South West Primary Care Alliance: Oxford November 29, 2017swpca.ca/Uploads/ContentDocuments/PCA...
71
SOUTH WEST PRIMARY CARE ALLIANCE: OXFORD NOVEMBER 7 TH , 2018 Sub Regional Clinical Lead: Dr. Jitin Sondhi Primary Care Alliance Co-Chair: Dr. Gerry Rowland
Transcript of South West Primary Care Alliance: Oxford November 29, 2017swpca.ca/Uploads/ContentDocuments/PCA...
-
SOUTH WEST PRIMARY
CARE ALLIANCE: OXFORD
NOVEMBER 7TH, 2018
Sub Regional Clinical Lead: Dr. Jitin Sondhi
Primary Care Alliance Co-Chair: Dr. Gerry Rowland
-
Agenda
• Review of Previous Minutes (completed online)
• Review of SRIT
• Oxford RAAM clinic
• Access to Team Based Care Survey
• Review and Feedback on Priorities
• FIT: Colon Cancer Screening update by CCO
-
RAAM Clinic in Oxford
• LHIN leadership approved clinic in Oxford
• Located in CHC
• Updates regarding timeline and opening will be posted
• Seeking physician to participate in the clinic• FFS
• No overhead costs
• Stipend weekly for participation in meeting
• Target audience are those with Opioid and Alcohol Use Disorders
• Team will consist of physician, NP and addictions and mental health counsellors on scene
• Goal is for rapid access from clinic and ED
-
Access to Team Based Care
• Improve access to FHO/FHG physicians
• Complete survey to help with my business plan and
proposal
• Goal is to respect physician autonomy in business
arrangement and not impact on resources available to
patients and providers based on type of practice.
• Survey takes 2 min at most
• Please do this now
• https://www.surveymonkey.com/r/MXC5C65
• Link is available in your newsletter sent October 4th, 2018
https://www.surveymonkey.com/r/MXC5C65
-
OXFORD SRIT Driver Diagrams
• Based on July meeting
• Drive work from SRIT members
• Please review and provide input directly to Jitin or Gerry.
-
Broaden access to
inter-professional
resources through
collaboration and
partnership
Availability of inter-professional resources
Collaboration between sectors and providers
Uptake of new models of coordination and planning
Primary Drivers Secondary Drivers Change Ideas
Advise and champion local initiatives -i.e., Clinical
Connect and CSSN Central Intake
Champion initiatives that increase access i.e., Rapid
Access to Addiction Medicine (RAAM) model
Champion uptake of Coordinated Care Plans
Communication with patients and caregivers
Providers are accountable to each other and to patients
Providers are aware of what services are available within
and across sectors
Access Driver Diagram
Providers have access todigital health records
Co-locate staff
Youth Wellness Hub
LHIN Home and Community Care relationship with
Primary Care
-
Create a shared understanding of
current initiatives and available programs
and resources to improve patient access and flow
Collaboration betweenproviders and sectors
Ease of navigation for online resources
Primary Drivers
Communication between providers
Secondary Drivers Change Ideas
Sector representatives to present to SRIT abouttheir
services
Links on provider websites toother regional services
Make thehealthline.ca more intuitive for patients and
caregiversCommunication with
patients and caregivers
Provider awareness of services available across
sectors
Availability of information online
Communication Driver Diagram
Communication between patients / peer-to-peer
groups
Communication with broader community
Peer-to-peer / community groups’ awareness of
programs and initiatives
Round table updates at each SRIT meeting
Provide information for local social media platforms
Communication with non-healthcare services related to social determinants of
health
SRIT to undertakeservice mapping exercise
Availability of paper-basedinformation
Providers know who to call in other sectors for client /
patient referrals SRIT to engage with City / County representatives when
needed
Broaden access to HealthChat
Presentations to service clubs (Optimists, Legion etc.)
