
Statement of Principles concerning soft tissue sarcoma No ...

Warren Chow, M.D.Division of Medical Oncology
UCSF 7th Annual Clinical Cancer UpdateJanuary 25, 2008
Soft Tissue Sarcoma Chemotherapy:
Past, Present, Future

Disclosure Statement
• Research funding from:– Pfizer Pharmaceuticals– Ariad Pharmaceuticals– Food and Drug Administration
• FDA Orphan Products Development Grants Program– Arqule, Inc.– Eli Lilly Pharmaceuticals– Sarcoma Alliance for Research thru
Collaboration
Sarcoma Introduction
• Cancer of the connective tissue• Soft-tissue sarcomas: Estimated 9,530
cases in U.S. in 2006 (M 5,720 / F 3,810)– Deaths: 3,500 (M 1,830 / F 1,670)
• Bone sarcomas: Estimated 2,760 in U.S. in 2006 (M 1,500 / F 1,260)– Deaths: 1,260 (M 730 / F 530)
Jemal A, et al. CA: Cancer J for Clin. 55:1, 2005
Soft-Tissue Sarcoma MajorHistologic Subtypes: >50 subtypes
• Undiff Pleomorphic (MFH) (28%)• Liposarcoma (15%)• Leiomyosarcoma (12%)• Unclassified (11%)• Synovial sarcoma (10%)• Malignant peripheral nerve sheath (6%)• GIST (5%)• Fibrosarcoma (3%)• Angiosarcoma (2%)• Epithelioid (1%)
Coindre JM, et al. Cancer. 91:1914, 2001.Fletcher DM, et al. WHO Classification: Tumours of Soft Tissue
and Bone. IARC Press, 2002.
Bone Sarcoma Histologic Subtypes
• Osteosarcoma (36%)• Chondrosarcoma (10-25%)• Ewing sarcoma (6-8%)
Dorfman HD. Bone Tumors. Mosby, Inc., St. Louis, 1998.Damron TA. Oncology and Basic Science. Lippincott Williams
& Wilkins, Philadelphia, 2008.

Location
Cancer: Principles & Practice of Oncology.DeVita VT, et al. 6th ed, 2000, p. 1844.

Past…

Adjuvant Chemotherapy for Bone Sarcomas
• Osteogenic sarcoma– Cisplatin/Doxorubicin +/- High-Dose Methotrexate– Survival: <20% no Rx vs. >60% with Rx
• Ewing sarcoma family of tumors– Ifosfamide/Etoposide +
Vincristine/Doxorubicin/Cyclophosphamide– Survival: 20% no Rx vs. >70% with Rx
• Chondrosarcoma– Adjuvant chemotherapy NOT recommended
Meyers PA, et al. J Clin Oncol. 23:2004, 2005.Grier HE, et al. N Engl J Med. 348:694, 2003.
Adjuvant Chemotherapy for Soft-Tissue Sarcomas
• Meta-analysis of 14 randomized, doxorubicin-based adjuvant chemotherapy trials– 6% benefit for local recurrencelocal recurrence--free survivalfree survival
(p=0.016)– 10% benefit for distant recurrencedistant recurrence--free survivalfree survival
(p= 0.0003)– 10% benefit for overall recurrenceoverall recurrence--free survivalfree survival
(p=0.0001)– 4% benefit for overall survivaloverall survival (p=0.12)
Sarcoma Meta-analysis Collaboration. Lancet. 350:1647, 1997.

Traditional Sarcoma Chemotherapy
• Results of Two Consecutive Trials of Dose-Intensive Chemotherapy with Doxorubicin (A) and Ifosfamide (I) in Patients with Sarcomas– AI 75/10 (Doxorubicin 75 mg/m2/72 hr +
Ifosfamide 2 gm/m2/2 hr x 5 day)• Overall objective RR 69%69%• Febrile neutropenia 31%31% of cycles
– AI 90/10 (Doxorubicin 90 mg/m2/72 hr + Ifosfamide 2 gm/m2/2 hr x 5 day)
• Overall objective RR 59%59%• Febrile neutropenia 56%56% of cycles
Patel S, et al. Am J Clin Oncol. 21:317, 1998.
Adjuvant Chemotherapy for Soft-Tissue Sarcomas
• Italian adjuvant trial of 5 cycles of Epirubicin/ Ifosfamide for extremity STS (med. f/u 89.6 mos)– Only 104 patients (51 control; 53 observ.)
• Planned 95 pts/arm (tot. 190)• Interim analysis after 50% enrolled.• Two-sided p < 0.001 DFS
– Median DFS: 47 mos vs. 16 mos (p=0.09)– Median OS: NR vs. 49 mos (p=0.07)– 5-yr OS estimate: 66.0 % vs. 46.1% (p=0.04)
Frustaci S, et al. J Clin Oncol 19:1238, 2001.Frustaci S, et al. Oncology 65 (suppl 2):30, 2003.

Present…

Angiosarcoma of the Scalp or Face
• Paclitaxel 175 mg/m2 given over 1, 3, and 24 hr– Memorial-Sloan Kettering Cancer Ctr– 8/9 patients responded:
• 4 PR’s, 4 clinical CR’s, & 1 MR• Liposomal Doxorubicin
– Case reports of complete response in radio-resistant cutaneous angiosarcoma
Fata F, et al. Cancer. 86:2034, 1999.Eiling S, et al. Brit J Derm. 147:150, 2002.

84 y/o W/M w/ Scalp Angiosarcoma& CR after 4 Cycles of Paclitaxel
9/13/07 1/3/08

Radiation-induced Angiosarcoma of the Breast
• 82 y/o W/F Stage 1, ER/PR/Her-2(-) multifocal breast CA in 2001; lumpectomy, adjuvant AC & XRT.
• 2006, developed 1. 9 cm angiosarcoma (AS) of breast; simple mastectomy.
• Jan, 2007, developed multifocal AS chest wall recurrence; resected w/ flap Feb, 2007.
• April, 2007, developed recurrence outside of vascular flap.
• May, 2007, 2 cycles of paclitaxel 80 mg/m2/week for 6 weeks every 8 weeks.
• Surgery August, 2007; path CR.• Received 2 cycles of “consolidation” paclitaxel.
Observation since Nov, 2007.
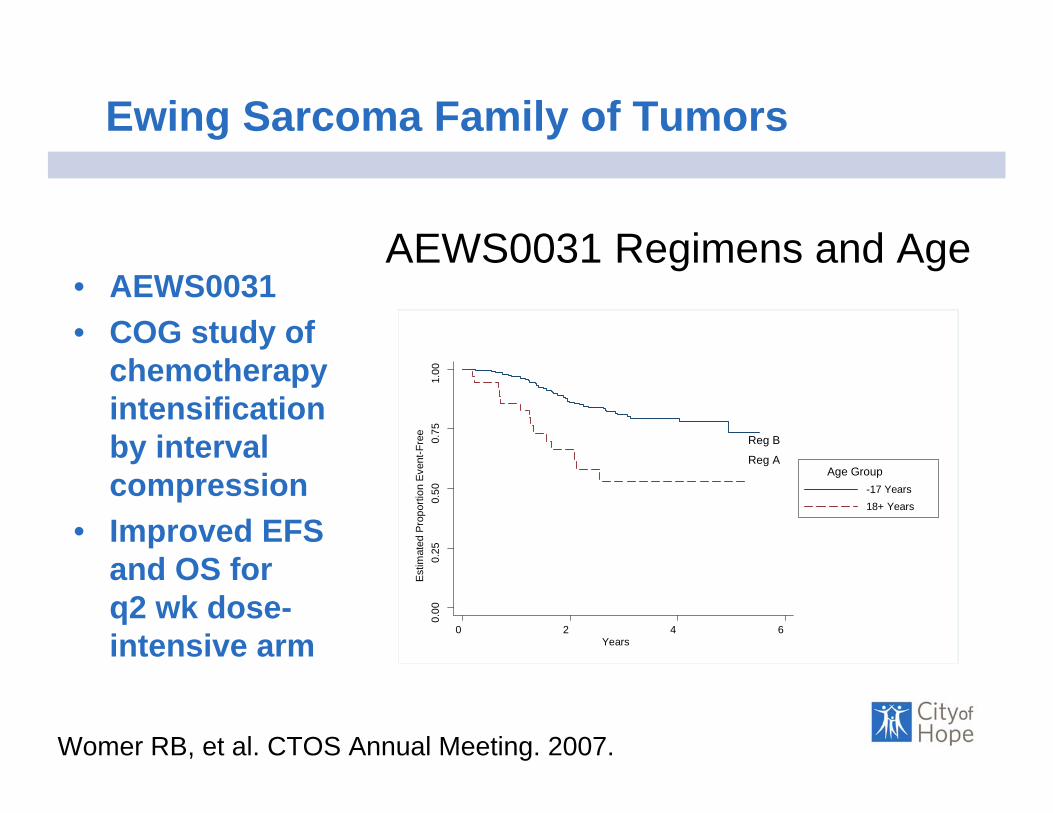
Ewing Sarcoma Family of Tumors
• AEWS0031• COG study of
chemotherapy intensification by interval compression
• Improved EFS and OS for q2 wk dose-intensive arm
Womer RB, et al. CTOS Annual Meeting. 2007.
AEWS0031 Regimens and Age
0.00
0.25
0.50
0.75
1.00
Estim
ated
Pro
porti
on E
vent
-Fre
e
0 2 4 6Years
-17 Years18+ Years
Age Group
Reg B0.
000.
250.
500.
751.
00Es
timat
ed P
ropo
rtion
Eve
nt-F
ree
0 2 4 6Years
-17 Years18+ Years
Age Group
Reg B
Reg A

