Social determinants of diagnostic labels in depression
9
Social Science & Medicine 62 (2006) 50–58 Social determinants of diagnostic labels in depression Susan McPherson , David Armstrong Tavistock & Portman NHS Trust, Belsize Centre, 94 Belsize Lane, London NW3 5NE, UK Available online 11 July 2005 Abstract The role of diagnostic labels in medicine is usually that of labelling an illness as a means of communication. Control over labelling processes in medicine is ordinarily imposed via medical schools, textbooks, education or by diagnostic manuals. Diagnostic labels often change following new discoveries in underlying pathology such as ‘consumption’ being relabelled as ‘TB’ or ‘cancer’. Sub-types of broad diagnostic labels also often emerge from such discoveries e.g. ‘lung cancer’ or ‘throat cancer’. In mental health, underlying pathology is the subject of ongoing debate spanning ideas including the brain as a faulty organ, faulty genetics and environmental problems. With controversy over pathology comes controversy over labels and the idea that labels may be used not just for communication, but as devices of social and professional control, arising out of a social process. This study explores the codification of the diagnostic label ‘depression’ which emerged in the twentieth-century and has proliferated with numerous sub-types over the last 40 years. The aim is to examine its social determinants and context. Medline is used as a data source for professional label usage. A range of depression sub-type labels in professional use was identified. This exercise revealed many official and ‘unofficial’ terms in professional use. Citation rate plots by year were then generated for these depression sub-type labels. The rise and fall of different labels are examined in relation to social determinants and context, including publication of diagnostic manuals DSM and ICD, power shifts in psychiatry, the discovery of psychiatric drugs and the shift from inpatient to community care. Exploring the changing use of official and unofficial labels over time in this way provides a novel historical perspective on the concept of depression in the late twentieth- century. r 2005 Elsevier Ltd. All rights reserved. Keywords: Depression; History of medicine; Diagnostic labels; DSM; Community care Introduction Diagnosis in medicine involves a process of classifying and attaching a label to an illness. Over the last two centuries medical classification has increasingly been based on the underlying pathological lesion or process as, given this physical or organic referent, it becomes easier to gain professional consensus about specific illnesses. What is pneumonia or appendicitis or cancer can be agreed internationally with reference to the presence or absence of certain clearly defined physical characteristics. In psychiatry, however, there is no such external biological referent to act as an anchor for diagnosis. Essentially, psychiatry classifies on the basis of patients’ patterns of symptoms which might vary according to how they are elicited and interpreted. The development of standardised psychiatric instru- ments and interviews over the last few decades has helped achieve some stability for researchers investigat- ing mental illness but clinicians, historically, have had ARTICLE IN PRESS www.elsevier.com/locate/socscimed 0277-9536/$ - see front matter r 2005 Elsevier Ltd. All rights reserved. doi:10.1016/j.socscimed.2005.05.021 Corresponding author. Tel.: +44 20 77945875; fax: +44 20 7435 8018. E-mail address: [email protected] (S. McPherson).
-
Upload
susan-mcpherson -
Category
Documents
-
view
217 -
download
2
Transcript of Social determinants of diagnostic labels in depression

ARTICLE IN PRESS
0277-9536/$ - se
doi:10.1016/j.so
�Correspondfax: +4420 743
E-mail addr
Social Science & Medicine 62 (2006) 50–58
www.elsevier.com/locate/socscimed
Social determinants of diagnostic labels in depression
Susan McPherson�, David Armstrong
Tavistock & Portman NHS Trust, Belsize Centre, 94 Belsize Lane, London NW3 5NE, UK
Available online 11 July 2005
Abstract
The role of diagnostic labels in medicine is usually that of labelling an illness as a means of communication.
Control over labelling processes in medicine is ordinarily imposed via medical schools, textbooks, education or by
diagnostic manuals. Diagnostic labels often change following new discoveries in underlying pathology such as
‘consumption’ being relabelled as ‘TB’ or ‘cancer’. Sub-types of broad diagnostic labels also often emerge from such
discoveries e.g. ‘lung cancer’ or ‘throat cancer’. In mental health, underlying pathology is the subject of ongoing debate
spanning ideas including the brain as a faulty organ, faulty genetics and environmental problems. With controversy
over pathology comes controversy over labels and the idea that labels may be used not just for communication, but as
devices of social and professional control, arising out of a social process. This study explores the codification of the
diagnostic label ‘depression’ which emerged in the twentieth-century and has proliferated with numerous sub-types over
the last 40 years. The aim is to examine its social determinants and context. Medline is used as a data source for
professional label usage. A range of depression sub-type labels in professional use was identified. This exercise revealed
many official and ‘unofficial’ terms in professional use. Citation rate plots by year were then generated for these
depression sub-type labels. The rise and fall of different labels are examined in relation to social determinants and
context, including publication of diagnostic manuals DSM and ICD, power shifts in psychiatry, the discovery of
psychiatric drugs and the shift from inpatient to community care. Exploring the changing use of official and unofficial
labels over time in this way provides a novel historical perspective on the concept of depression in the late twentieth-
century.
r 2005 Elsevier Ltd. All rights reserved.
