Standardization of Care of Gynaecological Cancers: Use of Practice Manual and Guidelines at the...
33
Standardization of Care of Gynaecological Cancers: Use of Practice Manual and Guidelines at the University College Hospital, Ibadan, Nigeria by Akin-Tunde A. Odukogbe*, Olutosin Awolude*, Timothy O. Oluwasola*, Olaitan Soyannwo+, Clement Okolo++, Yinka Ademola+++, Atara Ntekim**, Omolara Fagbenle**, Olusola Akinpelu*, Isaac F. Adewole*, Akinyinka O. Omigbodun* *Gynaecology Oncology Unit, Department of Obstetrics and Gynaecology, +Palliative Care Unit, ++Department of Pathology, +++Department of Surgery, **Department of Radiotherapy, College of Medicine, University of Ibadan / University College Hospital, Ibadan.
-
Upload
merryl-richard -
Category
Documents
-
view
259 -
download
8
Transcript of Standardization of Care of Gynaecological Cancers: Use of Practice Manual and Guidelines at the...

Standardization of Care of Gynaecological Cancers: Use of Practice Manual and Guidelines at the University College Hospital, Ibadan, Nigeria
by
Akin-Tunde A. Odukogbe*, Olutosin Awolude*, Timothy O. Oluwasola*, Olaitan Soyannwo+, Clement Okolo++, Yinka Ademola+++, Atara Ntekim**, Omolara Fagbenle**, Olusola Akinpelu*, Isaac F. Adewole*, Akinyinka O. Omigbodun*
*Gynaecology Oncology Unit, Department of Obstetrics and Gynaecology, +Palliative Care Unit, ++Department of Pathology, +++Department of Surgery, **Department of Radiotherapy, College of
Medicine, University of Ibadan / University College Hospital, Ibadan.

Abstract• BACKGROUND:Diminishing resources, evolving disease patterns and increasing patients’ awareness and desires demand cost – cutting, cross – coupling yet cost – effective approach to health care delivery systems. Cancer care represents the ultimate model requiring such an approach.• OBJECTIVE:We present a pioneer guidelines and standard of care manual for managing gynaecological cancers in low resource settings.• FEATURES:Introduction: Cancers are forming increasing proportions of diseases even in developing countries. By 2020, new cases per year will increase to 15 million, while mortality will be 12 million. In 2008, about 72% of cancer deaths occurred in low and middle income countries, where health care systems are dysfunctional.A multilevel approach to managing gynaecological cancers is outlined, with the primary, secondary and tertiary levels having well delineated but intertwined tasks assigned.Tertiary level care: A multidisciplinary method of care and control is presented. Use of data capturing forms: These forms, labelled GO1, GO2, GO3 and GO4 are presented. These have been formulated for a thorough initial assessment of patients and their diseases; detailed collection of operative findings and adequate monitoring of adjuvant therapy and follow up.CONCLUSION: Prevention, management and control of cancers, including gynaecological ones require innovative approaches especially in resource – challenged settings like Nigeria.

Introduction• Cancers are forming increasing proportions of
diseases in resource constrained countries. • By 2020, it is predicted that new cases will
increase to more than 15 million, while deaths from cancers will increase to 12 million people.(http://www.who.int/mediacentre/news/releases/2003/pr27/en/)
• Presently about 80% of cancers are in stages 3 and 4 at initial diagnosis (Odukogbe et al 2004, Obrien
2013).
Introduction
• Cancer prevention, care and control are very demanding in terms of manpower and materials (Obrien 2013, Adesina 2013, Morhason-Bello 2013).
• Populations in Africa have lowest human development indices (HDI).
• Cancer data collection systems in Africa are generally weak (Graham 2012).
• Innovative approaches by health care personnel required (Braithwaite 2012, Jedy – Agba 2012).

