
st… · Web viewSafety Strategy [email protected] Draft
37
Transcript of st… · Web viewSafety Strategy [email protected] Draft
We are seeking your views on how we improve the quality of health and social care services within Staffordshire.
Last year, we developed our quality framework. It sets out our overall direction for delivering high quality care. We want all our service users to receive the highest quality of care, and we will empower our Front Line teams to provide this.
Now, we want to look at the detailed ways that we will use to improve quality. We have developed three draft strategies that describe the detail:
Safety Strategy (this document) Effectiveness Strategy Experience Strategy
We have developed these strategies with key staff from our Quality Directorate, and we would like your comments on them:
Is the document easy to understand? Does it make sense? What is missing? What can be left out? Will the measures we have outlined tell us
what we need to know? Should we use any other measures? What barriers could stop us from
achieving these strategies?
Please respond to these consultation documents! The closing date for comments is 23 October 2013.
You can email your comments to [email protected]
2
Staffordshire and Stoke on Trent Partnership Trust Safety Strategy 2013-2013
Contents
1. Executive Summary..............................................................................................4
2. Introduction...........................................................................................................5
3. Purpose................................................................................................................7
4. Vision....................................................................................................................8
5. Aims / Objectives / Measures 2013 / 14.............................................................12
6. 2013 / 2014 Priorities..........................................................................................19
7. Implementation......................................................................................................25
8. Monitoring.............................................................................................................26
9. Review..................................................................................................................26
3

1. Executive SummarySetting the Scene
The Patient Safety Strategy provides the national and local context in creating a learning culture within which the safety of patients is translated into everyday practice. The strategy will provide a vision of what a safety orientated organisation would look like, how things should be done, how the values, norms and behaviours are to be embedded within the Partnership Trust and all its services. The Patient Safety Strategy will form a key element and foundation for the Quality Framework and will provide the detail in providing assurance in embedding a patient safety culture.
The Partnership Trusts Current Position
The Safety and Effectiveness Operational Groups, Effectiveness Group and the Safety and Effectiveness Sub-Committee will provide the oversight, steer and monitoring of achievement against this strategy whilst providing assurance to the Quality Governance Committee and Trust Board on the progress of embedding a safety culture within the Partnership Trust. The organisation will in 2013-14 establish service line reporting which will provide an opportunity to encourage further embedding of the safety and risk culture at a local level.
Implementation Plan and Action Planning
This section will set out how the Patient Safety Strategy will be implemented and monitored over 2013/2014. This will detail the specific aims that have been identified for the Partnership Trusts and provide an understanding as to how those aims will be monitored and their performance against them.
Core Objectives
During the coming year the main core objectives will be to:
• Engage leaders to focus on improving their safety culture
• Engage frontline clinicians and social care colleagues in patient safety
• Enable changes in behaviour locally through implementation.
Framework
Knowing how we are doing against this strategy is pivotal in knowing how well the Partnership Trust is doing in achieving the core objectives. So how we collate and utilise this information is pivotal in how we can measure and monitor our improvements and initiatives within this strategy. To support these objectives the Partnership Trust will continue to use the Seven Steps to Patient Safety Framework
4
with an emphasis on learning and implementing solutions to strengthen the Partnership Trust as a safe organisation.
2. Introduction
The Patient Safety Strategy strategic aim is to create a learning culture within which the safety of patients is translated into every day practice. The strategy will provide a vision of what a safety orientated organisation would look like, how things should be done, how the values, norms and behaviours are to be embedded within the Partnership Trust and all its services.
During the coming year the main aims will be to:
• Engage leaders to focus on improving their safety culture
• Engage frontline clinicians and social care colleagues in patient safety
• Enable changes in behaviour locally through implementation.
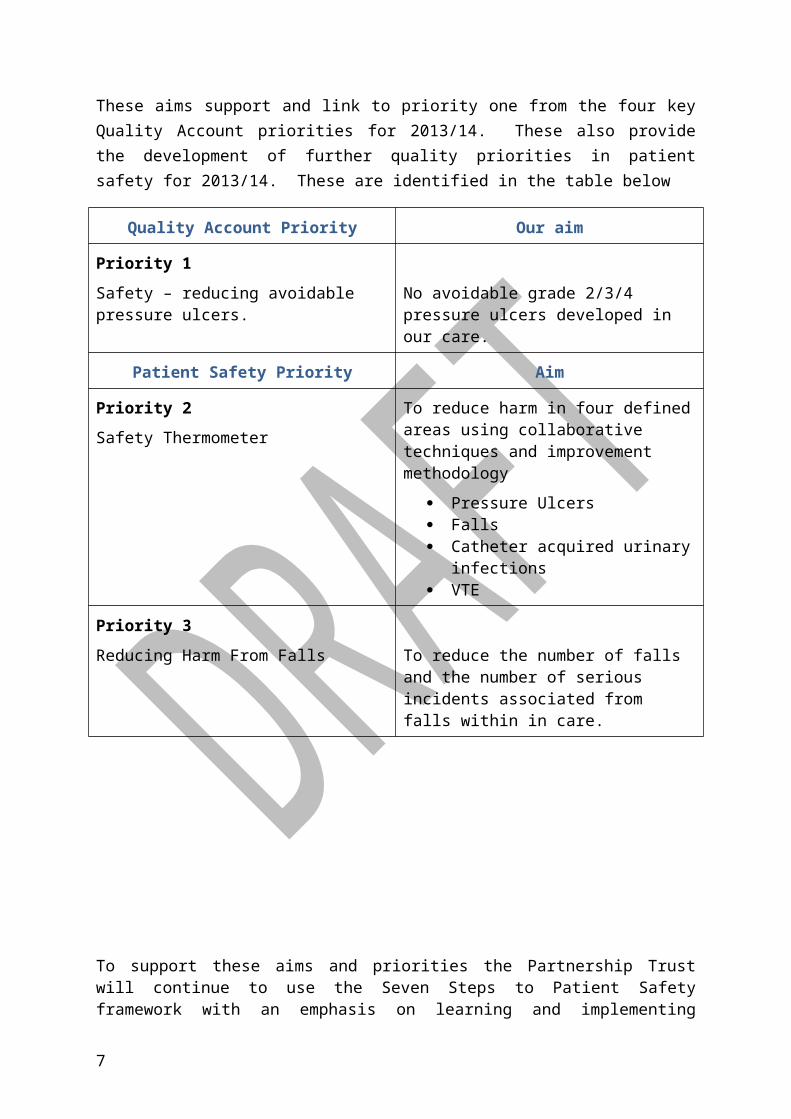
These aims support and link to priority one from the four key Quality Account priorities for 2013/14. These also provide the development of further quality priorities in patient safety for 2013/14. These are identified in the table below
Quality Account Priority Our aim
Priority 1Safety – reducing avoidable pressure ulcers.
No avoidable grade 2/3/4 pressure ulcers developed in our care.
Patient Safety Priority Aim
Priority 2Safety Thermometer
To reduce harm in four defined areas using collaborative techniques and improvement methodology
Pressure Ulcers Falls Catheter acquired urinary
infections VTE
Priority 3Reducing Harm From Falls To reduce the number of falls and the
number of serious incidents associated from falls within in care.
