ST101 Companion Diagnostics for Targeted Therapy in …handouts.uscap.org/2016_cm15_linde_1.pdf ·...
14
ST101 Companion Diagnostics for Targeted Therapy in Cancer David G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP September 9, 2012 © 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 1 Molecular Diagnostics in Lung Cancer: Is it worth it? Neal Lindeman, MD Director, Molecular Diagnostics Brigham and Women’s Hospital Associate Professor of Pathology Harvard Medical School American Society for Investigative Pathology Companion Meeting, USCAP March 12, 2016 Van Gogh, 1885 Introductions 2 I *DO* have conflicts of interest! Astra Zeneca – consulting re: engaging pathologists in clinical trials (selumetinib in KRAS+ lung cancer) Molecular Pathology: in the middle of a storm 4 Patients and Docs Notas: Industry Euros: Government Boreas: Insurance Zephyros: Academics
Transcript of ST101 Companion Diagnostics for Targeted Therapy in …handouts.uscap.org/2016_cm15_linde_1.pdf ·...
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 1
Molecular Diagnostics in Lung Cancer:Is it worth it?
Neal Lindeman, MD
Director, Molecular DiagnosticsBrigham and Women’s Hospital
Associate Professor of Pathology Harvard Medical School
American Society for Investigative PathologyCompanion Meeting, USCAP
March 12, 2016
Van Gogh, 1885
Introductions
2
I *DO* have conflicts of interest!
Astra Zeneca – consulting re: engaging pathologists in clinical trials(selumetinib in KRAS+ lung cancer)
Molecular Pathology: in the middle of a storm
4
Patients and Docs
Notas: Industry
Euros: Government
Boreas: Insurance
Zephyros:Academics
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 2
Academics: we started this� What is our true Conflict of Interest?
• Publications• Grants• Career development• Centers of excellence
� “Precision Medicine”• Optimism: better outcomes• Blurring of research and practice
• “n of one” experiments• “basket” trials
� Fun and Interesting 5
Industry: Fanning the flames� Venture Capital: quicker ROI than drugs
• Take loss build market sell� Tech manufacturers: Outpacing “Moore’s Law”
• Sell boxes/juice
� Dx companies: LDT “loophole”• Bypass FDA• [IP protection]• More flexibility than hospitals
� Pharma: more successful trials• Better outcomes• “Save” failed drugs 6
Insurance: Cooling it down
� Evidence-based medicine• Pessimism in medicine• Do no harm
� Cost containment• Tests are expensive• Drugs are really expensive
� Distinction between research and practice• If it’s unproven, it’s an experiment• Patients and payers don’t pay for research 7
Government: Braking wind
� Regulation of lab tests• CLIA/CMS: labs as medical practice• FDA: tests as devices• “LDTs”: tests unique to one lab
� FDA: LDTs are unsafe• No clinical validity or utility• Lack of standardization
� FDA proposal• Premarket approval vs. standards-based 8
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 3
Patients and their doctors:What should we do?
� Is there clinical benefit to molecular diagnostics in cancer?• Under what circumstances?• How big is the benefit?• Should we pay for it?
Fundamental conflict:Evidence-based medicine vs. Precision Medicine
9
Use case: lung cancer
� Why lung cancer?• Very common
• Rapidly & inexorably progressive disease• Can assess outcomes quickly• Patients more willing to try novel therapies
• Multiple molecular alterations• Differing levels of utility
10
Case Presentation:
� 52 yr old female � Symptoms (months):
• Headaches• Light/dark sensitivity• Chronic dry cough
� MRI: • Enhancing dural mass
� DDx: ???