Africa lags behind other continents as regards personnel resources for managing diseases.
(World Health Report 2006)
WHO region Total health workforce
Number Density (per 1000 population)
Africa 1,640,000 2.3
Eastern Mediterranean 2,100,000 4.0
South – East Asia 7,040,000 4.3
Western Pacific 10,070,000 5.8
Europe 16,630,000 18.9
America 21,740,000 24.8
World 59,220,000 9.3

Introduction
• Multidisciplinary approach to cancer care– Gynaecological oncologist– Surgical oncologist / urologist– Radiation oncologist– Nurse oncologist – Psychology oncologists – Gynaecologic histopathologists – Anaesthetists / radiologists/ oncology pharmacists, – Palliative care specialists – Public health specialists / family physicians – Medical social workers– And several others WORKING CLOSELY TOGETHER.

Introduction
• Appropriately designed care interactively involves – Primary – Secondary, and – Tertiary levels of health care delivery, ATTAINABLE IN
OUR COUNTRY, NIGERIA, PRESENTLY.
Rationale
• Cancer control encompasses a package of diverse interventions aiming at reducing morbidity and mortality.
• Many patients receive affordable or available treatment rather than optimal treatment and those without financial capabilities are denied access to care, never reaching a centre capable of providing appropriate treatment.
Pre-Workshop Preparation Meetings
The team that laid the foundation of the first draft of this manual – Prof. A. O. Omigbodun, Drs. A. A. Odukogbe, O. A. Awolude, O. M. Akinpelu, O. O. Lawal, O. O. Kuku, B. O. Akinwunmi, E. H. Aikhuele, O. V. Omokhodion, R. M. E. Takpe, K. O. Ekunola and M. O. Adeniran.

The Stakeholders Meeting
• On Tuesday, the 24th of September 2013, a workshop was held in Ibadan, Nigeria involving representatives of all stake holders concerned with cancer care. It led to the formulation of this manual.
• The two corporate bodies that financed the workshop were:– ROCHE (Nigeria) Ltd.– MTN (Nigeria) Ltd.
• The printing of this manual was facilitated by Professor I. F. Adewole, the Vice-Chancellor of the University of Ibadan, Ibadan.

Participants At The Workshop• Prof. I. F. Adewole – Opening address Deputy Provost – Prof. Ogunsehinde • Prof. A. O. Omigbodun (Unavoidably absent) Paediatric Oncologist - Dr. B. Brown• Paediatric oncologist - Dr. B. Brown Public Health Nurse Specialist – Mrs. Opemipo Maxwell• Dr. O. A. Awolude Departmental staff – Mr. Kabiru Adebiyi• Dr. T. A. O. Oluwasola Dr. O. O. Kuku• Dr. O. M. Akinpelu Dr. O. O. Lawal• Dr. B. O. Akinwunmi Dr. Kemi Omokhodion• Dr. Benjamin Oranye CMD Prof. Tope Alonge (Absent)• Dr. E. H. Aikhuele Provost, Prof. Segun Akinyinka (Rep Deputy Provost)• Dr. A. O. Ayeni Mrs. Olateru – Olagbegi Kemi – DD Blood bank• Dr. U. J. Oshemi Social Works Department – Mrs. Lola Umar• Dr. R. M. E. Takpe Family Physician – Dr. Sola Mosuro• Prof. O. A. Arowojolu. HOD, O & G Oncology Psychologist – Dr. Chioma Asuzu (Speaker 9)• The Chief Resident, O & G (Dr. Akin Fadipe) Psychologist – Mr. Olugbemi Olukolade• Speaker 1 (O & G) – Dr. A. A. Odukogbe Breast surgeon – Dr. T. O. Ogundiran (Absent)• Speaker 2 (Pathology) – Dr. C. A. Okolo Haematologist – Dr. J. O. Olaniyi• Speaker 3 (Surgery) – Dr. F. Ademola Radiologist – Dr. A. Adeyinka (Absent)• Speaker 4 (Radiation Oncologist) – Dr. Atara Ntekim Prof. E. O. Olapade – Olaopa (Absent with apology)• Speaker 5 (Palliative Care Spec) – Prof. Olaitan Soyannwo Dr. Folashire• Speaker 6 (Nurse Oncologist) – Mrs. Omolara Fagbenle MTN Crew led by Mrs. Toke Gbenro – Adegbite (Speaker 7)• Matron, SW4 – Mrs. Iyabo Hussein. Other matrons and ward sisters • Matron, Gynaecologic Clinic – Mrs. A. A. Rojaiye ROCHE crew led by Dr. Funke Adeleye (Speaker 8)• Matron, O & G Theatre – Mrs. C. O. Atolagbe (Rep. Matron Akinola)• Matron, Laparoscopy room – Mrs. Adeola Arowolo Dr. Bukonla Olaniyan• Matron, Colposcopy room – Mrs. O. Payne• Mrs. Patricia Oniawa – DDN, Clinicals. (Rep. Mrs. Orekha)• DD Pharmacy – Mr. I. Irabor (Rep Mrs. Oduntan)• CMAC, Prof. Jesse Otegbayo (Absent)• Anaesthetist – Dr. Monisola Sonaike

