Special Forms of Rhinosinusitis - orl-hno.ch · or aerobic/anaerobic) or invasive fungal sinusitis...
58
Special Forms of Rhinosinusitis Vasculitis, Autoimmune Disease, Immuno-deficiencies… Patrick Dubach, Chefarzt HNO Klinik Buergerspital Solothurn Konsiliarus Universitätsklinik HNO, Kopf- und Halschirurgie Inselspital Bern
Transcript of Special Forms of Rhinosinusitis - orl-hno.ch · or aerobic/anaerobic) or invasive fungal sinusitis...

Special Forms of RhinosinusitisVasculitis, Autoimmune Disease, Immuno-deficiencies…
Patrick Dubach, Chefarzt HNO Klinik Buergerspital Solothurn
Konsiliarus Universitätsklinik HNO, Kopf- und Halschirurgie Inselspital Bern

Klinik für HNO-, Kopf- und Halschirurgie
Team Approach for Special Cases!
AUTO? IMMUNO? Factor X?
• Alternative Diagnosis: Auto-Immune,
Immundeficency, atypical rare infections,
Neoplasm……
Nose, Ear, Larynx:
Polychondritis?Sinus, Middle
Ear, Mastoid:
Vasculitis?
Oral mucosa:
Lupus, Crohn?
Salivary Glands:
Sjögren,
Sarcoidosis?

Klinik für HNO-, Kopf- und Halschirurgie
SUMMARY:
• …in case of abnormal prolongated or repetitive
rhinological disease
• RED FLAGS: Think of special forms of RS and
check
–Patients History
–? Autoimmune diseases (rheumatologic disease,
immunosupressants, disorder of immune system)
–? Infections (atypical organism, co-infection (HIV))
–? Neoplasia

Klinik für HNO-, Kopf- und Halschirurgie
Schedule
• The BIG THREE of autoimmune GRANULOMATEOUS
diseases for the rhinologist
Not in detail:
• Atypical Infection and Fungal RS
• The immuno-supressed patient
IATROGENIC IMMUNOSUPPRESSION
(transplantion or rheumatologic patients)
UNCONTROLLED DIABETES, renal and
hepatic insufficiency

Klinik für HNO-, Kopf- und Halschirurgie
•40 year old male patient
•suffering from stuffy nose and nasal crusts
since years
•presented with discrete bilateral epistaxis
and intermittant unilateral epiphora
•Chronic cough and fatigue
Case 1: Bleeding Crusts

