
1.6 (x, y) x y quadrants first quadrant second quadrant third quadrant fourth quadrant.
1
SMCH/HCDS/20: Indian Public Health Standard-I
Quadrant-I
Personal Details
Role Name Affiliation
Principal Investigator
Prof. CP Mishra Department of Community Medicine,
Institute of Medical Sciences, Banaras
Hindu University, Varanasi
Paper Coordinator
Prof. Najam Khalique Department of Community Medicine,
J N Medical College, AMU, Aligarh
Content Writer
Dr. Urfi Assistant Professor
Department of Community Medicine,
J N Medical College, AMU, Aligarh
Content Reviewer
Prof. M. Athar Ansari
Department of Community Medicine,
J N Medical College, AMU, Aligarh
Description of Module
Items Description of Module
Subject name Social Medicine & Community Health
Paper name Health Care Delivery System
Module name/Title Indian Public Health Standard I
Module Id SMCH/HCDS/20
Pre-requisites Understanding of organization and functioning of health system.
Objectives
To know about IPHS guidelines for sub-centres and their
functioning.
Keywords
Antenatal Care, Primary Health Centres, Quality Assurance,
Village Health and Nutrition Day.
2
Indian Public Health Standards (IPHS) I and Guidelines for Sub Centres
Introduction
National Rural Health Mission (NRHM) was launched to strengthen the Rural Public Health
System and has since met many hopes and expectations.(1)The Mission seeks to provide effective
health care to the rural populace throughout the country with special focus on the States and Union
Territories (UTs), which have weak public health indicators and/or weak infrastructure. Towards this
end, the Indian Public Health Standards (IPHS) for Sub-centres, Primary Health Centres (PHCs),
Community Health Centres (CHCs), Sub-District and District Hospitals were published in January
2007 and have been used as the reference point for public health care infrastructure planning and up-
gradation in the States and UTs. IPHS are a set of uniform standards foreseen to improve the quality
of health care delivery in the country. The IPHS documents have been revised keeping in view the
changing protocols of the existing programmes and introduction of new programmes especially for
Non-Communicable Diseases. Flexibility is allowed to suit the diverse needs of the states and regions.
Our country has a large number of public health institutions in rural areas from Sub-centres at the
most peripheral level to the district hospitals. It is highly desirable that they should be fully functional
and deliver quality care. These IPHS guidelines will act as the main driver for continuous
improvement in quality and serve as the bench mark for assessing the functional status of health
facilities. States and UTs to adopt these IPHS guidelines for strengthening the Public Health Care
Institutions and put in their best efforts to achieve high quality of health care for our people across the
country, which further will also help the country in achieving the National and Millennium
Development Goals.
IPHS standards were given during the year 2007, which were revised again in 2012. We will
proceed with the latest guidelines, vis 2012. For the simplicity of readers, we have divided this section
into two parts, Part 1 will cover guidelines for Sub centre and PHC while Part 2 will deal with CHC,
Sub-District/ Divisional Hospital and District Hospitals. IPHS Part 1 will be discussed in this chapter.
Learning Outcomes
Upon completion this module, the reader should be able to :
State the need of guidelines for Sub - Centre
Mention the objectives of the Indian Public Health Standards for Sub-Centre
Categorize Sub-Centres
List services provided by Sub - Centre
Identify logistic and infrastructure requirement for sub centre.
Mention about record maintenance and reporting at sub centre
Mention approach to quality assurance and accountability at sub centre level.
Main Text
1. Need of guidelines for Sub - Centre
3
The Sub-centres are vital peripheral institutions for providing primary health care to the people and
play a vital role in the implementation of various Health & Family Welfare programmes at the grass-
root level. One of the important components of National Rural Health Mission (NRHM) is to
strengthen the Sub-centres to the level of Indian Public Health Standards (IPHS). The primary focus
of Sub-centre remains the Reproductive and Child Health (RCH) services. In order to provide quality
care at sub centre, IPHS are being prescribed to provide basic promotive, preventive and few curative
primary health care services to the community and achieve and maintain an acceptable standard of
quality of life.
