Sonography for Surveillance of Patients With Crohn Disease
6
Sonography for Surveillance of Patients With Crohn Disease rohn disease is a chronic inflammatory condition of the bowel characterized by periods of quiescence and inflam- matory activity or “disease flares.” Although genetic factors, dysbiosis, and altered immunity are implicated in inflammatory bowel disease, the etiology is unknown. 1 The peak age of onset is early in life, between 15 and 40 years, thus affecting patients during their most productive years with potential for substantial social and personal costs. 2,3 Crohn disease tends to complicate over time, with the development of fistulas and fibrostenotic lesions. As a result, sur- gical intervention rates in the prebiologic era were high. 4 However, early and appropriate medical management can alter the course of this disease, with reductions in surgical rates and hospitalization. 3,5 Detection of disease activity through objective monitoring is key to changing the long-term outcome and disability. Monitoring clinical symptoms alone is inadequate: the presence or absence of these does not reflect disease activity. Routine endoscopic moni- toring is also not feasible because it is an invasive examination with associated risks and the need for preparation. Computed tomogra- phy (CT) with dedicated small-bowel imaging or enterography has been the modality of choice to date, but there is mounting evidence questioning its safety and repeatability, given ionizing radiation exposure in these young patients. 6,7 Magnetic resonance imaging (MRI) is a radiation-free alternative and has also been shown to be effective in detection of inflammatory activity. 8 However, this modality is expensive, and the lack of access precludes routine use. Transabdominal sonography is a highly effective modality for detecting inflammatory activity in Crohn disease, equal to that of CT or MRI. 9,10 Sonography is particularly sensitive in detecting ileocecal Crohn disease compared to the reference standard ileo- colonoscopy and thus is a useful initial screening tool to aid in diagnosis. 11 Postoperative Crohn disease recurrence is also reli- ably detected with sonography, a suggested surrogate for endo- scopic evaluation. 12,13 It is an effective modality in the detection of complications such as strictures, fistulas, and abscesses, with sur- gical pathologic confirmation showing sensitivity as high as 100%. 14 Although there are little existing data on the utility of any transmural modality in routine monitoring of disease activity in asymptomatic patients, there is a move toward more frequent obser- vation, given the disconnect between symptoms and disease. Sonog- raphy is a superb modality for monitoring stable patients with a Kerri L. Novak, MSc, MD, FRCPC, Stephanie R. Wilson, MD, FRCPC Received May 7, 2012, from the Department of Medicine, Division of Gastroenterology (K.L.N., S.R.W.), and Department of Radiology (S.R.W.), University of Calgary, Calgary, Alberta, Canada. Revision requested May 17, 2012. Revised manu- script accepted for publication June 5, 2012. Address correspondence to Stephanie R. Wilson, MD, FRCPC, Foothills Medical Center, 1403 29th St NW, Calgary, AB T2N 2T9, Canada. E-mail: stephanie.wilson@albertahealth- services.ca Abbreviations CT, computed tomography; MRI, magnetic resonance imaging C ©2012 by the American Institute of Ultrasound in Medicine | J Ultrasound Med 2012; 31:1147–1152 | 0278-4297 | www.aium.org SOUND JUDGMENT SERIES Invited paper The Sound Judgment Series consists of invited articles highlighting the clinical value of using ultrasound first in specific clinical diagnoses where ultrasound has shown comparative or superior value. The series is meant to serve as an educational tool for medical and sonography students and clinical practitioners and may help integrate ultrasound into clinical practice.
Transcript of Sonography for Surveillance of Patients With Crohn Disease

Sonography for Surveillance of PatientsWith Crohn Disease
rohn disease is a chronic inflammatory condition of thebowel characterized by periods of quiescence and inflam-matory activity or “disease flares.” Although genetic factors,
dysbiosis, and altered immunity are implicated in inflammatorybowel disease, the etiology is unknown.1 The peak age of onset isearly in life, between 15 and 40 years, thus affecting patients duringtheir most productive years with potential for substantial social andpersonal costs.2,3 Crohn disease tends to complicate over time, withthe development of fistulas and fibrostenotic lesions. As a result, sur-gical intervention rates in the prebiologic era were high.4 However,early and appropriate medical management can alter the course ofthis disease, with reductions in surgical rates and hospitalization.3,5
Detection of disease activity through objective monitoring iskey to changing the long-term outcome and disability. Monitoringclinical symptoms alone is inadequate: the presence or absence ofthese does not reflect disease activity. Routine endoscopic moni-toring is also not feasible because it is an invasive examination withassociated risks and the need for preparation. Computed tomogra-phy (CT) with dedicated small-bowel imaging or enterography hasbeen the modality of choice to date, but there is mounting evidencequestioning its safety and repeatability, given ionizing radiationexposure in these young patients.6,7 Magnetic resonance imaging(MRI) is a radiation-free alternative and has also been shown to beeffective in detection of inflammatory activity.8 However, thismodality is expensive, and the lack of access precludes routine use.
