
Smith-Farrington - 1E Monitoring Over-Sedation.ppt · Monitoring Over-Sedation in Adult ... •...
20
Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain ASPMN 21 st National Conference Tucson, AZ September 9, 2011 0845-0945 1 Monitoring Over‐Sedation in Adult and Pediatric Patients Receiving Opioids for Pain Michele Farrington, BSN, RN, CPHON michele‐[email protected] Staff Nurse Anne Smith, MSN, RN‐BC anne‐m‐[email protected] Advanced Practice Nurse Department of Nursing Services and Patient Care University of Iowa Hospitals and Clinics, Iowa City, Iowa Acknowledgement Special acknowledgement and thanks to the Pain Resource Nurses and Pain Staff Nurse Champions on the Nursing Pain Management Subcommittee for their support and assistance with this project! Speaker Disclosure Statement •The speakers have no industry relationships to disclose. •No off‐label use will be discussed.
Transcript of Smith-Farrington - 1E Monitoring Over-Sedation.ppt · Monitoring Over-Sedation in Adult ... •...

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
1
Monitoring Over‐Sedation in Adult and Pediatric Patients Receiving
Opioids for Pain
Michele Farrington, BSN, RN, CPHONmichele‐[email protected]
Staff Nurse
Anne Smith, MSN, RN‐BCanne‐m‐[email protected]
Advanced Practice Nurse
Department of Nursing Services and Patient CareUniversity of Iowa Hospitals and Clinics, Iowa City, Iowa
Acknowledgement
Special acknowledgement and thanks to the Pain Resource Nurses and Pain Staff Nurse
Champions on the Nursing Pain Management Subcommittee for their support and assistance
with this project!
Speaker Disclosure Statement
•The speakers have no industry relationships to disclose.
•No off‐label use will be discussed.

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
2
Objectives
• Outline steps for an evidence‐based practice project.
• Identify factors that place adult and pediatric patients receiving opioid analgesia at higher risk for over‐sedation and respiratory depression.
• Outline monitoring responsibilities of nursing staff to reduce the patient’s risk of over‐sedation and respiratory depression after opioid administration.
• Discuss development and implementation of a policy to address monitoring over‐sedation in patients receiving opioid analgesia.
• Describe evaluation strategies related to monitoring over‐sedation in patients receiving opioid analgesia and future improvement plans.
Evidence-Based Practice Framework
The Iowa Model ofEvidence-Based Practice to Promote Quality Care
Problem Focused Triggers1. Risk Management Data2. Process Improvement Data3. Internal/External Benchmarking Data4. Financial Data5. Identification of Clinical Problem
Knowledge Focused Triggers1. New Research or Other Literature2. National Agencies or Organizational
Standards & Guidelines3. Philosophies of Care4. Questions from Institutional
Standards Committee
ConsiderOther
Triggers
Is this Topica PriorityFor the
Organization?
Form a Team
Yes
No = a decision Point
DO NOT REPRODUCE WITHOUT PERMISSION
REQUESTS TO:Office of Nursing Research & EBP
The University of Iowa Hospitals and ClinicsIowa City, IA 52242-1009
Revised: April 1998 © UIHC(Titler, Kleiber, Steelman, et al., 2001)

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
3
Project TriggersFall 2008
• Problem‐Focused
– Over‐sedation events in patients of all ages within our institution and across the country
• Knowledge‐Focused
– New published recommendations and literature
Purpose
• Standardize monitoring for over‐sedation in adult and pediatric patients receiving opioid analgesia in order to provide safe care for patients with pain
The Iowa Model ofEvidence-Based Practice to Promote Quality Care
Problem Focused Triggers1. Risk Management Data2. Process Improvement Data3. Internal/External Benchmarking Data4. Financial Data5. Identification of Clinical Problem
Knowledge Focused Triggers1. New Research or Other Literature2. National Agencies or Organizational
Standards & Guidelines3. Philosophies of Care4. Questions from Institutional
Standards Committee
ConsiderOther
Triggers
Is this Topica Priority
For theOrganization?
Form a Team
Yes
No = a decision Point
DO NOT REPRODUCE WITHOUT PERMISSION
REQUESTS TO:Office of Nursing Research & EBP
The University of Iowa Hospitals and ClinicsIowa City, IA 52242-1009
Revised: April 1998 © UIHC(Titler, Kleiber, Steelman, et al., 2001)

