SOME RECENT ADVANCES IN FOETAL PHYSIOLOGY · The foetal circulation. The course of the foetal...
8
RECENT ADVANCES IN FOETAL PHYSIOLOGY Based on a Lecture given at the Combined Post Graduate School of Queen Charlotte's Hospital and the Chelsea Hospital for Women By S. G. CLAYTON, M.D., M.S., F.R.C.S., M.R.C.O.G. Assistant Obstetric and Gynaecological Surgeon, Kinig's College Hospital; Assistant Obstetric Surgeon, Queen Charlotte's Hospital In I90I Ballantyne's ' Plea for a pro- maternity hospital' led to the first establish- ment of hospital beds for the specific purpose of studying the physiology and pathology of pregnancy. Although he quickly realized and strongly urged. the value of antenatal care to the mother, Ballantyne's original aim was chiefly to discover means of saving foetal life ' to prevent miscarriage and that most terrible of all events the dead birth, and to cure before birth the diseases and deformities of the foetus.' Parsons (1946) has emphasized that infant care must begin before birth, and only by a study of the normal can we hope to understand the abnormal. For this reason a mere obstetrician ventures to review a little of the recent work of physiologists, arbitrarilv selecting topics suitable for inclusion in a short article. Oxygenation of the foetus. Barcroft and many others have made great contributions to this subject. The foetal tissues require large amounts of oxygen, 1.25 ml. per kilo per minute at term (Haselhorst and Strom- berger I932), and special physiological mech- anisms are necessary to supply the increasing foetal demands, though it cannot be over- stressed that there are wide differences between the placentae of different species, and the results of animal experiments must not be applied to man without reserve. i. Increased oxygen could be supplied by increasing the oxygen content of maternal blood, but actually the oxygen capacity of maternal blood falls during pregnancy to 15.5 volumes per cent. (nornmal I9 vols. per cent.) because of the lowered red cell count and reduced alkali reserve. 2. An increased flow of maternal blood through the uterus would serve the same pur- pose, and in fact occurs, but in rabbit experi- ments the flow lags behind the increasing foetal needs, as is shown by the progressive fall in the oxygen content of the blood in the uterine veins. (Barcroft et al., 1933, 1934.) 3. An increased flow of foetal blood through the placenta would have the same effect. The foetal blood pressure rises progressively during pregnancy in the sheep and the volume of blood traversing the placenta increases, though at term the gain is only proportional to the rise in foetal weight. (Barcroft et al., 1939.) 4. The ' diffusion constant ' of the placenta might alter, that is the ease with which oxygen can cross the placental barrier. Diffusion is slow in the syndesmochorial placenta of the cow., but this observation cannot reasonably be applied to the human haemochorial placenta: In late pregnancy the trophoblast covering the villi is thinner, but the total area of villi does not increase after mid-pregnancy after which maximal foetal growth occurs. 5. The foetal blood has an increased avidity for oxygen. Foetal blood at term contains over 15.5 gm. of haemoglobin per ioo ml. and has an oxygen capacity of 2I volumes per cent. It is commonly stated that this is due to a high red cell count, but during early foetal life the count is low, and at term human cord blood is not polycythaemic. The poly- cythaemia appears within an hour after birth (Wintrobe and Schumacker, 1936). But though the corpuscles are not more numerous, they are larger and have a higher mean haemoglobin content. The interesting discovery has been made that in many species foetal haemoglobin has different qualities from adult haemoglobin. In the goat, for example, Barcroft and his co- workers (1934) found that the oxygen dis- 474 SOME Protected by copyright. on October 29, 2020 by guest. http://pmj.bmj.com/ Postgrad Med J: first published as 10.1136/pgmj.23.264.474 on 1 October 1947. Downloaded from
Transcript of SOME RECENT ADVANCES IN FOETAL PHYSIOLOGY · The foetal circulation. The course of the foetal...

