. Dispute Resolution
1. Upon request by a party state, the Commission shall attempt to resolve disputes related to the
Compact that arise among party states and between party and non-party states.
2. The Commission shall promulgate a rule providing for both mediation and binding dispute
resolution for disputes, as appropriate.
3. In the event the Commission cannot resolve disputes among party states arising under this
Compact:
i. The party states may submit the issues in dispute to an arbitration panel, which will be
comprised of individuals appointed by the Compact administrator in each of the affected party
states and an individual mutually agreed upon by the Compact administrators of all the party
states involved in the dispute.
ii. The decision of a majority of the arbitrators shall be final and binding.
d. Enforcement
1. The Commission, in the reasonable exercise of its discretion, shall enforce the provisions and
rules of this Compact.
18
21
2. By majority vote, the Commission may initiate legal action in the U.S. District Court for the District
of Columbia or the federal district in which the Commission has its principal offices against a party
state that is in default to enforce compliance with the provisions of this Compact and its
promulgated rules and bylaws. The relief sought may include both injunctive relief and damages.
In the event judicial enforcement is necessary, the prevailing party shall be awarded all costs of
such litigation, including reasonable attorneys’ fees.
3. The remedies herein shall not be the exclusive remedies of the Commission. The Commission
may pursue any other remedies available under federal or state law.
ARTICLE X
Effective Date, Withdrawal and Amendment
a. This Compact shall become effective and binding on the earlier of the date of legislative enactment of
this Compact into law by no less than twenty-six (26) states or December 31, 2018. All party states to
this Compact, that also were parties to the prior Nurse Licensure Compact, superseded by this
Compact, (“Prior Compact”), shall be deemed to have withdrawn from said Prior Compact within six
(6) months after the effective date of this Compact.
b. Each party state to this Compact shall continue to recognize a nurse’s multistate licensure privilege to
practice in that party state issued under the Prior Compact until such party state has withdrawn from
the Prior Compact.
c. Any party state may withdraw from this Compact by enacting a statute repealing the same. A party
state’s withdrawal shall not take effect until six (6) months after enactment of the repealing statute.
d. A party state’s withdrawal or termination shall not affect the continuing requirement of the withdrawing
or terminated state’s licensing board to report adverse actions and significant investigations occurring
prior to the effective date of such withdrawal or termination.
e. Nothing contained in this Compact shall be construed to invalidate or prevent any nurse licensure
agreement or other cooperative arrangement between a party state and a non-party state that is
made in accordance with the other provisions of this Compact.
19
22

f. This Compact may be amended by the party states. No amendment to this Compact shall become
effective and binding upon the party states unless and until it is enacted into the laws of all party
states.
g. Representatives of non-party states to this Compact shall be invited to participate in the activities of
the Commission, on a nonvoting basis, prior to the adoption of this Compact by all states.
ARTICLE XI
Construction and Severability
This Compact shall be liberally construed so as to effectuate the purposes thereof. The provisions of this
Compact shall be severable, and if any phrase, clause, sentence or provision of this Compact is declared
to be contrary to the constitution of any party state or of the United States, or if the applicability thereof to
any government, agency, person or circumstance is held invalid, the validity of the remainder of this
Compact and the applicability thereof to any government, agency, person or circumstance shall not be
affected thereby. If this Compact shall be held to be contrary to the constitution of any party state, this
Compact shall remain in full force and effect as to the remaining party states and in full force and effect as
to the party state affected as to all severable matters.
20
23
111 E. Wacker Drive, Ste. 2900, Chicago, IL 60601312.525.3600 nursecompact.com
Unlocking Access to Nursing Care Across the Nation
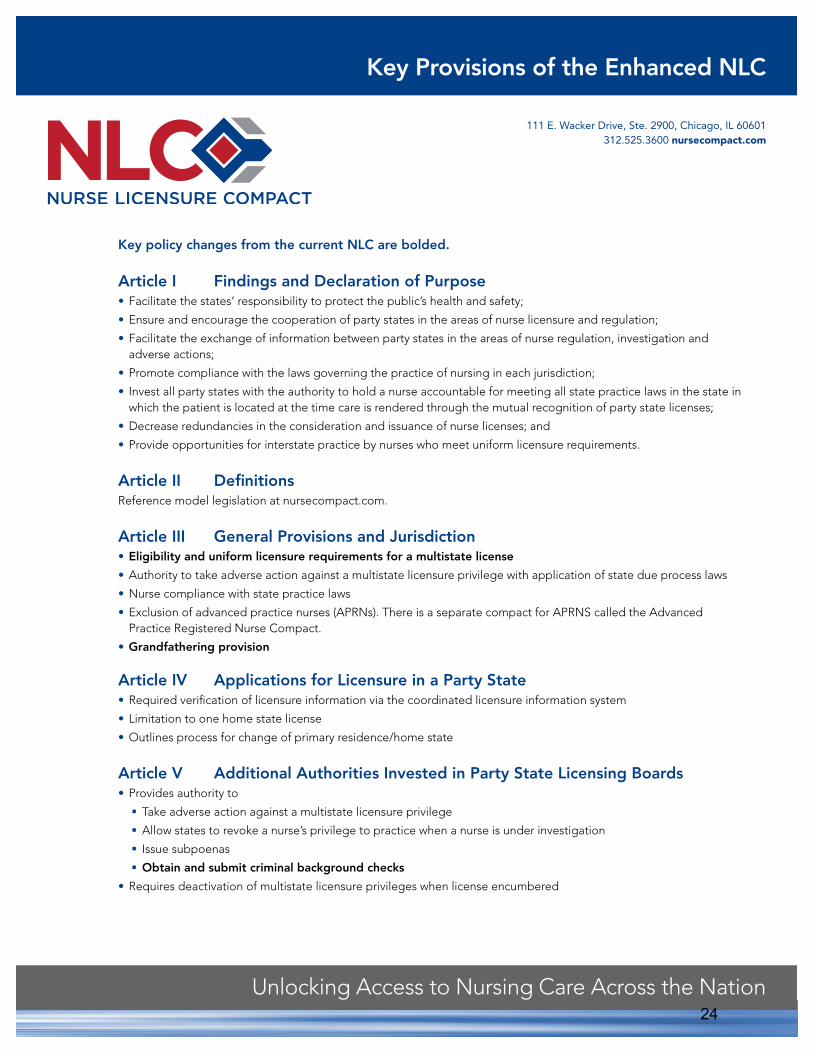
Key policy changes from the current NLC are bolded.
Article I Findings and Declaration of Purpose
Article II Definitions
Article III General Provisions and JurisdictionEligibility and uniform licensure requirements for a multistate license
Grandfathering provision
Article IV Applications for Licensure in a Party State
Article V Additional Authorities Invested in Party State Licensing Boards
Obtain and submit criminal background checks
Key Provisions of the Enhanced NLC
24

For more information about the NLC, visit nursecompact.com or email [email protected].
Article VI Coordinated Licensure Information System and Exchange of Information
Article VII Establishment of the Interstate Commission of Nurse Licensure Compact Administrators Establishes the governing body as a public agency known as an “Interstate Commission.”
Article VIII RulemakingAllows for rules to be adopted directly by the Commission. Such rulemaking is legally binding in all party states. There is no requirement that rules be ratified or adopted by individual states. Such rulemaking authority has been permitted and exercised by other interstate compacts. The procedural requirements are based on the national Model Administrative Procedures Act, which is similar to most state APAs and includes:
Provision for notice to the public of proposed and adopted rulesOpportunity for commentOpportunity for public hearingConsideration and voting upon proposed rulesResponding to comments received
Article IX Oversight, Dispute Resolution and Enforcement
Improved dispute resolution processes; andTermination from the NLC in the event no other means of compliance has been successful.
Article X Effective Date, Withdrawal and AmendmentAddresses the method for states to enter, withdraw from or amend the NLC.
Article XI Construction and Severability
25

111 E. Wacker Drive, Ste. 2900, Chicago, IL 60601312.525.3600 nursecompact.com
Unlocking Access to Nursing Care Across the Nation
FAQs: The Enhanced Nurse Licensure CompactWhat Policy Makers Need to Know
Why should our state join the Nurse Licensure Compact (NLC)?Dramatic changes are occurring in health care delivery. It is common for patients to travel across state lines for health care. Nurses often provide care across state borders both physically and electronically. The single state license (one license for every state in which the nurse practices) is not economical for nurses or employers. The current licensure model limits mobility of nurses and access to care for patients. In addition, it requires nurse educators that teach online students across the country to hold multiple licenses. The 100-year-old licensure model needs updating and the NLC offers an innovative approach that is safe and in lockstep with 21st century health care.
How does the NLC benefit our state?• Creates a model that allows nurses to practice freely among member states while still allowing states to retain
autonomy and the authority to enforce the state nurse practice act.• Eliminates redundancy, duplicative regulatory processes and unnecessary fees.• Improves access to licensed nurses during a disaster or other times of great need for qualified nursing services.• Benefits military spouses with nursing licenses who often relocate every two years.
How does the NLC keep patients safe? All nurses practicing under a multistate license must meet a minimum set of licensure requirements, including a fingerprint federal criminal background check. These requirements are based on the highest regulatory standards for licensed health care professionals. Nurses who fail to meet these requirements will not be eligible for a multistate license, and multistate privileges will be removed from nurses when disciplinary actions are taken against a home state multistate license.
Who supports the NLC and why? In a nationwide survey (2014), 70 percent of nurses support their state joining the NLC. The NLC has removed barriers and impediments to borderless practice. State hospital associations and health care facilities in every state support the NLC, as well as numerous nursing organizations.
Why is this idea coming forward now?The NLC is not a new idea. It has been in existence for 15 years, with 25 participating states, and has proven itself effective and safe. Recently all state boards of nursing met to add enhancements to the NLC to make it safer and better than ever.
How does the NLC support states’ rights?While the NLC has a minimum set of licensure requirements that all nurses must meet before obtaining a multistate license, a state entering the NLC still maintains its standards, scope of practice and discipline procedures. The NLC is the best way to regulate the practice of nursing while facilitating interstate practice and allowing each state to have jurisdiction over remote state nurses practicing within the state.
26