11
Case Presentation:
� 52 yr old female � Symptoms (months):
• Headaches• Light/dark sensitivity• Chronic dry cough
� MRI: • Enhancing dural mass
� Differential Dx: • Tumor
• Meningioma• Lymphoma• Metastasis • Primary CNS tumor
• Granuloma• Sarcoidosis• Tuberculosis
• Chronic meningitis• Wegener’s
12
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 4
Case presentation:� Brain biopsy:
13
Case presentation:
� Brain biopsy:• Adenocarcinoma
• Lung• Colon• Other
14
Case Presentation
� Follow-up imaging studies• 5 cm lung mass• Additional masses:
• Lung (x2), liver (x2), bone
� Non-small Cell Lung Cancer, Stage IV
15
Lung Cancer is Bad
� Survival @ 18 months:• Stage I: 49 – 65% • Stage II: 39 - 55%• Stage III: 4 – 15%• Stage IV: 1%
� Median survival:• Stage I/II: 17 – 32 months• Stage III: 9 - 22 months• Stage IV: 16 – 36 weeks
Van Gogh, 1885 16
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 5
Lung Cancer is Bad for society
� 14% of cancers
� 28% of deaths
� 71% mortality
American Cancer Society, 2011
Cancer Mortality, 2011
ng
al
st
as
te
ia
ma
er
ry
er
ey
S
ma
ma
us
id
Deaths
LungColorectal
LeukemiaProstate
PancreasBreast
LymphomaLiver
OvaryBladderKidneyCNS
MelanomaEndometrium
Thyroid
Myeloma
20K20K
40K
60K
80K
100K
120K
140K
160K
U.S. Cancer Deaths, 2011
17
Lung Cancer Treatment: 2004
� Stage I: surgery� Stage II: surgery� Stage IIIA: surgery
• +/- XRT• +/- chemotherapy
� Stage IIIB: chemo + XRT� Stage IV: chemo, palliation
18
Return to Case:� History:
• Never smoked• Course:• 4/01: Carboplatin-Paclitaxel
• Response for 6 wks• Progression by 12/01
• 12/01: Cetuximab (Erbitux)• Stabilization for 4 mos• Progression by 7/02
8/02
5/03
19
Return to Case:� History:
• Never smoked• Course:• 4/01: Carboplatin-Paclitaxel
• Response for 6 wks• Progression by 12/01
• 12/01: Cetuximab (Erbitux)• Stabilization for 4 mos• Progression by 7/02
• 8/02: Gefitinib (Iressa)• Sustained response for 30 mos
8/02
5/03
20
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 6
Return to Case:� History:
• Never smoked• Course:• 4/01: Carboplatin-Paclitaxel
• Response for 6 wks• Progression by 12/01
• 12/01: Cetuximab (Erbitux)• Stabilization for 4 mos• Progression by 7/02
• 8/02: Gefitinib (Iressa)• Sustained response for 30 mos• Relapse in 2/05
8/02
5/03
2/05
21
Case summary:
� 52F nonsmoker with stage IV NSCLC• Expected survival: ~ 6 mos• Likelihood of being alive after 18 mos: ~1%
� Initial treatment with platinum chemo• Initial response, but quick relapse
� Tried two anti-EGFR study agents• Erbitux: progressed on therapy• Iressa: regression, 30 mos after Dx!
22
What is EGFR and why target it?
23
EGFR signaling simplified:
