Stage I Endometrial Carcinoma: Value of MR Imaging in ...
6
J ou rnal of the Korean Radiological Society, 1994 : 31 (4) : 731-735 Stage I Endometrial Carcinoma: Value of MR Imaging in Determining Depth of Myometriallnvasion 1 Jin Joo Lee , M.D. , Kie Hwan Kim , M.D. , Byung Hee Lee , M.D. , Soo Yil Chin , M. D. , Eui Don Lee , M.D.2 , Kyung Hee Lee , M.D.2 Purpose: In patients with endometrial carcinoma , preoperative knowledge of myometrial tumor extension has important prognostic and therapeutic impli- cations. The purpose of this study was to assess the usefulness of magnetic reson- ance (MR) imaging in preoperative evaluation of myometrial invasion of early stage endometrial ca rci noma. Materials and Methods : MR imaging findings of 31 consecutive patients with histologically proved endometrial carcinoma , were prospectively analyzed and compared with pathologic results. Myometrial invasion was classified into three groups: absence of myometrial invasion , superficial and deep invasion in accord- ancewith clinical stage IA, IB , IC respectively . Results: MR imaging had an accuracy of 74.2% , a sensitivity of 85.7%, and a specificity of 70 .8% in stage IA : 67.7% , 46.2% , 83.3% in stage ’ B (n=13) : 93. 5%, 81.8%, 100% in stage IC (n=11) respectively. Overall accuràcy was 79.9%. Nine of ten incorrect cases were underestimated , and one was overestimated. Degree of invasiveness was underestimated in cases with adenomyosis , small tumor showing focal wall thickening , and faint junctional zone in postmeno- pausal women. Conclusion : The results of this study show that MR imaging can be used to dis- tinguish superficial and deep penetration of myometrium in endometrial carci- noma. Index Words: Uterine neoplasms , MR Uterine neoplasms , staging INTRODUCTION In endometrial carcinoma even with disease appar- ently limited to the uterus , survival may be affected by several factors , including histologic tumor grade and depth of myometr ial tumor invasion. 80th of them cor- relate with the prevalence of Iymph node metastasis. Abeler reported that the depth of myometrial invasion was the most important prognostic factor in his study of 1566 patients with endometrial carcinoma(1). Although histopathology and tumor grade may be determined by diagnostic curettage prior to surgery , myometrial in- vas ion could be evaluated only after hysterectomy. Re- cently , magnetic resonance (MR) imaging has become ' Oepartment o fD iag n ost icR ad iology. Korea Can cerCen ter H ospit al ' Oepartmen t ofGyn ecology , KoreaCancer Center H ospital R eceived May20. 1994; Accepte dJul y13 , 1 994 Add ress repri nt req u es tst o: Jin Joo L ee , M .O., Oepar tmen t o fD iag n osti cR adi Korea Can cer Cente r H os pi ta l. 21 5-4 , Gongn eung-dong , Nowon-gu , Seou l, 139-240Korea. Te l. 82-2-974-2501 F ax.82- 2-978-2005 the imaging technique of choice for evaluating myome- trial invasion of endometrial carcinoma(2 , 3) . On the basis of MR imaging results , in patients with deep myometrial invasion and at high risk for Iymph node metastasis , preoperat ive radiat ion therapy or chemo- therapy would be indicated. We assessed the value of MR imaging in determin - ing myometrial invasion in stage 1 endometrial carci- noma. MATERIALS and METHODS This study was based on 31 consecutive patients (aged 36 -67 years , mean ; 52.9 years) with histologic- ally verified endometrial adenocarcinoma between October 1991 and March 1994. Twenty - two patients were postmenopausal and nine were premenopausal No patient had previously received chemotherapy or radiation therapy. Clinical stage of all patients was st- age 1 according to the classificat ion system of the 1 nte-
Transcript of Stage I Endometrial Carcinoma: Value of MR Imaging in ...

Journal of the Korean Radiological Society, 1994 : 31 (4) : 731-735
Stage I Endometrial Carcinoma: Value of MR Imaging in Determining Depth of Myometriallnvasion 1
Jin Joo Lee, M.D., Kie Hwan Kim, M.D. , Byung Hee Lee, M.D. ,
Soo Yil Chin , M .D. , Eui Don Lee, M.D.2, Kyung Hee Lee, M.D.2
Purpose: In patients with endometrial carcinoma, preoperative knowledge of myometrial tumor extension has important prognostic and therapeutic implications. The purpose of this study was to assess the usefulness of magnetic resonance (MR) imaging in preoperative evaluation of myometrial invasion of early stage endometrial ca rci noma.