For more information about the NLC, visit nursecompact.com or email [email protected].
What is the fiscal impact on my state by joining the NLC?There is a nominal annual fee (currently $6,000) for NLC membership, though the overall fiscal impact of the NLC is unique and varies from state to state. NCSBN offers states grants of financial assistance to help offset the expense of joining and implementing the NLC. NCSBN is also funding the ongoing operational expenses of the compact governing body, the Interstate Commission of Nurse Licensure Compact Administrators.
Who opposes the NLC and why?In a few states, some nurse unions oppose the NLC; however, in the 25 current compact member states, no empirical evidence suggests that the NLC has ever been the basis for interfering in, or acting as an impediment to, lawful activities of any union acting on behalf of its member nurses. In fact, the model compact statute includes an enabling provision explicitly stating that “this compact does not supersede existing state labor laws.”
Does our state belong to any other compacts like this?While the NLC is the first interstate compact for a licensed profession, each state is already a member of an average of 25 interstate compacts. The NLC facilitates cross-border practice of nursing whether physically or via telehealth and puts critical systems in place that help keep patients safe. In 2015 the advent of new interstate licensure compacts for physicians, emergency medical technicians, psychologists and physical therapists began. Many states are introducing legislation regarding these additional compacts as well.
27

What Educators Need to Know About the Enhanced Nurse Licensure CompactA Brief History of the Nurse Licensure Compact (NLC)
R emoving barriers to cross-border practice, the Nurse Licensure Compact (NLC) is an interstate agreement allowing a nurse to have one license and the privilege to practice in other compact states. Implemented in
2000, the NLC fosters public protection and access to care through the mutual recognition of one state-based license that is enforced locally and recognized nationally. Along with a majority of state nurses associations, hospital associa-tions and health care facilities in every state overwhelmingly support the NLC. The NLC includes important patient safety features such as facilitation of the sharing of licensure, investigative and disciplinary action information among member states.
Since the NLC’s initial launch, advances in technology and an increasingly mobile nursing workforce and patient population have created the need to break down barriers to interstate practice. Access to care has expanded. Telehealth has transformed care delivery and erased geographic boundaries. In recent years, hundreds of bills with the goal of enabling telehealth in more than 44 states were introduced. The NLC has the ability to remove the licensure barrier to telehealth practice for more than 4 million nurses. While this change has transpired, other health professions have developed interstate licensure agreements and Congress began discussing the possibility of national licensure.
The Publication That Brings Nursing Regulation & Education Together SPECIAL ISSUE | MARCH 2017
IN THIS ISSUE …
Do faculty need more than one nursing license?
What will the enhanced NLC (eNLC) mean for nurses?
Compact Maps
Two Compacts Compared
continued on page 2
Compact StatusThe 2017 legislative session has gotten off to an exciting start. Utah and Arkansas became the first states in 2017 to enact the eNLC. Of the 21 states planning to introduce legislation, 18 have introduced eNLC legislation. In addition to Arkansas and Utah, those states include: Colorado, Georgia, Illinois, Iowa, Kentucky, Maine, Maryland, Massachusetts, Mississippi, Montana, Nebraska, Nevada, New Jersey, North Dakota, South Carolina and West Virginia. (see map on page 3). The effective date for the eNLC is the sooner of 26 states enacting the eNLC, or on Dec. 31, 2018. On the effective date, the Interstate Commission is formed and will begin to adopt rules to facilitate the implementation of the eNLC. The actual implementation of the compact by the states occurs six months after the effective date. This is the date on which nurses with eNLC multistate licenses may begin practicing in eNLC states. Once effective, the eNLC will recognize the current NLC for six months. After that, the eNLC will only be effective in eNLC states.
28

In 2013, NCSBN’s members began to discuss what the optimal licensure model would look like and eventually agreed that revising the current NLC (implemented in 25 states between 2000 and 2016) and the current APRN Compact (which was developed in 2001 but never implemented) would be in the best interests of all. In March of 2015 revisions to the two compacts were completed and in May 2015 a special assembly of delegates representing all BONs (two from each state) approved the new compacts. An ambitious initiative was kicked off to commit staff and financial resources to advocate for state adoption of the newly enhanced NLC (eNLC) and the APRN Compact.
Moving Forward—the Enhanced Nurse Licensure Compact (eNLC)Like the NLC, the eNLC increases access to health care, protects patient safety, reduces costs and supports state-of-the-art health care delivery. It also enhances nurses’ mobility across states and allows nurses to quickly cross state borders when there is a disaster. The eNLC is also cost-effective, since an organization may share the expenditure of
multiple licenses nurses can incur by crossing state lines. It also removes multiple and duplicate regulatory requirements, cutting down costs for nurses.
New provisions to the eNLC (as compared to the original NLC) include uniform license requirements (all states have the same licensure requirements) and state authority to obtain and submit criminal background checks.
In order to receive a multistate license in the eNLC, a nurse must meet the home state’s qualifications, graduate from a board of nursing-approved nursing education program, pass the NCLEX-RN® or NCLEX-PN® Exam, have no active discipline on their license, submit to a criminal background check, have no prior state or federal felony convictions and have a valid Social Security number. The eNLC also contains a grandfathering provision: a nurse already holding a home multistate license on their compact’s effective date can retain and renew that license. A nurse who
changes their primary state of residence after the NLC’s effective date must meet the new eNLC requirements to obtain a multistate license from their new home state.
To join, individual states must first enact eNLC model legislation. NCSBN staff are working with state legislatures to help accomplish this by testifying at committee hearings, participating in telephone and in-person meetings with legislators in target states, and drafting language to help bills move forward.
What Educators Need to Know continued from page 1
SPECIAL ISSUE | MARCH 2017 www.ncsbn.org 2
The eNLC is also cost-effective, since an organization may share the expenditure of multiple licenses nurses can incur by crossing state lines.
The effective date for the eNLC is the sooner of 26 states enacting the eNLC, or on Dec. 31, 2018. On the effective date, the Interstate Commission is formed and will begin to adopt rules to facilitate the implementation of the eNLC. The actual implementation of the compact by the states occurs six months after the effective date. This is the date on which nurses with eNLC multistate licenses may begin practicing in eNLC states. Once effective, the eNLC will recognize the current NLC for six months. After that, the eNLC will only be effective in eNLC states.
What is the Difference Between When the eNLC Becomes “Effective” and When It Is “Implemented?”
29

Y ou may if you are faculty teaching didactic courses, or supervising clinical experiences, and your students are located outside the state in which your nursing pro-
gram is located. Just as nurses who work in clinical settings and care for patients in another state via telehealth, faculty who teach online students located in another state usually require additional nursing licenses unless a state offers an exemption for faculty or it is currently part of the Nurse Licensure Compact (NLC).
Many faculty and their deans are unaware of this important requirement. In most states, faculty must abide by the same principle as nurses in clinical practice. Practice is where the patients (or students) are located. Therefore, if the students are located in states different from the home state of the nursing program, faculty require additional licenses. Faculty teaching in online programs should refer to NCSBN’s website for details regarding this.
One exception to this rule is the NLC. If you are licensed in a state that is a member of the NLC and the students are located in other NLC states, you do not need an additional license to teach in those states; you most likely have a multistate license and have already been granted the privilege to practice. See the map of current NLC states below.
Presently, 25 states are members of the NLC, however, the newly enhanced NLC (eNLC) is now being adopted by states and will replace the NLC in these states. This newly enhanced compact offers more uniformity in terms of licensure requirements and it is expected to have greater participation that will extend beyond the original 25 states. For more information on the eNLC see nursecompact.com.
Once the implementation of the eNLC compact occurs (six months after the effective date), it will be important for educators in eNLC states to know which states are part of the eNLC and which states are not, including those states that remain active in the NLC and do not enact the eNLC. They will need licenses to practice (or teach by distance learning) if they do not reside in a state that is a member of the eNLC. This information will also be important for students.
States are also beginning to adopt the APRN Compact, so faculty and advanced practice registered nurse (APRN) students should stay up to date on the APRN Compact as well.
If your state has introduced a bill to enact the eNLC you can help pass the legislation by contacting your legislator. Access these websites for information on how to do that, and keep up on which states have adopted the eNLC and APRN Compact.
Do Faculty Need More Than One Nursing License?
SPECIAL ISSUE | MARCH 2017 www.ncsbn.org 3
NH
MD
RI
DE
GUAM
MARIANAISLANDS (MP) AMERICAN
SAMOA (AS)
VIRGIN ISLANDS
ME
ID
UT
AZ
CO
NM
TX
NE
SD
ND
IA
WI
AR
MS
TN
KY
SC
NC
VAMO
DC
MT
NH
MDDE
GUAM
MARIANAISLANDS (MP) AMERICAN
SAMOA (AS)
VIRGIN ISLANDS
ME
ID
UT
AZOK
FL
NV
NE
SD
ND
IA
MS
TN
SC
VAMO
DC
MT
WY
MA
NJCOIL
WVKY
AR
GA
MAP 2:
States that have enacted the eNLC
States that have filed for eNLC (as of 3/8/2017)
MAP 1:
States in NLC
30