� Ligand binds� Receptor Dimerization � Phosphorylation� Downstream signaling
• RASRAFERK• JAKSTAT• PIK3CAAKTmTOR
� Cells proliferate, survive
Very commonly overexpressed in human carcinomas24
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 7
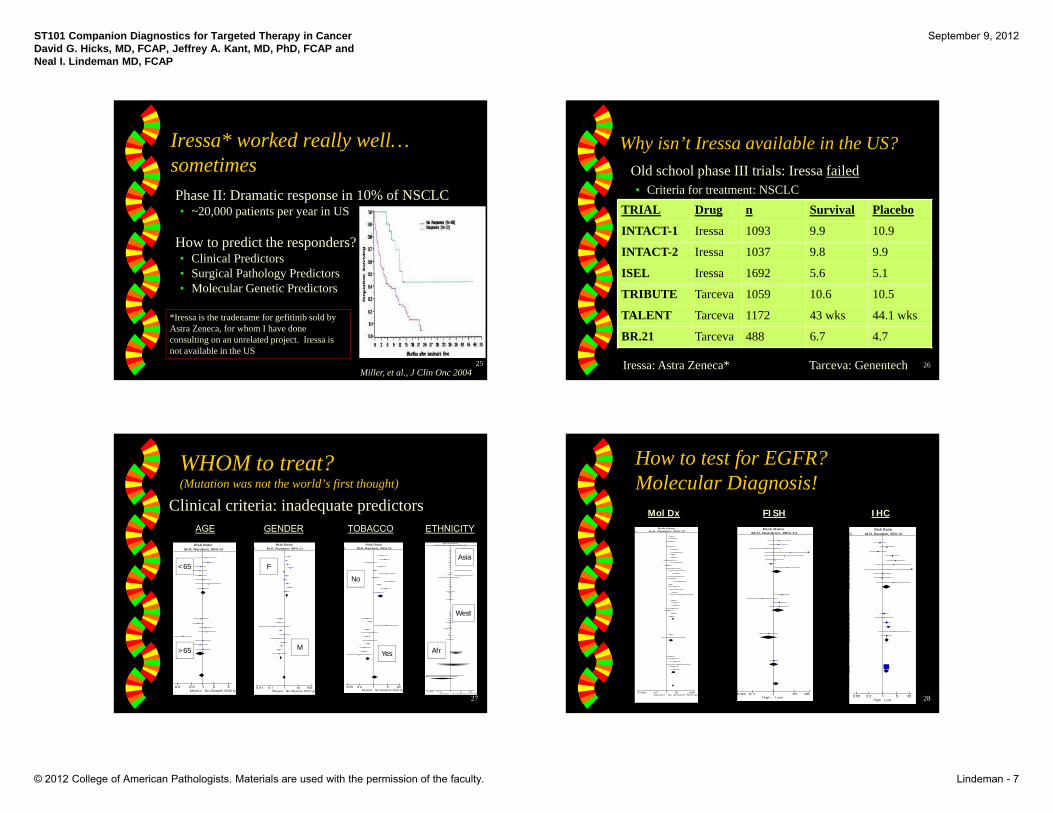
Iressa* worked really well… sometimes
� Phase II: Dramatic response in 10% of NSCLC • ~20,000 patients per year in US
� How to predict the responders?• Clinical Predictors• Surgical Pathology Predictors• Molecular Genetic Predictors
Miller, et al., J Clin Onc 200425
*Iressa is the tradename for gefitinib sold by Astra Zeneca, for whom I have done consulting on an unrelated project. Iressa is not available in the US
Why isn’t Iressa available in the US?� Old school phase III trials: Iressa failed
• Criteria for treatment: NSCLCTRIAL Drug n Survival Placebo
INTACT-1 Iressa 1093 9.9 10.9
INTACT-2 Iressa 1037 9.8 9.9
ISEL Iressa 1692 5.6 5.1
TRIBUTE Tarceva 1059 10.6 10.5
TALENT Tarceva 1172 43 wks 44.1 wks
BR.21 Tarceva 488 6.7 4.7
26Iressa: Astra Zeneca* Tarceva: Genentech
WHOM to treat?(Mutation was not the world’s first thought)
� Clinical criteria: inadequate predictors
IRisk Ratio
M-H, Random, 95% CI
0.01 0.1 1 10 100Mutant No Mutant/ Wild typ
GENDERRisk Ratio
M-H, Random, 95% CI
0.2 0.5 1 2 5Mutant No Mutant/ Wild typ
AGE
CIRisk Ratio
M-H, Random, 95% CI
0.05 0.2 1 5 20Mutant No Mutant/ Wild typ
TOBACCORisk Ratio
M-H, Random, 95% CI
0.05 0.2 1 5 20Mutant No Mutant/ Wild typ
ETHNICITY
<65
>65
F
M
No
Yes
Asia
West
Afr
27
IHCRisk Ratio
M-H, Random, 95% CI
0.02 0.1 1 10 50High Low
FISH
How to test for EGFR?Molecular Diagnosis!
CI
]]]]]]]]]]]
]]]]]]]
]]
Risk RatioM-H, Random, 95% CI
0.05 0.2 1 5 20High Low
IRisk Ratio
M-H, Random, 95% CI
0.002 0.1 1 10 500Mutant No Mutant/ Wild typ
Mol Dx
28
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 8
What hath EGFR wrought?Oncologic Transformation� Old School:
• Nonspecific therapy targets all replicating cells• High toxicity, low efficacy
• Stage, grade, histology determine therapy• Small cell / Non-small cell
� New Wave:• Target specific problematic molecule
• Less toxicity, ?higher efficacy?• Molecular classification helps determine therapy
29
Lung Cancer, c. 2005-2008� Horrible, lethal cancer from which most
patients died quickly, for decades, with no major improvements in outcome
� EGFR Hope• Pessimism: Evidence-based medicine
• Better definition of when EGFR helps
• Optimism: Personalized medicine• Search for other genes with similar effects
30
What is a favorable outcome?Radiographic Response Progression-free Survival
Overall Survival
Goss, ASCO, 2010
Evidence-based medicine:What is a response?
