COLOMBIA Cali, Marzo 17 de 2005 PLAN DE IMPLEMENTACION DEL SGRI.
Upload
carlos-cuelloCategory
view
213download
1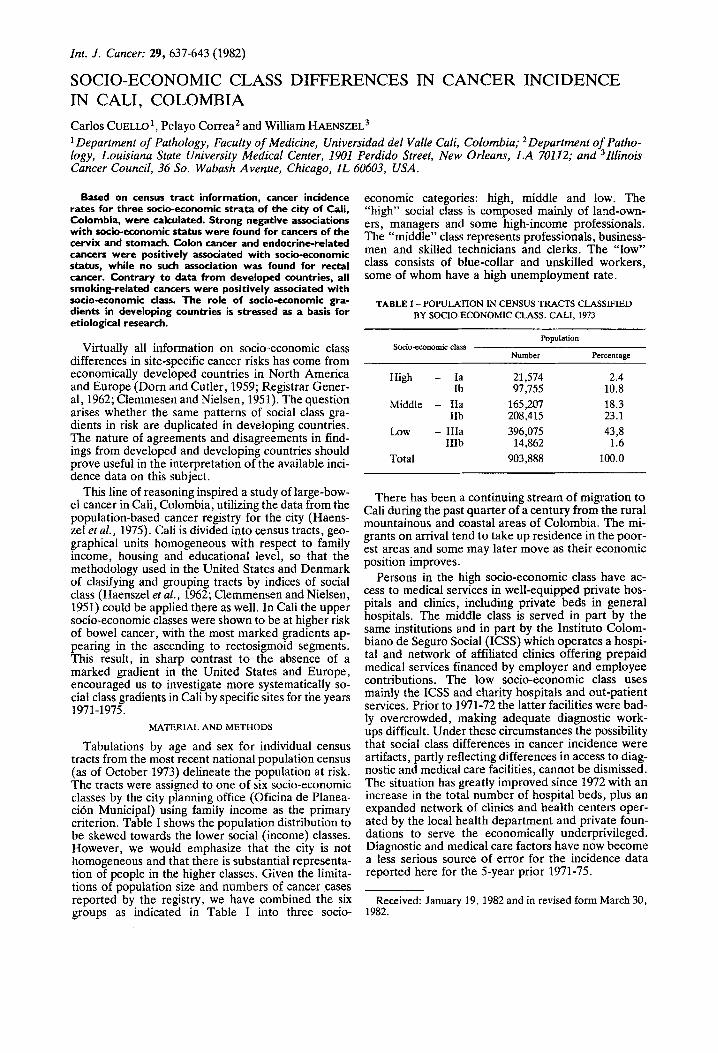
Int. J . Cancer: 29, 637-643 (1982)
SOCIO-ECONOMIC CLASS DIFFERENCES IN CANCER INCIDENCE IN CALI, COLOMBIA Carlos CUELLO~, Pelayo Correa2 and William HAENSzEL3 Department of Pathology, Faculty of Medicine, Universidad del Valle Cali, Colombia; Department of Patho-
logy, Louisiana State University Medical Center, 1901 Perdido Street, New Orleans, LA 70112; and Illinois Cancer Council, 36 So. Wabash Avenue, Chicago, IL 60603, USA.
Based on census tract information, cancer incidence rates for three socio-economic strata of the city of Cali, Colombia, were calculated. Strong negative associations with socio-economic status were found for cancers of the cervix and stomach. Colon cancer and endocrine-related cancers were positively associated with socio-economic status, while no such association was found for rectal cancer. Contrary to data from developed countries, all smoking-related cancers were positively associated with socio-economic class. The role of socio-economic gra- dients in developing countries is stressed as a basis for etiological research.
Virtually all information on socio-economic class differences in site-specific cancer risks has come from economically developed countries in North America and Europe (Dom and Cutler, 1959; Registrar Gener- al, 1962; Clemmesen and Nielsen, 1951). The question arises whether the same patterns of social class gra- dients in risk are duplicated in developing countries. The nature of agreements and disagreements in find- ings from developed and developing countries should prove useful in the interpretation of the available inci- dence data on this subject.
This line of reasoning inspired a study of large-bow- el cancer in Cali, Colombia, utilizing the data from the population-based cancer registry for the city (Haens- zel et al., 1975). Cali is divided into census tracts, geo- graphical units homogeneous with respect to family income, housing and educational level, so that the methodology used in the United States and Denmark of clasifying and grouping tracts by indices of social class (Haenszel et al., 1962; Clemmensen and Nielsen, 1951) could be applied there as well. In Cali the upper socio-economic classes were shown to be at higher risk of bowel cancer, with the most marked gradients ap- pearing in the ascending to rectosigmoid segments. This result, in sharp contrast t o the absence of a marked gradient in the United States and Europe, encouraged us to investigate more systematically so- cial class gradients in Cali by specific sites for the years 197 1-1 975.