Materials and Methods : MR imaging findings of 31 consecutive patients with histologically proved endometrial carcinoma, were prospectively analyzed and compared with pathologic results. Myometrial invasion was classified into three groups: absence of myometrial invasion, superficial and deep invasion in accordancewith clinical stage IA, IB, IC respectively.
Results: MR imaging had an accuracy of 74.2%, a sensitivity of 85.7%, and a specificity of 70.8% in stage IA (n=기 : 67.7%, 46.2%, 83.3% in stage ’B (n=13) : 93. 5%, 81.8%, 100% in stage IC (n=11) respectively. Overall accuràcy was 79.9%. Nine of ten incorrect cases were underestimated, and one was overestimated. Degree of invasiveness was underestimated in cases with adenomyosis, small tumor showing focal wall thickening , and faint junctional zone in postmenopausal women.
Conclusion : The results of this study show that MR imaging can be used to distinguish superficial and deep penetration of myometrium in endometrial carcinoma.
Index Words: Uterine neoplasms, MR Uterine neoplasms, staging
INTRODUCTION
In endometrial carcinoma even with disease apparently limited to the uterus, survival may be affected by several factors , including histologic tumor grade and depth of myometr ial tumor invasion. 80th of them correlate with the prevalence of Iymph node metastasis. Abeler reported that the depth of myometrial invasion was the most important prognostic factor in his study of 1566 patients with endometrial carcinoma(1). Although histopathology and tumor grade may be determined by diagnostic curettage prior to surgery , myometrial invasion could be evaluated only after hysterectomy. Recently , magnetic resonance (MR) imaging has become
'Oepartment ofDiagnostic Radiology. Korea CancerCenter Hospital 'Oepartment ofGynecology, KoreaCancer Center Hospital Received May20. 1994; AcceptedJuly 13,1994 Address reprint requests to: Jin Joo Lee , M.O., Oepartment ofD iagnostic Radi 。 l ogy , Korea Cancer Center Hospi ta l. 215-4, Gongneung-dong, Nowon-gu, Seoul, 139-240Korea. Tel. 82-2-974-2501 Fax.82-2-978-2005
the imaging technique of choice for evaluating myometrial invasion of endometrial carcinoma(2 , 3). On the basis of MR imaging results , in patients with deep myometrial invasion and at high risk for Iymph node metastasis , preoperative radiat ion therapy or chemotherapy would be indicated.
We assessed the value of MR imaging in determining myometrial invasion in stage 1 endometrial carcinoma.
MATERIALS and METHODS
This study was based on 31 consecutive patients (aged 36 -67 years, mean ; 52.9 years) with histologically verified endometrial adenocarcinoma between October 1991 and March 1994. Twenty - two patients were postmenopausal and nine were premenopausal No patient had previously received chemotherapy or radiation therapy. Clinical stage of all patients was stage 1 accord ing to the classification system of the 1 nte-
η

Journal of the Korean Radiological Society, 1994 : 31(4) : 731 - 735
rnational Federation of Gynecology and Obstetrics(4) Myometrial spread was classified as absent (stage
IA) , superficial (stage 18 , less than 50% of myometrial thickness) and deep (stage IC , 50% or more of myometrial thickness). Patients with disease at other stage were excluded from the study because in those cases radiation therapy would be the treatment of choice and consequently no pathologic specimens could be obtained to be compared with.
MR images were obtained within two weeks before surgery. MR examination was performed with a 1.0 T unit (SMT -100 X, Shimadzu , Japan). The matrix size was 256 X 256 , with a 28 cm field of view , and the data were displayed in a 256 X 256 matrix. The section thickness was 5 mm with an intersection gap of 2 mm. T1 -weighted [500 -700/20 -30 (TR/TE)] and T2 -weighted [2000 -2500/80 -95 (TR/TE)] spin -echo images were obtained in sagittal and axial planes with two signal average. Gadolinium - enhanced T1 -weighted images were added in both axial and sagittal planes. After rapid bolus injection of Gadopentetate dimeglumine (2cc/kg of body weight), MR images were obtainted 10 minutes later.