32
Gideon M. Blumenthal et al. JCO doi:10.1200/JCO.2014.59.0489
PFS vs ORR OS vs ORR/PFSSame data,
different display
Why not OS? Crossover
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 9
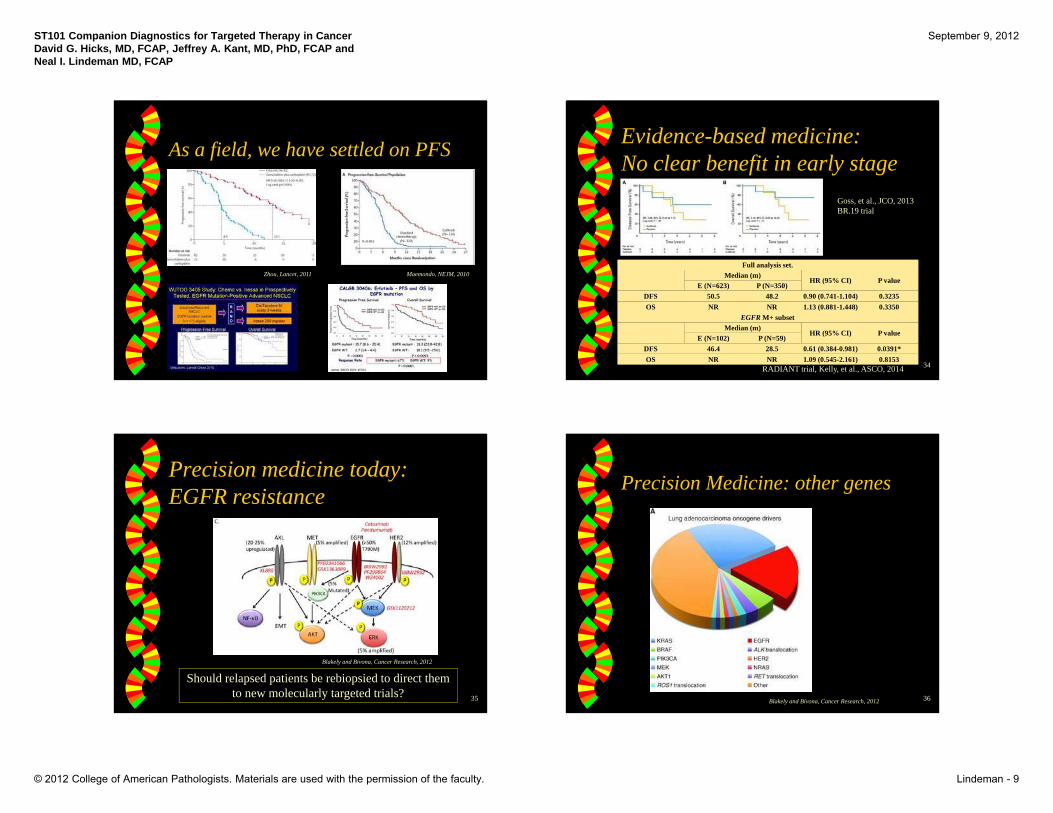
As a field, we have settled on PFS
Zhou, Lancet, 2011 Maemondo, NEJM, 2010
Evidence-based medicine:No clear benefit in early stage
34
Goss, et al., JCO, 2013BR.19 trial
Full analysis set.Median (m)
HR (95% CI) P valueE (N=623) P (N=350)
DFS 50.5 48.2 0.90 (0.741-1.104) 0.3235OS NR NR 1.13 (0.881-1.448) 0.3350
EGFR M+ subsetMedian (m)
HR (95% CI) P valueE (N=102) P (N=59)
DFS 46.4 28.5 0.61 (0.384-0.981) 0.0391*OS NR NR 1.09 (0.545-2.161) 0.8153
RADIANT trial, Kelly, et al., ASCO, 2014
Precision medicine today:EGFR resistance
35
Blakely and Bivona, Cancer Research, 2012
Should relapsed patients be rebiopsied to direct them to new molecularly targeted trials?