Klinik für HNO-, Kopf- und Halschirurgie
Circular Stenosis

Klinik für HNO-, Kopf- und Halschirurgie
Ulcerated Crusts

Klinik für HNO-, Kopf- und Halschirurgie
Granulomatosis with Polyangiitis GPA(AKA Wegener Granulomatosis)
• 50-100 per million Europeans
• „Autoimmune disease“ with histological triad:
–Necrosis (46%), granuloma (42%), vasculitis (16%)
–Cave: ENT biopsy in 50% suggestive/in 10% classical
• Staging possibilities
–ELK staging system (organs with high vascularization)
–E: ENT, L:Lung, K: Kidney
–„Limited“ vs Generalized/Systemic Disease
–„Vasculitic“ (GN, pulmonary hemorrage) vs
„Granulomatous“ (ENT, pulmonary nodules)
Klinik für HNO-, Kopf- und Halschirurgie
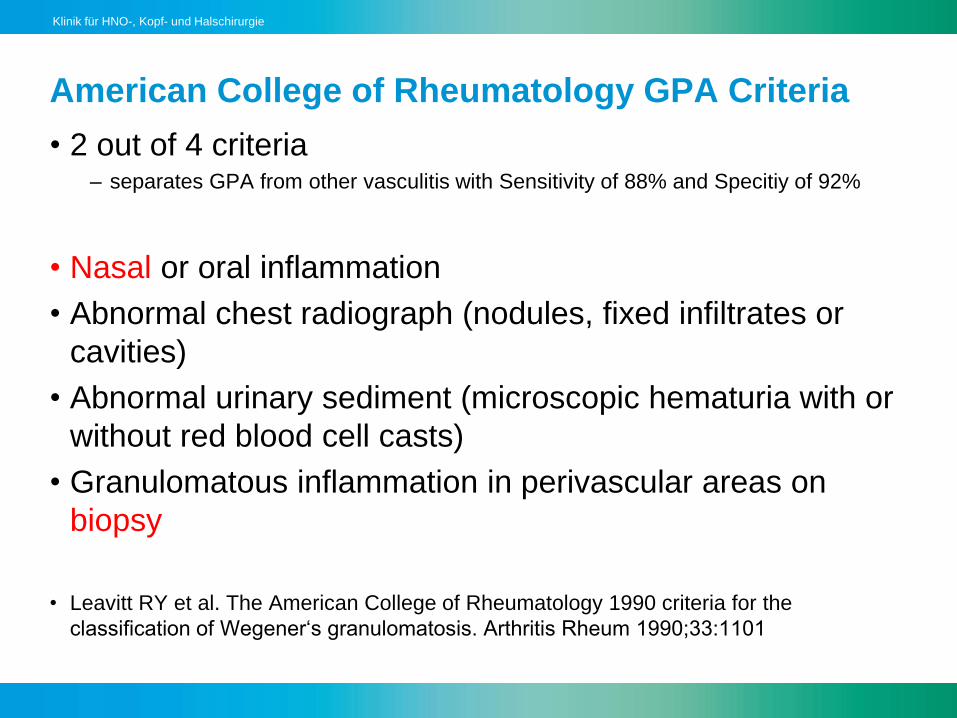
American College of Rheumatology GPA Criteria
• 2 out of 4 criteria – separates GPA from other vasculitis with Sensitivity of 88% and Specitiy of 92%
• Nasal or oral inflammation
• Abnormal chest radiograph (nodules, fixed infiltrates or
cavities)
• Abnormal urinary sediment (microscopic hematuria with or
without red blood cell casts)
• Granulomatous inflammation in perivascular areas on
biopsy
• Leavitt RY et al. The American College of Rheumatology 1990 criteria for the
classification of Wegener‘s granulomatosis. Arthritis Rheum 1990;33:1101

Klinik für HNO-, Kopf- und Halschirurgie
0
10
20
30
40
50
60
70
80
90
100
Clinical Presentation (n=62): ENT Bern
WG
non-WG
GPA Leading Symptoms
Borner U et al Am J Rhinol Allergol 2012:475-480.

Klinik für HNO-, Kopf- und Halschirurgie
Saddle nose: 28% (Holle et al 2010)
• 29.9.

Klinik für HNO-, Kopf- und Halschirurgie
Septal Perforation:
24% (Holle et al 2010)
Biopsy if focal inflammed target
i.e. directed and deep (i.e. bleeding)
Biopsies… you want vessels…
Klinik für HNO-, Kopf- und Halschirurgie
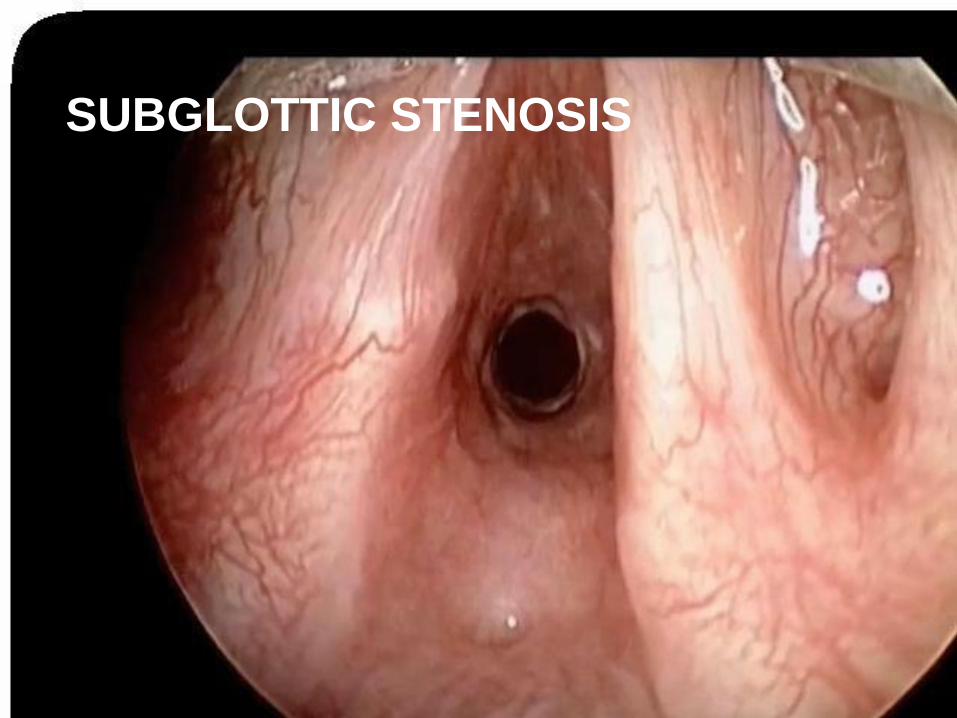
SUBGLOTTIC STENOSIS

