
Spine Symposium 2016 BACK PAIN IN CHILDREN & … fileHNP 9. Juvenile ankylosing spondylitis 10.Deg...
84
Spine Symposium 2016 BACK PAIN IN CHILDREN & ADOLESCENTS: More common than you think! John P. Lubicky, MD Department of Orthopaedic Surgery
Transcript of Spine Symposium 2016 BACK PAIN IN CHILDREN & … fileHNP 9. Juvenile ankylosing spondylitis 10.Deg...

Spine Symposium 2016
BACK PAIN IN CHILDREN
& ADOLESCENTS:
More common than you think!
John P. Lubicky, MD
Department of Orthopaedic Surgery

Back Pain in Adults
• World statistics show that 60
to 80% of adults will
experience BP at least once
and it will become chronic in 5
to 10%.
Adult Office Visits 1989/90
1. Hypertension 5.5%
2. Pregnancy care 5.2%
3. General exam 4.1%
4. Acute URI 3.3%
5. Back Pain 2.8% (15
million visits, possibly
as high as 4.5%)
6. Depression,anxiety,n
eurosis 2.7%
7. Diabetes 2.6%
8. Cancer 2.2%
9. Degenerative joint
disease 2.1%
10.Acute LRI 2.0%
Hart et al 1995
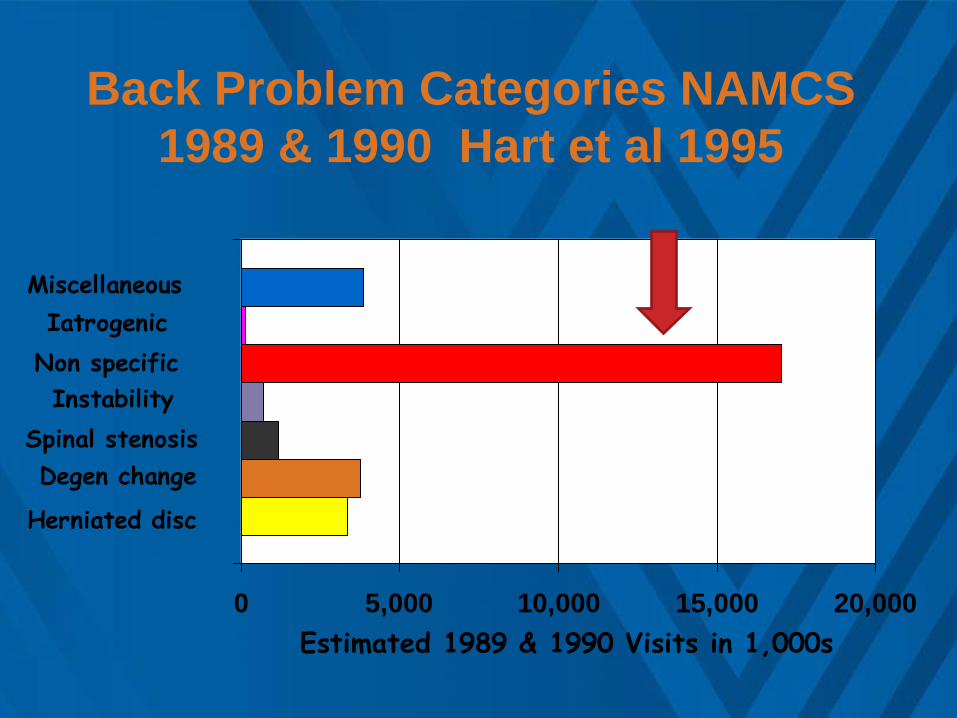
Back Problem Categories NAMCS
1989 & 1990 Hart et al 1995
Herniated disc
Degen change
Spinal stenosis
Instability
Non specific
Iatrogenic
Miscellaneous
0 5,000 10,000 15,000 20,000
Estimated 1989 & 1990 Visits in 1,000s

How serious is back pain in childhood
and adolescence ?
What is its frequency?
Kids now know the pain scale!
For the vast majority of complainers no
objective abnl are ever found
Back Pain in Children
Back pain is an uncommon but serious
complaint in children and almost always has an
identifiable etiology
which is usually really serious
Old and Incorrect Textbook Teaching
Back Pain in Children NEW TEACHING
Back pain has become more & more common
as a CC w/o + findings of any kind
Body habitus – variable
Families demand million dollar W/U
Kids now know the pain scale!
Back Pain in Children
• Common complaint in children and adolescents
• Increases with age and is recurrent
• True prevalence is not well recognized (20-70 lifetime%)
• Frequently either over or under investigated
• Parents/families - may be enablers or seeking reassurance

Annual Incidence of BP associated with secondary
school life during ages 11+ to 15+ yr Burton 1996
12 13 14 15 0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
Child's Age (years)
11.8% 9.8%
14.6%
21.5%
Back Pain in Children
• Lifetime Prevalence 13 to 51%
• Point Prevalence 1 to 33%
• Recurrent Prevalence 7 to 27%
• Sought Treatment 8 to 16%
• Interfere sch/leisure 7 to 27%
Jones 2004