SPECIAL ISSUE | MARCH 2017 www.ncsbn.org 4
What Will the Enhanced NLC (eNLC) Mean for Nurses? What does the eNLC mean for nurses in the current NLC?
If your state enacts the eNLC, you will be grandfathered and no further action is needed, unless you move to another state. Then you will be required to meet all the uniform licensure requirements to receive a multistate license from that state.
The states that are part of the eNLC are not exactly the same as the original NLC. If you have an eNLC multistate license, you can only practice in those designated eNLC states (see map on page 3). You will need a single state license issued by every other state in which you plan to practice to continue to deliver care in each of those states..
What does the eNLC mean for employers? Your nurses will now be able to practice (in person or by telehealth)
in other eNLC states with just one license obtained in their state of residence.
Faculty and military spouses will just need one license to teach or practice across states in the eNLC.
The eNLC is only for registered nurses (RNs) or licensed practical/vocational nurses (LPNs/VNs), not for advanced practice registered nurses (APRNs). APRNs have another compact that states are considering.
What are the Uniform Licensure Requirements for an eNLC multistate license?An applicant for licensure in a state that is part of the eNLC will need to meet the following uniform licensure requirements:
1. Has met the requirements for licensure in the home state (state of residency);
2. a. Has graduated from a board of nursing-approved education program; or
b. Has graduated from a foreign education program (approved by the authorized accrediting body in the applicable country and verified by an independent credentials review agency);
3. Has passed an English proficiency examination (applies to graduates of a foreign education program not taught in English or if English is not the individual’s native language);
4. Has passed the NCLEX-RN or PN Examination or predecessor exam;
5. Is eligible for or holds an active, unencumbered license (i.e., without active discipline);
6. Has submitted to state and federal fingerprint-based criminal background checks;
7. Has no state or federal felony convictions;
8. Has no misdemeanor convictions related to the practice of nursing (determined on a case-by-case basis);
9. Is not currently a participant in an alternative program;
10. Is required to self-disclose current participation in an alternative program; and
11. Has a valid United States Social Security number.
31
SPECIAL ISSUE | MARCH 2017 www.ncsbn.org 5
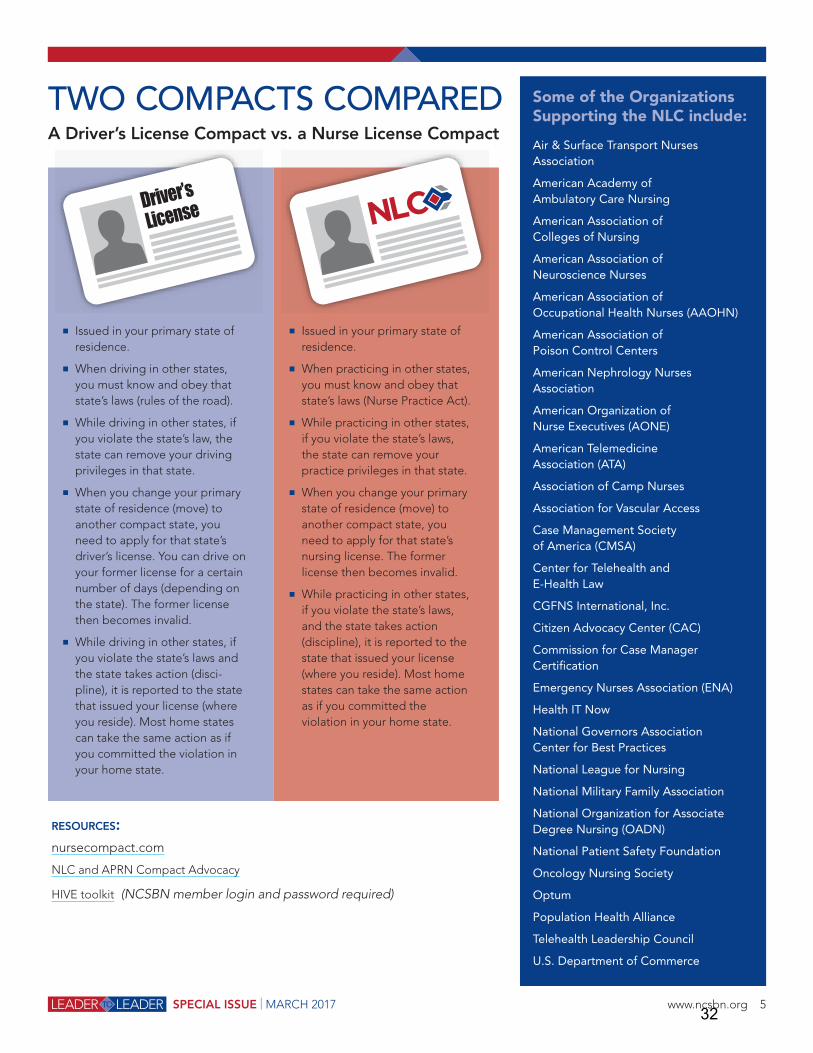
TWO COMPACTS COMPAREDA Driver’s License Compact vs. a Nurse License Compact
Issued in your primary state of residence.
When driving in other states, you must know and obey that state’s laws (rules of the road).
While driving in other states, if you violate the state’s law, the state can remove your driving privileges in that state.
When you change your primary state of residence (move) to another compact state, you need to apply for that state’s driver’s license. You can drive on your former license for a certain number of days (depending on the state). The former license then becomes invalid.
While driving in other states, if you violate the state’s laws and the state takes action (disci-pline), it is reported to the state that issued your license (where you reside). Most home states can take the same action as if you committed the violation in your home state.
RESOURCES:nursecompact.com
NLC and APRN Compact Advocacy
HIVE toolkit (NCSBN member login and password required)
Issued in your primary state of residence.
When practicing in other states, you must know and obey that state’s laws (Nurse Practice Act).
While practicing in other states, if you violate the state’s laws, the state can remove your practice privileges in that state.
When you change your primary state of residence (move) to another compact state, you need to apply for that state’s nursing license. The former license then becomes invalid.
While practicing in other states, if you violate the state’s laws, and the state takes action (discipline), it is reported to the state that issued your license (where you reside). Most home states can take the same action as if you committed the violation in your home state.
Some of the Organizations Supporting the NLC include:
Air & Surface Transport Nurses Association
American Academy of Ambulatory Care Nursing
American Association of Colleges of Nursing
American Association of Neuroscience Nurses
American Association of Occupational Health Nurses (AAOHN)
American Association of Poison Control Centers
American Nephrology Nurses Association
American Organization of Nurse Executives (AONE)
American Telemedicine Association (ATA)
Association of Camp Nurses
Association for Vascular Access
Case Management Society of America (CMSA)
Center for Telehealth and E-Health Law
CGFNS International, Inc.
Citizen Advocacy Center (CAC)
Commission for Case Manager Certification
Emergency Nurses Association (ENA)
Health IT Now
National Governors Association Center for Best Practices
National League for Nursing
National Military Family Association
National Organization for Associate Degree Nursing (OADN)
National Patient Safety Foundation
Oncology Nursing Society
Optum
Population Health Alliance
Telehealth Leadership Council
U.S. Department of Commerce
!"#$%"&'()#*%+'%
32
111 E. Wacker Drive, Ste. 2900, Chicago, IL 60601312.525.3600 nursecompact.com
Unlocking Access to Nursing Care Across the Nation
Introduction• The eNLC, much like the current NLC, will develop rules
to facilitate its administration and operation.• In the eNLC, rulemaking powers are exercised by
the governing body, the Commission, made up of a representative from each member state who is the executive director of the state board of nursing (BON) or designee of the party state.
• Each member state has a seat on the Commission and therefore has a voice and a vote in the rulemaking process.
• This process is very similar to the rulemaking process that most state BONs have in place today (see more details of the process outlined on page 2). The eNLC Rulemaking Procedures are consistent with provisions of the Model State Administrative Procedures Act (APA), which is the basis for most existing State APAs.
• The eNLC rules are dependent on the statute(s) they purport to implement. Therefore, each rule must be premised on corresponding compact statute(s). As such, the Commission cannot draft rules related to other areas of a state’s Nurse Practice Act (NPA) as it would be outside of the Commission’s scope of authority. For example, the rulemaking authority of the eNLC, the Commission, could not promulgate a rule pertaining to scope of practice, since the eNLC does not address scope of practice in the statute.
• The rules are administrative in nature and seek to clarify and give further definition to the statutes.
• The rules are related to the operations and
Anticipated Process for Rulemaking by the Commission
implementation of the eNLC. As examples, the Model Rules of the current NLC can be viewed online at https://www.ncsbn.org/NLC_Model_Rules.pdf.
• Final rules will ultimately by adopted by the Commission after the eNLC becomes effective. Some examples of potential rules for the enhanced NLC may include the following:1. A multistate license shall not be issued by a party state
to any individual whose primary state of residence is another party state.
2. A license issued by a party state authorizing practice only in that state and not authorizing practice in other party states (a single state license) shall be clearly identified as valid only in the state of issuance. The license will be identified in Nursys, the national licensure database, as a single state license.
3. Before a multistate license is issued: a. That party state shall query Nursys to determine
current licensure status, current or previous disciplinary action, and any current significant investigative information.
b. If an applicant is found to be under investigation in another party state, the new home state shall contact the investigating state to determine eligibility for licensure.
• In fact, many of the policies of the current NLC will be suggested as eNLC rules. Those policies can be viewed online at https://www.ncsbn.org/Policies_per_081315.pdf.
Why is rulemaking being done this way?• In making comprehensive enhancements to the NLC
(adopted May 2015), one goal was to bring the current NLC up to common, modern interstate compact standards. Rulemaking by the governing Commission is standard practice among modern interstate compacts and necessary for efficiency, consistency and clarity.
• Traditional rulemaking processes have proven to be inefficient for interstate commissions. In the current NLC’s 17-year history, a state-by-state staggered rule
promulgation process has hindered rule consistency across member states. For example, in 2012, the Nurse Licensure Compact Administrators (NLCA) voted to amend a rule, which then needed to be implemented via each state’s rulemaking processes. As of 2017, three states still have not implemented the amended rule. Rulemaking processes by the Commission in the eNLC eliminates this type of problem and allows for the adoption of rules and amendments to rules to occur simultaneously among member states.
33
For more information about the NLC, visit nursecompact.com or email [email protected]/17
NCSBN’s Role • On May 5, 2015, NCSBN’s Delegate Assembly voted to
adopt the model language of the eNLC legislation. In August of 2015, NCSBN’s Board of Directors appointed a work group to do the preliminary work of drafting proposed rules for the eNLC. This work group consisted of executive directors of six member boards as well as an attorney and NCSBN staff. The work group has met regularly since its inception.
• Since only the future Commission has the authority to draft, amend or adopt eNLC rules, the final version of proposed eNLC rules developed by the work group will be forwarded to the future Commission as recommendations for consideration. The recommendations of the work group are not binding on the Commission. Upon commencement of the
Commission, it is anticipated that rulemaking will be among its initial priorities. The Commission may choose to accept, reject or accept with revisions the recommendations of the work group.
• Prior to forwarding the work group’s recommendations to the Commission, NCSBN will disseminate the recommendations to its member boards and key stakeholders for comment. This does not preclude the public comment period that the Commission will post as a procedure of its rulemaking process, as defined in eNLC statute. It is anticipated the distribution of the work group recommendations will take place in the spring of 2017. Recommended rules and comments received will be forwarded to the Commission upon the eNLC’s effective date.
The Commission’s Rulemaking Process 1. The Commission files notice of proposed rulemaking at least 60 days prior to meeting:
a. On the Commission website; andb. On each member board website (or state publication for publishing of proposed rules).
2. The notice of proposed rulemaking includes:a. The time, date and location of the meeting; b. The text of the proposed rule or amendment (with the reason for the rule);c. A request for public comments; andd. A process for public to attend meeting or submit comments.
3. Commission schedules public hearing before it adopts a rule or amendment.a. The place, time and date of hearing is published.b. Anyone may have the opportunity to comment orally or in writing. c. The Commission gives consideration to all written and oral comments received.
4. Rules and/or amendments to the rules are voted on and adopted at Commission meetings.
Summary 1. The rules the Commission promulgates only pertain to operations and implementation of the eNLC. The rules help
to operationalize the eNLC and to bring clarity where needed. Rules do not pertain to other areas of a state’s NPA, such as scope of practice, grounds for discipline, etc.
2. Citizens of each eNLC state will still be provided with notice about a proposed rule and will have the ability to comment on a rule or amendment.
3. Rulemaking by the Commission is not new to any state. State legislatures in 50 states have already enacted three interstate compacts which include rulemaking by the Commissions of those compacts. The three interstate compacts are:a. Interstate Compact for Adult Offender Supervision;b. Interstate Compact for Juveniles; andc. Interstate Compact for the Education of Military Children.
34

