Spondyloarthropathies & FMF+

of 18
-
Upload
rashed-shatnawi -
Category
Documents
-
view
225 -
download
0
Transcript of Spondyloarthropathies & FMF+
-
8/18/2019 Spondyloarthropathies & FMF+
1/18
30
Spondyloarthropathies & FMF
Khaldoon Alawneh
Zaid Zreigat
10 / 12 / 2009
-
8/18/2019 Spondyloarthropathies & FMF+
2/18
1
Spondyloarthropathies
Spondyloarthropathies “as the name implies” are diseases affecting primarily
the spine(vertebrae) . May affect other organs (the peripheral joints and other
organs ).
“The famous” Spondyloarthropathies is : Ankylosing Spondylitis…like when yousay connective tissue disease the first that crosses your mind is SLE or when you
say arthritis the first thing that crosses your mind is Rheumatoid Arthritis.
Spondyloarthropathies share similar characteristics :
They affect the spine (Inflammatory axial spine involvement )
Asymmetrical peripheral arthritis while in Rheumatoid Arthritis and SLE
it’s symmetrical arthritis
Enthesopathy (Inflammation of the insertion of the tendons )
Inflammatory eye disease another common feature
Mucocutaneous features
Rheumatoid factor negative: this is used to differentiate between
Spondyloarthropathies and rheumatoid arthritis
High frequency of HLA B27 Antigen
Familial aggregation : all the rheumatic diseases have familial aggregation
Rheumatoid factor negative doesn’t exclude rheumatoid arthritis,, and it was a
rare case of rheumatoid factor positive it doesn’t role out
Spondyloarthropathies… but those were the common features.
One of our colleagues asked about Rheumatoid arthritis: Doesn’t Rheumatoid
arthritis as a disease has spinal involvement ?
Rheumatoid arthritis typical affect the cervical vertebrae and mostly the upper
part of the cervical spine, while in Spondyloarthropathies, there is a progressive
involvement of the spine besides the primary disease is within the spine.
Spondyloarthropathies include: Ankylosing Spondylitis, Psoriatic Arthritis,
Reactive Arthritis, Reiter’s syndrome(Which is a form of reactive arthritis ),Enteropathic Arthritis (associated with Ulcerative colitis and Crohn’s) , Juvenile
Ankylosing Spondylitis.
-
8/18/2019 Spondyloarthropathies & FMF+
3/18
2
HLA B27 Association :
Ankylosing Spondylitis : characteristics of Back Pain
It’s a disease of young age…most people present before the age of 40 ,
therefore the criteria of Ankylosing Spondylitis is that the onset of the
disease happens before the age of 40, gradual onset, duration is longer than
3 months , associated with morning stiffness, decrease with exercise (
inflammatory back pain)
There are two types of back pain : Inflammatory and mechanical
In the inflammatory type the pain improve with exercise like in the case of
Ankylosing Spondylitis….in the mechanical type the pain worsen with exercise like
Disk disease
So in osteoarthritis the pain improves at rest and worsen on activity…while in
inflammatory arthritis like Ankylosing Spondylitis the pain improves withexercise..the patient wakes up stiff (one piece) in the morning, with time 1-2
hour the patient gets better with activity, if he/she rests again in the afternoon
the patient become stiff again!
A Colleague asked about Lambert-Eaton Syndrome concerning pain relief after
exercise.
Lambert-Eaton syndrome to differentiate it from Myasthenia Graves :
Both are muscle diseases ( explained in previous lectures)..in Lambert-EatonSyndrome the patient improves with exercise while in Myasthenia Graves the
patient’s condition worsen with exercise that they need rest or sleep to improve.
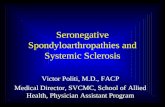
The highest association is with
Ankylosing Spondylitis….this figuregives you a idea about HLA
association.. as you can see
Reactive Arthritis has a high
association with less association in
the case of Inflammatory Bowel
Disease
-
8/18/2019 Spondyloarthropathies & FMF+
4/18
3
New York criteria for diagnosis of Ankylosing Spondylitis :
1.
limited lumber motion
2.
Lower back pain for three months, improve with exercise, not relieved by
rest
3. Reduced chest expansion
4.
bilateral ,grade 2 to 4, sacroiliitis on x-ray
5. unilateral ,grade 3to 4, sacroiliitis on x-ray
The important thing to know is with Ankylosing Spondylitis the age group is young
age group with inflammatory back pain with 3 months duration, reduced chestexpansion ,with sacroiliitis on x-ray the grading ( grade 2-4 bilateral/3-4
unilateral ) isn’t that important to us.