Duration of LBP by Age for Boys with LBP
Taimela 1997
23%
47%
70%
30%
23%
20% 47%
30%
10%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
9 10 11 12 13 14 15 16Age (years)
Recurr/chroni
c
< 1month
< 1week

Back Pain in Children
1. Normal life experience (NSMLBP)
(? MusculoliNgamentous or
lordotic mechan.)
2. Pars interarticularis
pathology
3. Tumors
4. Intraspinal pathology
5. Scoliosis
6. Scheuermann’s
kyphosis (Atypical lumbar)
7. Discitis/osteomyelitis
8. HNP
9. Juvenile ankylosing
spondylitis
10.Deg Disc Disease
11.Minor fxs/anomalies
Etiology

Etiology of LBP (Turner ‘89)
• Spondylolysis 13%
• Infection 8%
• Tumor 6%
• Disc problem 6%
• NSMLBP 50%
Causes of NSMLBP
1. Anthropometry
1. Height
2. BMI
2. Lifestyle factors
1. Physical activity
2. Sedentary activity
3. Mechanical load
1. School bag
4. Psychological
a) Negative affect and psychosocial experiences Balague 1995/Brattberg 1994
b) Conduct/Emotional issues Watson 2003
c) Other psychosomatic sxs Vikat 2000/Jones 2003
Does LBP in Childhood
Predispose to LBP in Adulthood ?
BP in the growth period and familial
occurrence of back disease are
important risk factors for BP later in life,
with an observed probability of 88% if
both factors are present. No correlation
with x-ray changes as adolescents.

Non Specific Mechanical LBP
There is good evidence that children with BP
are more likely to report negative psychosocial
experiences, and there is some evidence to
support the hypothesis that such negative
experiences predict those at high risk of future
onset of LBP
Jones 2004

Back Pain in Children
• Younger children have difficulty
localizing their pain
• Important information includes nature of
onset, duration, frequency, severity,
aggravating and relieving factors,
associated systemic complaints, when
does it occur and presence of leg or
buttock pain
History

Back Pain in Children
• Essentially identical to that in an adult
• Stiffness or significant limitation of motion is
more problematic than in the adult
• Fever, marked tenderness, or neurological
abnormality all indicate a more serious
underlying etiology
Physical exam
Mechanical LBP
• Pain in lumbar area only
• Variably provocative
hyperextension/flexion pain
• Extension contracture of LS spine
• can’t touch toes
• secondary thoracic kyphosis
Micheli 1995

Back Strain
• Tender over the muscle
• Pain on provocative stretching
• Acute onset
Micheli 1995

Back Pain in Children
• AP, lateral x-rays (obliques = ? )
• Conventional or SPECT bone scan
• MRI
• CT/myelogram
• CBC, ESR
• EMG/NCS not generally helpful
Diagnostic work up
Back Pain in Children
• Abnormalities on SPECT that may be missed
with conventional bone scan
• Pedicle/pars pathology
• Spinous process pathology
• Vertebral body or endplate abnormalities
SPECT Bone Scan

SPECT vs Whole Bone Scan
Pars Interarticularis Pathology
• Stress fx
• Early fracture of a small number of trabecula in the pars, generally a hot bone scan with
normal x-ray. Probably represents the incipient state
• Spondylolysis defect
• complete pars defect w/o slippage
• Spondylolisthesis (lytic type)
• Pars defect with slippage

Pars Interarticularis Pathology
• Stress fx
• Acute phase (potential to heal)
• Healing phase
• Spondylolysis defect
• Acute phase (? Potential to heal)
• Chronic (no potential to heal)
• Spondylolisthesis (lytic type)
• Always chronic (no potential to heal)

Pars Interarticularis Pathology
• Stress fx
• Spondylolysis
• Spondylolisthesis
(lytic)
( commonly )
( uncommonly )

Pars Interarticularis Pathology
• Occurs only rarely before
5 yrs of age
• Probably developmental
condition with genetic
predisposition (40 %
prevalence in Eskimos)
• May represent a stress or
fatigue fx of an inherently
weak pars
• Due to repetitive stress
rather than acute injury
Etiology

Pars Interarticularis Pathology
• Prevalence of spondylolysis was 4.4% at
age 6 years increasing to 6% by
adolescence
• The majority of cases are asymptomatic
and require no treatment
Doubousset 1997
Fredrickson

Pars Interarticularis Pathology
• Onset of symptoms typically during
adolescent growth spurt, frequently
in association with basketball or
gymnastics
• Symptoms may disappear if sporting
activity is ceased
History