Market health care services in the community (bulletin
boards / newspapers/ flyers)
-
Improve transitions for complex patients
being discharged from hospital through
system partnerships and collaboration
Communication betweenproviders and patients
Best-practices areimplemented
Provider access to digital health records
Primary Drivers Secondary Drivers Change Ideas
SRIT members champion uptake of Health Links CCPs within sectors
CMHA, CHC & NPLC access toCHRIS
IT support for primary care
Communication between providers
Uptake of Health Links Coordinated Care Plans
Transitions Driver Diagram
Focus on relationshipbuilding among providers
Primary Care Practitioner uptake of Emerg. Dept. notification software
SRIT champion Clinical Connect
SRIT champion CSSN Central Intake
Rounds and Situation Tables tohelp coordinate transitions
Patient experience incorporated into transition
planning / protocols
Proactively seek patient feedback ontransition experience
Share sector education at Care Coordination meetings
Sector updates at each SRIT meeting
SRIT to review IDEAS transitions pilot from Grey Bruce
Successful LHIN and / or provincial projects / pilots
that could be scaled
Discharge planning at admission
Co-location of staff
SRIT champion expansion of BSO Mobile Teams for LTC
-
Improve access to assisted living and
supportive housing through knowledge
transfer and accountability
Primary Drivers Secondary Drivers Change Ideas
Appropriate Residential Settings Driver Diagram TBD Fall 2018
-
Presenter Disclosure
12
• Dr. Jan Owen, Primary Care Lead
South West Regional Cancer Program
Dr. Brian Yan, Endoscopy Lead
South West Regional Cancer Program
• Relationships with commercial interests:
o Grants/Research Support: None
o Speakers Bureau/Honoraria: None
o Consulting Fees: None
o Other: Employees of Cancer Care Ontario
• Potential for conflict(s) of interest:
o None
• All information provided in presentation has been provided by Cancer
Care Ontario.
-
Learning Objectives
13
1. To describe how the colorectal cancer screening
process is changing in Ontario
2. To demonstrate how the fecal immunochemical test
(FIT) results in high yield colonoscopy
3. To discuss how primary care providers (PCPs)
should manage their patients who receive an
abnormal FIT result
-
Question
14
You have a patient who is 62 years old, with no family
history of colorectal cancer (CRC) and is asymptomatic.
She has recently moved to Canada and has never been
screened for CRC. How would you screen this individual for
CRC, assuming all of these tests were available to you?
a. Colonoscopy
b. gFOBT
c. FIT
d. Flexible sigmoidoscopy
e. No screening
-
• In 2018, it is estimated that approximately 6,376 men
will be diagnosed with colorectal cancer and
approximately 1,811 will die from it
• Second leading cause of cancer deaths.
• In 2018, it is estimated that approximately 5,219
women will be diagnosed with colorectal cancer and
approximately 1,548 will die from it
• Third leading cause of cancer deaths.
Colorectal cancer is the 2nd most commonly
diagnosed cancer in Ontario
Colorectal Cancer in Ontario
15
-
Ontario’s ColonCancerCheck (CCC) Program
• Canada’s first organized province-wide colorectal (CRC)
screening program
• CCC sends letters to eligible individuals
• Screening offered to ages 50-74
– Via primary care provider
– Average risk: guaiac fecal occult blood test (gFOBT)*
– Increased risk (≥1 FDR with CRC): colonoscopy
16
*flexible sigmoidoscopy (FS) every 10 years is an acceptable screening test
-
Sources: Tinmouth et al. Program in Evidence-based Care (PEBC) Evidence
Summary 2015; 15-14
gFOBT vs. No Screening
17
OutcomesRelative effect
(95% CI*)
# of person-years
(# of studies)
CRC mortality
(follow up range: 17-30
years)
RR* 0.87
(0.82 to 0.92)
5,344,100
(4 RCTs*)
CRC incidence
(follow up range: 17-30
years)
RR 0.96
(0.90 to 1.02)
4,866,448
(5 RCTs)
13% reduction in
death
*CI=confidence interval, RR= relative risk, RCT= randomized control trial
-
Impact of Organized Screening Through the
CCC Program
18
Between 2008 (launch of CCC) and 2014, over 4 million
CCC program gFOBTs have been completed
Estimated detection of 7,460 colorectal cancers
-
Organized CRC Screening in Canada
19
Fecal immunochemical test (FIT)=
in 8 provinces, 2 territories
-
20
CCC is planning to
implement FIT as the
recommended test for
people at average risk of
CRC
-
21
gFOBT vs. FIT Lab Parameters
gFOBT FIT
Measures Heme; non-specific Globin; human
Test technique Guaiac; peroxidase Immunochemical
Lower limit of blood
detection300–600 µg Hb/g* 10–20 µg Hb/g
InterferenceVitamin C, other
sources of HbNone
No dietary or medicine restrictions
Detects much smaller
levels of blood in stool
*Hb=hemoglobin
Source: Tinmouth J, et. al. Gut. 2015 Aug;
64(8):1327-37.