Transabdominal sonography is a highly effective modality fordetecting inflammatory activity in Crohn disease, equal to that ofCT or MRI.9,10 Sonography is particularly sensitive in detectingileocecal Crohn disease compared to the reference standard ileo-colonoscopy and thus is a useful initial screening tool to aid indiagnosis.11 Postoperative Crohn disease recurrence is also reli-ably detected with sonography, a suggested surrogate for endo-scopic evaluation.12,13 It is an effective modality in the detection ofcomplications such as strictures, fistulas, and abscesses, with sur-gical pathologic confirmation showing sensitivity as high as100%.14 Although there are little existing data on the utility of anytransmural modality in routine monitoring of disease activity inasymptomatic patients, there is a move toward more frequent obser-vation, given the disconnect between symptoms and disease. Sonog-raphy is a superb modality for monitoring stable patients with a
Kerri L. Novak, MSc, MD, FRCPC, Stephanie R. Wilson, MD, FRCPC
Received May 7, 2012, from the Department ofMedicine, Division of Gastroenterology (K.L.N.,S.R.W.), and Department of Radiology (S.R.W.),University of Calgary, Calgary, Alberta, Canada.Revision requested May 17, 2012. Revised manu-script accepted for publication June 5, 2012.
Address correspondence to Stephanie R.Wilson, MD, FRCPC, Foothills Medical Center,1403 29th St NW, Calgary, AB T2N 2T9, Canada.
E-mail: [email protected]
AbbreviationsCT, computed tomography; MRI, magneticresonance imaging
C
©2012 by the American Institute of Ultrasound in Medicine | J Ultrasound Med 2012; 31:1147–1152 | 0278-4297 | www.aium.org
SOUND JUDGMENT SERIES
Invited paper
The Sound Judgment Series consists ofinvited articles highlighting the clinicalvalue of using ultrasound first in specificclinical diagnoses where ultrasound hasshown comparative or superior value. Theseries is meant to serve as an educationaltool for medical and sonography studentsand clinical practitioners and may helpintegrate ultrasound into clinical practice.
3108online.qxp:Layout 1 7/19/12 10:40 AM Page 1147

number of additional advantages: it is inexpensive andwidely available, and real-time imaging with potential for 3-dimensional reconstruction can optimally characterizecomplications such as partial small-bowel obstruction. It issafe and noninvasive with easy repeatability and patient tol-erability. Inflammatory activity, reflected by excess bloodflow in the bowel wall, is shown on color Doppler imagingand more sensitively with the use of contrast agents, withpotential for actual quantification and objective measure-ment of blood flow and therefore inflammatory activity.15
Although sonography of the bowel is a highly effec-tive modality, there are limitations. First, operator experi-ence and expertise are more important in evaluation ofthe bowel compared to sonographic evaluation of otherabdominal organs. Acquisition of technical expertise andadequate time are essential to survey the entire smalland large bowel. The reproducibility of sonographicinflammatory parameters is a commonly suggested limita-tion of bowel sonography; however, there is strong evidencethat inter-rater agreement on key parameters such as bowelwall thickness is high.16
Consistent identification of the anatomic site of inflam-mation is also identified as a potential limitation. More than80% of patients with Crohn disease have small-bowelinvolvement, often the distal terminal ileum. Patients withactive Crohn disease generally have a distinctively thick-ened bowel, which becomes relatively gasless compared tothe normal bowel. This condition creates a mass effect.Therefore, as disease worsens, the pathologic characteris-tics improve the likelihood of detection. Areas that may bemore challenging to identify include those deeper withinthe pelvis (rectum or ileoanal pouch) and proximal smallbowel (duodenum). Considerable challenges may also arisewith a complex surgical history, and accurate identificationof the anatomic location can be limited in this circumstance.
Obesity, particularly body mass indices of 30 orgreater, may hamper a sonographic study of any portionof the abdomen. Failure of sonography should not be pred-icated on body habitus alone, however. A low body massindex with little abdominal wall fat is advantageous forsonography compared to CT and MRI, which are bothimproved by the presence of intra-abdominal fat.