ABN E-NEWS
Follow us on Facebook and Twitter (@AlBoardNsg)
- - -
-
-‐
-‐
-
-
35

-
-
- -
- -
-
- -
- -
-
--
36

38
12
39

THE NURSING LICENSURE COMPACT AND APRN COMPACT: A BAD OPTION FOR WASHINGTON
I. INTRODUCTION
The National Council of State Boards of Nursing (NCSBN), a private, Chicago-based trade association, has recently proposed revised versions of two previously proposed compacts for multistate nursing practice: a Nursing Licensure Compact (NLC) for registered nurses and licensed practical nurses and an Advanced Practice Registered Nurse (APRN)* Compact.
The NCSBN Compacts are a bad option for Washington, for Washington nurses and for Washington patients. Washington lawmakers should reject them.
NCSBN portrays the Compacts as advancing public protection and access to care, but in fact they would do neither. The NLC and APRN Compacts authorize nurses in party states (states that participate in the compacts) to practice in all other party states. A nurse would hold a “multistate license” from her or his home state (defined as the state of residence) granting privileges to practice in all other party states. Both compacts define the site of a nurse’s practice as the state in which the patient is located at the time services are provided. This would apply not only to nurses who are physically present and providing care to patients in another state; it would also apply to nurses who are providing services through electronic communications. Thus, a nurse might be physically located in Washington but, if providing assessment, advice, counseling or other services via phone or computer to a patient in another state, she or he would be considered to be practicing in that other state.
* APRNs include nurse practitioners, certified nurse- midwives, certified registered nurse anesthetists and clinical nurse specialists – regulated in Washington as Advanced Registered Nurse Practitioners (ARNPs).
NCSBN proposed a prior version of the NLC in 1998 but found limited success in convincing states to adopt it. By 2010, twenty-four states had joined the NLC. In the five years since, one additional state joined. Twenty-five states and the District of Columbia, accounting for almost two-thirds of the U.S. population, declined to adopt it. Among the states rejecting the previous NLC are Washington, Oregon, Nevada, California, New York, Florida and NCSBN’s home state, Illinois. NCSBN’s prior APRN Compact, launched in 2002, was even less successful: it was adopted by only three states and never implemented.
However, since proposing the revised NLC and APRN Compact in 2015, NCBSN has launched an aggressive lobbying effort to convince lawmakers in several states, including Washington, to adopt them.
The Washington State Nurses Association (WSNA) and the American Nurses Association (ANA) are committed to reasonable, efficient regulation of nursing practice across states. But the current NCSBN Compacts pose several serious concerns:
• Despite claims that the Compacts will improve public protection and access to care, they will do neither.
• Instead, they create troubling new complications in regulating nursing practice by imposing unworkable approaches such as defining practice as occurring wherever the patient is located, even when care is provided remotely through electronic communication.
• The APRN Compact will create additional new complications for advanced practice and contains contradictory language regarding
40
!2!"
whether Washington ARNPs will have to practice under physician oversight when practicing out-of-state;
• The Compacts erode Washington state sovereignty by creating powerful and unaccountable new private bureaucracies with significant power over the states.
• The Compacts will impose new but undetermined expenses and likely result in revenue losses that could result in decreased services or increased licensure fees.
• Proponents’ comparisons to existing compacts—such as driver’s license agreements/compacts and the Interstate Medical Licensure Compact—fall short; there are fundamental differences between them and the NCSBN Compacts.
II. THE NCSBN COMPACTS DO NOT IMPROVE PUBLIC PROTECTION
Proponents of the revised NCBSN Compacts argue that they will enhance nursing licensing boards’ ability to protect the public. But the few improvements promised by the Compacts can be accomplished—and, to large extent, have already been accomplished—through less complex, intrusive and overreaching means than adopting the Compacts.
A. The Compacts’ major protections are already in place or pending in Washington
For example, the Compacts call for states’ participation in a coordinated licensing information system. But participation in such a system does not require states to adopt the NCSBN Compacts. In fact, almost all states (including Washington) already participate in the current information system, NURSYS. That system makes information on nurses’ licensure status and discipline history available to the public. (Currently, NURSYS makes information on significant investigations
available only to Compact states. This could be expanded to include other states).
The Compacts require criminal background checks, including fingerprinting or other biometric testing. (The prior versions of the Compacts did not include this requirement). But states can require this without adopting the Compacts. A growing number of states already do. Washington requires federal criminal background checks on out-of-state applicants, and a proposal to require them for all applicants is pending. The Uniform Licensing Requirements put forward by NCSBN in 2011 include this requirement, together with other standards and practices designed to improve public protection. NCSBN has urged all boards of nursing--not just those who participate in the Compacts--to adopt the Uniform Licensing Requirements.
In other words, currently any nurse who wishes to practice in Washington must obtain a Washington license and meet Washington’s standards, which already include screening their licensure history, federal criminal background checks for out-of-state applicants, and are anticipated to include such background checks for all applicants. The Compacts are not needed for any of these measures—these provisions in the Compacts would do nothing to improve public protection in Washington.
B. Despite these protections, important gaps remain
In addition, while criminal background checks and participation in NURSYS are important steps toward protecting the public, they leave some significant gaps that the Compact does not address. States vary in their disciplinary procedures and standards: conduct that would result in investigation and discipline in one state may not do so in another state. Depending on the state in which that conduct occurs, it may not be reported at all. And NURSYS depends on each state board to enter discipline data efficiently—if a state fails to do
41

!3!"
so, other states cannot be notified in a timely manner.
C. The Compacts would allow out-of-state nurses to practice without meeting Washington’s requirements
Although the Compacts require that a nurse practicing in a party state must comply with the state practice laws of the state in which the client is located at the time service is provided, the parameters of this requirement are not made clear.
The NLC allows any nurse with an unencumbered license in her or his home state to practice in other party states. But some states differ in regard to nursing education program requirements, including requirements for supervised clinical experiences. And states vary widely in their requirements for license renewal. For example, in 2011, the Washington State Nursing Care Quality Assurance Commission (NCQAC) adopted continuing competence requirements: Washington nurses must have at least 531 hours of active practice and 45 hours of continuing education every three years. And in 2014, the legislature approved new requirements that RNs, LPNs and most ARNPs—among other health professionals—complete an approved, one-time training of at least 6 hours in suicide assessment, treatment, and management.
The NCSBN Compacts do not directly address continued competence issues, but there is ample reason to believe that Washington’s requirements for continued competence would not apply to out-of-state nurses practicing here if the Compacts are adopted. In a 2012 document regarding the prior version of the NLC, the Nursing License Compact Administrators (NLCA) emphasized that nurses are not held to the continued competence requirements of any state other than their home state—if they are licensed in their home state, they qualify to practice in any other party state1. There is no reason to expect that the language of the current NLC will lead to a different
interpretation. Yet some states have no requirements at all for continued licensure beyond paying a renewal fee. Some have other requirements that may fall short of Washington’s—e.g., having no requirements for recent active nursing practice or no requirements for continuing education. No state other than Washington requires training in assessing, treating and managing suicide.
If Washington adopts the Compacts, we will have ceded our right to determine and enforce the standards for practice that our policy- makers have determined are necessary to ensure safe practice. Why set clear standards for competent practice if they will apply to some nurses practicing in our state but not others?
D. There is no reason to expect the Compacts to improve access to care in Washington
Despite claims that the Compacts will improve access to care, there is no evidence to suggest that they would do so for Washington. Out-of- state nurses who want to practice in Washington are able to do so without significant delay: NCQAC processes endorsement of out-of-state licenses rapidly. Nor is there evidence that the Compacts will increase access to telehealth services (i.e., services provided through electronic communications technologies) in Washington. Further, Washington is a pioneer in authorizing ARNPs to practice without the unnecessary restrictions that have imposed barriers to access in other states. The Compacts would do nothing to promote access to their services.
III. THE COMPACTS CREATE TROUBLING NEW COMPLICATIONS IN REGULATING NURSING PRACTICE
While the Compacts would offer no real improvement in public protection or access, in several respects they would create significant new complications in regulating nursing practice.
42

!4!"
A. Defining practice as taking place in patient’s location is an unworkable approach
The issues sound simple: Nurses are increasingly mobile, but current state-based licensure requires multiple licenses for nurses who practice in more than one state. And the increasing use of electronic communications technologies means that many nurses are practicing across state lines. The Compacts, we are told, will provide a clearer legal basis for their practice.
The NLC and APRN Compact both define nursing practice as taking place in the location where the patient is receiving services. This may be logical when a nurse is providing care while physically present in another state. But when providing care remotely through electronic technologies, it creates significant complications.
Some nurses work in settings such as call centers or advice lines that are set up as “telehealth” practices that primarily use communications technologies to assess, advise and/or counsel patients remotely in their homes. These nurses provide services to patients from multiple states, often in the course of a few hours. Because the Compacts say that practice takes place where the patient is located, these nurses would be expected to be familiar with the practice acts, rules and policies of each of those states.
However, under the Compacts, any use of communications technologies across state lines would be considered interstate practice. When the NLC says “A nurse practicing in a party state must comply with the state practice laws of the state in which the client is located at the time service is provided,” it does not distinguish designated telehealth practices—those in which nurses practice primarily through electronic communications technologies—from settings in which larger numbers of nurses work, such as
outpatient clinics and practices, emergency departments, surgical practices, case management, and other settings or roles in which nurses often have preadmission, post- discharge or ongoing contact with patients.
Some of those patients may reside out of state. And virtually any patient may be out of state or even out of the country temporarily—on vacation, on a business trip, or visiting family. The ubiquitous use of mobile communications devices, such as smart phones, tablets, and laptop computers, means that a nurse may be providing services to a “local” patient who happens to be in another state or country at the time. The nurse may not even be aware that the patient is temporarily out of state.
Consider these scenarios:
An out-of-state patient seeking treatment in Washington: A patient from Eastern Idaho chooses to seek elective surgery at a Spokane hospital. Shortly after discharge, the patient calls to ask questions about follow-up care and speaks to a wound care nurse. Later, the patient alleges that the nurse gave incorrect advice and that the patient suffered complications as a result. Although the patient chose to receive care from Washington providers, the nurse will now need to answer to the Idaho Board of Nursing, and possibly to the Idaho court system as well—in addition to Washington State.
A local patient temporarily out of state: A patient who lives in Olympia is seen in the emergency department of an Olympia hospital. A few days later, while visiting family in Montana, the patient receives a follow-up call on her cell phone from a nurse at the hospital. The patient later alleges that the nurse gave advice that exceeded her scope of practice. The nurse would be considered to be practicing nursing in Montana, perhaps without even knowing it. She would be subject to Montana’s jurisdiction and judged according to Montana’s scope of practice laws.
A nursing faculty member with students who are out of state: Because the Compacts state
43