Pars Interarticularis Pathology
• Pain is in low back but may radiate to
buttocks or proximal thigh
• Symptoms are increased by activity and
decreased by rest
• Pain not present at night
History
Pars Interarticularis Pathology
• Lumbar tenderness
• Restricted ROM ( in high grade slips)
• Hamstring tightness ( in high grade slips )
• Neuro exam normal ( except in high grade)
• Flat or square buttock with listhetic gait ( in high
grade)
• SLR negative for sciatica
Physical exam

Pars Interarticularis Pathology
• Plain radiographs (+/-obliques) will usually
show lysis or slip but will not show stress
reaction or distinguish between acute and
established lysis
• Spect bone scan frequently necessary for
stress fx diagnosis and for judging state of
healing
Diagnosis
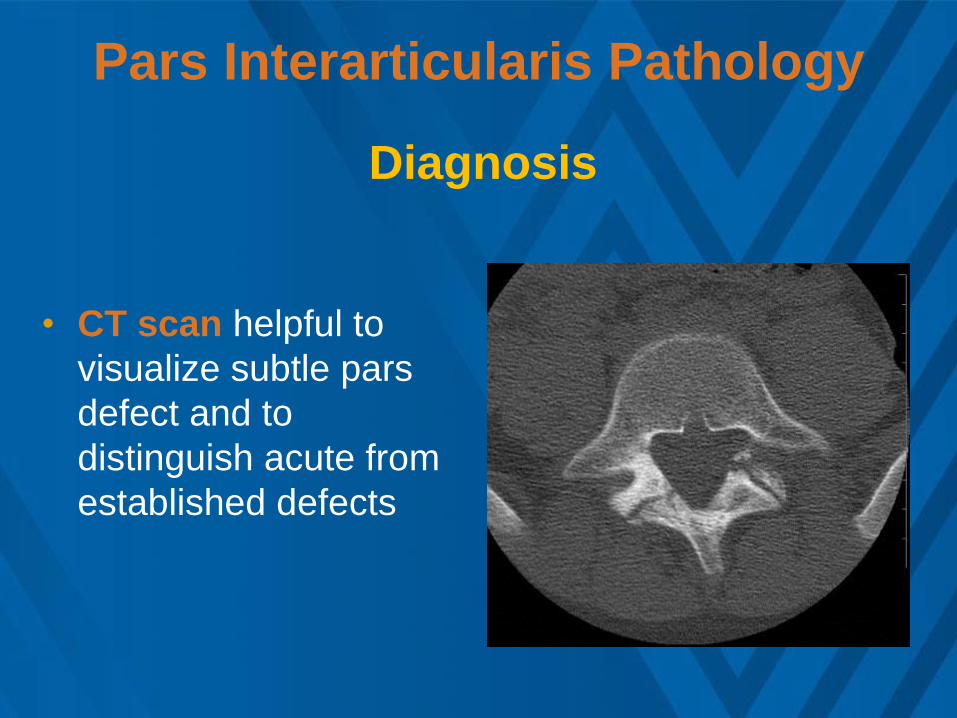
Pars Interarticularis Pathology
• CT scan helpful to
visualize subtle pars
defect and to
distinguish acute from
established defects
Diagnosis

MRI and Stress Fx
• MRI very helpful if
neural decompression
is contemplated
• Will also show very
early stress rx

Pars Interarticularis Pathology
• Avoidance of aggravating activities
• Mild anti-inflammatory medication
• Corset or TLSO ???
• Abdominal strengthening exercises ???
• Formalized physical therapy ???
Treatment

Pars Interarticularis Pathology
• Controversial
• Not entirely predictable
• stress reaction greater than lysis
• Need “hot” bone scan
• May not be influenced by any conservative
measure other than avoidance of aggravating
sporting activity
Healing potential of stress reaction or lysis ?

Pars Interarticularis Pathology
Only 2 of 29 young patients (avg. 21
yrs. range 13-31) healed an acute lysis
defect with conservative treatment
Healing potential
Daniel 1995

Pars Interarticularis Pathology
• CT follow up of 40 young athletes with
normal x-rays and positive bone scans
showed that 45% had chronic lysis, 40%
still with acute fx in various stages of
healing, and only 15% with healed fx
Congeni 1997

Pars Interarticularis Pathology
• Conservative treatment produced
healing in 73% of early defects, only
38% of intermediate, and none of the
chronic defects
Healing potential
(185 patients under age 18 yrs.)
Morita 1995

Pars Interarticularis Pathology
• If symptoms are not present with normal ADL,
but recur when child or adolescent returns to
sports, then adolescent and family have to
decide the relative importance of pain vs.
sports. There is no “danger” worry.
• This is a family decision
Treatment

Pars Interarticularis Pathology
• Surgical fusion indicated for any patient with
refractory pain occurring during routine ADL
• Surgical fusion or pars repair indicated for
any patient desiring, but unable, to return to
sporting activity
• Surgical fusion or pars repair not indicated in
asymptomatic patient, regardless of the
severity of a slip
Surgical treatment