2. Objectives of the Indian Public Health Standards for Sub-Centre
a. To specify the minimum assured services that Sub-centre is expected to provide through this
facility.
b. To maintain an acceptable quality of care for these services
c. To facilitate monitoring and supervision of these facilities.
d. To make the services provided more accountable and responsive to people’s needs
3. Categorization of Sub-Centres
Sub-Centres have been categorized into two types - Type A and Type B.
Type A : Type A Sub Centre will provide all recommended services except that the facilities for
conducting delivery will not be available here.
Type B (MCH Sub-Centre): Type B Sub-centre, will provide all recommended services including
facilities for conducting deliveries at the Sub-centre itself. They should be provided with all labour
room facilities and equipment including Newborn care corner. ANMs of these Sub-centres should be
SBA trained.
4. Services to be provided in a Sub-Centres (2)
These services are called assured services and are as follow.
4.1.Maternal Health care(3)
i. Antenatal care:
a. Early registration of all pregnancies, within first trimester.
b. Minimum 4 ANC visits. Suggested schedule:
1st visit: Within 12 weeks, for registration, history and first antenatal check-up
2nd visit: Between 14 and 26 weeks
3rd visit: Between 28 and 34 weeks
4th visit: Between 36 weeks and term.
c. Associated services like general examination such as height, weight, B.P., anaemia,
abdominal examination, breast examination, Iron & Folic Acid Supplementation, injection
tetanus toxoid, treatment of anaemia etc.
4
d. laboratory investigations like Urine Test for pregnancy confirmation, haemoglobin
estimation, urine for albumin and sugar and linkages with PHC for other required tests.
e. Identification of high risk pregnancy cases and appropriate and timely referral.
g. Counselling on diet, rest, advice on institutional deliveries, pre-birth preparedness, danger
signs.
h. Provide information about provisions under current schemes like Janani Suraksha Yojana.
i. Identify suspected RTI/STI case, provide counseling, basic management and referral
services. Counselling & referral for HIV/AIDS.
ii. Intra-natal care:
a. Promotion of institutional deliveries
b. Skilled attendance at home deliveries when called for.
c. Appropriate and timely referral of high risk cases which are beyond her capacity of
management.
For Type B Sub-centre: Managing labour using Partograph.
a. Identification and management of danger signs during labour.
b. Basic fist aid treatment for PPH, Eclampsia, Sepsis and prompt referral of such cases.
c. Minimum 24 hours of stay of mother and baby after delivery at Sub-centre.
iii. Postnatal care:
a. Initiation of early breast-feeding within one hour of birth.
b. Ensure post-natal home visits.
c. Counselling on diet & rest, hygiene, contraception, essential newborn care, immunization
and infant and young child feeding.
4.2.Child health care
i. Newborn Care Corner: In the Labour Room to provide Essential Newborn Care, if the
Deliveries take Place at the Sub-centre (Type B).
ii. Essential Newborn Care: Maintain the body temperature and prevent hypothermia
[provision of warmth/Kangaroo Mother Care (KMC)], maintain the airway and breathing,
initiate breastfeeding within one hour, infection protection, cord care, and care of the eyes.
Post natal visits.
iii. Counselling on exclusive breast-feeding for 6 months and appropriate and adequate
complementary feeding.
iv. Immunization Services: Full Immunization of all infants and children including Vitamin
A prophylaxis.
v. Prevention and control of childhood diseases like malnutrition, infections, ARI, Diarrhea,
Fever, Anemia etc.
4.3.Family Planning and Contraception
a. Education, Motivation and counselling to adopt appropriate Family planning methods. �
b. Provision of contraceptives such as condoms, oral pills, emergency contraceptives, Intra
Uterine Contraceptive Devices (IUCD) insertions.
5
c. Follow up services.
4.4.Safe Abortion Services (MTP): Counselling and appropriate referral for safe abortion services
(MTP) for those in need.
4.5.Curative Services
a. Provide treatment for minor ailments including fever, diarrhea, ARI, worm infestation and First
Aid.
b. Appropriate and prompt referral.
c. Once a month clinic by the PHC medical officer is desirable.
d. To provide AYUSH treatment.
4.6. Adolescent Health Care : Education, counselling and referral.
4.7.School Health Services: Screening, treatment of minor ailments, immunization, de-worming,
prevention and management of Vitamin A and nutritional deficiency anemia.