Precision Medicine: other genes
36Blakely and Bivona, Cancer Research, 2012
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 10
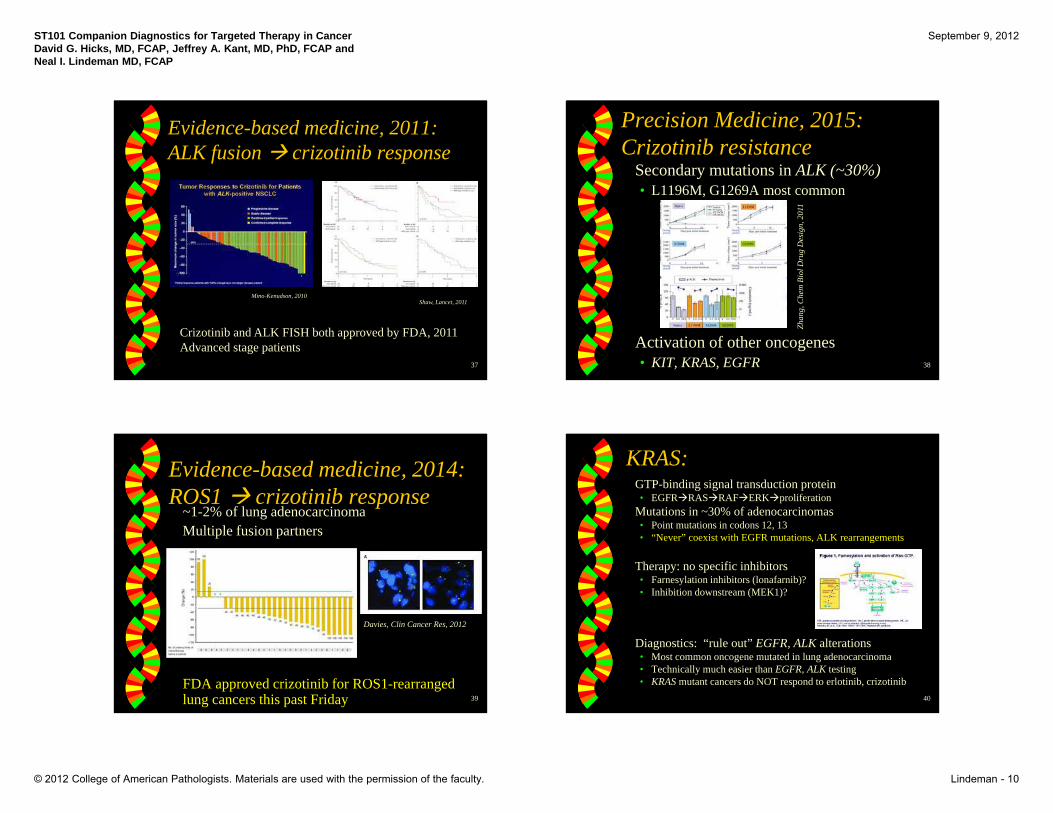
Evidence-based medicine, 2011:ALK fusion crizotinib response
Crizotinib and ALK FISH both approved by FDA, 2011Advanced stage patients
37
Mino-Kenudson, 2010Shaw, Lancet, 2011
Precision Medicine, 2015:Crizotinib resistance� Secondary mutations in ALK (~30%)
• L1196M, G1269A most common
� Activation of other oncogenes• KIT, KRAS, EGFR
Zhan
g, C
hem
Bio
l Dru
g D
esig
n, 2
011
38
Evidence-based medicine, 2014:ROS1 crizotinib response� ~1-2% of lung adenocarcinoma� Multiple fusion partners
� FDA approved crizotinib for ROS1-rearranged lung cancers this past Friday 39
Davies, Clin Cancer Res, 2012
KRAS:� GTP-binding signal transduction protein
• EGFRRASRAFERKproliferation� Mutations in ~30% of adenocarcinomas
• Point mutations in codons 12, 13• “Never” coexist with EGFR mutations, ALK rearrangements
� Therapy: no specific inhibitors• Farnesylation inhibitors (lonafarnib)?• Inhibition downstream (MEK1)?