Klinik für HNO-, Kopf- und Halschirurgie
Midline Destructive Lesions: What disease is this?
1….
2……
3……
Klinik für HNO-, Kopf- und Halschirurgie
•48y old nurse suffering from nasal
obstruction and anosmia since 2 years
•Polypectomy and sphenoethmoidectomy but
recurrent nasal block by polyps within 3
months
•Since 10y: Bronchial asthma
•Blood eosiniophilia >10%
Case 2: The hydra of nasal polyps

Klinik für HNO-, Kopf- und Halschirurgie
Churg Strauss

Klinik für HNO-, Kopf- und Halschirurgie
Klinik für HNO-, Kopf- und Halschirurgie
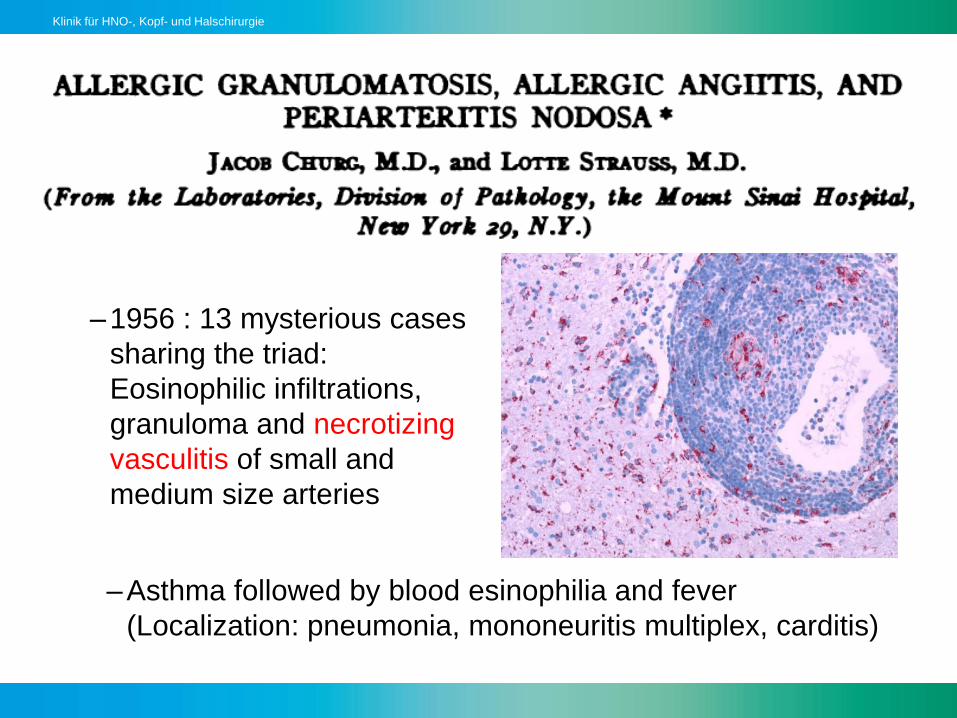
–1956 : 13 mysterious cases
sharing the triad:
Eosinophilic infiltrations,
granuloma and necrotizing
vasculitis of small and
medium size arteries
–Asthma followed by blood esinophilia and fever
(Localization: pneumonia, mononeuritis multiplex, carditis)
Klinik für HNO-, Kopf- und Halschirurgie
American College of Rheumatology EGPA:Eosinophilic Granulomateous Polyangiits AKA Churgh Strauss Disease
• Four out 6 criteria gives EGPA diagnosis with sensitivity
85% and specificity of 99.7%
• Asthma
• Transient pulmonary opacities
• Blood eosinophilia >10% or 1500/mm3
• Mononeuritis (multiplex)
• Paranasal sinus abnormalities
• Biopsy with eosinophilic paravasal infiltrates
• Masi AT et al. The American College of Rheumatology 1990 criteria fo the Classification
of Churg Strauss Syndrome. Arhtritis Rheum 1990;33:1094
Alternative Lanham Criteria with Asthma, Eos1500/ul and vasculitis in 2 or more extrapulmonary organs