RECENT ADVANCES IN FOETALPHYSIOLOGY
Based on a Lecture given at the Combined Post Graduate School of Queen Charlotte's Hospital andthe Chelsea Hospitalfor Women
By S. G. CLAYTON, M.D., M.S., F.R.C.S., M.R.C.O.G.Assistant Obstetric and Gynaecological Surgeon, Kinig's College Hospital; Assistant Obstetric Surgeon,
Queen Charlotte's Hospital
In I90I Ballantyne's ' Plea for a pro-maternity hospital' led to the first establish-ment of hospital beds for the specific purposeof studying the physiology and pathology ofpregnancy. Although he quickly realized andstrongly urged. the value of antenatal care tothe mother, Ballantyne's original aim waschiefly to discover means of saving foetal life
' to prevent miscarriage and that mostterrible of all events the dead birth, and to curebefore birth the diseases and deformities ofthe foetus.' Parsons (1946) has emphasizedthat infant care must begin before birth, andonly by a study of the normal can we hope tounderstand the abnormal. For this reason amere obstetrician ventures to review a little ofthe recent work of physiologists, arbitrarilvselecting topics suitable for inclusion in ashort article.
Oxygenation of the foetus. Barcroft andmany others have made great contributionsto this subject. The foetal tissues requirelarge amounts of oxygen, 1.25 ml. per kiloper minute at term (Haselhorst and Strom-berger I932), and special physiological mech-anisms are necessary to supply the increasingfoetal demands, though it cannot be over-stressed that there are wide differences betweenthe placentae of different species, and theresults of animal experiments must not beapplied to man without reserve.
i. Increased oxygen could be supplied byincreasing the oxygen content of maternalblood, but actually the oxygen capacity ofmaternal blood falls during pregnancy to15.5 volumes per cent. (nornmal I9 vols. percent.) because of the lowered red cell countand reduced alkali reserve.
2. An increased flow of maternal bloodthrough the uterus would serve the same pur-
pose, and in fact occurs, but in rabbit experi-ments the flow lags behind the increasingfoetal needs, as is shown by the progressivefall in the oxygen content of the blood in theuterine veins. (Barcroft et al., 1933, 1934.)
3. An increased flow of foetal blood throughthe placenta would have the same effect. Thefoetal blood pressure rises progressively duringpregnancy in the sheep and the volume ofblood traversing the placenta increases, thoughat term the gain is only proportional to therise in foetal weight. (Barcroft et al., 1939.)
4. The ' diffusion constant ' of the placentamight alter, that is the ease with which oxygencan cross the placental barrier. Diffusion isslow in the syndesmochorial placenta of thecow., but this observation cannot reasonably beapplied to the human haemochorial placenta:In late pregnancy the trophoblast covering thevilli is thinner, but the total area of villi doesnot increase after mid-pregnancy after whichmaximal foetal growth occurs.
5. The foetal blood has an increased avidityfor oxygen. Foetal blood at term containsover 15.5 gm. of haemoglobin per ioo ml.and has an oxygen capacity of 2I volumes percent. It is commonly stated that this is dueto a high red cell count, but during earlyfoetal life the count is low, and at term humancord blood is not polycythaemic. The poly-cythaemia appears within an hour after birth(Wintrobe and Schumacker, 1936). But thoughthe corpuscles are not more numerous, they arelarger and have a higher mean haemoglobincontent.The interesting discovery has been made
that in many species foetal haemoglobin hasdifferent qualities from adult haemoglobin. Inthe goat, for example, Barcroft and his co-workers (1934) found that the oxygen dis-
474
SOME
Protected by copyright.
on October 29, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.264.474 on 1 O
ctober 1947. Dow
nloaded from

October 1947 CLAYTON: Some Recent Advances in Foetal Physiology 475
sociation curve of foetal blood shows a ' shiftto the left,' while the maternal blood curveshows a ' shift to the right,' meaning that alow oxygen tension foetal blood will take upmore oxygen than maternal blood. The curvesare differently shaped, so that the foetal curveis steeper at low oxygen pressures. The shiftof the maternal curve is due to the reducedalkalinity of maternal blood. The alteredfoetal curve is due to the presence of a differenttype of haemoglobin. (Roos and Romijin,I938. McCarthy, I933.)
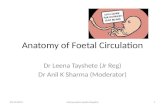
In man the curve for solutions of foetalhaemoglobin does not show the same results(Harrowitz, 1935), but the same general state-ment is true for whole foetal blood; its oxygendissociation curve lies ' to the left ' of that ofthe mother's blood. (Eastman et al., 1933.) Inother words, foetal blood can take up oxygenat tensions at which maternal blood losesoxygen. For technical reasons it is mostdifficult to discover the actual saturation ofthe blood entering and leaving the placentain man. The published results are discussedby Windle (1940) who concludes that unmbilicalvein blood is about 70 per cent. saturated, ahigher figure than is usually given.