4.8.Endemic Diseases: Assisting in detection, Control and reporting of local endemic diseases such
as Malaria, Kala Azar, Japanese encephalitis, Filariasis, Dengue etc.
4.9.Disease Surveillance, Integrated Disease Surveillance Project (IDSP) : Surveillance about any
abnormal increase in various diseases.
4.10.Water and Sanitation
4.11.Out reach/Field Services
i. Village Health and Nutrition Day (VHND)
VHND should be organised at least once in a month in each village with the help of Medical
Officer, Health Assistant Female (LHV) of PHC, HWM, HWF, ASHA and AWW. The ANM is
accountable for these services. Participation of Anganwadi workers, ASHAs and community
volunteers would be essential for mobilization of beneficiaries and local organizational support.
The services to be provided at VHND are listed below.
a. Early registration and Antenatal care for pregnant women.
b. Immunization and Vitamin A administration to all under 5 children
c. Coordination with ICDS programme for Supplementary nutritional services for its
beneficiaries.
d. Family planning counseling and distribution of contraceptives.
e. Registration of Births and Deaths.
ii. Home Visits Essential
a. For skilled attendance at birth
b. Post natal and newborn visits
c. To check out on disease incidences and report notifiable disease.
iii. House-to-House Surveys
These surveys would be done once annually, preferably in April. The surveys would include:
a. Age and sex of all family members.
6
b. Assess and list eligible couples and their unmet needs for contraception.
c. Identify persons with suspicious of leprosy and refer
d. Identify persons with blindness, list and refer:
e. Identify persons with hearing impairment/ deafness, list and refer.
f. Annual mass drug administration in filaria endemic areas.
iv. Community Level Interactions
a. Focus group discussions
b. Health Communication especially as related to National Health programmes
c. BCC activities.
4.12.Training of Trained Birth Attendants and ASHA/community health volunteers.
4.13. Co-ordinate services of anganwadi worker, ASHA, village health and sanitation committee.
4.14. National Health Programmes
Communicable Disease Programme
i. National AIDS Control Programme (NACP):
a. Condom promotion & distribution of condoms to the high risk groups.
b. Help and guide patients with HIV/AIDS receiving ART with focus on adherence.
c. IEC activities to enhance awareness and preventive measures about STIs and HIV/AIDS,
PPTCT services and HIV-TB coordination.
ii. National Vector Borne Disease Control Programme (NVBDCP):
a. Collection of Blood slides of fever patients
b. Rapid Diagnostic Tests (RDT) for diagnosis of Pf malaria in high Pf endemic areas.
c. Appropriate anti-malarial treatment.
d. Assistance for integrated vector control activities in relation to Malaria, Filaria, JE, Dengue,
Kala-Azar etc. as prevalent in specific areas.
e. Prevention of breeding places of vectors through IEC and community mobilization.
f. Annual mass drug administration with single dose of Diethyl carbamazine (DEC) to all elligible
population at risk of lymphatic filariasis.
g. Promotion of use of insecticidal treated nets.
h. Record keeping and reporting as per programme guidelines.
iii. National Leprosy Eradication Programme (NLEP):
a. Health education to community regarding signs and symptoms of leprosy, its complications,
curability and availability of free of cost treatment.
b. Referral of suspected cases of leprosy and its complications to PHC.
c. Provision of subsequent doses of MDT and follow up.
iv. Revised National Tuberculosis Control Programme (RNTCP):
a. Referral of suspected symptomatic cases to the PHC/Microscopy centre.
b. Provision of DOTS at Sub-centre, proper documentation and follow-up.
c. Care should be taken to ensure compliance and completion of treatment in all cases.
7
Non-communicable Disease (NCD) Programmes
i. National Programme for Control of Blindness (NPCB):
ii. National Programme for Prevention and Control of Deafness (NPPCD)
iii. National Mental Health Programme:
iv. National Programme for Prevention and Control of Cancer, Diabetes, Cardiovascular
Diseases and Stroke.
v. National Iodine Deficiency Disorders Control Programme
vi. National Tobacco Control Programme
vii. Disability Prevention
5. Logistics, Infrastructure and support at sub centre.
5.1. Drugs
The essential drugs should be available at the sub centre. Accurate records of stock should be
maintained.