Gemcitabine and Docetaxel• MSKCC: Combination first tested in
leiomyosarcoma of uterus or other organs.– Gemcitabine 900 mg/m2/90 min (D1, D8) + Docetaxel 100
mg/m2/1 hr D8 + G-CSF– Overall RR 53%53% (20% SD)
• U. Michigan: Tested in other sarcoma histologies.– Gemcitabine 675 mg/m2/90 min (D1, D8) + Docetaxel 100
mg/m2/1 hr D8 + G-CSF– Responses observed in leiomyosarcoma, osteosarcoma,
angiosarcoma, MFH, malignant peripheral nerve sheath tumor, and Ewing’s sarcoma.
Hensley ML, et al. J Clin Oncol. 20:2824, 2002.Leu KM, et al. J Clin Oncol. 22:1706, 2004.

Gemcitabine and Docetaxel
Maki RG et al. J Clin Oncol. 25:2755, 2007.
• SARC Cooperative Group randomized phase II study of gemcitabine +/-docetaxel– Gemcitabine 1200 mg/ m2/90 min (D1, D8)
every 21 days.– Gemcitabine 900 mg/m2/90 min (D1, D8) +
Docetaxel 100 mg/m2/1 hr D8 + G-CSF every 21 days.
– RR 8% vs. 16%– Leiomyosarcomas and MFH/HGUPS most
responsive.

Adjuvant Chemotherapy for Soft-Tissue Sarcomas
• EORTC randomized, phase III trial of 5 cycles of Doxorubicin (75 mg/m2) & Ifosfamide (5 gm/m2) q 21d vs. obs for high grade STS of any site.
• 351 pts accrued between 1995-2003.• LMS (15%), lipo (13%), MFH (11%), SS (11%)• 66% extremity; 34% trunk/pelvis; 40% > 10 cm• 73% completed the prescribed 5 cycles of Rx
– 63% completed without dose reduction/delay• 5-yr RFS 53% obs arm vs. 51% CT arm• 5-yr OS 69% obs arm vs. 64% CT arm
Woll PJ, et al. Proc ASCO 25:10008a, 2007.
Targeted Therapies for Soft-Tissue Sarcomas

Gastrointestinal Stromal Tumors (GIST)
• Most common gastrointestinal sarcoma• Highest incidence in the 40-60 year age group• Recently identified as a distinct clinical and
histopathologic entity• GIST have an incidence of 14.5 per million
annually (comparable with CML)• U.S. Population 296,000,000 ≅ 4,300/year
Cancer Facts & Figures. 2003.
Fletcher et al. Hum Pathol. 2002;33:459.
Miettinen et al. Pol J Pathol. 2003;54:3.
Joensuu et al. Lancet Oncol. 2002;3:655.
Kindblom et al. Ann Oncol. 2002;13:157. Abstract 577O.
Kindblom. At: http://www.asco.org.

