Soft Tissue Sarcoma - The University of Tennessee … Tissue Sarcoma Presley Regional Trauma Center...
33
Soft Tissue Sarcoma Presley Regional Trauma Center Department of Surgery University of Tennessee Health Science Center Memphis, Tennessee
Transcript of Soft Tissue Sarcoma - The University of Tennessee … Tissue Sarcoma Presley Regional Trauma Center...

Soft Tissue Sarcoma
Presley Regional Trauma Center
Department of Surgery
University of Tennessee Health Science Center
Memphis, Tennessee

• Collective term for an unusual and diverse
group of malignancies that arise from cells
of the embryonic mesoderm
• Account for 1% of adult and 15% of
pediatric tumors
• Comprise more than 50 distinct histologic
subtypes
Soft Tissue Sarcoma

• May occur anywhere in the body
• 43% - extremities
• 15% - RP
• 10% - trunk
• 19% - viscera
• 13% - other
Soft Tissue Sarcoma
• Unclear and controversial
• Genetic factors
• Chemical exposure
• Lymphedema
Etiology

• Chromosomal abnormalities
- Translocations
- Point mutations
- Deletions
• Regulatory genes
- p53
- RB1
Etiology

• Ionizing radiation
- Often do not become clinically apparent until
long after inciting exposure
- Osteosarcoma
- Malignant fibrous histiocytoma
• Chemical carcinogenesis
- Thorotrast
- Vinyl chloride
- Arsenic
Etiology

Pathologic Classification

• Categorized on the basis of the tissue type
from which it is believed to originate
• Subtypes may be defined by
histochemistry, flow cytometry, EM, tissue
culture and cytogenetic analysis
• Useful in determining which therapy is
best – not part of staging system
STS

• Best indicator of biologic aggressiveness
and metastatic potential
• Defined by tumor’s cellularity, nuclear
atypia, degree of necrosis and mitotic
activity
• AJCC staging system integrates tumor
grade, size, depth of tissue invasion,
degree of nodal involvement and mets
Grade

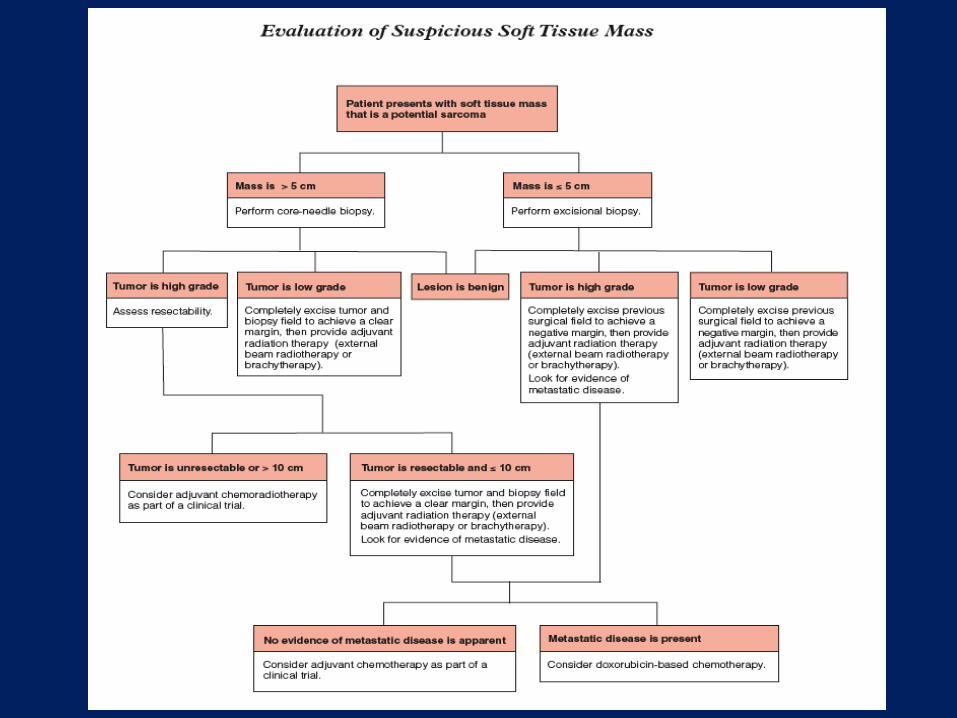
Clinical Evaluation

• Asymptomatic mass
• Painless and large
• Often noticed because of h/o recent
trauma to the area
• 38% are > 10 cm
Presentation