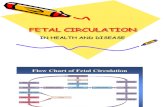
The foetal circulation. The course of thefoetal circulation has been studied in the foetallamb by cineradiology after the injection ofradio-opaque fluid into the circulation, byBarclay, Franklin and Pritchard (i944). Theyalso made comparative anatomical studies andit is reasonable to apply their conclusions tothe human foetus. They firmly support theWolff-Ziegenspeck theory of the intra-cardiaccourse of the, foetal blood; which states thatblood from the superior vena cava leaves theright auricle through the tricuspid valve, whilethe blood from the inferior vena cava splits intotwo streams. The larger left stream directlyenters the left auricle through the foramenovale, while the smaller right stream mixeswith the blood from the superior vena cavain the right auricle. In the particular pointof the splitting of the inferior caval stream thistheory differs from both the classical theoriesof crossed streams (Sabatier) and total mixture(Pohl-Kellogg). It does not conflict with theview that the blood in the left ventricle ismore oxygenated than that in the rightventricle. The inferior caval stream splits on
the posterior free curved edge of the interatri a 1septum (crista dividens) which is shown inthe diagrams.
s" .vC
*v\\ g.> --C-D,l.CRA.
/ RN...
L' -:,V..
FIG. I.-Diagram to show Barclay et al.'s conception ofCrista dividens.
The same workers studied changes thatoccur in the circullation at birth, and onlyfrom lack of space do we fail to review all theirconclusions, but two details of particularobstetric interest may be mentioned. (i)Before closure of the umbilical circulationblood normally enters the foetus from theplacenta, partly accounting for the postnatalpolycythaemia, and providing a foetal reserveof the constituents of haemoglobin. In man50 ml. passes on the average (Haselhorst andAllmeling, 1930). (2) The extra-abdominalparts of the umbilical vessels are not in-nervated (Spivack, I943), but they contractactively from the placental end first whenrespiration is established. In man, mechanicalstimulation is relatively slight, and the stimulusis uncertain. Cooling, fall of blood pressureor of oxygen tension are not found to beconstant factors. (The reviewer wonders ifthe contraction of the uterus on the placentamay play some part in closing the circulationthrough it.)The foetal heart rate has been studied in
various species, but incompletely in man.WTindle (I940) correlates the observations ofseveral workers and concludes that ' the foetalheart pumps blood about as fast as it can with-out much control by the nervous system.' Thevagi are capable of conduction during foetal
Protected by copyright.
on October 29, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.264.474 on 1 O
ctober 1947. Dow
nloaded from

176 POST GRADUATE MEDICAL JOURNAL October I947
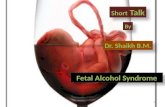
,I ERATR4AL -SEPTUM*(ISTA DIVIDfN-S
IA.AVA-L E .OF"';
FORAMEtj -0X Id,,. S.''': '
FIG. 2.-Diagram of Cblique Cardiac section. Modified from Ziegenspeck I905.
life in some species, but vagal slowing is lessthan in adults. In the human foetus at term,unlike other species, the blood pressure isprobably higher than the threshold for theaortic and carotid sin,us reflexes, so that slow-ing of the foetal heart may occur if the bloodpressure rises (Marey reflex). This wouldaccount for the slowing of the foetal heart withuterine contractions, when the pressure risesin the umbilical veins. Anoxia will also causebradycardia by direct effect on the pacemakerof the heart (Bauer, I98) and this mayaccotnt for the more dangerous and persistentslowing that occurs in prolonged labour.