SPONDYLOLYSIS - PLSF

SPONDYLOLYSIS – PARS
REPAIR

SPONDYLOLYSIS
PLSF + PARS REPAIR

Spinal Column Tumors
• Rare occurrence
• Primary malignant spinal column tumors
are very rare (Ewing’s , osteosarcoma)
• Most malignant lesions are metastatic
• Benign lesions are much more common
than malignant

Spinal Column Tumors
• Osteoid osteoma
• Osteoblastoma
• Eosinophilic granuloma
• Fibrous dysplasia
• Aneurysmal bone cyst
• Osteochondroma
Benign Lesions
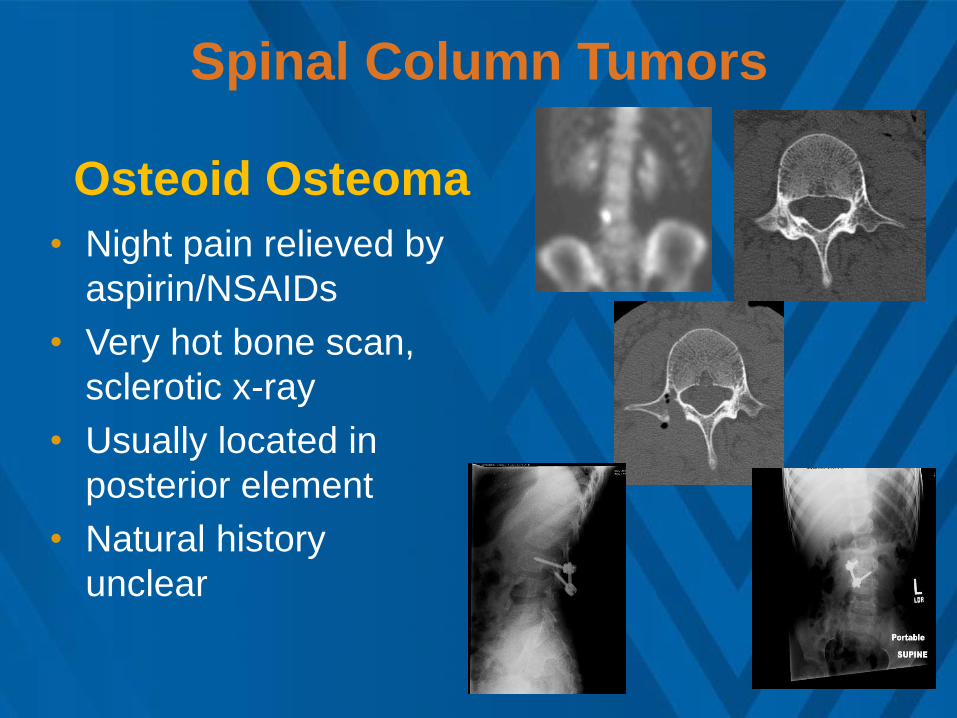
Spinal Column Tumors
• Night pain relieved by
aspirin/NSAIDs
• Very hot bone scan,
sclerotic x-ray
• Usually located in
posterior element
• Natural history
unclear
Osteoid Osteoma

Spinal Column Tumors
• Classic appearance is vertebra plana
(compression fx )
• May present before collapse
• Produces pain, occasionally neuro findings
• Spontaneous resolution of symptoms occurs,
but complete reconstitution of vertebral body
does not
Eosinophilic granuloma

Spinal Column Tumors
• Cold bone scan possible
• Skeletal survey helpful
• May involve anterior and posterior elements
• “Vertebra plana”
• Radiation not indicated
• Needle biopsy if any question
• Surgery for neuro compression only
Eosinophilic Granuloma

Eosinophilic Granuloma

Intraspinal Pathology
• Malignant astrocytoma
• Lipoma
• Syringomyelia
• Tethered spinal cord
• Diastomatomyelia
• Chiari malformation
• Ependymoma
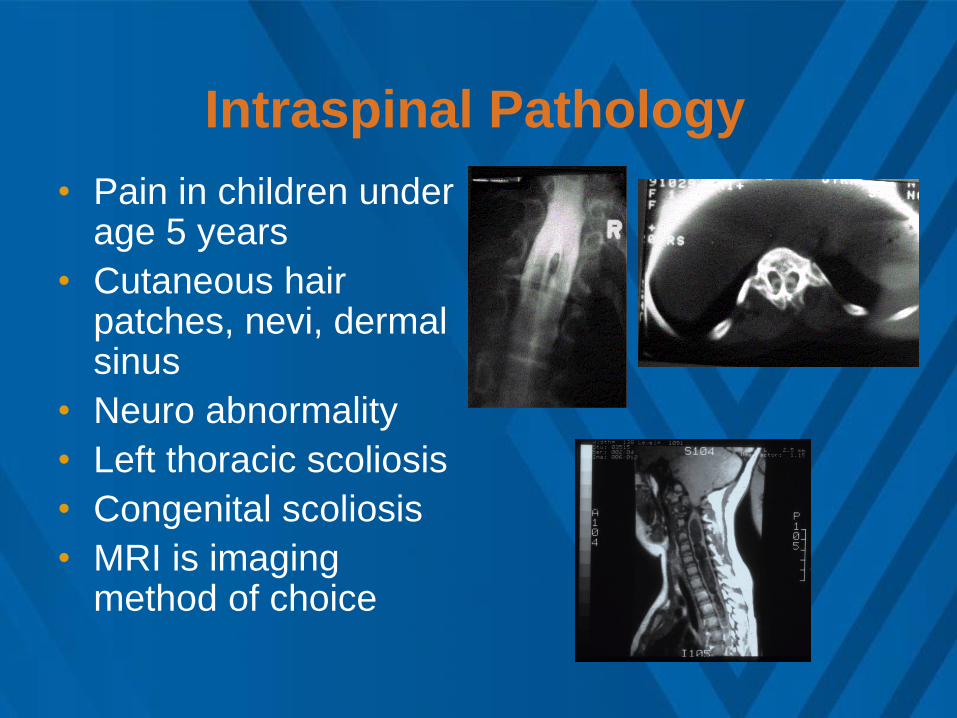
Intraspinal Pathology
• Pain in children under age 5 years
• Cutaneous hair patches, nevi, dermal sinus
• Neuro abnormality
• Left thoracic scoliosis
• Congenital scoliosis
• MRI is imaging method of choice