Complications associated with Crohn disease are wellappreciated on sonography, but open fistulas and drainagesites may be problematic in patients with severe fistulizingdisease, limiting transducer placement on the skin. In addi-tion, discomfort may further limit examination. Complexfistulizing disease is often readily identified; however, theremay be challenges associated with mapping of tracks, givensurrounding inflammation and tethering, similar to any
other modality. Certainly, partial small-bowel obstructionsare shown on real-time sonography, and examination ofcomplex disease is generally well tolerated by patients,given the lack of bowel preparation or need for contrastagents.
Although the above factors are considerations in thechoice of sonography for the study of the bowel, as avidultrasound enthusiasts, we support the use and choice ofsonography as a first-line modality for evaluation of allpatients with Crohn disease, both for routine surveillanceand for evaluation at the time of acute exacerbation.
Case Description
A 38-year-old man with long-standing ileocolonic Crohndisease diagnosed at 21 years of age underwent emergentileocolonic resection at presentation for suspected acuteappendicitis. He was well for a decade, but after symptomsof intermittent severe abdominal pain developed, he wasreferred to gastroenterology. Ileocolonoscopy revealed anulcerated and stenosed ileocolic anastomosis with a com-pletely normal colon. He also had a cutaneous perianalopening with active drainage on perianal examination,consistent with a perianal fistula. He was given combina-tion therapy of infliximab and methotrexate and was inclinical remission for 2 years with normal blood test resultsand a lack of perianal symptoms. A sonographic examina-tion performed 1 year after initiation of medical therapyshowed no abnormalities with no evidence of inflam-matory activity, including the perianum.
One year later, the patient continued to be in clinicalremission, with no symptoms of Crohn disease, other thanintermittent scant drainage from his known perianal cutaneous opening. Subsequent surveillance sonographicexaminations, however, revealed dramatic interval deterioration with extensive small-bowel thickening(Figure 1, A and B), hyperemia of the bowel on colorDoppler imaging (Figure 1, C and D), abundant mesen-teric inflammatory fat, and proximal disease in a skip lesion distribution. There were also multiple sites of nar-rowing with incomplete mechanical bowel obstruction(Figure 1, E–G), evidenced by fluid-filled dilated seg-ments of the small bowel with to-and-fro peristalsis beforesegments with constant luminal apposition and wall thick-ening. The total length of the abnormal bowel was esti-mated to be 40 cm. Maximal wall thickness was measuredat 8 mm. In addition, a clear intersphincteric rectocuta-neous fistulous tract was identified on transperinealsonography (Figure 1H) without associated complica-tions, specifically no ischiorectal fossa abscess.
Novak and Wilson—Sonography for Surveillance of Patients With Crohn Disease
J Ultrasound Med 2012; 31:1147–11521148
3108online.qxp:Layout 1 7/19/12 10:40 AM Page 1148

J Ultrasound Med 2012; 31:1147–1152 1149
Novak and Wilson—Sonography for Surveillance of Patients With Crohn Disease
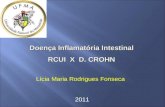
Figure 1. Images from a 38-year-old man with Crohn disease for 17 years who previously underwent ileocolic resection. He was feeling well after
2 years of taking infliximab and methotrexate for recurrent disease in the neoterminal ileum. A previous sonographic examination 1 year earlier
yielded normal findings, showing a marked initial positive response to therapy. The following images are from a surveillance scan. A and B, Long-
axis and axial images of the neoterminal ileum show marked wall thickening with some loss of wall layering. The bowel measures 9 mm in thick-
ness (threshold is 3 mm). C and D, Corresponding color Doppler images. The profuse easily shown blood flow is a reflection of active inflammation.
(continued)
A B
C D
3108online.qxp:Layout 1 7/19/12 10:40 AM Page 1149

Commentary
The lack of clinical symptoms despite active disease, con-firmed on endoscopy, is well documented.17 Furthermore,postoperative recurrence of Crohn disease is almostinevitable over time, and the need for a second operationin the absence of medical therapy is high.18 Many of thesepatients remain asymptomatic despite disease recur-rence. Alternatively, the number of patients with Crohndisease who have typical symptoms such as diarrhea andabdominal pain in the context of quiescent disease is high,
approaching 60%.19,20 Therefore, differentiating activefrom inactive disease clinically is challenging. Serologicmeasures of inflammation such as C-reactive protein arealso unreliable in consistently detecting disease.21 There-fore, other noninvasive means of routinely evaluating theinflammatory activity in patients with Crohn disease isimperative to detect disease and prevent complicationseven when patients feel well. Sonography is an idealmodality for this purpose. It is key in the routine manage-ment of inflammatory bowel disease in a number of coun-tries in Europe and in our department.