Foetal respiratory movements. AlthoughAhlfeld observed respiratory movements inthe human foetus in utero in i888, thesemovements have only been carefully in-vestigated recently. Reliable observations aredifficult to secure, for the mere opening of theuterus sets up abnormal conditions. Barcroftand Barron (I937) and Barcroft (I942) de-scribed the respiratory movements of thefoetal lamb and have put forward an attractivetheory to explain the events observed, but itis fair to remark that alternative theories arepossible (Windle, 1940), and that only doubtfLlconfirmation of the events, let alone thetheory, has been possible in the human foetus.The lamb has a gestation period of about
147 days, and the foetus was observed throughthe amnion after opening the uterus underspinal anaesthesia. The first response toexternal stimulation is observed on the 34thday, when stimulation of the area just belowthe eye (Vth nerve ending) causes a singletwitch of the head. At first stimulation o
other areas is ineffective, but gradually thesensitive area extends, and other muscles alsorespond, including the diaphragm. After atime rhythmical movements appear, and bythe 42nd day the foetus easily responds tostimulation, giving an initial writhing move-ment, which is followed by rhythmical res-piratory movements. If the foetus is asphyx-iated these responses cease.
Between 50 and 6o days a dramatic changeoccurs. The foetus becomes unresponsive tostimuli, and this quiescence persists until afterdelivery. During this stage asphyxia restoresthe earlier foetal activity, and responses similarto those of the earlier stage reappear. Barcroftand Barron suggested that foetal movementswere inhibited by a higher centre, which couldbe paralysed by asphyxia, when the lowerpattern of movement reappeared. They sec-tioned the brain stem of the foetus above thepons, and found that the responsivenessreturned.There is no space to discuss much recent
work on the wider problems of the genesis ofreflexes and nervous activity in the foetus.(See Windle, I940, for discussion and refer-ences.) The human foetus is certainly nottotally inert in late pregnancy, and apart fromlimb movements many complex reflexesnormally occur, for example swallowing, andany inhibition cannot be unselective. Speciesdifferences are very real; the opossumbreathes independently I2 days after concep-tion, when it climbs up to the mother's pouch!Many investigatidns have been nmade of the
response of the foetal respiratory centre tooxygen lack and carbon dioxide excess, and
Protected by copyright.
on October 29, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.264.474 on 1 O
ctober 1947. Dow
nloaded from

October I947 CLAYTON: Some Recent Advances in Foetal Physiology 477
100
LJI1f
zLLi
0
toomm OXYGEN TENSION
FOETAL BLOODPREGNANT WOMANNON PREGNANT
FIG. 3.-From Eastnen et al. Johns Hopkins Hospital Bulletin.
the importance of the subject to the obstetricianjustifies detailed discussion. Windle and hisco-,workers (I938) found clear evidence thatcarbon dioxide stimulated the respiratorycentre of the foetal cat. When the motherbreathed pure oxygen the foetus was inert;with 8-io per cent. carbon dioxide in oxygenrapid shallow respiration occurred; with5-8 per cent. oxygen in nitrogen the motherbecame cyanosed and foetal gasping occurred.Similar results were obtained in the guinea-
pig (Windle et al., 1939), but only inconstantresults in the rabbit (Snyder et al., I937).Barcroft and his colleagues (I940) investigatedthe foetal sheep and- found that respiratorymovements did not occur when the bloodleaving the brain was 30 per cent. saturatedwith oxygen, and began when this blood wasI0-25 per cent. saturated. Eastman andothers (I933) estimated the oxygen and carbondioxide content of human cord blood atbirth, and found that apnoea prevailed when
Protected by copyright.
on October 29, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.264.474 on 1 O
ctober 1947. Dow
nloaded from

POST GRADUATE MEDICAL JOURNAL
the blood was more than 50 per cent. sat-urated with oxygen irrespective of the carbondioxide level; the observations did not permitfull deduction of the part played by carbondioxide at lower oxygen levels.Though unproven, it is believed that the
human foetal centre responds to the samestimuli as the adult centre, though at a higherthreshold. If the oxygen saturation is over50 per cent. there is apnoea irrespective of thecarbon dioxide concentration. If the oxygensaturation falls the centre responds to thespecific stimulus of carbon dioxide, becomingmore sensitive as the oxygen level falls, untilabout 25 per cent. oxygen saturation is reached.At that level there is gasping reminiscent ofLumsden's primitive type of respiration, andbelow that level the centre is paralysed and willnot respond to any stimulus. Apart from in-creasing the sensitivity of the centre to carbondioxide it is doubtful if oxygen lack has anydirect effect on the centre, though Barcroft(1942) suggests that gasping respiration maybe a direct response to oxygen lack. The partplayed by aortic and carotid sinus reflexes isunknown.At the moment of birth the respiratory centre
is sensitized by anoxaemia, and bombardedby afferent stimuli. Cutaneous stimuli due tomanipulations and cold (Barcroft, 1941) arereinforced by stimuli from muscles and jointsnewly exposed to the full effect of gravity,and by internal stimuli set up by the changesin the circulation.