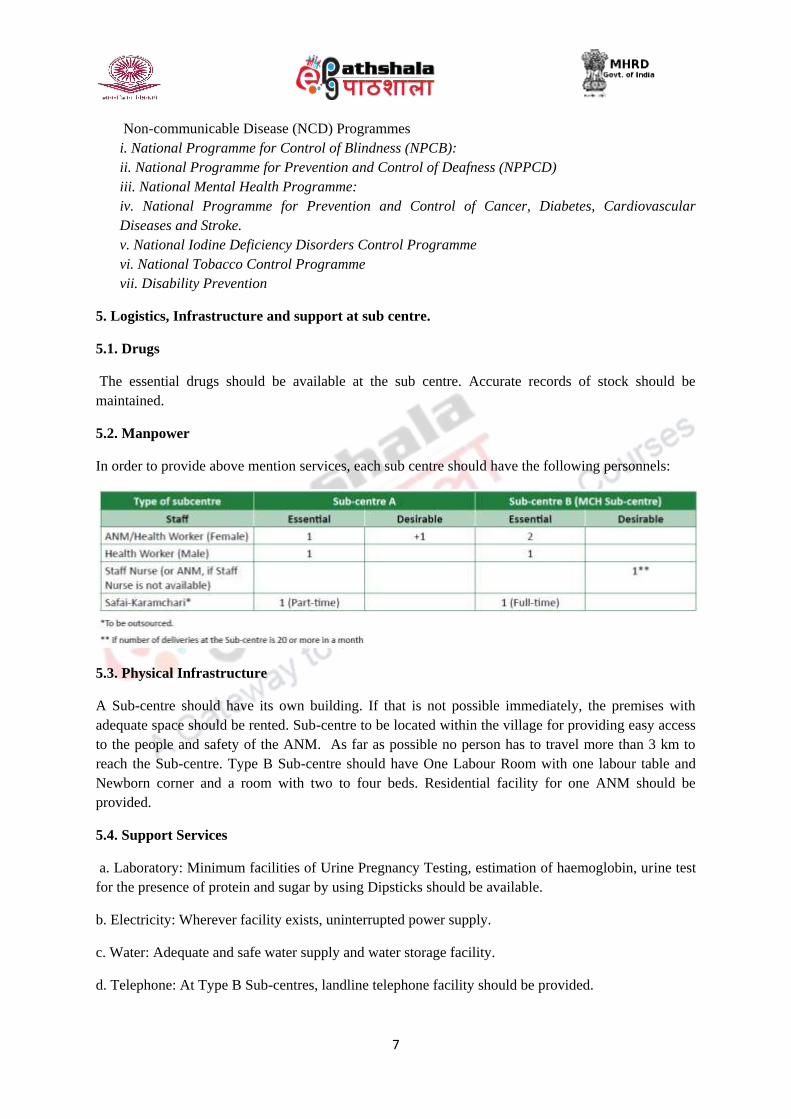
5.2. Manpower
In order to provide above mention services, each sub centre should have the following personnels:
5.3. Physical Infrastructure
A Sub-centre should have its own building. If that is not possible immediately, the premises with
adequate space should be rented. Sub-centre to be located within the village for providing easy access
to the people and safety of the ANM. As far as possible no person has to travel more than 3 km to
reach the Sub-centre. Type B Sub-centre should have One Labour Room with one labour table and
Newborn corner and a room with two to four beds. Residential facility for one ANM should be
provided.
5.4. Support Services
a. Laboratory: Minimum facilities of Urine Pregnancy Testing, estimation of haemoglobin, urine test
for the presence of protein and sugar by using Dipsticks should be available.
b. Electricity: Wherever facility exists, uninterrupted power supply.
c. Water: Adequate and safe water supply and water storage facility.
d. Telephone: At Type B Sub-centres, landline telephone facility should be provided.
8
e. Toilet
6.Record Maintenance and Reporting
Proper maintenance of records of services provided at the Sub-centres and the morbidity/mortality
data is necessary for assessing the health situation in the Sub-centre area. In addition, all births and
deaths under sub- centre should be documented and sex ratio at birth should be monitored and
reported.
7. Quality Assurance and Accountability
This can be ensured through regular skill development training/Continuing Medical Education (CME)
of health workers (at least one such training in a year), as per guidelines of NRHM.