Novak and Wilson—Sonography for Surveillance of Patients With Crohn Disease
J Ultrasound Med 2012; 31:1147–11521150
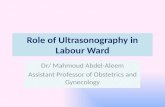
Figure 1. (continued) E, Fixed angulation of a very thick and black neoterminal ileum, well proximal to the anastomosis. On the left, the lumen shows
fixed apposition, and on the right, there is fluid distention suggesting an element of stricture. There is abundant echogenic inflammatory fat. F, At a
point more proximal in the neoterminal ileum, there is dilated bowel on the left with an abrupt transition to thick bowel with luminal apposition on the
right, suggestive of another stricture with incomplete mechanical bowel obstruction. G, At yet another point more proximal, there is a fixed, very
acute angulation of a thickened segment. Dilated fluid-filled bowel is shown both proximally and distally. H, Axial transperineal view of the anal canal.
There is a hypoechoic inflammatory mass (arrows) posterolateral to the left side of the anal canal. The internal opening, in the 6-o’clock position
directly posterior, is slightly more caudal and not shown here. Impression: active recurrent disease of the neoterminal ileum. There is a multifocal
stricture, fixed acute angulation, incomplete mechanical bowel obstruction, and a perianal inflammatory mass.
E F
G H
3108online.qxp:Layout 1 7/19/12 10:40 AM Page 1150

The interval or frequency for transmural monitoringof Crohn disease is uncertain. In the case described here,the surveillance interval was likely too long: despite highlyeffective medical therapy and the absence of clinical symp-toms, the patient had severe active persistent diseasedetectable 1 year after an examination yielded normalfindings. This situation is not uncommon: a substantialnumber of patients who respond initially to biologictherapy lose the response over time.22 The referencestandard target for assessing the response to medicaltherapy is endoscopic, to establish mucosal healing, butfrequent routine endoscopic evaluation is not acceptableto most patients. There are no clearly established surro-gates for mucosal healing in widespread use, but sono-graphic assessment is certainly a candidate. There is a needfor a validated scoring system reflecting sonographicinflammatory activity to be included with other measuresof disease activity.
Wall thickness measurement is central to sonographicdetermination of disease activity.23,24 However, the additionof color Doppler evaluation of the bowel in this case furtherillustrates the severity of the disease. This combined demon-stration of severe disease strongly substantiates the presenceof inflammation; therefore, contrast- enhanced sonographyif performed is less additive in this case. Although contrastenhancement is a powerful tool for showing inflammation,this case is an excellent example of demonstrated severeactive disease without the requirement for either intravenousaccess or contrast agent injection.
Given the predilection of Crohn disease for the ter-minal ileum and right colon, a sonographic examinationstarts with axial orientation of the right flank from thehepatic edge to the right iliac fossa looking for the wall andgas shadow suggestive of the ascending colon. Once local-ized, the terminal ileum is identified at the ileocecal valve.The remainder of the colon can generally be continuouslyfollowed from the ascending colon to the rectum. Fur-thermore, because of their fixed mesenteric locations, thesegments of the colon can all be identified on the basis oftheir known locations and positions within the abdomen.
The entire small bowel is systematically evaluated byperforming a series of axial scans from the right flank to theleft flank with overlap of the scanning planes. The smallbowel is not as easy to strictly identify; however, both thelocation and appearance are helpful. The jejunum is local-ized in the left upper quadrant with a characteristic feath-ery appearance of the valvulae conniventes. The smallbowel in the 3 remaining quadrants is more likely to beileum, with a more variable appearance.
Selection of the correct ultrasound probe is criticalfor successful sonographic evaluation of the bowel. Theinitial survey may be performed with a 4- to 6-MHz probefor systematic identification of thickened segments ofbowel and evidence of complications. These low- frequency evaluations are necessary to avoid overlookingdeeply positioned fluid collections. Localized regions ofinterest should then undergo detailed evaluation withhigher-frequency probes (7–9 MHz), either linear orcurved, for superior bowel wall resolution. In women,endovaginal probes are ideal to study both the rectosig-moid colon and portions of the terminal ileum locateddeep in the true pelvis. Finally, the ultrasound machineshould be optimized for high contrast and low flow oncolor Doppler imaging.