GIST: Origin
• GIST share several characteristics with interstitial cells of Cajal (ICC)– Pacemaker cells of the gut– Mixture of neural and myogenous features by electron
microscopy– Expression of KIT (CD117) in ~95% of cases
• ICC hyperplasia is evident in the GI tract of patients with familial GIST
• GIST and ICC may arise from a common mesenchymal stem cell of the enteric neural plexus
Sircar et al. Am J Surg Pathol. 1999;23:377.Wang et al. Arch Pathol Lab Med. 2000;124:1471.
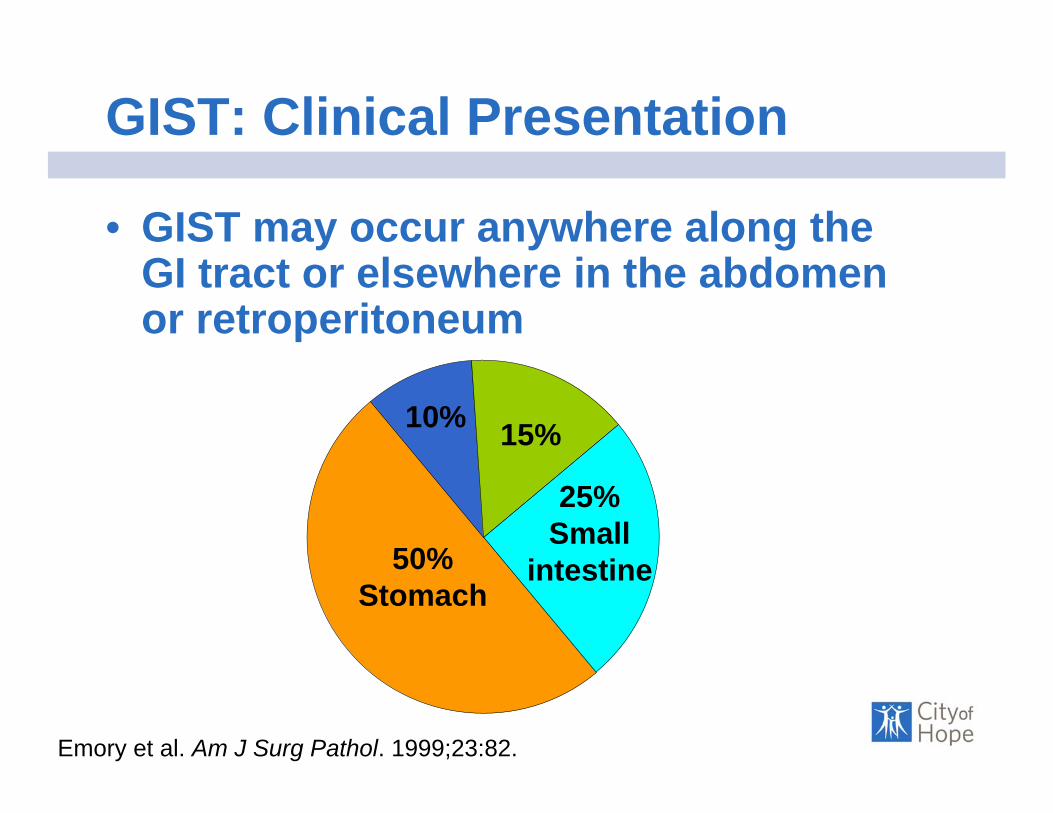
GIST: Clinical Presentation
• GIST may occur anywhere along the GI tract or elsewhere in the abdomen or retroperitoneum
Emory et al. Am J Surg Pathol. 1999;23:82.
50%Stomach
25%Small
intestine
10% 15%
Colon Other (rectum, esophagus, mesentery, retroperitoneum)
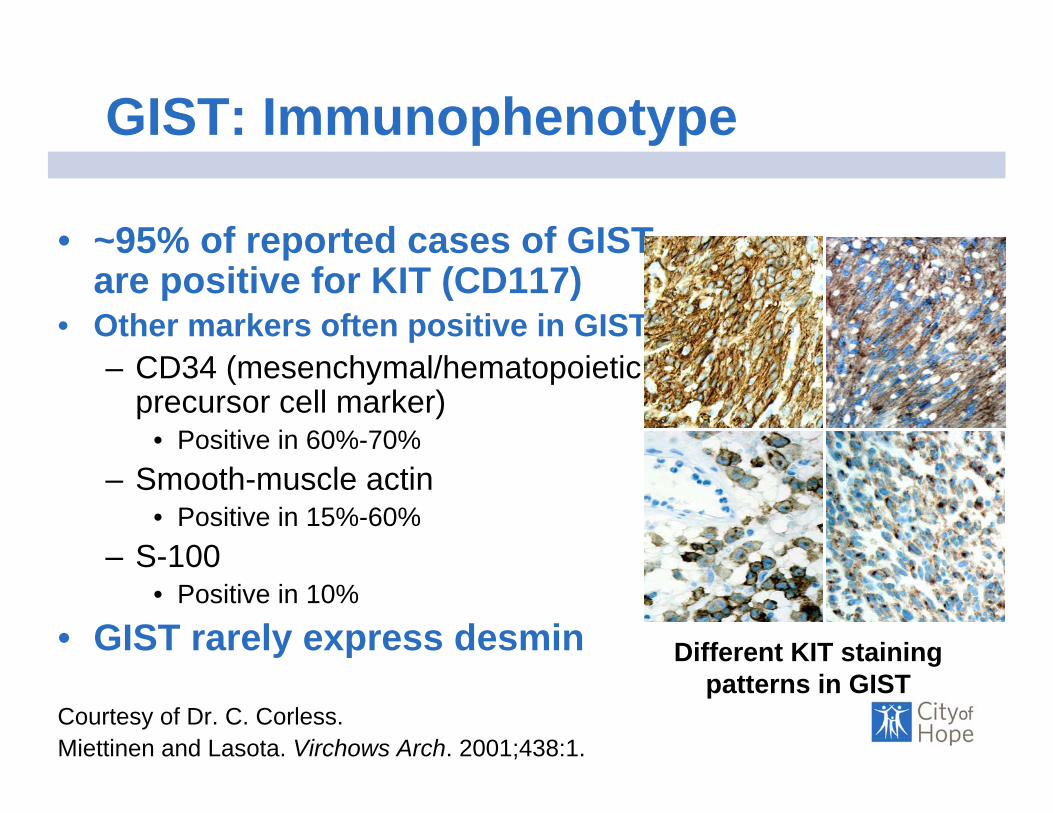
GIST: Immunophenotype
• ~95% of reported cases of GIST are positive for KIT (CD117)
• Other markers often positive in GIST– CD34 (mesenchymal/hematopoietic
precursor cell marker)• Positive in 60%-70%
– Smooth-muscle actin• Positive in 15%-60%
– S-100• Positive in 10%
• GIST rarely express desmin Different KIT staining patterns in GIST
Courtesy of Dr. C. Corless.Miettinen and Lasota. Virchows Arch. 2001;438:1.

279:577-580, 1998
GIST: Identification of KITGain-of-Function Mutations
• KIT staining was positive in 46 of 49 GIST (94%)• 5 of 6 GIST had mutations in KIT gene• Mutant forms of KIT are constitutively active• Proposed that GIST may originate from ICCs• Studies in knock-in mice with KIT mutations
– Demonstrated that constitutive KIT signaling is sufficient to induce GIST– Parallel with the pathology seen with familial KIT mutations, eg,
mastocytosis
Sommer et al. Proc Natl Acad Sci U S A. 2003;100:6706.Hirota et al. Science. 1998;279:577.

GIST: Platelet-Derived Growth Factor Receptor Alpha (PDGFRA) Mutations
• PDGFRA mutations are present in ~5%-7% of GIST– Mutually exclusive with KIT mutations– 35% of KIT wildtype GIST have PDGFRA mutations
• Downstream activation targets of KIT are also activated by PDGRFA mutations in GIST– AKT– MAP kinase– STATs
Heinrich M et al. Science. 2003;299:708.

Heinrich et al. Hum Pathol. 2002;33:484.Corless et al. Proc Am Assoc Cancer Res. 2003;44. Abstract R4447.
KIT and PDGFRA Mutations in GIST
Membrane
Cytoplasm
Exon 11 (67.5%)
Exon 9 (11%)
Exon 13 (0.9%)
Exon 17 (0.5%)
Exon 12 (0.9%)
Exon 18 (6.3%)
KIT PDGFRA
Overall mutation frequency: 87.4%
Exon 14 (0.3%)

Normal KIT Signaling
PP PADP P
P
PP PATP
SIGNALING
Kinasedomains
Substrate
Effector
• The KIT kinase domain activates a substrate protein, eg, PI3 kinase, by phosphorylation
• This activated substrate initiates a signaling cascade culminating in cell proliferation and survival
Adapted from Savage and Antman. N Engl J Med. 2002;346:683.Scheijen and Griffin. Oncogene. 2002;21:3314.
Imatinib Mesylate: Background
• A selective tyrosine kinase inhibitor of– KIT– c-Abl/Arg– PDGFRA/B
• First used in Philadelphia chromosome–positive (Ph+) CML
Druker et al. Nat Med. 1996;2:561.
Class: Phenylaminopyrimidines
C29H31N7O•CH4SO3
MW 589.7
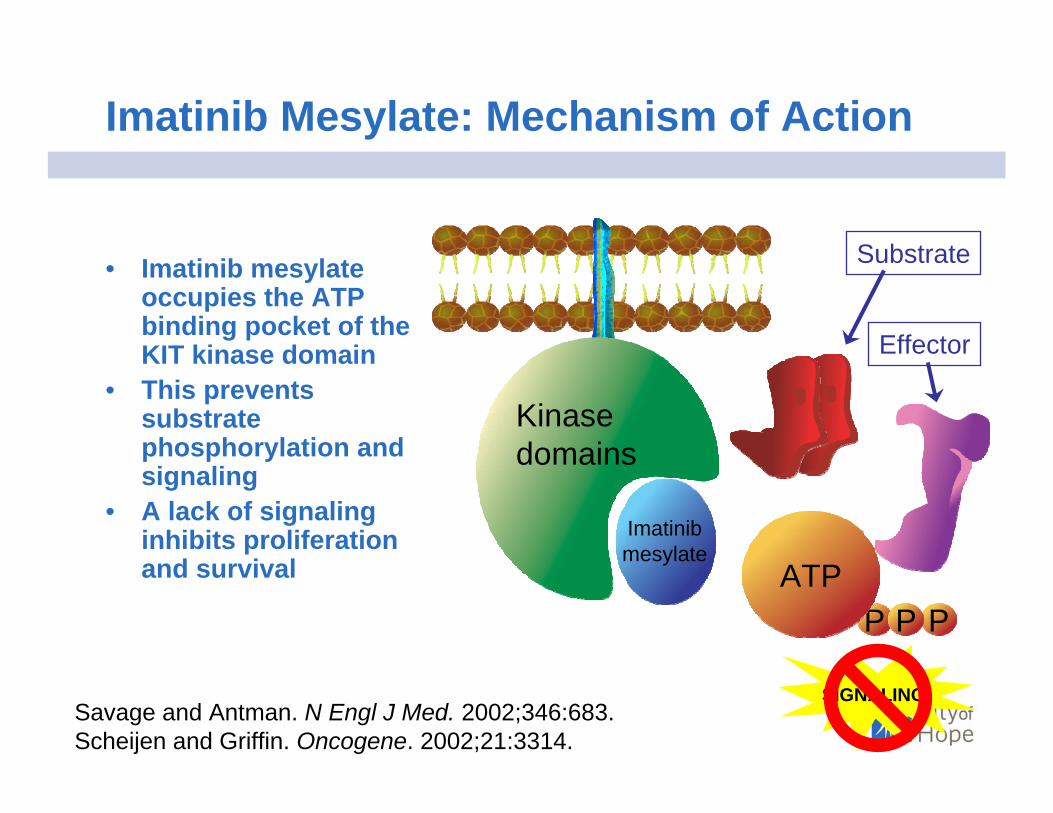
Imatinib Mesylate: Mechanism of Action
P
PP PATP
SIGNALING
Imatinibmesylate
Kinasedomains
• Imatinib mesylate occupies the ATP binding pocket of the KIT kinase domain
• This prevents substrate phosphorylation and signaling
• A lack of signaling inhibits proliferation and survival
Savage and Antman. N Engl J Med. 2002;346:683.Scheijen and Griffin. Oncogene. 2002;21:3314.
Substrate
Effector
First Patient With GIST to Receive Imatinib Mesylate: Proof-of-Concept
• Exploratory study with oral imatinib mesylate at 400 mg/d
• Dramatic clinical response– Disappearance of excess metabolic activity at
4 weeks by 18FDG-PET– 75% reduction in tumor size at 8-month follow-up– Tumor biopsies showed histologic evidence of myxoid
degeneration and lack of mitotic activity– Symptomatic relief
Joensuu et al. N Engl J Med. 2001;344:1052.