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
4
Organizational Priority
• Existed before the project started due to adverse patient event
• Pressure to quickly make changes was challenging
The Iowa Model ofEvidence-Based Practice to Promote Quality Care
Problem Focused Triggers1. Risk Management Data2. Process Improvement Data3. Internal/External Benchmarking Data4. Financial Data5. Identification of Clinical Problem
Knowledge Focused Triggers1. New Research or Other Literature2. National Agencies or Organizational
Standards & Guidelines3. Philosophies of Care4. Questions from Institutional
Standards Committee
ConsiderOther
Triggers
Is this Topica PriorityFor the
Organization?
Form a Team
Yes
No = a decision Point
DO NOT REPRODUCE WITHOUT PERMISSION
REQUESTS TO:Office of Nursing Research & EBP
The University of Iowa Hospitals and ClinicsIowa City, IA 52242-1009
Revised: April 1998 © UIHC(Titler, Kleiber, Steelman, et al., 2001)
Team FormationJanuary – May 2009
• Primary team members– Pain Resource Nurses
• Represent all nursing divisions
• Informatics
• Secondary team members– Staff Nurse Champions
– Nursing Pain Management Subcommittee
– Interdisciplinary Pain Committee
– External Pain Experts

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
5
Is Therea SufficientResearch
Base?
Assemble Relevant Research & Related Literature
Critique & Synthesize Research for Use in Practice
Pilot the Change in Practice1. Select Outcomes to be Achieved2. Collect Baseline Data3. Design Evidence-Based
Practice (EBP) Guideline(s)4. Implement EBP on Pilot Units5. Evaluate Process & Outcomes6. Modify the Practice Guideline
Base Practice on OtherTypes of Evidence1. Case Reports2. Expert Opinion3. Scientific Principles4. Theory
Conduct Research
Yes No
= a decision Point
DO NOT REPRODUCE WITHOUT PERMISSION
REQUESTS TO:Office of Nursing Research & EBPThe University of Iowa Hospitals and ClinicsIowa City, IA 52242-1009
Revised: April 1998 © UIHC
(Titler, Kleiber, Steelman, et al., 2001)
Literature SearchJanuary – May 2009
• Articles and evidence obtained from benchmarking and gleaned from available pain journals and books
• Contacted pain expert
(C. Pasero)
Is Therea SufficientResearch
Base?
Assemble Relevant Research & Related Literature
Critique & Synthesize Research for Use in Practice
Pilot the Change in Practice1. Select Outcomes to be Achieved2. Collect Baseline Data3. Design Evidence-Based
Practice (EBP) Guideline(s)4. Implement EBP on Pilot Units5. Evaluate Process & Outcomes6. Modify the Practice Guideline
Base Practice on OtherTypes of Evidence1. Case Reports2. Expert Opinion3. Scientific Principles4. Theory
Conduct Research
Yes No
= a decision Point
DO NOT REPRODUCE WITHOUT PERMISSION
REQUESTS TO:Office of Nursing Research & EBPThe University of Iowa Hospitals and ClinicsIowa City, IA 52242-1009
Revised: April 1998 © UIHC
(Titler, Kleiber, Steelman, et al., 2001)

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
6
Synthesis of EvidenceJanuary – December 2009
• Why should you monitor your patient receiving opioids?– To ensure adequate oxygenation,
ventilation, and patient safety
– To evaluate response to treatment
• The first 24 hours is the most crucial time for monitoring:
– After surgery
– When existing doses of analgesics are altered
– When new analgesic modalities are introduced
(Pasero, 2009; Pasero & McCaffery, 2008)
Synthesis of Evidence (cont.)
• Patients at risk for over‐sedation– Obstructive sleep apnea, snoring, obesity, and/or BMI >35
– Age
– End‐stage organ failure
– Altered CNS function
– Concurrent use of sedating medications
(American Society of Anesthesiologists Task Force on Neuraxial Opioids, 2009; DuBose & Berde, 1997; Hagle, Tutag Lehr, Brubakken, & Shippee, 2004; ISMP, 2009; Nisbet & Mooney‐Cotter, 2009; Overdyk, 2008; Pasero, 2009; Stoelting & Weinger, 2009; Valdez‐Lowe, Ghareeb, & Artinian, 2009; Weber, Ghafoor, & Phelps, 2008; Weinger, 2007)
Synthesis of Evidence (cont.)
• Patients at risk for over‐sedation (cont.)– Supplemental oxygen use (oximetry may mask hypoventilation)
– Patient Controlled Analgesia (especially with a basal rate)
– Caregiver Controlled Analgesia
– Altered airways
(American Society of Anesthesiologists Task Force on Neuraxial Opioids, 2009; DuBose & Berde, 1997; Hagle, Tutag Lehr, Brubakken, & Shippee, 2004; ISMP, 2009; Nisbet & Mooney‐Cotter, 2009; Overdyk, 2008; Pasero, 2009; Stoelting & Weinger, 2009; Valdez‐Lowe, Ghareeb, & Artinian, 2009; Weber, Ghafoor, & Phelps, 2008; Weinger, 2007)

