SMARTER BUSINESS. BETTER PATIENT CARE.If you do not want UBM Medica to make your contact information...
59
O PIOID CRISIS How we got here Your role in the solution Policy efforts to fight back Plus DIRECT PRIMARY CARE Physician lessons learned BUNDLED PAYMENTS Pros vs. cons SMARTER BUSINESS. BETTER PATIENT CARE. MedicalEconomics.com JUNE 25, 2016 VOL. 93 NO. 12 COMBAT CYBERATTACKS Simple steps to protect your data
Transcript of SMARTER BUSINESS. BETTER PATIENT CARE.If you do not want UBM Medica to make your contact information...

OPIOIDCRISIS
How we got hereYour role in the solutionPolicy efforts to fi ght back
Plus
DIRECT PRIMARY CARE
Physician lessons learned
BUNDLED PAYMENTS
Pros vs. cons
SMARTER BUSINESS. BETTER PATIENT CARE. MedicalEconomics.com JUNE 25, 2016 VOL. 93 NO. 12
COMBAT
CYBERATTACKS
Simple steps to protect your data

MEDICAL ECONOMICS��]��JUNE 25, 2016 MedicalEconomics.com4
READ MORE INSIDE Legislative efforts to halt the opioid crisis PAGE 38
n March, the CDC released a new guideline for physi-cians prescribing opioids, recommending that doctors try less addic-
tive drugs, such as ibuprofen, before prescribing highly addictive pills and that they only give a few days’ supply in most cases.
Th e recommendations are meant for primary care doctors and do not apply to prescriptions for patients re-ceiving cancer or end-of-life treatment, or to patients who have had surgery. Th ese guidelines come after a growing backlash from some physician groups and organizations who have opposed the practice of opioid prescriptions for routine pain.
Many physicians have prescribed opioids to patients for conditions such as back pain and arthritic pain over the past two decades. Th is came as a result of pharmaceutical companies and some medical experts attesting that opioids could be used to treat common conditions without fear of addiction. Later those claims would be found to be false even though drug companies have profi ted from a $2 billion industry of popularly marketed and sold drugs such as Oxycontin, Percocet and Vicodin.
Th ough some physicians and agen-cies do not support the guideline, the soaring death toll and data supporting the opioid crisis has brought together
many doctors and regulators who were previously on opposite sides of the debate.
Th ough the CDC guideline and other new measures from government regulators such as the Food and Drug Administration (FDA) are targeting physicians, the crisis we are facing has not occurred from physicians overpre-scribing in isolation.
Equally complicit in the crisis have been pharmaceutical companies ad-vertising opioids as safe and not addic-tive, as well as governmental agencies such as the Centers for Medicare & Medicaid Services (CMS) deciding that a patient’s satisfaction score during a hospitalization is as important in re-imbursement as the patient’s survival and whether or not they obtained a hospital-acquired infection.
When part of the patient satisfac-tion score is linked directly to the management of their pain during their hospital stay, there is undeniably
a pressure for physicians to provide opioids to patients even if they feel they may not necessarily need them. Arguably these measures were initiated in legislature years after the culture of treating pain changed in the U.S. medical community as a result of a campaign by the American Pain Society (APS) to treat pain as the “fi fth vital sign.”
Once this new perception of treat-ing pain as a vital sign caught on, orga-nizations such as the Veterans Health Administration and the Joint Commis-sion on Accreditation of Healthcare Or-ganizations began to adopt the slogan and called on physicians to manage patients’ pain.
But just as with any slogan or plan, there must be regulations in place after implementation. Many physicians took “manage pain” to mean “prescribe opioids” and this led to a now billion-dollar industry.
Ultimately, the blame can be placed on many, but the imminent threat to public health that the opioid crisis promises must be addressed now by cooperation between physicians, legislators, pharmaceutical companies and the regulatory boards who oversee them.
Rashmee Patil, MD, is a board-certifi ed internal medicine physician practicing in New York State. How should the United States solve the opioid crisis? Tell us at [email protected].
FIRST TAKE
I
Save blame for later, it’s time to work together to solve the opioid crisis
BY RASHMEE PATIL, MD
“Many physicians took ‘manage pain’ to mean ‘prescribe opioids’ and this led to a now billion-dollar industry.”

MedicalEconomics.com MEDICAL ECONOMICS��]��JUNE 25, 2016 5
Referenced in MedLine®
MEDICAL ECONOMICS (USPS 337-480) (Print ISSN: 0025-7206, Digital ISSN: 2150-7155) is published semimonthly (24
times a year) by UBM Medica, 131 W. First St., Duluth, MN 55802-2065. Subscription rates: one year $95, two years $180 in
the United States & Possessions, $150 for one year in Canada and Mexico, all other countries $150 for one year. Singles copies
(prepaid only): $18 in US, $22 in Canada & Mexico, and $24 in all other countries. Include $6.50 for U.S. shipping and handling.
Periodicals postage paid at Duluth, MN 55806 and at additional mailing offices. Postmaster: Send address changes to Medical
Economics, PO Box 6085, Duluth, MN 55806-6085. Canadian GST Number: R-124213133RT001 Publications Mail Agreement
number 40612608. Return undeliverable Canadian addresses to: IMEX Global Solutions, PO Box 25542 London, ON N6C 6B2
CANADA. Printed in the USA.
© 2016 UBM. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means,
electronic or mechanical including by photocopy, recording, or information storage and retrieval without permission in writing
from the publisher. Authorization to photocopy items for internal/educational or personal use, or the internal/educational or
personal use of specific clients is granted by UBM for libraries and other users registered with the Copyright Clearance Center,
222 Rosewood Dr. Danvers, MA 01923, 978-750-8400 fax 978-646-8700 or visit http://www.copyright.com online. For uses
beyond those listed above, please direct your written request to Permission Dept. fax 440-756-5255 or email: mcannon@
advanstar.com. SMARTER BUSINESS ■ BETTER PATIENT CARE is used pending trademark approval.
UBM Medica provides certain customer contact data (such as customers name, addresses, phone numbers, and e-mail
addresses) to third parties who wish to promote relevant products, services, and other opportunities that may be of interest to
you. If you do not want UBM Medica to make your contact information available to third parties for marketing purposes, simply
call toll-free 866-529-2922 between the hours of 7:30 a.m. and 5 p.m. CST and a customer service representative will assist you
in removing your name from UBM Medica’s lists. Outside the US, please phone 218-740-6477.
Medical Economics does not verify any claims or other information appearing in any of the advertisements contained in the
publication and cannot take responsibility for any losses or other damages incurred by readers in reliance of such content.
Medical Economics cannot be held responsible for the safekeeping or return of unsolicited articles, manuscripts,
photographs, illustrations, or other materials.
Library Access Libraries offer online access to current and back issues of Medical Economics through the EBSCO host
databases.
To subscribe, call toll-free 888-527-7008. Outside the U.S., call
218-740-6477.
THE LAST WORD
PAGE 59
The rise of direct payComprehensive primary care improves patients’ health, and the best way to provide that may be direct primary care, writes Joseph E. Scherger, MD
IN EVERY ISSUE
6 Interactive
9 Your voice
14 Our advisers
16 Vitals
58 Advertiser index
38 Opioid reform efforts in DC Physicians want to ensure they retain
treatment decision-making power
39 Practice succession planning Making the transition successful
requires proper planning
41 Coding insights Defining active patient management
when billing incident-to
43 The threat of cyberattacks As the danger grows, physicians must
understand how to safeguard records
48 Dismissing problem patients There’s a right way and a wrong way to
remove patients from your practice
49 Bundled payments A payment model of the future
provides risks and rewards for doctors
54 Physician-led ACOs Accountable care organizations
succeed when doctors are in charge
The opioid crisisHow we got here and doctors’ role in the solution
PAGE 28
VOLUME 93 ISSUE 12JUNE 25, 2016

MEDICAL ECONOMICS ❚ JUNE 25, 2016 MedicalEconomics.com6
TWITTER TALK
FOLLOW US ON TWITTER TO RECEIVE THE LATEST NEWS AND PARTICIPATE IN THE DISCUSSION.
WWW.MEDICALECONOMICS.COMINTERACTIVE
Kelly Collins, MD, often hears patients venting about high
copays and insurance denials. “A lot of my patients are
struggling,” says Collins, who runs a solo family practice in
Bellevue, Nebraska. Collins is not alone. A large portion of the
145 physicians who responded to an exclusive Medical
Economics poll reported that they are seeing greater numbers
of angry patients these days. bit.ly/angrypatients
How anger is fraying the doctor-patient relationship
TOP HEADLINES NOW
HIPAA resouce center
The latest on how to keep your practice compliant
with federal privacy and security rules
MedicalEconomics.com/tag/hipaa-resource-center
HIPAA AUDITS
Here’s our 7 best tips for doctors to
prepare for the 2016 HIPAA audits:
http://buff.ly/1LRi2iU
LEADERSHIP
How can doctors take on leadership
positions in today’s challenging
healthcare environment?
http://ow.ly/U0tJE
CODING
#coding can make or break your
medical practice. Follow these steps
to hire the right person.
http://ow.ly/NS1iQ
HIGH DEDUCTIBLES
Why physicians must adjust how they
practice
http://buff.ly/1QJWgun
HEALTH IT
Silicon Valley’s vision to transform
healthcare #google #technology
http://buff.ly/1nuKs6J
MOC
MOC, recertifications are ‘cancers’
doctors should rally against via @
hlgreenberg
http://buff.ly/1QAmCkE
@MedEconomics
Medical Economics is part of the ModernMedicine Network, a Web-based portal for health professionals offering best-in-class content and tools in a
rewarding and easy-to-use environment for knowledge-sharing among members of our community.
PA R T O F T H E
MedicalEconomics.com
FACEBOOK.COM/MEDICALECONOMICS @MEDECONOMICS
HIPAA mistakes
10 common practice errors you must avoid,
and how to improve your data security
bit.ly/hipaamistakes
EHRs and malpractice
How to avoid a lawsuit related to your
electronic health record system
http://bit.ly/EHRlawsuit
Quality metrics
Why doctors, not data, must drive the
future of healthcare
bit.ly/morethanmetrics
The fight over patient records
The struggle for ownership in a time of
technology and patient choice
http://bit.ly/recordownership

One TestA simple blood test that may make IBS no longer just a diagnosis of exclusion
One AnswerProprietary ELISA test based on 2 validated biomarkers—anti-CdtB and anti-vinculin
In One DayTM
Results are reported to the healthcare provider within 24 hours after specimen receipt
For more information on IBSchek:Visit IBSchek.com
Call 1-877-IBS-CHEK (427-2435)
IBSchek™ may simplify the path to a...
IBSchek is the only quick and reliable blood test for the diagnosis of IBS.
©2016 Commonwealth Laboratories, LLC.39 Norman Street Salem, MA 01970 CWI15039 F-409 Rev:B
Now you can order IBSchek through
in over 2000 sites across the US
TM

MEDICAL ECONOMICS��]��JUNE 25, 2016 MedicalEconomics.com8
SOURCES GUIDE TO THE ACTIVITY OF YOUR COLLEAGUES IN THIS ISSUE
“It’s become the shortest path to money for crooks.”RICK KAM, PRESIDENT, ID EXPERTS
READ ABOUT CYBER ATTACKS ON PAGE 43
52%of physicians say patients are to blame for the increasing use of opioids, according to an exclusive survey
READ ABOUT THE OPIOID CRISIS ON PAGE 28
“I’m definitely happier now because I can be the kind of physician I want to be.”JULIE GUNTHER, MD, BOISE, IDAHO
READ MORE ABOUT DIRECT PAY ON PAGE 18
Customer service 877-922-2022
Editorial 800-225-4569
Advertising 732-596-0276
Classifieds 800-225-4569
Back Issues 218-740-6477
Reprints 877-652-5295, ext. 121
Subscription Correspondence Medical Economics, P.O. Box 6085, Duluth, MN 55806-6085
CONTENT
SARA MICHAELVP, Content & Strategy
GEORGE G. ELLIS JR., MD, FACPChief Medical Adviser
KEITH L. MARTINContent Channel Director203-523-7112 / [email protected]
JEFFREY BENDIX, MASenior Editor440-891-2684 / [email protected]
CHRIS MAZZOLINI, MS Content Manager440-891-2797 / [email protected]
ROSE SCHNEIDERContent Specialist440-891-2707 / [email protected]
ERICA SPREY Associate Editor203-523-7118 / [email protected]
DESIGN
NANCY BITTEKER Director, Design and Digital Production
ROBERT McGARR Group Art Director
PRODUCTION
KAREN LENZENProduction Director
AUDIENCE DEVELOPMENT
JOY PUZZOVP, Marketing & Audience Development
CHRISTINE SHAPPELLDirector, Audience Development
WENDY BONGAudience Development Manager218-740-7244 / [email protected]
PUBLISHING & SALES
GEORGIANN DeCENZOExecutive Vice President, Managing Director
KEN SYLVIAVice President, Group Publisher
ERIC TEMPLE-MORRISPublisher503-203-1060 / [email protected]
ANA SANTISOAssociate Publisher732-346-3032 / [email protected]
MONIQUE MICHOWSKINational Account Manager732-346-3098 / [email protected]
DAVID DePINHOStrategic Content Solutions Director732-346-3053 / [email protected]
JOHN CURRIDNational Sales Manager212-600-3134 / [email protected]
TOD McCLOSKEYSales Manager Classified/Display Advertising440-891-2739 / [email protected]
JOANNA SHIPPOLIAccount Manager, Recruitment Advertising440-891-2615 / [email protected]
RENÉE SCHUSTERList Account Executive440-891-2613 / [email protected]
MAUREEN CANNONPermissions440-891-2742 / [email protected]
SARAH CAMERON MIFSUD VP, Digital Solutions
DANIEL ADAMSAccount Director, Digital Solutions203-252-0937 / [email protected]
ALEX CALAccount Director, Digital Solutions203-523-7042 / [email protected]
TERRY TETZLAFFDigital Traffic Coordinator
DAVID DONOVANVP, Digital Products
AMANDA ROMBACHAssociate Director, Custom Solutions
MEG BENSONSpecial Projects Director
AMY ERDMANVP, Marketing
GAIL KAYEDirector of Marketing & Research Services
REPRINTS877-652-5295 ext. 121 / [email protected] Outside US, UK, direct dial: 281-419-5725. Ext. 121