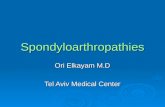
In this figure we can see a typical case of AnkylosingS pondylitis…spine became one piece !! and the neck is
affected.
Usually in Ankylosing Spondylitis clinically starts inthe lower region of the back then goes upward until the
patient’s back becomes “one piece”…when the patient
tries to flex his back it moves like it’s one piece.. when
we want to flex our backs we use our spine with a little
help from the hips…this patient can use his hips only
to bend his back as u can see in the picture… he can’t bend without the hips!!
-
8/18/2019 Spondyloarthropathies & FMF+
5/18
4
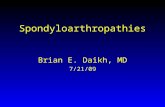
In this figure we can c a patient with Ankylosing Spondylitis and the
progression of the disease(from left to right) in the second picture we can se
that he began to show signs and then it got worse that his back became “one
piece” (the 3rd picture) and then he even lost the usage of his hips and his hips
also became fixed (the 4
th
picture) and then he got better due to hipreplacement his body became “straight” again. So as we can see in Ankylosing
Spondylitis after the spine eventually the joints become affected and the
common sites the large joint (hip joint in this case) .
Spondyloarthropathies : Nonvertebral Symptoms
1. Asymmetrical Peripheral Arthritis
2.
Arthritis of the Toe Interphalangeal joints
3. Sausage Digits : in Rheumatoid arthritis the inflammation is limited to the
joint….but in Ankylosing Spondylitis the inflammation is not restricted to
the joint only it affects the ligaments around the joint...and the whole digit
becomes bigger like a Sausage because the whole digit is inflamed.
4.
Achilles Tenosynovitis: is the inflammation of the fluid-filled sheath (called
the synovium) that surrounds Achilles tendon.
5. Plantar Facsiitis : inflammation of the Plantar Fascia associated with pain.
6. Costochondritis*: eventually the costochondrial joints (articulations
between the ribs and the costal cartilage) they become fused and there will be
no chest expansion
*Costochondritis : inflammation of one or more costal cartilages, characterized by localtenderness and pain of the anterior chest wall that may radiate, but without the local
swelling typical of Tietze syndrome.
http://en.wikipedia.org/wiki/Inflammationhttp://en.wikipedia.org/wiki/Fluidhttp://en.wikipedia.org/wiki/Synoviumhttp://en.wikipedia.org/wiki/Tendonhttp://en.wikipedia.org/wiki/Tendonhttp://en.wikipedia.org/wiki/Synoviumhttp://en.wikipedia.org/wiki/Fluidhttp://en.wikipedia.org/wiki/Inflammation
-
8/18/2019 Spondyloarthropathies & FMF+
6/18
5
7. Iritis : which is uveitis (inflammation of the uveal tract: iris, ciliary body, and choroid)
8. Mucocutaneous Leasions
Recurrent Iritis caused Synechiae(adhesions
between the lens and iris : in this figure we seerecurrent uveitis with irregular pupil…. typically
anterior uveitis happen in Ankylosing Spondylitis
while in Bechet’s disease the most common is
posterior uveitis which is very bad…so here we
see anterior uveitis with conjunctivitis and the
pupil becomes irregular because of the posterior
adhesions
Early Sacroiliitis : here the sacroiliac
joint is inflamed eventually this joint will
disappear but early there will be sclerosis
then there will be irregularity the join will
disappear
Advanced Sacroiliitis ,Fused Sacroiliac
joints: here we cant detect any joint it’s
completely fused even the vertebrae looks
fused too
Syndesmophytes(an outgrowth of bone
attached to a ligament),
apophyseal(outgrowth of bone) joint
fusion,disc peripheral
ossification(Ankylosing Spondylitis):
Here we can see calcification of the
ligament due to chronicinflammation…eventually the whole spine
becomes calcified
-
8/18/2019 Spondyloarthropathies & FMF+
7/18
6
Ankylosing Spondylitis.
