Special Populations: Pediatrics Arthur G. Roberts.
27
Special Populations: Pediatrics Arthur G. Roberts
-
Upload
merry-mccormick -
Category
Documents
-
view
223 -
download
0
Transcript of Special Populations: Pediatrics Arthur G. Roberts.
Special Populations: Pediatrics
Arthur G. Roberts

Is there a difference in blood flow (Q) between an athlete and non-athlete?
• Blood flow increases during exercise.• At rest, blood flow is similar to non-athletes,
except that it takes less beats/min to push the same amount of blood.
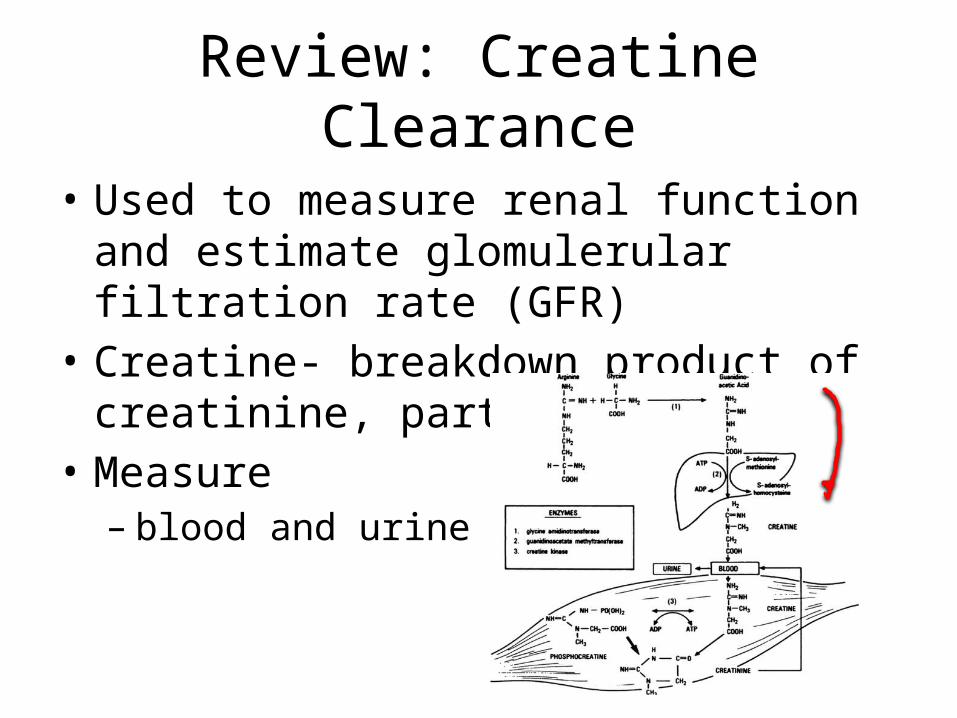
Review: Creatine Clearance
• Used to measure renal function and estimate glomulerular filtration rate (GFR)
• Creatine- breakdown product of creatinine, part of muscle
• Measure– blood and urine
Age Classifications
• Neonate- to 1 month post utero• Infant- 1 month to 2 years• Child- 2 and 12 years • Pre-adolescent and adolescent- 13 to 17 years• Adult- >18 years of age

Absorption Affected
• Gastric acid secretion• Bile salt formation• Gastric emptying time• Intestinal motility• Bowel length and effective absorptive surface• Microbial flora

Effects on Absorption
• decrease in gastric pH– neonates, infants, young children– pH = 6-8 at birth (vaginal delivery, amniotic fluid)– increases to body weight ~2-3 years
• increase of basic drugs– penicillin
• decrease of weakly acidic drugs– phenytoin, phenobarbital
Effects on Absorption
• decrease gastric and intestinal motility (neonates and infants)– Peristalsis absent in first 2-4 days– Adult values reached in in 6-8 months– Prolonged diarrheal episodes may contribute
• decrease bile acids by 50% (neonates)– impaired absorption of lipid solubile drugs or
vitamins.• b-glucuronidase activity increases (breast milk)

Effects of Distribution: Body Composition

Effects on Distribution: Blood Volume
• Premature infants- 98 mL/kg• At 1 year- 86 mL/kg• > 1 year- 77 mL kg