MedicalEconomics.com MEDICAL ECONOMICS��]��JUNE 25, 2016 9
YOUR VOICE Have a comment? SEND YOUR THOUGHTS TO [email protected]
FACEBOOK.COM/MEDICALECONOMICS @MEDECONOMICS
e were all taught in medi-cal school that the way to treat and control disease is to identify the cause. No control is possible un-
less identification occurs.This also applies to the social sci-
ences. In order to control defensive medicine, we must first identify the root cause.
Contrary to the innuendos in the article, “Defensive medicine vs. value-based care (Medical Econom-ics, March 25, 2015),” the root cause is not doctors: i.e. bad records, bad EMR, physician sloth or stupidity. The root cause is that defensive medicine is driven by lawyers who file endless meritless and frivolous lawsuits.
Why do they do this? Because there is little financial risk in doing so.
Especially if many suits can be settled pretrial. The American Rule in turn drives this practice of champerty and barratry—each party is responsible for its own attorney’s fees. The rule protects the plaintiff lawyer from financial penalty.
On the other hand, the rest of the industrialized planet uses the English Rule—the losing party pays the prevailing party’s attorneys’ fees. This English rule forces plaintiff lawyers to reconsider who and what they sue.
Richard Anderson is correct—the solution is not medical reform but tort reform. This will not be accomplished by caps on damages, safe harbors, no blame compensation laws etc. Defen-sive medicine will only be contained by tort reform—replacement of the American Rule by a loser pays system.
Any other tort reform is a Band-Aid. Plaintiff lawyers should at least be subject to similar financial risk as other professionals. It is no accident that the U.S., with 5% of the planet’s population, employs 75% of the plan-ets lawyers.
It’s called jackpot justice and not only drives defensive medicine, it causes unnecessary duplicate and defensive practice by virtually all-personal and business activity in the country.
We are all held hostage to the American Rule. Because of the English rule, doctors in my native Canada pay 60% less for malpractice insurance.
Calvin S. Ennis, MDPASCAGOULA, MISSISSIPPI
W
Certification should be as untouchable as a PhDOne of the biggest lessons that I got after reading “Maintenance of certification:
inside the physician revolt (Medical Economics, March 25, 2016)” is how even within
the ‘house of medicine,’ physicians have to remain vigilant.
Besides insurance companies and malpractice lawyers, there are many forces
such as the ABSM each with their own special ambitions and desires to extend their
influence over doctors.
For medicine enters into just about every segment of our lives. And in our
capitalistic culture, there are always those industries with the capability and strength
to look for new area of profit—pharmaceutical companies and makers of medical
instruments immediately come to mind.
The ABMS would do well to do away with their punitive approach and provide
self-assessment tests with answer booklets for doctors in their various specialties.
Initial certification should be as untouchable as a Bachelor of Arts or PhD degree.
Edward Volpintesta, MDBETHEL, CONNECTICUT
Tort reform necessary to solve defensive medicine
Be honest with patients about antibioticsIn reference to the article, “When you ignore
a patient’s cry for antibiotics” (Physicians
Practice/Medical Economics, April 10,
2016),” I agree with everything Dr. Frank said
except this: Instead of telling the patient that
they don’t NEED antibiotics, I tell them that
antibiotics won’t HELP.
Patients think they need anything that could
possibly help, but if I can convince them that
antibiotics won’t, they are more willing to let it
go. Of course I offer symptomatic relief to be
sure they know do want them to get better.
Janis Eiler, MDCINCINNATI, OHIO

MEDICAL ECONOMICS ❚ JUNE 25, 2016 MedicalEconomics.com14
OUR ADVISERS HAVE A QUESTION FOR OUR ADVISERS? [email protected]
EDITORIAL CONSULTANTS
PRACTICE MANAGEMENT
Judy Beewww.ppgconsulting.com
La Jolla, CA
Keith Borglum, CHBCProfessional Management and Marketing
Santa Rosa, CA
Kenneth Bowden, CHBCBerkshire Professional Management
Pittsfi eld, MA
Michael D. Brown, CHBCHealth Care Economics Indianapolis, IN
Frank Cohen, MPAwww.frankcohengroup.com
Clearwater, FL
Virginia Martin, CMA, CPC, CHCO, CHBCHealthcare Consulting Associates
of N.W. Ohio Inc. Waterville, OH
Rosemarie NelsonMGMA Healthcare Consultant Syracuse, NY
Mark D. Scroggins, CPA, CHBCClayton L. Scroggins Associates Inc.
Cincinnati, OH
Gray Tuttle Jr., CHBCThe Rehmann Group Lansing, MI
Michael J. Wiley, CHBCHealthcare Management
and Consulting Services Bay Shore, NY
H. Christopher Zaenger, CHBCZ Management Group Barrington, IL
Karen ZupkoKaren Zupko & Associates Chicago, IL
TAXES & PERSONAL FINANCE
Lewis J. Altfest, CFP, CPAAltfest Personal Wealth Management
New York City
Robert G. Baldassari, CPAMatthews, Carter and Boyce Fairfax, VA
Todd D. Bramson, CFPNorth Star Resource Group Madison, WI
Glenn S. Daily, CFPInsurance consultant New York City
Barry Oliver, CPA, PFSThomas, Wirig, Doll & Co.
Capital Performance Advisors
Walnut Creek, CA
Gary H. Schatsky, JDIFC Personal Money Managers New York City
David J. Schiller, JDSchiller Law Associates Norristown, PA
Edward A. Slott, CPAE. Slott & Co. Rockville Centre, NY
HEALTH LAW & MALPRACTICE
Barry B. Cepelewicz, MD, JDGarfunkel Wild, PC Stamford, CT
John M. Fitzpatrick, JDWheeler Trigg Kennedy, LLP Denver, CO
Alice G. Gosfi eld, JDAlice G. Gosfi eld and Associates
Philadelphia, PA
James Lewis Griffi th Sr., JDFox Rothschild Philadelphia, PA
Lee J. Johnson, JDMount Kisco, NY
Lawrence W. Vernaglia, JD, MPHFoley & Lardner, LLP Boston, MA
The board members and consultants contribute expertise and analysis that help shape the content of Medical Economics.
Mary Ann Bauman, MDInternal MedicineOklahoma City, OK
John L. Bender, MD, MBAFamily MedicineFt. Collins, CO
Maria Y. Chandler, MD, MBABusiness of Medicine, PediatricsIrvine, CA
George G. Ellis Jr., MDInternal MedicineYoungstown, OH
David C. Judge, MDInternal MedicineCambridge, MA
Jeffrey M. Kagan, MDInternal MedicineNewington, CT
Melissa Lucarelli, MDFamily MedicineRandolph, WI
Elizabeth A. Pector, MDFamily MedicineNaperville, IL
Kenneth R. Kubitschek, MDInternal MedicineAsheville, NC
Joseph E. Scherger, MDFamily MedicineLa Quinta, CA
Salvatore S. Volpe, MDInternal Medicine-PediatricsStaten Island, NY

Enter today! MedicalEconomics.com/2016-physician-writing-contestSee link above ror complete rules and regulation.
PHYSICIAN WRITING CONTEST CALL FOR ENTRIES
MAKING TIME FOR PATIENTSBetween stagnant reimbursements, ever-shifting mandates,
hectic schedules and the everyday challenges of running a
practice, you have a lot on your plate. What’s more, you are
expected to make and keep solid relationships with patients
during their brief—and usually infrequent—visits to your offi ce.
How are you preserving valuable ties to your patients to truly
address their care needs amid all your other priorities?
Share with your peers in our latest Physician Writing Contest.
DEADLINE 11:59 P.M. EDT, FRIDAY, JULY 15
PRIZES 1st place $1,000 2nd place $500 3rd place $250

MEDICAL ECONOMICS��]��JUNE 25, 2016 MedicalEconomics.com16
The rate of American adults who
smoke fell to 15% last year—the
biggest one-year decline in more
than 20 years, according to a new
Center for Disease Control and
Prevention (CDC) report.
The rate had previously fallen
2% from 2014, when about 17% of
adults in a large national survey said
they had recently smoked.
While the smoking rate has been
declining for decades, it usually
drops only 1 point or less in a year,
writes Boston.com.
The last time there was a large
decline was from 1992 to 1993,
when the smoking rate fell 1.5%,
Brain King, of the CDC, told the
website.
Why the rate has declined so
rapidly in 2015, and whether it will
happen again, is not so transparent.
“Experts attribute recent
declines to the mounting impact
of anti-smoking advertising
campaigns, cigarette taxes and
smoking bans,” writes the website.
The increased marketing of
electronic cigarettes, as well as
their growing popularity, has also
played a likely role. Nevertheless, it
has not been made clear whether
this will help further decrease
American smokers, or contribute to
an increase.
Several CDC surveys have shown
a boom in e-cigarette use among
teenagers, and health officials have
said they are fearful many of these
children will get hooked on nicotine
and become smokers later in life.
Regardless, health officials are
optimistic, in part due to regulators
turning their attention to the
potential dangers of e-cigarettes.
U.S. adult smoking rate falling fastStudy finds most physicians
support cost-consciousness in medicine
There is limited knowledge regard-ing physicians’ views on health ser-vice overuse or their awareness of the American Board of Internal Medicine (ABIM) Foundation’s Choosing Wisely campaign.
A recent study conducted by the American Journal of Managed Care set out to change this and found that while primary care physicians were more aware of the campaign than special-ists, most doctors supported cost-con-sciousness in medicine and embrace
their responsibility in reducing costs. “The overuse of healthcare servic-
es is receiving attention as physicians are increasingly asked to embrace financial stewardship and payment reform pushes provider groups to consider value,” the study’s authors wrote. “In the past, there was little agreement on classification of servic-es as low-value and no consensus on which mechanisms were most effec-tive in reducing the use of these low-value services.”
VitalsTHE
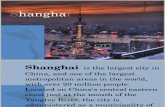
Primary care physician opinions
Cost control & treatment overuseA survey of primary care physicians shows they are increasingly engaged
with efforts to contain healthcare costs.
Source: The American Journal of Managed Care
Physicians should be aware of/ adhere to clinical guidelines
Doctors need to limit unnecessary tests
Physicians have a responsibility to control costs
Statement
Doctors are too busy to worry about costs
Physicians across specialties are likeminded in their commitment
to reducing unnecessary treatments
Cost is only important for out-of-pocket
98.2%
Percentage that agree
97.7%
93.6%
30.5%
17.6%
8.7%

TO DATE 1
*
8 MILLIO
N
PRESCRIPTIO
NS
MO
RE THAN
Please see additional Important Safety Information and brief summary
of full Prescribing Information on the following pages.
IMPORTANT SAFETY INFORMATION CONTRAINDICATIONS
>> History of a serious hypersensitivity reaction to INVOKANA®
>> Severe renal impairment (eGFR <30 mL/min/1.73 m2), end-stage renal
disease, or patients on dialysis
INVOKANA® is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus.
INVOKANA® is not recommended in patients with type 1 diabetes or for the treatment of diabetic ketoacidosis.
* Data on fi le. Based on TRx data sourced from IMS NPA Database, weekly data through 4/8/16.
In the treatment of type 2 diabetes, along with diet and exercise, INVOKANA® can
AWAKEN A TRANSFORMATION

INVOKANA® 300 mg + metformin and a sulfonylurea (n=377)
Januvia® (sitagliptin) 100 mg + metformin and a sulfonylurea (n=378)
–0.66
–1.03
8.13% 8.12%Mean baseline:
Adjusted Mean Change in A1C From Baseline at 52 Weeks (%)2
INVOKANA® starting dose: 100 mg once daily. In patients tolerating the starting dose who have an eGFR ≥60 mL/min/1.73 m2 and require
additional glycemic control, the dose can be increased to 300 mg once daily.2
Indicated trademarks are registered trademarks of their respective owners.
IMPORTANT SAFETY INFORMATION (cont’d)
WARNINGS and PRECAUTIONS >> Hypotension: INVOKANA® causes intravascular volume contraction. Symptomatic hypotension can occur after initiating INVOKANA®,
particularly in patients with impaired renal function (eGFR <60 mL/min/1.73 m2), elderly patients, patients on either diuretics or medications that
interfere with the renin-angiotensin-aldosterone system, or patients with low systolic blood pressure. Before initiating in patients with ≥1 of these
characteristics, volume status should be assessed and corrected. Monitor for signs and symptoms after initiating.
>> INVOKANA® 300 mg difference from Januvia® 100 mg: –0.37% (95% CI: –0.50, –0.25; P<0.05)
>> In a prespecified analysis, superiority was determined once noninferiority was confirmed3*
INVOKANA® 300 mg demonstrated superior reductions in A1C,*
body weight,† and systolic blood pressure (BP)† vs Januvia® 100 mg2,3
AWAKEN A TRANSFORMATION
In the treatment of type 2 diabetes, along with diet and exercise, INVOKANA® can
Prespecified
secondary
endpoints:
Adjusted mean change in body weight from baseline at 52 weeks2:
>> Difference from Januvia®: –2.8% (–5.3 lb)
(95% CI: –3.3, –2.2; P<0.001)
Adjusted mean change in systolic BP from baseline at 52 weeks3:
>> Difference from Januvia®: –5.9 mm Hg
(95% CI: –7.6, –4.2; P<0.001)