Intradural tumor

Scoliosis and Back Pain • Children frequently
complain of low grade back pain with scoliosis, especially after the diagnosis has been made
• Pain not severe, doesn’t interfere with activity
• Work up not necessary unless other factors present

Scoliosis and Back Pain
• Work up necessary if : • Curve other than right
thoracic, particularly if left thoracic, hyperkyphosis, lack of rotation or presence of any congenital anomaly
• Rapid progression
• Neurological findings present

Lumbar Scheuermann’s

Discitis/Osteomyelitis
• Variation of a single bacterial disease
with x-ray appearance dependent on
chronicity of involvement (sterile discitis
probably doesn’t exist)
• Infection probably begins in body and
traverses small vascular channels to
reach disc

Discitis/Osteomyelitis
• Discitis more common than osteomyelitis
• increased awareness of protean
presentation
• early use of bone scan
• recognition that disease is bacterial in
origin with earlier antibiotic coverage

Discitis/Osteomyelitis
• Back pain unrelieved by rest, abrupt
onset is typical
• Fever, systemic illness, malaise
• Refusal to walk, abdominal pain in the
young child
• Spasm, decreased back motion ,
reactive scoliosis
History/Physical

Discitis/Osteomyelitis • X-ray is initially normal, but bone scan will always be
hot
• Later x-ray will show disc space narrowing and end
plate erosion
• MRI may show changes in vertebral body marrow
signal even before x-ray finding of disc space
narrowing
Discitis/Osteomyelitis
• Mainstay of treatment is antibiotics
• Biopsy frequently negative for bacteria
• Brace or cast probably not necessary
• Surgery not necessary for discitis, and only
infrequently necessary for osteomyelitis
Treatment

HNP in the Child
• Almost never the etiology of LBP in pre teen,
but should be considered in teenager
• LBP without classic radiculopathy is possible
but not common
• Spinal rigidity
• Pain more severe than lysis pain
• MRI is best imaging tool
• Treatment is similar to adult
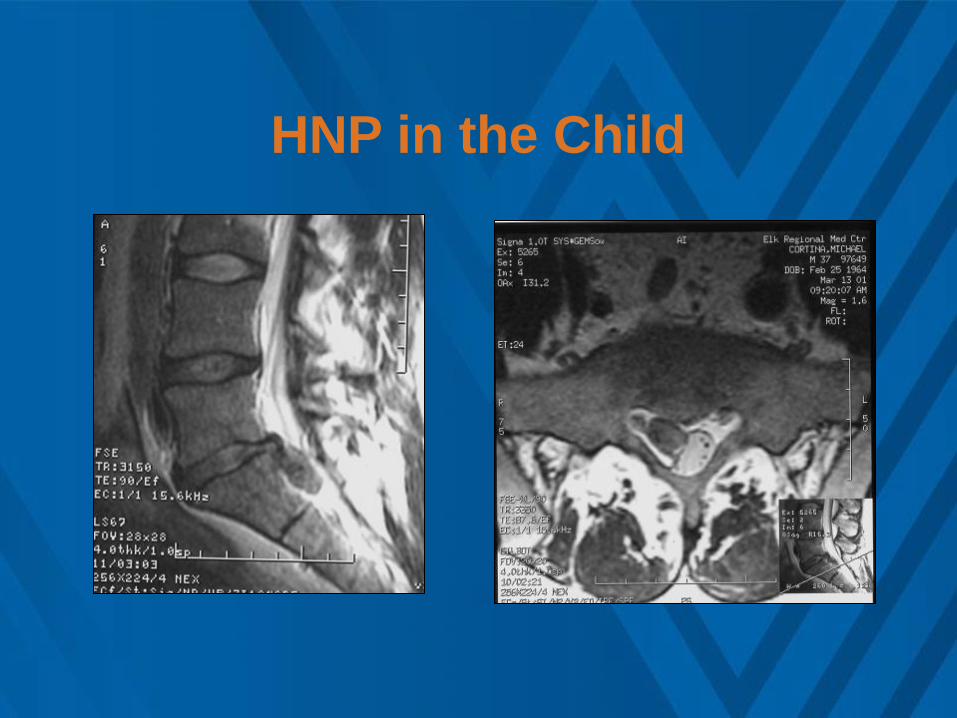
HNP in the Child