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
7
Synthesis of Evidence (cont.)
• Various sedation tools reviewed, such as:
– Richman Agitation‐Sedation Scale
– Riker
– Motor Activity Assessment Scale
– Ramsey Sedation Scale
– Post‐Anesthesia Care Unit considerations
– Pasero Opioid‐Induced Sedation Scale
• Chosen because it was developed for monitoring and early detection of unintended sedation with opioid administration
• Sedation usually precedes respiratory depression
Is Therea SufficientResearch
Base?
Assemble Relevant Research & Related Literature
Critique & Synthesize Research for Use in Practice
Pilot the Change in Practice1. Select Outcomes to be Achieved2. Collect Baseline Data3. Design Evidence-Based
Practice (EBP) Guideline(s)4. Implement EBP on Pilot Units5. Evaluate Process & Outcomes6. Modify the Practice Guideline
Base Practice on OtherTypes of Evidence1. Case Reports2. Expert Opinion3. Scientific Principles4. Theory
Conduct Research
Yes No
= a decision Point
DO NOT REPRODUCE WITHOUT PERMISSION
REQUESTS TO:Office of Nursing Research & EBPThe University of Iowa Hospitals and ClinicsIowa City, IA 52242-1009
Revised: April 1998 © UIHC
(Titler, Kleiber, Steelman, et al., 2001)
Pilot April – June 2010
• Units Chosen – 3RCP (adult med/surg, ortho, urology)
– 3JCP (pediatric med/surg, including trauma, hem/onc, and bone marrow transplant)
– 4RCP (adult cardiology)
– 7RCS (adult leukemia and bone marrow transplant)
• Units Excluded ‐ ICU

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
8
Pilot (cont.)
• Pre‐pilot web‐based knowledge survey completed on the pilot units (n=76)
• Policy developed
– Respiratory monitoring
– Sedation scale
• Electronic medical record documentation
updated
Monitoring Guidelines
• 2 required components:– Respiratory Assessment*
• Respiratory rate• Respiratory rhythm/pattern• Respiratory effort• Respiratory depth• Airway characteristics
(e.g., presence of snoring)
– Sedation Assessment• POSS scale
*Based on nursing judgment, patients alert, awake and/or participating inactivities may not require a full respiratory assessment
[American Society of Anesthesiologists Task Force on Neuraxial Opioids, 2009;McCaffery & Pasero, 1999; Pasero, 2009; Pasero & McCaffery, 2008; Wells, Pasero &McCaffery (2008). Improving the quality of care through pain assessment andmanagement. In R. G. Hughes (Eds.), Patient Safety and Quality: An evidence‐basedhandbook for nurses, (Ch. 17). (AHRQ Publication No. 08‐0043). Rockville, MD: Author. Obtained @ http://www.ahrq.gov/qual/nurseshdbk/]
Monitoring Guidelines (cont.)
• Frequency of Assessment based on:– Route and Delivery
• Opioid IV infusions/Drips/PCA/CCA with and without a basal rate• Scheduled or PRN doses, any route
• Special consideration for sleeping patients– Assess respiratory status first– Assess sedation (e.g. responsiveness to stimuli, such as, patient stirs when the bed is bumped)
– Awaken patient if concerned or patient is snoring
• End‐of‐life and Palliative Care patients– Monitoring can be requested by LIP