!5!"
that the site of practice is the location where the client is receiving services, nursing faculty in Washington could find themselves subject to the jurisdiction of other states if they have students who are located in other Compact states, either as residents or visitors. This would apply to faculty who teach on-line courses— and potentially to any course if the faculty member is in contact via email, telephone or the Web with a student who is out of state at the time.
B. Regulating practice while physically out of state does not require a complex new regulatory mechanism
In care that involves the nurse’s physical presence, identifying the site of practice as the location where the patient is receiving services is less complicated, since it is also the site where the nurse is located at the time. However, the limited instances in which a nurse is temporarily located in another state do not warrant a whole new complex regulatory mechanism. Some nurses may practice occasionally in a neighboring state. When “traveling” nurses, who work for agencies that assign nurses to hospitals around the country, require multiple licenses, that detail and expense is generally the responsibility of the nurse’s employing agency. When nurses seek to volunteer assistance following a disaster, states will generally permit out-of-state nurses to practice on a temporary basis.
Of course, a far more common scenario is when a nurse changes residence from one state to another and plans to practice in the new state. Currently that nurse needs to obtain a license in her new state. Under the NCSBN Compacts, this requirement would not change: a nurse who changes her state of residence would still be required to obtain a license in her new home state.
C. The Compacts will mean losing opportunities to ensure that nurses practicing here are familiar with Washington nursing practice
Each state in the U.S. enacts and enforces its own nurse practice act. These practice acts reflect some differences from state to state. As noted earlier, these often include differences in curriculum and clinical experience requirements, especially for basic practice. States differ in standards for delegating tasks or assigning functions to other nursing personnel. They differ with regard to scopes of practice, particularly for licensed practical nurses (LPNs), which has implications not only for out-of-state LPNs practicing in Washington, but also for RNs who work with them.
Requiring nurses to be licensed in Washington before practicing here provides an opportunity to educate them about the specifics of nursing practice and regulation in Washington and to inform them of changes in relevant state legislation, regulation or policy related to nursing practice. If Washington adopts the Compacts, it means that almost any nurse licensed in another party state—literally hundreds of thousands of nurses—would be authorized to practice here without any official notice or any contact at all with the Nursing Care Quality Assurance Commission.
D. The Compacts’ definition of “home state” is confusing and illogical
Under the Compacts, a nurse’s “home state”— the state in which the nurse resides—is the state that issues her or his license. That state authorizes the nurse’s multistate privileges. Thus, a nurse who lives in Oregon or Idaho and commutes into Washington for work could no longer be licensed in Washington. The nurse would instead need to be licensed in her or his state of residence and be authorized by that state to practice in other party states, including Washington. If a nurse who lives and works in Washington moves across the state border while remaining at the same job in Washington, the nurse would need to inactivate her or his Washington license and obtain a license in the new state of residence, even if she or he has no intention of practicing there. A nurse might spend her entire career practicing in
44

!6!"
Washington yet be required to be licensed in another state.
E. The APRN Compact creates additional complications for advanced practice nursing Washington is a pioneer in recognizing the critical role that APRNs play in ensuring access to high quality, affordable health care. Our state has been a model for the rest of the nation in promoting APRNs’ ability to practice to the full extent of their education and training. It is vitally important that we continue to play a leadership role in advanced nursing practice. Unfortunately, adopting the APRN Compact would pose some serious concerns.
The APRN Compact defines APRN as “a registered nurse who has gained additional specialized knowledge, skills and experience through a program of study recognized or defined by the Interstate Commission of APRN Compact Administrators . . . , and who is licensed to perform advanced nursing practice.” In other words, the new Interstate Commission would “recognize or define” educational standards for APRN practice, and Washington would be bound by those standards, which have not yet been determined.
Washington imposes no legal requirements for APRNs to practice under the supervision of or in collaboration with another health professional. The APRN Compact seems at first to be consistent with Washington law when it states that “[a]n APRN issued a multistate license is authorized to assume responsibility and accountability for patient care independent of a supervisory or collaborative relationship with a physician. This authority may be exercised in the home state and in any remote state in which the APRN exercises a multistate licensure privilege.” However, the APRN Compact also states that “[a]n APRN practicing in a party state must comply with the state practice laws of the state in which the client is located at the time service is provided.”
It is not clear how these two provisions can be reconciled. There are still several states in which practice laws require a supervisory or collaborative relationship with a physician. Will Washington APRNs be expected to comply with these requirements? Since APRNs are considered to be practicing in the state where the patient is located, does this mean that even APRNs who are physically located in Washington but providing services remotely will need to comply with a remote state’s requirements for supervision or collaboration? Would a collaborative or supervisory relationship need to be established with a physician in the remote state?
F. Adopting the Compacts could result in significant loss of state revenue
Adopting the NCSBN Compacts would threaten a significant potential loss of revenue for supporting nursing practice and regulation in Washington State. The Nursing Care Quality Assurance Commission is supported by licensing and renewal fees. The Washington Center on Nursing is supported by a surcharge on those fees. Under the Compacts, out-of-state nurses practicing in Washington (including those who commute to Washington to work) would no longer be licensed here; they would be licensed in their states of residence instead, so they would no longer pay fees for licensing and renewal here. (This loss of revenue might be partially offset by fees from Washington residents who practice in other states and would need to be licensed here). In other states, potential loss of licensing revenue has been a major factor in deciding not to adopt the prior NLC. For example, in 2002 the Virginia General Assembly’s Joint Commission on Health Care estimated a total loss of revenue to their Board of Nursing of more than $400,000 biennially if Virginia joined the NLC2. (Virginia subsequently joined, raising their licensing fees for all Virginia- licensed nurses in order to avoid this substantial revenue loss). In 2014, the Kansas Board of Nursing predicted a $376,667 loss of revenue if
45

!7!"
it joined the NLC3 (which it declined to do). A 2013 report to the California board that licenses licensed vocational nurses (equivalent to LPNs in Washington) also noted that joining the NLC would result in a “substantial loss of revenue” to that state’s nursing licensure boards4. There is no mechanism for charging fees to out- of-state licensees practicing in the state in order to recoup these losses. Indiana sought to join the NLC and enacted a provision authorizing a $25 filing fee for out-of-state privileges. Their attempt to join the NLC was rejected and Indiana subsequently repealed the legislation. Today, Indiana remains a non-Compact state. In addition to probably revenue losses, Washington would likely face set-up expenses in joining the Compacts as well as fees to the Interstate Commissions created under the compacts (fees which have yet to be determined). Faced with revenue loss and additional expenses resulting from joining the NCBSN Compacts, the only options would be to reduce services or to increase fees for Washington nurses.
IV. THE COMPACTS WOULD SIGNIFICANTLY ERODE WASHINGTON’S STATE SOVEREIGNTY
A. Interstate compacts are
powerful instruments; adopting them requires careful deliberation and balancing
In the U.S., states regulate health care practice within their borders, in keeping with the basic tenets of federalism. The NCSBN Compacts purport to build on existing state regulatory structures, but they would actually erode states’ powers by superimposing new and complicated regulatory mechanisms that create two powerful and unaccountable “Interstate Commissions,” one for the NLC and one for the APRN Compact.
Interstate compacts are very powerful instruments. They are adopted in statute by participating states, but they also function as
contracts. The provisions of a compact have the force of law. They take precedence over existing laws that may conflict with it. By adopting a compact, the state willingly gives up some of its own autonomy. Clearly, a step like this requires very careful deliberation and balancing—evaluating how much autonomy is surrendered, under what circumstances, and whether the purported benefits justify the risks to the state and its citizens. A careful examination of the NLC and APRN Compact reveals that purported benefits do not justify the risks.
B. The Compacts create unaccountable new private bureaucracies with significant power over participating states
Both the NLC and the APRN Compact create an “Interstate Commission” with broad implementation and enforcement powers, including adopting rules and assessing payments from participating states. Each state would have a representative to the NLC’s Interstate Commission and the APRN Compact’s Interstate Commission. That representative would be the head of the state licensing board or designee, who also serves as the administrator of the Compacts for each party state. (Each state would have one vote on each of the Interstate Commissions, regardless of the state’s population or number of licensees).
The Interstate Commissions’ rules and decisions are binding on all member states. The Compacts include procedures for notice-and- comment rulemaking, although they include no specific length for the comment period. The Compacts also provide for emergency rulemaking, using a notably broad approach to determining when “emergency” rules are needed: it includes not only actions to respond to an imminent threat to public health, safety or welfare, but also to prevent a loss of Commission or party state funds or to meet a deadline for the adoption of an administrative rule that is required by federal law or rule.
46
!8!"
The Interstate Commissions also have the power to adopt budgets and collect annual assessments from each party state to cover the cost of their operations, based on a formula that they will determine. The Commissions can terminate a state for defaulting in the performance of its obligations or responsibilities under the Compacts or Commission rules.
In other words, by adopting the Nurse License Compact and the APRN Compact, Washington would be bound by decisions to adopt rules and to assess payments to fund yet-to-be-determined budgets, based on a yet-to-be-determined formula.
Compounding this problem, there is no oversight or accountability for the Commission’s decisions. While each state’s representative is accountable to her or his own state, the Commissions themselves are accountable to no one. And there is no mechanism to appeal their decisions, with one narrow exception: the right to appeal a decision to terminate a state from the Compact. (And that appeal can only be filed in the U.S. District Court for the District of Columbia or the federal district in which the Commission has its principal offices).
A state can withdraw voluntarily from either Compact only by adopting a new statute to do so, at least six months before withdrawing. The state remains bound by the Compact (and responsible for paying assessments) until then.
C. Washington nurses would be subject to other states’ jurisdiction
As noted earlier, according to the NCBSN Compacts, a nurse who practices in a party state under a multistate licensure privilege will be subject to “the jurisdiction of the licensing board, the courts and the laws of the party state in which the client is located at the time service is provided.” This means that a nurse might be located in Washington and communicating via telephone, computer or other electronic communications technology with a patient in
another state and find herself or himself subject to that state’s licensing board, courts and laws.
Not only could that state revoke the nurse’s privileges to practice there; the Compacts authorize licensing boards in one party state to issue subpoenas for hearings and investigations for attendance and testimony from another party state. So a Washington nurse could be compelled to travel to another state to participate in a hearing or to respond to an investigation for alleged conduct that occurred while she was in Washington providing services remotely. While the Compact does state that the board or court in the other state would pay fees and travel expenses, this does not address the unnecessary disruption and burden involved— let alone the fact that the nurse would be subject to that state’s procedures and standards for investigation and discipline. And this would also represent a new financial burden for states.
Investigation and discipline procedures vary from state to state. While the Compacts say that the home state will apply its own state laws to determine appropriate action to take against a nurse’s license, Washington nurses could still face investigations and hearings in another state based on alleged conduct that occurred in Washington, even if those allegations would not have been sufficient for Washington to take action against the nurse’s license.
And, of course, it would be ironic (to say the least) to think that a nurse might be compelled to make a personal appearance in a distant state because of allegations arising from providing services to a patient in that state remotely via telephone or computer.
The Compact language granting jurisdiction to other states is notably broad: It is not limited to authority over the nurse’s ability to practice nursing. The plain language suggests that this would apply to civil and criminal liability as well.
47