Left:squaring of vertebra,
Right:anteriorlongitudinal ligament
calcification : we can see
calcification around the discs (left)
and calcification around the
anterior longitudinal ligament
Ankylosing Spondylitis :Bamboo spine
,ossification follow the contour of
intervertebral discs : here we see that the
disease is more advanced we can’t
differentiate between the vertebrae…thereare calcifications around the lateral ligaments
and around the posterior and anterior
ligaments…so calcification all around the
vertebrae eventually they’ll have a square
shape and they call it bamboo spine
Ankylosing Spondylitis:calcaneal (related to
calcaneus bone) spur(a spine or projection
from a bone) and erosion: we said that
plantar fasciitis is one of the symptoms we
can see inflammation of the plantar fascia
it’s associated with pain. Also the Achilles
tendon could be damaged… we can see a
calcaneal spur(ر س) (notice the arrow)partof plantar fasciitis is the projection of the
spur but this is not the problem, the
problem is that there’s an inflammation in
the whole fascia.. Sergeants in the past
used to remove this spur but the result
wasn’t as good as expected
-
8/18/2019 Spondyloarthropathies & FMF+
8/18
7
Reiter’s Syndrome : like we said before it’s a form of reactive arthritis
Reiter’s Syndrome is associated with :
1. Inflammatory Eye Disease ( like in Ankylosing Spondylitis )
2.
Balanitis (inflammation of the glans penis or the clotiris ) .Oral Ulceration
or keratoderma
3.
Enthesopathy
4.
Sacroiliitis
So there are some similarities but the skin lesions in Reiter’s Syndrome
different
Apical fibrosis in Ankylosing
Spondylitis : Lung fibrosis could
occur in Ankylosing Spondylitis
There are some similarities between Reiter’s
Syndrome and Ankylosing Spondylitis….but thereare some special criteria for Reiter’s Syndrome..
Patients are presented with Urethritis or
Cervicitis associated with gonorrhea or with
other diseases that can activate reactive
arthritis or Reiter’s Syndrome like Chlamydia or
gonorrhea like we said…other criteria is
Infectious Diarrhea: typical Reiter was
infectious Diarrhea not renal tract infection….
Like in Ankylosing Spondylitis
-
8/18/2019 Spondyloarthropathies & FMF+
9/18
8
Then the doctor told a story about a patient he treated : a female in her
thirties she complained of Fever, Back Pain and Skin rash like the previous one..
Doctors thought that this is Urosepsis a pseudomonas infection but the urine
culture always came back negative with high WBC count because of the
Urethritis , they gave her antibiotics and NSAIDs and she improved because if
she got infection in the urinary tract it’ll improve with antibiotics and the
NSAIDs that happened several times…when she came to Dr. Alawneh they took
an x-ray and it showed bilateral sacroiliitis and extensive changes in her
spine..not even one time she had a documentation of her having an infection and
the rash that the doctors thought that it was a Urosepsis and an infection wasindeed a part of the disease she had ( Reactive Arthritis ) the doctor gave her
immunosuppressant and she did well and still doing well for 3 years now =)
As we said the infectious bacteria that causes
urinary tract infection in Reiter’s Syndrome
mainly gonorrhea and on top of that another
Urogenital infection could take place like
Chlamydia trachomatis and Ureaplasma …in thegastrointestinal tract Yersinia, Salmonella
,Shigella and Campylobacter can trigger
reactive arthritis the same in the case of
Chlamydia Pneumoniae in the respiratory tract
infections .