� Diagnostics: “rule out” EGFR, ALK alterations• Most common oncogene mutated in lung adenocarcinoma• Technically much easier than EGFR, ALK testing• KRAS mutant cancers do NOT respond to erlotinib, crizotinib
40
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 11
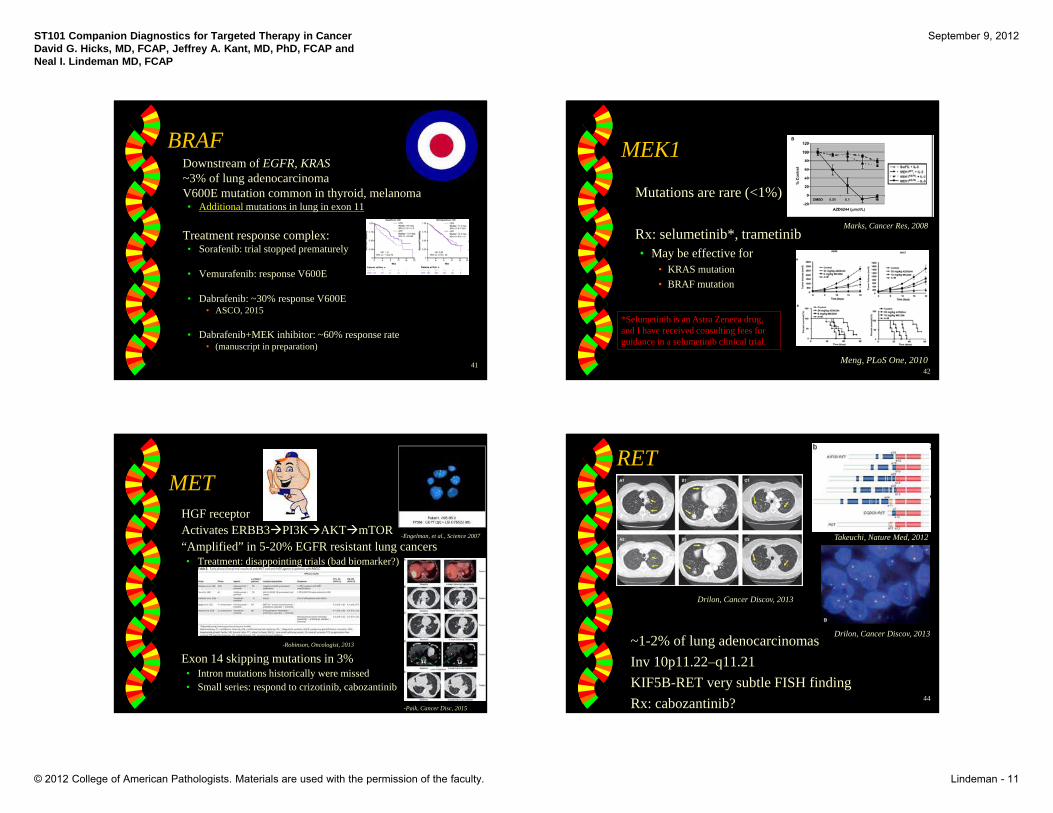
BRAF� Downstream of EGFR, KRAS� ~3% of lung adenocarcinoma� V600E mutation common in thyroid, melanoma
• Additional mutations in lung in exon 11
� Treatment response complex: • Sorafenib: trial stopped prematurely
• Vemurafenib: response V600E
• Dabrafenib: ~30% response V600E• ASCO, 2015
• Dabrafenib+MEK inhibitor: ~60% response rate• (manuscript in preparation)
41
MEK1
� Mutations are rare (<1%)
� Rx: selumetinib*, trametinib• May be effective for
• KRAS mutation• BRAF mutation
Meng, PLoS One, 2010
Marks, Cancer Res, 2008
42
*Selumetinib is an Astra Zeneca drug, and I have received consulting fees for guidance in a selumetinib clinical trial.
MET� HGF receptor� Activates ERBB3PI3KAKTmTOR� “Amplified” in 5-20% EGFR resistant lung cancers
• Treatment: disappointing trials (bad biomarker?)