-
22
gFOBT vs. FIT Lab Parameters
gFOBT FIT
# of samples
required3 1
Lab process Manual Automated
Results Qualitative Qualitative or quantitative
StabilityLess stable at high
temperatures and over time
• Kit delivery and return
• Kit inventory management
-
23
• At-home stool sample screening test
• 1 sample
• Tube designed for easy sampling
• No dietary or medication restrictions
Easier to use
FIT Usability for Participants
-
Sources:
1.Lee JK, Liles EG, Bent S, Levin TR, Corley DA. Accuracy of fecal
immunochemical tests for colorectal cancer: systematic review and meta-analysis.
Ann Intern Med 2014;160:171-181.
2. Canadian Task Force on Preventive Health Care. Screening for Colorectal
Cancer [Internet]. Ottawa, Canada: Canadian Task Force on Preventive Health
Care; 2014. Available from: http://canadiantaskforce.ca/guidelines/published-
guidelines/colorectal-cancer/
Accuracy for CRC: One Time Test
24
Sensitivity Specificity
FIT
(n=19 studies)82% 94%
gFOBT
(n=9 studies)47.1% 96.1%
FIT is comparable to mammography & Pap test
-
*HRA= High risk adenoma
Source: Tinmouth et al. Program in Evidence-based
Care Evidence Summary 2015; 15-14
FIT vs. gFOBT – Clinical Implications
25
OutcomesRelative effect
(95% CI*)
# of person-years
(# of studies)
Participation rateRR 1.16
(1.05 to 1.28)
52,038
(6 RCTs*)
CRC/HRA* detectionRR 2.15
(1.58 to 2.94)
51,634
(5 RCTs)
• 2X more accurate
• Detects CRC and HRA
16% improvement
in participation
-
Adenoma to Cancer
26
FIT detects
gFOBT detects
CancerHRA
FIT has potential to reduce
the incidence of CRC
-
When will FIT be Available in Ontario?
Funding Communications
Program
design
Laboratories
ITQuality
assurance
• Until further notice: gFOBT remains the recommended CRC
screening test in Ontario
• We are actively working towards FIT: coming soon!
27
-
FIT vs. Colonoscopy
28
-
Quintero: FIT vs. Colonoscopy
29
Large RCT in
Spain
Ages 50-69
Biennial FIT vs.
one-time
colonoscopy
Primary outcome:
CRC- death at 10
years
Reflects only first
round results
Mailed invitation
to participate
Source: Quintero E., et. al., NEJM 2012;366:697-706
-
Quintero: Patients Prefer FIT
26,599
invited for FIT
1% offered
FIT
opted for
colonoscopy
23% offered
colonoscopy
opted for FIT
26,703
invited for colonoscopy
36% responded 28% responded
30
FIT is preferred by patients when given the option
-
Quintero: Diagnostic Yield- Intention to Screen
31
Colonoscopy
n=26,703
FIT
n=26,599
P-value
CRC detection 30 33Not
significant
HRA 514 231
-
Question
32
After you explain the benefits of FIT, your patient still feels
they may want to have a colonoscopy and asks about
potential risks. What are the risks associated with
colonoscopy?