MR images were analyzed in terms of location and size of tumor, depth of myometrial invasion , endocervical extension , and detection of any associated diseases such as leiomyoma, adenomyosis. On MR images, tumor was identified as enhancing mass and high signal intensity attached to endometrial surface Tumor confined to the endometrium was diagnosed when the low signal intensity band around tumor (junctional zone) appeared to be intact. Myometrial invasion was diagnosed in the case of segmentally disrupted junctional zone on axial or sagittal T2 -weighted images. In patients in whom the junctional zone was indistinct, the presence of a smooth interface between endome trium and myometrium was considered a reliable sign that the myometrium was not involved with the tumor. Conversely , irregular endometrium myometrium interface was considered a sign of myometrial invasion(5)
AII patients underwent primary surgery including a thorough exploratory staging , total abdominal hysterectomy , bilateral salpingo - oophorectomy, and selective biopsy of paraaortic and pelvic nodes.
MR imaging findings were compared with pathologic results ofthese surgical specimens.
Table 1 . MR Imaging Stage vs Pathology Stage in Endometrial Carcinoma
Path。\MR IA 18 IC Total
IA 6 o 7 18 7 6 0 13 IC 0 2 9 11 Total 13 9 9 31
Patho ; pathologic stage MR ; MRstage
RESUlTS
On pathologic examination , the stage of the tumor was IA in 7 cases , 18 in 13 , and IC in 11. Average tumor
a
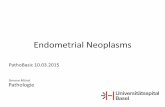
b Fig. 1. a, b. Stage IA endometrial carcinoma a. Transaxial contrast-enhanced T1-weighted (SE 500/20) image shows focallesion in anterior endometrial wall ofthe uterine fundus (arrow) as lower signal intensity than the myometrium b. Sagittal T2-weighted (2000 /80) image shows irregular junctional zone underneath an endometrial mass representing inner myometrial invasion (arrow). However following path이。glc
examination revealed blood clot and cellular debris without residual tumor or myometrial invasion
m
ι

size was 1.1 cm in the stage IA cases , 1.5 cm in stage 18 and 5.0 cm in stage IC.
Twenty -one patients (67.7 %) were correctly staged with MR imaging , and ten (32.3%) were incorrectly staged (Table 1) . Errors in determining the depth of myometrial tumor invasion were underestimation in nine and overestimation in one
In stage IA (n=7) , six were correctly staged and one was overestimated as stage 18. In thatcase , path이 oglc
result showed no residual mass but cellular debris and blood clot (Fig. 1). 1 n stage 18 (n =13) , only six were correctly assessed and the remaining seven were underestimated as stage IA. Those underestimated cases revealed coexisiting adenomyosis (n=1) (Fig. 2) , leiomyoma (n=2) , and focal infiltrative lesion (eg. microinvasion) (n=4) . In stage IC (n=11) , nine were correctly staged with MR images (Fig. 3). Remaining two were underestimated as stage 18. 80th of them revealed faintjunctional zone on MR imaging.
MR imaging had an accuracy of 74.2% , sensitivity of 85.7% and specificity of 70.8% in stage IA; 67.7% , 46 2% , 83.3% in stage 18 ;93.5%, 81.8%, 100% in stage IC, respectively (Table 2). Overall accuracy was 79. 9% in the assessment of myometrial invasion of endometrial carcinoma.