� Exon 14 skipping mutations in 3%• Intron mutations historically were missed• Small series: respond to crizotinib, cabozantinib
-Engelman, et al., Science 2007
43
-Robinson, Oncologist, 2013
-Paik, Cancer Disc, 2015
RET
� ~1-2% of lung adenocarcinomas� Inv 10p11.22–q11.21� KIF5B-RET very subtle FISH finding� Rx: cabozantinib?
Takeuchi, Nature Med, 2012
44
Drilon, Cancer Discov, 2013
Drilon, Cancer Discov, 2013
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 12
NTRK1
� ~3% of lung adenocarcinoma� Chromosomal rearrangements� Mutant Cell lines inhibited by pan-TKI
Vaishnavi, Nature Med, 2013
45
Evidence regression
46
EGFR: multiple Phase III RCTs, PFS
ALK: Phase II, ORR
RET: case reports
NTRK1: mice
MEK1: cell lines
The list goes on…� ERBB2� NRG1� RIT1� NF1� PIK3CA� AKT1� NRAS� mTOR
47
But wait, there’s more: Squamous carcinoma!� FGFR1 amplification: 20%
� DDR2 mutation: 5%
� KIT/PDGFRA amplification: 10%
Dutt, et al., PLoS ONE, 2011 Ramos, et al., Cancer Biol Ther, 2009
Hammerman, et al., Cancer Discovery, 201148
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 13
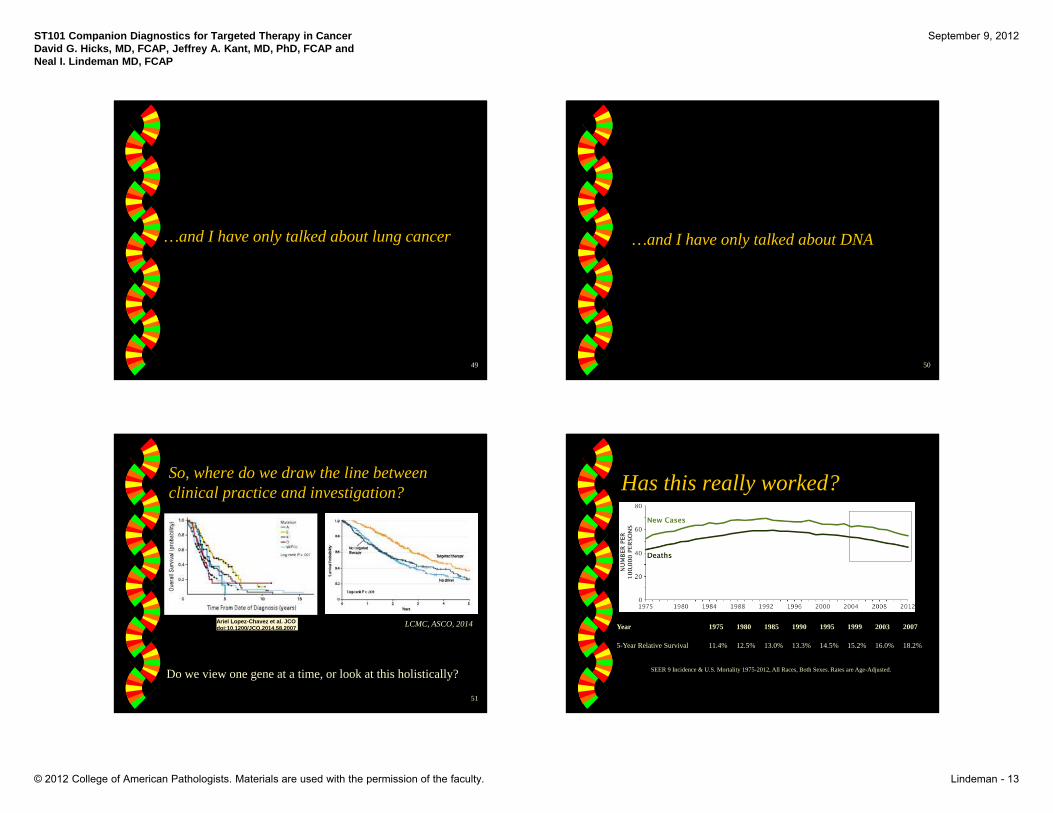
…and I have only talked about lung cancer
49
…and I have only talked about DNA
50
So, where do we draw the line between clinical practice and investigation?
