Solid Tumors of the Body and Tail of the Pancreas

of 12
-
Upload
anny-barr-robl -
Category
Documents
-
view
38 -
download
0
Transcript of Solid Tumors of the Body and Tail of the Pancreas
Solid Tumors of the Body and Tail of the Pancreas
Katherine A. Morgan, MD David B. Adams, MD Section of Gastrointestinal and Laparoscopic Surgery, Medical University of South Carolina, 25 Courtenay Drive Suite 7018, MSC 290, Charleston, SC 29425, USA
Solid lesions of the body and tail of the pancreas challenge all the diagnostic and technical skills of the modern gastrointestinal surgeon. The information available from modern computed tomography (CT), magnetic resonance (MR), and endoscopic ultrasound (EUS) imaging provide diagnostic and anatomic data that give the surgeon precise information with which to plan an operation and to discuss with the patient during the preoperative visit. A preoperative evaluation includes a thorough history and a pancreas protocol CT scan, supplemented by MR imaging and EUS when needed, to differentiate between the various potential diagnoses. These same modalities can be essential in proper staging in the case of malignant lesions, thus aiding in management decisions. Most lesions ultimately require operative resection, barring metastatic disease, with the notable exception of autoimmune pancreatitis.
There was a time when the diagnosis and surgical treatment of solid tumors of the body and tail of the pancreas began in pessimism and ended in futility. Identifying resectable malignancies of the pancreas was much less common than identifying tumors that were unresectable or frequently margin-positive, with associated patient survival that rarely exceeded 6 months. Patients with long-term survival of pancreatic ductal cancer were so few that many questioned whether distal pancreatectomy for adenocarcinoma was an indicated procedure. Patients with Whipple's triad and a small insulinoma in the tail of the pancreas were few. Autoimmune pancreatitis was unknown. Computed tomography (CT) scanning was not used so freely by emergency room and primary care physicians; thus small, asymptomatic tumors were rarely discovered. The precise identification and biopsy of small lesions in the tail and body of the pancreas by a flexible endoscope with an ultrasonic probe were unheard of. However, with widespread use of CT and magnetic resonance imaging (MRI) scanning for patients with gastrointestinal and nongastrointestinal disorders, the identification of benign and malignant conditions of the pancreas that are favorable surgical challenges with excellent long-term outcomes has instilled new interest and enthusiasm in the diagnosis and management of solid tumors of the body and tail of the pancreas. The practice of abandoning pancreatic resection for unexpected celiac axis tumor invasion has largely been replaced by a laparoscopic spleen-preserving distal pancreatectomy for an early cancer or a benign tumor. Solid tumors of the body and tail of the pancreas continue to represent a relatively uncommon clinical entity. The most likely diagnosis of a solid tumor remains ductal adenocarcinoma, which holds a poor prognosis similar to cancer in the head of the pancreas but is not incurable when discovered at a favorable stage. Many other potential diagnoses occur and may follow a benign course with excellent long-term survival rates. Management of these tumors has progressed notably over the past decade, paralleling advances in technology and surgical technique. Improvements in radiographic imaging modalities have enabled diagnosis with a good degree of certainty. Minimally invasive surgery is an exciting and dynamic tool in the approach to these patients. Radiography Evaluation of a patient with a solid tumor of the body and tail of the pancreas includes an attempt to obtain diagnosis to help guide management. Various radiographic studies are valuable in this differentiation. Beyond diagnosis, preoperative staging with radiography help is essential to guide management. Computed tomography
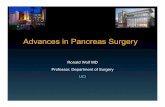
CT is the premier imaging test for diagnosing and staging solid pancreatic tumors. The modern CT capability (multiphase contrast-enhanced, thin section, spiral, or multidetector) has maintained this modality's utility in the face of other developing technologies (ie, MRI and endoscopic ultrasound [EUS]). CT can detect small lesions (>1 cm diameter) and give clues to diagnosis based on enhancement (hypovascular, hypervascular) and behavioral (invasion of nearby structures) characteristics. CT gives valuable information about vascular involvement, local invasion, and metastatic disease to help guide management decisions including resectability (Fig. 1). In a recent meta-analysis, modern CT has been shown to have a sensitivity and specificity of 91% and 85%, respectively, for diagnosis of pancreatic cancer, and a sensitivity and specificity of 81% and 82%, respectively, for resectability. The primary limitation of CT is in the ability to detect small peritoneal and liver metastases.[1]
Fig. 1 Axial contrasted dynamic CT image depicts a solid mass in the body of the pancreas, consistent with a pancreatic adenocarcinoma.
Magnetic resonance MR shows excellent results in terms of tumor detection and staging in evaluation of solid tumors of the pancreas. There have been multiple studies comparing MR with CT in the assessment of pancreatic masses, but none has shown significant benefit of MR over CT. MR has been shown to have a sensitivity and specificity of 84% and 82%, respectively, for diagnosis of pancreatic cancer, and a sensitivity and specificity of 82% and 78%, respectively, for resectability.[1] MR may have better differentiation of the characteristics of liver lesions, and magnetic resonance cholangiopancreatography (MRCP) allows for important specifics in the evaluation of cystic masses but confers no clear benefit in solid masses. Endoscopic ultrasound EUS was introduced approximately 25 years ago, with the goal of improved visualization of the pancreas as compared with conventional imaging. EUS can be useful in the diagnosis and localization of solid tumors of the body and tail of the pancreas. Functional neuroendocrine tumors of the pancreas are often diagnosed based on the associated clinical syndrome and confirmatory laboratory evidence of functional hormone hypersecretion. EUS is useful for localization of small tumors. In a prospective study of 82 patients with functional pancreatic neuroendocrine tumors, EUS was found to have a sensitivity and accuracy of 93%, with a specificity of 95%.[2] In solid tumors of the body and tail of the pancreas, including nonfunctional neuroendocrine tumors, pancreatic adenocarcinoma, and metastatic lesions, EUS can be useful in detecting and better characterizing small tumors (sensitivity 95%100%) and, particularly with the aid of fine-needle aspiration (FNA), can help in diagnosis (sensitivity 80%90%, specificity 100%). The differentiation of pancreatic adenocarcinoma arising in the setting of chronic pancreatitis is a primary cause for a false negative test.[3] Because of the potential for complications (overall 2.2%, pancreatitis 2%, tumor seeding











![Solid and Cystic Pseudopapillary Tumor of the Pancreas: A Case …€¦ · Cystic tumors of the pancreas are often misdiagnosed as pseu docysts and are inappropriately managed [8].](https://static.fdocuments.us/doc/165x107/5f6d9c61a7374f61f46d815b/solid-and-cystic-pseudopapillary-tumor-of-the-pancreas-a-case-cystic-tumors-of.jpg)