5
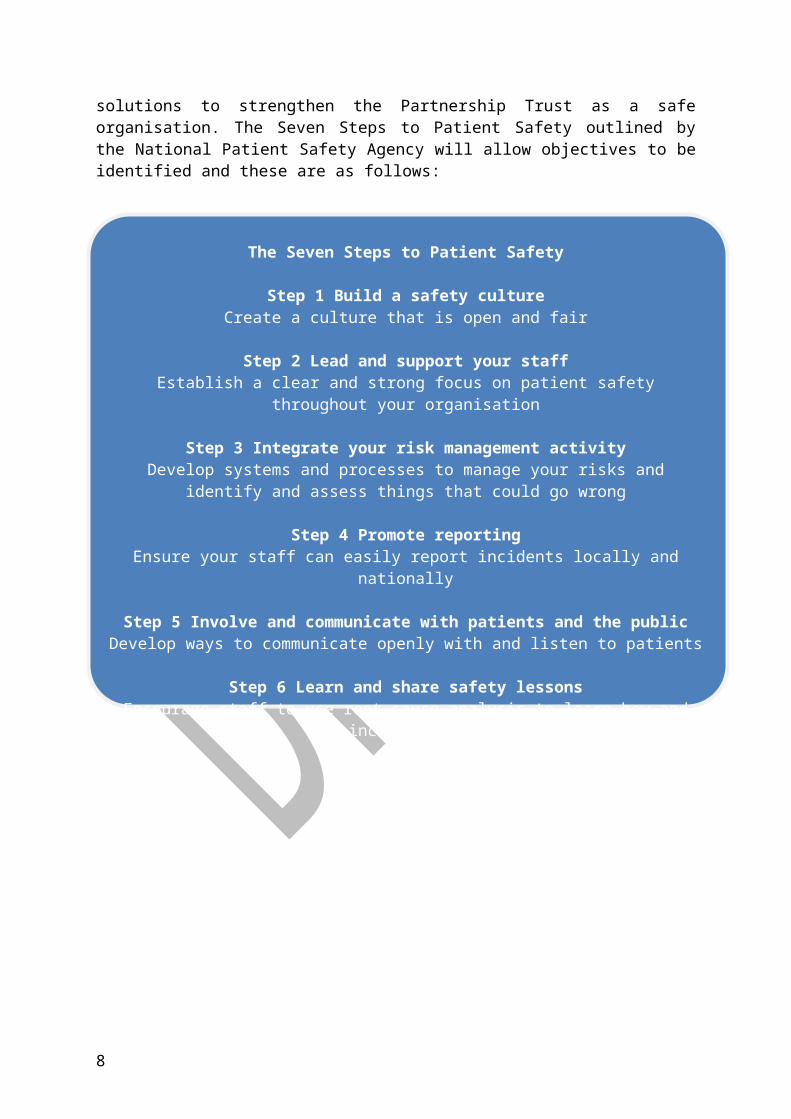
To support these aims and priorities the Partnership Trust will continue to use the Seven Steps to Patient Safety framework with an emphasis on learning and implementing solutions to strengthen the Partnership Trust as a safe organisation. The Seven Steps to Patient Safety outlined by the National Patient Safety Agency will allow objectives to be identified and these are as follows:
6
The Seven Steps to Patient Safety
Step 1 Build a safety cultureCreate a culture that is open and fair
Step 2 Lead and support your staffEstablish a clear and strong focus on patient safety throughout your organisation
Step 3 Integrate your risk management activityDevelop systems and processes to manage your risks and identify and assess
things that could go wrong
Step 4 Promote reportingEnsure your staff can easily report incidents locally and nationally
Step 5 Involve and communicate with patients and the publicDevelop ways to communicate openly with and listen to patients
Step 6 Learn and share safety lessonsEncourage staff to use root cause analysis to learn how and why incidents happen
Step 7 Implement solutions to prevent harmEmbed lessons through changes to practice, processes or systems
National Patient Safety Agency July 2004 ©
3. Purpose
What do we mean by Patient Safety?
The principles for patient safety have been developed within the strategic context of The Partnership Trust and from best practice, such as those set out by the National Patient Safety Agency (NPSA) in the publication NPSA Seven Steps to Patient Safety.
Having staff that are appropriately skilled is recognised as a key feature of the Patient Safety Initiative. This includes high risk areas of practice such as medicines management, blood administration, intravenous therapy and prevention of infection.
What do we hope to achieve as the outcomes for the organisation?
By adopting this framework it is endeavoured that this will further develop a proactive safety culture and to develop a culture where patient safety is integral to organisational business.
The Partnership Trust will continue to develop its safety culture where patient safety influences all aspects of service provision process to:
Ensure all providers encourage staff to speak up about any concerns relating to patient safety.
Ensure providers promote an environment where mistakes and untoward adverse events are identified and reported quickly and managed in a positive, responsive and generally a non-punitive way.
Ensure that lessons learned are fed back to patients and staff.
Ensure that lessons learned influence future provider plans and any new or service redesign.
Ensure providers develop ways to communicate openly with and listen to patients.
Ensure that all staff are aware and follow the ‘Being Open’ policy
7
Ensure that all staff receive an induction on the Management of Risk, Assessing Risk, Root Cause Analysis’, Being Open and Patient, Health and Safety.
Ensure that all staff will receive Root Cause Analysis training commensurate with their level of responsibility.
In order to understand our present position on the above objectives, we will undertake a baseline assessment of the safety culture, as part of a wider review of the overall quality framework across the organisation. The assessment will provide a detailed Improvement Plan in order to drive progress. It will consider a variety of issues, including:
Senior management visibility and commitment to safety
Communication between staff and managers
Attitudes to incident reporting, blame and punishment
Factors in the workplace that influence performance, such as equipment and environment.
4. VisionThe vision of the Patient Safety Strategy is that it will promote patient safety as key elements in the following areas over the next five years in line within the Quality Framework. This will promote and develop the following areas:
Provide Leadership and Support:
We will lead the care service provision and will establish a clear and strong focus on patient safety throughout the organisation. There will be a programme of training and education provided across the Partnership Trust to ensure that all staff are working in the same safe way, with systems and processes that support that.
This Strategy is focused on embedding patient safety into the culture of The Partnership Trust, its leaders and teams who are responsible for providing services. It aims to establish ownership of patient safety, at all levels from the Board, Senior Managers to front line staff. A key aspect of this will be establishing Service line reporting in service areas across the Trust who will have shared responsibility for driving improvements across the quality agenda, including patient safety
To demonstrate that safety is a priority and that the management of the organisation is committed to improvement, leaders must be visible and active in leading patient safety improvements
8
Strengthen Board Safety Culture:
Renew and sustain the Boards engagement and commitment to quality and safety.
Strengthen the integration of quality and patient safety into the routine board agenda.
Improve the Board’s ability to oversee quality and safety. Spread the engagement to all members of the Board.
We will continue with ‘Walk Arounds’ by Executive Directors and senior managers.
We will introduce service user Safety Briefings as part of the organisations remit to share learning in the Word, Patient Safety Newsletter, One liner’s through the Communication team and Team briefings.
The Partnership Trust will ensure the Board agenda continues to have Patient Safety as its first item and increase the proportion of time the Board considers for patient safety.
The Partnership Trust will through the new service line reporting measure the success of all patient safety support programmes such as training, policies and procedures and incident reporting.
Integrate Risk Management activities:We will work collaboratively with community partners continuing to develop systems and processes to identify, assess and manage risks to patient safety. We will continue to achieve compliance with the relevant standards and elements related to patient safety through developing systems and providing evidence of implementation and audit of these systems within commissioning processes
The Partnership Trust will ensure that there is an effective needs assessment, responsive services and a skill, knowledgeable workforce supported by research based information.