Section and contributors
Section 1 – Introduction: Dr. A. A. Odukogbe, Dr. O. A. Awolude, Dr. T. A. O. Oluwasola, Dr. O. O. Lawal, Prof. A. O. OmigbodunSection 2 – Initial Assessment at the Tertiary Institution: Dr. A. A. Odukogbe, Dr. C. Okolo, Dr. O. O. Kuku, Dr. O. M. Akinpelu, Dr. O. A. AwoludeSection 3 – Operative Procedures: Dr. F. Ademola, Dr. O. M. Akinpelu, Dr. O. A. AwoludeSection 4 – Post-operative Care of Gynaecological Cancer Patients – Chemotherapy: Dr. A. A. Odukogbe, Dr. O. A. Awolude, Dr. O. M. Akinpelu, Dr. O. B. Akinwunmi, Prof. I. F. AdewoleSection 5 – Pre-and / or Postoperative Radiation Therapy: Dr. A. Ntekim, Dr. A. FolasireSection 6 – Palliative and Nursing Care: Prof. O. Soyannwo, Mrs. O. Fagbenle, Dr. B. OranyeSection 7 – Follow-up: Dr. T. A. O. Oluwasola, Dr. Happiness AikhueleAppendices 1 -7

Why This Manual?
• To bridge identified gaps in multidisciplinary and multicare level approach to cancer management.
• To reduce the burden of gynaecological cancers, through improved communication between specialists / carers.
• To formulate standardized guidelines, suitable for our environment, in the diagnosis, treatment and follow up of gynaecological cancers.

Primary and Secondary Health Care Levels
• Important in the prevention, early management and follow up care through: family health information, education and
counselling on susceptibility to, causes and courses of female reproductive tract cancers and related diseases .
vaccination against human papillomavirus infection.ensuring (i) uptake and (ii) continued use of cervical
and other cancers’ screening tests while delivering patient – friendly services.

Primary and Secondary Health Care Levels
Early suspicion / detection of cancers. Minimal diagnostic evaluations.THERE SHOULD BE EARLY REFERRAL OF SUSPECTED
CASES TO THE GYNAECOLOGICAL ONCOLOGY UNITS AT DESIGNATED TERTIARY CENTRES.
Provision of primary and secondary levels of palliative care at these community levels.
Provision of the necessary lifelong follow up and support of cancer patients, in conjunction with the tertiary centre.
Need For Tertiary Care
• Availability of advanced diagnostic and management machinery.
• CT Scan, MRI, PET Scan, Immunochemistry etc
• Availability of specialized and ultraspecialized professionals in cancer management.
• Availability of advanced research capabilities.• Training of all cadres of practitioners.• Availability of other supportive care.• Best outcome for patient care.

Initial Assessment At The Tertiary Institution
• Use of clinical proforma (Form GO 1) for data capturing.• Investigative work up.