MATERIAL AND METHODS
Tabulations by age and sex for individual census tracts from the most recent national population census (as of October 1973) delineate the population at risk. The tracts were assigned to one of six socio-economic classes by the city planning office (Oficina de Planea- cion Municipal) using family income as the primary criterion. Table I shows the population distribution to be skewed towards the lower social (income) classes. However, we would emphasize that the city is not homogeneous and that there is substantial representa- tion of people in the higher classes. Given the limita- tions of population size and numbers of cancer cases reported by the registry, we have combined the six groups as indicated in Table I into three socio-
economic categories: high, middle and low. The “high” social class is composed mainly of land-own- ers, managers and some high-income professionals. The “middle” class represents professionals, business- men and skilled technicians and clerks. The “low” class consists of blue-collar and unskilled workers, some of whom have a high unemployment rate.
TABLE I -POPULATION IN CENSUS TRACTS CLASSIFIED BY SOCIO-ECONOMIC CLASS. CALI. 1973
Population Socio-economic class
Percentage Number
High - la 21,574 2.4 Ib 97,755 10.8
Middle - Ila 165,207 18.3 23.1
L o w - IIIa 396,075 43,8 IIIb 14,862 1.6
Total 903,888 100.0
IIb 208,415
There has been a continuing stream of migration to Cali during the past quarter of a century from the rural mountainous and coastal areas of Colombia. The mi- grants on arrival tend to take up residence in the poor- est areas and some may later move as their economic position improves.
Persons in the high socio-economic class have ac- cess to medical services in well-equipped private hos- pitals and clinics, including private beds in general hospitals. The middle class is served in part by the same institutions and in part by the Instituto Colom- biano de Seguro Social (ICSS) which operates a hospi- tal and network of affiliated clinics offering prepaid medical services financed by employer and employee contributions. The low socio-economic class uses mainly the ICSS and charity hospitals and out-patient services. Prior to 1971-72 the latter facilities were bad- ly overcrowded, making adequate diagnostic work- ups difficult. Under these circumstances the possibility that social class differences in cancer incidence were artifacts, partly reflecting differences in access to diag- nostic and medical care facilities, cannot be dismissed. The situation has greatly improved since 1972 with an increase in the total number of hospital beds, plus an expanded network of clinics and health centers oper- ated by the local health department and private foun- dations to serve the economically underprivileged. Diagnostic and medical care factors have now become a less serious source of error for the incidence data reported here for the 5-year prior 1971-75.
Received: January 19, 1982 and in revised form March 30, 1982.

TABL
E U
- AG
E-A
DJU
STE
D C
AN
CE
R I
NC
IDE
NC
E R
AT
ES
PER
100,ooO PO
PUL
AT
ION
FO
R T
HR
EE
SO
CIO
-EC
ON
OM
IC C
LA
SSE
S B
Y SITE
AN
D S
EX
. CA
LI,
197
1-19
75
Men
W
omen
Si
te
Hia
h M
iddl
e L
OW
H
igh
Mid
dle
LO
W
All
sites
A
ll si
tes,
exc
ludi
ng sk
in
Bucc
al c
avity
Ph
aryn
x Es
opha
gus
Stom
ach
Larg
e in
test
ine
Rec
tum
Bi
liary
pas
sage
Pa
ncre
as
Lary
nx
Lung
and
bro
nchu
s M
elan
oma
Oth
er sk
in
Brea
st
Cex
vix
uter
i C
orpu
s ute
ri
Ova
ry
Pros
tate
Te
stic
le
Blad
der
Kid
ney
and
othe
r ur
inar
y Br
ain
and
cent
ral n
ervo
us sy
stem
Th
yroi
d Ly
mph
omas
H
odgk
in’s
dise
ase
Leuk
emia
(non
-mel
anom
a)
107.
3 11
8.3
130.
5
81.8
91
.5
102.
3 2.
2 4.
0 6.
7 0.
2 0.
9 2.
6 0.
6 1.
7 3.
7 10
.3
14.0
18
.6
1.5
3.0
5.4
0.3
1.1
2.8
0.1
0.6
2.2
0.8
2.0
4.1
3.6
4.5
7.3
7.7
10.7
14
.7
0.1
0.6
2.2
21.7
26
.8
33.2
-
8.5
11.8
15
.9
0.4
1.6
4.1
4.9
7.5
11.0
1.
1 2.
5 4.
9 0.
7 2.
0 4.
4 0.
2 0.
9 2.
6 3.
7 6.
1 9.
5 0.
4 1.
3 3.
3 2.
9 4.
9 7.
8
101.
6 10
8.4
115.
6 83
.8
90.4
97
.6
114.
0 12
4.1
135.
0
82.2
88
.3
94.8
74
.2
80.4
87
.1
91.9
10
0.9
110.
8 1.
5 2.
4 3.
7 1.
2 2.
1 3.
4 1.
0 2.
2 4.
2 0.
6 1.
2 2.
2 0.
2 0.
6 1.
5 c0
.05
0.2
1.1
0.5
1.1
2.1
0.6
1.3
2.5
0.5
0.4
1.4
19.7
22
.7
26.1
18
.7
21.9
25
.6
5.6
7.9
10.9
1.
3 2.
2 3.
4 1.