We will continue to identify, assess and manage risks to patient safety proactively as well as reactively; the SEOG will oversee this. Patient safety risks will be documented within the Trust Risk Register. Each risk is assessed and graded according to the approved Risk Assessment and Risk Treatment Procedure and where relevant an action plan is formulated and carried through by the appropriate Manager.
In addition risks are identified through a structured approach to addressing the requirements of the Care Quality Commission. These incorporate all corporate and governance requirements. The Partnership Trust will continue to achieve compliance with the relevant standards and elements related to patient safety through developing systems and providing evidence of implementation and audit of these systems
9
We will review and refresh our risk management structures and processes to ensure there is a clear path for escalation and monitoring from “Ward to Board”.
We will develop and agree a process for supporting the annual review process for the Care Quality Commission.
We will develop a front line to Board level dashboard of indicators of patient safety.
Promote Reporting:We will promote incident reporting and ensure that staff can easily report incidents locally and nationally. The Partnership Trust will continue to refine our approach to incident reporting and providing feedback through the Safeguard electronic system.
The Partnership Trust will ensure that providers have in place an appropriate incident reporting system.
All incidents are expected to be managed by the appropriate services manager with support from the Risk Team if necessary. Each incident is monitored and each Operational Manager is expected to support the instigation of all root cause analysis.
We will agree a common language for patient safety incidents with all partners based upon National Patient Safety Agency (NPSA) guidance
We will review the links between local and national reporting to ensure consistency of approach
We will review incident reporting procedures for all care providers, learning lessons from the best to improve reporting, including the introduction of an incident hotline and online reporting generic email box/one telephone number
We will strengthen our work on promoting the importance of incident reporting with all staff through the development of quality assurance process and education.
We will consider developing targets for increasing in incident reporting either across priority areas or services this will include near miss reporting
We will work with colleagues across the Quality Directorate to ensure there is effective linking of reporting and managing of related incidents, PALS, complaints and risks.
Involve the Public and Communicate with patients:
We will proactively build continuous and meaningful engagement with public and patients to develop ways to involve and communicate openly with patients and the public.
We will continue to build on our successes with patient and public involvement/Experience from our Patient Experience Strategy, with particular focus on:
10
How we involve patients and the public in developing safer services
How we involve patients in their own care and treatment risks
By being open: encourage an open, two way dialogue between health professional and patients when things go wrong
We will review and refresh lines of communication and listening processes in particular we will use a range of methods to gain feedback from patients such as patient stories good & poor experiences, PREMs - real time feedback surveys/ touch Screens, hand held advanced technologies.
Learn and Share:
We will promote and specify continuous improvements by ensuring that we encourage all Partnership Trust staff to use root cause analysis to learn how and why incidents happen and share safety lessons learnt
When a patient safety incident occurs the important issue is not ‘who is to blame ’but ‘how and why it occurred’
To promote learning we need to have a systematic approach in which staff know what type of incidents should be reported, what information is needed and when and how to analyse and act on this information.
Significant event audit and root cause analysis are systematic investigation techniques that look beyond the individuals concerned and seek to understand the underlying causes and environmental context in which the incident happened.
We will deliver root cause analysis training for mangers and investigating officers to ensure that there is a cohort of expertise to facilitate robust investigations.
We will consider other learning opportunities and use best practice as it emerges
We will develop processes for the performance management of Serious Incidents
We will ensure the Never Events framework is implemented and that processes are developed to ensure lessons are learnt from Never Events and Near misses.
We will work on and develop, closing the gap on the differences between the reporting of all incidents between health and Social Care and Offender Health.
Implement Solutions to prevent Harm:
We will manage knowledge and implement solutions to prevent harm and embed a ‘lessons learned’ culture:
We will strengthen our processes to incorporate learning into care and programmes pathway design.
11
We will review the distribution and assurance processes for Central alert systems and NPSA rapid response alerts
We will use nationally recognised solutions to prevent harm.
5. Aims / Objectives / Measures 2013 / 14The vision of the Patient Safety Strategy is that it will promote patient safety as key elements in the following areas over the next five years in line with the Quality Framework. For 2013/14 the Patient Safety Strategy needs to identify aims and objectives to ensure the long-term vision is achieved whilst supporting the Quality Account priorities and Patient Safety Priorities for 2013 / 14.
Therefore the aims and objectives for 2013 /14 are detailed below with specific measures to monitor the progress and success of the Patient Safety Strategy implementation and will promote and develop the following areas:
Aim Engage leaders to focus on improving their safety culture
To support the aim to engage leaders and improve the safety culture the first two steps of the framework will be utilised and will encompass:
Step 1 Build a Safety Culture
The context for patient safety is complex. Patient safety is one component of quality alongside effectiveness and patient experience. Patient safety needs to be achieved without compromising the safety of staff and the public. The context for the safety of each individual patient is set by their surroundings, environment and circumstances therefore the risks posed within each care setting need to be continually assessed and regularly recorded.
The work on improving patient safety began with the publication of An Organisation with a Memory (DoH, 2000). Prior to this, incidents were reported manually, little analysis of data was undertaken and staff did not generally receive feedback. The emphasis was on reporting what, where, when and who. How and reasons why incidents occurred were not robustly considered, hence little learning, if any, took place.
The Partnership Trust has put in place a number of processes and systems to develop a safety culture within the organisation.
Being Open Policy:
Incident Management Policy
Risk Management Strategy and Policy
12
Objective
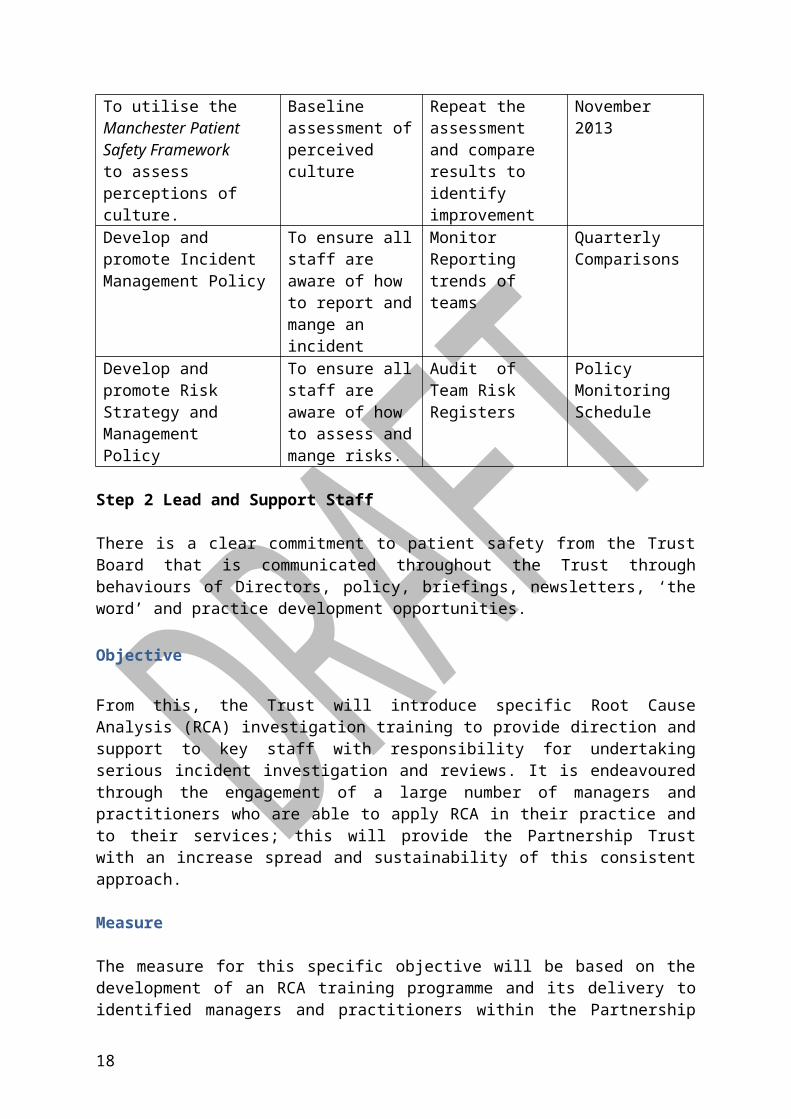
To develop a proactive safety culture within the Partnership Trust where patient safety is integral to service delivery. The Partnership Trust has adopted the Manchester Patient Safety Framework (MaPSaF) (UoM 2006) which was developed in partnership with the NPSA to gauge the safety culture of an organisation. MaPSaF uses nine dimensions of patient safety culture and for each of these describe what an organisation would look like at five levels of safety culture.