Klinik für HNO-, Kopf- und Halschirurgie
EGPA: Clinical Stages
• Prodromal Phase: 2nd and 3rd decade
–Atopic disease: Allergic rhinitis (50% with polyps) and asthma
• Eosinophilic Phase:
–Peripheral blood esinophilia and inflitration of multiple organs
• Vasculitic Phase: 3rd and 4th decade
–Vasculitis with paravasal eosinophilic granuloma and
necrosis
• Red flags: Eosinophilic Myocarditis, Glomerulonephitis

Klinik für HNO-, Kopf- und Halschirurgie
EGPA:
• 10 bis 15 per million Europeans
• No gender preference
• Third frequent ANCA associated vasculitis after
GPA and microscopic polyangitis
• Histological Trias: Vasculitis, esosinsophilc tissue
infiltrates and granuloma

Klinik für HNO-, Kopf- und Halschirurgie
EGPA Manifestationen
• Pulmonary 90% (Nodules, migrating infiltrates)
• Skin 66%: Subcutaneous nodules (granuloma) and
palpable purpura (vasculitis), livedo reticularis
• Upper Airway (and ear) 48%: Chronic rhinosinusits (60%
with polyps in case series n=29)
• Heart 15-30%: CARDITIS responsible for 50% of deaths by
EGPA: → echocardiographia and ECG (heart failure and
arrythmia)
• Mononeuritis (multiplex) 75% and Glomerulonephritis 22%
Klinik für HNO-, Kopf- und Halschirurgie
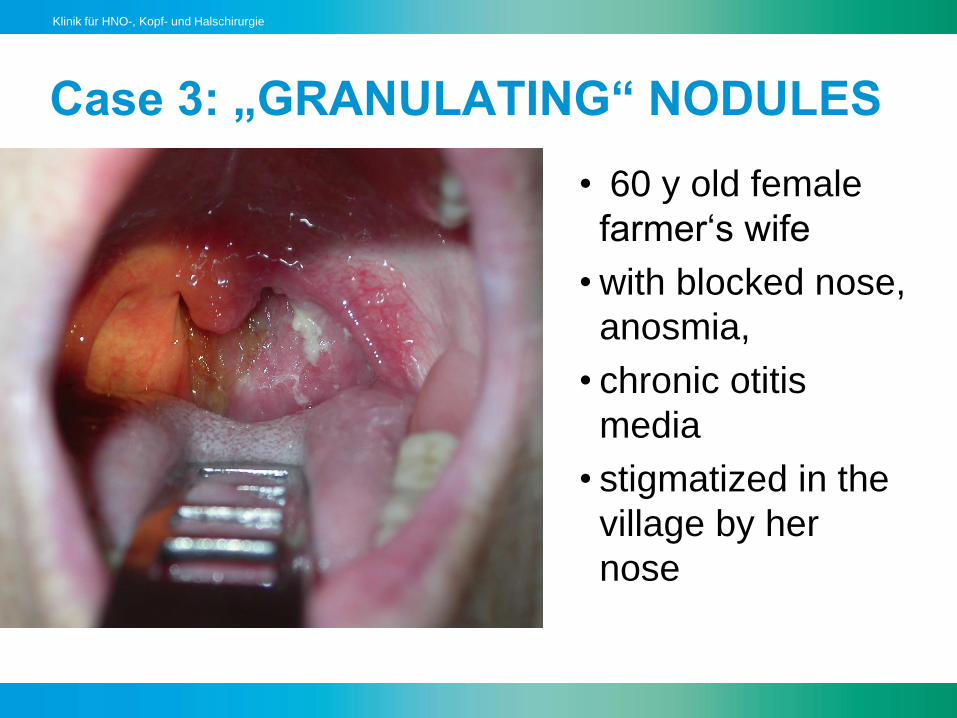
Case 3: „GRANULATING“ NODULES
• 60 y old female
farmer‘s wife
• with blocked nose,
anosmia,
• chronic otitis
media
• stigmatized in the
village by her
nose