!9!"
V. COMPARISONS TO OTHER COMPACTS FALL SHORT
A. A nursing license is not like a driver’s license
Proponents often draw an analogy between the NCSBN Compacts and driver’s licenses, based on the fact that a driver’s license issued in one state permits the license holder to drive in any other state, subject to motor vehicle laws of the state in which she or he is driving. But this comparison is very limited at best.
Driving in another state invariably means that the driver is physically present in that state. But nursing services are increasingly provided remotely, through electronic communication technologies. In fact, this is a major argument offered for adopting the NCSBN Compacts). This is a fundamental difference between nursing licenses and driver’s licenses.
A driver’s license authorizes an individual to engage in an activity—operating a motor vehicle. A nursing license authorizes an individual to practice a profession. It involves a broad range of cognitive and psychomotor skills and functions based on a specialized body of knowledge acquired through an approved academic program. Also, determining violations of motor vehicle laws is largely based on facts. Penalties are often prescribed in law. Determining violations of nurse practice acts and deciding appropriate penalties often requires evaluating a wide range of circumstances, particularly when a nurse is suspected of practicing incompetently.
B. The Interstate Medical Licensure Compact includes important differences with the NCSBN Compacts
In addition to the NCSBN Compacts, interstate compacts for other health professions have been developed or are being developed. Of these, the Interstate Medical Licensure Compact (IMLC), which addresses interstate licensure and practice of physicians, has drawn the most
attention. It has been adopted by eleven states so far.
Unlike nursing, there are virtually no differences from state to state in the scope of practice for medicine. Furthermore, the IMLC differs from the NCSBN Compacts in several significant ways:
• Rather than granting a multistate license to practice in all other party states, the IMLC still requires a physician to be licensed in each state in which she or he seeks to practice. The IMLC authorizes a physician to apply for an expedited license from that state or states. The board of medicine in that state then evaluates whether the physician is eligible for an expedited license. If granted, the physician is licensed in that state, pays fees to that state and must renew the license periodically.
• Unlike the NCSBN Compacts, which specify that a nursing license is issued in the nurse’s “home state”—i.e., the state of residence—the IMLC provides that a physician has a “state of principal license," which can be the state of residence, a state in which the physician practices at least 25% of the time, or the state of the physician’s employer. The physician may later redesignate another state as the state of principal license.
• The IMLC specifies that physicians must comply with the state’s continuing education requirements in order to renew the license. The NCSBN Compacts do not directly address whether out-of-state nurses will be required to comply with states’ continuing competence rules (such as continuing education) but, as noted earlier, it appears that they will not.
• The IMLC provides that if its Interstate Commission exercises its rulemaking authority in a manner that is beyond the scope of the purposes of the Compact,
48

!10!"
that action “shall be invalid and have no force or effect.” The NCSBN Compacts include no such limitation.
• The IMLC provides that anyone may file a petition for judicial review of any rules adopted by its Interstate Commission. The NCBSN Compacts include no provision for challenging their Interstate Commissions’ rules.
• The IMLC states explicitly that decisions of the actions of its Interstate Commission shall not override existing state authority to regulate the practice of medicine. The NCSBN Compacts contain no similar provision regarding regulation of nursing practice.
VI. THE ALTERNATIVE: FOCUS ON TELEHEALTH Telehealth—delivering services through electronic communication technology—offers great potential for increasing access to care, enhancing patient engagement and experiences of care and reducing costs. Nurses have provided advice, counseling and triage via telephone for many decades; this was never seen as posing regulatory complications. It is the development and proliferation of computer technologies and handheld devices have transformed telehealth practice and raised questions about how best to regulate the interstate use of these technologies.
The NCSBN Compacts represent a flawed attempt to address these regulatory challenges. WSNA agrees that they must be addressed. But doing so does not require adopting a comprehensive change in regulating nursing practice—especially not the broad, complex, cumbersome and inflexible mechanisms proposed by the NCSBN Compacts. Instead, efforts should focus on the discreet issues posed by interstate telehealth practice.
VII. CONCLUSION: ADOPTING THE NCSBN COMPACTS IS A BAD OPTION FOR WASHINGTON Unfortunately, Washington lawmakers who have concerns about any provisions in the NCSBN Compacts have no opportunity to do anything about them at this point: In order to join the NLC and/or the APRN Compact, Washington would have to adopt them as they are, without any substantive changes. The Compacts could be amended later, but that would require every Compact state to enact a new statute to do so.
Thus, the only two options available to Washington are:
• To adopt each Compact as is, despite multiple concerns; or
• To reject the Compacts.
WSNA and the American Nurses Association (ANA) remain committed to finding common ground with NCBSN and others on effective regulatory measures, particularly with regard to interstate telehealth practice, that are workable and realistic, that offer real solutions, and that respect state sovereignty. None of this, unfortunately, describes the NCSBN Compacts. The Compacts are a bad option for Washington. Washington lawmakers should reject them. We can and must work toward better, more effective approaches.
REFERENCES #"NLCA (2011), Response to ANA Updated NLC Talking Points. Retrieved from https://www.ncsbn.org/4_ANA_TP_Revised_031112.pdf $"Joint Commission on Health Care (2002). Multi-State Nurse Licensure Compact Study. Retrieved from http://leg2.state.va.us/dls/h&sdocs.nsf/fc86c2b17a1cf388 852570f9006f1299/c5934246b8c2a81585256b650059b2 54/$FILE/RD15_2002.pdf %"Kansas State Board of Nursing (2014). “Why Kansas Does Not Belong to the Nurse Licensure Compact.” Nursing Newsletter, 27(4): 1-2. Retrieved from http://www.ksbn.org/nursingnewsletter/2014/4qtr2014.pdf 4 Bello-Jones, T. (2013). “Multi - State Licensure Compact for California Nurses.” Retrieved from http://www.bvnpt.ca.gov/pdf/bm11_13/8.pdf
49