Effects on Distribtuion
• Plasma Protein Binding– reduced Albumin (bilirubin and various drugs)• Newborn- 3.1 g/dL (66% of adult)• 1-3 years- 3.8 g/dL• 4-6 years- 4.4 g/dL• >7 years- 4.7 g/dL • reduced affinity• increased Vd
– reduced a-1-acid glycoprotein (orosomucoid)• increased Vd of basic drugs

Metablism and Elimination
• Liver metabolism– All enzymes, but activity reduced– Phase I (20-70%) of adult (neonate)• reduced hydroxylation and N-demethylation• capacity reduction the same• increased methylation
– Phase II reaches adult values in 3-4 years• reduced conjugation
– UGTs- chloramphenicol-”gray baby syndrome”

Metabolism and Elimination: Renal Clearance
• Creatine Clearance– (1 day)- 18 mL/min/1.73 m2
– (6 days)- 36 mL/min/1.73 m2
– (1-5 months) – 70 mL/min/1.73 m2
– (6-11 months) – 100 mL/min/1.73 m2
– (adult)-112 mL/min/1.73 m2

Metabolism and Elimination: Renal Clearance
• Decreased renal function 20-40% of adult• Decreased glomerular filtration rate– ~40 mL/min/1.73 m2 (neonate)• premature infants even lower
• Decreased Tubular Secretion and transporter-mediated Reabsorption
• Increased t1/2, increase dosing interval
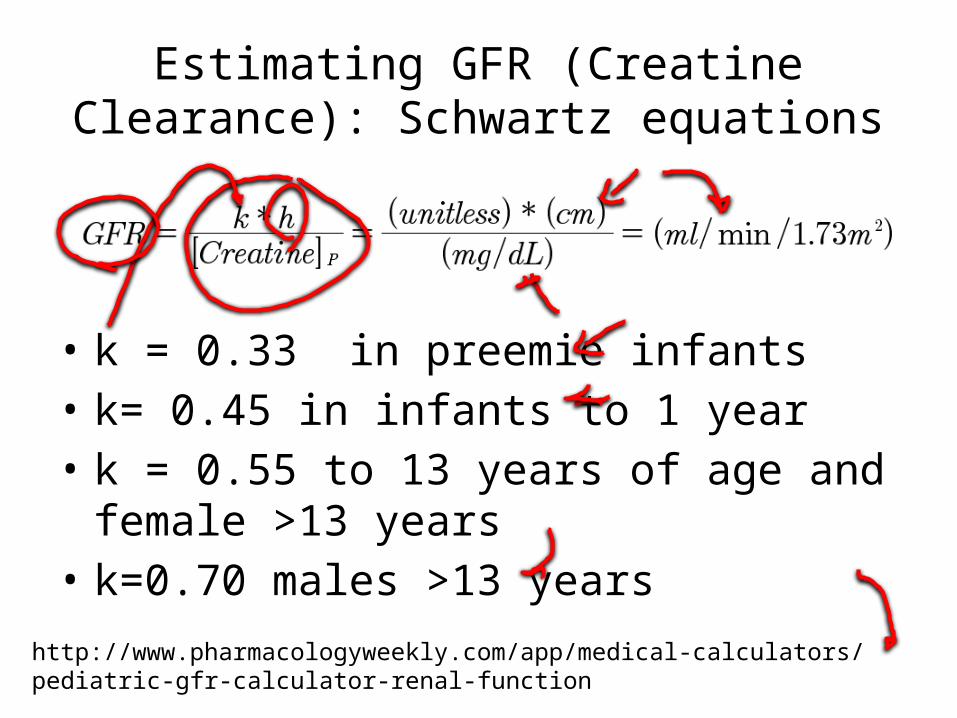
Estimating GFR (Creatine Clearance): Schwartz equations
• k = 0.33 in preemie infants• k= 0.45 in infants to 1 year• k = 0.55 to 13 years of age and female >13
years• k=0.70 males >13 years
http://www.pharmacologyweekly.com/app/medical-calculators/pediatric-gfr-calculator-renal-function

What the hell is 1.73 m2?
• normalization• refers to standardized body surface area of a
70 kg man– from 8 children, 7 adults in 1928– areas of mean and women age 25 prior to
actuarial tables

Aminoglycosides (Antibiotic)
Streptomycin
Gram-negative antibacterial therapeutic agent
Examples• Escherichia Coli (E. coli)• Salmonella• Shigella

Aminoglycosides: Baby’s Reaction
• Neonates– increased Vd (0.5-0.6 L/kg) (dosage?)
– increased t1/2 (dosing interval?)
• Infants and children– increased Vd (0.4-0.5 L/kg) (dosage?)
– t1/2 normalizes (dosing interval)
• Adults– Vd (0.25-0.35 L/kg)
– t1/2 (Streptomycin) = 3 hours– dosing interval = 8-12 hours
http://www.globalrph.com/aminoglycosides.htm

Aminoglycosides: Cystic Fibrosis Cystic fibrosis transmembrane conductance regulator (CFTR)

Aminoglycosides: Cystic Fibrosis
• Increased Vd– increased lean body mass/kg– increased tissue binding
• 25% Increased Cl, shorter t1/2 (GFR)• dosing? and dosing interval?