Keywords: Depression; History of medicine; Diagnostic labels; DSM; Community care
Introduction
Diagnosis in medicine involves a process of classifying
and attaching a label to an illness. Over the last two
centuries medical classification has increasingly been
based on the underlying pathological lesion or process
as, given this physical or organic referent, it becomes
easier to gain professional consensus about specific
e front matter r 2005 Elsevier Ltd. All rights reserve
cscimed.2005.05.021
ing author. Tel.: +4420 77945875;
5 8018.
ess: [email protected] (S. McPherson).
illnesses. What is pneumonia or appendicitis or cancer
can be agreed internationally with reference to the
presence or absence of certain clearly defined physical
characteristics. In psychiatry, however, there is no such
external biological referent to act as an anchor for
diagnosis. Essentially, psychiatry classifies on the basis
of patients’ patterns of symptoms which might vary
according to how they are elicited and interpreted.
The development of standardised psychiatric instru-
ments and interviews over the last few decades has
helped achieve some stability for researchers investigat-
ing mental illness but clinicians, historically, have had
d.

ARTICLE IN PRESSS. McPherson, D. Armstrong / Social Science & Medicine 62 (2006) 50–58 51
little constraint on their use of diagnostic labels. Indeed,
cross-national studies have shown the considerable
differences in diagnostic patterns in different countries
(Lee, 2002). There is also some evidence of differences
between individual psychiatrists within the same country
(Fabrega, Ahn, Boster, & Mezzich, 1990). Managing
this diagnostic heterogeneity has therefore been a major
task for maintaining the identity and credibility of
psychiatry: one of the main strategic approaches has
been to codify classification decisions in the form of
diagnostic manuals.
Diagnostic manuals came to the fore in medicine
during the twentieth-century when international com-
parisons of death rates became important. The Interna-
tional Classification of Disease (ICD) allowed some
standardisation of causes of death such that rates could
reliably be compared across countries and across time.
The success of the early ICD meant that subsequent
revisions gradually incorporated illnesses that did not
necessarily cause death, including mental illness. By the
sixth revision of 1948, guidance on diagnosing psychia-
tric illness was fully incorporated. In 1952 the American
Psychiatric Association (APA) produced their own
version of this guidance as the diagnostic and statistical
manual of mental disorders (DSM). Since then the two
systems have remained in parallel, each publishing
revisions every few years.
One of the aims of DSM and ICD was to provide a
language for communication (or control) both within
psychiatry as well as for other professionals dealing with
mental illness such as psychologists, primary care
workers, social workers and occupational therapists
(see Frances, First, Pincus, Widiger, & Davis, 1990).
However, labels given by these diagnostic manuals do
not in themselves dictate the range of terms employed by
such professionals and they have no legal status other
than for reporting national morbidity statistics to the
World Health Organisation (WHO) and for reimburse-
ment for health insurance in the USA and some other
countries with health insurance systems. ‘Unofficial’
labels are used by professionals both outside and within
psychiatry for purposes of intra- or inter-professional
communication. This was demonstrated in a study by
Pincus, Davis, and McQueen (1999) which aimed to find
out what terms and definitions were being used in
professional literature for ‘subthreshold depression’. A
literature review was carried out using the term
‘subthreshold depression’ as well as a variety of other
similar terms known to be relatively synonymous. The
study identified a wide variety of terms and definitions
employed in the published professional literature refer-
ring to depression that was ‘not clinically significant’.
These terms included some used in DSM and ICD as
well as other terms not found in either system. If a
variety of different labels exist for one such area of
depression, it is more than likely that a wide range of
sub-type labels exist for the broader totality of
depression.
The diagnosis of illnesses such as depression must
constitute a constant struggle between the standardising
forces—as represented by the manual authors—and the
idiosyncrasies of the labelling systems used by individual
clinicians. This tension between standardisation and
heterogeneity is the subject of this study that examines
the social determinants and context of how depression
became codified over the last 40 years. Given the lack of
reference to underlying pathology, these codes are likely
to be the product of a social process that includes the
publication and revisions of diagnostic manuals them-
selves, mental health policy such as the shift from
inpatient to community care, the discovery of successive
generations of psychiatric drugs and the power struggles
in psychiatry between biological psychiatry (i.e., those
who stressed the biological or organic causes of mental
illness) and psychoanalytic-oriented psychiatrists. These
will be the main social contexts explored in relation to
the codification of depression.
Methods
Medline, which electronically indexes articles from
1966 onwards, was used as the main source of data on
the use of psychiatric diagnostic terms for depression.