Intrauterine respiratory movements maydraw liquor amnii into the lungs, but certainlyonly in small quantities unless asphyxialgasping occurs (Windle et al., I939).
Maternal diet and foetal development. Noreview of the mass of new work on foetalmetabolism and placental transmission ispossible here, and only a brief survey of theeffect of maternal diet on the development ofthe foetus. As regards the total diet, maternaldeficiency has little effect on human birthweight, unless at starvation level (Ebbs et al.,1942) (Peoples League, I942). In the sheepimpaired maternal nutrition in the first two-thirds of pregnancy has little effect on foetaldevelopment, but underfeeding in the lastthird lowers the birth weight (Wallace, I944).On the other hand overfeeding did not affect
the foetal weight, though the weight of theewe increased (Hammond, 1933). Summerlambs weigh more on the average than springlambs, and Toverud (I933) found the same inchildren. It is suggested that the differenceis due to the better quality rather than quantityof food. A child of fuil weight may be born to apoorly fed mother, and this may be explainedby the principle of ' competing metabolism,'which "states that where there is a commonsource of supply, more active tissues will takeup more nutrient than less active. The foetaltissues have a high metabolic rate and competesuccessftilly against the maternal tissues.Apart from inherited factors, the weight ofoffsprinlg may be related to that of the motherbecause of this principle. The foal of a shirestallion and Shetland mare is small, whereasthe foal of a Shetland stallion and shire mareis large; the rapid metabolism of the smallerShetland mare competes more successfullywith that of the foetus (Walton and Hammond,1938).Apart from gross weight, inadequate diet
may affect development and postnatal health.The possible relationship of dietary deficiencyto anatomical abnormality is mentioned later.Huggett (I94I) has given figures which indicatethat over two-thirds of the foetal substance isbuilt up in the last trimester of pregnancy:
Composition of the human foetus in gms.Lunar Bodymonth wt. Water Protein Fat Ash
Fifth .. 300 26o 22 3 5 1.5Seventh I000 8oc 100 25 30Tenth .. 3200 2420 400 350 9o
Average daily deposition in gms.Through-out preg-nancy .. II.4 8.6 I.4 1.25
Last threemonths.. 26.2 19.3 3.6 3.9
Lastmonth. . 35.7 23.6 6.4 5.0
0.32
0.71
2.0
The same applies to the foetal content ofnitrogen, calcium, phosphorus and iron (Swan-son and Iob, I939) The following approxi-mate figures illustrate the point:
Composition of the human foetus in gms.Lunarmonth Nitrogen Calcium Phosphorus IronFifth . 2 z o.IosSeventh .. ii 3 0.0Tenth ...S 15 0.3
'478 October I1947P
rotected by copyright. on O
ctober 29, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.264.474 on 1 October 1947. D
ownloaded from

CLAYTON: Some Recent Advances in Foetal Physiology4
During the last third of pregnancy the foetusbuilds up a store of various essential mineralsand vitamins, many of which are short duringthe 'negative phase' that follows birth. Ifthere is a deficient maternal diet, or if pre-mature birth occurs, the infant has poorreserves and is more likely to suffer frompostnatal deficiency disease, and to show suchdisease earlier than other infants. For ex-ample, with maternal iron deficiency postnatalanaemia may occur (Parsons, 1932), and Ebbset al. (1941) state that anaemia and rickets aremore frequent in the children of women takinga poor diet than in the children of those whosediet was supplemented in the last three monthsof pregnancy. Mellanby (193I) showed howantenatal nutrition can affect the teeth, evenof the permanent dentition.
Developmental abnormalities. Lastly, we mayperhaps refer to a subject that is as muchpathological as physiological. As Professor ofTeratology at Edinburgh, Ballantyne wouldhave been interested in modern embryology,which is largely physiological in method.By unconscious convention we have looselyreserved the term 'congenital abnormality'for structural defect of unknown cause; andindeed as soon as a cause is found the disease isclassified under some other! heading. Forexample hydrops foetalis was formerly re-garded as an anomaly of development, we nowspeak of haemolytic disease.