Reiter's heel tendonitis: here we can see
swelling of the Achilles Tendon insertion.. Thisswelling can be seen clinically as an
evidence…this swelling happens to be tender, a
severe inflammation in the insertion occur that
leads to rupture of the Achilles Tendon
Reiter's pustules ( a small, circumscribed elevation of
the skin, containing purulent material.) : this rash is
common and it’s a classical rash for Reiter’s
Syndrome
-
8/18/2019 Spondyloarthropathies & FMF+
10/18
9
Reiter's
Keratoderma
blenorrhagica:
This is another rash
that comes withReiter’s
Reiter's:Pustules+
Keratoderma
blenorrhagica :
This is a more
aggressive rash
Reiter's Balanitis circinata:
This genital rash is different
from the genital rash in
Bechet’s disease which is more
on the scrotum
Reiter's tongue lesion:
Like in Bechet’s and SLE oral
ulcers happen in Reiter’s
Syndrome
Reiter's palate erosion:
This is a more extensive oral ulcer that involves
the palate…if u had a patient with these kind of
ulcers and back pain think about Reactivearthritis
Reiter's syndrome conjunctivitis:
Here’s one of the eye manifestation in Reiter’s like in
Ankylosing Spondylitis…but the difference between
Reiter’s and Ankylosing Spondylitis is that in Reiter’s
it’s more conjunctivitis than anterior Uveitis butReiter’s can cause Anterior Uveitis..also Bechet’s and
Rehumatoid arthritis can cause these manifestations
-
8/18/2019 Spondyloarthropathies & FMF+
11/18
10
Nail dystrophy seen in Reiter's and
psoriasis:
Psoriasis is one of the Spondyloarthropathies
So you can see nail abnormalities in Reiter’s
and in Psoriasis
Asymmetrical Sacroiliitis(more common in
Reiter's ):
As you can see in Reiter’s patients have
Sacroiliitis like in Ankylosing Spondylitis but
in Reactive Arthritis it’s more a symmetrical
one side is more affected than the other or
unilateral on the contrary in Ankylosing
Spondylitis it’s a more aggressive disease
and the Sacroiliitis is bilateral
Plantar periostitis seen in Reiter's(also seenin Rheumatoid Arthritis Ankylosing Spondylitis
, and Psoriasis) :
Here the calcaneal spur is more obvious than it’s
in the previous one …. Notice in Rheumatoid
Arthritis there’s arthritis but without any bone
reaction on the contrary in
Spondyloarthropathies there will be an extensive
bone reaction on the periosteum so we’ll see
inflammation of the periosteum.
The summery of this slide is that Psoriatic
Arthritis can mimic other arthritis including
Rheumatoid Arthritis.. sometimes patients may
present with symmetrical arthritis like in
Rheumatoid Arthritis without any rash (it’s
delayed) 2-3 months/year after presentation
patients get the rash so these patients may bediagnosed as Rheumatoid Arthritis patients then
the diagnosis is changed after the rash appear!!
-
8/18/2019 Spondyloarthropathies & FMF+
12/18
11
Other Clinical Characteristics of Psoriatic Arthritis :
1. No rheumatoid nodules
2. Rheumatoid Factor (RF) Negative although patient’s may present with signs
and Symptoms like in Rheumatoid Arthritis.
3. Inflammatory Arthritis in Distal InterPhalangeal joints : the patient may come
only with this complication like in Gout
4. Asymmetrical Arthritis : arthritis in one side or in one side more than the
other
5. Spondylitis Sacroiliitis often asymptomatic
6. Arthritis Mutilans : severe extensive arthritis with destruction (characterizedby resorption of bones and the consequent collapse of soft tissue. When this affects
the hands, it can cause a phenomenon sometimes referred to as "telescoping fingers.")
7. sausage digits
8. nail pitting or onycholysis (loosening of the nails, beginning at the free border, and usuallyincomplete)
9. syndesmophytes (an osseous excrescence attached to a ligament.)
10. paravertebral ossification
11. Enthesopathy
Most of these characteristics are characteristics of Spondyloarthropathies
Patterns of Arthritis in Psoriasis :1.
Spondylitis : Sacrloiliitis with progression to the spine
2. Distal Interphalangeal Joint Arthritis
3. Oligoarticular Asymmetrical Arthritis
4. Polyarticular(involving many joints) Symmetrical Arthritis : like in
Rheumatoid Arthritis
5.