DISCUSSION
Endometrial carcinoma is uncommon malignant neoplasm in Korea , accounting for 1.6% of all malignant neoplasm of female genital tract(6). Endometrial carcinoma is , however, the third most common malignancy arising in female genital tract , following cervical carcinoma and ovarian carcinoma. Endometrial carcinoma tends to be diagnosed at early stage due to abnormal vaginal bleeding. The high cure rate for localized endometrial carcinoma has emphasized the importance of early detection and treatment
MR imaging is widely accepted as an useful diagnostic tool for women with pelvic tumor. 8ecause of its capacity to produce multiplanar images and its unsurpassed soft tissue contrast , MR imaging is superior t。ultrasonography or computed tomography for determining the extent of uterine masses(3 , 7). In endometrial carcinoma, contrast between carcinoma and normal endometrium is accentuated on MR image. Detec-
Jin Joo Lee. et al: Stage I Endometrial Carcinoma
tion of small tumors confined to endometrium is possible on enhanced images(3 , 8, 9). Furthermore , the enhanced sequences allowed better assessment of myometrial invasion (5 , 9)
a
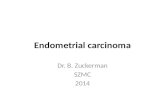
b Table 2. Diagnostic Accuracy 01 MR Imaging in Stage 1 Endo- Fig. 2. a, b. Stage IB endometrial carcinoma rnetrial Carcinoma (%a. Transaxial T2-weighted (SE 2000/80) image shows a small
endometrial tumor (short arrow) and underlying local adenomyosis (curved arrow). Underlying adenomyosis obscures the presence 01 myometrial invasion b. Sagittal T2-weighted (SE 2000/80) image demonstrates endometrial mass (short arrow) and local adenomyosis (curved arrow). Pathologic result reveals superlicial myometrial invasion B : bladder V: vaginal canal
Stage Accuracy Sensitivity Specilicity PPV NPV
IA (n =7) 74.2 85.7 70.8 46.2 94.4
IB(n= 13) 67.7 46.2 83.3 66.7 68.2 IC (n =11) 93.5 81.8 100 100 90.9
* PPV: positive predictive value NPV : negative predictive value
1 j η

Journal of the Korean Radiological Society, 1994 : 31 (4) : 731-735
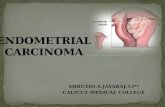
a b Fig. 3. a, b. Stage IC endometrial carcinoma a. Transaxial contrast-enhanced T1-weighted (SE 500 /20) image shows a large lobulated endometrial mass occupying inner half ofthe myometrium. The degree of enhancement of a mass is lower than that of the surrounding myometrium, showing substantial interface (arrowheads) b. Transaxial T2-weighted (SE 2000/80) image shows a tumor (T) separable from fluid in the endometrial cavity (C). Junctional zone in the leftanterior aspect is disrupted and outer myometrial invasion is evident (curved arrow).
The depth of myometrial penetration is an important prognostic factor. Depth of myometrial invasion strongly correlates with the presence of Iymph node metastases. The incidence of pelvic Iymph node metastases varies with depth of myometrial invasion as follows tumor limited to endometrium only (1 %l, superficial invasion (5%) and deep invasion(31 %). The incidence of aortic Iymph node metastases varies with depth of myometrial invasion approximately as follows : tumor limited to endometrium only (1 %) , superficial invasion (3%) , deep invasion (18%) (1 이.
In evaluating myometrial invasion with T2-weighted MR images, accuracy has been reported in range of 74-87%(2, 7, 11 , 12). MR concordance with histologic examination is about 80% for staging endometrial carcinoma and 82% for distinguishing superficial from deep myometrial invasion(2). Contrast-enhanced MR imaging may be indicated for correct interpretation of myometrial invasion in preoperative assessment of endometrial carcinoma(3). Lien et al reported MR accuracy in deep invasion was 82%, with sensitivity of 91 % and specificity of 64 %(11). Sironi et al reported a sensitivity and specificity of MR assessment in stage 1 endometrial carcinoma; 57% , 16% in stage IA, 74%, 74% in stage 18, 88%, 85% in stage IC , respectively (13). The accuracy of MR imaging in our study (79.9%) was similar to the results of other authors.
In our cases which were incorrectly staged , all büt 。ne were understaged. Two cases of deeply invasive tumor were understaged as superficial invasion on MR images. Remaining seven cases of superficial myometrial invasion were underestimated as cases of no myometrial invasion. In these cases, the presence of adenomyosis or leiomyomas seemed to be a factor interfering with accurate MR interpretation. The pres-
ence of polypoid tumors that induced marked deformity of the uterine cavity was mainly responsible for such MR errors(13). Other factors were the small tumor showing focal wall thickening and retained fluid in endometrial cavity. Minimal or microscopic invasion was the most common reason for underestimating myometriaJ invasion , regardless ofthe imaging technique (3).