Developmental abnormalities can be dividedinto two groups:
i. Primary, due to the genetic structure ofthe zygote, which Mx e have no present means ofaltering.
2. Secondary, due to adverse influencesacting on-the embryo, and here we have moreknowledge, partly based on the experiments ofSpemann, Harrison, and Child. It was foundthat if a developing embryo was exposed tothe action of a noxious agent, abnormalitiesof structure were produced which were in-dependent of the nature of the agent, and onlydepended on the stage of development reached.Such diverse agents as heat and cold, radiation,and various chemical substances were used.The embryo shows ' axial gradients,' and atany particular stage of development the mostactive regions of the embryo are relativelyelectronegative and are mlore susceptible to
toxic agents. Although the cxperiments havenot been confirmed in mammals, the sameprinciple that ' teratolQgical agents are non-specific' may be found true for humanembryos. What agents are possible in man ?
i. Abnormal maternal diet. There is littleevidence that human anatomical abnormalitiesare due to maternal dietary deficiencies;though Maxwell (I929) described foetal ricketsin cases of maternal ostemalacia, this is atleast in theory a reversible foetal change. Itis doubtful how far conclusions based onanimal dietary experiments can be applied tohuman pregnancy. For example the effectof vitamin E deficiency in producing abortionin rats has been the basis for the therapeuticuse of this substance. In the rat part of theplacenta is vascularized by yolk sac vessels,and in vitamin E deficiency these vessels ares t r a-n gl e d b y proliferation o f yolk sacmesoderm. The human placental vessels are ofallantoic origin, and vitamin E deficiency wouldnot be expected to have the same result inmnan. Again in species with epitheliochorial(pig) or syndesmochorial (cow) placentae,maternal iodine deficiency causes foetal athy-reosis, but this does not occur in man, asmaternal thyroxin can cross the placentalbarrier in man. (Smith, I9I9.) In animalsgross nutritional deficiencies will producesevere abnormality; for example, oculardefects in the litter of a sow with vitamin Alack, and skeletal defects with various de-ficiencies in rats (Warkany et al., 1943; War-kany, 1945). Further studies are needed in man.
2. Impaired placental circulation. Theeffect of impaired :placental circulation inproducing abnormalities is illustrated by theacardiac monstrosity found wit4 uniovulartwins, and by cases of advanced ectopicgestation, in which as many as half of theinfants are abnormal.
3. Intrauterine pressure and ' amniotic ad-hesions.' The possibility that a few abnor-malities such as talipes are sometimes due tointrauterine pressure cannot be totally denied,but Streeter (I935) has shown that ' in-trauterine amputations' and ' amniotic ad-hesions' are not due to pressure but to afailure of vascularization .and differentiationin the tissues involved. Such deformities areoften multiple, and are possibly due to the
October 1947 479P
rotected by copyright. on O
ctober 29, 2020 by guest.http://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.23.264.474 on 1 October 1947. D
ownloaded from

480 POST GRADUATE MEDICAL JOURNAL October I947
action of some adverse agent on the limb budsat their critical stage of active proliferation.
4. Virus or other infection. Gregg (1941)first noticed the association between maternalrubella in early pregnancy and congenitalcataract and heart disease. Other observershave confirmed his findings and attributedother defects such as deafness, mental defect,microcephaly, and dental abnormalities to thesame cause (Swan et al., I943, 1944, 1946;Martin, i945). There is some suggestiveevidence that other virus infections may alsoproduce defects (see Editorial, Lancet, 1947),but we are not concerned here with detaileddiscussion of this evidence but only with thebroad fact that intrauterine infection willdisturb the normal physiology of development.The majority of abnormalities due to rubellaoccur with infection during the first threemonths; with later infection many infantsescape. Swan found the average time of in-fection in cases of cataract and of deafnesscorrespond with the critical embryonic agesfor the development of eye or ear, and Evans(I944) found the same for dental defects.With later infection, when organogenesis islargely complete, gross abnormalities of struc-ture are not produced, and foetal reaction re-sembles that of the newborn.