Similar Rate of Hypoglycemia and Overall Tolerability Profile to Januvia®2-4§
Superior Reductions vs Januvia®2,3‡>> A1C*
>> Body weight†>> Systolic BP†
Preferred Coverage for Most Commercial and Medicare Part D Patients1
Please see additional Important Safety Information and brief summary of full Prescribing Information on the following pages.
Learn more and register for updates at
INVOKANAhcp.com
Incidence of any AE, Januvia® 100 mg: 77.5%; INVOKANA® 300 mg: 76.7%
Incidences of specific AEs were similar between groups, except for:
Male/female genital mycotic infection, Januvia® 100 mg: 0.5%/4.3%; INVOKANA® 300 mg: 9.2%/15.3%
Similar overall incidence of AEs vs Januvia®3
A randomized, double-blind, active-controlled 52-week study of 755 patients with type 2 diabetes who were inadequately controlled on maximally or
near-maximally effective doses of metformin (≥2000 mg/day, or ≥1500 mg/day if higher dose not tolerated) and a sulfonylurea. The primary endpoint
was the change in A1C from baseline to week 52.2,3
>> Ketoacidosis: Reports of ketoacidosis, a serious life-threatening condition requiring urgent hospitalization, have been identified in patients with type
1 and 2 diabetes mellitus receiving SGLT2 inhibitors, including INVOKANA®. Before initiating INVOKANA®, consider factors in patient history that may
predispose to ketoacidosis, including pancreatic insulin deficiency, caloric restriction disorders, and alcohol abuse. In patients treated with INVOKANA®,
consider monitoring for ketoacidosis and temporarily discontinuing in clinical situations known to predispose to ketoacidosis (eg, prolonged fasting due
to acute illness or surgery).
>> Impairment in Renal Function: INVOKANA® increases serum creatinine and decreases eGFR. Patients with hypovolemia may be more susceptible
to these changes. Renal function abnormalities can occur after initiation. More frequent renal function monitoring is recommended in patients
with an eGFR <60 mL/min/1.73 m2.
>> Hyperkalemia: INVOKANA® can lead to hyperkalemia. Patients with moderate renal impairment who are taking medications that interfere with potassium
excretion or medications that interfere with the renin-angiotensin-aldosterone system are more likely to develop hyperkalemia. Monitor serum potassium
levels periodically in patients with impaired renal function and in patients predisposed to hyperkalemia due to medications or other medical conditions.
* Noninferiority of INVOKANA® + metformin and a sulfonylurea to Januvia® + metformin and a sulfonylurea was assessed based on a prespecified margin of 0.3% for the upper limit of the 2-sided 95% CI for the comparison in the primary last observation carried forward analysis. If noninferiority was demonstrated, then superiority was assessed, as determined by an upper bound of the 95% CI around the between-group difference (INVOKANA® minus Januvia®) of <0.0%.3
† Prespecified secondary endpoint. INVOKANA® is not indicated for weight loss or as an antihypertensive treatment.
‡ INVOKANA® 300 mg vs Januvia® 100 mg.
§ Similar overall incidence of adverse events vs Januvia® 100 mg across multiple studies.3,4

Canagliflozin is licensed from Mitsubishi Tanabe Pharma Corporation.
Janssen Pharmaceuticals, Inc.
© Janssen Pharmaceuticals, Inc. 2016 May 2016 048359-160504
IMPORTANT SAFETY INFORMATION (cont’d)
>> Urosepsis and Pyelonephritis: There have been reports of serious
urinary tract infections, including urosepsis and pyelonephritis,
requiring hospitalization in patients receiving SGLT2 inhibitors, including
INVOKANA®. Treatment with SGLT2 inhibitors increases this risk. Evaluate
patients for signs and symptoms and treat promptly.
>> Hypoglycemia With Concomitant Use With Insulin and Insulin
Secretagogues: INVOKANA® can increase the risk of hypoglycemia when
combined with insulin or an insulin secretagogue. A lower dose of insulin or
insulin secretagogue may be required to minimize the risk of hypoglycemia
when used in combination with INVOKANA®.
>> Genital Mycotic Infections: INVOKANA® increases risk of genital mycotic
infections. Patients with history of these infections and uncircumcised
males were more likely to develop these infections. Monitor and treat
appropriately.
>> Hypersensitivity Reactions: Hypersensitivity reactions (eg, generalized
urticaria), some serious, were reported with INVOKANA®; these reactions
generally occurred within hours to days after initiation. If reactions occur,
discontinue INVOKANA®, treat per standard of care, and monitor until signs
and symptoms resolve.
>> Bone Fracture: Increased risk of bone fracture, occurring as early as
12 weeks after treatment initiation, was observed in patients using
INVOKANA®. Consider factors that contribute to fracture risk prior to
initiating INVOKANA®.
>> Increases in Low-Density Lipoprotein (LDL-C): Dose-related increases in
LDL-C can occur with INVOKANA®. Monitor LDL-C and treat per standard
of care after initiating.
>> Macrovascular Outcomes: There have been no clinical studies
establishing conclusive evidence of macrovascular risk reduction
with INVOKANA® or any other antidiabetic drug.
DRUG INTERACTIONS
>> UGT Enzyme Inducers: Rifampin: Co-administration of INVOKANA® with
rifampin decreased INVOKANA® area under the curve (AUC) by 51% and
therefore may decrease efficacy. If an inducer of UGT enzymes must be
co-administered with INVOKANA®, consider increasing the dose to
300 mg once daily if patients are currently tolerating INVOKANA® 100 mg
once daily, have an eGFR ≥60 mL/min/1.73 m2, and require additional
glycemic control. Consider other antihyperglycemic therapy in patients
with an eGFR <60 mL/min/1.73 m2 who require additional glycemic control.
>> Digoxin: There was an increase in the AUC and mean peak drug
concentration of digoxin (20% and 36%, respectively) when
co-administered with INVOKANA® 300 mg. Monitor appropriately.
>> Positive Urine Glucose Test: Monitoring glycemic control with urine
glucose tests is not recommended in patients taking SGLT2 inhibitors
as SGLT2 inhibitors increase urinary glucose excretion and will lead to
positive urine glucose test results. Use alternative methods to monitor
glycemic control.
>> Interference With 1,5-Anhydroglucitol (1,5-AG) Assay: Monitoring
glycemic control with 1,5-AG assay is not recommended as measurements
of 1,5-AG are unreliable in assessing glycemic control in patients taking
SGLT2 inhibitors. Use alternative methods to monitor glycemic control.
USE IN SPECIFIC POPULATIONS
>> Pregnancy Category C: There are no adequate and well-controlled
studies of INVOKANA® in pregnant women. During pregnancy, consider
appropriate alternative therapies, especially during the second and third
trimesters.
>> Nursing Mothers: It is not known if INVOKANA® is excreted in human milk.
Because of the potential for serious adverse reactions in nursing infants,
discontinue INVOKANA®.
References: 1. Data on file. Janssen Pharmaceuticals, Inc., Titusville,
NJ. 2. INVOKANA® [prescribing information]. Titusville, NJ: Janssen
Pharmaceuticals, Inc. 3. Schernthaner G, Gross JL, Rosenstock J,
et al. Canagliflozin compared with sitagliptin for patients with
type 2 diabetes who do not have adequate glycemic control with
metformin plus sulfonylurea: a 52-week randomized trial [published
correction appears in Diabetes Care. 2013;36(12):4172]. Diabetes Care.
2013;36(9):2508-2515. 4. Lavalle-González FJ, Januszewicz A, Davidson J,
et al. Efficacy and safety of canagliflozin compared with placebo and
sitagliptin in patients with type 2 diabetes on background metformin
monotherapy: a randomised trial. Diabetologia. 2013;56:2582-2592.
Supplemental tables available at: http://link.springer.com/article/
10.1007%2Fs00125-013-3039-1. Accessed November 16, 2015.
>> Pediatric Use: Safety and effectiveness in patients <18 years of age have
not been established.
>> Geriatric Use: 2034 patients ≥65 years and 345 patients ≥75 years were
exposed to INVOKANA® in 9 clinical studies. Patients ≥65 years had a higher
incidence of adverse reactions related to reduced intravascular volume (eg,
hypotension, postural dizziness, orthostatic hypotension, syncope, and
dehydration), particularly with the 300-mg dose, compared to younger
patients; more prominent increase in the incidence was seen in patients
who were ≥75 years. Smaller reductions in HbA1c relative to placebo were
seen in patients ≥65 years (‒0.61% with INVOKANA® 100 mg and ‒0.74%
with INVOKANA® 300 mg) compared to younger patients (‒0.72% with
INVOKANA® 100 mg and ‒0.87% with INVOKANA® 300 mg).
>> Renal Impairment: Efficacy and safety were evaluated in a study
that included patients with moderate renal impairment (eGFR 30 to
<50 mL/min/1.73 m2). These patients had less overall glycemic efficacy and
a higher occurrence of adverse reactions related to reduced intravascular
volume, renal-related adverse reactions, and decreases in eGFR compared
to patients with mild renal impairment or normal renal function (eGFR
≥60 mL/min/1.73 m2); patients treated with 300 mg were more likely to
experience increases in potassium. INVOKANA® is not recommended in
patients with severe renal impairment (eGFR <30 mL/min/1.73 m2), with
end-stage renal disease, or receiving dialysis.
>> Hepatic Impairment: INVOKANA® has not been studied in patients with
severe hepatic impairment and is not recommended in this population.
OVERDOSAGE
>> In the event of an overdose, contact the Poison Control Center and employ
the usual supportive measures, eg, remove unabsorbed material from the
gastrointestinal tract, employ clinical monitoring, and institute supportive
treatment as needed.
ADVERSE REACTIONS
>> The most common adverse reactions associated with INVOKANA® (5%
or greater incidence) were female genital mycotic infections, urinary tract
infections, and increased urination.
Please see brief summary of full Prescribing Information at right and
on the following pages.
04
433
4-1
5120
7