The database was first searched using the search term
‘depression.mp’ which identified articles where ‘depres-
sion’ featured in the title, keywords or abstract. The data
set was downloaded and cleaned in reference manager
(including the removal of duplicates) and imported into
SPSS. SPSS was then used to generate a random sample
of 50 articles for every fifth year in the data set. This
resulted in 350 articles, the titles and abstracts of which
were then scanned to identify any depression sub-type
labels used.
In order to explore further the range of sub-type labels
identified, the labels were divided into clusters which
represented the underlying type of illness classification.
Clusters were identified by an inductive process of
grouping sub-type labels in terms of an implicit under-
standing of their meaning (given that definitions were
not considered systematically in this process as these
may vary and change over time and are outside the
scope of this study). These clusters were agreed by both
authors. Bipolar disorder and manic depression were
excluded from this study in order to focus on the
concepts and labels for low mood rather than mania.
Each sub-type label identified from the search of a
sample of articles was then used to perform a Medline
search across the whole database to identify articles
where the term features in the title, keywords or
abstract. Each data set was then downloaded into
reference manager.

ARTICLE IN PRESSS. McPherson, D. Armstrong / Social Science & Medicine 62 (2006) 50–5852
Once each data set was cleaned, it was exported to
SPSS to allow easier manipulation of data. SPSS was
used to count the number of citations for each search
term by year. This figure was converted into a citation
rate by dividing the number of citations for the search
term by the number of citations for depression in that
year. This was multiplied by 10,000 to get whole
numbers. The citation rate for each term was graphed
over time with the number of ‘depression’ citations
plotted on a second axis.
Results and discussion
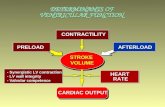
Changing patterns of diagnostic labelling reflect a
number of contextual events. The main events explored
in this paper are the publication dates of diagnostic
manuals, namely DSM II in 1968, DSM III in 1980 and
DSM IV in 1994. But the successive editions of DSM
were themselves related to shifts in psychiatry itself. In
particular, there was a major power shift in the APA
that occurred around the time of preparation and
publication of DSM III during which the psychoanalytic
psychiatrists lost political ground to biological psychia-
trists, e.g. Grob (1991), Bayer and Spitzer (1985) and
Havens (1985). Also, developments in the use of
psychiatric drugs, illustrated by key shifts from mono-
amine oxidase inhibitors (MOAIs) falling out of grace
following reports of their severe hepatotoxic and
hypertensive effects through the domination of the
tricyclics, to the introduction of the very successful
selective serotonin reuptake inhibitors (SSRIs) (Ban,
2001), are likely to have had an effect on depression
diagnosis. This period also witnessed a significant shift
from inpatient to community care as well as a number of
key governmental and legal landmarks (Geller, 2000),
which are summarised in Fig. 1.
Depression sub-type labels identified and used in this
study are listed in Table 1. Labels were also clustered
into categories which refer to an implicit understanding
of their meaning.
Table 2 shows information for each sub-type label.
The first column gives the year that the label first
Fig. 1. Social context timeline. 1Mental Retardation Facilities and Co
88–164) passes; it contains funds for constructing community mental
appeals rules that an individual could not be committed to the hospita
facility available to care for her. 3A U.S. district court judge in the Dist
since the District’s Hospitalization of the Mentally Ill Act becam
controversial throughout the rest of the century. 4Congress overrides P
Sharing on Health Services Act. The bill includes expanded funding for
must provide. 5The National Institute of Mental Health awards con
Support Program. 6Surgeon General Julius B. Richmond, M.D., rele
Chronically Mentally Ill. 7The State Comprehensive Mental Health Se
and implement comprehensive mental health plans for community-ba
appeared in Medline (i.e. the citation rate was greater
than zero for the first time). The peak rate column gives
the highest citation rate for each label and the year in
which this citation rate occurred. Finally, the table
shows the citation rate in 2000. As can be seen from
Table 2, peak citation rates range from 9.05 (‘exogenous
depression’) to 1097.5 (‘major depression’). However, in
spite of this very large range, the majority of labels
cluster at the bottom of this range. The three most
dominant labels are ‘major depression’, ‘endogenous
depression’ and ‘dysthymia’. Fig. 2 plots citation rates
for each of the three dominant sub-type labels on the
left-hand (primary) axis. The right-hand (secondary)
axis shows the total number of ‘depression’ citations.
This line can be seen to be rising steadily over the period
under consideration. The most prominent feature of
Fig. 2 is that ‘major depression’ can be seen to increase
very steeply from zero around 1980 and to dominate the
plot thereafter.
The term major depression was first introduced in
1980 with DSM III. Since this term was not found in any
indexed articles before DSM III yet became very
common afterwards, it is reasonable to conclude that
this significant increase in the use of the term was at least
in part a product of the publication of DSM III. The
parallel ICD system did not use the term major
depression, suggesting a particular influence for DSM.