Summary
In the public sector, a Sub-centre is the most peripheral and first point of contact between the primary
health care system and the community. In the field of rural health, the objective was to establish: one
Sub-centre for a population 5000 people in the plains and for 3000 in tribal and hilly areas. A Sub-
centre provides interface with the community at the grass-root level, providing all the primary health
care services. As Sub-centres are the first contact point with the community, the success of any
nation-wide programme would depend largely on the well functioning Sub-centres providing services
of acceptable standard to the people. The current level of functioning of the Sub-centres is much
below the expectations. In order to provide quality care in these Sub-centres, Indian Public Health
Standards (IPHS) were being prescribed to provide basic primary health care services to the
community and achieve and maintain an acceptable standard of quality of care. These standards
would help monitor and improve functioning of the Sub Centre.
References:
1. National Rural Health Mission 2005-2012 – Reference Material (2005), Ministry of Health &
Family Welfare, Government of India.
2. Govt. Of India(2012) Indian Public Health Standards Guidelines for Sub Centres, Ministry of
health and family welfare, New Delhi.
3. Guidelines for Ante-Natal Care and Skilled Attendance at Birth by ANMs and LHVs (2005),
Maternal Health Division, Department of Family Welfare, Ministry of Health & Family
Welfare, Government of India.
9
Guidelines for Primary Health Centres as per Indian Public Health Standards (IPHS)
Introduction
The concept of Primary Health Centre (PHC) in India was given by the Bhore Committee in
1946 as a basic health unit to provide as close to the people as possible, an integrated curative and
preventive health care to the rural population with emphasis on preventive and promotive aspects of
health care. The Bhore committe aimed at having a health centre to serve a population of 10,000 to
20,000 with 6 medical officers, 6 public health nurse and supporting staff, which even after span of 70
years has not been implemented.
PHC is the first contact point between village community and the Medical Officer. The health
planners in India have visualized the PHC and its Sub-Centres (SCs) as the proper infrastructure to
provide health services to the rural population. These centres were functioning as peripheral health
service institutions with little or no community involvement. Increasingly, these centres came under
criticism, as they were not able to provide adequate health coverage, partly, because they were poorly
staffed and equipped and lacked basic amenities.
Learning Outcomes
Upon completion this module, the reader will be able to:
To understand the need for a proper set of guidelines for Primary Health Centre (PHC)
Enumerate objectives of the Indian Public Health Standards for PHC
Describe the services provided by PHC
Identify infrastructure and human resource requirement for PHC
Mention approach to quality assurance and accountability at PHC level.
Understand monitoring of PHC functioning.
State requirement for ensuring accountability at PHC
Main Text
1. Need for a proper set of guidelines for Primary Health Centre (PHC)
IPHS For PHC has been prepared keeping in view the resources available with respect to functioning
requirement for PHC with minimum standard as building, manpower, instrument, drugs and other
facilities. The standards prescribed are for a PHC covering 20,000 to 30,000 population with 6 beds.
2. Objectives of the Indian Public Health Standards for PHC
i. To provide comprehensive primary health care to the community through the PHC.
ii.To achieve and maintain an acceptable standard of quality of care.
iii. To make the services more responsive and sensitive to the needs of the community.
3. Services at the Primary Health Centre for meeting the IPHS(1)
10
From Service delivery angle, PHCs may be of two types, – Type A PHC: PHC with delivery load of
less than 20 deliveries in a month, and Type B PHC: PHC with delivery load of 20 or more deliveries
in a month. They will be providing assured services which will cover all the essential elements of
preventive, promotive, curative and rehabilitative primary health care which are as follows:
3.1.Medical care
a. OPD services: A total of 6 hours of OPD services for six days in a week.
b. 24 hours emergency services:Appropriate management of injuries and accident, and First Aid
should be provided by PHC.
c. Referral services. In-patient services (6 beds).