0 1.
8 3.
0 1.
5 2.
7 4.
5 1.
0 1.
8 2.
9 0.
9 1.
7 2.
9 0.
5 0.
4 1.
4 1.
3 2.
2 3.
4 0.
7 1.
4 2.
5 1.
5 2.
8 4.
7 1.
1 1.
9 3.
0 1.
1 2.
0 3.
4 1.
0 2.
1 3.
9 1.
8 2.
8 4.
1 1.
0 1.
8 3.
1 0.
1 0.
6 1.
8 5.
9 7.
6 9.
7 5.
8 7.
7 10
.1
1.4
2.7
4.7
0.7
1.4
2.5
0.3
0.8
1.7
0.2
0.9
2.3
17.3
20
.1
23.5
7.
9 9.
9 12
.5
19.1
23
.2
28.1
-
-
22.7
27
.3
32.8
9.
7 12
.8
16.8
2.
1 3.
6 5.
8 c
-
5.1
7.4
10.5
-
-
-
-
8.0
9.9
12.3
5.
6 7.
6 10
.0
-
0.5
1.0
1.9
0.6
1.2
2.2
-
2.4
3.5
5.0
2.0
3.1
4.7
0.8
1.7
3.2
0.5
1.1
2.0
0.1
0.4
1.0
0.2
0.9
2.3
2.0
3.1
4.5
1.3
2.1
3.3
1.9
3.5
6.0
0.6
1.2
2.2
0.1
0.5
1.3
2.2
3.8
6.2
3.6
5.0
6.7
4.9
6.5
8.5
1.7
3.2
5.4
0.6
1.3
2.3
2.2
3.3
4.9
0.6
1.6
3.3
3.1
4.4
6.0
2.6
3.7
5.2
1.3
2.7
4.8
135.
4
116.
3 1.
6 0.
3 0.
2 12
.4
2.1
0.9
3.1
1.0
0.2
1.8
0.6
17.1
15
.2
28.0
2.
6 4.
9
0.5
1 .o
1.1
2.6
1.9
0.4
2.3
112.
5
122.
9 2.
4 0.
7 0.
5 14
.5
3.0
1.5
4.3
1.7
0.5
2.7
1.1
19.6
17
.6
31.2
3.
7 6.
3 - I
1.0
1.7
1.8
3.7
2.8
0.9
3.3
149.
6
129.
5 3.
5 1.
4 1.
1 17
.0
4.2
2.4
5.8
2.7
1.2
3.9
1.9
22.5
20
.4
34.8
5.
0 8.
1
1.8
2.7
2.8
5.0
4.0
1.7
4.5
112.
1
102.
0 1.
3 0.
5 0.
3 9.
6 0.
4 0.
4 1.7
0.5
0.1
1.6
<0.0
5 8.
4 10
.2
34.0
1.
2 4.
2
0.4
0.4
0.7
2.1
2.1
0.6
2.6
118.
9 12
6.2
108.
6 11
5.6
2.2
3.4
1.0
1.9
0.7
1.5
11.7
14
.2
0.9
1.8
0.9
1.8
2.7
4.1
1.1
2.1
r
0.5
1.3
6 0.
2 2.
5 0.
7 3.
8 > 3
10.3
12
.5
r
12.3
15
.0
37.8
42
.0
2.0
3.2
5.6
7.4
-
-
0.9
1.8
0.9
1.7
1.3
2.2
3.2
4.6
3.1
4.5
1.2
2.1
3.8
5.3
CANCER INCIDENCE IN CALI
% -
5 -
a -
:: 5 -
639
f P
i C 4 I l l l
Newly-diagnosed cancer cases of Cali residents dur- ing the 5-year period 1971-75, for which the October 1973 census was the approximate midpoint, were clas- sified by census tract of residence in a manner consis- tent with that described above for the population cen- sus data. The cancer registry covering the city of Cali has been in operation since 1962. The information is collected by active search through the files of hospitals and other medical facilities, supplemented by an an- nual survey by trained groups of medical students of the records in these same institutions and in the offices of local practitioners and laboratories. All cancer diagnoses, including those entered on death certifi- cates, have a very high probalitity of being entered in the registry. The accumulated backlog of case reports accurately distinguishes new diagnoses from previous- ly reported cases. The local medical school has an active department of pathology and diagnostic evi- dence is good; 85 % of all diagnoses were microscopi- cally confirmed.
Sex-and age-specific incidence rates were calculated for the three socio-economic classes using the registry and census data. Because there were relatively small numbers of cases for each site, we adjusted the rates for age by the direct method, using as the standard population the 1973 census population for Cali (both sexes combined) (Table 11). Use of the same standard population permits the age-adjusted rates for each sex to be compared with each other.
Because of the small number of cases observed, the age-specific and age-adjusted rates are subject to sub- stantial chance variation. To indicate the degree of variability the approximate 95 % confidence limits of the age-adjusted rates in Table I1 have been estimated using tables prepared by Mantel (Haenszel et af., 1962).