Joensuu et al. N Engl J Med. 2001;344:1052.
Imatinib Mesylate for Nonresectable and Metastatic GIST: Case Study (cont’d)
Multiple liver and upper abdominal 18FDG-accumulating
metastases
A marked decrease in 18FDG uptake 4 weeks after starting imatinib mesylate (400 mg/d)
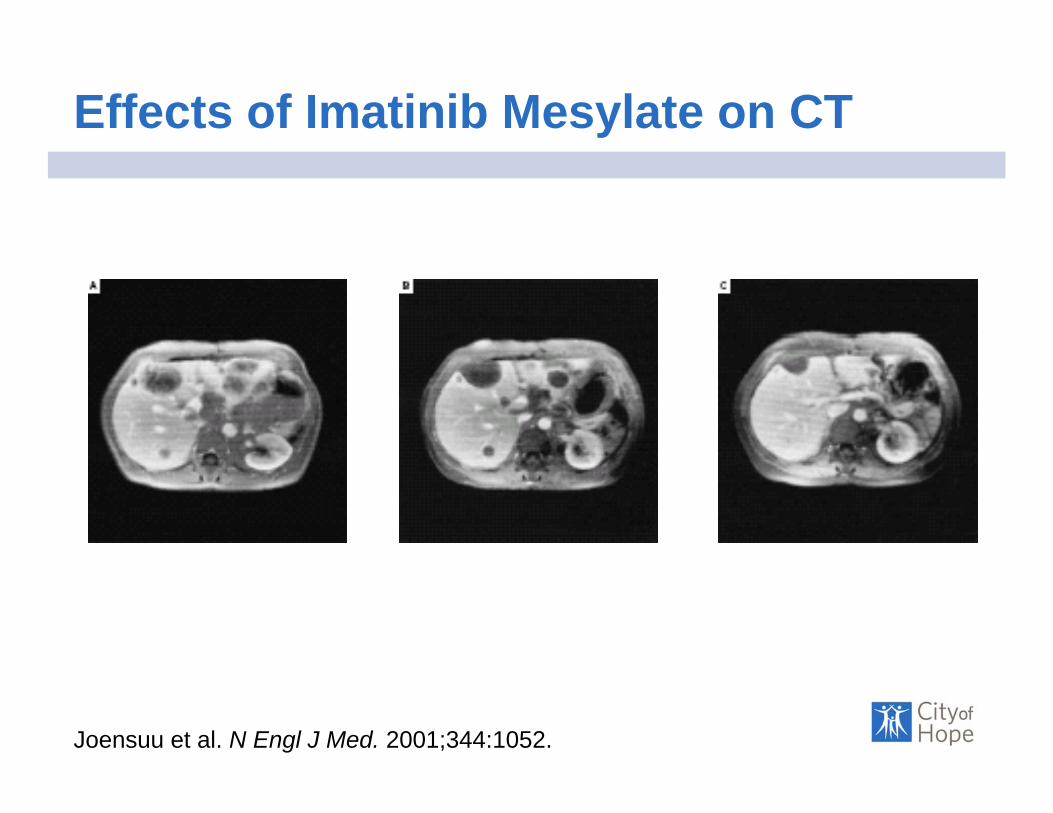
Effects of Imatinib Mesylate on CT
Joensuu et al. N Engl J Med. 2001;344:1052.
Pre-Treatment Week 4 8 Months

Effects of Imatinib on Histology
Joensuu et al. N Engl J Med. 2001;344:1052.
Pre-Treatment 3 WeeksPost-Treatment
H&E
Ki-67
CD117

GIST: KIT Mutation Location Predicts Imatinib Mesylate Responsiveness
• KIT mutations are predictive of response to imatinib mesylate
• Exon 11 mutants respond best
Blanke et al. ASCO 2004 Gastrointestinal Cancers Symposium. Abstract 2.
020
40
6080
100
% o
f tot
al
KIT Exon 11(n=85)
KIT Exon 9(n=23)
No mutation(n=9)
PD/NESDPR
Imatinib Mesylate Therapy of GIST With Weak/Negative KIT Expression
• Approximately 5% of GIST are KIT-negative• Weak/negative KIT staining is not predictive
of a poor response to imatinib mesylate• KIT-negative GIST may express imatinib
mesylate–sensitive mutant KIT or PDGFRA– Documented clinical responses in KIT-
negative GIST
Debiec-Rychter et al. J Pathol. 2004;202:430.Medeiros et al. Am J Surg Pathol. 2004;28:889.