Arthritis Mutilans : as we said before it’s very sever destruction and the
bone of the Joint completely disappear
-
8/18/2019 Spondyloarthropathies & FMF+
13/18
12
Psoriatic arthritis ,rash, nail dystrophy,
sausage digit : notice the diffuse swelling in
the phalanges not localized swelling like in
Rheumatoid arthritis…you can see nail
dystrophy, Distal Interphalangeeal jointsaffected and rash so this is psoriasis
Psoriatic arthritis:rash,nail dystrophy,and
arthritis :
Here you can see that the Distal
Interphalangeal(DIP) joints is affected and
skin changes so this is Psoriasis
Psoriatic arthritis affecting DIPs , PIPs
,sausage digit, no rash :
This is a more severe presentation…notice the
shortening of the fingers because the bone is
destroyed (resorbed) so when an x-ray is takenthere will be no bone . Psoriasis can cause Swan
Neck fingers like in Rheumatoid Arthritis
Psoriasis nail dystrophy and arthritis:
This a closer image showing nail dystrophy
( progressive changes that may result from defective
nutrition of a tissue or organ) and arthritis. So
what’s important in psoriasis is nail and/or skin
changes + Arthritis and on top of that Distal
Interpharangeal joints are affected +
sacroiliitis which are not included in the case of
Rheumatoid Arthritis
Psoriasis nail pitting :
There’s no pitting in normal nails “everybody
should check his/her nails for pitting” ,the
doctor said!! Because Psoriasis isn’t anuncommon disease 2% of people suffer from
Psoriasis
-
8/18/2019 Spondyloarthropathies & FMF+
14/18
13
Dactylitis ( inflammation of one or more fingers )
in psoriatic arthritis :
Here the whole digit is inflamed this doesn’t
happen in Rheumatoid Arthritis …other causes
of dactylitis: like in babies for example one
year old baby with dactylitis can be caused byan infection, TB can cause Dactylitis
Psoriatic arthritis : soft tissue swelling,joint
destruction,erosions
DIPs,PIPs,MCPs( metacarpopharangeal ) :
This is an x-ray for a patient with psoriatic
arthritis we can see that the bone disappeareddue to severe destruction..and we can see the
over reaction of the bone due to severe
periosteal reaction while in Rheumatoid
Arthritis there’s no reaction the patient x-ray
Progressive joint changes in Psoriatic
Arthritis(pencil in cup):Here we can see the DIPs are affected, like
we said before in Rheumatoid Arthritis DIPs
aren’t affected, with time and progression
of the disease the joints look like a pencil in
a cup as u see in C (
ر ص
قم
ثل
)
Psoriatic arthritis severe changes in
DIPs,less in PIPs and minimal in MTPs :
Here again we an see that Distal
Interphalangeal joints are affected the
most in psoriasis to a less extent Proximal
Interphlangeal joints with minimal
changes in the Metacarpophrangeal joints
-
8/18/2019 Spondyloarthropathies & FMF+
15/18
14
Treatment Of Psoriatic Arthritis :
We won’t go into details of the treatment of Psoriatic Arthritis, it’s very similar
to the treatment of Rheumatoid Arthritis ,
The main drug for treatment is Methotrexate which is beneficial to the skin
and joints (used to treat Ankylosing Spondylitis also )
Anti TNF Drugs like infliximab , etanercept and adalimumab that block the TissueNecrosis Factor, they are useful both in the psoriatic skin changes and psoriatic
Arthritis also they are affective in the Treatment of Ankylosing Spondylitis
Prevent eye complications by early recognition and treatment
Treat symptoms with NSAIDs
Physical therapy, stretching and exercises to preserve spine and joints
function
Maintain good posture
Be aware of association between Spondyloarhtropathies and other diseases
Inflammatory bowel disease
Aortitis, aortic regurgitation(in ankylosing spondylitis 1%)
Inflammatory eye disease
Pulmonary fibrosis in ankylosing spondylitis 1%
Severe reactive arthritis and HIV :there is a Severe reactive Arthritis in the
HIV
http://en.wikipedia.org/wiki/Infliximabhttp://en.wikipedia.org/wiki/Infliximabhttp://en.wikipedia.org/wiki/Etanercepthttp://en.wikipedia.org/wiki/Adalimumabhttp://en.wikipedia.org/wiki/Adalimumabhttp://en.wikipedia.org/wiki/Etanercepthttp://en.wikipedia.org/wiki/Infliximab
-
8/18/2019 Spondyloarthropathies & FMF+
16/18
15
FMF( Familial Mediterranean Fever)
This disease is important in our area, it’s rare in other parts of the world.
“Back in the days the patients presented to the hospital with abdominal pain
,one of the manifestations of this disease, fever and the WBC’s count elevated.
These patients go to the surgeon who suspects Appendicitis or Cholecystitis
then he/she removes the appendix the first time, the problem is still there, the
next time the gall bladder will be removed. The third time the patients came
with intestinal obstructions due to surgical adhesions so they go under
laparotomy (a surgical procedure involving an incision through the abdominal
wall to gain access into the abdominal cavity). Because back then there was noCT scan, so the surgeon to protect himself and the patient had to open the
patient up, nowadays CT scan is available and we can do laproscopy to diagnose
the disease”
SO FMF :
Is an Autosomal recessive disease
Characterized by attacks of Serositis (refers to inflammation of the seroustissues of the body, the tissues lining the lungs (pleura), heart (pericardium),
and the inner lining of the abdomen (peritoneum) and organs within) and fever
patients come with abdominal pain /chest pain or joint pain , and rarely with
pericarditis
Attacks are acute and sudden last from 6-96 hours
First attack before age 20 in 90% of the cases
Clinical Characteristics :
Abdominal pain in 95% mostly as acute abdomen and peritonitis but some times
mild
Mono arthritis with effusion in 75%, mostly knees, ankles or wrists.