3.2.Maternal and Child Health Care Including Family Planning
a) Antenatal care
i. Early registration of all pregnancies ideally in the first trimester
ii.Minimum 4 antenatal checkups and provision of complete package of services.
iii. Lab investigations like Haemoglobin, Urine albumin and sugar, RPR test for syphilis and
Blood Grouping and Rh typing.
iv.Nutrition and health counseling.
v.Identification and management of high risk cases and timely referral.
vi.Tracking of missed and left out ANC.
b) Intra-natal care: (24-hour delivery services both normal and assisted) (2)
i.Promotion of institutional deliveries.
ii.Management of normal deliveries.
iii. Assisted vaginal deliveries.
iv.Manual removal of placenta.
v. Appropriate and prompt referral.
vi.Management of Pregnancy Induced ypertension including referral.
vii.Minimum 48 hours of stay after delivery.
viii.Managing labour using Partograph.
c) Postnatal Care
i. Home visits by ANM of the concerned area.
ii.Initiation of early breast-feeding within one hour of birth.
iii.Counseling on nutrition, hygiene, contraception, essential new born care and immunization.
iv. Others: Provision of facilities under Janani Suraksha yojana.
d) New Born care
i.Facilities for Essential New Born Care (ENBC) and Resuscitation.
ii.Early initiation of breast feeding with in one hour of birth.
iii.Management of neonatal hypothermia, infection protection, cord care and identification of sick
newborn and prompt referral.
e) Care of the child
11
i. Routine and Emergency care of sick children including Integrated Management of Neonatal
and Childhood Illnesses (IMNCI) strategy and inpatient care. Prompt referral of sick children
requiring specialist care.
ii. Counseling on exclusive breast-feeding for 6 months and appropriate and adequate
complementary feeding from 6 months of age.
iii.Assess the growth and development of the infants and under 5 children and make timely
referral.
iv.Full Immunization of all infants and children
v. Vitamin A prophylaxis
vi. Prevention and control of routine childhood diseases, infections like diarrhoea, pneumonia
malnutrition and anemia.
g) Family Welfare
i.Education, Motivation and Counseling to adopt appropriate Family planning methods.
ii.Provision of contraceptives such as condoms, oral pills, emergency contraceptives, IUCD
insertions.
iii. Referral and Follow up services to the eligible couples adopting permanent methods
iv.Counseling and appropriate referral for couples having infertility.
v. Permanent methods like Tubal ligation and vasectomy/NSV.
3.3.Medical Termination of Pregnancies
Counseling and appropriate referral for safe abortion services (MTP) for those in need. MTP
using Manual Vacuum Aspiration (MVA) technique will be provided in PHCs, where trained
personnel and facility exist. Timely referral to the facility approved for 2nd trimester of MTP.
3.4.Management of RTIs/STDs
3.5.Nutrition Services
a.Diagnosis of and nutrition advice to malnourished children, pregnant women and others
b.Diagnosis and management of anaemia and vitamin A deficiency.
c. Coordination with ICDS
3.6.School Health:
Teachers screen students on a continuous basis and ANMs/HWMs along with doctors should visit
the schools for screening, treatment of minor ailments and referral. Overall services to be provided
under school health shall include:
i. Screening, health care and referral: Screening of general health, Anaemia/Nutritional status,
visual acuity, hearing problems, dental check up, common skin conditions, Heart defects, physical
disabilities, learning disorders, behavior problems, etc.
ii. Immunization: Fixed day activity
iii. Micronutrient (Vitamin A & IFA) management:
iv. De-worming
v. Mid Day Meal:
12
3.7.Adolescent Health Care:
a. Adolescent and Reproductive Health
b. Nutritional Counselling
c. STI/RTI management
d. Referral Services for VCTC and PPTCT services and services for Safe termination of pregnancy
3.8.Promotion of Safe Drinking Water and Basic Sanitation:
3.9.Prevention and control of locally endemic diseases like malaria, Kala Azar, Japanese Encephalitis
3.10.Collection and reporting of vital events.
3.11.Health Education and Behaviour Change Communication (BCC).