HNP in the Child
• Teenagers may
present with a clinical
picture similar to HNP
but MRI confirms an
injury to the posterior
vertebral limbus- most
common at L4-5
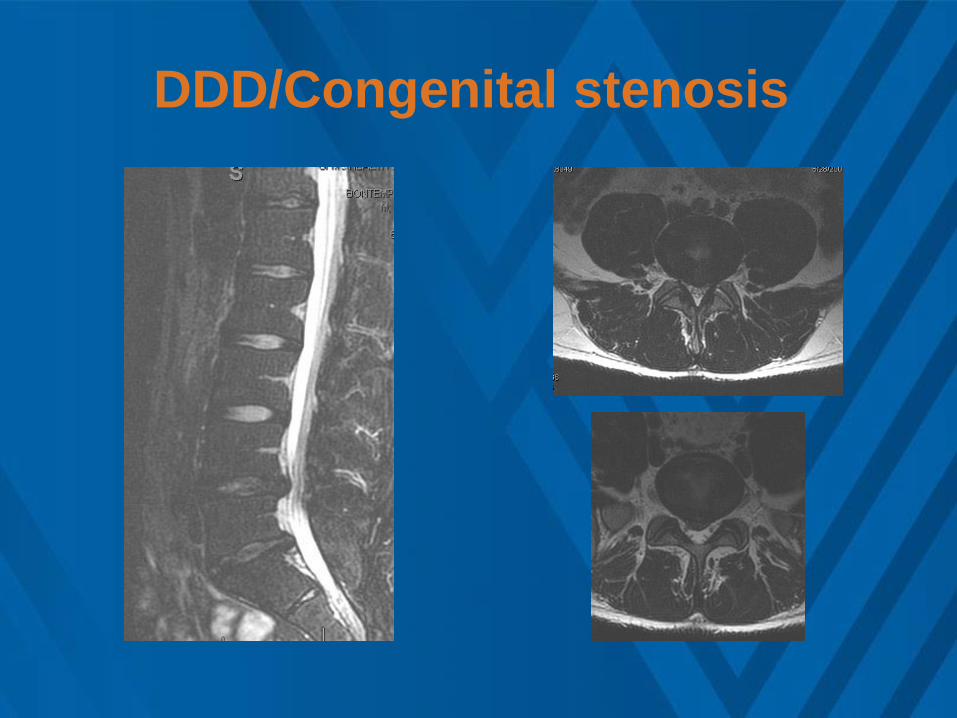
DDD/Congenital stenosis

DDD/Congenital stenosis
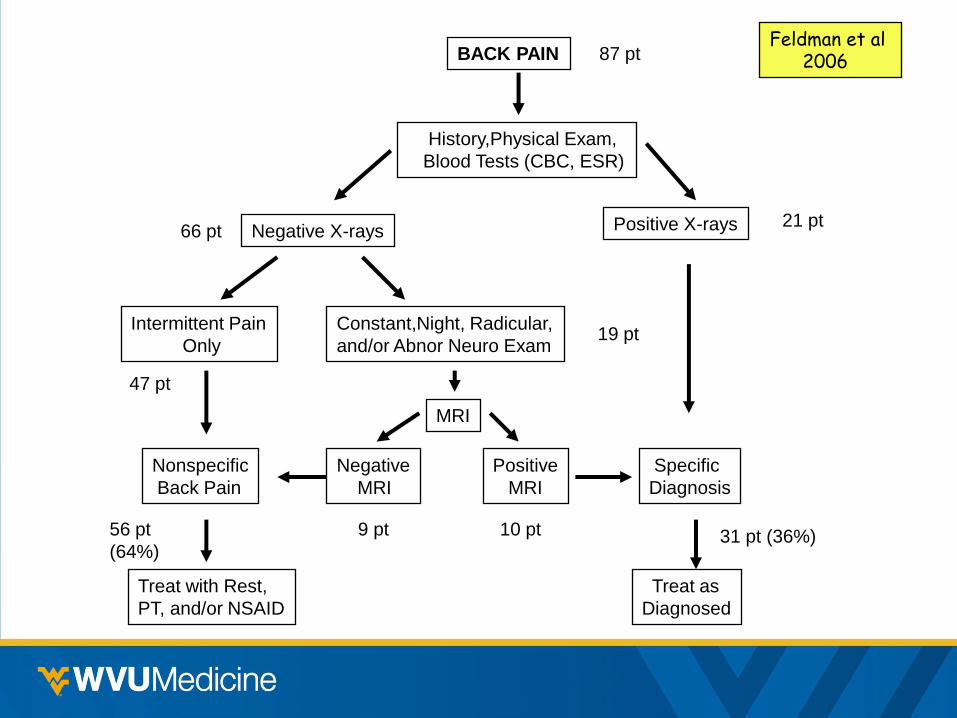
BACK PAIN
History,Physical Exam,
Blood Tests (CBC, ESR)
Negative X-rays
Intermittent Pain
Only
Constant,Night, Radicular,
and/or Abnor Neuro Exam
Positive X-rays
MRI
Negative
MRI
Positive
MRI
Specific
Diagnosis
Treat as
Diagnosed
Nonspecific
Back Pain
Treat with Rest,
PT, and/or NSAID
Feldman et al 2006 87 pt
21 pt 66 pt
19 pt
10 pt 9 pt
47 pt
56 pt
(64%) 31 pt (36%)
BP in the Child/Adolescent
• More common than once believed
• Usually not due to serious pathology
• Must be thoughtfully investigated to rule out the treatable etiologies
Conclusions