RESULTS
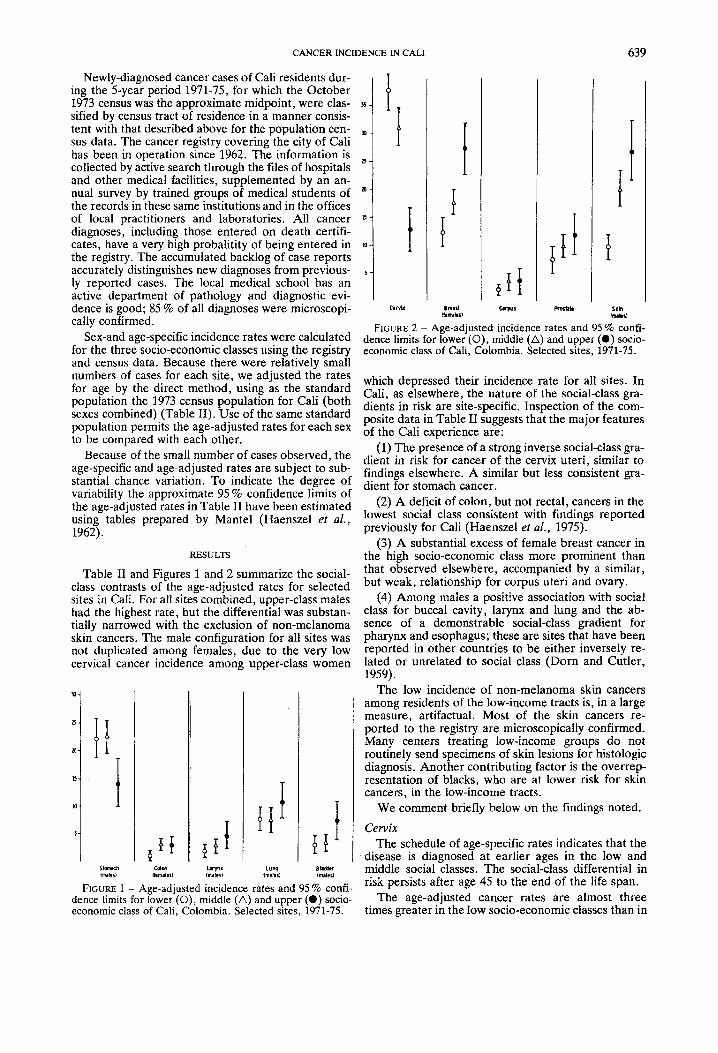
Table I1 and Figures 1 and 2 summarize the social- class contrasts of the age-adjusted rates for selected sites in Cali. For a11 sites combined, upper-class males had the highest rate, but the differential was substan- tially narrowed with the exclusion of non-melanoma skin cancers. The male configuration for all sites was not duplicated among females, due to the very low cervical cancer incidence among upper-class women
a-
:: :I 5 -
t [ I
T
I I
FIGURE 2 - Age-adjusted incidence rates and 95 % confi- dence limits for lower (0), middle (A) and upper (0) socio- economic class of Cali, Colombia. Selected sites, 1971-75.
which depressed their incidence rate for all sites. In Cali, as elsewhere, the nature of the social-class gra- dients in risk are site-specific. Inspection of the com- posite data in Table I1 suggests that the major features of the Cali experience are:
(1) The presence of a strong inverse social-class gra- dient in risk for cancer of the cervix uteri, similar to findings elsewhere. A similar but less consistent gra- dient for stomach cancer.
(2) A deficit of colon, but not rectal, cancers in the lowest social class consistent with findings reported previously for Cali (Haenszel et af., 1975).
(3) A substantial excess of female breast cancer in the high socio-economic class more prominent than that observed elsewhere, accompanied by a similar, but weak, relationship for corpus uteri and ovary.
(4) Among males a positive association with social class for buccal cavity, larynx and lung and the ab- sence of a demonstrable social-class gradient for pharynx and esophagus; these are sites that have been reported in other countries to be either inversely re- lated or unrelated to social class (Dom and Cutler, 1959).
The low incidence of non-melanoma skin cancers among residents of the low-income tracts is, in a large measure, artifactual. Most of the skin cancers re- ported to the registry are microscopically confirmed. Many centers treating low-income groups do not routinely send specimens of skin lesions for histologic diagnosis. Another contributing factor is the overrep- resentation of blacks, who are at lower risk for skin cancers, in the low-income tracts.
We comment briefly below on the findings noted.
Cervix The schedule of age-specific rates indicates that the
disease is diagnosed at earlier ages in the low and middle social classes. The social-class differential in risk persists after age 45 to the end of the life span.
The age-adjusted cancer rates are almost three
SlDmaCh C O l M L l r y l " LUW Bllddlr lmlnl lhmalirl imaleil fnl1llSl IMllrl
FIGURE 1 - Age-adiusted incidence rates and 95 % confi- dence limits for ibwe;(O), middle (A) and upper (0) socio- economic class of Cali, Colombia. Selected sites, 1971-75. times greater in the low socio-economic classes than in

640 CUELLO ET AL.
TABLE in - AGE-ADJUSTED CANCER INCIDENCE RATES PER 100,WO POPULATION BY SOCIO-ECONOMIC CLASS FOR SELECED HORMONE-DEPENDENT SITES. CALI, 1971-1975
All ages Age 55 and over -.