5. Hormones. In some species male sexualhormones produced by one twin will affect a
second twin, producing a sterile freemartin.(Lillie, 1917, 1923; EIughes, I929.) Pseudo-hermaphroditism has been experimentally pro-duced in rats by injection of heterosexualhormones (Greene and Burrill, 1939), butthere is no evidence that human anatomicalabnormalities are produced by maternal ortwin hormones.There is no real division between the gross
abnormalities that we have been discussingand foetal disease of later onset. Once themain embryonic systems are laid downadverse agents could not be expected toproduce gross defects, but the more subtleabnormalities of the central nervous system,for example, are of the same essential nature,in that tracts developing at the particulartime are most damaged. But this idea mustnot be forced too far; in later foetal lifeadverse agents may act more selectively thanin early embryonic life.This review is not presented as a complete
or even a balanced. account of recent advancesin foetal physiology, but only in the hope ofshowing the interest and potential practicalvalue of these physiological researches. Ex-perimental investigation of human pregnancywill always be difficult, if not impossible, andonly by a wide survey of comparative physi-ology can reasonable deductions about thehuman foetus be made.
BIBLIOGRAPHY
AHLFELD, F. (I888), Verhandl. deutsh. Geselsch. Gynak., 2, 203.BALLANTYNE, J. W. (I90I), Brt. Mfed. journ., z, 8I3BARCLAY, A. E., FRANKLIN, K. J., and PRITCHARD, M.
M. L. (I944), 'The Foetal Circulation.' Oxford: Blackwell.BARCROFT, J., HERKEL, W. and HILL, R. M. (1933), J.
Physiol., 77, 194.BARCROFT. J., ELLIOTT, R. H. E., FLEXNER, L. B, HALL,
F. G., HERKEL. W., McCAR¶IHY, E. F., McCLURKIN,T. and TALAAT, M. (I934),Y. Physiol., 83, ;92.
BARCROFT, J., FLEXNE R, L. B., HERKEL, W., McCARTHY,E. F. and McCLURKIN, T. (I934), J. Physiol., 83, 215.
BARCROFT, J. and BARRON, D. H. ( 1937, J. Physiol., 91, 329.BARCROFT, J., KENNEDY, J. A. and MASON, M. F. (939),
.7. PhyS1ol., 95, I73, 269.BARCROFT, J., BARRON, D. H., COWIE, A. T. and
FORSHAM, P. H. (I940), 7. Physsol., 97, 338.BARCROFT, J. (I94I), Lancet, 2. 92.BARCROFT, J. (I942), Lancet, 2, 117.BAUER, D. J. (I938), Y. Physsol., 93, 90.BAUER, D. J.( 1938), _7. Physiol., 95, I87.EASTMAN, N. J., GEILING, E. M. K. and DELAWDER,
A M. (1933), Yohns Hopkins Hosp. Bull. 47, 22I.EBBS J. H., TISDALL, W. F. and SCOTT, W. A. (I941), .7
RUtrit, 22, 5I5.EBBS J. H., MOYLE, W. J., et al. (I942), Canad. M.A.j., 46, 1.
EDITORIAL, Lancet (1947), x, 639.EVANS, M. W. (I944), Med. J. Austral., I, 409.GREGG, N. M. (I 941 ), Trans. Ophth. Soc. Austral., 3, 35.GREENE, R. R. and BURRILL, M. W. (I939), Amer.J. Physiol.
126, 452, 510.HAMMOND, J. (I933), ' Growth and Development of Mutton
Qualities in Sheep.' Edinburgh.HASELHORST, G. and ALLMELING, A. (1930), Ztschv.
Geburtsh. Gynak., 98, f03.HASELHORST, G. and STROMBERGER, K. (1932), Ztschr.
Geburtsh. Gynak., 102, I6.HUGGETT, A. ST. G. (941), Physiol. Rev., 21, 438-462HUGGETT, A. c T. G. (I 944), Proc. Nutrit. Soc., 2, 20.HUGHES, W. (1929), Anat. Rec., 41, 213.LANCET, Editorial (1947), I, 639.LILLIE, F. R. (1923), Biol. Bull., 44, 47.LILLIE, F. R. (19I7), J. Exp. Zool., 23, 37I.McCARTHY E. F. (I 923),J. Physiol., 80, 206.MARTIN, S. M. (1945), Brit. Med. journ., i, 855.MAXWELL, J. P. (I929), Proc. Roy. Soc. Med., 23, 639.MELLANBY, M. (193I), Brit. Med. Journ., 2, 595.PARSONS, L. (I946), Y. Obst. Gyn. Brit. Emp., 53,1IPARSONS, L. (I932), Acta Pa diat., 13, 378.PEOPLES' LEAGUE OF HEALTH, Laacet (1942).