Measure
For 2013 – 2014 the objective is to use this framework as a measure with the Partnership Trust Senior Management Team and frontline staff to assess perceptions of culture. This will provide the Partnership Trust with a baseline for improvement and comparison in the future years and will be compared to the staff survey results for 2013/14.
Aim Outcome Assurance Mechanism
Date
To utilise the Manchester Patient Safety Frameworkto assess perceptions of culture.
Baseline assessment of perceived culture
Repeat the assessment and compare results to identify improvement
November 2013
Develop and promote Incident Management Policy
To ensure all staff are aware of how to report and mange an incident
Monitor Reporting trends of teams
Quarterly Comparisons
Develop and promote Risk Strategy and Management Policy
To ensure all staff are aware of how to assess and mange risks.
Audit of Team Risk Registers
Policy Monitoring Schedule
Step 2 Lead and Support Staff
There is a clear commitment to patient safety from the Trust Board that is communicated throughout the Trust through behaviours of Directors, policy, briefings, newsletters, ‘the word’ and practice development opportunities.
Objective
From this, the Trust will introduce specific Root Cause Analysis (RCA) investigation training to provide direction and support to key staff with responsibility for undertaking serious incident investigation and reviews. It is endeavoured through the engagement of a large number of managers and practitioners who are able to apply
13
RCA in their practice and to their services; this will provide the Partnership Trust with an increase spread and sustainability of this consistent approach.
Measure
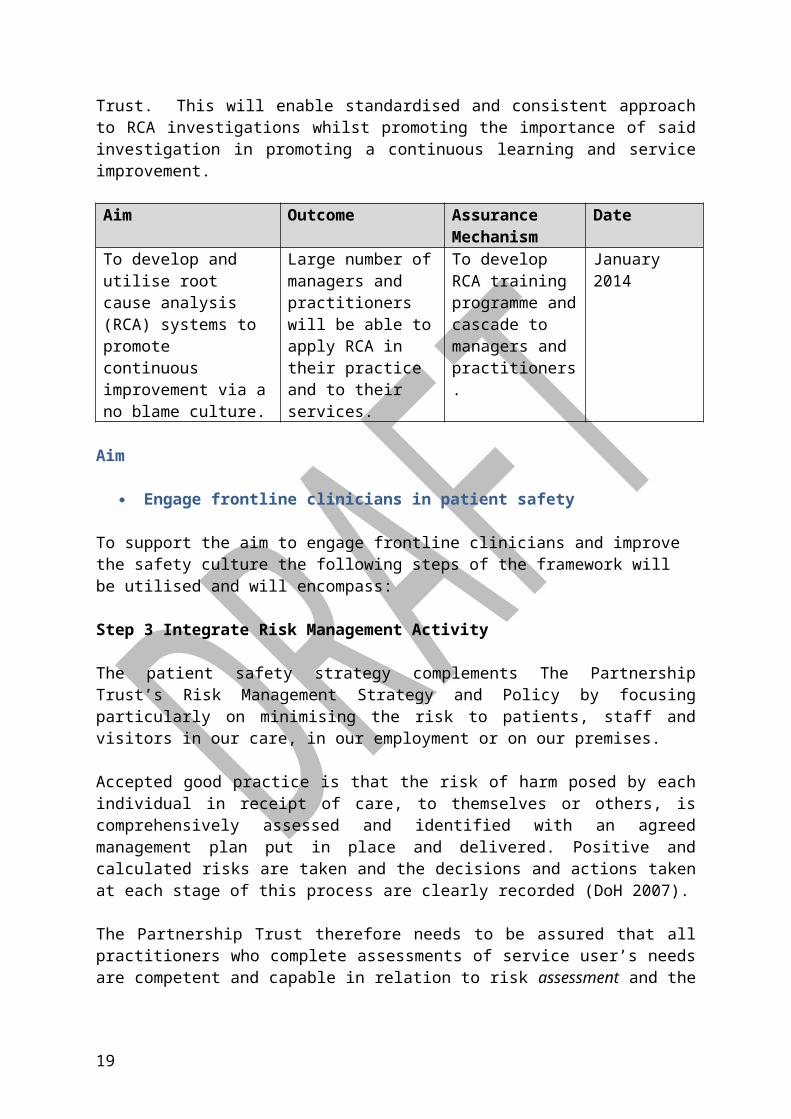
The measure for this specific objective will be based on the development of an RCA training programme and its delivery to identified managers and practitioners within the Partnership Trust. This will enable standardised and consistent approach to RCA investigations whilst promoting the importance of said investigation in promoting a continuous learning and service improvement.
Aim Outcome Assurance Mechanism
Date
To develop and utilise root cause analysis (RCA) systems to promote continuous improvement via a no blame culture.
Large number of managers and practitioners will be able to apply RCA in their practice and to their services.
To develop RCA training programme and cascade to managers and practitioners.
January 2014
Aim
Engage frontline clinicians in patient safety
To support the aim to engage frontline clinicians and improve the safety culture the following steps of the framework will be utilised and will encompass:
Step 3 Integrate Risk Management Activity
The patient safety strategy complements The Partnership Trust’s Risk Management Strategy and Policy by focusing particularly on minimising the risk to patients, staff and visitors in our care, in our employment or on our premises.
Accepted good practice is that the risk of harm posed by each individual in receipt of care, to themselves or others, is comprehensively assessed and identified with an agreed management plan put in place and delivered. Positive and calculated risks are taken and the decisions and actions taken at each stage of this process are clearly recorded (DoH 2007).
The Partnership Trust therefore needs to be assured that all practitioners who complete assessments of service user’s needs are competent and capable in relation to risk assessment and the management of risk. Competent means they know how to, and are capable means, they do it consistently on an on-going basis.