INVOKANA®
(canagliflozin) tablets, for oral use Brief Summary of Prescribing Information.
INDICATIONS AND USAGEINVOKANA® (canagliflozin) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus [see Clinical Studies (14) in full Prescribing Information].
Limitation of Use: INVOKANA is not recommended in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis.
CONTRAINDICATIONS• History of a serious hypersensitivity reaction to INVOKANA, such as
anaphylaxis or angioedema [see Warnings and Precautions and Adverse Reactions].
• Severe renal impairment (eGFR less than 30 mL/min/1.73 m2), end stage renal disease (ESRD), or patients on dialysis [see Warnings and Precautions and Use in Specific Populations].
WARNINGS AND PRECAUTIONSHypotension: INVOKANA causes intravascular volume contraction. Symptomatic hypotension can occur after initiating INVOKANA [see Adverse Reactions] particularly in patients with impaired renal function (eGFR less than 60 mL/min/1.73 m2), elderly patients, patients on either diuretics or medications that interfere with the renin-angiotensin-aldosterone system (e.g., angiotensin-converting-enzyme [ACE] inhibitors, angiotensin receptor blockers [ARBs]), or patients with low systolic blood pressure. Before initiating INVOKANA in patients with one or more of these characteristics, volume status should be assessed and corrected. Monitor for signs and symptoms after initiating therapy.
Ketoacidosis: Reports of ketoacidosis, a serious life-threatening condition requiring urgent hospitalization have been identified in postmarketing surveillance in patients with type 1 and type 2 diabetes mellitus receiving sodium glucose co-transporter-2 (SGLT2) inhibitors, including INVOKANA. INVOKANA is not indicated for the treatment of patients with type 1 diabetes mellitus [see Indications and Usage].
Patients treated with INVOKANA who present with signs and symptoms consistent with severe metabolic acidosis should be assessed for ketoacidosis regardless of presenting blood glucose levels, as ketoacidosis associated with INVOKANA may be present even if blood glucose levels are less than 250 mg/dL. If ketoacidosis is suspected, INVOKANA should be discontinued, patient should be evaluated, and prompt treatment should be instituted. Treatment of ketoacidosis may require insulin, fluid and carbohydrate replacement.
In many of the postmarketing reports, and particularly in patients with type 1 diabetes, the presence of ketoacidosis was not immediately recognized and institution of treatment was delayed because presenting blood glucose levels were below those typically expected for diabetic ketoacidosis (often less than 250 mg/dL). Signs and symptoms at presentation were consistent with dehydration and severe metabolic acidosis and included nausea, vomiting, abdominal pain, generalized malaise, and shortness of breath. In some but not all cases, factors predisposing to ketoacidosis such as insulin dose reduction, acute febrile illness, reduced caloric intake due to illness or surgery, pancreatic disorders suggesting insulin deficiency (e.g., type 1 diabetes, history of pancreatitis or pancreatic surgery), and alcohol abuse were identified.
Before initiating INVOKANA, consider factors in the patient history that may predispose to ketoacidosis including pancreatic insulin deficiency from any cause, caloric restriction, and alcohol abuse. In patients treated with INVOKANA consider monitoring for ketoacidosis and temporarily discontinuing INVOKANA in clinical situations known to predispose to ketoacidosis (e.g., prolonged fasting due to acute illness or surgery).
Impairment in Renal Function: INVOKANA increases serum creatinine and decreases eGFR. Patients with hypovolemia may be more susceptible to these changes. Renal function abnormalities can occur after initiating INVOKANA [see Contraindications and Adverse Reactions]. More frequent renal function monitoring is recommended in patients with an eGFR below 60 mL/min/1.73 m2.
Hyperkalemia: INVOKANA can lead to hyperkalemia. Patients with moderate renal impairment who are taking medications that interfere with potassium excretion, such as potassium-sparing diuretics, or medications that interfere with the renin-angiotensin-aldosterone system are at an increased risk of developing hyperkalemia [see Dosage and Administration (2.2) in full Prescribing Information and Adverse Reactions].
Monitor serum potassium levels periodically after initiating INVOKANA in patients with impaired renal function and in patients predisposed to hyperkalemia due to medications or other medical conditions.
Urosepsis and Pyelonephritis: There have been postmarketing reports of serious urinary tract infections including urosepsis and pyelonephritis requiring hospitalization in patients receiving SGLT2 inhibitors, including INVOKANA. Treatment with SGLT2 inhibitors increases the risk for urinary tract infections. Evaluate patients for signs and symptoms of urinary tract infections and treat promptly, if indicated [see Adverse Reactions].
Hypoglycemia with Concomitant Use with Insulin and Insulin Secretagogues: Insulin and insulin secretagogues are known to cause hypoglycemia. INVOKANA can increase the risk of hypoglycemia when combined with insulin or an insulin secretagogue [see Adverse Reactions]. Therefore, a lower dose of insulin or insulin secretagogue may be required to minimize the risk of hypoglycemia when used in combination with INVOKANA.
Genital Mycotic Infections: INVOKANA increases the risk of genital mycotic infections. Patients with a history of genital mycotic infections and uncircumcised males were more likely to develop genital mycotic infections [see Adverse Reactions]. Monitor and treat appropriately.
Hypersensitivity Reactions: Hypersensitivity reactions, including angioedema and anaphylaxis, have been reported with INVOKANA. These reactions generally occurred within hours to days after initiating INVOKANA. If hypersensitivity reactions occur, discontinue use of INVOKANA; treat and monitor until signs and symptoms resolve [see Contraindications and Adverse Reactions].
Bone Fracture: An increased risk of bone fracture, occurring as early as 12 weeks after treatment initiation, was observed in patients using INVOKANA. Consider factors that contribute to fracture risk prior to initiating INVOKANA [see Adverse Reactions].
Increases in Low-Density Lipoprotein (LDL-C): Dose-related increases in LDL-C occur with INVOKANA [see Adverse Reactions]. Monitor LDL-C and treat if appropriate after initiating INVOKANA.
Macrovascular Outcomes: There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with INVOKANA or any other antidiabetic drug.
ADVERSE REACTIONSThe following important adverse reactions are described below and elsewhere in the labeling:
• Hypotension [see Warnings and Precautions]
• Ketoacidosis [see Warnings and Precautions]
• Impairment in Renal Function [see Warnings and Precautions]
• Hyperkalemia [see Warnings and Precautions]
• Urosepsis and Pyelonephritis [see Warnings and Precautions]
• Hypoglycemia with Concomitant Use with Insulin and Insulin Secretagogues [see Warnings and Precautions]
• Genital Mycotic Infections [see Warnings and Precautions]
• Hypersensitivity Reactions [see Warnings and Precautions]
• Bone Fracture [see Warnings and Precautions]
• Increases in Low-Density Lipoprotein (LDL-C) [see Warnings and Precautions]
Clinical Studies Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to the rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Pool of Placebo-Controlled Trials: The data in Table 1 is derived from four 26-week placebo-controlled trials. In one trial INVOKANA was used as monotherapy and in three trials INVOKANA was used as add-on therapy [see Clinical Studies (14) in full Prescribing Information]. These data reflect exposure of 1667 patients to INVOKANA and a mean duration of exposure to INVOKANA of 24 weeks. Patients received INVOKANA 100 mg (N=833), INVOKANA 300 mg (N=834) or placebo (N=646) once daily. The mean age of the population was 56 years and 2% were older than 75 years of age. Fifty percent (50%) of the population was male and 72% were Caucasian, 12% were Asian, and 5% were Black or African American. At baseline the population had diabetes for an average of 7.3 years, had a mean HbA1C of 8.0% and 20% had established microvascular complications of diabetes. Baseline renal function was normal or mildly impaired (mean eGFR 88 mL/min/1.73 m2).
Table 1 shows common adverse reactions associated with the use of INVOKANA. These adverse reactions were not present at baseline, occurred more commonly on INVOKANA than on placebo, and occurred in at least 2% of patients treated with either INVOKANA 100 mg or INVOKANA 300 mg.
INVOKANA® (canagliflozin) tablets

Table 1: Adverse Reactions From Pool of Four 26−Week Placebo-Controlled Studies Reported in ≥ 2% of INVOKANA-Treated Patients*
Adverse ReactionPlaceboN=646
INVOKANA100 mgN=833
INVOKANA300 mgN=834
Female genital mycotic infections†
3.2% 10.4% 11.4%
Urinary tract infections‡ 4.0% 5.9% 4.3%
Increased urination§ 0.8% 5.3% 4.6%
Male genital mycotic infections¶
0.6% 4.2% 3.7%
Vulvovaginal pruritus 0.0% 1.6% 3.0%
Thirst# 0.2% 2.8% 2.3%
Constipation 0.9% 1.8% 2.3%
Nausea 1.5% 2.2% 2.3%
* The four placebo-controlled trials included one monotherapy trial and three add-on combination trials with metformin, metformin and sulfonylurea, or metformin and pioglitazone.
† Female genital mycotic infections include the following adverse reactions: Vulvovaginal candidiasis, Vulvovaginal mycotic infection, Vulvovaginitis, Vaginal infection, Vulvitis, and Genital infection fungal. Percentages calculated with the number of female subjects in each group as denominator: placebo (N=312), INVOKANA 100 mg (N=425), and INVOKANA 300 mg (N=430).
‡ Urinary tract infections include the following adverse reactions: Urinary tract infection, Cystitis, Kidney infection, and Urosepsis.
§ Increased urination includes the following adverse reactions: Polyuria, Pollakiuria, Urine output increased, Micturition urgency, and Nocturia.
¶ Male genital mycotic infections include the following adverse reactions: Balanitis or Balanoposthitis, Balanitis candida, and Genital infection fungal. Percentages calculated with the number of male subjects in each group as denominator: placebo (N=334), INVOKANA 100 mg (N=408), and INVOKANA 300 mg (N=404).
# Thirst includes the following adverse reactions: Thirst, Dry mouth, and Polydipsia.
Abdominal pain was also more commonly reported in patients taking INVOKANA 100 mg (1.8%), 300 mg (1.7%) than in patients taking placebo (0.8%).
Pool of Placebo- and Active-Controlled Trials: The occurrence of adverse reactions for canagliflozin was evaluated in a larger pool of patients participating in placebo- and active-controlled trials.
The data combined eight clinical trials [see Clinical Studies (14) in full Prescribing Information] and reflect exposure of 6177 patients to INVOKANA. The mean duration of exposure to INVOKANA was 38 weeks with 1832 individuals exposed to INVOKANA for greater than 50 weeks. Patients received INVOKANA 100 mg (N=3092), INVOKANA 300 mg (N=3085) or comparator (N=3262) once daily. The mean age of the population was 60 years and 5% were older than 75 years of age. Fifty-eight percent (58%) of the population was male and 73% were Caucasian, 16% were Asian, and 4% were Black or African American. At baseline, the population had diabetes for an average of 11 years, had a mean HbA1C of 8.0% and 33% had established microvascular complications of diabetes. Baseline renal function was normal or mildly impaired (mean eGFR 81 mL/min/1.73 m2).
The types and frequency of common adverse reactions observed in the pool of eight clinical trials were consistent with those listed in Table 1. In this pool, INVOKANA was also associated with the adverse reactions of fatigue (1.7% with comparator, 2.2% with INVOKANA 100 mg, and 2.0% with INVOKANA 300 mg) and loss of strength or energy (i.e., asthenia) (0.6% with comparator, 0.7% with INVOKANA 100 mg, and 1.1% with INVOKANA 300 mg).
In the pool of eight clinical trials, the incidence rate of pancreatitis (acute or chronic) was 0.9, 2.7, and 0.9 per 1000 patient-years of exposure to comparator, INVOKANA 100 mg, and INVOKANA 300 mg, respectively.
In the pool of eight clinical trials, hypersensitivity-related adverse reactions (including erythema, rash, pruritus, urticaria, and angioedema) occurred in 3.0%, 3.8%, and 4.2% of patients receiving comparator, INVOKANA 100 mg, and INVOKANA 300 mg, respectively. Five patients experienced serious adverse reactions of hypersensitivity with INVOKANA, which included 4 patients with urticaria and 1 patient with a diffuse rash and urticaria occurring within hours of exposure to INVOKANA. Among these patients, 2 patients discontinued INVOKANA. One patient with urticaria had recurrence when INVOKANA was re-initiated.
Photosensitivity-related adverse reactions (including photosensitivity reaction, polymorphic light eruption, and sunburn) occurred in 0.1%, 0.2%, and 0.2% of patients receiving comparator, INVOKANA 100 mg, and INVOKANA 300 mg, respectively.
Other adverse reactions occurring more frequently on INVOKANA than on comparator were:
Volume Depletion-Related Adverse Reactions: INVOKANA results in an osmotic diuresis, which may lead to reductions in intravascular volume. In clinical studies, treatment with INVOKANA was associated with a dose-dependent increase in the incidence of volume depletion-related adverse reactions (e.g., hypotension, postural dizziness, orthostatic hypotension, syncope, and dehydration). An increased incidence was observed in patients on the 300 mg dose. The three factors associated with the largest increase in volume depletion-related adverse reactions were the use of loop diuretics, moderate renal impairment (eGFR 30 to less than 60 mL/min/1.73 m2), and age 75 years and older (Table 2) [see Dosage and Administration (2.2) in full Prescribing Information, Warnings and Precautions, and Use in Specific Populations].
Table 2: Proportion of Patients With at Least One Volume Depletion-Related Adverse Reaction (Pooled Results from 8 Clinical Trials)
Baseline Characteristic
Comparator Group*
%
INVOKANA 100 mg
%
INVOKANA 300 mg
%
Overall population 1.5% 2.3% 3.4%
75 years of age and older† 2.6% 4.9% 8.7%
eGFR less than 60 mL/min/1.73 m2† 2.5% 4.7% 8.1%
Use of loop diuretic† 4.7% 3.2% 8.8%
* Includes placebo and active-comparator groups† Patients could have more than 1 of the listed risk factors
Falls: In a pool of nine clinical trials with mean duration of exposure to INVOKANA of 85 weeks, the proportion of patients who experienced falls was 1.3%, 1.5%, and 2.1% with comparator, INVOKANA 100 mg, and INVOKANA 300 mg, respectively. The higher risk of falls for patients treated with INVOKANA was observed within the first few weeks of treatment.
Impairment in Renal Function: INVOKANA is associated with a dose-dependent increase in serum creatinine and a concomitant fall in estimated GFR (Table 3). Patients with moderate renal impairment at baseline had larger mean changes.
Table 3: Changes in Serum Creatinine and eGFR Associated with INVOKANA in the Pool of Four Placebo-Controlled Trials and Moderate Renal Impairment Trial
PlaceboN=646
INVOKANA 100 mgN=833
INVOKANA 300 mgN=834
Pool of Four Placebo-Controlled Trials
BaselineCreatinine (mg/dL) 0.84 0.82 0.82
eGFR (mL/min/1.73 m2) 87.0 88.3 88.8
Week 6 Change
Creatinine (mg/dL) 0.01 0.03 0.05
eGFR (mL/min/1.73 m2) -1.6 -3.8 -5.0
End of Treatment Change*
Creatinine (mg/dL) 0.01 0.02 0.03
eGFR (mL/min/1.73 m2) -1.6 -2.3 -3.4
PlaceboN=90
INVOKANA 100 mgN=90
INVOKANA 300 mgN=89
Moderate Renal Impairment Trial
Baseline Creatinine (mg/dL) 1.61 1.62 1.63
eGFR (mL/min/1.73 m2) 40.1 39.7 38.5
Week 3 Change
Creatinine (mg/dL) 0.03 0.18 0.28
eGFR (mL/min/1.73 m2) -0.7 -4.6 -6.2
End of Treatment Change*
Creatinine (mg/dL) 0.07 0.16 0.18
eGFR (mL/min/1.73 m2) -1.5 -3.6 -4.0
* Week 26 in mITT LOCF population
In the pool of four placebo-controlled trials where patients had normal or mildly impaired baseline renal function, the proportion of patients who experienced at least one event of significant renal function decline, defined as an eGFR below 80 mL/min/1.73 m2 and 30% lower than baseline, was 2.1% with placebo, 2.0% with INVOKANA 100 mg, and 4.1% with INVOKANA 300 mg. At the end of treatment, 0.5% with placebo, 0.7% with INVOKANA 100 mg, and 1.4% with INVOKANA 300 mg had a significant renal function decline.
In a trial carried out in patients with moderate renal impairment with a baseline eGFR of 30 to less than 50 mL/min/1.73 m2 (mean baseline eGFR 39 mL/min/1.73 m2) [see Clinical Studies (14.3) in full Prescribing Information], the proportion of patients who experienced at least one event of significant renal function decline, defined as an eGFR 30% lower than baseline,
INVOKANA® (canagliflozin) tablets INVOKANA® (canagliflozin) tablets