The APA had a much greater budget for producing,
disseminating and training for the DSM than the WHO
had for the ICD. This may have therefore made the
DSM more accessible, certainly to American audiences
if not further afield with global sales of video training
materials. Furthermore, while the ICD eventually made
headway in producing operationalised versions of its
manuals, the DSM made faster progress by incorporat-
ing these various versions into training for relevant
professionals. Perhaps at an even more practical level,
published medical literature tends to be dominated in
terms of volume and impact by US journals. North
American journals, while open to authors from around
the world, may also have an inherent publication bias in
favour of US authors using DSM language, in that the
language is familiar and the writing style will conform
mmunity Mental Health Centers Construction Act of 1963 (P.L.
health centers (CMHCs). 2In Lake vs. Cameron a U.S. court of
l until hospital officials determined there was no less restrictive
rict of Columbia orders an outpatient commitment, the first ever
e effective in 1964. Outpatient commitment would remain
resident Ford’s veto of the Nurse Training and Health Revenue
CMHCs and increases the number of essential services CMHCs
tracts to 16 states under a new project called the Community
ases a 457-page report entitled Toward a National Plan for the
rvices Plan Act of 1986 (P.L. 99–660) requires states to develop
sed services for people with severe mental illness.

ARTICLE IN PRESS
Manuals Power struggles
Drugs Community Care (USA) Psychiatric
inpatients(USA)
1963 MOAI CMHCs established1
1966scandals Lake vs Cameron2
452,000
1967
1968 DSM II 399,000
1969
1970 338,000
1971
1972 Outpatient commitment order3 275,000
1973
1974 216,000
1975
APA
pre
dom
inan
tly
psyc
hoan
alyt
ic
CMHC expanded funding4
1976 171,000
1977 NIMH Community Support Program5
1978 154,000
1979 ICD 9
1980
DSM III APA powerstruggles
Toward a National Plan for the Chronically Mentally Ill 6
1981
Lith
ium
fir
st u
sed
to tr
eat
man
ic d
epre
ssio
n
1982
1983 Tri
cycl
ics
dom
inat
e m
arke
t
1984
1985
1986
State Comprehensive Mental Health
Services Plan Act 7 111,000
1987 DSM IIIR
1988
1989
1990 91,000
1991
1992 ICD 10 83,000
1993
APA
P pr
edom
inan
tlybi
olog
ical
1994 DSM IV 72,000
1995
1996 62,000
1997
1998
SSR
Is in
trod
uced
1999
2000 DSM IVTR
↑ ↑
Psychiatric Psychiatry
138,000
↓ ↓
↓ ↓
↓ ↓
S. McPherson, D. Armstrong / Social Science & Medicine 62 (2006) 50–58 53

ARTICLE IN PRESS
Table 1
Sub-type labels and clusters
Cluster Label
Causal Endogenous depression
(relating to the aetiology
of depression)
Exogenous depression
Reactive depression
Temporal Postnatal depression
(relating to the timing
or duration of illness)
Recurrent depression
Chronic depression
Acute depression
Dysthymia
Severity of symptoms Major depression
(relating to the severity
of depression)
Minor depression
Mild depression
Severe depression
Nature of symptoms Atypical depression
(relating to the nature
of symptoms)
Melancholic depression
Psychotic depression
Neurotic depression
Melancholia
Treatment response Treatment resistant depression
(relating to the patient’s
response to treatment)
Refractory depression
S. McPherson, D. Armstrong / Social Science & Medicine 62 (2006) 50–5854
more often to the US method of scientific reporting.
Once the DSM discourse had established a hegemony
within the USA, it would have been able to spread as an
international discourse, with an ever-increasing trend to
use language that can be globally understood.
The dramatic success of ‘major depression’ is not
matched by any other sub-type label introduced by other
versions of DSM or ICD. Given that the DSM is written
by and controlled by the APA, the success of ‘major
depression’ as a label can also be seen as a success for the
profession of psychiatry in controlling language use
around this diagnosis. The APA was given authority by
the US government to devise a classification system for
mental disorders that would be used for official national
statistics and financial processes in the health system.
The explicit authority over mental health labelling given
to psychiatrists by this process is one aspect of the social
context in which the development of the manual took
place.
The coining of the term ‘major depression’ may also
be considered in the context of the earlier asylum
closures and the ongoing development of community
care, as illustrated in Fig. 1. These developments posed
both an opportunity and a threat for the profession of
psychiatry. In one sense, community care posed a threat
to psychiatry in that the responsibility of care for the
mentally ill could become dispersed among other
professions such as primary care physicians, nurses
and new mental health professions such as community-
based psychiatric nurses. In another sense, community
care provided an opportunity for the mental health field
as a whole to expand and to create more work for
psychiatrists as mental illness was construed as a
continuum, from the severely psychotic to the general
worries and stresses of everyday life. With this dual
threat and opportunity posed by community care,
psychiatry may have needed to set boundaries around
areas of mental health that psychiatry would own or
control and to keep them apart from other professions
involved in mental health. In terms of depression, this
may have meant creating categories of psychiatric and
non-psychiatric depression—hence ‘major depression’
which might be considered severe enough to require
psychiatric input and, by implication, ‘minor depression’
to be dealt with by other professionals. Supporting this
interpretation, ‘minor depression’ is present in DSM III,
but is ill-defined, appearing within the ‘Not Otherwise
Specified’ category; it was considered by DSM authors
to be within the remit of primary care rather than
psychiatry (Pincus et al., 1999).