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
9
Sedation LevelModified Pasero Opioid‐Induced Sedation Scale
(POSS)
0 = Sleep and easy to arouse Acceptable; no action necessary; may increase opioid dose if needed/ordered
1 = Awake and alertAcceptable; no action necessary; may increase opioid dose if needed/ordered
2 = Slightly drowsy, easily arousedAcceptable; no action necessary; may increase opioid dose if needed/ordered
3 = Frequently drowsy, arousal, drifts off to sleep during conversationUnacceptable; continue to monitor more frequently until return to baseline; notify
LIP and consider calling the Rapid Response Team and giving dilute naloxone
4 = Somnolent, minimal or no response to physical stimulationUnacceptable; stop opioid; continue to monitor more frequently until return to
baseline; notify LIP and consider calling the Rapid Response Team and giving dilute naloxone
(McCaffery & Pasero, 1999; Pasero, 2009; Pasero & McCaffery, 2008)
Frequency of Assessment
• Opioid IV infusions/Drips/PCA/CCA with and without a basal rate, and/or long‐acting or sustained released opioids– At initiation
– Initial re‐assessment after opioid administration should consider factors such as:
• Peak effect of opioid administered
• Patient activity
• Risk factors for over‐sedation
• Previous exposure to sedation(Note: if the patient has been on ongoing opioid therapy for more than 24 hours and then is
switched over to a long‐acting or sustained release opioid, monitoring may proceed at the
current frequency; monitoring does not need to start over when a new opioid is started)
Frequency of Assessment (cont.)
• Opioid IV infusions/Drips/PCA/CCA with and without a basal rate, and/or long‐acting or sustained released opioids (cont.)
– Every hour for 12 hours
– Then every 2 hours for 12 hours
– Then every 4 hours for duration if:
• POSS Score < 3
• Respiratory rate at baseline
• Absence of respiratory distress, apnea, and snoring

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
10
Frequency of Assessment (cont.)
• Opioid IV infusions/Drips/PCA/CCA with and without a basal rate, and/or long‐acting or sustained released opioids (cont.)
– More frequent per nursing discretion if:• POSS Score of 3 or 4
• Change in respiratory rate
• Presence of respiratory distress/apnea/snoring
• Patient unstable
• Patient condition warrants– Notify LIP
– Consider calling Rapid Response Team
– Consider giving dilute Naloxone
Frequency of Assessment (cont.)
• Nurse Administered (e.g. PRN or scheduled) doses, any route ‐ each dose given– At initiation
– Initial re‐assessment after opioid administration should consider factors such as:
• Peak effect of opioid administered
• Patient activity
• Risk factors for over‐sedation
• Previous exposure to sedation
– After the initial 24 hours, stable patients receiving around the clock opioid dosing, should have re‐assessments for sedation and pain level completed every 4 hours
Pilot Documentation Flowsheet