a. Colonoscopy-related perforation
b. Post-polypectomy bleeding
c. Risks related to bowel preparation
d. Risks related to the use of sedation
e. All of the above
-
Answer
33
e. All of the above
-
Colonoscopy Associated Complications: Calgary
34
Complication
N=18,456
Total # adverse events: 119
Event rate*
*per 1,000 colonoscopies
Bleeding 2.93
Perforation 0.22
Post-polypectomy syndrome 0.16
Cardiac 0.22
Syncope/hypertension 0.27
GI symptoms (minor and transient) 1.95
Splenic/hepatic hematoma 0.11
Other 0.60
Colonoscopy is not a benign procedure
-
Screening with Colonoscopy vs FIT
35
FIT: more people screened • same number of
colonoscopies • more cancers detected
Outcome Yield Yield
CRC 400 8,000
HRA 10,000 45,000
Average risk
colonoscopyFIT+ colonoscopy
20x
4.5x
yield
with FIT
1.3 million screened100,000 screened
100,000 scoped 100,000 scoped
-
FIT Experience in Alberta
36
-
Colorectal Cancer Screening in Alberta
37
Before fecal immunochemical test FIT roll out:
• Primary care providers preferred colonoscopy over gFOBT
• Only 23.5% gFOBT participation in Calgary zone
Introduction of FIT:
• Rapid uptake of the test
• 31‒35% FIT participation in Calgary zone
• Primary care providers quickly saw value of screening with
FIT
-
38
0
500
1000
1500
Ref
erra
l Vol
ume
July/13 Oct Jan/14 April July Oct Jan/15 Apr July Oct Jan/16 AprMonth
Urgent Priority Urgent
Moderate Routine
by Triage Priority
CCSC Monthly Referral Volumes
FIT introduced Nov 20130
50
01
000
15
00
Re
ferr
al V
olu
me
Jan/13 Apr Jul Oct Jan/14 April July OctMonth
gFOBT+/FIT+ Average Risk for CRC
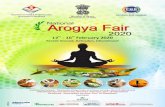
Figure 3: 2013-14 Monthly Referral Volumes
FIT Roll Out: Impact on Colonoscopy in Calgary,
Alberta
0
500
1000
1500
Refe
rral V
olume
July/13 Oct Jan/14 April July Oct Jan/15 Apr July Oct Jan/16 AprMonth
Urgent Priority Urgent
Moderate Routine
by Triage Priority
CCSC Monthly Referral Volumes
Introduction of FIT
Source: Alberta Health Services. First Year Experience with the Fecal
Immunochemical Test. June 2015.
-
Calgary: Lesions Detected at Colonoscopy
39Source: Alberta Health Services. First Year Experience with the Fecal
Immunochemical Test. June 2015.
-
Benefits of FIT: Summary
40
Better test usability
Increased participation
More follow-up colonoscopies
Higher positivity rate
More cancers and HRAs
detected
Increased sensitivity
Anticipated decrease in CRC
incidence and mortality
-
FIT vs. Colonoscopy: Summary
41
• Patients prefer FIT
• FIT is safer than colonoscopy
• FIT is as good as colonoscopy at detecting CRC in
average risk people
• FIT-positive colonoscopy is high yield – colonoscopy used
in people most likely to benefit
FIT → better risk–benefit ratio of screening
The CCC program does not recommend screening for
average risk people with colonoscopy
-
Transition to FIT
42
-
CCC Eligibility Criteria for FIT
43
Eligibility criteria have not changed
Note: Patients must have a valid Ontario Health Insurance Plan number
-
Question
44
Your patient is a 56 year old woman who had a colonoscopy
completed in 2016 following an abnormal (positive) gFOBT
result. Her scope revealed one small hyperplastic polyp on
the sigmoid colon. When and how should she next be
screened?