Protected by copyright.
on October 29, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.264.474 on 1 O
ctober 1947. Dow
nloaded from

October I947 CLAYTON: Some Recent Advances in Foetal Physiology, 48I
ROOS, J. and ROMIJN, C. (0938), J. Physioi., 92, 249.SMITH, G. E. (x919), Endocrinol., 3, 362.SNYDER, F. F. and ROSENFELD, M. (I 937). Amer. J. Physiol.,
x"19, '53.SPIVACK, M. ( I945), Anat. Rec., 8s, 85.STREETER, G. L. (935), Harvey Lectures, 1933-34, p. 204,
Baltimore.SWA1N, C., TOSTEVIN, A. L. and BLACK, G. H. B. (1946),
'Med.4. Austral., 2, 889.SWAN, C, TOSTEVIN, A. L. and BLACK, G. H.-B. (I944),
Med. Y. Austral., 1, 409.SWAN, C., TOSTEVIN, A. L. and BLACK, G. H. B. (1942),
Med. J. Austral., 2, 201.SWANSON, W. W. and lOB. V. (1939), Amer. J. Obst. Gyn.,
38, 382.TOVERUD, K. (X933), Amer. J. Dis. Child., 46, 954.
WALLACE, L. R. (1944), J. Physiol., 104, 34 P.WALTON, A. and HAMMOND, J. (I938), Proc. Royal Soc. B.,
125- 311.WARKANY, J.( 945), Amer.3'. Dis. Child., 99, .330.WARKANY, J., NELSON, R. C. and SCHRAFFENBERGER, E.
(I943), Amer. J. Dzs. Child., 65, 822.WINDLE, W. F. (1940), 'Physiology of the Fetus.' Saunders
Phladel phia.WINDLE, W. F., MONNIER, M. and STEELE, A. G. (939),
Phys. Zoil1., II, 425.WINDLE, W. F., BECKER, R. F., BARTH, E. E. and SCHUTZ,
M. D. (1938), Surg. Gyn. Obst., 69, 705.WINTROBE, M. M. and SCHUMACKER, H. B. (1936), Amer.
J7. Anat., 53, 313.WINTROBE, M. M. and SCHUMACKER, H. B. (I935), 7ourn-
Clin. Invest., I9, 837.
TEACHER AND STUDENT
There are two aspects in which we may view the teacher-as a worker and 'in-structor in science, and as practitioner and professor of the art; and these corres-pond to the natural division of the faculty into the medical school proper and thehospital.
SIR WILLIAM OSLER.
NOTICE TO CONTRIBUTORSi. All papers for publication must be in the hands of the Editor at least ten weeks before the proposed
date of publication.2. All papers should be typewritten as concisely as possible, with double spacing and a good margin. Sub-
headings should be clearly shown.3. Papers may be illustrated at the discretion of the Editor, with six or less illustrations, electrocardio-
graphs, X-rays, or line drawings, etc. Blocks may be obtained after use at the usual trade rates.
4. References to papers or other publications in the text must be shown by giving the name of the authorand the year of publication (with or without brackets). At the end of the paper these references shouldbe arranged alphabetically according to the R.S.M. svstem.Thus: (If to a Journal)
Author's name (year), journal, page, e.g.: ATKINSON, J. (192I), J. Biol. Chem., 47, 134.(If to a book).Author's name (date of publication), title of book, place of publication, e.g.: BROWN, C. D.
(I935), " Diseases of the Skin," London.5. Reprints of articles may be obtained provided notice is given when returning the corrected galley
proof.6. Contributors should send their manuscripts to
T HE EDITOR,Post Graduate Medical Journal,
I, Wimpole Street,London, W.i, England.
Protected by copyright.
on October 29, 2020 by guest.
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.23.264.474 on 1 O
ctober 1947. Dow
nloaded from