High Middle Low High Middle Low
Females Breast 27.3 17.6 12.3 146.9 99.4 77.5 Endometrium 3.6 3.7 2.0 33.1 30.1 14.9 Ovary 7.4 6.3 5.6 48.2 31.0 21.0 Colon 2.7 3.0 0.9 34.8 29.9 9.9
Prostate 11.8 9.9 7.6 153.8 99.1 104.0 Colon 3.0 2.2 1.8 42.1 18.2 11.9
Males
the upper ones. Indications of a strong socio-economic gradient were first detected by studying the distribu- tion of cases in the different boroughs of the city (Cor- rea and Llanos, 1966).
A study of precursor lesions in autopsy and surgical specimens failed to show a socio-economic gradient in the prevalence of such lesions, suggesting that promo- tional rather than initiating factors are responsible for the excessive rates in lower socio-economic strata (Duque ef al., 1979).
Stomach The deficit in risk for the high-income tracts was
most pronounced at age 55 and over. The dominant epidemiological characteristic of stomach cancer in Cali is the high risk among migrants from the moun- tainous Andean regions and the low risk for persons born in the tropical coastal regions of Colombia (Cor- rea et al., 1970). Both groups are represented in the low and middle classes and confounding with birth- place probably accounts for the failure to detect a dif- ference in risk between the two lower social classes.
Large bowel The excess of large bowel (colon) cancers in the
upper social classes is consistent with observations on a larger series of cases assembled during 1962-71 (Haenszel ef al., 1975). The present series pinpoints a social-class gradient among persons over age 55 (see Table 111). The findings for colon resemble those for breast and other endocrine-related sites.
While tumor localization was not studied in detail for the present series, the available information sup- ports the conclusion drawn earlier of an excess risk concentrated in the sigmoid and adjacent segments.
No social-class gradient for this site has been de- scribed in North America and western Europe and we have suggested that its expression in Cali may be link- ed to profound local social-class differences in dietary intake of animal protein and fats (Haenszel et al., 1975; Boyd ef al., 1964). Breast
The age-specific rates show upper-class women to have higher risks throughout the life span. The social- class gradient in risk is most pronounced at post- menopausal ages. The curve of log-incidence for women in the high social class displays the positive slope characteristic of developed countries while the results for the middle and low classes suggest a zero or
negative slope, the latter corresponding to the experi- ence of developing countries. The correlation between social class and slope of the postmenopausal curve was also described in the Cali data for 1962-71, which used a slightly different scheme for the combination of census tracts by social class (Cuello and Duque, 1978).
Cuello and Duque (1978) in their examination of the 1962-71 Cali data also observed that the social- class differences in incidence were concentrated in the class of infiltrating carcinomas with marked fibrosis, particularly at ages over 55. The ability to demon- strate that the breast cancer differentials are concen- trated in a histologic type category and are not an across-the board effect strengthens the inference that the reported social-class gradient is real and not an observational artifact.
Other hormone-dependent sites The high risk in the upper social classes noted for
breast may extend to other hormone-dependent sites such as endometrium, ovary, prostate and colon. Co- lon is placed in this category because of the similar patterns of geographic variation in risk for breast and colon and other epidemiological evidence for sex-link- ed factors in the etiology of colon cancer (Correa and Haenszel, 1978). Table I11 shows the age-adjusted rates (all ages) by social-class for these sites with a separate comparison for ages 55 and over (also age- adjusted). The latter results indicate that the experi- ence at older ages is a major contributor to the ap- parent social-class gradient in risk that prevails in Cali for these sites.
Smoking-rela fed sites The sites with well-documented associations with
tobacco use include buccal cavity and pharynx (ex- cluding salivary gland), esophagus, larynx, lung and urinary bladder (Doll and Hill, 1964). Since the pat- terns of social-class variation in risk may be influenced by associations between social class and tobacco use, it may be helpful to consider the data for these sites as an entity. Inspection of the detailed age-specific rates did not change the information conveyed by summary comparisons of the age-adjusted rates, presented in Table 11.
The collective Cali findings are readily summarized: the presence of social-class gradients in risk was li- mited to males. With the exception of pharynx and esophagus, higher incidence rates for the smoking-re- lated sites were reported for middle- and upper-class males. The absence of elevated rates for pharynx and esophagus among males in the lower socio-economic classes of Cali, sufficient to produce an inverse social- class gradient in risk, runs contrary to experience in other populations. Nevertheless, indirect evidence suggests that our data reflect well the actual situation. The Cali incidence for these two sites is modest when viewed in the perspective of international compari- sons, and for the overall Cali rates to rank higher in international comparisons a substantially elevated risk in the lower social classes would be required.
The Cali data agree with findings reported in the US, Denmark and England that the associations with social class for the smoking-related sites are more strongly expressed among men than among women.