a. Re-screen in 10 years with colonoscopy
b. Re-screen in 10 years with FIT
c. Re-screen in five years with colonoscopy
d. Re-screen in two years with FIT
e. Re-screen in two years with colonoscopy and biennially
thereafter
-
Answer
45
b. Re-screen in 10 years with FIT
• As per ColonCancerCheck Surveillance Guidelines1,
average risk people with hyperplastic polyps in the rectum
or sigmoid colon should re-screen in ten years with a FIT.
Following a normal colonoscopy, people at average risk of
colorectal cancer do not need to continue to re-screen with
colonoscopy, and the patient should return to screening
with the FIT in ten years.
• As outlined within ColonCancerCheck Screening
Recommendations2, people ages 50-74 without a family
history of colorectal cancer could choose to be screened
with flexible sigmoidoscopy every 10 years instead of FIT.
-
Confirm mailing
address for FIT kit, patient
address & date of birth*
Explain to patient how to complete
FIT
Submit completed
FIT requisition to central lab
Lab will mail pre-labelled
FIT kit to patient
How to Order FIT for Patients
46
* People who live on a First Nation reserve can request a FIT kit through a health centre or nursing station.
Step 1 Step 2 Step 3 Step 4
Submit completed
FIT requisition to central lab*
Lab will mail pre-
labelled FIT kit to
patient
-
Requisition Changes
47
Regular lab requisition
cannot be used to
request CCC program
FIT
CCC gFOBT will be
removed from regular
lab requisition
-
New FIT Requisition
48
• Valid for 6 months
from lab receipt
• Supports patients
who are home
insecure
-
Ensure Your Patients Get Their FIT
49
Alternate FIT kit delivery
option
Confirm that patient address
information is up-to-date:
• to obtain a FIT kit
• to receive results
-
Why Centralized Distribution?
50
Program challenges Future State (FIT)
• 11.1% of program gFOBT
require re-testing
• Majority of rejected tests due
to mislabeling
• gFOBT shelf-life: 3 years
• FIT shelf life: 12-18 months
Pre-labeled kits
with patient
identifiers
Inventory
management at
central site
-
Completing FIT: 3 Steps for Patients
51
Check label accuracy and clearly record
specimen collection date on
FIT tube
Complete FIT
Mail or drop off completed FIT to the lab as soon
as possible*
Step 1 Step 2 Step 3
-
52
FIT Return
Completed FIT kit should be returned as soon as possible
to the lab
• Mail
o Regular mail
o Expedited mail included for some areas
• Drop off at lab specimen collection centres
• Cancer Care Ontario is working on confirming options to
support FIT return for people living on a First Nation
reserve and in rural and remote areas
-
53
Supporting Patients
• Patient-friendly FIT
materials are being
developed, including FIT
instructions that use more
visuals than words
• FIT instructions will be
available in 20+ languages
and in accessible format
online
-
*For people ages 50–74.