The terms major and minor depression fall into the
‘severity of symptoms’ cluster set out in Table 1. These
clusters, which were derived from labels identified in
Medline from 1966 to 2000, might usefully be compared
to previous clusters or dimensions of mental illness in
order to establish whether ‘severity’ is indeed a new
concept in mental illness. The eight criteria that were
used to classify mental disorder by the nineteenth-
century French alienists provide a useful comparison.
According to Berrios (1999), these were the cause of the
disorder (aetiological), the substratum of the disorder
(e.g. anatomy), the clinical outcome (whether curable or
incurable), actuarial (according to what was observed in
the statistics of the main asylums in France), phenom-
enological (according to whether or not the disorder
included delusions), ‘natural’ (i.e. whether it corre-
sponded to ‘real types’ as given in nature), psychological
(i.e. what mental faculty was assumed to be impaired)
and disease course. There are some clear similarities with
the diagnostic clusters identified in this paper. The
aetiological criterion is identical to the causal cluster; the
clinical outcome criterion similar to the treatment
response cluster; the phenomenological criterion similar
to the nature of symptoms cluster and the disease course
criterion similar to the temporal cluster. The only cluster
identified in the present study that does not have a
counterpart in these eight criteria is the ‘Severity of
symptoms’ category, which could therefore be seen as
something new to twentieth-century psychiatric think-
ing. This may suggest that the domain of psychiatry has

ARTICLE IN PRESS
Table 2
Sub-type labels: appearance in Medline, peak citation rate and year 2000 citation rate
Label Appearance year Peak year Citation rate 2000
Year Citation rate
Endogenous depression 1966 1982 300.26 15.79
Reactive depression 1966 1981 58.85 3.51
Chronic depression 1966 1996 50.78 49.12
Dysthymia 1966 1994 198.25 135.09
Mild depression 1966 1987 57.23 35.09
Psychotic depression 1966 1999 66.06 36.84
Neurotic depression 1966 1979 84.78 8.77
Melancholia 1966 1967 149.05 31.58
Postnatal depression 1968 1997 70.41 63.16
Recurrent depression 1968 1994 51.92 29.82
Severe depression 1968 1999 160.44 119.3
Atypical depression 1968 1984 45.2 14.04
Acute depression 1970 1999 28.31 12.28
Treatment resistant depression 1974 1996 44.16 28.07
Minor depression 1975 1997 55.91 35.09
Exogenous depression 1978 1981 9.05 0
Refractory depression 1978 1996 35.33 21.05
Major depression 1979 1997 1097.54 985.96
Melancholic depression 1981 1997 37.27 14.04
0
200
400
600
800
1000
1966
1967
1968
1969
1970
1971
1972
1973
1974
1975
1976
1977
1978
1979
1980
1981
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
Cit
atio
n R
ate
0
1000
2000
3000
4000
5000
6000
All
Dep
ress
ion
Cit
atio
ns
Dysthymia Endogenous Depression Major Depression All Depression Citations (2nd Axis)
All
othe
r la
bels
belo
w t
his
line
Fig. 2. Citation rate of dominant depression sub-type labels 1966–2000.
S. McPherson, D. Armstrong / Social Science & Medicine 62 (2006) 50–58 55
broadened since the nineteenth-century, when psychia-
trists’ work was largely restricted to asylums where
psychoses were usually present. Twentieth-century
psychiatry may be seen to require the new dimension
of ‘severity’ in order to reflect its expansion out of
asylums and into the community.

ARTICLE IN PRESSS. McPherson, D. Armstrong / Social Science & Medicine 62 (2006) 50–5856
The ability of the APA to control diagnostic practice
through its DSM manuals, however, was not charac-
terised by total success. On the one hand, it failed to
suppress some terms and, on the other, was not always
successful in its prescription of what terms were
acceptable. ‘Endogenous depression’, for example, was
removed from the classification system by the authors of
DSM III, yet remained in use for years later and is the
second most dominant label up until the mid-1990s (see
Fig. 2). Furthermore, ‘dysthymia’, a term which DSM
III redefined from reflecting a problem of personality to
a depressive disorder (Ramana & Paykel, 1992), did not
have anything like the success of ‘major depression’ and
did not get adopted until the late 1980s.