was 6.9% with placebo, 18% with INVOKANA 100 mg, and 22.5% with INVOKANA 300 mg. At the end of treatment, 4.6% with placebo, 3.4% with INVOKANA 100 mg, and 2.2% with INVOKANA 300 mg had a significant renal function decline.
In a pooled population of patients with moderate renal impairment (N=1085) with baseline eGFR of 30 to less than 60 mL/min/1.73 m2 (mean baseline eGFR 48 mL/min/1.73 m2), the overall incidence of these events was lower than in the dedicated trial but a dose-dependent increase in incident episodes of significant renal function decline compared to placebo was still observed.
Use of INVOKANA has been associated with an increased incidence of renal-related adverse reactions (e.g., increased blood creatinine, decreased glomerular filtration rate, renal impairment, and acute renal failure), particularly in patients with moderate renal impairment.
In the pooled analysis of patients with moderate renal impairment, the incidence of renal-related adverse reactions was 3.7% with placebo, 8.9% with INVOKANA 100 mg, and 9.3% with INVOKANA 300 mg. Discontinuations due to renal-related adverse events occurred in 1.0% with placebo, 1.2% with INVOKANA 100 mg, and 1.6% with INVOKANA 300 mg [see Warnings and Precautions].
Genital Mycotic Infections: In the pool of four placebo-controlled clinical trials, female genital mycotic infections (e.g., vulvovaginal mycotic infection, vulvovaginal candidiasis, and vulvovaginitis) occurred in 3.2%, 10.4%, and 11.4% of females treated with placebo, INVOKANA 100 mg, and INVOKANA 300 mg, respectively. Patients with a history of genital mycotic infections were more likely to develop genital mycotic infections on INVOKANA. Female patients who developed genital mycotic infections on INVOKANA were more likely to experience recurrence and require treatment with oral or topical antifungal agents and anti-microbial agents. In females, discontinuation due to genital mycotic infections occurred in 0% and 0.7% of patients treated with placebo and INVOKANA, respectively [see Warnings and Precautions].
In the pool of four placebo-controlled clinical trials, male genital mycotic infections (e.g., candidal balanitis, balanoposthitis) occurred in 0.6%, 4.2%, and 3.7% of males treated with placebo, INVOKANA 100 mg, and INVOKANA 300 mg, respectively. Male genital mycotic infections occurred more commonly in uncircumcised males and in males with a prior history of balanitis or balanoposthitis. Male patients who developed genital mycotic infections on INVOKANA were more likely to experience recurrent infections (22% on INVOKANA versus none on placebo), and require treatment with oral or topical antifungal agents and anti-microbial agents than patients on comparators. In males, discontinuations due to genital mycotic infections occurred in 0% and 0.5% of patients treated with placebo and INVOKANA, respectively. In the pooled analysis of 8 controlled trials, phimosis was reported in 0.3% of uncircumcised male patients treated with INVOKANA and 0.2% required circumcision to treat the phimosis [see Warnings and Precautions].
Hypoglycemia: In all clinical trials, hypoglycemia was defined as any event regardless of symptoms, where biochemical hypoglycemia was documented (any glucose value below or equal to 70 mg/dL). Severe hypoglycemia was defined as an event consistent with hypoglycemia where the patient required the assistance of another person to recover, lost consciousness, or experienced a seizure (regardless of whether biochemical documentation of a low glucose value was obtained). In individual clinical trials [see Clinical Studies (14) in full Prescribing Information], episodes of hypoglycemia occurred at a higher rate when INVOKANA was co-administered with insulin or sulfonylureas (Table 4) [see Warnings and Precautions].
Table 4: Incidence of Hypoglycemia* in Controlled Clinical Studies
Monotherapy(26 weeks)
Placebo(N=192)
INVOKANA 100 mg(N=195)
INVOKANA 300 mg(N=197)
Overall [N (%)] 5 (2.6) 7 (3.6) 6 (3.0)
In Combination with Metformin(26 weeks)
Placebo + Metformin
(N=183)
INVOKANA 100 mg + Metformin
(N=368)
INVOKANA 300 mg + Metformin
(N=367)
Overall [N (%)] 3 (1.6) 16 (4.3) 17 (4.6)
Severe [N (%)]† 0 (0) 1 (0.3) 1 (0.3)
In Combination with Metformin(52 weeks)
Glimepiride + Metformin
(N=482)
INVOKANA 100 mg + Metformin
(N=483)
INVOKANA 300 mg + Metformin
(N=485)
Overall [N (%)] 165 (34.2) 27 (5.6) 24 (4.9)
Severe [N (%)]† 15 (3.1) 2 (0.4) 3 (0.6)
In Combination with Sulfonylurea(18 weeks)
Placebo + Sulfonylurea
(N=69)
INVOKANA 100 mg + Sulfonylurea
(N=74)
INVOKANA 300 mg + Sulfonylurea
(N=72)
Overall [N (%)] 4 (5.8) 3 (4.1) 9 (12.5)
Table 4: Incidence of Hypoglycemia* in Controlled Clinical Studies (continued)
In Combination with Metformin + Sulfonylurea(26 weeks)
Placebo + Metformin + Sulfonylurea
(N=156)
INVOKANA 100 mg + Metformin + Sulfonylurea
(N=157)
INVOKANA 300 mg + Metformin + Sulfonylurea
(N=156)
Overall [N (%)] 24 (15.4) 43 (27.4) 47 (30.1)
Severe [N (%)]† 1 (0.6) 1 (0.6) 0
In Combination with Metformin + Sulfonylurea(52 weeks)
Sitagliptin + Metformin + Sulfonylurea
(N=378)
INVOKANA 300 mg + Metformin + Sulfonylurea
(N=377)
Overall [N (%)] 154 (40.7) 163 (43.2)
Severe [N (%)]† 13 (3.4) 15 (4.0)
In Combination with Metformin + Pioglitazone(26 weeks)
Placebo + Metformin + Pioglitazone
(N=115)
INVOKANA 100 mg + Metformin + Pioglitazone
(N=113)
INVOKANA 300 mg + Metformin + Pioglitazone
(N=114)
Overall [N (%)] 3 (2.6) 3 (2.7) 6 (5.3)
In Combination with Insulin(18 weeks)
Placebo(N=565)
INVOKANA 100 mg(N=566)
INVOKANA 300 mg(N=587)
Overall [N (%)] 208 (36.8) 279 (49.3) 285 (48.6)
Severe [N (%)]† 14 (2.5) 10 (1.8) 16 (2.7)
* Number of patients experiencing at least one event of hypoglycemia based on either biochemically documented episodes or severe hypoglycemic events in the intent-to-treat population
† Severe episodes of hypoglycemia were defined as those where the patient required the assistance of another person to recover, lost consciousness, or experienced a seizure (regardless of whether biochemical documentation of a low glucose value was obtained)
Bone Fracture: The occurrence of bone fractures was evaluated in a pool of nine clinical trials with a mean duration of exposure to INVOKANA of 85 weeks. The incidence rates of adjudicated bone fractures were 1.1, 1.4, and 1.5 per 100 patient-years of exposure in the comparator, INVOKANA 100 mg, and INVOKANA 300 mg groups, respectively. Fractures were observed as early as 12 weeks after treatment initiation and were more likely to be low trauma (e.g., fall from no more than standing height), and affect the upper extremities [see Warnings and Precautions].
Laboratory and Imaging Tests: Increases in Serum Potassium In a pooled population of patients (N=723) with moderate renal impairment (eGFR 45 to less than 60 mL/min/1.73 m2), increases in serum potassium to greater than 5.4 mEq/L and 15% above baseline occurred in 5.3%, 5.0%, and 8.8% of patients treated with placebo, INVOKANA 100 mg, and INVOKANA 300 mg, respectively. Severe elevations (greater than or equal to 6.5 mEq/L) occurred in 0.4% of patients treated with placebo, no patients treated with INVOKANA 100 mg, and 1.3% of patients treated with INVOKANA 300 mg.
In these patients, increases in potassium were more commonly seen in those with elevated potassium at baseline. Among patients with moderate renal impairment, approximately 84% were taking medications that interfere with potassium excretion, such as potassium-sparing diuretics, angiotensin-converting-enzyme inhibitors, and angiotensin-receptor blockers [see Warnings and Precautions and Use in Specific Populations].
Increases in Serum Magnesium: Dose-related increases in serum magnesium were observed early after initiation of INVOKANA (within 6 weeks) and remained elevated throughout treatment. In the pool of four placebo-controlled trials, the mean percent change in serum magnesium levels was 8.1% and 9.3% with INVOKANA 100 mg and INVOKANA 300 mg, respectively, compared to -0.6% with placebo. In a trial of patients with moderate renal impairment [see Clinical Studies (14.3) in full Prescribing Information], serum magnesium levels increased by 0.2%, 9.2%, and 14.8% with placebo, INVOKANA 100 mg, and INVOKANA 300 mg, respectively.
Increases in Serum Phosphate: Dose-related increases in serum phosphate levels were observed with INVOKANA. In the pool of four placebo controlled trials, the mean percent change in serum phosphate levels were 3.6% and 5.1% with INVOKANA 100 mg and INVOKANA 300 mg, respectively, compared to 1.5% with placebo. In a trial of patients with moderate renal impairment [see Clinical Studies (14.3) in full Prescribing Information], the mean serum phosphate levels increased by 1.2%, 5.0%, and 9.3% with placebo, INVOKANA 100 mg, and INVOKANA 300 mg, respectively.
Increases in Low-Density Lipoprotein Cholesterol (LDL-C) and non-High-Density Lipoprotein Cholesterol (non-HDL-C): In the pool of four placebo-controlled trials, dose-related increases in LDL-C with INVOKANA were observed. Mean changes (percent changes) from baseline in LDL-C relative to
INVOKANA® (canagliflozin) tablets INVOKANA® (canagliflozin) tablets