FIT Results and Follow-Up by PCP
54
PCP will arrange for
follow-up colonoscopy
to be performed within
8 weeks
Do NOT repeat FIT
Results
Repeat FIT in the next
few weeks– new
requisition required
Normal result
Abnormal result
Invalid result or
rejected deviceLab will send FIT
result to primary
care provider (PCP)
Cancer Care Ontario
will send FIT result
letter to patient
-
55
Supporting Patients
• Patients will continue to receive CCC program
correspondence
o Invitations/recalls
o Reminders
o Results
• Physician-linked correspondence helps
increase screening rates
-
The Patient Perspective
56
An abnormal FIT result can be stressful for your
patient and their family
• Explain that an abnormal FIT:
o Needs timely follow-up with colonoscopy within eight
weeks
o Is NOT a cancer diagnosis
o Can identify a polyp before it becomes cancerous
-
How to Manage Patients
with an Abnormal FIT
57
-
Follow-Up of Abnormal FIT Results
58
Time to colonoscopy after gFOBT+ result
2 months 4 months 6 months
48% of people receive a
colonoscopy within 8 weeks
of a gFOBT+ result
Approximately 20% of
individuals are lost to
follow-up at 6 months
Benchmark: follow-up within 8 weeks
-
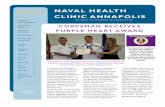
Importance of Follow-Up
59
Follow-up
No follow-up
Patients with an abnormal FIT who do not undergo colonoscopy are
more likely to die from CRC
Source: Lee et al., Association Between Colorectal Cancer Mortality
and Gradient Fecal Hemoglobin Concentration in Colonoscopy
Noncompliers. J Natl Cancer Inst (2017) 109(5)
-
60
Importance of Timely Follow-Up
Impact of diagnostic delay is seen within months
- Significantly higher risk of CRC after 6 months
Time to colonoscopy
after FIT+% cases receiving colonoscopy after FIT+
Any CRC Advanced-stage CRC
8-30 days 2.97% 0.81%
2 months 2.78% 0.70%
3 months 3.06% 0.69%
4-6 months 3.14% 0.88%
7-12 months 4.56% 1.49%
>12 months 7.55% 3.13%
Source: Corley et al. JAMA 2017;317(16):1631-41.
-
Carefully Consider Where Follow-Up Occurs
61
• FIT+ colonoscopies are more complex → require more
expertise, time and resources
-
Question
62
You have a patient who is 62 years old, with no family
history of colorectal cancer (CRC) and is asymptomatic.
She has recently moved to Canada and has never been
screened for CRC. How would you screen this individual for
CRC, assuming all of these tests were available to you?
a. Colonoscopy
b. gFOBT
c. FIT
d. Flexible sigmoidoscopy
e. No screening
-
Screening Until FIT is Available
63
Do not delay!
Continue to screen your patients with gFOBT
until FIT is available through the CCC program
-
Clinical Pearls
64
Use FIT, not colonoscopy
FIT+ colonoscopy needed within 8 weeks
Centralized FIT kit distribution will minimize errors
Screen with gFOBT until FIT is available
-
Questions?
65
-
Appendix
66
-
67
Considerations
• Post polypectomy surveillance recommendations are primarily
intended for endoscopists to ensure appropriateness of
colonoscopy
– When referring for endoscopist surveillance, include prior scope &
path report if available
• How should PCPs manage cases where endoscopist
recommendation does not align with surveillance guidelines?
• Endoscopist recommendation may be influenced by other factors not
accounted for in the surveillance guidelines, such as quality of
colonoscopy:
– Adequate bowel preparation, complete procedure to cecum,
careful examination of colonic mucosa
• Guidelines can be used to assist discussion with endoscopists
-
68
CRC Mortality in LRA vs General Population
• 25% significant relative risk reduction in CRC mortality of
LRA vs. general population
– Standardized mortality ratio = 0.75 (95% CI: 0.63–0.88)
Loberg et al. N Engl J Med 2014
CRC Mortality in Low Risk Adenoma vs.
General Population
-
69
Switching to FIT After Average Risk Colonoscopy
Systematic Review: Risk of advanced neoplasia and
death with low risk adenomas
• No evidence to support surveillance in people with LRA
– Lower risk of CRC and CRC mortality compared to
the general population
– Small increase in relative risk for high risk adenoma at
4-10 years compared to those with normal
colonoscopy
-
Patient Attachment
70
• PCPs can still register to
accept and roster new
patients who require
follow-up
• Code Q043A or Q053A
-
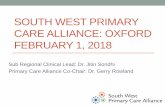
Evaluation: Physician Linked vs. Unlinked letters
Uptake of FOBT in 6 months
16.9
9.2
0
20
40
60
Summary
Resp
on
den
ts (
%)
PCP linked 2012 Unlinked 2012
%
%