Klinik für HNO-, Kopf- und Halschirurgie
Klinik für HNO-, Kopf- und Halschirurgie

Klinik für HNO-, Kopf- und Halschirurgie
Chronic Otitis media

Klinik für HNO-, Kopf- und Halschirurgie
Sarcoidosis
• DIAGNOSIS OF EXCLUSION of the granulamtous
diseases (GPA, specific infection (fungi, Tbc/MAI,
Leishmaniosis, foreign body granuloma)
Can involve every organ
• Rhinosinusitis, dacryostenosis 10%
• Sialadenosis e.g. Heerford Syndrom (febris uveo-
parotidea)
• Cutaneous: Lupus Pernio, Erythema nodosum (25%)

Klinik für HNO-, Kopf- und Halschirurgie
§
Granulomatous Dacryoadenitis

Klinik für HNO-, Kopf- und Halschirurgie

Klinik für HNO-, Kopf- und Halschirurgie
Palatal Fistula
Klinik für HNO-, Kopf- und Halschirurgie
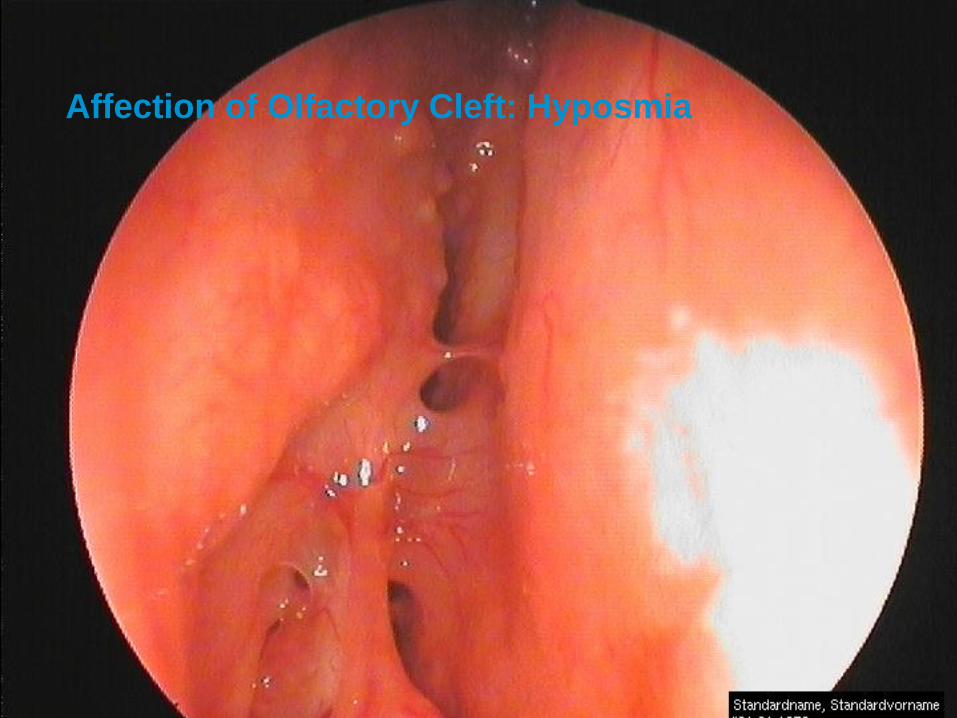
oAffection of Olfactory Cleft: Hyposmia
Klinik für HNO-, Kopf- und Halschirurgie
Sarcoidosis
• 100 to 200 per million(blacks 3-4x more frequent)
• Mulitsystemic granulomatous disease of unknown origin
Histologically characterized by non-caseating granulomas
• Typically manifested in young adults
• Lung >90% affected (50% subclinical presentation)
–Hilar lymphadenopathia
–Pulmonary reticular opacities
• Extrapulmonary sarcoidosis:
–Mostly Skin, eyes, reticulendothelial and musculosceletal
system, 10% also nervous system 5% heart disease.