Objective
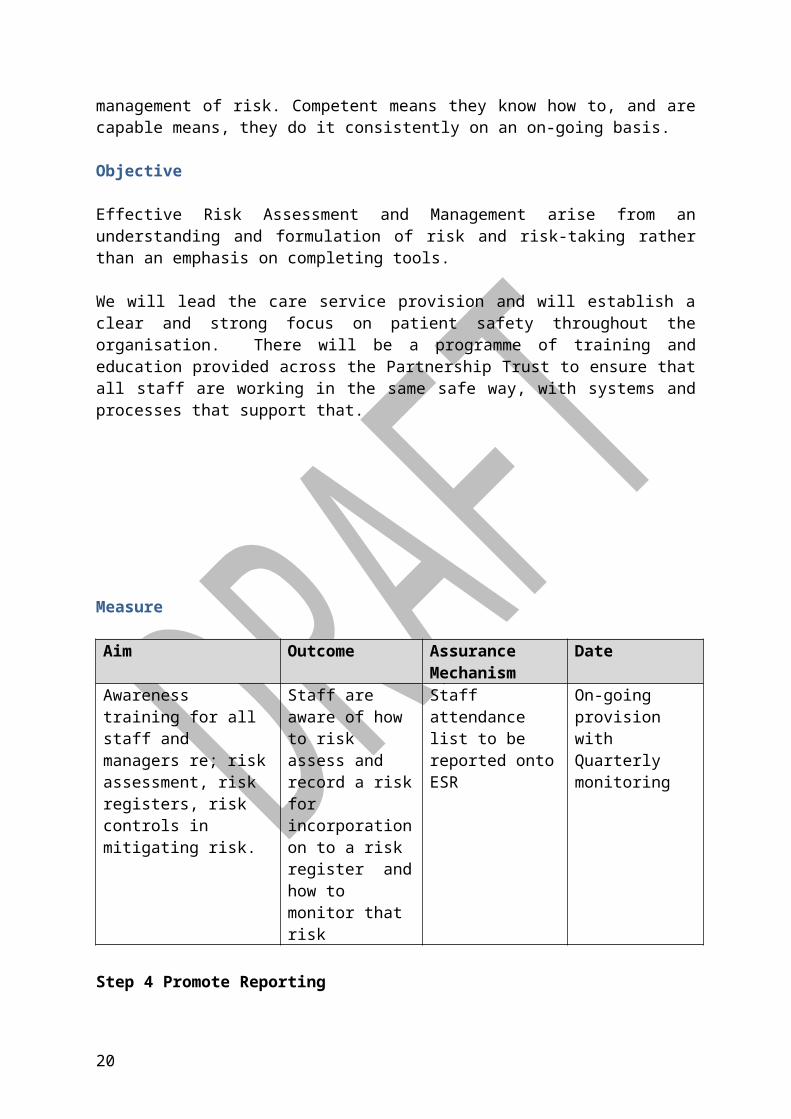
Effective Risk Assessment and Management arise from an understanding and formulation of risk and risk-taking rather than an emphasis on completing tools.
14
We will lead the care service provision and will establish a clear and strong focus on patient safety throughout the organisation. There will be a programme of training and education provided across the Partnership Trust to ensure that all staff are working in the same safe way, with systems and processes that support that.
Measure
Aim Outcome Assurance Mechanism
Date
Awareness training for all staff and managers re; risk assessment, risk registers, risk controls in mitigating risk.
Staff are aware of how to risk assess and record a risk for incorporation on to a risk register and how to monitor that risk
Staff attendance list to be reported onto ESR
On-going provision with Quarterly monitoring
Step 4 Promote Reporting
The Partnership Trust views incident reporting as a very positive aid to managing patient safety. The information we collect allows us to analyse what and where safety issues may be occurring. Investigation of incidents allows us to learn lessons and make changes to reduce the risks of recurrence.
All staff are actively encouraged to report any incident that gives them cause for concern. The Partnership Trust is committed to an open and transparent culture of raising safety concerns to ensure that the safety of people who use our services is safeguarded.
The Safeguard electronic incident reporting system has enhanced the culture of reporting for staff and the system requires managers to actively participate in the reporting of incidents in order to reduce the likelihood that they will re-occur.
Objective
Effective education, training and supervision systems are needed to support these in practice.
Incident reporting training is a key focus in the training staff receive in relation to risk management and incident reporting.
15
We will promote incident reporting by all service providers and ensure that provider staff can easily report incidents locally and nationally. The Partnership Trust will continue to refine our approach to incident reporting and providing feedback through the Safeguard electronic system.
Measure
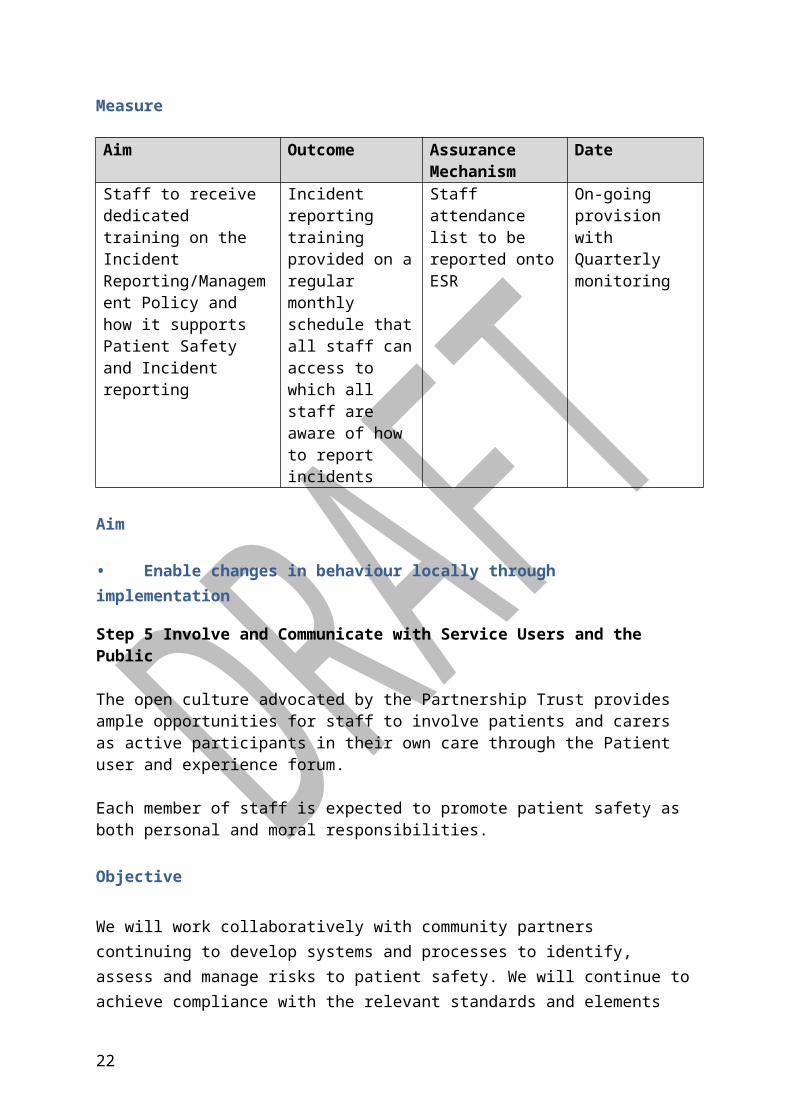
Aim Outcome Assurance Mechanism
Date
Staff to receive dedicated training on the Incident Reporting/Management Policy and how it supports Patient Safety and Incident reporting
Incident reporting training provided on a regular monthly schedule that all staff can access to which all staff are aware of how to report incidents
Staff attendance list to be reported onto ESR
On-going provision with Quarterly monitoring
Aim
• Enable changes in behaviour locally through implementation
Step 5 Involve and Communicate with Service Users and the Public
The open culture advocated by the Partnership Trust provides ample opportunities for staff to involve patients and carers as active participants in their own care through the Patient user and experience forum.