In one case, the cause of overestimation was probably hyperplastic myometrium and blood clo t. Presence of myoma or distended endometrial cavity sometimes complicated the assessment of myometrial invasion (3 , 11). Endometrial hyperplasia, submucosal leiomyoma, blood clots may increase the endometrial thickness or widen the uterine cavity , simulating endometrial carcinoma(2).
Endometrial carcinoma usually occurs in postmenopausal women in whom the junctional zone is faint This factor complicated the assessment of myometrial invasion as wel l. Although , MR imaging showed low specificity for tumor detection , it showed hi gh accu racy in staging of histologically documented endometrial carcinoma (2)
This study concluded that MRI was a very useful diagnostic tool in assessing the depth of myometrial invasion in stage 1 endometrial carcinoma.
REFERENCES
1. Abeler VM, Kjorstad KE. Endometrial adenocarcinoma in Norway. Cancer 1991 ; 67: 3093-31 03
2. Hricak H. Stern JL, Fisher MR, Shapeero LG , Winkler ML, Lacey CG. Endometrial carcinoma staging by MR imaging. Radiology
1987 ; 162 : 297-305 3. Yamash ita Y, Mizutani H, Torashima M, et al. Assessment of
myometrial invasion by endometrial carcinoma : transvaginal
m
여

Jin Joo Lee. et a/: Stage 1 Endometrial Carcinoma
sonography vs. contrast-enhanced MR imaging. AJR 1993 ; 161 : 11 : 95-1 06
595-599 9. Thurnher SA. MR imaging 01 pelvic masses in women :contrast-
4. FIGO stages-1988 Revision. GynecolOncol1989 ; 35 : 125-127 enhanced vs. unenhanced images. AJR 1992 ; 159 : 1243-1250
5. Sironi S, Colombo E, Villa G et al. Myometrial invasion by 10. Smith RC, McCarthy S. Magnetic resonance staging 01 neo-
endometrial carcinoma: assessment with plain and gadoli - plasms 01 uterus. Radiologic Clinics o( North America 1994; 32
nium-enhanced MR imaging. Radiology 1992 ; 185: 207-212 109-131
6. TS Lee, KH Cho, JG Ahn et al. Malignancies olthe lemale genital 11. Li en HH, Blomlie V, Trope C, Kaern J, Abeler VM. Cancer 01 the
organs , 10 years experience. A study 01 incidence and endometrium : Value 01 MR imaging in determining depth 01 in-
histopathology Journal o( the Korean Association of Obstetrics vasion intomyometrium. AJR1991 ; 157: 1221-1223
andGynecology 1991 ; 34: 1425-1432 12. Hricak H, Rubinstein LV, Gherman GM , Karstaedt N. MR imaging
7. Del Maschio A, Vanzulli A, Sironi S, et al. Estimating the depth 01 evaluation 01 endometrial carcinoma : result 01 an NCI cooperat-
myometrial involvement by endometrial carcinoma: ellicacy 01 ive study. Radiology 1991 ; 179 : 829-832
transvaginal sonographyvs. MR imaging‘ AJR1993 ;533-538 13. Sironi S, Taccagni G, Garancini P, Belioni C, Del Maschio A.
8. Hricak H, Hamm B, Semelka RC , et a l. Carcinomas 01 uterus: use Myometrial invasion in endometrial carcinoma: assessment by
01 gadopentetate dimeglumine in MR imaging. Radiology 1991 ; MR imaging. AJR 1992 ; 158: 565-569
대 한 방사 선 의 학회 지 1994 ; 3 1( 4) : 731 - 735
제 I 기 자궁내막암의 근층침범 진단에 었어서 MRI의 유용성
원자력병원 진단방사선과원자력병원 산부인과
이진주 · 김기환 · 이병회 · 진수일 · 이의돈1. 이경희 1
목 적 :자궁내막암 환자에서 자궁근층 침범정도는 환자의 예후를 판정하거나 치료방침을 결정하는데 중요한 요소이다.
저자들은 자궁내막암 환자에서 근층 침범 여부와 그 침범된 갚이를 진단하는데 있어 자기공명영상 (MRI ) 의 유용도를 알고
자전향적 연구를시행하였다.