Klinik für HNO-, Kopf- und Halschirurgie
Extrapulmonary Sarcoidosis
• Reticuloendothelial system commen: Lymphadenopathia
40%, hepato-splenomegalia 20%
• Skin 25%: Papules, plaques, erythema nodosum with e.g.
Löfgren Syndrome
• Eyes 20%:Uveitis, iritis
• URT involvement rare 10%: CRS and Laryngitis
• Renal (50% Calci-uria) and Neurological 4% (basal
meningitis)
• Exocrine glands 4%: Xerostomia, Xerophtalmia
• Bone: Zysts

Klinik für HNO-, Kopf- und Halschirurgie
Synopsis
• Sarcoidosis
• No ANCA
• Urine Ca ↑
(up to 40%)
• WBC normal
• Hilar
Lymphadeno
• ACE↑ in 50%
• Serum-Ca↑ in
10%
• EGPA
• p-ANCA
• Urine may be
abnormal
• > 10% Eos
• Pulmonary
infiltrates
• ACE normal
• Serum-Ca
normal
• GPA
• c-ANCA
• Urine red
casts and
proteine
• Tc and Lc ↑
• Pulmonary
nodules
• ACE normal
• Serum-Ca
normal

Klinik für HNO-, Kopf- und Halschirurgie
Therapy:
• Treatment of underlying systemic diseasse
(rheumatologist, nephrologist), rule out specific infections
(fungi, tbc…) and tumor
• Nasale irrigations (NaCl, Babyshampoo,…)
• Bactrim prophylaxis
• Topical steroids
• Systemic: Prednison, cyclophosphamide
• Azathioprine or methotrexat
• Biologicals….rituximab (moab to deplete B-cells)
• Surgery only if not avoidable (DCR,saddle nose correction)

Klinik für HNO-, Kopf- und Halschirurgie
Differential Diagnosis: Spezific
Rhinitis on infectious grounds
• Bilder aus www.google.ch/images

Klinik für HNO-, Kopf- und Halschirurgie
Spezific Rhinitis-Rhinosinusitis
Diagnose:
• Bilder aus www.google.ch/images

Klinik für HNO-, Kopf- und Halschirurgie
Spezifische Rhinitis-Rhinosinusitis
• Bilder aus www.google.ch/images
Klinik für HNO-, Kopf- und Halschirurgie
Spezific Rhinitis-Rhinosinusitis
• Eg Leshmaniasis
–Protozoon (transmitted by sandflies, host rodents,
marcrophages, endothelial cells)
– Lesions are defined by affected tissue types and host
response
•Leishmaniasis of the old world (Mediterranian area,
Alepobeule): superficial cutaneous form
•Viszerale form (Kala-Azar in India)
•Mukocutenous form (Espundia in Central- and South
America)

Klinik für HNO-, Kopf- und Halschirurgie
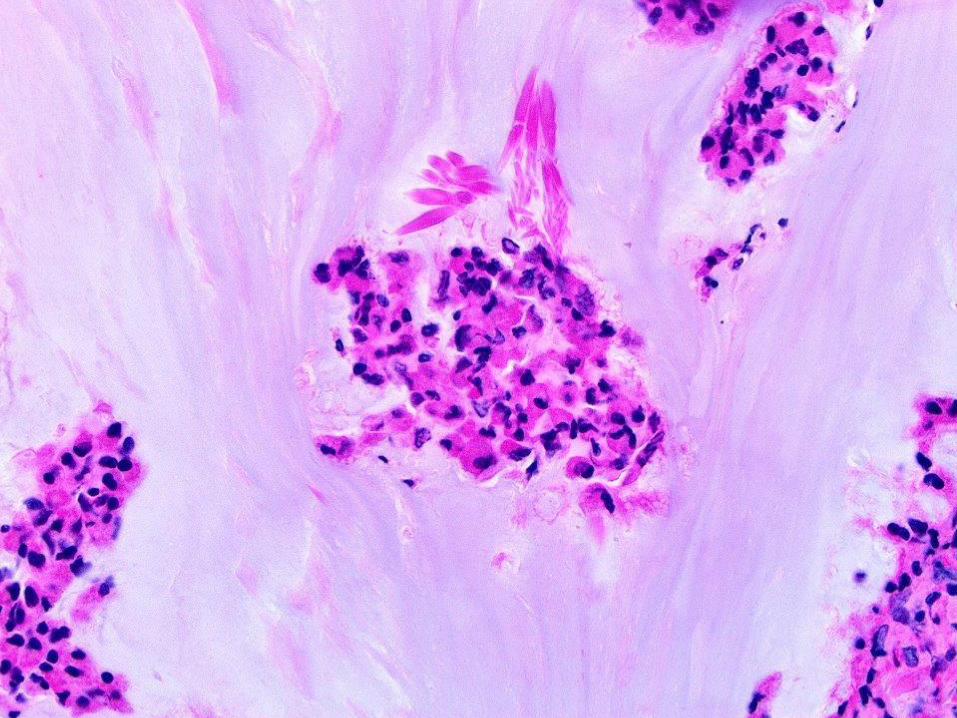
Spezifische Rhinitis-RhinosinusitisDiagnostics: microscopic
visualization of protozoon in
macrophages and endothelial
cells
Th: Antimon, Amphotericin B
Bild aus www.google.ch/images