7/28/16 9:58 AMOccupational Licensing Doesn’t Seem to Restrict Nurses’ Mobility - Real Time Economics - WSJ
Page 1 of 4http://blogs.wsj.com/economics/2016/07/22/occupational-licensing-doesnt-seem-to-restrict-nurses-mobility/
For nurses, teachers, barbers, and others licensed professions,a license can be both a blessing and a curse. Licensing has been shownto raise some workers’ pay by restricting new entrants, but it can alsolimit mobility, since some licenses don’t transfer automatically fromone state to another.
For economists studying the phenomenon, though, the (bipartisan)consensus of late is that licensing is a major labor-market buzzkill.Standard economic theory and a growing body of research says ithinders mobility, compared with unlicensed professions. That hasoutsize effects on groups such as military spouses, who movefrequently and somewhat involuntarily.
That’s why the White House and the Heritage Foundation are
This copy is for your personal, non-commercial use only. To order presentation-ready copies for distribution to your colleagues, clients or customers visithttp://www.djreprints.com.
http://blogs.wsj.com/economics/2016/07/22/occupational-licensing-doesnt-seem-to-restrict-nurses-mobility/
REAL TIME ECONOMICS EMPLOYMENT
Occupational Licensing Doesn’t Seemto Restrict Nurses’ MobilityA multi-state agreement allowing nurses to practice across borders didn't affect migrationrates, economists found
|
When states joined a multi-state licensure agreement to allow nurses to work across borders,there was no significant impact on nurses' mobility and other labor market outcomes, a new studyfinds. PHOTO: JOHN MOORE/GETTY IMAGES
Jul 22, 2016 6:30 am ET
By
ANNA LOUIE SUSSMAN
50
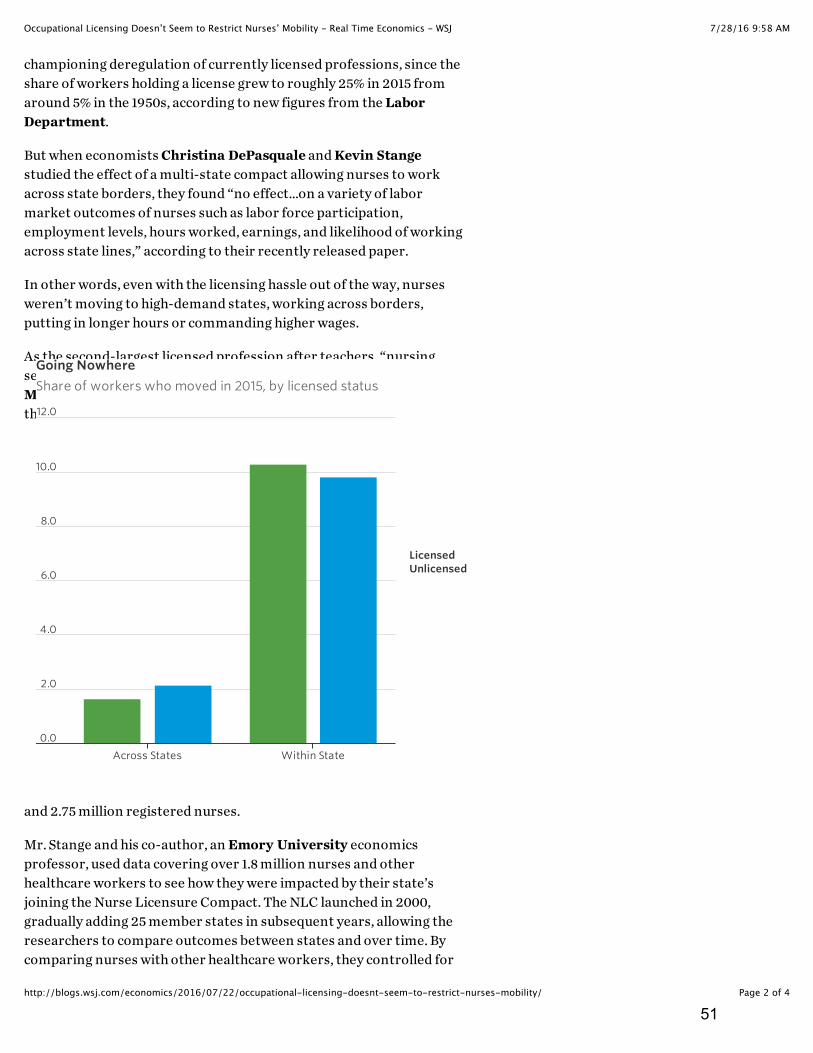
7/28/16 9:58 AMOccupational Licensing Doesn’t Seem to Restrict Nurses’ Mobility - Real Time Economics - WSJ
Page 2 of 4http://blogs.wsj.com/economics/2016/07/22/occupational-licensing-doesnt-seem-to-restrict-nurses-mobility/
championing deregulation of currently licensed professions, since theshare of workers holding a license grew to roughly 25% in 2015 fromaround 5% in the 1950s, according to new figures from the LaborDepartment.
But when economists Christina DePasquale and Kevin Stangestudied the effect of a multi-state compact allowing nurses to workacross state borders, they found “no effect…on a variety of labormarket outcomes of nurses such as labor force participation,employment levels, hours worked, earnings, and likelihood of workingacross state lines,” according to their recently released paper.
In other words, even with the licensing hassle out of the way, nursesweren’t moving to high-demand states, working across borders,putting in longer hours or commanding higher wages.
As the second-largest licensed profession after teachers, “nursingseemed like a good one to look at,” said Mr. Stange, a University ofMichigan public policy professor. The Labor Department estimatesthere are currently 700,000 licensed practical and vocational nurses
and 2.75 million registered nurses.
Mr. Stange and his co-author, an Emory University economicsprofessor, used data covering over 1.8 million nurses and otherhealthcare workers to see how they were impacted by their state’sjoining the Nurse Licensure Compact. The NLC launched in 2000,gradually adding 25 member states in subsequent years, allowing theresearchers to compare outcomes between states and over time. Bycomparing nurses with other healthcare workers, they controlled for
Going Nowhere
Share of workers who moved in 2015, by licensed status
LicensedUnlicensed
Across States Within State
0.0
2.0
4.0
6.0
8.0
10.0
12.0
51

7/28/16 9:58 AMOccupational Licensing Doesn’t Seem to Restrict Nurses’ Mobility - Real Time Economics - WSJ
Page 3 of 4http://blogs.wsj.com/economics/2016/07/22/occupational-licensing-doesnt-seem-to-restrict-nurses-mobility/
other dynamics in a given state’s healthcare system or job market.
“We just don’t find a very big effect of eliminating these cross-statebarriers on those kinds of outcomes,” said Mr. Stange.
So what is happening? Like any good economist, Mr. Stange wascareful to say he couldn’t tell for sure. But he cited a familial or socialconnection to a place; a general decline in labor market fluidity, or thepossibility that applying for another state’s license is not actually thatonerous.
“It’s a pain, but it’s not inconvenient enough to move the needle onpeoples’ working behavior,” said Mr. Stange.
Morris Kleiner, a University of Minnesota economist who hasstudied licensing extensively, offered a complementary explanation:Nurses’ interstate migration is less affected by licensing than otherlicensed professionals. In forthcoming research, he and University ofMinnesota co-author Janna Johnson found nurses are more mobilethan lawyers, teachers, hairdressers and dentists. He also pointed outthat nurses, who are largely women, could be secondary earners intheir households, and therefore more likely to move in accordancewith their husbands’ careers.
“It’s often a household decision, and a lot of these barriers to mobilityare not that great,” he said.
RELATED
In Obama’s Budget, an Effort to Rein in Occupational Licensing (Feb.29)
In State Job Licensing, Uneven Regulation of Workers–and theEconomy (Feb. 8)
White House Warns States On Job-Licensing Requirements (July 30,2015)
New York’s Licensing Barricade Against Military Spouses (Feb. 13,2015)
Where Just a Misdemeanor Could Keep You Out of a Job (April 26)
Share this:
ACADEMICS (HTTP://BLOGS.WSJ.COM/ECONOMICS/TAG/ACADEMICS/)
52

7/28/16 9:58 AMOccupational Licensing Doesn’t Seem to Restrict Nurses’ Mobility - Real Time Economics - WSJ
Page 4 of 4http://blogs.wsj.com/economics/2016/07/22/occupational-licensing-doesnt-seem-to-restrict-nurses-mobility/
EMPLOYMENT
(HTTP://BLOGS.WSJ.COM/ECONOMICS/TAG/EMPLOYMENT-2/)
JOBS (HTTP://BLOGS.WSJ.COM/ECONOMICS/TAG/JOBS/)
LABOR MARKET REGULATION
(HTTP://BLOGS.WSJ.COM/ECONOMICS/TAG/LABOR-MARKET-
REGULATION/)
LICENSING (HTTP://BLOGS.WSJ.COM/ECONOMICS/TAG/LICENSING/)
MOBILITY (HTTP://BLOGS.WSJ.COM/ECONOMICS/TAG/MOBILITY/)
NURSING (HTTP://BLOGS.WSJ.COM/ECONOMICS/TAG/NURSING/)
OCCUPATIONAL LICENSING
(HTTP://BLOGS.WSJ.COM/ECONOMICS/TAG/OCCUPATIONAL-
LICENSING/)
REGULATION
(HTTP://BLOGS.WSJ.COM/ECONOMICS/TAG/REGULATION/)
REGULATIONS
(HTTP://BLOGS.WSJ.COM/ECONOMICS/TAG/REGULATIONS/)
Copyright 2014 Dow Jones & Company, Inc. All Rights Reserved
This copy is for your personal, non-commercial use only. Distribution and use of this material are governed by our Subscriber Agreement and by copyright law. Fornon-personal use or to order multiple copies, please contact Dow Jones Reprints at 1-800-843-0008 or visit www.djreprints.com.
53

Attachment J
MEMORANDUM To: Board Members Ohio Board Of Nursing From: Betsy Houchen Executive Director
Subject: New/Enhanced Compact – Areas For Consideration Date: March 24, 2016 The Board reviewed and discussed the following areas of concern at the 2015 and 2016 Board Retreat. The areas of concern are provided again for review and consideration. Authority of the Interstate Commission Article VII establishes “a joint public entity known as the Interstate Commission of Nurse Licensure Compact Administrators” (Commission) composed of the party states that adopt the new Compact. Article VII also grants powers to the Commission. • Paragraph (b)(1): “Each party state shall have and be limited to one administrator…” • Paragraph (b)(2): “Each administrator shall be entitled to one (1) vote with regard to the
promulgation of rules and creation of bylaws and shall otherwise have an opportunity to participate in the business and affairs of the Commission….”
⇒ Consideration: Each member, regardless of the number of licenses regulated, or the amount of fees paid to the Commission, is represented by one person and has one vote.
• Paragraph (g) and (g)(1) “The Commission shall have the following powers: To promulgate
uniform rules to facilitate and coordinate implementation and administration of this Compact. The rules shall have the force and effect of law and shall be binding in all party states.”
⇒ Consideration: The Commission will have the power to enact rules that are binding
on each State in the Compact by a simple majority vote. Each State would be subject to administrative rules not passed at the State level.
• Paragraph (a)(2): The Commission will be subject to the laws of the state in which it is
organized, i.e., Illinois.
⇒ Consideration: If there is a dispute between Ohio and the Commission or another party state, the matter will be handled in the Illinois court system.
• Paragraphs (b)(5) and (i): “The Commission may convene in a closed, non-public meeting”
for certain reasons; the Commission has immunity/defenses to lawsuits.
54

⇒ Consideration: the Commission is not subject to any independent auditor or legal
authority with oversight over its operations or finances, and has immunity/indemnification from lawsuits.
• Paragraph (g)(6): The Commission shall have the following powers: “To hire employees… fix
compensation, define duties…”
• Paragraph (c): “The Commission shall, by a majority vote of the administrators, prescribe bylaws or rules to govern its conduct as may be necessary or appropriate to carry out the purposes and exercise the powers of the Compact, including but not limited to: …providing reasonable standards and procedures: for the establishment and meetings of other committees; and governing any general or specific delegation of any authority or function of the Commission.”
⇒ Consideration: The Commission is to be fully staffed and all of its costs will be paid
for by annual assessments on members; the Commission would have exclusive say in how much each member is assessed. At this time, the cost for each party state to support the Commission is unknown.
Many of these provisions may violate the Ohio Constitution, the Ohio Open Meetings Act, the Ohio Ethics Law and other Ohio statutes. The budget impact is uncertain but due to required assessments, it is anticipated that it will not be budget neutral. (See discussion below under Fiscal Implications.) Grandfathering Article III, paragraph (g) specifies that nurses who currently hold a multi-state license would retain their multi-state license. The exceptions would be (1) nurses who change their primary state of residence, must meet the requirements of the new Compact; or (2) a nurse who “fails to meet the multi-state licensure requirements due to a criminal conviction, enrollment in an alternative program, an adverse action or any other event occurring after the Compact’s effective date, shall be ineligible to retain or renew a multi-state license and the nurse’s multi-state license shall be revoked or deactivated in accordance with applicable Commission rules.”
⇒ Consideration: Nurses who currently have multi-state license under the old Compact would be grandfathered into the new Compact. Therefore, nurses who never had criminal records checks could hold a multi-state license under the new Compact.
Misdemeanors Article III, paragraph (c)(7) states that for an applicant to obtain or retain a multi-state license in the home state, the individual “has not been convicted or has entered into an agreed disposition, of a misdemeanor offense related to the practice of nursing as determined on a case-by-case basis….”
⇒ Consideration: Each State will make its own case-by-case determination about whether to impose discipline for misdemeanors. If the state takes action on a misdemeanor, other party states could take action based on the other State’s action, but if the State where the misdemeanor occurred declines to take action, the Board would not be aware of the misdemeanor.
Alternative Program for Chemical Dependency (AP) Article III, paragraphs (c)(9) and (10) state that a nurse enrolled in AP cannot obtain or retain a multi-state license and that the nurse is “subject to self-disclosure requirements regarding current participation in an alternative program.”
55