3.12.Other National Health Programmes(3)
a. Revised National Tuberculosis Control Programme (RNTCP)
All PHCs to function as DOTS Centres to deliver treatment through DOTS providers and
treatment of common complications of TB and side effects of drugs, record and report on RNTCP
activities. Facility for Collection and transport of sputum samples should be present.
b. National Leprosy Eradication Programme
Diagnosis and management of Leprosy and its complications including reactions. Counselling
for leprosy patients for regularity/completion of treatment and prevention of disability.
c. Integrated Disease Surveillance Project (IDSP): Laboratory services for diagnosis of Malaria,
Tuberculosis, and tests for detection of faecal contamination of water and chlorination level.
d. National Programme for Control of Blindness (NPCB)
i. The early detection of visual impairment and their referral.
ii. Provision of Basic treatment of common eye diseases.
e. National Vector Borne Disease Control Programme (NVBDCP)
i. Diagnosis of Malaria, JE, Kala-azar, and Dengue cases, microscopic confirmation and treatment.
ii. Complete treatment of microfilaria positive cases with DEC and Mass Drug Administration (MDA)
along with management of side reactions, if any.
f. National AIDS Control Programme
i. IEC activities to enhance awareness and preventive measures about STIs and HIV/AIDS.
ii. Organizing School Health Education Programme.
13
iii. Condom Promotion & distribution of condoms to the high risk groups.
iv. Help and guide patients with HIV/AIDS receiving ART with focus on adherence
v. Screening of persons practicing high-risk behaviour and its referral.
g. National Programme for Prevention and Control of Deafness (NPPCD)
h. National Mental Health Programme (NMHP)
i. National Programme for Prevention and Control of Cancer, Diabetes, CVD and Stroke (NPCDCS)
3.13.Referral Services: Appropriate and prompt referral of cases needing specialist care. Appropriate
support to patient during transport to be available.
3.14.Training
a. Imparting training to undergraduate medical students and intern doctors in basic health care.
b. Orientation training of male and female health workers in various National Health Programmes
c. Skill based training to ASHAs.
d. Initial and periodic Training of paramedics in treatment of minor ailments.
e.All health staff of PHC must be trained in IMEP.
3.15. Basic Laboratory and Diagnostic Services
i. Routine urine, stool and blood tests.
ii.Diagnosis of RTI/STDs with wet mounting, Grams stain, etc.
iii.Blood smear examination malarial.
iv.Blood for grouping and Rh typing.
v. Rapid tests for pregnancy.
vi.RPR test for Syphilis surveillance
vii.Rapid test kit for fecal contamination of water.
viii.Estimation of chlorine level
3.16. Monitoring and Supervision
i. Monitoring and supervision of activities of Sub Centre through periodic visits by LHV
ii. Monitoring of all National Health Programmes
iii.Monitoring activities of ASHAs
iv. Health educator will monitor all IEC and BCC activities
v.Health Assistants Male and LHV should visit Sub Centres once a week.
vi.Timely payment of JSY beneficiaries.
vii.Timely payment of TA/DA to ASHAs.
3.17. Functional Linkages with Sub-Centres:
There shall be a monthly review meeting at PHC chaired by MO.Village Health and Nutrition
day at Anganwadi Centres are to be organised under PHC supervision.