IDENTIFICATIONName, Address of patient / next of kin:
Hospital number:Telephone number:
Date of birth: Age last birthday (yrs): Marital status: Occupation:Educational qualification: Religion: Tribe: Husband’s occupation:Husband’s educational qualification: Next of kin (if different from husband): Relationship:
Addresses (including that of next of kin, if applicable): Phone number / s:Source of referral: Level of care:
GYNAECOLOGICAL HISTORYMenarche: Flow (days): Cycle length (days): Regularity:
Dysmenorrhoea (type and drugs used, if positive): Menorrhagia:Parity:Deliveries
1 2 3 4 5 6Year of delivery Gestational age at delivery (weeks)
Mode of delivery* Sex/es of baby Length of breastfeeding (months)
*Vaginal (VD), Caeserean section (CS), Forceps (FP), Vacuum extraction (VE), Abortions
1 2 3 4 5 6Year Pregnancy confirmed* Gestational age at termination Type** Termination type+ ( + number of times) Histological confirmation *Urine pregnancy test (UPT), Ultrasound (USS). **Spontaneous (SP), Voluntary termination (VT)

Contraception: 1 2 3 4Type Year started Duration of use Last normal menstrual period: Past menstrual period 1: Past menstrual period 2:
PRESENTING COMPLAINTS AND DURATION1 2 3 4
SYSTEMIC REVIEW1. Cardiovascular 2. Haematological 3. Respiratory 4. Gastrointestinal 5. Genitourinary 6. Central nervous system 7. Dermatological 8. Musculoskeletal 9. Ophthalmological 10. Otorhinolaryngological
FAMILY HISTORYDisease Type of relation Disease Type of relation Disease Type of relation1.Hypertension 2. Diabetes
mellitus 3. Genital cancer
(type)
4. Breast cancer 5. Other cancers OthersMEDICAL AND SURGICAL HISTORY
1 2 3 4
DRUG HISTORY AND ALLERGIESDrugs used presently:Allergies:
SEXUAL HISTORYCoitarche: Age at first delivery: Number of sexual partners:Sexually transmitted diseases:Year: Type: Lesion: Treatment: Contact tracing:
SOCIAL HISTORY

Smoking (state number and frequency)
Alcohol (state type, amount and frequency)
Controlled drugs (state type, amount and frequency)
EXAMINATIONGENERAL CONDITION:Height (m):
Weight (kg): BMI (kg/m2) Body surface area(m2)
Thyroid:
Breasts (discharge, mass. State side):
Peripheral lymphadenopathy (State location and the characteristics): Pedal and other oedema: RESPIRATORY SYSTEM:Excursions per min: Right lung field: Left lung field:CARDIOVASCULAR SYSTEM:Pulse rate:
Blood pressure: Heart sounds:
ABDOMEN:Inspection:Liver:
Spleen:
Right kidney:
Left kidney:
Uterus:
Ascites, tenderness and other masses;
PELVIC EXAMINATION:Vulva:
Vagina:
Cervix (including excitation tenderness):
Uterus:
Right adnexa (including tenderness): Left adnexa (including tenderness):
Pelvic side wall:
Pouch of Douglas:
Discharge:
Bleeding:

Operative Procedures
• Optimal cytoreduction is the goal, where feasible– If cytoreductive surgery is performed by physicians with
training in gynaecological oncology, a survival advantage can be achieved when compared with surgery performed by general surgeons or generalist gynaecologists.

Surgical Staging Sheet(Form GO 3)
• specially designed form used for detailed recording of findings at surgery: – helps in the proper documentation of the stage of the
disease which assists in prognosticating, training and research.
– also useful in determining and auditing further treatment for cancer patient.