For many years, we have performed transperinealsonographic evaluation of the anal canal and perianal softtissues in patients with Crohn disease who have knownfistulas or perianal pain. The technique is established asan accurate modality in both men and women, withpotential for the addition of transvaginal scanning toincrease accuracy in women.25 The identification of inter-nal and external openings, inflammatory tracts, and anyassociated abscess is noninvasive, accurate, and easilyrepeated, facilitating close monitoring.26,27 Thus, moni-toring responses to both surgical and medial therapy ofperianal disease is readily accessible. Transrectal sonog-raphy can facilitate characterization of disease in patientswith more proximal disease or supralevator extension ofinflammatory changes. This examination can be painfulfor patients, however, and is infrequently performed forthis indication in our center.
Fibrostenotic complications or strictures are areas offixed luminal apposition with dilated proximal bowel,often accompanied by excess and dysfunctional to-and-fro peristalsis. Accurate assessment of the degree towhich the stricture is inflammatory versus fibrotic innature continues to be a challenge regardless of thetransmural imaging modality. The inflammatory activ-ity of a stricture is similar to non-narrowed thickenedbowel with an increased blood supply, shown onDoppler imaging, which may be further characterizedwith microbubble contrast agents. Contrast furtherincreases the sensitivity for detecting inflammation.15
Elastography used to evaluate bowel wall stiffness is apromising technology that may prove helpful in discern-ing the predominant etiology of the stricture. It is cur-rently being investigated in our center.
J Ultrasound Med 2012; 31:1147–1152 1151
Novak and Wilson—Sonography for Surveillance of Patients With Crohn Disease
3108online.qxp:Layout 1 7/19/12 10:40 AM Page 1151

Summary
Crohn disease is a complex chronic systemic inflammatorydisease that frequently has complications and requires closemonitoring to prevent disability. Current medical therapieshave demonstrated success in the alteration of the naturalhistory; however, a substantial number of patients do notrespond to medical therapy or lose the response over time,as shown here. There is a shift in the management of Crohndisease to move beyond symptoms in identifying diseaseactivity early and to treat to target, with mucosal healing asthe goal, and not just for improvement of symptoms. Sono-graphic measurements of wall thickness and blood flow tothe bowel wall are accurate measures of disease activity.Sonography is an excellent surrogate for mucosal healing,with easy repeatability so that frequent assessments can bemade to facilitate early intervention.
References
1. Hansen TS, Jess T, Vind I, et al. Environment factors in inflammatorybowel disease: a case-control study based on a Danish inception cohort.J Crohns Colitis 2011; 5:577–584.
2. Ekbom A, Helmick C, Zack M, Adami HO. The epidemiology of inflammatory bowel disease: a large, population-based study in Sweden.Gastroenterology 1991; 100:350–361.
3. Lichtenstein G, Yan S, Bala M, Blank M, Sands BE. Infliximab mainte-nance treatment reduces hospitalizations, surgeries, and procedures in fis-tulizing Crohn’s disease. Gastroenterology 2005; 128:862–869.
4. Schwartz DA, Loftus EV Jr, Tremaine WJ, et al. The natural history offistulizing Crohn’s disease in Olmsted County, Minnesota. Gastroenterology2002; 122:875–880.
5. Feagan BG, Panaccione R, Sandborn WJ, et al. Effects of adalimumabtherapy on incidence of hospitalization and surgery in Crohn’s disease:results from the CHARM study. Gastroenterology 2008; 135:1493–1499.
6. Brenner DJ, Hall EJ. Computed tomography: an increasing source of radi-ation exposure. N Engl J Med 2007; 357:2277–2284.
7. Peloquin JM, Pardi DS, Sandborn WJ, et al. Diagnostic ionizing radiationexposure in a population-based cohort of patients with inflammatorybowel disease. Am J Gastroenterol 2008; 103:2015–2022.
8. Dinter DJ, Chakraborty A, Brade J, et al. Endoscopy and magnetic reso-nance imaging in patients with Crohn’s disease: a retrospective single-centre comparative study. Scand J Gastroenterol 2008; 43:207–216.
9. Horsthuis K, Bipat S, Bennink RJ, Stoker J. Inflammatory bowel diseasediagnosed with US, MR, scintigraphy, and CT: meta-analysis of prospec-tive studies. Radiology 2008; 247:64–79.