Klinik für HNO-, Kopf- und Halschirurgie
• 50 000 species, only 300 pathogenic in humans
• Acute vs Chronic (longer than 12 weeks) infections
Non-invasive
• FUNGUS BALL («Truff», Aspergillom, Mycetom)
• ALLERGIC FUNGAL RHINOSINUSITIS: RARE (moist and
hot regions)
Invasive ((vs non-allergic eosinophilic RS))
• ACUTE INVASIVE: MUCOR (Aspergillus in case of acute
leucemia)
• CHRONIC INVASIVE: RARE (Granulomatous in dry hot
regions) and non-granulomatous form
Fungi

Klinik für HNO-, Kopf- und Halschirurgie
Chronic Mycetoma
• Left maxillary sinus: Typical brown fungus ball and
radiopaque inclusion on Rx (Mn, Mg, Hg,.. )
• Aspergillus fumigatus (75%), flavus (7%), Chrysosporium

Klinik für HNO-, Kopf- und Halschirurgie
ACUTE INVASIVE FUNGAL SINUSITIS
Cavernous sinus thrombosis by Mucor

Klinik für HNO-, Kopf- und Halschirurgie
Mucormycosis
• Immuno-compromised host (reduced innate immune
system)
–Ketoacidosis, severe neutropenia
• Molds on plants, angiotropism (invasion, thrombosis)
• Clinical signs:
• Pain, Necrosis (Eschar of the palate)
• GET TISSUE FOR HISTOLOGY: Angio-invasion and
thrombosis by Mucor (culture only in 50% later positive)
• Therapy: «Face-ectomy», Amphotericin B iv, correction of
underlying disease

Klinik für HNO-, Kopf- und Halschirurgie
Allergic fungal Rhinosinusitis
• Warm and hot climate (Saudi Arabia, Southern US)
• First detected in: Early recurrent polyposis, peanut butter
mucus (ie. eosinophilic mucin) in combination with Allergic
bronchopulmonary Aspergillosis with similar mucus plugs
in the lung.
• Diagnostic criteria
– Gell & Coombs type I hypersensitivity (history, skin, or serology)
– Polyposis
– CT findings
– Eosinophilic mucus;
– Positive fungal stain and no fungal invasion
Bent, Kuhn, Oto-HNS 1994;111:580-88
Meltzer, Hamilos, Hadley, Lanza, Marple, et. al. JACI 2004;114:S155-S212.

Klinik für HNO-, Kopf- und Halschirurgie
AFR: Serpigineous opacifications and polyps
source:
www.radiopaedia
Hyperdense
mass
in the sinus
and classical
serpiginous
hypodens rim

Klinik für HNO-, Kopf- und Halschirurgie

Klinik für HNO-, Kopf- und Halschirurgie
Allergic Mucin (Peanut butter)
• Gross findings -indistinguishable from ABPA
– Thick viscosity
– Tan, black, green
• Histology– Non-invasive fungus
• Grocott
• GMS
• H&E stains show
– Inflammatory cells
– Eosinophils
– Charcot-Leyden Crx
Klinik für HNO-, Kopf- und Halschirurgie
Klinik für HNO-, Kopf- und Halschirurgie
Treatment: (Caveat high recurrency rate)
• Establishing diagnosis
• Extensive surgery removing all «mucus plugs» and
creating large sufficient fenestration for gravity dependent
self clearance
• Aggressive post-op care with saline irrigation, office based
cleaning
• Long time steroids (duration controversial)
• Controversial: Antifungal (Azole) rinsing, immunotherapy