placebo were 4.4 mg/dL (4.5%) and 8.2 mg/dL (8.0%) with INVOKANA 100 mg and INVOKANA 300 mg, respectively. The mean baseline LDL-C levels were 104 to 110 mg/dL across treatment groups [see Warnings and Precautions].
Dose-related increases in non-HDL-C with INVOKANA were observed. Mean changes (percent changes) from baseline in non-HDL-C relative to placebo were 2.1 mg/dL (1.5%) and 5.1 mg/dL (3.6%) with INVOKANA 100 mg and 300 mg, respectively. The mean baseline non-HDL-C levels were 140 to 147 mg/dL across treatment groups.
Increases in Hemoglobin: In the pool of four placebo-controlled trials, mean changes (percent changes) from baseline in hemoglobin were -0.18 g/dL (-1.1%) with placebo, 0.47 g/dL (3.5%) with INVOKANA 100 mg, and 0.51 g/dL (3.8%) with INVOKANA 300 mg. The mean baseline hemoglobin value was approximately 14.1 g/dL across treatment groups. At the end of treatment, 0.8%, 4.0%, and 2.7% of patients treated with placebo, INVOKANA 100 mg, and INVOKANA 300 mg, respectively, had hemoglobin above the upper limit of normal.
Decreases in Bone Mineral Density: Bone mineral density (BMD) was measured by dual-energy X-ray absorptiometry in a clinical trial of 714 older adults (mean age 64 years) [see Clinical Studies (14.3) in full Prescribing Information]. At 2 years, patients randomized to INVOKANA 100 mg and INVOKANA 300 mg had placebo-corrected declines in BMD at the total hip of 0.9% and 1.2%, respectively, and at the lumbar spine of 0.3% and 0.7%, respectively. Additionally, placebo-adjusted BMD declines were 0.1% at the femoral neck for both INVOKANA doses and 0.4% at the distal forearm for patients randomized to INVOKANA 300 mg. The placebo-adjusted change at the distal forearm for patients randomized to INVOKANA 100 mg was 0%.
Postmarketing Experience: Additional adverse reactions have been identified during postapproval use of INVOKANA. Because these reactions are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
Ketoacidosis [see Warnings and Precautions]
Anaphylaxis, Angioedema [see Warnings and Precautions]
Urosepsis and Pyelonephritis [see Warnings and Precautions]
DRUG INTERACTIONSUGT Enzyme Inducers: Rifampin: Co-administration of canagliflozin with rifampin, a nonselective inducer of several UGT enzymes, including UGT1A9, UGT2B4, decreased canagliflozin area under the curve (AUC) by 51%. This decrease in exposure to canagliflozin may decrease efficacy. If an inducer of these UGTs (e.g., rifampin, phenytoin, phenobarbital, ritonavir) must be co-administered with INVOKANA (canagliflozin), consider increasing the dose to 300 mg once daily if patients are currently tolerating INVOKANA 100 mg once daily, have an eGFR greater than 60 mL/min/1.73 m2, and require additional glycemic control. Consider other antihyperglycemic therapy in patients with an eGFR of 45 to less than 60 mL/min/1.73 m2 receiving concurrent therapy with a UGT inducer and require additional glycemic control [see Dosage and Administration (2.3) and Clinical Pharmacology (12.3) in full Prescribing Information].
Digoxin: There was an increase in the AUC and mean peak drug concen-tration (Cmax) of digoxin (20% and 36%, respectively) when co-administered with INVOKANA 300 mg [see Clinical Pharmacology (12.3) in full Prescribing Information]. Patients taking INVOKANA with concomitant digoxin should be monitored appropriately.
Positive Urine Glucose Test: Monitoring glycemic control with urine glucose tests is not recommended in patients taking SGLT2 inhibitors as SGLT2 inhibitors increase urinary glucose excretion and will lead to positive urine glucose tests. Use alternative methods to monitor glycemic control.
Interference with 1,5-anhydroglucitol (1,5-AG) Assay: Monitoring glycemic control with 1,5-AG assay is not recommended as measurements of 1,5-AG are unreliable in assessing glycemic control in patients taking SGLT2 inhibitors. Use alternative methods to monitor glycemic control.
USE IN SPECIFIC POPULATIONSPregnancy: Teratogenic Effects: Pregnancy Category C: There are no adequate and well-controlled studies of INVOKANA in pregnant women. Based on results from rat studies, canagliflozin may affect renal development and maturation. In a juvenile rat study, increased kidney weights and renal pelvic and tubular dilatation were evident at greater than or equal to 0.5 times clinical exposure from a 300 mg dose [see Nonclinical Toxicology (13.2) in full Prescribing Information].
These outcomes occurred with drug exposure during periods of animal development that correspond to the late second and third trimester of human development. During pregnancy, consider appropriate alternative therapies, especially during the second and third trimesters. INVOKANA should be used during pregnancy only if the potential benefit justifies the
potential risk to the fetus.
Nursing Mothers: It is not known if INVOKANA is excreted in human milk. INVOKANA is secreted in the milk of lactating rats reaching levels 1.4 times higher than that in maternal plasma. Data in juvenile rats directly exposed to INVOKANA showed risk to the developing kidney (renal pelvic and tubular dilatations) during maturation. Since human kidney maturation occurs in utero and during the first 2 years of life when lactational exposure may occur, there may be risk to the developing human kidney. Because many drugs are excreted in human milk and because of the potential for serious adverse reactions in nursing infants from INVOKANA, a decision should be made whether to discontinue nursing or to discontinue INVOKANA, taking into account the importance of the drug to the mother [see Nonclinical Toxicology (13.2) in full Prescribing Information].
Pediatric Use: Safety and effectiveness of INVOKANA in pediatric patients under 18 years of age have not been established.
Geriatric Use: Two thousand thirty-four (2034) patients 65 years and older, and 345 patients 75 years and older were exposed to INVOKANA in nine clinical studies of INVOKANA [see Clinical Studies (14.3) in full Prescribing Information].
Patients 65 years and older had a higher incidence of adverse reactions related to reduced intravascular volume with INVOKANA (such as hypotension, postural dizziness, ortho static hypotension, syncope, and dehydration), particularly with the 300 mg daily dose, compared to younger patients; a more prominent increase in the incidence was seen in patients who were 75 years and older [see Dosage and Administration (2.1) in full Prescribing Information and Adverse Reactions]. Smaller reductions in HbA1C with INVOKANA relative to placebo were seen in older (65 years and older; -0.61% with INVOKANA 100 mg and -0.74% with INVOKANA 300 mg relative to placebo) compared to younger patients (-0.72% with INVOKANA 100 mg and -0.87% with INVOKANA 300 mg relative to placebo).
Renal Impairment: The efficacy and safety of INVOKANA were evaluated in a study that included patients with moderate renal impairment (eGFR 30 to less than 50 mL/min/1.73 m2) [see Clinical Studies (14.3) in full Prescribing Information]. These patients had less overall glycemic efficacy and had a higher occurrence of adverse reactions related to reduced intravascular volume, renal-related adverse reactions, and decreases in eGFR compared to patients with mild renal impairment or normal renal function (eGFR greater than or equal to 60 mL/min/1.73 m2). Dose-related, transient mean increases in serum potassium were observed early after initiation of INVOKANA (i.e., within 3 weeks) in this trial. Increases in serum potassium of greater than 5.4 mEq/L and 15% above baseline occurred in 16.1%, 12.4%, and 27.0% of patients treated with placebo, INVOKANA 100 mg, and INVOKANA 300 mg, respectively. Severe elevations (greater than or equal to 6.5 mEq/L) occurred in 1.1%, 2.2%, and 2.2% of patients treated with placebo, INVOKANA 100 mg, and INVOKANA 300 mg, respectively [see Dosage and Administration (2.2) in full Prescribing Information, Warnings and Precautions, and Adverse Reactions].
The efficacy and safety of INVOKANA have not been established in patients with severe renal impairment (eGFR less than 30 mL/min/1.73 m2), with ESRD, or receiving dialysis. INVOKANA is not expected to be effective in these patient populations [see Contraindications and Clinical Pharmacology (12.3) in full Prescribing Information].
Hepatic Impairment: No dosage adjustment is necessary in patients with mild or moderate hepatic impairment. The use of INVOKANA has not been studied in patients with severe hepatic impairment and is therefore not recommended [see Clinical Pharmacology (12.3) in full Prescribing Information].
OVERDOSAGEThere were no reports of overdose during the clinical development program of INVOKANA (canagliflozin).
In the event of an overdose, contact the Poison Control Center. It is also reasonable to employ the usual supportive measures, e.g., remove unabsorbed material from the gastrointestinal tract, employ clinical monitoring, and institute supportive treatment as dictated by the patient’s clinical status. Canagliflozin was negligibly removed during a 4-hour hemodialysis session. Canagliflozin is not expected to be dialyzable by peritoneal dialysis.
PATIENT COUNSELING INFORMATIONSee FDA-approved patient labeling (Medication Guide).
Instructions: Instruct patients to read the Medication Guide before starting INVOKANA (canagliflozin) therapy and to reread it each time the prescription is renewed.
Inform patients of the potential risks and benefits of INVOKANA and of alternative modes of therapy. Also inform patients about the importance of
INVOKANA® (canagliflozin) tablets INVOKANA® (canagliflozin) tablets

MEDICAL ECONOMICS ❚ JUNE 25, 2016 17
(Even) more MedEcSEE WHAT YOU MAY HAVE BEEN MISSING IN OUR ENEWSLETTER AND ON OUR WEBSITE
adherence to dietary instructions, regular physical activity, periodic blood glucose monitoring and HbA1C testing, recognition and management of hypoglycemia and hyperglycemia, and assessment for diabetes complications. Advise patients to seek medical advice promptly during periods of stress such as fever, trauma, infection, or surgery, as medication requirements may change.
Instruct patients to take INVOKANA only as prescribed. If a dose is missed, advise patients to take it as soon as it is remembered unless it is almost time for the next dose, in which case patients should skip the missed dose and take the medicine at the next regularly scheduled time. Advise patients not to take two doses of INVOKANA at the same time.
Inform patients that the most common adverse reactions associated with INVOKANA are genital mycotic infection, urinary tract infection, and increased urination.
Inform female patients of child bearing age that the use of INVOKANA during pregnancy has not been studied in humans, and that INVOKANA should only be used during pregnancy only if the potential benefit justifies the potential risk to the fetus. Instruct patients to report pregnancies to their physicians as soon as possible.
Inform nursing mothers to discontinue INVOKANA or nursing, taking into account the importance of drug to the mother.
Laboratory Tests: Due to its mechanism of action, patients taking INVOKANA will test positive for glucose in their urine.
Hypotension: Inform patients that symptomatic hypotension may occur with INVOKANA and advise them to contact their doctor if they experience such symptoms [see Warnings and Precautions]. Inform patients that dehydration may increase the risk for hypotension, and to have adequate fluid intake.
Ketoacidosis: Inform patients that ketoacidosis has been reported during use of INVOKANA. Instruct patients to check ketones (when possible) if symptoms consistent with ketoacidosis occur even if blood glucose is not elevated. If symptoms of ketoacidosis (including nausea, vomiting, abdominal pain, tiredness, and labored breathing) occur, instruct patients to discontinue INVOKANA and seek medical advice immediately [see Warnings and Precautions].
Serious Urinary Tract Infections: Inform patients of the potential for urinary tract infections, which may be serious. Provide them with information on the symptoms of urinary tract infections. Advise them to seek medical advice if such symptoms occur [see Warnings and Precautions].
Genital Mycotic Infections in Females (e.g., Vulvovaginitis): Inform female patients that vaginal yeast infection may occur and provide them with information on the signs and symptoms of vaginal yeast infection. Advise them of treatment options and when to seek medical advice [see Warnings and Precautions].
Genital Mycotic Infections in Males (e.g., Balanitis or Balanoposthitis): Inform male patients that yeast infection of penis (e.g., balanitis or balanoposthitis) may occur, especially in uncircumcised males and patients with prior history. Provide them with information on the signs and symptoms of balanitis and balanoposthitis (rash or redness of the glans or foreskin of the penis). Advise them of treatment options and when to seek medical advice [see Warnings and Precautions].
Hypersensitivity Reactions: Inform patients that serious hypersensitivity reactions, such as urticaria, rash, anaphylaxis, and angioedema, have been reported with INVOKANA. Advise patients to report immediately any signs or symptoms suggesting allergic reaction, and to discontinue drug until they have consulted prescribing physicians.
Bone Fracture: Inform patients that bone fractures have been reported in patients taking INVOKANA. Provide them with information on factors that may contribute to fracture risk.
Active ingredient made in Belgium
Manufactured for:Janssen Pharmaceuticals, Inc.Titusville, NJ 08560
Finished product manufactured by:Janssen Ortho, LLCGurabo, PR 00778
Licensed from Mitsubishi Tanabe Pharma Corporation
© 2013 Janssen Pharmaceuticals, Inc.
051446-160415
INVOKANA® (canagliflozin) tablets
Receive timely
information
on the latest
developments
in primary
care practice
management,
fi nances, health
law, and other
matters vital to
your livelihood by
signing up for Medical Economics eConsult,
delivered to your email box for free.
BE SUCCESSFUL IN YOUR PRACTICE, WITH THE HELP OF OUR EXPERTS
Sign up today! Visit MedicalEconomics.com/enewssignup
“THE HEALTHCARE
system must transform and payment reform represents one pathway that is rapidly diff using,” according to Michael Chernew, PhD, of the Harvard Medical School, Department of Health Care Policy, Boston, MA, who spoke about payment reform at the 2015 American College of Cardiology meeting in March.
Chernew highlighted payment reform as one solution to the continual and unsustainable rise in healthcare spending. This reform includes reductions in payments to providers and plans, as well as a movement away from the current fee-for-service payment model to bundled
payments by episode and patient (global payment).
Among the range of public strategies for reforming payment, Chernew focused on the trend in growth of Accountable Care Organizations (ACOs) and data showing an estimated total savings of $146.9 million during 2011-2012 in what he called the “pioneer” ACOs. Most of these savings were seen in eight ACOs that saw reductions in spending ranging from $32.58 to $102.21 per benefi ciary per month.
Chernow also emphasized that ACOs do not have a negative impact on patient experiences, citing data showing that overall care ratings improve.
ACOs show payment reform is possible

MedicalEconomics.com18
IN DEPTH
MEDICAL ECONOMICS ❚ JUNE 25, 2016
by JANET COLWELL Contributing author
Entrepreneurial docs make it work by cutting out third-party payers and negotiating with suppliers
Physicians chart new path into direct primary care
PRIMARY CARE physician Jeff rey Gold, MD, followed a traditional career path when he fi nished his residency about 10 years ago. He started at a private clinic then joined a large physician group in the Boston, Massachu-setts area. Five years into that job, however, he became disillusioned by the system and began to consider striking out on his own.
“Working as an employee worked well for about fi ve years when I was busy and starting a family and wanted the guaranteed salary,” says Gold, a family physician and owner of Gold Direct Care in Marblehead, Massachusetts. “Th en one day I realized I was actually annoyed at a patient for talk-ing too long and realized it wasn’t really her I was annoyed with, but a healthcare system that gives me about 10 minutes with each patient.”
It was around that time that he heard about the direct primary care (DPC) move-ment that was beginning to gain traction in a few states. Th e model is similar to con-cierge care, in which patients pay a premium
for better access and extra services, but with a couple of key diff erences.
In concierge practices, physicians typi-cally collect monthly or annual fees for extra services while also billing third-party insur-ance, whereas most DPC practices operate on a cash-only basis and do not work with third-party payers (although patients are encouraged to have catastrophic coverage.) In addition, DPC practices typically charge much less—about $77/month, on average, compared with an average of around $180/month at concierge practices.
Gold eventually left his job to launch Gold Direct Care in February 2015. He hopes to break even by the end of this year if mem-bership continues to grow at its current pace of 12 to 15 enrollees per month.
Gold is part of a small but growing seg-ment of primary care physicians who have adopted the DPC model, says Julie Gunther, MD, a Boise, Idaho-based DPC family physi-cian who serves on the steering committee of the DPC Coalition, a national advocacy
HIGHLIGHTS
The biggest barriers
to DPC entry for many
physicians are fear
about loss of income
during the transition and
aversion to taking risks.
Direct pay offers
savings over traditional
practice that balance
out some of the start-up
costs. For example,
direct practices do not
need staff to handle
third-party billing.
Operations
This is the fi rst in a new series, “Innovations in Practice,” exploring new practice models and creative avenues where physicians are working to best serve their patients.