Back Pain in the Child/Adolescent
Need for
Surgery
should
be
Rare
Back Pain in Children in Perspective
• Annual incidence of LBP rose from 11.8% at age
12yr to 21.5% at 15+ years (Burton 1996)
• Annual incidence of migraine h/a in kids (age 11-
15 yrs) is 16% (Abu-Arefeh 1994)
• Annual incidence of migraine h/a in adults is
15% (Mounstephen 1995)

Lifetime Prevalence of LBP (%)
Burton 1996
11.6%
21.4%28.8%
38.5%
50.4%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
11 12 13 14 15
Child's Age (years)
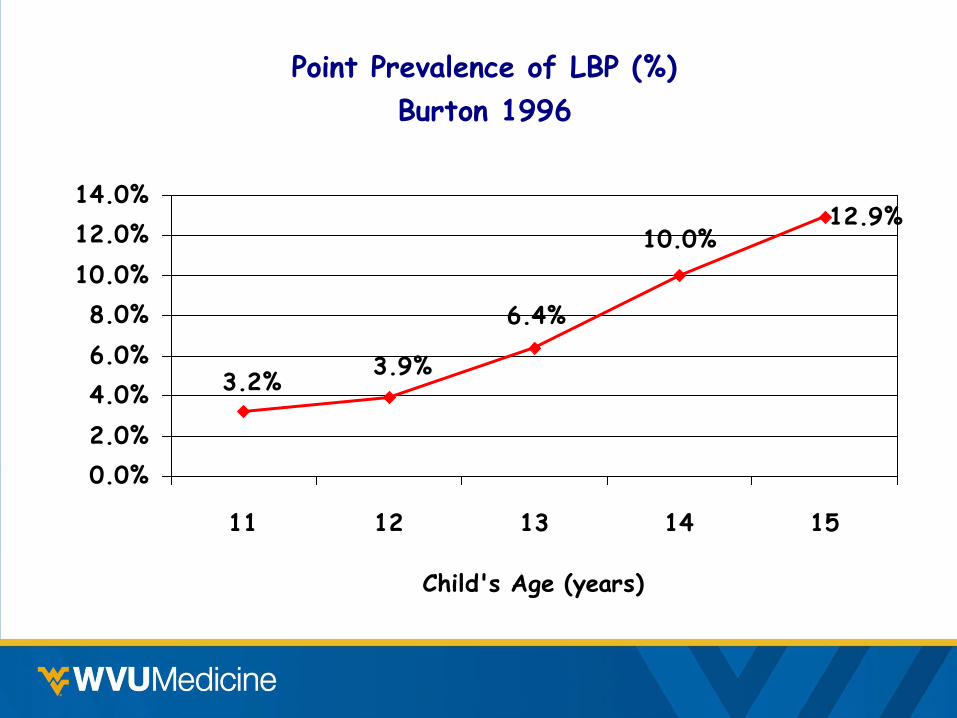
Point Prevalence of LBP (%)
Burton 1996
12.9%10.0%
6.4%
3.9%3.2%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
11 12 13 14 15
Child's Age (years)

Yearly Prevalence of LBP Interfering with
School Work or Leisure Activity
Taimela 1997
1%
6%
18%18%
0%
5%
10%
15%
20%
7 10 14 16Age (years)
Back Pain in Children
Psychological Factors
1. If parents have LBP more likely in child
(Balague 1995, Gunzburg 1999)
2. More BP in 9 yr olds also reporting feelings of
unhappiness, sleeplessness, and perceptions
of ill health (Gunzburg 1999)
3. Strong association between LBP and
emotional problems, conduct problems, h/a,
abdominal pain, sore throat, and daytime
tiredness (Watson 2003)