SURGICAL STAGING FORM GO 3
Patient’s name:
Date: Hospital number:
Age (years):
Abdominal incision type: Low transverse Midline
Paramedian
Cytology:
Fresh frozen histology:
GROSS FINDINGSUterus:
Fallopian tube (right):
Fallopian tube (left):
Ovary (right):
Ovary (left):
Stomach:
Omentum:
Intestines:
Colon / Rectum:
Liver:
Gall bladder:
Spleen:
Pancreas:
Diaphragm:
Kidney (right): Kidney (left):
Ureter (right):
Ureter (left):

Bladder:
Lymph nodes:
1. External iliac – 2. Internal iliac –
3. Obturator – 4. Common iliac –
5. Para – aortic –
Ascites:
Pouch of Douglas:
Peritoneal surfaces:
Peritoneal washings:
Description of operation performed:
FOR VULVAL CANCERS
Lead Surgeon/s: Consultant/s- Senior registrar/s-
Assistant surgeons: Senior registrar /s- Registrar/s -
Name and signature of recorder: Date: Designation:

General Post-operative Care
• General counselling on clinical status and the operative findings.
• Post-operative fluid management.• Post-operative antibiotics, analgesics and other
necessary drugs (including anticoagulants).• Adjuvant chemotherapy or radiotherapy or both.• Hormonal therapy.• Palliative care (including parenteral nutrition).

Cancer Chemotherapy Chart (GOU 3)CANCER CHEMOTHERAPY CHART (Form GOU – 05)
NAME: WARD: HOSP. No: DATE: COURSE:DIAGNOSIS: STAGE / SCORE:DRUGS: D1 D2 D3 D4 D5 D6 D7 D8 D9 D10 D11
1.2.3.4.5.6.7.8.9.10.LIVER FUNCTION TESTS D0 D1 D2 D3 D4 D5 D6 D7 D8 D9 D10 D11 D12 D13 D14 D15 D16
BILIRUBIN (Total and Conjugated) ALKALINE PHOSPHATASE AST ALT ALBUMIN/GLOBULIN. TOTALELECTROLYTES AND UREA Na+
K+
Cl -
HCO3-
UREA URIC ACID CREATININEFULL BLOOD COUNT PACKED CELL VOLUME WHITE BLOOD CELL COUNT PLATELETSULTRASONOGRAPHYCHEST X – RAY TUMOUR MARKERS URINE PREGNANCY TEST (bhcG level)

WHO Analgesic Ladder- Administer drugs by mouth- Administer by the clock- For the individual- Attention to details- Adjuvants include sedatives, anxiolytics,
anti - depressants Step 1: Non – opioids
Step 2: Weak opioids +/- non – opioids
Step 3: Strong opioids +/- non – opioids
+/- adjuvants
Step 1
Step 2
Step 3
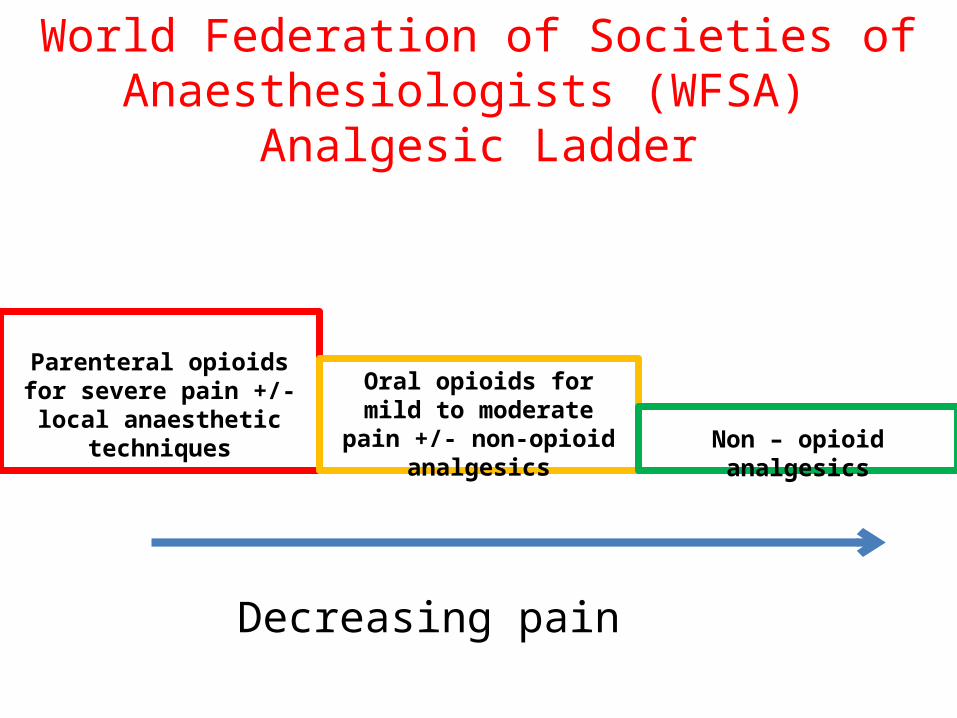
World Federation of Societies of Anaesthesiologists (WFSA) Analgesic Ladder
Decreasing pain
Parenteral opioids for severe pain +/- local anaesthetic
techniques
Oral opioids for mild to moderate pain +/- non-
opioid analgesics
Non – opioid analgesics