Efficacy of Imatinib Mesylate in KIT-Negative GIST (S0033): PFS
Blackstein et al. J Clin Oncol. 2005;23(suppl 16):818s. Abstract 9010. Blackstein et al. At: http://www.asco.org/ac/1,1003,_12-002511-00_18-0034-00_19-005041,00.asp. Accessed July 2005.
100
80
60
40
20
00 12 24 36 48 60
Months
% o
f pat
ient
s
KIT-negative GIST (n=14) 43%KIT-positive GIST (n=376) 48%
P=0.413
2-year PFS
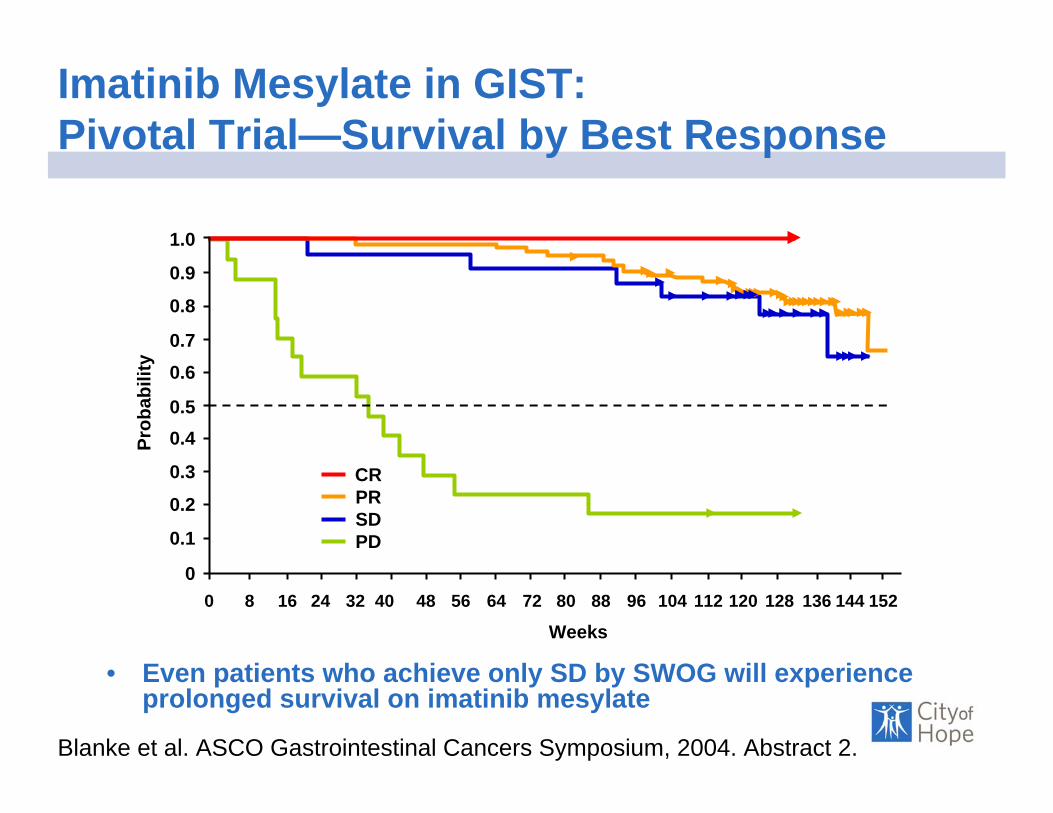
Imatinib Mesylate in GIST: Pivotal Trial—Survival by Best Response
• Even patients who achieve only SD by SWOG will experience prolonged survival on imatinib mesylate
Blanke et al. ASCO Gastrointestinal Cancers Symposium, 2004. Abstract 2.
1.0
0.9
0.8
0.70.6
0.50.4
0.3
0.2
0.1
0
Prob
abili
ty
0 8 16 24 32 40 48 56 64 72 80 88 96 104 112 120 128 136 144 152
Weeks
CRPRSDPD

“We Should Desist Using RECIST, at Least in GIST”
• RECIST is insensitive in evaluating GIST response treated with imatinib.
• 172 met. GIST lesions eval. in 40 pts.• Mean size (5.3 cm), density (72.8 HU), SUVmax
(5.8).• 33/40 good response on FDG-PET.• Decrease in size >10% or tumor density of
>15% on CT had sensitivity 97% & specificity 100% by FDG-PET.
Choi H et al. J Clin Oncol 25:1753, 2007.Benjamin RS, et al. J Clin Oncol 25:1760, 2007.

“We Should Desist Using RECIST, at Least in GIST”

Adjuvant Imatinib for GIST• ACOSOG Z9001 [A Phase III Randomized
Double-blind Study of Adjuvant Imatinib vs. Placebo in Patients Following Resection of Primary GIST]
• Pts with GIST > 3 cm, not ruptured, nor multifocal eligible for randomization to imatinib400 mg/day for 1 yr vs. placebo.
• Interim results reported 97% RFS for imatinib vs. 83% for placebo @ 1 yr.
• On-going adjuvant trials in Europe– EORTC: 2 years imatinib vs. observation– Scandinavian Sarcoma Group: 1 yr vs. 3 yr of imatinib
The Next Intergroup GIST Study
• SWOG S0502: A Phase III Randomized Study of Imatinib, with or without Bevacizumab, in Patients with Metastatic or Unresectable GIST.

Other Potential Imatinib-Sensitive Sarcomas
• Dermatofibrosarcoma Protuberans– Uncommon, low-gr, fibrohistiocytic tumor of interm.
malignant potential of dermis and subcutis– Caused by autocrine/paracrine activation of platelet-
derived growth factor receptor-B (PDGFR-B) via translocation (COL1A1-PDGFB fusion)
• Rubin BP, et al. J Clin Oncol. 20:3586, 2002.– SARC004: Phase II Study of IM in DFSP
• Extraabdominal Desmoid Tumors (Fibromatosis)– Rare, monoclonal tumor of deep musculoaponeurotic
structures• Mace J, et al. Cancer. 95:2373, 2002.
– SWOG S0525: Phase II Study of IM in Desmoid Tumors
Other Potential Imatinib-Sensitive Sarcomas
• Chordomas– Very, rare tumor that originate from remnant of notochord.
• Casali PG, et al. Cancer. 101:2086, 2004.
• Ewing’s Sarcoma/PNET?– Phase 2 trial of IM for tx of pediatric solid tumors: A
Children’s Oncology Group Study• Bond M, et al. Pediatr Blood Cancer. E-pub, 2006.• 1/24 pts with PR.
– Phase 2 SARC trial (Chugh D. Proc ASCO 22: 90001a, 2004).
• 0/13 pts with PR– Imatinib mesylate therapy for recurrent Ewing’s family of
tumors (EFT) [Chow WA, et al. Proc ASCO. 22:9054a, 2004]
• 1/7 pts with PR (Kit & PDGFR-a expression)
Imatinib Resistance in GIST
GIST: Mechanisms of Potential Resistance to Imatinib Mesylate
• Resistance can be primary or secondary (following initial response)
• Mechanisms– Imatinib mesylate–resistant mutations in
KIT or PDGFR-A kinase domain– KIT or PDGFR-A gene amplification– Activation of alternative kinase
• Resistance may be evidenced as progression of some lesions but not others
Fletcher et al. Proc Am Soc Clin Oncol. 2003;22:815. Abstract 3275.

Pretreatment 6 months 10 months
Imatinib Mesylate in GIST:Focal Resistance Following Response
Courtesy of Dr. R. DeMatteo.
GIST: Sunitinib Treatment
• An inhibitor of the receptor tyrosine kinases PDGFR, VEGFR, KIT, RET, and FLT3 – Has antiangiogenic effects on HUVECs in vitro
• Achieved tumor control in conjunction with irradiation in murine tumor models
• Clinical activity observed in patients intolerant of or who progressed on imatinib mesylate
• DLT: fatigue, nausea, vomitingHUVECs = human umbilical vein endothelial cells.Demetri et al. Proc Am Soc Clin Oncol. 2003;22:814. Abstract 3273.Mendel et al. Clin Cancer Res. 2003;9:327.Hallahan et al. Proc Am Soc Clin Oncol. 2003;22:873. Abstract 3508.

GIST Resistant to Imatinib Mesylate:Phase II Trial of Sunitinib
• 65% of patients in a phase I/II trial experienced clinical benefit
Demetri et al. Proc Am Soc Clin Oncol. 2004;23:195. Abstract 3001.Demetri et al. At: http://www.asco.org/ac/1,1003,_12-002511-00_18-0026-00_19-008902.asp. Accessed July 2004.
8
58
35
010203040506070
PR SD PD
% o
f pat
ient
s
N=92