CANCER INCIDENCE IN CALI 641
However, the tendency for risk to rise with social-class (direct association) for several of the smoking-related sites is not reproduced in data from other sources and may be unique to Cali. The data for males from the US, Denmark and England (Fraumeni et al., 1969; Kahn, 1966; Doll and Peto, 1976) have consistently described an inverse (not a direct) relationship with social-class for buccal cavity, pharynx, esophagus, larynx and lung. The male bladder-cancer risk appears unrelated to social-class.
The data on social-class differences from the United States and western Europe relate primarily to condi- tions 20-30 years earlier. It is conceivable that, over time, the inverse gradients have been gradually trans- formed to direct gradients in risk for smoking-related sites, but this seems highly unlikely. Doll and Pet0 (1976) have commented on the greater tendency for upper-class men to discontinue cigarette use and this phenomenon should operate to reinforce the inverse gradient in risk rather than to weaken it.
DlSCUSSION
Social-class per se is not an etiological factor and any social-class gradient in cancer risk must reflect indirect associations between social-class and other causative factors. There is no reason to believe that the indirect associations will be the same in all coun- tries and all environments and inconsistencies among populations in social-class risk gradients for specific sites may be expected. Indee& inter-population varia- bility in social-class gradients may provide clues on etiology to complement other evidence. We comment briefly on some of the Cali findings from this point of view. Cervix uteri
Several studies have identified early age at first coitus, multiple partners and related aspects of sex and reproductive history as risk factors for cervical carcinoma (Boyd and Doll, 1964; Rotkin, 1973). More intense exposure to these factors among women in the lower social classes is common to Cali and com- munities in developed and developing countries gen- erally. The universally observed inverse social-class gradient for cervical carcinoma can be interpreted as consistent with an important role for sex and repro- ductive history and related exposures as determinants of the level of risk. Breast
A prominent feature of the Cali experience, a com- munity at low to intermediate risk for breast cancer, is the substantial excess liability to this disease among upper-class women, much of which is concentrated in the post-menopausal ages. A social-class risk gradient in either direction has not been an important charac- teristic of the breast cancer experience of women in the United States and western Europe (Dorn and Cutler, 1959; Clemmesen and Nielsen, 1951). The largest excess risk among women in the highest social- class suggested by the occupational mortality data for England and Wales, 40 %, falls well short of the two- fold and greater differential described by the Cali data. The situation with respect to social-class differ- ences in low-risk populations in other parts of the world remains to be determined.
An explanation of the Cali results should therefore emphasize a search for features present in Cali and absent elsewhere, or vice-versa. One of the firmly- established facts of breast-cancer epidemiology is the protective effect of early age at first full-term pregnan- cy. McMahon and co-workers (1973) have found this effect to prevail without exception in all populations studied by them. While a tendency to older maternal ages could raise breast cancer incidence among upper- class women, it is difficult to see why such an effect should be more strongly expressed in Cali than in other populations.
Given the evidence that estrogen plays a role in human breast cancer, the possibility for social-class effects mediated by differential exposure to exoge- nous estrogen (oral contraceptives, conjugated estro- gens for menopausal symptoms) might be entertained. Hard evidence for increased breast cancer risk among users of oral contraceptives and conjugated estrogens is lacking. The firmly documented excess risk linked to conjugated estrogens is limited to endometrial car- cinomas (Spengler et al., 1981). Furthermore, the use of exogenous estrogens in Cali has never reached the levels attained in North America and they seem un- likely candidates to account for the observed social- class differential.
The estrogen fraction hypothesis has been advanced by McMahon et al. (1971), who noted higher estriol ratios (estrone + estrodioVestrio1) in Asian and Afri- can women in the early years of reproductive life in populations at low breast-cancer risk and speculated on the protective effects of estriol. No studies have been conducted in Cali to determine whether social- class differences in estriol ratios, similar to those found in contrasts between communities at high and low risk, exist. Work along these lines should be at- tempted. Differences in internal hormonal environ- ment should presumably reflect nutritional factors and suggestive associations of diet with breast cancer have been reported (Carroll et al., 1968). Inter-country variation in breast-cancer risk has been correlated with per capita variation in fat comsumption (Correa, 1981). There is also a close correspondence in the dis- tribution of breast cancer risk with those for colon cancer and arteriosclerotic heart disease, both dis- eases linked to dietary etiologies (Wynder and Shigematsu, 1967). While there is no good evidence from studies of individuals relating breast cancer risk to diet intake, de Waard (1973) has reported height and weight (which can be considered a surrogate vari- able for nutrition) to descriminate among individuals for breast cancer risk.
The situation within Cali provides several parallels to that presented by the global comparisons. The ex- cess risk of breast cancer in the upper social-class of Cali coincides well with the Cali findings for large- bowel cancer and myocardial infarction (Haenszel et al., 1975). In this respect the congruence between the social-class differences within Cali and those described by inter-country variation is striking. The Cali social- class differences in disease risk are also accompanied by extreme differences in diet. A 1964 food consump- tion survey in Cali reported a 5-fold greater excess in the upper social-class in per capita consumption of beef, pork, eggs and milk accompanied by minimal

642 CUELLO ET AL.
differences for starchy vegetables (rice, corn, plan- tain, yucca, potatoes, beans) (Arag6n, 1964). The lower social-class diet is very high in starch, while the consumption of animal protein and fats is effectively limited to the upper socio-economic classes. We be- lieve that diet-mediated effects are the most promising explanation for the observed social-class differences and that studies in Cali to test this hypothesis should be pursued.