Palliative and Nursing Care for Gynaecological Cancer Patients
• The principles include:– Effective communication (truth telling) about the nature
of the disease and available strategies for cure, control and palliation. Timely and efficient use of such strategies.
– Ethical issues• Autonomy, Beneficience, Non-maleficence, Justice• Do Not Resuscitate (DNR), Living Will, Euthanasia
– Legal issues– Caring for the carers– Sexual needs and considerations


References1. http://www.who.int/mediacentre/news/releases/2003/pr27/en/2. Odukogbe A A, Adebamowo C A, Ola B, Olayemi O, Oladokun A, Adewole I F, Omigbodun A O,
Aimakhu C O, Okunlola M A, Fakulujo O and Oluyemi F. A. Ovarian cancer in Ibadan: characteristics and management. Journal of Obstetrics and Gynecology. 2004. 24 (3): 294 – 297.
3. O'Brien M, Mwangi-Powell F, Adewole IF, Soyannwo O, Amandua J, Ogaja E, Okpeseyi M, Ali Z, Kiwanuka R, Merriman A. Improving access to analgesic drugs for patients with cancer in sub-Saharan Africa. Lancet Oncol. 2013 Apr;14(4):e176-82. doi: 10.1016/S1470-2045(12)70343-1.
4. Adesina A, Chumba D, Nelson AM, Orem J, Roberts DJ, Wabinga H, Wilson M, Rebbeck TR. Improvement of pathology in sub-Saharan Africa. Lancet Oncol. 2013 Apr;14(4):e152-7. doi: 10.1016/S1470-2045(12)70598-3.
5. Morhason-Bello IO, Odedina F, Rebbeck TR, Harford J, Dangou JM, Denny L, Adewole IF. Challenges and opportunities in cancer control in Africa: a perspective from the African Organisation for Research and Training in Cancer. Lancet Oncol. 2013 Apr;14(4):e142-51. doi: 10.1016/S1470-2045(12)70482-5.
6. Graham A, Adeloye D, Grant L, Theodoratou E, Campbell H. Estimating the incidence of colorectal cancer in Sub-Saharan Africa: A systematic analysis. J Glob Health. 2012 Dec;2(2):20404. doi: 10.7189/jogh.02.020204.
7. Braithwaite D, Boffetta P, Rebbeck TR, Meyskens F. Cancer prevention for global health: a report from the ASPO International Cancer Prevention Interest Group. Cancer Epidemiol Biomarkers Prev. 2012 Sep;21(9):1606-10. doi: 10.1158/1055-9965.EPI-12-0848. Epub 2012 Jul 31.
8. Jedy-Agba E, Adebamowo C. Knowledge, attitudes and practices of AIDS associated malignancies among people living with HIV in Nigeria. Infect Agent Cancer. 2012 Oct 25;7(1):28. doi: 10.1186/1750-9378-7-28.
9. World Health Report 2006: working together for health. Geneva: World Health Organization, 2006.

Thank You&
Happy Weekend