MedicalEconomics.com 19 MEDICAL ECONOMICS ❚ JUNE 25, 2016
group. DPC first started to take hold in the United States in the late 1990s. To-day, there are about 345 DPC clinics in 45 states, up from 300 in 39 states about a year ago, says Gunther.
GETTING STARTEDThe biggest barriers to entry for many physicians are fear of losing income dur-ing the transition and aversion to taking risks, says Gunther. “You do need to have some tolerance of risk and interest in en-trepreneurship but we have a very sup-portive community that can help you get started.”
For Gold, visiting an established practice was instrumental in his deci-sion to convert to DPC. As part of his market research, he flew to Wichita, Kansas, to meet with family physi-cian Josh Umbehr, MD, founder of Atlas MD, and returned home completely sold on making the transition.
“I was seeing 25 patients a day and they were seeing 25 patients in a week between three physicians,” Gold recalls. “They had some wealthy patients but they also had many working-class pa-tients who were looking for affordable, high-quality care where they wouldn’t be treated like a number—that’s what really convinced me to give it try.”
Umbehr launched Atlas MD straight out of residency in 2010 and has since taken on four partners and grown to 600 patients per physician. Perceiving a lack of DPC resources and help for new prac-tices, he created an online DPC curricu-lum for start-ups and has provided free consulting to more than 165 physicians over the past two years.
“Most doctors we talk to are afraid of change,” says Umbehr, who also has a DPC podcast and blog. “They’re often afraid of the business side, such as how to set prices or how to handle medications and labs. We walk them through all these issues and show them how it works in ac-tual practice.”
His online curriculum outlines the basic costs of starting up as well as tips on buying equipment and answering common patient questions, among other topics. Umbehr
Direct pay Operations
24
Three physicians who have started direct
primary care (DPC) practices offered the
following tips for getting started.
1Look for support The DPC industry, though still small, has gained a passionate following, says Jeffrey Gold, MD, owner of
Gold Primary Care in Marblehead, Massachusetts. Physicians with established DPC practices often are willing to help newcomers at no cost. Visiting one of those practices and witnessing how the model works first-hand can give you confidence to move forward.
2Don’t do it halfway Some physicians choose to start with a hybrid DPC model, where some patients continue to use third-party
insurance, in the hope of making a gradual transition. However, it quickly becomes difficult to juggle two models and two sets of patients with different levels of benefits, says Josh Umbehr, MD, founder of Atlas MD in Wichita, Kansas. “It may feel safer at first but it can actually make your life harder.”
3Negotiate with suppliers
Physicians often are hesitant to negotiate wholesale rates with drug companies and labs, but the discounts
can be substantial–up to 95% off retail rates in some cases, says Umbehr. And those discounts are key to providing value to patients and keeping your costs down. “Most doctors know that drug prices are inflated but they don’t realize how easy it is to get cash rates.”
4Think like an entrepreneur
Many physicians are afraid of the business side of running a DPC practice but they often underestimate
their abilities, says Julie Gunther, MD, who runs a DPC practice in Boise, Idaho. “If you can start a central line or perform a C-section, you can figure out how to run a small business,” she says.
LESSONS LEARNED

IndicationsProAir® RespiClick (albuterol sulfate) Inhalation Powder is indicated in patients 12 years of age and older for the treatment or prevention of bronchospasm with reversible obstructive airway disease and for the prevention of exercise-induced bronchospasm.
Important Safety Information7���/,�'/® RespiClick (albuterol sulfate) Inhalation Powder is contraindicated in patients with
hypersensitivity to albuterol or patients with a severe hypersensitivity to milk proteins. Rare cases of hypersensitivity reactions, including urticaria, angiodema, and rash have been reported after the use of albuterol sulfate. There have been reports of anaphylactic reactions in patients using inhalation therapies containing lactose
7���/,�'/® RespiClick can produce paradoxical bronchospasm that may be life-threatening. Discontinue ProAir® RespiClick and institute alternative therapy if paradoxical bronchospasm occurs
7���##"�$,/�*,/#�",0#0�,$��/,�'/® RespiClick than usual may be a marker of acute or chronic deterioration of asthma and requires reevaluation of treatment
7���/,�'/® RespiClick alone may not be adequate to control asthma in many patients. Early consideration should be given to adding anti-infl ammatory agents, e.g., corticosteroids
7���/,�'/® RespiClick, like other beta-adrenergic agonists, can produce clinically signifi cant cardiovascular effects in some patients, as measured by heart rate, blood pressure, and/or symptoms. If such effects occur, the drug may need to be discontinued
7���/,�'/® RespiClick, as with all sympathomimetic amines, should be used with caution in patients with cardiovascular disorders (especially coronary insuffi ciency, cardiac arrhythmias, and hypertension), convulsive disorders, hyperthyroidism, and diabetes
7����1�)'1'#0�&�3#� ##+�/#-,/1#"�'+��00,!'�1',+�4'1&�#5!#00'3#�20#�,$�'+&�)#"�06*-�1&,*'*#1'!�drugs in patients with asthma. Do not exceed the recommended dose
7���**#"'�1#�&6-#/0#+0'1'3'16�/#�!1',+0�*�6�,!!2/���'0!,+1'+2#��/,�'/® RespiClick immediately
In two observational studies, 33% to 67% of patients using pMDIs* had poor hand–breath coordination during inhalation1,2
A spacer is intended to help with pMDI use, but you or your patients may be looking for an option that doesn’t rely on a separate device to help3
A breath-actuated inhaler, like ProAir® RespiClick (albuterol sulfate) Inhalation Powder, is an option to consider for these patients
ProAir® and RespiClick™ are trademarks owned by Teva Respiratory, LLC.
©2015 Teva Respiratory, LLC PRS-40374

Learn more at ProAir.com
For Your Appropriate Patients
References: 1. Giraud V, Roche N. Misuse of corticosteroid metered-dose inhaler is associated with decreased asthma stability. Eur Respir J. 2002;19(2):246-251. 2. Khassawneh BY, Al-Ali MK, Alzoubi KH, et al. Handling of inhaler devices in actual pulmonary practice: metered-dose inhaler versus dry powder inhalers. Resp Care. 2008;53(3):324-328. 3. National Asthma Education and Prevention Program (NAEPP). Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma—Full Report 2007. Bethesda, MD: US Department of Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute; August 2007. 4. Dolovich MB, Ahrens RC, Hess DR, et al. Device selection and outcomes of aerosol therapy: evidence-based guidelines: American College of Chest Physicians/American College of Asthma, Allergy, and Immunology. Chest. 2005;127(1):335-371.
Important Safety Information (continued)4���*'�"*®���+("�$"�#���$�-,�*'$�+-$��,����&!�$�,"'&��'/��*�%�1�(*'�-���+" &"7���&,�!1('#�$�%"��"&�+'%��(�,"�&,+��/!"�!�!�+�,!��(',�&,"�$�,'�(*'�-�����.�*+����*�"'.�+�-$�*������,+���!�����*��+��"+�-+-�$$1�,*�&+"�&,��&',�*�)-"*"& �+-(($�%�&,�,"'&
4���',�&,"�$��*- �"&,�*��,"'&+���&�'��-*�/",!���,���$'�#�*+���"-*�,"�+���" '0"&��'*�%'&'�%"&��'0"��+��"&!"�",'*+���&��,*"�1�$"���&,"��(*�++�&,+
4���&��'&,*'$$���+,-�"�+�'���*'�"*®���+("�$"�#����.�*+���.�&,+�,!�,�'��-**����,��&�"&�"��&���*�,��'���,�$��+,����&�� *��,�*�,!�&�($����'�"&�$-�������#�(�"&����.+�����(�"&����.+������ �+,*'�&,�*","+�."*�$����.+������+"&-+�!�����!�����.+�������&�8-*"&�*1�,*��,�"&���,"'&����.+����
Please see Brief Summary of full Prescribing Information on following pages.
* (��� (*�++-*"2���%�,�*����'+��"&!�$�*�† ���� +!'*,���,"& ���,��� '&"+,�
�!��'&$1������((*'.����%-$,"��'+���*�+�-��"&!�$�*�+(��"7���$$1���+" &���,'��$"%"&�,��,!��&�����'*�!�&�6�*��,!��''*�"&�,"'&��-*"& 8"&!�$�,"'&
4�����*��,!���,-�,���"&!�$�*���+" &���,'����-+���/",!'-,���+(���*4
�*�&+","'&�1'-*��((*'(*"�,��(�,"�&,+��*'%���(���������"&!�$�*�,'
���*&�%'*���,��*'�"*��'%

BRIEF SUMMARY OF PRESCRIBING INFORMATION FOR ProAir® RespiClick (albuterol sulfate) Inhalation PowderSEE PACKAGE INSERT FOR FULL PRESCRIBING INFORMATION1 INDICATIONS AND USAGE1.1 BronchospasmPROAIR RESPICLICK (albuterol sulfate) inhalation powder is indicated for the treatment or prevention of bronchospasm in patients 12 years of age and older with reversible obstructive airway disease.1.2 Exercise-Induced BronchospasmPROAIR RESPICLICK is indicated for the prevention of exercise-induced bronchospasm in patients 12 years of age and older. 4 CONTRAINDICATIONSUse of PROAIR RESPICLICK is contraindicated in patients with a history of hypersensitivity to albuterol and/or severe hypersensitivity to milk proteins. Rare cases of hypersensitivity reactions, including urticaria, angioedema, and rash have been reported after the use of albuterol sulfate. There have been reports of anaphylactic reactions in patients using inhalation therapies containing lactose [see Warnings and Precautions (5.6)].5 WARNINGS AND PRECAUTIONS5.1 Paradoxical BronchospasmPROAIR RESPICLICK can produce paradoxical bronchospasm that may be life threatening. If paradoxical bronchospasm occurs, PROAIR RESPICLICK should be discontinued immediately and alternative therapy instituted.5.2 Deterioration of AsthmaAsthma may deteriorate acutely over a period of hours or chronically over sev-eral days or longer. If the patient needs more doses of PROAIR RESPICLICK, this may be a marker of destabilization of asthma and requires re-evaluation of the patient and treatment regimen, giving special consideration to the possible need for anti-inflammatory treatment, eg, corticosteroids.5.3 Use of Anti-Inflammatory AgentsThe use of beta-adrenergic-agonist bronchodilators alone may not be adequate to control asthma in many patients. Early consideration should be given to add-ing anti-inflammatory agents, eg, corticosteroids, to the therapeutic regimen.5.4 Cardiovascular EffectsPROAIR RESPICLICK, like other beta-adrenergic agonists, can produce clinically significant cardiovascular effects in some patients as measured by pulse rate, blood pressure, and/or symptoms. Although such effects are uncommon after administration of PROAIR RESPICLICK at recommended doses, if they occur, the drug may need to be discontinued. In addition, beta-agonists have been reported to produce ECG changes, such as flattening of the T-wave, prolongation of the QTc interval, and ST segment depression. The clinical significance of these findings is unknown. Therefore, PROAIR RESPICLICK, like all sympathomimetic amines, should be used with caution in patients with cardiovascular disorders, especially coronary insufficiency, cardiac arrhythmias, and hypertension.5.5 Do Not Exceed Recommended DoseFatalities have been reported in association with excessive use of inhaled sympathomimetic drugs in patients with asthma. The exact cause of death is unknown, but cardiac arrest following an unexpected development of a severe acute asthmatic crisis and subsequent hypoxia is suspected.5.6 Immediate Hypersensitivity ReactionsImmediate hypersensitivity reactions may occur after administration of albuterol sulfate, as demonstrated by rare cases of urticaria, angioedema, rash, broncho-spasm, anaphylaxis, and oropharyngeal edema. PROAIR RESPICLICK contains small amounts of lactose, which may contain trace levels of milk proteins. Hypersensitivity reactions including anaphylaxis, angioedema, pruritus, and rash have been reported with the use of therapies containing lactose (lactose is an inactive ingredient in PROAIR RESPICLICK). The potential for hypersen-sitivity must be considered in the clinical evaluation of patients who experience immediate hypersensitivity reactions while receiving PROAIR RESPICLICK.5.7 Coexisting ConditionsPROAIR RESPICLICK, like all sympathomimetic amines, should be used with caution in patients with cardiovascular disorders, especially coronary insuffi-ciency, cardiac arrhythmias, and hypertension; in patients with convulsive dis-orders, hyperthyroidism, or diabetes mellitus; and in patients who are unusu-ally responsive to sympathomimetic amines. Clinically significant changes in systolic and diastolic blood pressure have been seen in individual patients and could be expected to occur in some patients after use of any beta-adrenergic bronchodilator. Large doses of intravenous albuterol have been reported to aggravate preexisting diabetes mellitus and ketoacidosis.5.8 HypokalemiaAs with other beta-agonists, PROAIR RESPICLICK may produce significant hypokalemia in some patients, possibly through intracellular shunting, which has the potential to produce adverse cardiovascular effects. The decrease is usually transient, not requiring supplementation.6 ADVERSE REACTIONSUse of PROAIR RESPICLICK may be associated with the following:Ê UÊÊ*>À>`�Ý�V>�ÊLÀ��V��ë>Ã�Ê[see Warnings and Precautions (5.1)]Ê UÊÊ>À`��Û>ÃVÕ�>ÀÊ vviVÌÃÊ[see Warnings and Precautions (5.4)]Ê UÊÊ ���i`�>ÌiÊ�Þ«iÀÃi�Ã�Ì�Û�ÌÞÊÀi>VÌ���ÃÊ[see Warnings and Precautions (5.6)]Ê UÊÊ�Þ«��>�i��>Ê[see Warnings and Precautions (5.8)]
ProAir® RespiClick (albuterol sulfate) Inhalation Powder
6.1 Clinical Trials ExperienceA total of 1120 subjects were treated with PROAIR RESPICLICK during the clinical development program. The most common adverse reactions (*1% and >placebo) were back pain, pain, gastroenteritis viral, sinus headache, and uri-nary tract infection. Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug can-not be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.Adults and Adolescents 12 years of Age and Older: The adverse reaction infor-mation presented in Table 1 below concerning PROAIR RESPICLICK is derived from the 12-week blinded treatment period of three studies which compared PROAIR RESPICLICK 180 mcg four times daily with a double-blinded matched placebo in 653 asthmatic patients 12 to 76 years of age.Table 1: Adverse Reactions Experienced by Greater Than or Equal to 1.0% of Patients in the PROAIR RESPICLICK Group and Greater Than Placebo in three 12-Week Clinical Trials1
Preferred Term Number (%) of patientsPROAIR RESPICLICK
180 mcg QIDN=321
Placebo
N=333
Back pain 6 (2%) 4 (1%)
Pain 5 (2%) 2 (<1%)
Gastroenteritis viral 4 (1%) 3 (<1%)
Sinus headache 4 (1%) 3 (<1%)
Urinary tract infection 4 (1%) 3 (<1%)1. This table includes all adverse events (whether considered by the investigator drug related or unrelated to drug) which occurred at an incidence rate of greater than or equal to 1.0% in the PROAIR RESPICLICK group and greater than placebo.
In a long-term study of 168 patients treated with PROAIR RESPICLICK for up to 52 weeks (including a 12-week double-blind period), the most commonly reported adverse events greater than or equal to 5% were upper respiratory infection, nasopharyngitis, sinusitis, bronchitis, cough, oropharyngeal pain, headache, and pyrexia.In a small cumulative dose study, tremor, palpitations, and headache were the most frequently occurring (*5%) adverse events. 6.2 Postmarketing ExperienceIn addition to the adverse reactions reported from clinical trials with PROAIR RESPICLICK, the following adverse events have been reported during use of other inhaled albuterol sulfate products: Urticaria, angioedema, rash, broncho-spasm, hoarseness, oropharyngeal edema, and arrhythmias (including atrial fibrillation, supraventricular tachycardia, extrasystoles), rare cases of aggra-vated bronchospasm, lack of efficacy, asthma exacerbation (potentially fatal), muscle cramps, and various oropharyngeal side-effects such as throat irritation, altered taste, glossitis, tongue ulceration, and gagging. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure.In addition, albuterol, like other sympathomimetic agents, can cause adverse reactions such as: angina, hypertension or hypotension, palpitations, central nervous system stimulation, insomnia, headache, nervousness, tremor, muscle cramps, drying or irritation of the oropharynx, hypokalemia, hyperglycemia, and metabolic acidosis.7 DRUG INTERACTIONSOther short-acting sympathomimetic bronchodilators should not be used concomitantly with PROAIR RESPICLICK. If additional adrenergic drugs are to be administered by any route, they should be used with caution to avoid deleterious cardiovascular effects.7.1 Beta BlockersBeta-adrenergic-receptor blocking agents not only block the pulmonary effect of beta-agonists, such as PROAIR RESPICLICK, but may produce severe bronchospasm in asthmatic patients. Therefore, patients with asthma should not normally be treated with beta-blockers. However, under certain circumstances, eg, as prophylaxis after myocardial infarction, there may be no acceptable alternatives to the use of beta-adrenergic-blocking agents in patients with asthma. In this setting, consider cardioselective beta-blockers, although they should be administered with caution.7.2 DiureticsThe ECG changes and/or hypokalemia which may result from the administration of non-potassium sparing diuretics (such as loop or thiazide diuretics) can be acutely worsened by beta-agonists, especially when the recommended dose of the beta-agonist is exceeded. Although the clinical significance of these effects is not known, caution is advised in the coadministration of beta-agonists with non-potassium sparing diuretics. Consider monitoring potassium levels.7.3 DigoxinMean decreases of 16% and 22% in serum digoxin levels were demonstrated after single dose intravenous and oral administration of albuterol, respectively, to normal volunteers who had received digoxin for 10 days. The clinical signif-