51
Ariel Lopez-Chavez et al. JCO doi:10.1200/JCO.2014.58.2007 LCMC, ASCO, 2014
Do we view one gene at a time, or look at this holistically?
Has this really worked?
Year 1975 1980 1985 1990 1995 1999 2003 2007
5-Year Relative Survival 11.4% 12.5% 13.0% 13.3% 14.5% 15.2% 16.0% 18.2%
SEER 9 Incidence & U.S. Mortality 1975-2012, All Races, Both Sexes. Rates are Age-Adjusted.
ST101 Companion Diagnostics for Targeted Therapy in CancerDavid G. Hicks, MD, FCAP, Jeffrey A. Kant, MD, PhD, FCAP and Neal I. Lindeman MD, FCAP
September 9, 2012
© 2012 College of American Pathologists. Materials are used with the permission of the faculty. Lindeman - 14
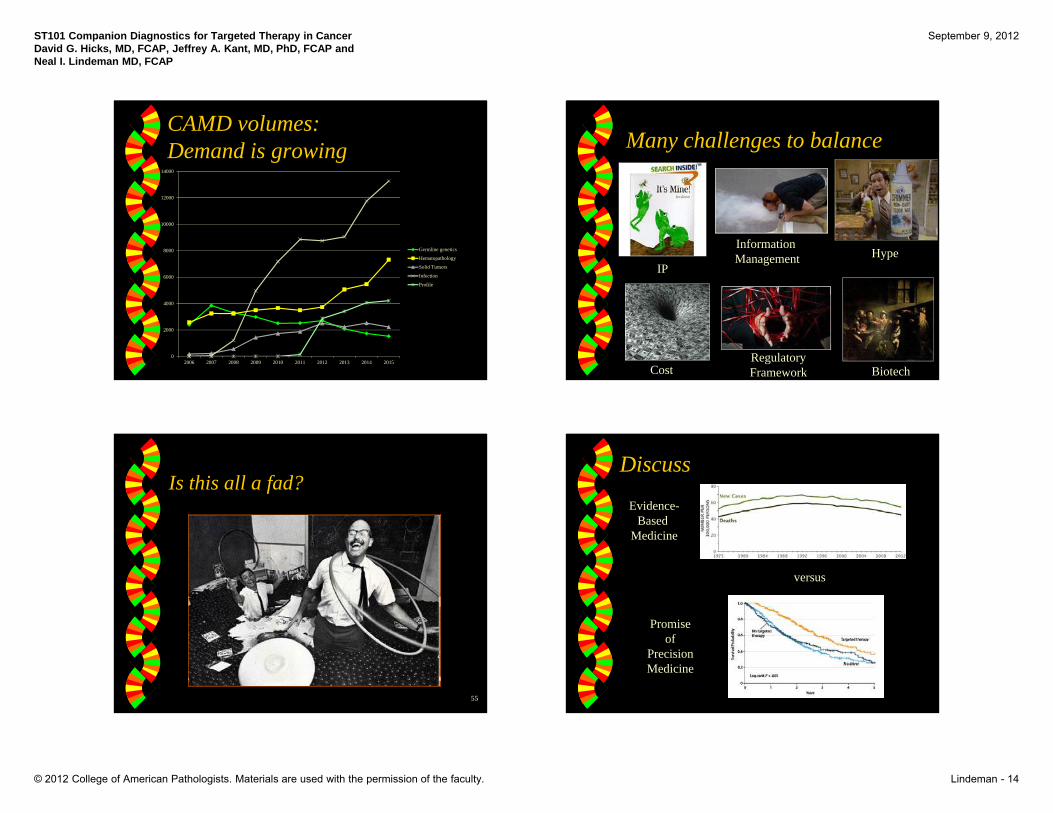
CAMD volumes:Demand is growing
0
2000
4000
6000
8000
10000
12000
14000
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Germline genetics
Hematopathology
Solid Tumors
Infection
Profile
Many challenges to balance
IP
Information Management Hype
CostRegulatoryFramework Biotech
Is this all a fad?
55
Discuss
versus
Evidence-Based
Medicine
Promise of
Precision Medicine