Each member of staff is expected to promote patient safety as both personal and moral responsibilities.
Objective
We will work collaboratively with community partners continuing to develop systems and processes to identify, assess and manage risks to patient safety. We will continue to achieve compliance with the relevant standards and elements related to patient safety through developing systems and providing evidence of implementation and audit of these systems within commissioning processes
16
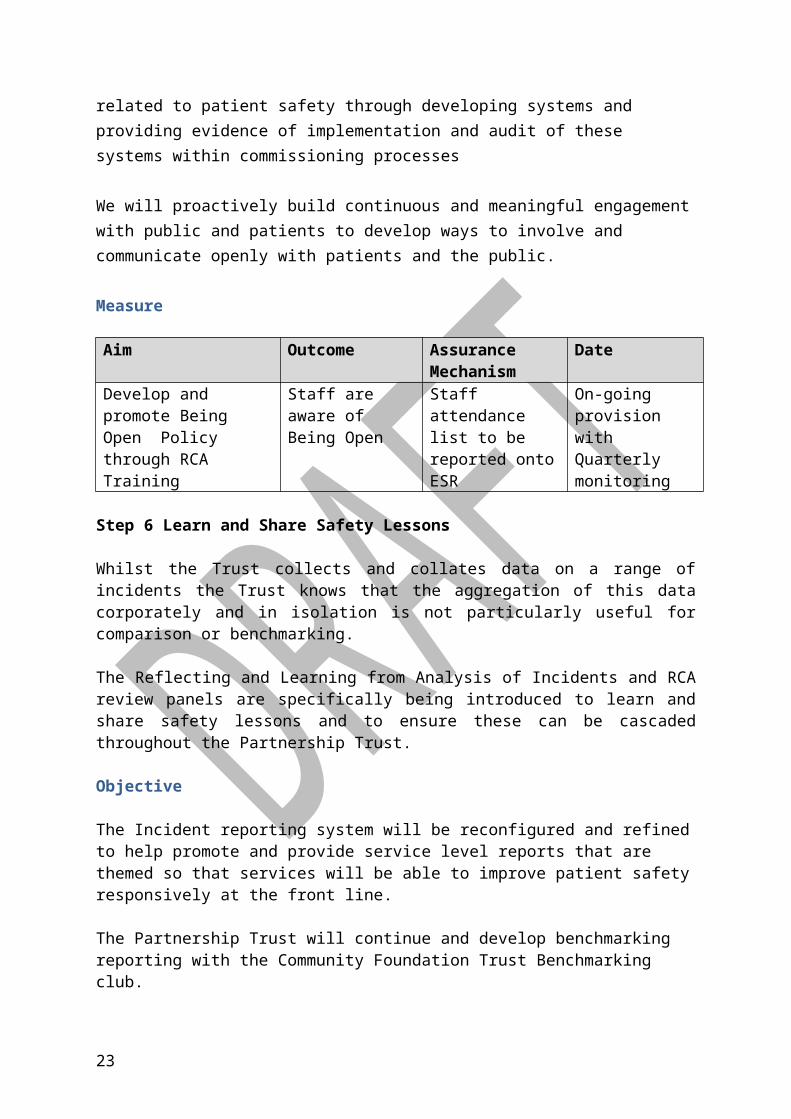
We will proactively build continuous and meaningful engagement with public and patients to develop ways to involve and communicate openly with patients and the public.
Measure
Aim Outcome Assurance Mechanism
Date
Develop and promote Being Open Policy through RCA Training
Staff are aware of Being Open
Staff attendance list to be reported onto ESR
On-going provision with Quarterly monitoring
Step 6 Learn and Share Safety Lessons
Whilst the Trust collects and collates data on a range of incidents the Trust knows that the aggregation of this data corporately and in isolation is not particularly useful for comparison or benchmarking.
The Reflecting and Learning from Analysis of Incidents and RCA review panels are specifically being introduced to learn and share safety lessons and to ensure these can be cascaded throughout the Partnership Trust.
Objective
The Incident reporting system will be reconfigured and refined to help promote and provide service level reports that are themed so that services will be able to improve patient safety responsively at the front line.
The Partnership Trust will continue and develop benchmarking reporting with the Community Foundation Trust Benchmarking club.
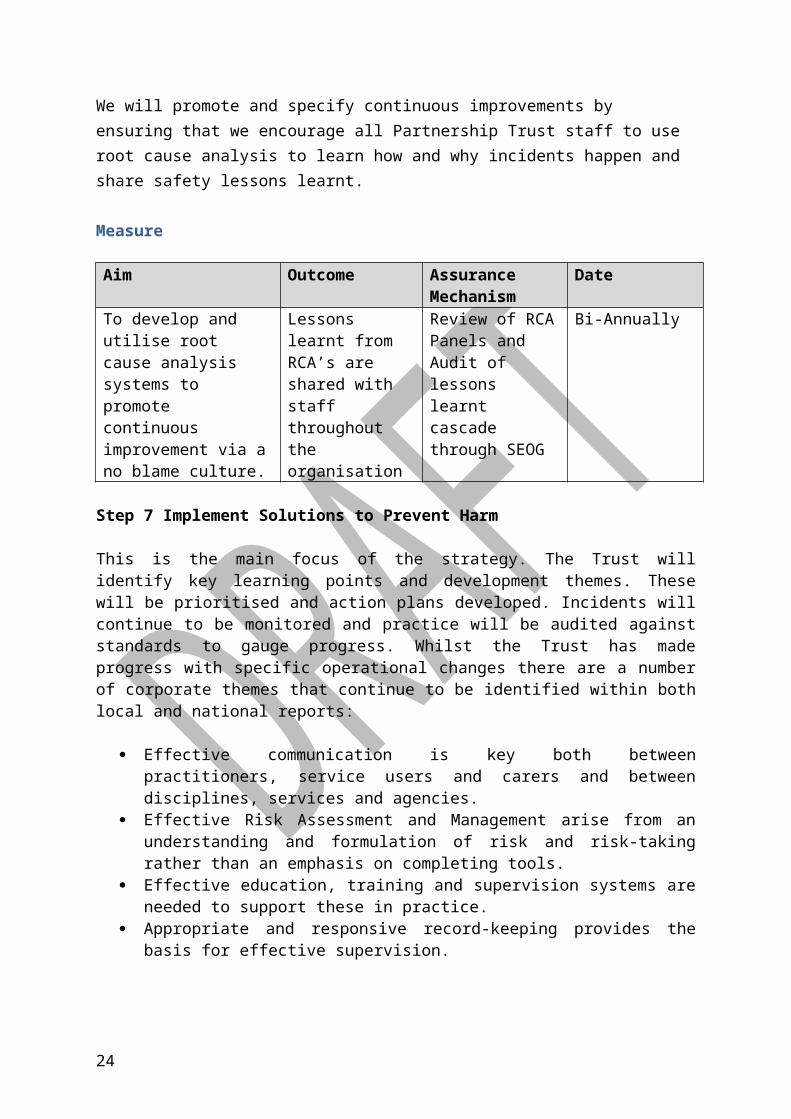
We will promote and specify continuous improvements by ensuring that we encourage all Partnership Trust staff to use root cause analysis to learn how and why incidents happen and share safety lessons learnt.