Klinik für HNO-, Kopf- und Halschirurgie
Defects of the Immune System: Primary Disease
• Innate system: Mucosal barriers, natural killer cells,
complement system
–Cystic fibrosis, primary cilliary dyskinesia
• Humoral System: 2/3 of defects of the immune system are
Immunglobuline associated diseases:
–Common Variable Immunodeficiency CVID (IgGs): variable
weakness for URT and GIT infections
–Selective IgA deficiency: 70% URT infections, otitis and
parotitis (rarely life threatening)
–Transiente Agammaglobulinemia of the newborne 6-
12months (3-6m to 2-3y) explains propensity to URT and GIT
infections
• Cellular and Combined Cellular/Humoral Defects

Klinik für HNO-, Kopf- und Halschirurgie
Secondary (Aquired) Immunodeficiencies
• Diabetes Mellitus, Hypothyreosis, Malnutrition
• Bone Marrow Transplantation: Brief but very serious
immunosuppression with bone marrow ablation
–Extremly sensitive to acute bacterial sinusitis (gram negative
or aerobic/anaerobic) or invasive fungal sinusitis
–Mucositis, lympadenopathia (tuberculosis)
• Solid Organ Transplantation: Delayed suppression of cell-
mediated immunity: Mostly established at 4w to 6m
–Viral infections EBV, CMV, HIV, Hep B and C
–Sinusitis (invasive fungal sinusitis is much rarer)
–Pneumonia

Klinik für HNO-, Kopf- und Halschirurgie
Aquired Immunodeficiencies
• Radiotherapy: Disruption of mucosal barriers and impaired
cellular immune response:
–Stomatitis (Candida in Xerostomia, reactivated HSV 1)
–Susceptibility to dental caries and gingivitis
• Chemotherapy: Direct effects on immune cells
–Stomatitis
–Leucocytes <500/cc
–Fungal infection especiall following anibiotic therapy
(Candida sepsis, Angioinvasive or pulmonary Aspergillosis,
Mucor rhino-orbito-frontal invasion)

Klinik für HNO-, Kopf- und Halschirurgie
Iatrogenic Immunosuppressant
• Mostly due to treatment of patient with vasculitis and
rheumotologic patients
• Prednisone 40-60mg/daily longer than 4 to 6 weeks
• Antiproliferative agents for B- and T- lymphocytes:
Methotrexat, Cyclophosphamide, Azathioprine,
Mycophenolate, Biologicals
• Immunophilin antagonist interfering with intracellular signal
transduction: Cyclosporin

Klinik für HNO-, Kopf- und Halschirurgie
Defects of the immune system: HIV Infection
• Look for untreated patients or acute infection
• 41-68% ENT manifestations (especially in acute infection)
• 70% generalized Lymphadenopathia and Waldeyer ring
hyperplasia
• Oral: 10% Ulcera (VZV with prodromal itching, CMV)
• HPV Papillome, mucosal Kaposi Sarkoma painfull blue-
livid nodules (Th: Surgery, Vinblastin injections, radiation)
• Oral hairy leukoplakia
• Candida mucositis (various forms: pseudomembranous,
erythematous, angular cheilitis, leukoplakia)
Klinik für HNO-, Kopf- und Halschirurgie
Acquired defects of immune system: HIV Infection
• Sinusitis only in 11-17%
–Adenoidhyperplasia and nasal obstruction (early stage)
–Sinunasal Kaposi Sarcoma DD: bacilliary angiomatosis
• External otitis with Pseudomonas, Aspergillus
• Ear canal Polyps by Tbc, Pneumocystis
• Parotid gland: Lymphoepithelial Cyst(s) DD: Sjögren
• Cave CD 4 Helper Cell Count <200/cc
• Laryngooesophagal Candidiasis, high indicence of chronic
RS, baciliary angiomatosis (Bartonella related)

Klinik für HNO-, Kopf- und Halschirurgie
SUMMARY AGAIN:
• ….in case of extremly prolongated or repetitive
disease
• RED FLAGS: THINK OF IT…AND CHECK
–Patients history: COCAINE, travel history, medication
–Autoimmune:
•c-/p-ANCA, urine sediment, creatinine, glucose
–Infections:
•Low threshold for biopsy: CULTURE AND HISTOLOGY
–Neoplasia (NK- T cell) lymphoma
•Deep biopsies in OR

Klinik für HNO-, Kopf- und Halschirurgie


