Chest pain/ pleuritis (unilateral)30%
Pericarditis rare 1% Above symptoms with fever or may be fever alone
http://en.wikipedia.org/wiki/Surgeryhttp://en.wikipedia.org/wiki/Abdominalhttp://en.wikipedia.org/wiki/Abdominal_cavityhttp://en.wikipedia.org/wiki/Inflammationhttp://en.wikipedia.org/wiki/Lungshttp://en.wikipedia.org/wiki/Pleurahttp://en.wikipedia.org/wiki/Pericardiumhttp://en.wikipedia.org/wiki/Peritoneumhttp://en.wikipedia.org/wiki/Peritoneumhttp://en.wikipedia.org/wiki/Pericardiumhttp://en.wikipedia.org/wiki/Pleurahttp://en.wikipedia.org/wiki/Lungshttp://en.wikipedia.org/wiki/Inflammationhttp://en.wikipedia.org/wiki/Abdominal_cavityhttp://en.wikipedia.org/wiki/Abdominalhttp://en.wikipedia.org/wiki/Surgery
-
8/18/2019 Spondyloarthropathies & FMF+
17/18
16
So the WBC’s Count and ESR during the attack will be elevated ( inflammatory
process without infection )…so all the acute phase proteins are elevated and the
patients present like peritonitis and the patient will jump if you touch her/his
abdomen…..the good physician is the one who takes good history and knows
about any previous attacks, takes family history because like we said it’s an
autosomal recessive disease other member maybe affected
Genetics of FMF :
Gene responsible has been located in short arm of chromosome 16
MEFV gene encodes protein (pyrin, marenostrin)
Pyrin gene mostly in cytoplasm of neutrophils or monocytes /regulateinflammation
There was 28 mutation now theirs is more than 50 mutations, some people are
presented with no mutations, the have the original disease without any
mutation we know , most common mutations M694V and V726A
M694V associated with more severe disease and higher risk of amyloidosis (any
chronic inflammation can trigger amyloidosis and eventually renal failure )some patients of FMF without treatment are on dialysis now
This is chromosome 16 with the most common mutations. Notice that the
M694V mutation we talked about that’s associated with amyloidosis is present
on location 10 on Chromosome 16
-
8/18/2019 Spondyloarthropathies & FMF+
18/18
17
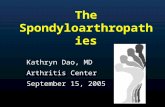
This chart shows the typical presentation of FMF patients they have fever
which decreases with time, abdominal pain, vomiting, and constipation typicalperitonitis like picture
Treatment :
Colchicine ,whish is a very good drug for treatment of FMF , is used to abort the
attack ( abort the attack in 60% of the cases and it modifies 20-30% of the
cases ) but sometimes Colchicine is not enough to abort the attack so we useNSAIDs with it, in a matter of fact NSAIDs are better in aborting the attack
but Colchicine is good to prevent the attacks and to prevent Amyloidosis
THE END
Done By : Zaid ZreigatFirst of all I’m very sorry for being sooo laaatee, I hope It didn’t affect anyone’s
studying
A7la salam la group il ba6ini group A 2o akeed ba5os bil thikir group A10.. my group :7amzeh Rsheidat, Mo3taz Mwafi, Ra2ed Abu 5ai6, 3omar Borini, m7amad 86ai6,
‘3aith 3a6eyeh , Muhanad 3beidat , Ma2moon Hdaib , Waleed abu Sale7, Jad
3abd il Sattar 2o akeed sabaya A 10 =p Noor 2o Tamam 2o Rand 2o Amani 2o
3abeer 2o Ala2
2o a7la ta7yeh la 7usam haddad , Ra3ed 6ahat ( asef jiddan sa3adet il na2eb =p)
,Anas Wardat,M7amad kleib, Ayham ba6ayneh, Rasheed Janaydeh, 3abdallah Bani
Fares , Firas 63ani,Areej Hassan
A2saf itha nseet 7ada 2o ana asef marra thanyeh 3ala il ta25eer
GOOD LUCK FOR ALL IN THE OSCE =)
www sawa2006 com