Measure
Aim Outcome Assurance Mechanism
Date
To develop and utilise root cause analysis systems to promote continuous improvement via a no blame culture.
Lessons learnt from RCA’s are shared with staff throughout the organisation
Review of RCA Panels and Audit of lessons learnt cascade through SEOG
Bi-Annually
Step 7 Implement Solutions to Prevent Harm
17
This is the main focus of the strategy. The Trust will identify key learning points and development themes. These will be prioritised and action plans developed. Incidents will continue to be monitored and practice will be audited against standards to gauge progress. Whilst the Trust has made progress with specific operational changes there are a number of corporate themes that continue to be identified within both local and national reports:
Effective communication is key both between practitioners, service users and carers and between disciplines, services and agencies.
Effective Risk Assessment and Management arise from an understanding and formulation of risk and risk-taking rather than an emphasis on completing tools.
Effective education, training and supervision systems are needed to support these in practice.
Appropriate and responsive record-keeping provides the basis for effective supervision.
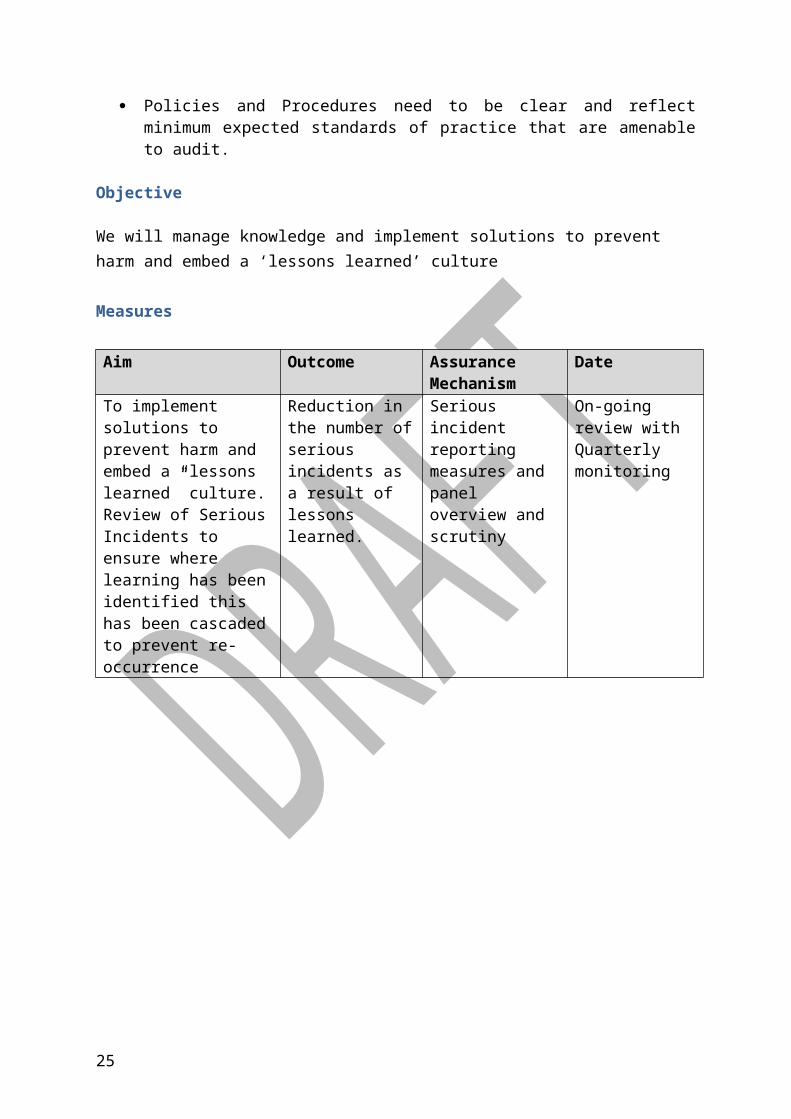
Policies and Procedures need to be clear and reflect minimum expected standards of practice that are amenable to audit.
Objective
We will manage knowledge and implement solutions to prevent harm and embed a ‘lessons learned’ culture
Measures
Aim Outcome Assurance Mechanism
Date
To implement solutions to prevent harm and embed a “lessons learned” culture. Review of Serious Incidents to ensure where learning has been identified this has been cascaded to prevent re-occurrence
Reduction in the number of serious incidents as a result of lessons learned.
Serious incident reporting measures and panel overview and scrutiny
On-going review with Quarterly monitoring
18
6. 2013 / 2014 Priorities
Quality Account Priority
Priority 1: Safety – reducing avoidable pressure ulcers
Our aim: no avoidable grade 2/3/4 pressure ulcers developed in our care.
Pressure ulcers cause patients long term pain and distress. Nationally, the “Safety Express” and “harm free care” initiatives are calling the NHS to build on its quality and safety processes. We recognise that one important aspect of harm free care is the absence of avoidable pressure ulcers.
As defined by the Department of Health: “Avoidable” means that the person receiving care developed a pressure ulcer and the provider of care did not do one of the following:
evaluate the person’s clinical condition and pressure ulcer risk factors; plan and implement interventions that are consistent with the person’s needs
and goals, and recognised standards of practice; monitor and evaluate the impact of the interventions; or Revise the interventions as appropriate.
To ensure specific actions from incidents are captured and cascaded throughout the Partnership Trust, specific panels have been established to scrutinise and identify learning from root cause analysis. Pressure Ulcers reported as serious incidents are presented to a tissue viability panel that has been established which meets monthly for; the review and challenge of root cause analysis reports relating to pressure ulcers, decision of avoidable/unavoidable, closure and lessons learnt.
Community nursing staff and team leaders attend the review panel to learn about the challenge process and the lessons learnt. This allows team leaders to direct audit within their team and to provide operational assurance on the implementation of recommendations and required service changes.
As part of improving our safety culture we want to continue our focus on eliminating all avoidable pressure ulcers for people in our care. Our safety strategy will describe how we will do this.
MeasureKey safety measures for reducing avoidable Pressure Ulcers
19
Measures we will report to our Board
Our current position
Avoidable pressure ulcers (grade 3 and 4) developed in our care and reported as incidents
Last year we reported 41 avoidable pressure ulcers (grade 3 and 4) as Serious Incidents.
Community acquired pressure ulcers (grade 3 and 4) will be reported as incidents.
Last year we reported 134 pressure ulcers (grade 3 and 4) and 37 of these were avoidable.
Hospital acquired pressure ulcers (grade 3 and 4) will be reported as incidents.
Last year we reported 12 pressure ulcers (grade 3 and 4) and 4 of those were avoidable.
All pressure ulcers applicable to care within the Partnership Trust are reported as adverse incidents
Last year we reported 1,063 incidents related to pressure ulcers and we know we need to do more in reducing those numbers reported.
Other measures we will use to track progress
Number of adverse incidents reported Last year we reported 6,140 incidents. We expect incident reporting to continue to rise and be a sign of a strong safety culture.
Percentage of reported incidents classified as serious incidents
281 Serious incidents were reported and equates to 4.6% of all incidents reported. We expect that the percentage of serious incidents will reduce whilst the numbers of incidents increase promoting a strong safety culture.