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
11
Pilot (cont.)
• Education
– In‐Services
– Rapid Cycle Improvement Method
– Unit Reference Binders
• Policy
• Research articles
• Educational material – PPT, case scenarios
• Opioid reference guides/cards, IV administration guidelines
– Pocket Cards
Sedation Assessment: POSS Scale
0 = Sleep and easy to arouse Acceptable; no action necessary; may increase opioid dose if needed/ordered
1 = Awake and alertAcceptable; no action necessary; may increase opioid dose if needed/ordered
2 = Slightly drowsy, easily arousedAcceptable; no action necessary; may increase opioid dose if needed/ordered
3 = Frequently drowsy, arousal, drifts off to sleep during conversationUnacceptable; Continue to monitor more frequently until return to baseline. Notify LIP and consider calling the Rapid Response Team and giving dilute naloxone
4 = Somnolent, minimal or no response to physical stimulationUnacceptable; stop opioid; Continue to monitor more frequently until return to baseline. Notify LIP and consider calling the Rapid Response Team and giving dilute naloxone
Peak Effects:PO opioids: 60 minutesIV opioids: 30 minutes
Pain Reassessment:Complete at the time of sedation re-assessment
Pocket Cards
Monitoring Standards for Sedation after Opioid Administration
Continuous Infusions/PCA/Frequent NCA*/longacting opioids:
Respiratory Assessment AND Sedation Assessment (POSS): • Prior to initiation• 1st reassessment considering peak, risk factors,
previous opioids, and patient activity• Then ever y 1 hr x 12 hrs; every 2 hrs x 12 hrs; then
every 4 hrs if stable
Scheduled, PRN Opioids, Infrequent/Routine NCA*:Respiratory Assessment AND Sedation Assessment (POSS): • Prior to administration (for first 24 hr if ATC)• Re‐assessment after each opioid dose considering peak,
risk factors, previous opioids, and patient activity (for first 24 hr if ATC – then q4 hrs if stable)
Respiratory Assessment Is:
• Respiratory rate, effort, depth, and airway characteristics
NCA= Nurse Controlled Analgesia via locked infusion pump
Is ChangeAppropriate for
Adoption inPractice?
Continue to EvaluateQuality of Care and
New Knowledge
No YesInstitute the Change in Practice
Monitor and Analyze Structure,Process, and Outcome Data
- Environment- Staff- Cost- Patient and Family
Disseminate Results
= a decision Point
DO NOT REPRODUCE WITHOUT PERMISSION
REQUESTS TO:Office of Nursing Research & EBP
The University of Iowa Hospitals and ClinicsIowa City, IA 52242-1009
Revised: April 1998 © UIHC
Titler MG, Kleiber C, Steelman V, Rakel B, Budreau G, Everett LQ, Buckwalter KC, Tripp Reimer T, & Goode C (2001). The Iowa Model of Evidence-Based Practice to Promote Quality Care. Critical Care Nursing Clinics of North America, 13(4):497-509.

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
12
Project IntegrationAugust – September 2010
• Infrastructure links– Inpatient Care (excluded
ICUs)
– Adult & Pediatrics
– Quality Management
– Staff Education Committee
– Professional Nursing Practice Committee (policy)
– Informatics
• Unit activities– Staff Nurse Involvement
– Unit Resource Manual
– APN Role
– NM Commitment
Policy & Staff Education Development
• Policy– Revised after pilot complete based on feedback
– Approved by the Professional Nursing Practice Committee (Aug. 2010)
• Staff Education– Approved by the Staff Education Committee (Aug. 2010)
• Informatics– Documentation changes in EMR completed (Aug. 2010)
Is ChangeAppropriate for
Adoption inPractice?
Continue to EvaluateQuality of Care and
New Knowledge
No YesInstitute the Change in Practice
Monitor and Analyze Structure,Process, and Outcome Data
- Environment- Staff- Cost- Patient and Family
Disseminate Results
= a decision Point
DO NOT REPRODUCE WITHOUT PERMISSION
REQUESTS TO:Office of Nursing Research & EBP
The University of Iowa Hospitals and ClinicsIowa City, IA 52242-1009
Revised: April 1998 © UIHC
Titler MG, Kleiber C, Steelman V, Rakel B, Budreau G, Everett LQ, Buckwalter KC, Tripp Reimer T, & Goode C (2001). The Iowa Model of Evidence-Based Practice to Promote Quality Care. Critical Care Nursing Clinics of North America, 13(4):497-509.

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
13
Implementation September 2010
• PowerPoint™ presentation on hospital computer education system
• Live in‐services
• One‐page flier
• Pocket cards
Revised Documentation
Documentation – Pain Report

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
14
Is ChangeAppropriate for
Adoption inPractice?
Continue to EvaluateQuality of Care and
New Knowledge
No YesInstitute the Change in Practice
Monitor and Analyze Structure,Process, and Outcome Data
- Environment- Staff- Cost- Patient and Family
Disseminate Results
= a decision Point
DO NOT REPRODUCE WITHOUT PERMISSION
REQUESTS TO:Office of Nursing Research & EBP
The University of Iowa Hospitals and ClinicsIowa City, IA 52242-1009
Revised: April 1998 © UIHC
Titler MG, Kleiber C, Steelman V, Rakel B, Budreau G, Everett LQ, Buckwalter KC, Tripp Reimer T, & Goode C (2001). The Iowa Model of Evidence-Based Practice to Promote Quality Care. Critical Care Nursing Clinics of North America, 13(4):497-509.
Post‐Implementation Knowledge SurveyApril – May 2011
• Completed by nurses on the pilot units (n=67)
• Used same web‐based knowledge survey (pre/post comparison)
Knowledge Survey Results
Strongly Disagree
Strongly Agree