The term ‘endogenous depression’ refers to a depres-
sion with biological origin. Although a fashionable term
before 1980 (see Fig. 2), DSM III abandoned all causal
terminology regarding depression, claiming to be
aetiologically neutral. DSM III was essentially written
by biological psychiatrists, for whom a classification
term reflecting a biological basis might seem a natural
choice, but the very existence of the term conjured into
opposition the idea that there could also be an
alternative type of depression that did not have a
biological origin (‘exogenous’ or ‘reactive’ in the
previous classifications). It is possible that biological
psychiatry would benefit from a labelling system which
excluded the possibility of any non-biological causes.
This effect can be noted in the objections to the removal
of this dimension and to the claims by DSM III authors
of aetiological neutrality, e.g. Sadler, Hulgus, and Agich
(1994) and van Praag (1990).
The control that biological psychiatrists exerted over
DSM III was a major element of the power struggle
within the APA (indicated in Fig. 1) around the time of
its publication. Previous versions of DSM had been
written by psychoanalytically orientated psychiatrists
and contained psychoanalytic terminology. DSM III
abandoned the term ‘neurotic’ under a great deal of
controversy and much resistance from the psycho-
analytic psychiatrists (Bayer & Spitzer, 1985). ‘Neurosis’
was perceived as referring to a psychological aetiology
and DSM III authors claimed to be intent on removing
aetiological labels from the classification system. Fol-
lowing heated debates and much media attention, a
compromise was reached between Spitzer (who led work
on DSM III) and the APA, whereby the term ‘neurosis’
and other psychoanalytically related terms would appear
in brackets next to their new equivalents (Bayer &
Spitzer (1985)).
The removal of endogenous depression from the
classification system, however, did not receive anything
near as much attention, perhaps because it was a term
allied to biological psychiatry—which had no wish to
defend it. Hence, while attention was focused on the
‘neurosis’ debate, the removal of endogenous depression
may prove to have been a more subtle assertion of
biological psychiatry’s power, removing the implication
that there could be any depression that did not have a
biological origin.
Why was it important for biological psychiatrists to
champion the complete medicalisation of depression?
Physicians outside of psychiatry might have been more
inclined towards this goal than psychiatry; moreover,
the psychopharmacological advances being made at the
time were sufficient to mark out a biological aspect of
mental illness without needing to rule out the possibility
of both biological and environmental causes. In fact, the
medicalisation of depression may have been a by-
product of the power struggle with psychoanalytic
psychiatry. It may also have been important to
psychiatrists in the context of a general need for the
greater professionalisation of psychiatry. Professional
status for any occupational group was enhanced
through control of an esoteric knowledge base, in
particular that of science. The discoveries of psychoac-
tive substances around this time as well as an improved
understanding of brain morphology and metabolism
created an opportunity for psychiatry to proclaim its
biomedical scientific credentials and ally itself to the rest
of medicine. This strategy had been partly compromised
by the deaths from hepatotoxicity arising from the
widespread use of the monoamine oxidase inhibitors
(MAOIs), so by the time of DSM III when the new
(and safer) tricyclics had been relatively established
(see Fig. 1), biological psychiatry may have needed to
recover ground from the MAOI scandals and over-
emphasise the view that depression could be treated with
drugs on a par with any other medical illness.
In spite of the success of biological psychiatry, the
increasing medicalisation of depression and publication
of DSM III, it is nevertheless notable that ‘endogenous
depression’ did not disappear from professional dis-
course. ‘Endogenous depression’ remained the second
most dominant term overall, even after 1980, despite a
gradual decline over subsequent years. It continued to
be used to some degree up to 2000 (see Fig. 2). This may
be testament to its great popularity before the publica-
tion of DSM III and the reluctance to abandon a term,
which perhaps dominated the professional trainings and
careers of the majority of those professionals who were
at the height of their careers in the 1980s and 1990s. It
may alternatively represent some resistance among the
rank and file of the profession to the removal of an
aetiological dimension and signal the existence of
members within the profession who resisted polarisation
into a medical or psychoanalytic camp and retained the
possibility of different causes of depression.
Before DSM III, the term ‘dysthymia’ referred to a
personality disorder (Ramana & Paykel, 1992). In 1980,
dysthymia was given an official place in DSM III’s
categorical axis I, being defined as a chronic mild form

ARTICLE IN PRESSS. McPherson, D. Armstrong / Social Science & Medicine 62 (2006) 50–58 57
of depression. However, the previous concept of
dysthymia as a personality disorder would likely cause
it to be more closely linked with chronicity rather than
mildness. Why did the authors of DSM III feel it
important to alter the definition of dysthymia? It may be
that as with ‘endogenous depression’, the concept of
personality disorder implied some alternative origin for
depression other than a biological origin. It may also
have implied that the illness was not treatable with drugs
if it was ingrained in a person’s personality. However,
the citation rate of ‘dysthymia’ indicates that the term
was not successful in the way that ‘major depression’
was; its usage did not rise significantly until the late
1980s and early 1990s (see Fig. 1). However, from 1994
to 2000, dysthymia is the most dominant label
after ‘major depression’. This perhaps reflects the
greater definition given to it in DSM IV and also a time
lag in the mental health professional community
adjusting to its reframing as a mood disorder rather
than a personality disorder. It may also reflect the
problematic issues surrounding the concept of chronicity
in DSM III.