20
Patient Safety Priorities
Priority 2: Safety Thermometer
“So, the first principle must be ‘do no harm’, When it goes wrong in the NHS, patients suffer and patients die. Safety for patients is at the heart of quality care and if the professional responsibility of nurses and doctors. So there is no trade off between
safety and efficiency”.
Rt Hon Andrew Lansley CBE, MP, Secretary of State for Health, June 2010 (Excerpt from: My ambition for patient- centered care’.
The Partnership Trust monitors the prevalence of harm using the NHS Safety Thermometer (against the 4 key harm; Pressure Ulcers, Falls with injury, Catheter Acquired UTI’s and Venous Thromboembolism (VTE)) within Community Hospitals and Community Nursing services.
The 2013/14 CQUIN Programme includes the NHS Safety Thermometer with a particular focus on reduction in overall pressure ulcer prevalence. The national CQUIN does not distinguish between new and old harms, with an expectation that all harms, regardless of origin will be reduced. The Partnership Trust aims to support other non NHS providers to reduce the incidence and prevalence of pressure ulcers through a structured education programme.
Pressure ulcers are commonly associated with increasing frailty, worsening health and a marker of poor care delivery. A pressure ulcer is described by the European Pressure Ulcer Advisory Panel (EUPAP) as ‘an area of localised damage to the skin and underlying tissue caused by pressure, shear, friction and/or a combination of these’. They typically occur over a bony prominence but can also be associated with the use of devices such as oxygen tubing (ears/nose), urinary catheters and indwelling intravenous lines to other areas of the body. Although more commonly found in elderly and frail individuals with long- term conditions, illness also increases risk factors which influence development at any age.
Within NHS services there has been a drive to eliminate all avoidable pressure damage, led by the former Chief Nursing Officer; Chris Beasley through the High Impact Actions for Nursing and Midwifery programme (2009). Since that time there has been a significant focus on and success in reducing, particularly, Grade 3 and 4, pressure damage within NHS care however the impact of this programme on the Care Home services has been less well documented.
Care homes, both Residential and Nursing, typically provide services to the most frail and vulnerable individuals in society, the majority of which are in the older age
21
group. Care homes are required, through their registration with the Care Quality Commission (CQC) to provide safe standards of care to those using their services. The complexity of those individuals using Care Home services can pose challenges to some providers, particularly in ensuring that their employees are suitably educated to meet the changing needs of their clients.
There are a number of key factors which may influence skin break down in addition, but not necessarily unrelated to, the individual’s physical and mental health; these include:
Factors that impact on an individual’s ability to move or change position Nutrition and hydration status Continence issues resulting in skin contamination
Key safety measures for Safety Thermometer
Measures we will report to our Board
Our current position
NHS Safety Thermometer
The data is collected monthly using a point prevalence audit methodology in line with guidance from the Department of Health.
The median Harm Free Care for the year March 2012 – March 2013 is 90.24% (range 87.92 – 92.62%) with the median No New Harm over the same period being 96.22% (range 95.46 – 97.34%). The aspirant direction of travel for Harm Free Care for the Partnership Trust is to be 95%
Pressure ulcer prevalenceThe current national (median) pressure ulcer prevalence is 6.6%
The pressure ulcer prevalence (median for previous 6 months) for the Partnership Trust was 6.9%. A reduction of 0.4% over 2013/14 has been proposed, phased over two 6 month periods.
Aim
The Partnership Trust will develop a two day programme addressing these factors which will support non NHS staff working in care home settings to identify those who are likely to be at risk of pressure damage and provide them with tools to put in place immediate preventative measures as well as give them key contacts where expert support and help can be sourced.
Measure
22
The two day programme developed by the Partnership Trust will support staff working in care home services in the prevention and management of pressure ulcers.
The programme will be delivered during October & November 2013 (day 1) and February & March 2014 (day 2) across the whole health economy. The Care Home providers peak activity/staffing challenges which typically occur during the summer months and around Christmas/New Year will be avoided. The programme will be delivered across Stoke on Trent, Newcastle under Lyme, Moorlands, Cannock & Rugeley, Burntwood, Lichfield & Tamworth, Stafford & Surrounds and the Seisdon peninsular (including Wombourne & Kinver). Venues are being sources across the health economy with the aim that these will be located in care home settings.
Day 1 Accountability & Safeguarding Assessment of Pressure Ulcer Risk Skin Inspection The SSKIN Bundle Assessment Tools
Day 2 Recap on Day 1 Nutrition Continence Pressure Ulceration and the Lower Limb and the Foot Equipment & Specialist Support Audit and Standards
Assurance Mechanism
The programme will be co-ordinated through the Workforce & OD Department and delivered by specialist teams/leads in Tissue Viability, Continence, Dietetics and Podiatry and supported by the Professional Leadership team.
Outcome
The programme is aimed at care Home Managers and Senior Care Workers so that change within individual organisations can be facilitated, thus reducing harm to service users. It is anticipated that this two day programme will initiate closer working practice between the Partnership Trust and Care Home providers.
Priority 3: Reducing Harm from Falls
23
To reduce the number of falls and the number of serious incidents associated from falls within in care.
Aim Outcome Assurance Mechanism
Date
24
7. ImplementationOverall approach to implementation
The Nursing and Quality Directorate will coordinate this annual strategy and the key priority areas for each year. The plan will contain actions shared across other directorates. The implementation of this strategy will:
form the basis of the patient safety strategy for 2013-2014 and will sit will be linked to the Efficiency and Patient Experience strategies by the overarching Quality Framework.
form the basis of a phased approach for subsequent years, ensuring progress against each of the theme areas while maintaining in-year flexibility for responding to quality issues
Supporting strategies and work streams for implementation
Key strategies and work streams to implementation, which will be developed by the Quality Directorate, are:
Safety Strategy Effectiveness Strategy Experience Strategy Quality Assurance Programme
Supporting strategies and work streams above provide detail on policies, systems and processes that will be developed or refined to achieve the six quality goals in this framework.
25
8. MonitoringMonitoring the implementation of the Safety Strategy under the Quality Framework
The safety strategy will be submitted to the Quality Governance Committee and thereafter will be monitored under Safety and Effectiveness Operational arrangements which are currently being formulated.
Monitoring the quality of care
Monitoring of the quality of care will take place primarily using the Quality Early Warning Intelligence System1 on a monthly basis at a team level. This system will be developed to provide regular tracking of performance relative to the Quality Goals in this framework.
Each year the Trust will produce a quality account, in parallel with the annual report and financial accounts.
After consulting and involving staff, service users and carers we will draw the priorities for each year’s quality account from this framework.
Consultation around the Quality Framework which is the overarching strategy for the Safety, Patient Experience and Effectiveness strategies has been undertaken and comments noted and acted upon. The Safety Strategy will be sent to Professional Leads for consultation and will also go to The Community Health Equalities Network.
The Safety Strategy will feed into the Quality Framework annual report will summarise the progress that has been made in implementing the framework.
Quality is monitored by the Board on a monthly basis, and the strategy will be driven by the Quality Governance Committee. – Documents will be shared with Professional leads as part of agreement of strategy.
9. Review
1
26
Supporting Documents
Risk Management Strategy
Risk Management Policy and Incident Report Writing Pack
Being Open Policy
Training and Development Policy
Supporting Staff Policy
Whistle blowing -Raising Concerns at work
Education and Training
Induction Policy
Integrated Business Plan
Quality Account
Quality Framework (2013-1018)
Development Plan
Claims Management Policy
27


