대상 및 방법:자궁내막암으로 진단받은 31 명의 환자에서 MRI 소견을 분석하여 근층 침범여부 및 그 정도를 판정하고 수
술후 병리소견과 비교하였다. 근층침범 정도는 FIGO Staging과 일치하도록 자궁내막층에 국한된 경우, 자궁근층의 50% 미
만이 침범된 경우, 자궁근층의 50% 이상이 침범된 경우로 분류하여 진단하였다.
결 과 :MRI 소견에의한 근층침범 진단의 정확도, 민감도, 특이도는 Stage IA 환자에서 74.2%. 85.7%. 70.8% 이고 Stage
IB 에서 각각 61-7%. 46.2% . 83.3% . Stage IC 에서 93-5%. 8 1.8%. 100% 이었다. MRI소견상 부정확한 예측을 보인 10여|중 9예
에서 understagingOI었으며 그 원인으로는 동반된 자궁내막증, 자궁근종, 혈종등에 의한 근층의 변형때문이거나 나이가 많
은 환자에서 junctional zoneOI 불명확한 때문이었다.
결 론 : MRI는 자궁내막암의 근층 침범정도를 진단하는데 매우 유용하나, 특히 동반된 자궁질환이 있는 경우맨 판정에 주
의해야한다.
m
ω

국제 학술대회 일정표 [IIIJ
1995/ 05/ 01 - 03 9th Int. Symposium on Radionuclides in Nephro_Urology venue : Santa Fe Hilton Santa Fe, New Mexico, USA. contact: Andrew Taylor, JR., M.O. , Emory University Hosptal
1364 Clifton Road , N .E., Atlanta, Georgia 30322, USA. (tel : 1-404 - 7274852; fax: 1-404 -7273889)
1995/ 05/ 15 -19 Annual Meeting of the Society of Computed Body Tomography venue: Grand Hyatt New York, NY, USA contact: Dapt. of Radiology, Virginia Mason Clinic,
P.O. 80x 900, Seattle, WA98111 , USA. (tel: 1 - 206 - 2236851; fax:
1995/ 05/15-20 32nd Annual Congress European Soc. of Paediatric Radiology (ESPR) venue: Utrecht, The Netherlands. contact: Dr. P.P.G. Kramer, Het Wilhelmina Kinderzkh.,
P.O. 80x 18009, 3501 CA Utrecht, The Natherlands (tel: 31 - 30-320637 ; fax: 31 -30-334825)
1995/ 05/17-21 28th Annual Conf . and Postgraduate Course in Head and Neck Radiology venue: Pittsburgh, PA, USA.
contact: Ms. 8eth A. Filip, Am.Soc.Head & Neck Radiol , 2210 Midwest Road , Oak 8rook, IL60521 , USA. (tel ’ 1 -708 - 5740660 ; fax: 1 -708 - 574066 1)
1995/ 05/ 28 -02 7th Asian & Oceanian Congress of Radiology venue: Putra World Trade Center Kuaia Lumpur, Maiaysia. contact: Dr. K. Kulaveerasingam, c/o Dept. of Radiology,
University Hospital, 59100 Kuala Lumpur, Malaysia. (tel: 60 - 3 - 7502069; fax: 60 - 3 - 7557740)
1995/ 06/04-08 58th Annual Scientific Meeting of the Canadian Association of Radiologists venue: Palais des Congres Montreal, Quebec, Canada contact: Suzanne Charette Ex. Dir. ,
5101 8uchan St., 5th Floor, Montreal, Queb. H4P 2R9, Canada. (tel: 1-514-7383111; fax: 1-514-7385199)
1995/ 06/ 12 -16 1995 Rontgen Centenary Congress/ Joint Congress of the B’R venue: Int. Convention Center 8irmingham, United Kingdom. contact: Vanessa Whitehead, 8ritish Inst. of Rad. (8IR)
36 Port1and Place, London WIN 4A T, United Kingdom (te1: 44 - 71 -4367807 ; fax: 44 -71 - 2553209)
1995/ 06/ 20-23 CAR ’ 95 Computer Assisted Radiology-9th Int. Symposium and Exhibition venue: ICC In t. Congress Center 8erlin, Germany. contact: Prof. H.U. Lemke, Techn. Univ. 8erlin,
Franklinstr. 28/29, 0-1000 8erlin 10, Germany (tel: 49-30-31473100 ; fax: 49-30-31431103)
-736-
제공 :대한방사선의학회 국제협력위원회