DSM III was seen as a breakthrough for psychiatric
classification in terms of its multiaxial system covering
the biopsychosocial model of mental illness and might
therefore be expected to capture the dimensions of
depression reflected in the clusters identified in the
present study. The five axes of DSM do cover some of
the clusters, but DSM noticeably lacks a ‘temporal’ axis
and a ‘treatment response’ axis. Notable also are the
labels identified in this study that do not appear in either
DSM or ICD—‘chronic depression’, ‘treatment resistant
depression’ and ‘refractory depression’, which all have
implications for the duration or course of illness.
‘Recurrent depression’ does not appear in DSM, but
does appear in ICD 10. Keller (Keller et al., 1995),
leading the DSM IV mood disorder group, described the
concern of some that DSM III had no provision for
chronic major depression in the distinction between
depression and dysthymia. Keller went on to defend the
DSM IV system which omitted ‘chronic major depres-
sion’, but did provide a classification frame for the
course of depression. This embraced the six potential
courses of depression which supposedly fitted the
majority of patients in the DSM IV mood disorder field
trials (Keller et al., 1995) and was reflected in DSM IV
largely within the categorical distinction between ‘dys-
thymia’ and ‘major depression’. Moreover, Williams,
who would later lead the DSM IV working group on the
multiaxial system, mentioned in 1985 the possibility of
considering a treatment-response axis (Williams, 1985)
to resolve the confusion of course of illness with severity,
problematic in DSM III. However, in a later report of
the DSM IV work group in 1990, this potential new axis
was firmly ruled out (Williams, Goldman, Gruenberg,
Mezzich, & Skodol, 1990).
The decisions by DSM III and IV authors to resist
either a temporal- or treatment-response axis, in spite of
problems associated with not having them, may be
considered within the social context of psychiatry. In
particular, a chronic dimension to depression may have
been considered a threat to the psychiatry profession in
the context of the rise of community care in that a
chronic illness lends more to the idea of long-term
management in the community rather than acute
treatment by psychiatrists. Chronicity also implies the
lack of a cure and this may also threaten psychiatry’s
shift to a medical model in which a disease can be cured
through advancement of science. However, as with the
ongoing use of ‘endogenous depression’, the slow
development of popularity of the term ‘dysthymia’ and
ongoing use of terms such as ‘chronic depression’ not
sanctioned in DSM III may indicate that the DSM
system failed to provide a meaningful representation of
course of illness acceptable to all mental health
professionals and that within the field are those who
employ concepts of the chronicity and the cyclical nature
of depression, in spite of the avoidance of these issues in
DSM III and IV.
Conclusion
Although the Oxford English Dictionary (2nd Edi-
tion, 1989) cites the first professional use of ‘depression’
in 1905 in ‘Psychological Review’, Snaith (1987)
describes a slightly earlier usage by Bevan Lewis in
1899: ‘‘In simple pathological depressiony the patient
exhibits a growing indifference to his former pur-
suitsy’’. Whatever its exact origins, however, it is clear
that the term ‘depression’ used as a medical label to
describe mood and mental health, especially in the
context of the ‘neuroses’, is a Western twentieth-century
phenomenon (Armstrong, 1980). In other words, the use
of the diagnostic label of depression is historically and
culturally located in very recent times. Furthermore, the
proliferation of sub-types of depression also reflects
contemporary social events and processes.
To a great extent, the integrity of psychiatry as a
medical specialty depends on the consistency of diag-
nostic labelling. Without consistency there would be
difficult communication within the professional com-
munity, as meetings, correspondence, textbooks and
journals would use conflicting language. Psychiatry
therefore needs a certain level of diagnostic stability
for its very survival. Yet, as pointed out earlier, it is
more difficult to achieve this degree of stability in an
area devoid of biological correlates with which to
anchor diagnostic definitions. The solution that has
therefore emerged in the second half of the twentieth-
century has been the Diagnostic Manual that would seek

ARTICLE IN PRESSS. McPherson, D. Armstrong / Social Science & Medicine 62 (2006) 50–5858
to impose consistency, stability and control on the
centripetal forces of clinical diagnosis.
In large part the Diagnostic Manuals have been
successful, albeit their influence has not always been
immediate. The most significant new diagnostic sub-type
introduced (by DSM III) has been ‘major depression’,
which rapidly dominated psychiatric thinking, for
reasons described. Other labels, such as dysthymia, have
taken longer to become established. But there have also
been notable ‘failures’, as in the continuing use of
‘endogenous depression’ despite its removal from the
formal classification. Ironically, as argued, some of these
survivals may be related to internal conflicts within
psychiatry on the best way to maintain a unified
hegemony.