Vancomycin

Vancomycin
• Neonates– Increased Vd (0.75 L/kg)• adult 0.62 L/kg
– Increased T1/2 6-11 hours• adults 4-6 hours
• Infants and children– Clearance 2-3x higher compared to adults– t1/2: 3-4 hours in infants
– t1/2:2-3 hours in children
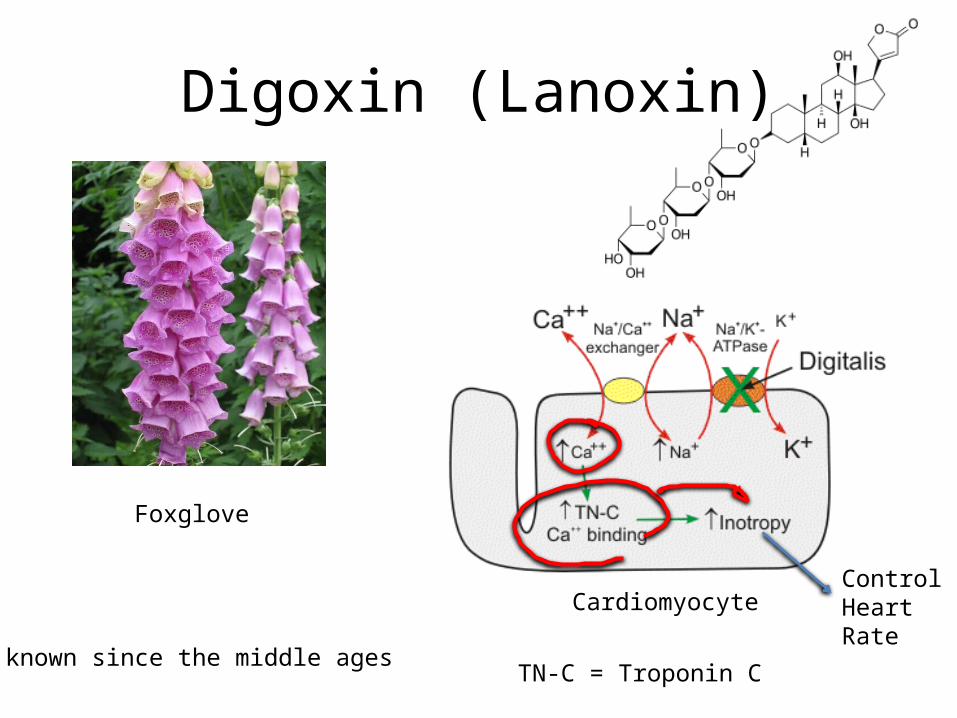
Digoxin (Lanoxin)
Cardiomyocyte
TN-C = Troponin C
Foxglove
known since the middle ages
ControlHeartRate

Digoxin
• Neonates– Decreased Cl and Vd– Digoxin-like immunoreactive substance (DLIS)
• associated with cardiomyopathy• structure similar to digoxin• interferes with therapy• baseline concentration may be required
• Infants– Increased Vd 11.9 L/kg
• Adult Vd 6L/kg

Digoxin Dosing

Theophylline
caffeine
PDE=PhosphodiesterasePKA=Protein Kinase A

Theophylline
• Indications in Pediatrics– Asthma– Premature apnea/bradycardia– Bronchopulmonary dysplasia
• Neonates– increased Vd, decreased Cl– lower loading and maintenance doses
• Children (1-4 years old)– increased Cl

Dosing









![Non-linear Pharmacokinetics Arthur G. Roberts. Linear Pharmacokinetics AUC dose K Cl dose [Drug] plasma time ln[Drug] plasma time Increasing Dose.](https://static.fdocuments.us/doc/165x107/56649eb35503460f94bba929/non-linear-pharmacokinetics-arthur-g-roberts-linear-pharmacokinetics-auc.jpg)