• Distant mets vary with tumor histology and
site of primary
• Extremity lung
• Abdominal and RP liver
• Few go to regional LN (2.6%)
Presentation

Management
• Foundation of treatment
• Amputation was once considered the only
option for cure
• Rosenberg et al (1982)
• Amputation is usually reserved for
extremity sarcomas that involve major
vessels, nerves or bones
Surgical Therapy

• Rosenberg et al (1982)
- 43 patients with extremity sarcoma
- Amputation – (n = 16)
- Limb-sparing surgery + radiation – (n = 27)
- All received adjuvant chemotherapy
- 5-year local recurrence slightly higher in LSS
- 5-year survival nearly identical
NCI

• Adequate resection involves excising a
margin of normal tissue along with any
areas through which biopsies have been
performed
• Compartmental resection or resection of
entire muscle groups provides no benefit
over WLE
• 1 to 2 cm margin should be the goal
Surgical Therapy

• Regional lymphadenectomy is not usually
indicated
• Tumor is in proximity to a LN basin
• Tumor is one of the following subtypes
- Rhabdomyosarcoma
- Epithelioid sarcoma
- Clear cell sarcoma
- Synovial sarcoma
- Vascular sarcoma
Surgical Therapy

Sarcoma Type Incidence of Nodal Metastases (%)
Rhabdosarcoma 11 - 36
Epithelioid Sarcoma 17 - 80
Clear Cell Sarcoma 25 - 50
Synovial Sarcoma 2 - 17
Vascular Sarcoma 11 - 40

• Dramatically changed the surgical
treatment of sarcomas
• Provides local control
• Brachytherapy
• Post-, pre-operative external beam
Radiation Therapy

• MSKCC
- 164 pts with extremity or superficial trunk
sarcoma
- Resection ± brachytherapy
- 76 month median f/u
- Local control rate better in BT group
- No difference in 5-year disease-specific
survival
Brachytherapy

• NCI
- 91 pts with high-grade STS
- Resection ± radiation
- All pts received adjuvant chemotherapy
- One local recurrence with radiation vs 8 with
no radiation
- No difference in overall survival
External Beam

• Canada
- 190 pts
- Closed because of wound complications
- Pre-op = 35% vs 17% with post-op
- No difference in local control
- Significant difference in overall survival that
slightly favored the pre-op group
Pre- vs Post-op External Beam

• Post-op chemo has been studied in multiple
prospective, randomized trials but small
sample sizes and differences among them
have made it difficult to interpret the data
• Sarcoma Meta-analysis Collaboration
• Post-op adjuvant chemotherapy is best
employed in the context of appropriate
clinical trials
Chemotherapy

• Allows delivery of agents through native
vasculature
• Permits assessment of effectiveness of tx
by pathologic analysis
• May facilitate tx of micromets
• May downstage tumors – making them
more amenable to resection
Pre-op Chemotherapy

• MD Anderson
- Retrospective, 46 pts extremity sarcomas
- Overall tumor response rate was 40%
- Significant improvement in both disease-free
and overall survival
• MSKCC
- Prospective, 29 pts
- Large, high-grade extremity sarcomas
- No benefit
Conflicting Data

• Given the lack of sufficient evidence for any
survival benefit, pre-op chemotherapy may
be considered in attempting to preserve
limb function but otherwise its use should
be limited to clinical trials
Conclusion

• Most interesting and exciting advances
• The characterization and targeting of the
tyrosine kinase receptor = c-kit
• GIST
Targeted Therapeutics
• Reserved for patients in whom LSS is not
possible
• Cannulate the arterial and venous supply
and apply a proximal tourniquet
• Bypass machine maintains mild
hyperthermia, oxygenation and circulates
chemotherapeutic agents in the limb
Isolated Limb Perfusion

• Extremity - local recurrence = 8 to 20%
• RP - local recurrence = 38 to 50%
• Salvage surgery is an option
• Radiation for those who did not receive it
previously
Recurrent STS

Metastatic Disease

• Lung mets present in 20% of pts with trunk
or extremity
• Resection may be attempted if pt is
medically fit, no extrathoracic disease is
present and the primary tumor is
controlled
• 3-year survival ranges from 23 to 54%
Resectable

• Distant mets may develop in as many as
50% of cases
• For the vast majority, only available
treatment option is systemic
chemotherapy
• Doxorubicin
Unresectable