Larynx, lung The risks for lung and larynx are strongly associated
with tobacco use and an explanation for the elevated rates among upper-class males in Cali, as opposed to the inverse social-class gradient observed in developed countries (Haenszel et al., 1956), should first consider the questions of social-class and tobacco use. In the developed countries there is no real economic barrier to tobacco use but a greater proportion of ex-smokers is found in the upper socio-economic classes. In Co- lumbia the domestically grown cigarettes traditionally contain black tobacco and the imported cigarettes contain the light tobacco used in the US. Imported cigarettes are expensive and their cost precludes wide- spread use by the lower-income groups, who smoke cigarettes made with the black tobaccos. Local blends of black and light tobaccos have been recently intro- duced. The important social-class distinction is the much greater exposure of upper-income males to cigarettes made with light tobaccos. The overall rate of cigarette consumption by males is not believed to vary widely by social-class.
Animal experiments have shown tars from black tobacco to be more carcinogenic than tars from light tobacco (MuAoz et a]., 1968). A lower dosage from use of black tobacco is, therefore, an unlikely explana- tion of the reduced incidence among lower socio- economic-class males. An alternative might be a dif- ference in effective exposures. A slightly higher daily consumption rate, an earlier age at adoption of the cigarette habit and deeper inhalation of cigarette smoke by upper-class men might produce the social- class gradient in risk. A differential in inhalation prac- tices seems plausible, since black tobacco has a high pH and a strong aroma, producing a smoke which is more difficult to inhale than the combustion products of light tobacco. The hypothesized effects would be similar to those for pipe and cigar smokers, in whom the excess risks are limited to the oral cavity and pharynx and do not involve also the lung as is the case for cigarette smokers. The difficulty with this reason-
ing is that the observed male excess in the highest socio-economic-class includes buccal cavity, where no difference should prevail. The number of cases in this site group is small, however, and the apparent gra- dient in Cali may be an artifact of sampling variation.
Esophagus, pharynx The few cases of pharyngeal and esophageal cancer
observed in males do not delineate any clear pattern with respect to social-class. This negative aspect is of interest. It is worth emphasizing that the Cali data do not suggest the inverse relationship of risk with social- class typically found elsewhere (Dorn and Cutler, 1959). Both the esophagus and pharynx have been linked with tobacco and alcohol consumption and the possibility of a synergetic response from exposure to both agents has been raised (Tuyns, 1977). Nutritional status of the host may also be involved. A possible explanation for the inverse risk pattern would be greater use of tobacco and alcoholic beverages and poorer nutritional status in the lower class. All these conditions would prevail in Cali as well as other com- munities and we must seek a reason for the absence of a risk gradient there. The key may prove to be the absence of contaminants in the major local alcoholic beverage used by the lower classes: aguardiente. Mor- ton has suggested tannin as a risk factor for esophage- al cancer (Morton, 1968) and aguardiente contains no tannins or other contaminants introduced by fermen- tation processes. Examples pointing to an important role for contaminants can be cited; for example, Po- land has a extremely high per capita consumption of alcohol and very modest rates of cancer of the pharynx and esophagus (Waterhouse et al., 1976). The basic alcoholic drink is vodka which, like aguardiente, has very few contaminants. Conclusion
The above data indicate that the pattern of social- class gradients for cancer of different sites as observed in developing communities may be at variance with what has been established in the populations of de- veloped countries. The effects of social-class on the dietary and smoking patterns of the population may be responsible for some of the differences. Etiological leads may be provided by comparing contrasting pat- terns in populations from several countries.
ACKNOWLEDGEMENTS
This work was supported by contract N01-CP-53521 and grant Pol-CA-28842, National Cancer Institute, USPHS.
REFERENCES
ARAG6N. L A . , Estimaci6n del consumo de algunos alimentos bisicos en la ciudad de Cali (Tesis de Grado). Universidad del Valle, Facultad de Ciencias Enonbmicas, Cali (1964).
BOYD, J.T., and DOLL, R., A study of the aetiology of carcinoma of the cervix uteri. Brit. J . Cancer, 18, 419-434 (1964).
BOYD, J., LANGMAN, M., and DOLL, R., The epidemiology of gastrointestinal cancer with special reference to causation. Gut, 5, 196-200 (1964).
CARROLL, K.K., GAMMEL, E.B., and PLUNKETT, E.R., Dietary fat and mammary cancer. Cannd. med. Ass. J . , 98, 590-594 (1968).