Clearly, struggles internal to psychiatry are important
in developing and maintaining diagnostic classifications.
At its most crude, this is illustrated by the group that
manages to achieve authorship of any Diagnostic
Manual; the triumph of biological over psychoanalytic
psychiatry (at least in the US) therefore had a major
impact on the diagnoses that patients were to subse-
quently receive. But psychiatry has also existed in a
rapidly changing healthcare and technological milieu
and in many ways, diagnosis has had to respond as
psychiatry adapted to a new environment, whether it
was the era of community care or pharmacological
developments that potentially transformed the thera-
peutic potential of its practitioners.
In summary, this study has argued that the publica-
tion of Diagnostic Manuals in psychiatry may have been
driven by and reflected the need for psychiatry to
establish and maintain a specific area of expertise in the
mental illness marketplace in order to survive as a
profession. In part this involved strengthening its
alliance with the rest of medicine through the medica-
lisation of mental illnesses such as depression and in part
developing medical models of mental illness in order to
create a dominant power base for itself as a profession:
for both of these goals, control over the diagnostic
labelling process was vital. This study provides an
example of how trends in labelling and language in
depression and mental health should not be taken at face
value, but considered as an indicator of important social
processes going on within the mental health professions.
References
Armstrong, D. (1980). Madness and coping. Sociology of
Health and Illness, 2, 293–315.
Ban, T. A. (2001). Pharmacotherapy of depression: A historical
analysis. Journal of Neural Transmission, 108, 707–716.
Bayer, R., & Spitzer, R. L. (1985). Neurosis, psychodynamics,
and DSM-III. A history of the controversy. Archives of
General Psychiatry, 42, 187–196.
Berrios, G. E. (1999). Classifications in psychiatry: A con-
ceptual history. Australian and New Zealand Journal of
Psychiatry, 33, 145–160.
Fabrega, H., Jr., Ahn, C. W., Boster, J., & Mezzich, J. E.
(1990). DSM III as a systemic culture pattern: Studying
intracultural variation among psychiatrists. Journal of
Psychiatric Research, 24, 139–154.
Frances, A., First, M., Pincus, H. A., Widiger, T., & Davis, W.
(1990). An introduction to DSM-IV. Hospital and Commu-
nity Psychiatry, 41, 493–494.
Geller, J. L. (2000). The last half-century of psychiatric services
as reflected in psychiatric services. Psychiatric Services, 51,
41–67.
Grob, G. N. (1991). Origins of DSM-I: A study in appearance
and reality. American Journal of Psychiatry, 148, 421–431.
Havens, L. (1985). Historical perspectives on diagnosis in
psychiatry. Comprehensive Psychiatry, 26, 326–336.
Keller, M. B., Klein, D. N., Hirschfeld, R. M., Kocsis, J. H.,
McCullough, J. P., Miller, I., et al. (1995). Results of the
DSM-IV mood disorders field trial. American Journal of
Psychiatry, 152, 843–849.
Lee, S. (2002). Socio-cultural and global health perspectives for
the development of future psychiatric diagnostic systems.
Psychopathology, 35, 152–157.
Pincus, H. A., Davis, W. W., & McQueen, L. E. (1999).
‘Subthreshold’ mental disorders. A review and synthesis of
studies on minor depression and other ‘brand names’.
British Journal of Psychiatry, 174, 288–296.
Ramana, R., & Paykel, E. S. (1992). Classification of affective
disorders. British Journal of Hospital Medicine, 47, 831–835.
Sadler, J. Z., Hulgus, Y. F., & Agich, G. J. (1994). On values in
recent American psychiatric classification. Journal of
Medicine and Philosophy, 19, 261–277.
Snaith, R. P. (1987). The concepts of mild depression. British
Journal of Psychiatry, 150, 387–393.
van Praag, H. M. (1990). The DSM-IV (depression) classifica-
tion: to be or not to be? Journal of Nervous and Mental
Disease, 178, 147–149.
Williams, J. B. (1985). The multiaxial system of DSM-III:
Where did it come from and where should it go? I. Its
origins and critiques. Archives of General Psychiatry, 42,
175–180.
Williams, J. B., Goldman, H. H., Gruenberg, A., Mezzich, J. E.,
& Skodol, A. E. (1990). DSM-IV in progress. The multiaxial
system.[comment]. Hospital and Community Psychiatry, 41,
1181–1182.


![[CREATING LABELS] MAKING TEXT DESIGNING LABELS … · [CREATING LABELS] MAKING TEXT DESIGNING LABELS PRINTING LABELS COMPLETED LABELS USEFUL FUNCTIONS USER'S GUIDE / Español Printed](https://static.fdocuments.us/doc/165x107/5e718e59f26dfc19d238892e/creating-labels-making-text-designing-labels-creating-labels-making-text-designing.jpg)