Imatinib Mesylate in GIST: Pivotal Trial—Survival by Best Response
• Even patients who achieve only SD by SWOG will experience prolonged survival on imatinib mesylate
Blanke et al. ASCO Gastrointestinal Cancers Symposium, 2004. Abstract 2.
1.0
0.9
0.8
0.70.6
0.50.4
0.3
0.2
0.1
0
Prob
abili
ty
0 8 16 24 32 40 48 56 64 72 80 88 96 104 112 120 128 136 144 152
Weeks
CRPRSDPD
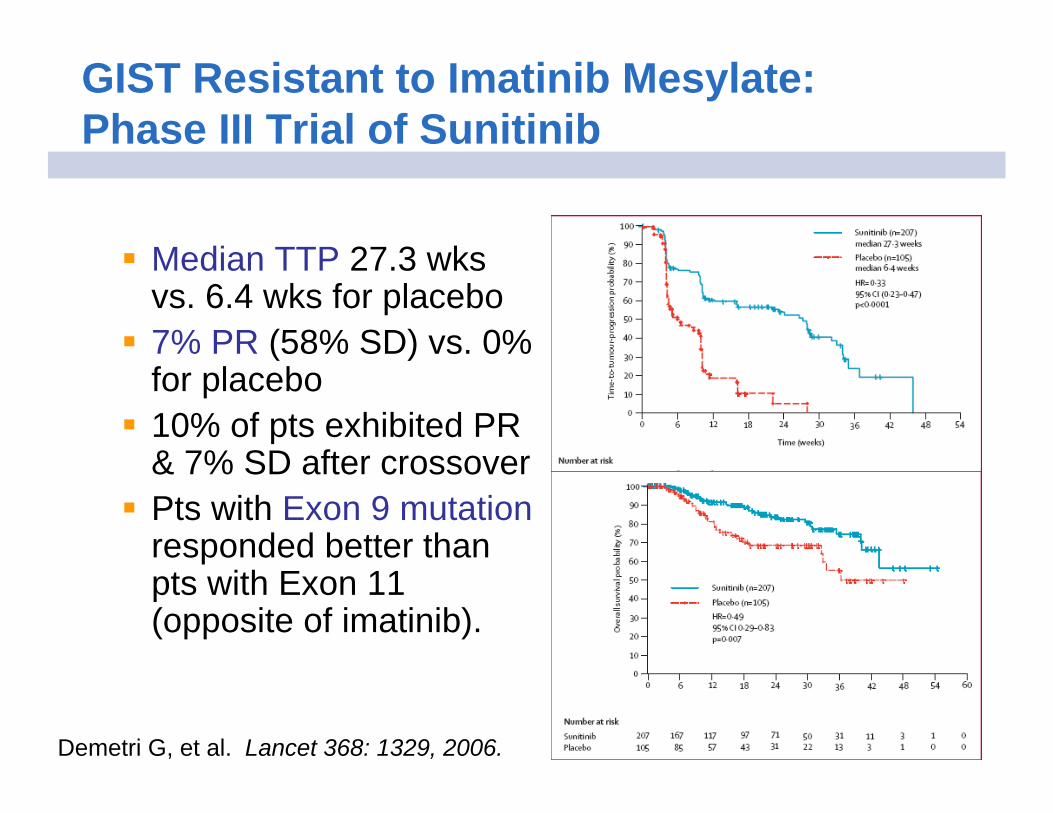
GIST Resistant to Imatinib Mesylate: Phase III Trial of Sunitinib
Median TTP 27.3 wks vs. 6.4 wks for placebo7% PR (58% SD) vs. 0% for placebo10% of pts exhibited PR & 7% SD after crossoverPts with Exon 9 mutationresponded better than pts with Exon 11 (opposite of imatinib).
Demetri G, et al. Lancet 368: 1329, 2006.

Future…
AP23573, an mTOR Inhibitor
• AP23573, an analog of rapamycin(Sirolimus)
• Inhibits the mammalian target of rapamycin(mTOR) protein kinase.
• mTOR is a central controller of cell proliferation
• Treatment of cells with rapamycin inhibits:– Cell growth– Cell division
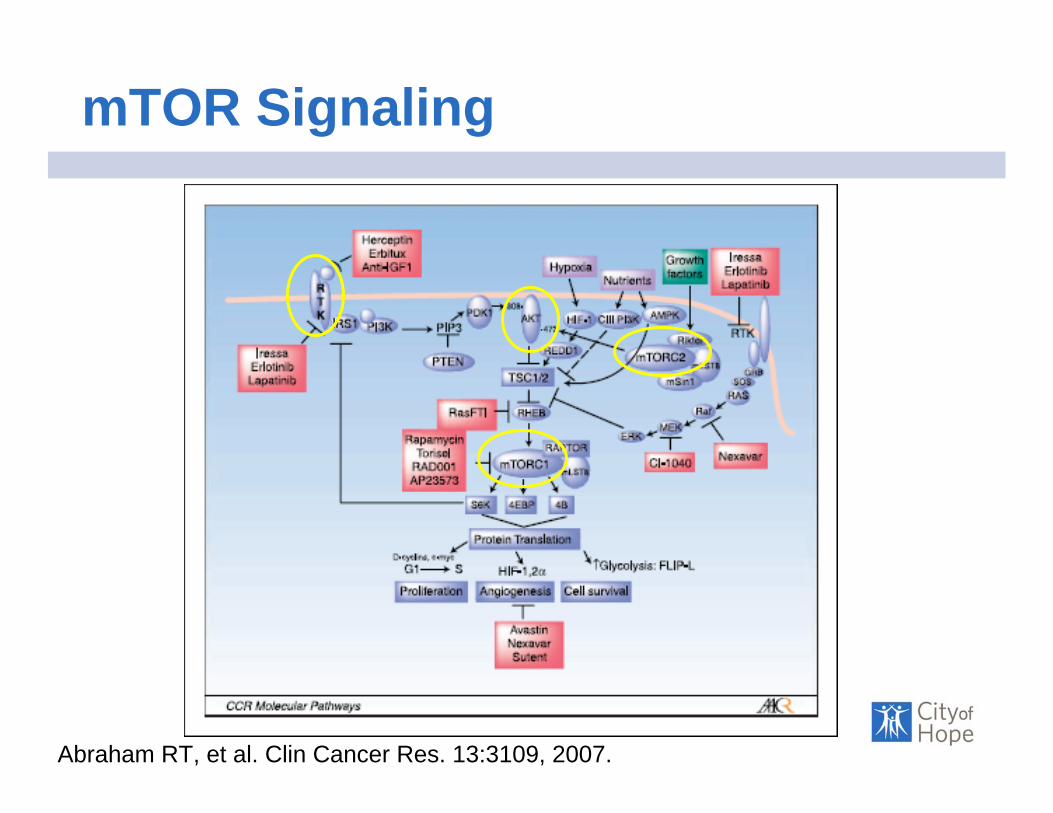
mTOR Signaling
Abraham RT, et al. Clin Cancer Res. 13:3109, 2007.
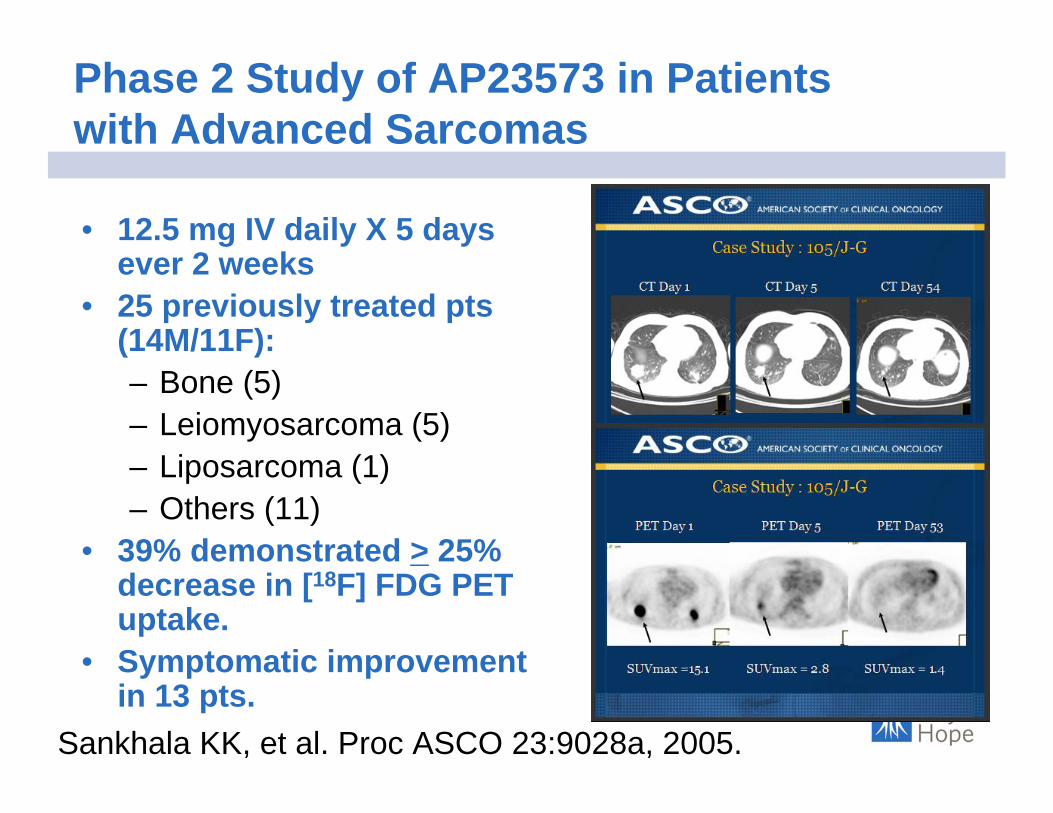
Phase 2 Study of AP23573 in Patients with Advanced Sarcomas
• 12.5 mg IV daily X 5 days ever 2 weeks
• 25 previously treated pts (14M/11F):– Bone (5)– Leiomyosarcoma (5)– Liposarcoma (1)– Others (11)
• 39% demonstrated > 25% decrease in [18F] FDG PET uptake.
• Symptomatic improvement in 13 pts.
Sankhala KK, et al. Proc ASCO 23:9028a, 2005.
Phase III Trial of AP23573 Maintenance Rx in STS/Bone Sarcomas
• Randomized, placebo-controlled, double-blinded trial to compare efficacy of PO AP23573 40 mg QDx5/week vs. placebo.
• Met. sarcoma patients who have CR/PR following 4-12 cycles of cytotoxicchemotherapy.
Ariad. Protocol AP23573-07-301, 2007.