CLEMMESEN, J., and NIEISEN, A . , The social distribution of cancer in Copenhagen, 1943 to 1947. Brir. J . Cancer, 5 , 159-171 (1951). CORREA, P., Epidemiologic correlations between diet and cancer frequency. Comer res., 41,3685-3690 (1981). CORREA, P., CUELLO, C., and DUQIJE, E., Carcinoma and intes- tinal metaplasia of the stomach on Colombian migrants. J . nut. Cancer Inst., 44, 297-306 (1970). C~RREA, P., and HAENSZEL, W . , Epidemiology of large bowel cancer. Advanc. Cancer Res., 26, 1-133 (1978). CORREA, P., and LLANOS, G., Morbidity and mortality from cancer in Cali, Colombia. J . nut. Cancer Inst., 36,717-745 (1966).

CANCER INCIDENCE IN CALI 643
CUELLO, C., and DUQUE, E., Breast cancer in Cali. In: An inter- national survey of the distribution of histologic types of breast cancer. UICC Technical Repori Series., Vol. 35, pp. 74-82, UICC, Geneva (1978). DE WAARD, F., Nurture and nature in cancer of the breast and the endometrium. In: R. Doll and 1. Vodopija (ed.), Host envi- ronment interactiom in the etiology of cancer in man. IARC Scien- tific Publication No. 7, International Agency for Research on Cancer, Lyon (1973). DOLL, R., and HILL, A.B., Mortality in relation to smoking: Ten years’ observations of British doctors. Brit. rned. J . , 1,1399-1410 (Part I) and 1460-1467 (Pan 11) (1964). DOLL, R., and PETO, R., Mortality in relation to smoking: 20 years’ observations on male British doctors. Brit. med. J . , 2,
DORN, H.F., and CUTLER, S.J., Morbidity from cancer in the United Stales. Public Health Monogr. 56, US Govt. Printing Of- fice, Washington, D.C. (1959). DUQUE, E., CUELLO, C., ARISTIZABAL, N., HAENSZEL, W., and CORREA, P. , Premalignant lesions of the cervix in women of Cali, Colombia. J. nat. Cancer Inst., 63,953-960 (1979). F u u m m , J.F., LLOYD, J.W., SMITH, E.M., and WAGONER, J . K . , Cancer mortality among nuns: role of marital status in etiol- ogy of neoplastic disease in women. J . nut. Cancer Inst., 42,455- 468 (1969). HAENSZEL, W., CORREA, P., and CUEUO, C. , Social-class differ- ences among patients with large bowel cancer in Cali, Colombia. J . nat. Cancer Inst., 54, 1031-1035 (1975). HAENSZEL, W., LOVELAND, D.B., and SIRKEN, M., Lung cancer mortality as related to residence and smoking histories. I. White males. J . nut. Cancer Inst., 28, 947-1001 (1962). HAENSZEL, W., SHIMKIN, M.B., and MILLER, H., Tobacco smok- ing patterns in the United States. Publ. Hltb Monogr., 45, US Govt. Printing Office, Washington, D.C. (1956).
1525-1536 (1976).
KAHN, H.A., The Dorn study of smoking and mortality among US Veterans: Report on eight and one half years of observation. Nut. Cancer Inst. Monogr., 19, 1-125 US Govt. Printing Office, Washington, D.C. (1966). MACMAHON, B., COLE, P. , and BROWN, J., Etiology of human breast cancer: a review. J . nat. Cancer h t . , 50, 21-42 (1973). MACMAHON, B., COLE, P., BROWN, J.B., AOKI, K., Lui, T.M., MORGAN, R.W., and Woo, N., Oestrogen profiles of Asian and North American women. Lancet, 2,900-902 (1971). MORTON, J.F., Plants associated with esophageal cancer cases in Curacao. Cancer Res., 28, 2268-2271 (1968). MuNoz, N., CORREA, P., and BOCK, F.G., Comparative car- cinogenic effect of two types of tobacco. Cancer, 21, 376-389 (1968). REGISTRAR GENERAL OF ENGLAND AND WALES, The Registrar General‘s Decennial Supplement, Occupational Mortality Tables, 1921, 1931, 1951, 1961. HM Stationary Office, London (1962). ROTKIN, I.D., A comparison review of key epidemiologic studies in cervical cancer related to current searches for transmissible agents. Cancer Res., 33, 1353-1367 (1973). SPENGLER, R.F., CLARKE, E.A., WOOLEVA, C.A., NEWMAN, A.M., and OSBORN, R.W., Exogenous estrogens and endomet- rial cancer: A case-control study and assesment of potential biases. Amer. J . Epidem., 114,497-506 (1981). TUYNS, A.J., PEQUIGNOT, G., and JENSEN, O.M., Le cancer de I’oesophage en Ilk-et-Vilaine en fonction des niveaux de con- sommation d’alcool et de tabac. Bull. Cancer, 64, 45-60 (1977). WATERHOUSE, J . , MUIR, C., CORREA, P., and POWELL, J., (ed.), Cancer incidence in five continents, Vol. 3. IARC Scientific Publi- cations No. I S , International Agency for Research on Cancer, Lyon (1976). WYNDER, E.L., and SHIGEMATSU, T., Environmental factors of cancer of the colon and rectum. Cancer, 20, 1520-1561 (1967).