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
15
Knowledge Survey Results (cont.)
Strongly Disagree
Strongly Agree
Knowledge Survey Results (cont.)
Strongly Disagree
Strongly Agree
Knowledge Survey Results (cont.)
Strongly Disagree
Strongly Agree

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
16
Evaluation
• Audit and Feedback
– Pain Resource Nurses
– Nurse Managers
– Assistant Nurse
Managers
– Pain Staff Nurse Champions
• Ongoing chart audits
Documentation – Pain Report
Documentation – Pain Report
Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
17
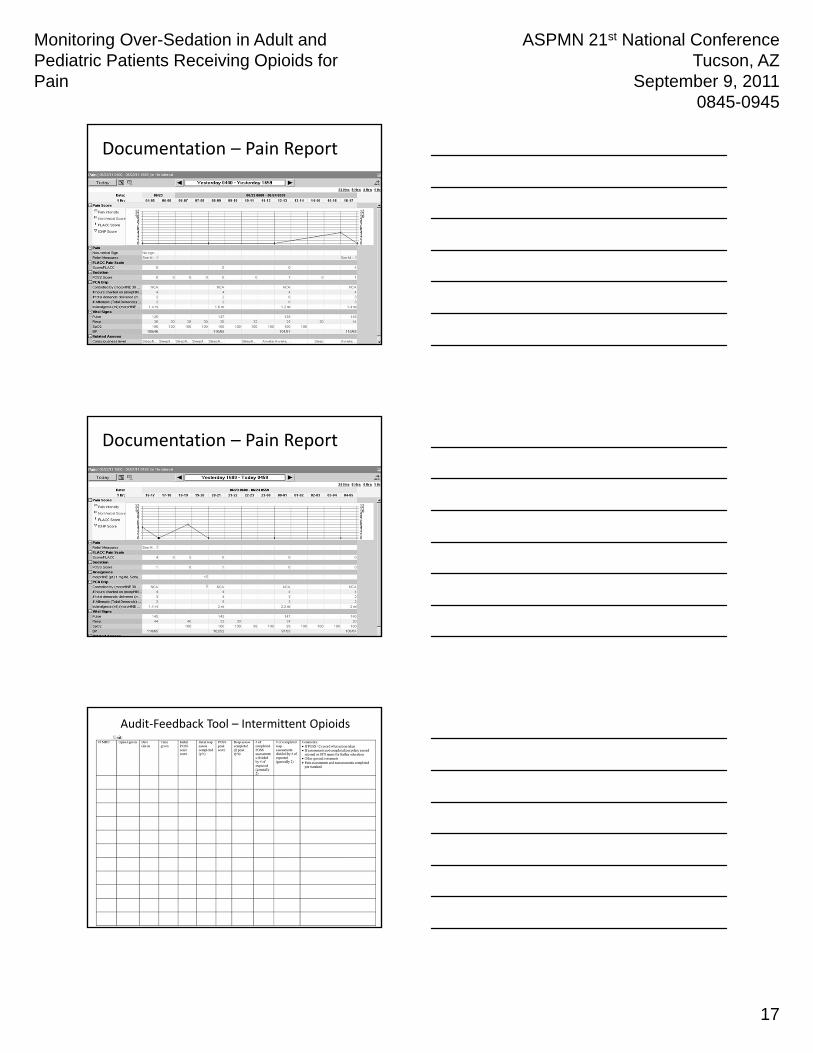
Documentation – Pain Report
Documentation – Pain Report
Audit‐Feedback Tool – Intermittent Opioids