Sorafenib
• Raf kinase, PDGFR-β, and VEGF-R inhibitor that inhibits tumor proliferation and angiogenesis.
• Multi-center, phase II trial for non-GIST sarcomas reported at ASCO, 2007.– 2/37 RECIST PR’s in leiomyosarcoma (6%
RR)– 3/23 PR’s in angiiosarcoma (13% RR)
• U. Chicago consortium trial in imatinib and sunitinib-resistant GIST.
D’Adamo DR, et al. Proc ASCO 25:10001a, 2007.Kindler HL, et al. Proc ASCO 26, 2008.
Dasatinib (BMS-354825)
• c-SRC is a proto-oncogene, non-receptor tyrosine kinase; induces VEGF expression thru STAT3.
• Dasatinib is a broad spectrum ATP-competitive inhibitor of SRC family kinases, BCR-ABL, c-KIT, EPhA2 receptor, and PDGFR-β.
• Dasatinib is 2-3 logs more potent than imatinibmesylate in inhibiting BCR-ABL .
• Dasatinib is capable of binding to both the open (active) and closed (inactive) conformations of c-ABL; imatinib mesylate can only bind to the inactive state.
SARC. Protocol 009, 2007.
Eli Lilly: LY573636
• Novel cytotoxic agent w/ activity across broad range of human cancer cell lines.
• Unique MOA unlike other cytotoxics.• Promotes apoptosis via increase ROS.• Phase II, open-label study as 2nd or 3rd line
therapy for unresectable or met STS (1 must be doxorubicin-based).
Eli Lilly and Co. Protocol H8K-MC-JZAD, 2007.

Amgen: Phase Ib/2 Study of AMG 655 + Doxorubicin for 1st line Rx of STS
• Tumor necrosis factor (TNF)-related apoptosis-inducing ligand (TRAIL) is natural ligand for TRAIL receptor 2 (DR5).
• Activation of TR2/DR5 initiates caspase cascade and apoptosis.
• AMG 655 mimics endogenous TRAIL.• Sarcomas express high levels of TR-1 and TR-2.• AMG 655 AE’s: fever, fatigue, anemia, nausea,
increased lipase, hypomagnesmia, lymphopenia.
Amgen. Protocol 20060324, 2007.

Insulin-like Growth Factor-1 Signaling
Sachdev, et al. Mol Cancer Ther 6: 1-12, 2007.
Sarcoma Alliance for Research thru Collaboration (SARC) #011
• Phase II Trial of R1507 (MoAb Insulin-Like Growth Factor-1 Receptor):– Ewing’s sarcoma– Osteosarcoma– Synovial sarcoma– Rhabdomyosarcoma– Other sarcomas
• High levels of IGF1R expressed in no. of pediatric solid tumors.
• R1507 inhibits downstream targets of IGF-1R (PI-3K, MAPK)
SARC. Protocol 011, 2007.
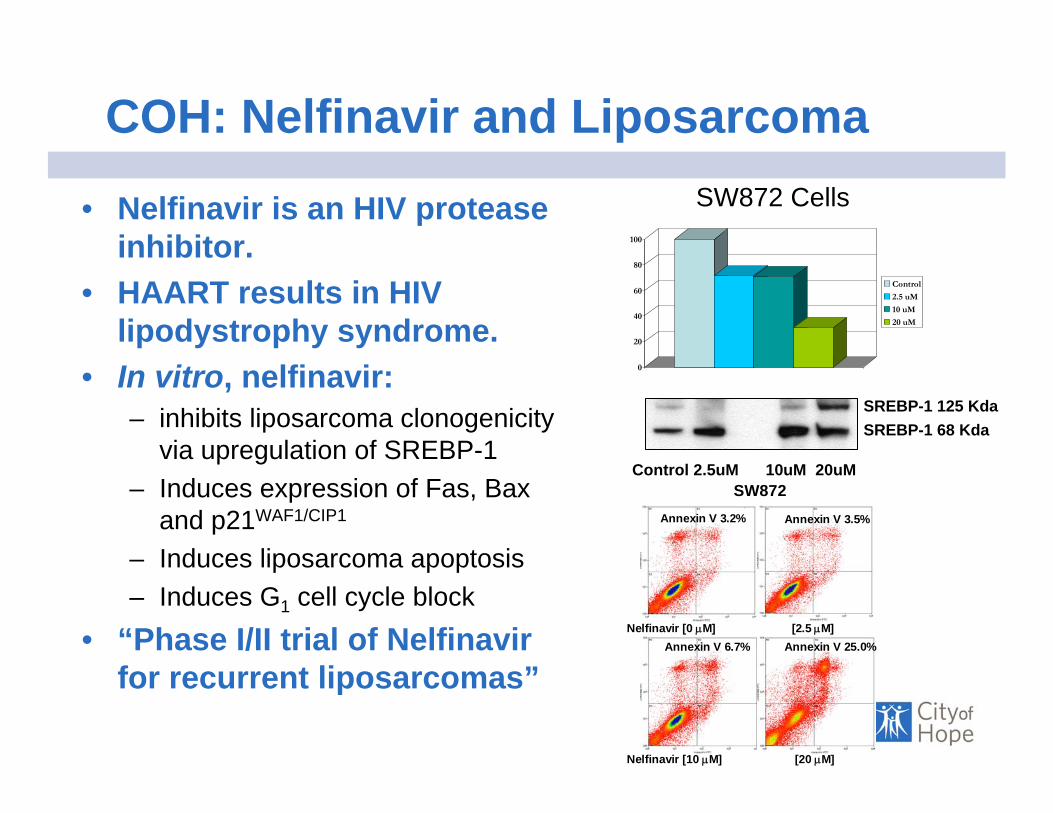
COH: Nelfinavir and Liposarcoma
• Nelfinavir is an HIV protease inhibitor.
• HAART results in HIV lipodystrophy syndrome.
• In vitro, nelfinavir:– inhibits liposarcoma clonogenicity
via upregulation of SREBP-1– Induces expression of Fas, Bax
and p21WAF1/CIP1
– Induces liposarcoma apoptosis– Induces G1 cell cycle block
• “Phase I/II trial of Nelfinavirfor recurrent liposarcomas”
0
20
40
60
80
100
Control
2.5 uM
10 uM
20 uM
SW872 Cells
Annexin V 3.2%
Annexin V 25.0%Annexin V 6.7%
Annexin V 3.5%
Nelfinavir [0 μM] [2.5 μM]
Nelfinavir [10 μM] [20 μM]
SW872Control 2.5uM 10uM 20uM
SREBP-1 125 KdaSREBP-1 68 Kda