Does LBP in Childhood Predispose
to LBP in Adulthood ?
1. Up to 1/3 of children have recurrent episodes
(Salminen ‘92,Taimela97, Viry ‘99)
2. 90% of school children with BP had BP in 25yr
longitudinal f/u (Harreby ‘95)
3. BP at age 18 yr in military recruits increased
risk of BP at age 40yr (Hellsing 2000)

Does LBP in Childhood Predispose
to LBP in Adulthood ?
4. BP at age 18 y/o in military recruits increased risk of BP at age 30 y/o (Darre ‘99)
5. 13 yr f/u of BP in adolescents did not predict future BP but did predict pain in general in adulthood (Fearon 2001)
6. 26% of adolescents with more than 30 days of BP had similar pain in 8 yr f/u (Hestbaek 2006 odds ratio 4)

Does LBP in Childhood Predispose
to LBP in Adulthood ?
7. BP in the growth period and familial
occurrence of back disease are important
risk factors for BP later in life, with an
observed probability of 88% if both factors
are present. No correlation with x-ray
changes as adolescents.
Harreby 1995 ( 25 yr. prospective cohort study of 640 Danish children )
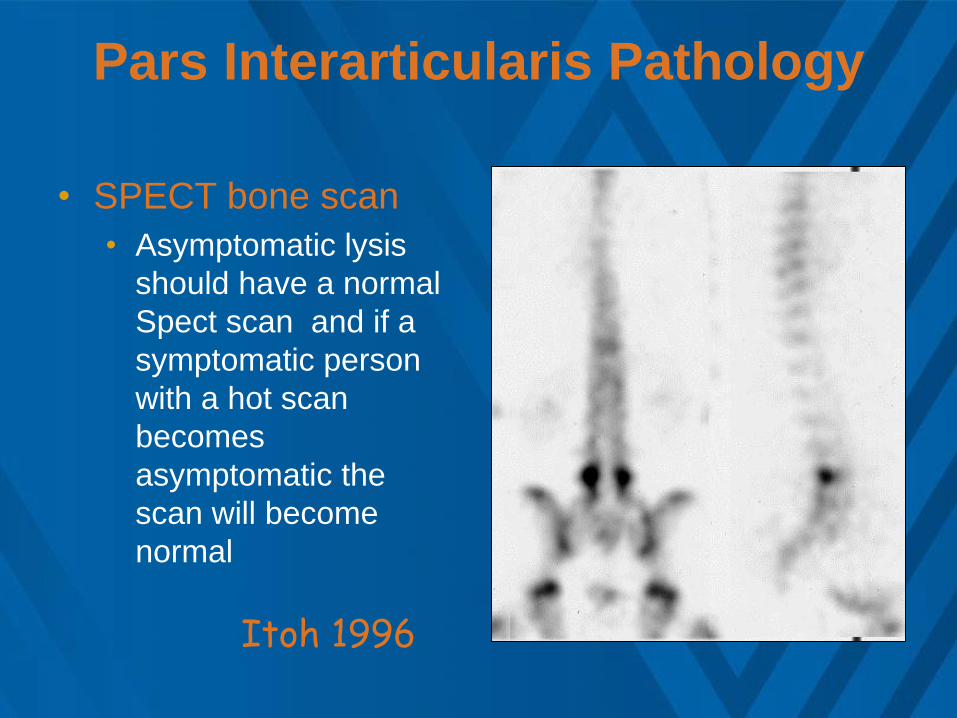
Pars Interarticularis Pathology
• SPECT bone scan
• Asymptomatic lysis
should have a normal
Spect scan and if a
symptomatic person
with a hot scan
becomes
asymptomatic the
scan will become
normal
Itoh 1996

Back Pain in the Child/Adolescent
• BP is common in adolescents, increases with age, is recurrent, generally does not deteriorate with time.
• Much of the symptomatology can be considered normal life experience
Conclusions
Does LBP in Childhood Predispose
to LBP in Adulthood ?
• LBP in adolescence is a significant risk factor for LBP in adulthood.
• The risk increases with increasing duration of BP in adolescence
Conclusions

Back Pain in the Child/Adolescent
• Psychosocial factors more important than mechanical factors in the reporting
of childhood LBP • Cause or effect?
• BP may be marker for somatization
Conclusions
Back Pain in the Child/Adolescent
• It is frequently not possible to provide a
definitive explanation for back pain in children
• Clinician should be knowledgeable in
diagnosis, natural history, and treatment of
the most common causes of BP
Conclusions

Back Pain in the Child/Adolescent
• Although the possibility of serious
spinal pathology must be
considered, the majority of
adolescent back trouble may be
considered a normal life experience
Conclusions
Burton 1996
1989-1990 NAMCS Groups per Hart
et al 1995
• MD FP/GP
• DO FP/GP
• General internal medicine
• Neurologists
• Orthopaedic surgeon
• Neurosurgeon


