10. Panés J, Bouzas R, Chaparro M, et al. Systematic review: the use of ultra-sonography, computed tomography and magnetic resonance imagingfor the diagnosis, assessment of activity and abdominal complications ofCrohn’s disease. Aliment Pharmacol Ther 2011; 34:125–145.
11. Sturm EJ, Cobben LP, Meijssen MA, van der Werf SD, Puylaert JB.Detection of ileocecal Crohn’s disease using ultrasound as the primaryimaging modality. Eur Radiol 2004; 14:778–782.
12. Castiglione F, Bucci L, Pesce G, et al. Oral contrast-enhanced sonogra-phy for the diagnosis and grading of postsurgical recurrence of Crohn’sdisease. Inflamm Bowel Dis 2008; 14:1240–1245.
13. Pallotta N, Giovannone M, Pezzotti P, et al. Ultrasonographic detectionand assessment of the severity of Crohn’s disease recurrence after ilealresection. BMC Gastroenterol 2010; 10:69–70.
14. Gasche C, Moser G, Turetschek K, Schober E, Moeschl P, OberhuberG. Transabdominal bowel sonography for the detection of intestinal com-plications in Crohn’s disease. Gut 1999; 44:112–117.
15. Ripollés T, Martinez MJ, Paredes JM, Blanc E, Flors L, Delgado F. Crohndisease: correlation of findings at contrast-enhanced US with severity atendoscopy. Radiology 2009; 253:241–248.
16. Fraquelli M, Sarno A, Girelli C, et al. Reproducibility of bowel ultra-sonography in the evaluation of Crohn’s disease. Dig Liver Dis 2008;40:860–866.
17. Rutgeerts P, Geboes K, Vantrappen G, Beyls J, Kerremans R, Hiele M.Predictability of the postoperative course of Crohn’s disease. Gastroen-terology 1990; 99:956–963.
18. Wolters FL, Russel MG, Sijbrandij J, et al. Phenotype at diagnosis predictsrecurrence rates in Crohn’s disease. Gut 2006; 55:1124–1130.
19. Keohane J, O’Mahony C, O’Mahony L, O’Mahony S, Quigley EM,Shanahan F. Irritable bowel syndrome-type symptoms in patients withinflammatory bowel disease: a real association or reflection of occultinflammation? Am J Gastroenterol 2010; 105:1788, 1789–1794.
20. Barratt SM, Leeds JS, Robinson K, et al. Reflux and irritable bowel syn-drome are negative predictors of quality of life in coeliac disease andinflammatory bowel disease. Eur J Gastroenterol Hepatol 2011; 23:159–165.
21. Borivant M, Leoni M, Taricotti D, Fais S, Squarcia O, Pallone F. The clin-ical significance of serum C reactive protein levels in Crohn’s disease: resultsof a prospective longitudinal study. J Clin Gastroenterol 1988; 10:401–405.
22. Hanauer SB, Feagan BG, Lichtenstein GR, et al. Maintenance infliximabfor Crohn’s disease: the ACCENT I randomised trial. Lancet 2002;359:1541–1549.
23. Migaleddu V, Scanu AM, Quaia E, et al. Contrast-enhanced ultrasono-graphic evaluation of inflammatory activity in Crohn’s disease. Gastroen-terology 2009; 137:43–52.
24. Tarján Z, Tóth G, Györke T, Mester A, Karlinger K, Makó EK. Ultrasoundin Crohn’s disease of the small bowel. Eur J Radiol 2000; 35:176–182.
25. Maconi G, Adrizzone S, Greco S, Radice E, Bezzio C, Bianchi Porro G.Transperineal ultrasound in the detection of perianal and rectovaginal fis-tulae in Crohn’s disease. Am J Gastroenterol 2007; 102:2214–2219.
26. Viganò C, Losco A, Caprioli F, Basilisco G. Incidence and clinical out-comes of intersphincteric abscesses diagnosed by anal ultrasonography inpatients with Crohn’s disease. Inflamm Bowel Dis 2011; 17:2102–2108.
27. Stewart LK, McGee J, Wilson SR. Transperineal and transvaginal sonog-raphy of perianal inflammatory disease. AJR Am J Roentgenol 2001;177:627–632.
Novak and Wilson—Sonography for Surveillance of Patients With Crohn Disease
J Ultrasound Med 2012; 31:1147–11521152
3108online.qxp:Layout 1 7/19/12 10:40 AM Page 1152