14
3.18. Record of Vital Events and Reporting
a. Recording and reporting of Vital statistics including births and deaths.
b. Maintenance of all the relevant records concerning services provided in PHC.
4.Infrastructure and human resource requirement
4.1.Infrastructure:
The PHC should have a building of its own. The surroundings should be clean. It should be centrally
located in an easily accessible area. The area chosen should have facilities for electricity, all weather
road communication, adequate water supply and telephone. There should be 4-6 beds in a Primary
Health Centre. Separate wards should be earmarked for males and females. Labour room should have
New Born care corner. Residential facilities should be available for Medical Officer, nursing staff,
pharmacist, laboratory technician and other staff. Computer with Internet connection should be
provided for Management Information System (MIS) purpose. The transport facilities with assured
referral linkages to be provided.(4)
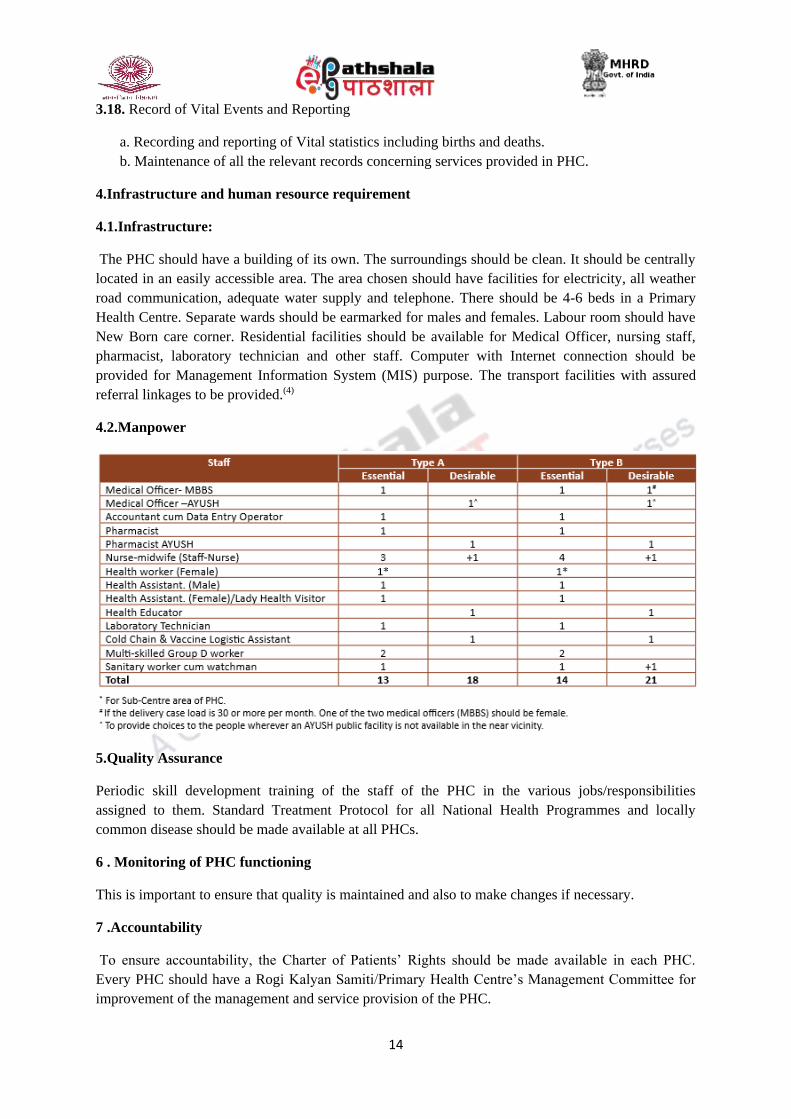
4.2.Manpower
5.Quality Assurance
Periodic skill development training of the staff of the PHC in the various jobs/responsibilities
assigned to them. Standard Treatment Protocol for all National Health Programmes and locally
common disease should be made available at all PHCs.
6 . Monitoring of PHC functioning
This is important to ensure that quality is maintained and also to make changes if necessary.
7 .Accountability
To ensure accountability, the Charter of Patients’ Rights should be made available in each PHC.
Every PHC should have a Rogi Kalyan Samiti/Primary Health Centre’s Management Committee for
improvement of the management and service provision of the PHC.
15
Summary:
Primary Health Centre is the cornerstone of rural health services- a first port of call to a qualified
doctor of the public sector in rural areas for the sick and those who directly report or referred from
Sub-Centres for curative, preventive and promotive health care. A typical Primary Health Centre
covers a population of 20,000 in hilly, tribal, or difficult areas and 30,000 populations in plain areas
with 6 indoor/observation beds. It acts as a referral unit for 6 Sub-Centres and refer out cases to CHC
and higher order public hospitals. Standards are the main driver for continuous improvements in
quality. Currently the IPHS for PHCs has been revised keeping in view the resources available with
respect to functional requirements such as building, manpower, instruments and equipment, drugs and
other facilities etc. The revised IPHS has incorporated the changed protocols of the existing health
programmes and new programmes and initiatives. These standards would also help monitor and
improve the functioning of the PHCs.
References:
1. Govt. Of India(2012) Indian Public Health Standards Guidelines for Primary Health Centres,
Ministry of health and family welfare, New Delhi.
2. Guidelines for Operationalising 24 x 7 PHC 3. (2005) (unpublished), Maternal Health
Division, Department of Family Welfare, Ministry of Health & Family Welfare, Government
of India.
3. RCH Phase II, National Program Implementation 5. Plan (PIP) (2005), Ministry of Health &
Family Welfare, Government of India.
4. Infrastructure Division, Department of Family Welfare; Ministry of Health & Family
Welfare, Government of India.


