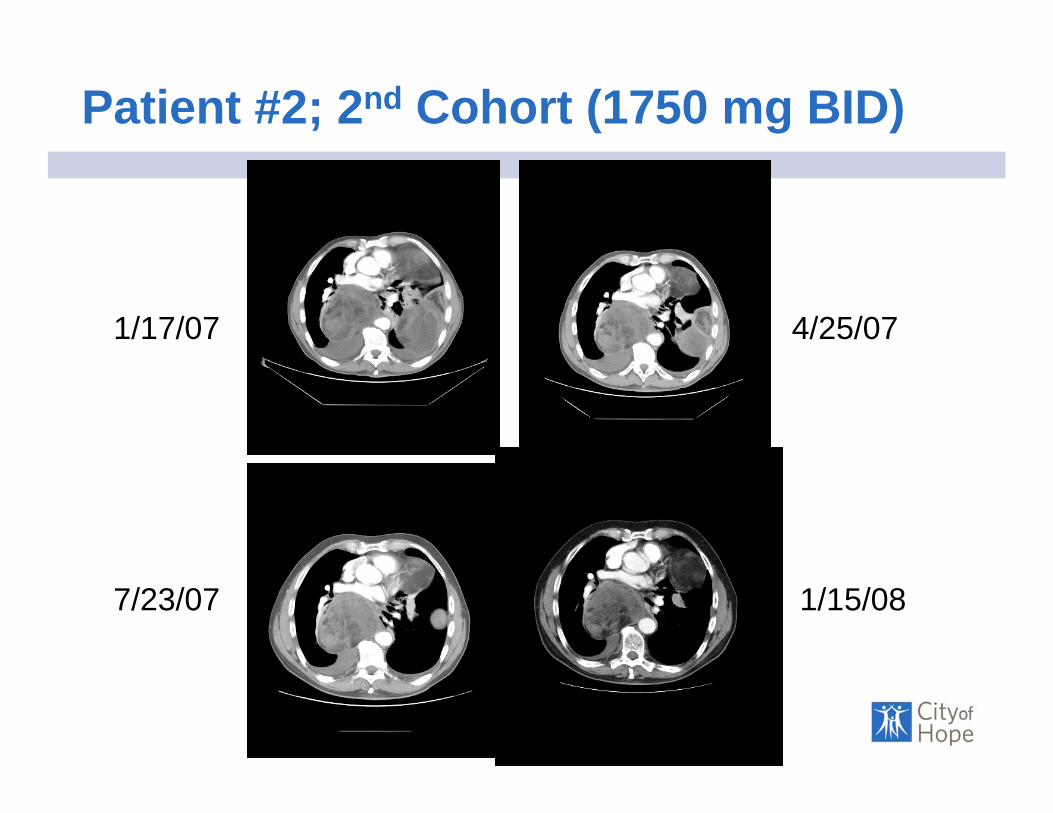
Patient #2; 2nd Cohort (1750 mg BID)
1/17/07 4/25/07
1/15/087/23/07

Patient #2; 2nd Cohort (1750 mg BID)
1/17/07 4/25/07
7/23/07 1/15/08
Patient #2; 2nd Cohort (1750 mg BID)
1/17/07 4/25/07
7/23/07 1/15/08

Conclusions
• Benefit of adjuvant chemotherapy with Ifosfamide and an anthracycline is probablyprobablylimited.
• Other chemotherapies indicated for specific specific histologichistologic types of sarcomas.
• Imatinib mesylate for GISTs has produced active research in tyrosine tyrosine kinasekinase inhibitioninhibitionfor GIST and other sarcomas.
•• New targetsNew targets are currently being identified in sarcomas, which may result in development of novel therapeutics.
Acknowledgements
• Chow Laboratory– Min Guan, Ph.D.– Chunling Jiang, Ph.D.– Song Guo (U. Wisconsin)
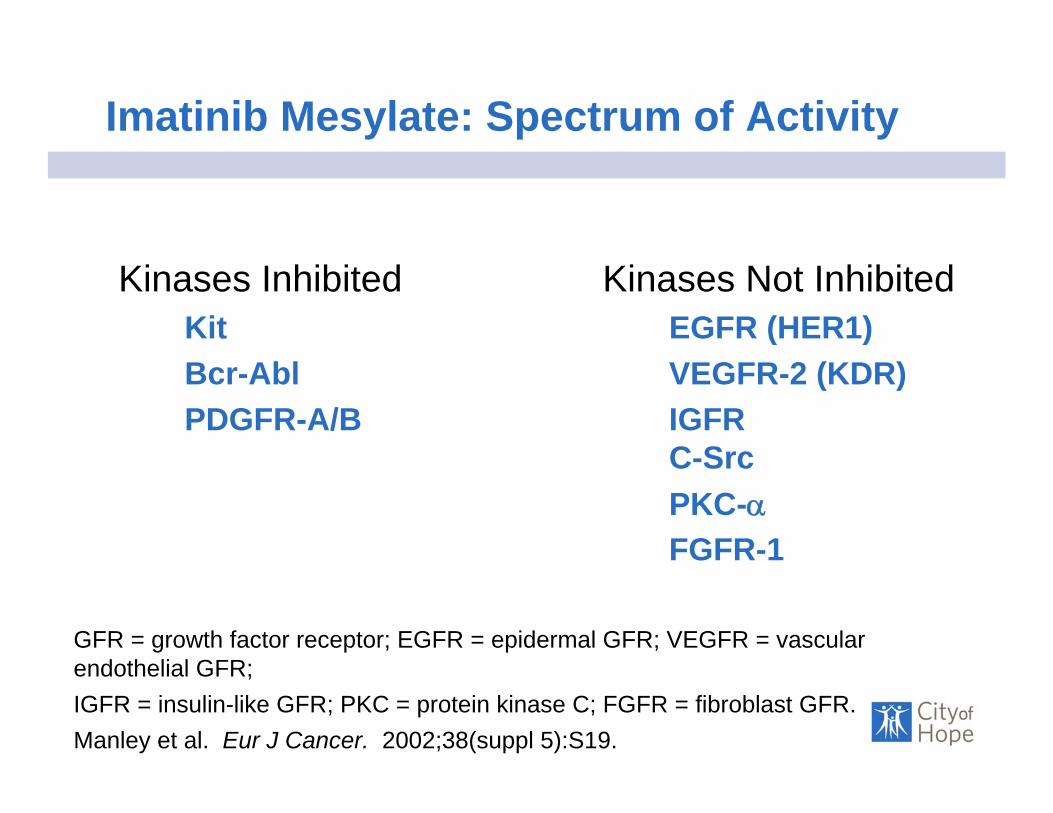
Imatinib Mesylate: Spectrum of Activity
Kinases Inhibited Kinases Not InhibitedKit EGFR (HER1)Bcr-Abl VEGFR-2 (KDR)PDGFR-A/B IGFR
C-SrcPKC-αFGFR-1
GFR = growth factor receptor; EGFR = epidermal GFR; VEGFR = vascular endothelial GFR; IGFR = insulin-like GFR; PKC = protein kinase C; FGFR = fibroblast GFR.Manley et al. Eur J Cancer. 2002;38(suppl 5):S19.

10 μM imatinib mesylate
GIST: Preclinical Efficacy of Imatinib Mesylate on GIST Cell Cultures In Vitro
• Imatinib mesylate inhibits proliferation and induces apoptosis in GIST cell culture
*GIST-882 and ST88-014 are GIST- and peripheral nerve sheath–derived cell lines, respectively.Tuveson et al. Oncogene. 2001;20:5054.
30
25
20
15
10
5
04 days 7 days
PBS
% A
nnex
in(+
), PI
(-)
0 1 3 50
102030405060708090
100
No.
of c
ells
×10
,000
Days
10 μM imatinib mesylate (GIST-882)PBS (GIST-882)
PBS (ST88-014)10 μM imatinib mesylate (ST88-014)


