Article V, paragraph (c) states that a party state has authority to place a nurse in an alternative program “in lieu of adverse action.” The paragraph further states that the home state shall deactivate the multi-state license privilege under the multi-state license for the duration of the nurse’s participation in an alternative program.
⇒ Consideration: Article V allows each State to place a nurse in AP, however, not all Boards know when nurses are participating in their State’s Alternative Program because, for example, the program is outsourced to a third party. If States do not know their AP participants, those licensees would be able retain multi-state licenses if the licensee did not report their participation to the State.
Uniform Licensure Requirements and Absolute Bars The Uniform Licensure Requirements (ULRs) adopted by NCSBN in 2012, are to be included in the new Compact rules rather than in statute. A copy of the ULRs is attached (Attachment F). The new Compact language and the ULRs do not include absolute bars for licensure, except that the ULRs specify if an “evaluation identifies sexual behaviors of a predatory nature the board of nursing should deny licensure.”
⇒ Consideration: The Ohio Nurse Practice Act includes absolute bars for licensure. The following list of crimes that make an individual ineligible for licensure in Ohio, or if already licensed, require an automatic suspension of licensure: aggravated murder, murder, voluntary manslaughter, felonious assault, kidnapping, rape, sexual battery, gross sexual imposition, aggravated arson, aggravated robbery, and aggravated burglary, as defined under Title XXIX [29] of the Ohio Revised Code, or, with regard to offenses committed in other jurisdictions, offenses comparable to the offenses defined in Title XXIX [29] of the Revised Code.
Conviction Language Article III, paragraphs (c)(7) and (8) state that for an applicant to obtain or retain a multi-state license in the home state, the individual “has not been convicted or found guilty, or has entered into an agreed disposition, of a felony offense…and has not been convicted or found guilty, or has entered into an agreed disposition, of a misdemeanor offense related to the practice of nursing….” For felonies and misdemeanors, the Ohio Nurse Practice Act specifies the Board can take action based on a “conviction of, a plea of guilty to, a judicial finding of guilt of, a judicial finding of guilt resulting from a plea of no contest to, or a judicial finding of eligibility for a pretrial diversion or similar program or for intervention in lieu of conviction for, …”
Consideration: The new Compact language, “not been convicted or found guilty, or has entered into an agreed disposition” is too narrow. Under Ohio law, the Board can also take action on judicial findings of eligibility for a pretrial diversion or similar program, or intervention in lieu of conviction. Without these options, the Board would need to base action on the underlying facts which would greatly lengthen the investigative and hearing processes.
Social Security Number Article III, Paragraph (c)(11) specifies that an applicant for a multi-state license would be required to have a social security number. This is not consistent with Ohio law or federal law. Conversion of Licenses When Licensee Changes State of Residency Article IV, paragraph (c) states that “If a nurse changes primary state of residence, by moving between two party states, the nurse must apply for licensure in the new home state and the multi-state license issued by the prior home state will be deactivated in accordance with applicable rules adopted by the Commission.” (Emphasis added.)
56

Article IV, paragraph (d) states that “If a nurse changes primary state of residence by moving from a party state to a non-party state, the multi-state license issued by the prior home state will convert to a single state license, valid only in the former home state.” (Emphasis added.)
⇒ Consideration: Ohio could not “convert” or “deactivate” a license without affording the licensee due process.
Mandatory Reporting Mandatory reporting is not a requirement in the new Compact. The TERCAP data has shown the importance of mandatory reporting to assure boards of nursing are receiving complaints and preventing unsafe practitioners from moving from employer to employer without the board of nursing knowing about the unsafe practice.
⇒ Consideration: Ohio is a mandatory reporting state. Response to Disaster Situations At the 2015 Midyear Meeting, the Compact was cited as being necessary to assure an adequate nursing workforce during disaster situations. However, single state licensure can also effectively address disaster situations. When this question has been presented to the Board, we have responded as follows:
Non-membership in the NLC does not impede the deployment of licensed nurses from other states to Ohio during a disaster, or the deployment of Ohio licensed nurses to declared disaster areas in other states. The Nurse Practice Act, Section 4723.32(G)(7), ORC, allows nurses who hold an active, valid license in another state to come to Ohio in the case of any declared disaster. Further, under Section 4723.32, ORC, providing emergency assistance does not require a nursing license in Ohio. During the aftermath of Hurricane Katrina, the Board encouraged and facilitated Ohio nurses to provide disaster relief by enrolling in the Medical Reserve Corp (MRC)/Red Cross (ARC), Through enrollment, state license status was verified; the deployment of nurses was organized so nurses were matched to the area of need, based on the nurse’s education and experience; and emergency relief training was provided as needed. Also, nurses with active, valid licenses in one state were considered federal employees and did not need a license to practice in the state where they are going. In addition, the ARC has negotiated reciprocal licensing agreements with each state, so if nurses with active, valid licenses in one state are activated through ARC, they are able to practice in other states without having a license to practice in that state.
Sharing of Investigative Information At the 2015 Midyear meeting, it was emphasized that an advantage of the Compact is that states can share investigative information with each other, which they could not do previously as single states.
⇒ Consideration: As a single state licensure board, Ohio is authorized to share investigative information with other boards of nursing under the Ohio Nurse Practice Act.
Effect of Disciplinary Actions in Other Compact States At the 2015 Midyear meeting, it was explained that if the home state takes a disciplinary action against a nurse, that action prevents the nurse from practicing in the remote states and the nurse is issued a single state license. However, if a remote state takes disciplinary action, the discipline is only effective in the remote state that took the action, so the nurse could continue to hold a multi-state license and practice in other Compact states. It was suggested that remote states
57

would check Nursys to determine if other remote states have taken disciplinary actions and then could bootstrap the action taken in the other remote state.
⇒ Consideration: If the remote state does not know the nurse is practicing in their state, it is not clear how the remote state would know to check the individual nurse’s license/discipline in Nursys? Perhaps it could be explored so when a nurse is disciplined in a home state or in a remote state, the multi-state license is revoked and the nurse could only be issued a single state license.
Fiscal implications Currently there is a $6,000 annual fee for Compact membership. The fiscal impact will vary from state to state. Ohio would need to conduct a fiscal analysis to determine the impact on loss of licensure fee revenues.
58
Re-Issued April 2016
MULTI-STATE NURSE LICENSURE
In 2005, the Ohio Board of Nursing (Board) examined issues and learned about the experience of some Compact states participating in multi-state licensure. Although the Board recognized that multi-state nurse licensure could be advantageous for occupational health nurses, traveling nurses, or employers, the Board discussed that potential risks of harm to the public outweigh the potential benefits. With multi-state licensure, nurses could be practicing in Ohio when they have not been held to the same standards of safe practice that Ohio has deemed important for public safety. For example, Ohio requires criminal records checks for licensure, but not all Compact states have the same requirement. Also, Ohio statute specifies that there are absolute bars to licensure. If an applicant has been convicted of certain crimes such as Murder and Rape, among others, the applicant cannot be considered for licensure in Ohio. The majority of Compact states either do not bar violent felonies, or impose only time-limited, rather than absolute, bars to licensure. Over the years, the Board reviewed the actual experience of other states and identified the potential impact of multi-state licensure on public safety. We were advised of nurses with multi-state licenses relocating to states as soon as they find themselves under investigation in their home state. While in theory, the home state would immediately report the investigation to the next state, the reality is neither state may learn of the relocation for a significant period of time. Furthermore, not all states have laws like that in Ohio permitting sharing of investigative information with other governmental entities. In addition, when the nurse moves to another state, the home state does not always continue its investigation. This means that Ohio would not receive vital information unless Ohio attempted to conduct an out-of-state investigation and this is not realistic. In fact, it is unclear whether Ohio would have the ability to compel the production of out-of-state documents or witnesses necessary to prepare a case. These are just some examples of issues that nursing boards across the country are attempting to address. On September 16, 2005, the Board voted to delay action seeking the introduction of interstate compact legislation until such time more information is gathered to assure that the benefits of multi-state licensure outweigh any risks related to public safety. Since 2005, the Board has discussed multi-state licensure at numerous meetings and continuously has worked at the national level to address Ohio’s concerns. While the Compact states are being encouraged to implement criminal records checks for licensure, several Compact states have not been successful in enacting the requirement. At this time, the Board continues to believe the potential risks of harm to the public outweigh the potential benefits because nurses with multi-state licenses could practice in Ohio without meeting the current statutory and regulatory standards established by the General Assembly and the Board to protect the public. The Board continues to address these issues at the national level through the National Council of State Boards of Nursing.
59

Re-Issued April 2016
In May 2015, NCSBN voted to approve a new Compact (New NLC). During the NCSBN Annual Meeting in August 2015, an information session for state attorneys, regarding the legal implications of the New NLC, was provided by the Compact Special Counsel and NCSBN Legal Counsel. The New NLC would need to be adopted by each of the 26 Compact member state legislatures. Potential obstacles to adoption identified by state attorneys participating in the information session included (but are not limited to) the following: (i) the New NLC would establish a Commission that would be funded by state revenue, but would not be subject to state transparency requirements (open meetings/open records acts); (ii) the Commission could adopt rules binding on Compact member states without undergoing state rule-making processes; (iii) concern was expressed that states would be ceding their legal authority to a privately operated Commission. The New NLC will not be effective until all but two of the Compact member state legislatures adopt the New NLC.
60