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
18
Audit‐Feedback Tool – Continuous Opioids
Chart Audit Data
POSS Reminders….(February 2011)
• Make it THOROUGH – Sedation assessment requires all these:– POSS Scale and Respiratory Assessment and Respiratory Rate
• for all opioids of all routes– Morphine, Dilaudid, Oxycodone, Lortab, Tylenol #3, etc.
• Make it EASY:– Complete Pain and Sedation Assessment together! (Sedation Assessment includes POSS, Respiratory Assessment and RR)
• Reassessments (for both pain and sedation) should occur at baseline and peak of intervention:‐ IVmedications peak: 30 minutes ‐ POmedications peak: 60 minutes
– If receiving ATC interventions:• After the first 24 hours, q 4 hr assessments may be done (including extended release opioids like OxyContin)
– Applies to patients who have been on the same opioid, same route and who have been stable over the previous 24 hours
• Make it ACCURATE:– Check your charting times
• It’s easy to chart that everything happened on the hour or the half hour (e.g. 1200, 1230, 1600, 1630) but is that accurate?
– Give IV analgesics over 5 minutes on the pump• Adjust your pain and sedation reassessment times if you:
– Administer the analgesic over a longer time– Do not have a fast enough carrier solution for the med to reach the patient in a timely fashion– Use a lot of extra tubing between the medication and the patient
» Priming volume of standard ext set + 1 stopcock = 4.2 ml» Priming volume of microbore ext set + 1 stopcock = 0.57ml
– Pass on to the next shift when the next sedation and pain assessments are due
• Keep your patients SAFE:– Continuous oximeters are required for pediatric patients with basals– Giving Benadryl to help patients sleep can be dangerous with opioids– Always be thinking about risk factors for over‐sedation when giving an opioid via any route
• Meds that increase sedation (e.g. ATIVAN, anticonvulsants, Benadryl, Phenergan)• Patient Conditions
– SNORING/airway/pulmonary compromise Infant < 12 months– Obesity Renal/Liver Insufficiency– Cognitive Impairment Neuromuscular Disease– Opioid naïve (< 5 days of opioid exposure) Head Trauma/Craniotomy– Sudden cessation of pain First 24 hours post‐op

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
19
Opioid Over‐Sedation Monitoring Change and Reminders(June 2011)
Continuous Pulse Oximetry: *****ONLY needed for the first 48 hours for pediatric patients with basal rates/opioid infusions (if stable) *******
• Sedation assessment and documentation MUST include:– POSS Scale Score – Respiratory Rate– Respiratory Assessment
• Respiratory rhythm or pattern• Respiratory effort• Respiratory depth• Airway characteristics
• All opioids and All routes (IV, PO)
• Assessment Frequency:– PRN or Scheduled Opioids
• Baseline• Peak (30 min for IV meds; 60 min for PO meds)• After 24 hrs of ATC dosing, may change to Q4 hrs for stable patients
– PCAs/NCAs/CCAs/Opioid Infusions• Baseline• Peak (30 min)• Q1 hr *12 hours• Q2 hrs *12 hours• Then Q4 hrs if stable
• PLEASE do not “complete” rows in POSS section of “Peds Cares” flowsheet– Someone may forget to re‐activate later when opioid given
Next Steps
• Targeted education/re‐infusion
• Continue audit/feedback
• Revisions to documentation in EMR
Is ChangeAppropriate for
Adoption inPractice?
Continue to EvaluateQuality of Care and
New Knowledge
No YesInstitute the Change in Practice
Monitor and Analyze Structure,Process, and Outcome Data
- Environment- Staff- Cost- Patient and Family
Disseminate Results
= a decision Point
DO NOT REPRODUCE WITHOUT PERMISSION
REQUESTS TO:Office of Nursing Research & EBP
The University of Iowa Hospitals and ClinicsIowa City, IA 52242-1009
Revised: April 1998 © UIHC
Titler MG, Kleiber C, Steelman V, Rakel B, Budreau G, Everett LQ, Buckwalter KC, Tripp Reimer T, & Goode C (2001). The Iowa Model of Evidence-Based Practice to Promote Quality Care. Critical Care Nursing Clinics of North America, 13(4):497-509.

Monitoring Over-Sedation in Adult and Pediatric Patients Receiving Opioids for Pain
ASPMN 21st National ConferenceTucson, AZ
September 9, 20110845-0945
20
Dissemination
• Posters
– Nursing Recognition Day (2010 & 2012)
– National Evidence‐Based Practice Conference (2012)
• Presentations
– 17th National Evidence‐Based Practice Pre‐Conference (April 2010)
– Evidence‐Based Practice Staff Nurse Internship (March 2011)
– ASPMN Conference (September 2011)
• Manuscript
Conclusion
• Don’t take on the world
• Be flexible
• Use data to support your efforts
• Include nurses caring for patients
Questions/Comments


