icance of these findings for patients with obstructive airway disease who are receiving albuterol and digoxin on a chronic basis is unclear. Nevertheless, it would be prudent to carefully evaluate the serum digoxin levels in patients who are currently receiving digoxin and PROAIR RESPICLICK.7.4 Monoamine Oxidase Inhibitors or Tricyclic AntidepressantsPROAIR RESPICLICK should be administered with extreme caution to patients being treated with monoamine oxidase inhibitors or tricyclic antidepressants, or within 2 weeks of discontinuation of such agents, because the action of albuterol on the cardiovascular system may be potentiated. Consider alterna-tive therapy in patients taking MAO inhibitors or tricyclic antidepressants.8 USE IN SPECIFIC POPULATIONS8.1 PregnancyTeratogenic Effects: Pregnancy Category C:There are no adequate and well-controlled studies of PROAIR RESPICLICK or albuterol sulfate in pregnant women. During worldwide marketing experience, various congenital anomalies, including cleft palate and limb defects, have been reported in the offspring of patients treated with albuterol. Some of the mothers were taking multiple medications during their pregnancies. No consistent pat-tern of defects can be discerned, and a relationship between albuterol use and congenital anomalies has not been established. Animal reproduction studies in mice and rabbits revealed evidence of teratogenicity. PROAIR RESPICLICK should be used during pregnancy only if the potential benefit justifies the poten-tial risk to the fetus.In a mouse reproduction study, subcutaneously administered albuterol sul-fate produced cleft palate formation in 5 of 111 (4.5%) fetuses at an exposure approximately eight-tenths of the maximum recommended human dose (MRHD) for adults on a mg/m2 basis and in 10 of 108 (9.3%) fetuses at approximately 8 times the MRHD. Similar effects were not observed at approximately one-thirteenth of the MRHD. Cleft palate also occurred in 22 of 72 (30.5%) fetuses from females treated subcutaneously with isoproterenol (positive control).In a rabbit reproduction study, orally administered albuterol sulfate induced cranioschisis in 7 of 19 fetuses (37%) at approximately 630 times the MRHD.In a rat reproduction study, an albuterol sulfate/HFA-134a formulation admin-istered by inhalation did not produce any teratogenic effects at exposures approximately 65 times the MRHD.Non-Teratogenic Effects: A study in which pregnant rats were dosed with radio-labeled albuterol sulfate demonstrated that drug-related material is transferred from the maternal circulation to the fetus. 8.2 Labor and DeliveryBecause of the potential for beta-agonist interference with uterine contractility, use of PROAIR RESPICLICK for relief of bronchospasm during labor should be restricted to those patients in whom the benefits clearly outweigh the risk. PROAIR RESPICLICK has not been approved for the management of pre-term labor. The benefit:risk ratio when albuterol is administered for tocolysis has not been established. Serious adverse reactions, including pulmonary edema, have been reported during or following treatment of premature labor with beta2- agonists, including albuterol.8.3 Nursing MothersPlasma levels of albuterol after inhaled therapeutic doses are very low in humans, but it is not known whether the components of PROAIR RESPICLICK are excreted in human milk.Caution should be exercised when PROAIR RESPICLICK is administered to a nursing woman. Because of the potential for tumorigenicity shown for albuterol in animal studies and lack of experience with the use of PROAIR RESPICLICK by nursing mothers, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.8.4 Pediatric UseThe safety and effectiveness of PROAIR RESPICLICK for the treatment or preven-tion of bronchospasm in children 12 to 17 years of age and older with reversible obstructive airway disease is based on two 12-week clinical trials in 318 patients 12 years of age and older with asthma comparing doses of 180 mcg four times
ProAir® RespiClick (albuterol sulfate) Inhalation Powder
daily with placebo, one long-term safety study in children 12 years of age and older, and one single-dose crossover study comparing doses of 90 and 180 mcg with albuterol sulfate inhalation aerosol (ProAir® HFA) in 71 patients [see Clini-cal Studies (14.1) in full Prescribing Information]. The safety and effectiveness of PROAIR RESPICLICK for treatment of exercise-induced bronchospasm in children 12 years of age and older is based on one single-dose crossover study in 38 patients age 16 and older with exercise-induced bronchospasm compar-ing doses of 180 mcg with placebo [see Clinical Studies (14.2) in full Prescrib-ing Information]. The safety profile for patients ages 12 to 17 was consistent with the overall safety profile seen in these studies.The safety and effectiveness of PROAIR RESPICLICK in pediatric patients below the age of 12 years have not been established. Overall, 120 children with asthma ages 4 to 11 years have participated in the PROAIR RESPICLICK clini-cal program, including 76 patients evaluated in 2 single-dose crossover clinical trials comparing PROAIR RESPICLICK to ProAir HFA at doses up to 180 mcg. 8.5 Geriatric UseClinical studies of PROAIR RESPICLICK did not include sufficient numbers of patients aged 65 and over to determine whether they respond differently from younger patients. Other reported clinical experience has not identified differ-ences in responses between elderly and younger patients. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy [see Warnings and Precautions (5.4, 5.7)].All beta2-adrenergic agonists, including albuterol, are known to be substantially excreted by the kidney, and the risk of toxic reactions may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.10 OVERDOSAGEThe expected symptoms with overdosage are those of excessive beta-adrenergic stimulation and/or occurrence or exaggeration of any of the symptoms listed under ADVERSE REACTIONS, eg, seizures, angina, hypertension or hypoten-sion, tachycardia with rates up to 200 beats per minute, arrhythmias, nervous-ness, headache, tremor, dry mouth, palpitation, nausea, dizziness, fatigue, malaise, and insomnia.Hypokalemia may also occur. As with all sympathomimetic medications, cardiac arrest and even death may be associated with abuse of PROAIR RESPICLICK.Treatment consists of discontinuation of PROAIR RESPICLICK together with appropriate symptomatic therapy. The judicious use of a cardioselective beta-receptor blocker may be considered, bearing in mind that such medica-tion can produce bronchospasm. There is insufficient evidence to determine if dialysis is beneficial for overdosage of PROAIR RESPICLICK.
Marketed by: Teva Respiratory, LLCHorsham, PA 19044Manufactured by: Teva Pharmaceutical Industries Ltd.Jerusalem, IsraelCopyright ©2015, Teva Respiratory, LLCAll rights reserved.ProAir® and RespiClick™ are trademarks owned by Teva Respiratory, LLCThis brief summary is based on the ProAir RespiClick full prescribing information dated March 2015.PRS-40076 March 2015
ProAir® RespiClick (albuterol sulfate) Inhalation Powder

MedicalEconomics.com24 MEDICAL ECONOMICS ❚ JUNE 25, 2016
Operations Direct pay
considers it a worthwhile investment of his time if it
helps promote and grow the DPC move-ment and raise public awareness of how it works.
Gold modeled his fee structure after Atlas MD, with five membership tiers based on age, ranging from $30 to $125 per month. The fee includes all office vis-its, unlimited communication with phy-sicians, same or next-day appointments, and discounts on labs, procedures and prescription medications.
Some DPC practitioners, including Gunther, charge a flat monthly rate to all patients, regardless of age. However, all practices share a commitment to keep-ing fees low enough to be affordable to most patients.
In 2015, almost 60% of the patients in DPC practices earned household in-comes of less than $95,000, which is still above the median but less than the aver-age at concierge practices, which ranges from $125,000 to $250,000, according to data collected by industry trade publica-tions DPC Journal and Concierge Medicine
Today. On average, the majority (68%) of DPC practices surveyed charge fees rang-ing from $25 to $85 per month.
Besides low fees, DPC practices tend to maintain small patient panels, the journal reports. As of June 2015, 60% of practices had panels of fewer than 300, although the goal is more than that. (Gold hopes to reach 600-800 per physi-cian.)
FINANCING THE START-UPFinancing can be a major barrier for many physicians looking to transition from tra-ditional fee-for-service practice to a rela-tively new model. According to Atlas MD, purchasing equipment such as EKG ma-chines, ultrasound, lasers or bone scan-ners can cost about $250,000. The other major cost is leasing and furnishing an office, which varies by location.
However, notes Umbehr, most of that equipment is optional or can be leased, and physicians can add items as their budget allows rather than purchase ev-erything at once.
Gold’s situation is unusual: he ob-
19
The Direct Primary Care Journal, an industry
trade publication, monitors developments in
the direct primary care industry. The following
are some of its key findings from data collected
between December 2012 and June 2015.
DIRECT PRIMARY CARE
MARKET PROFILE
Defining characteristics Monthly fees; no insurance accepted.
Setting 19% of DPC doctors practice in a group setting while nearly 81% operate solo practices. Most DPC clinics have one to three employees.
Fees The majority (68%) of DPC practices charge between $25 and $85 a month. For comparison, the average at concierge practices is about $182/month, according to a 2015 survey of 141 practices in 39 states published in the Journal of the American Board of Family Medicine.
Financial stability 90% of DPC physicians indicated that their practices are doing better financially compared with the previous year.
Home visits Nearly 50% of DPC physicians polled in 2014-2015 provided home visits, which are included in the monthly patient subscriber fee. Thirty-eight percent indicated they do not provide home visits while 12% charge an additional but nominal fee for home care visits.
Specialties Over 80% of DPC practices are run by family medicine or internal medicine physicians.
Future growth Based on interviews with industry experts, investors and DPC physicians, the growth rate for DPC practices should be roughly 5%-9% over the next few years.

MedicalEconomics.com 25 MEDICAL ECONOMICS ❚ JUNE 25, 2016
OperationsDirect pay
tained start-up funding from a wealthy pa-tient who was interested in supporting the DPC movement. The patient loaned Gold about $400,000 at a reasonable interest rate and terms specifying payback at 75% of practice profits until paid off. He used the money for office space, new equipment and salary support in the practice’s first year.
As a result, Gold was able to avoid taking on a high-interest bank loan and didn’t have to worry about closing his doors in the early months when patient enrollment was low.
However, it’s possible to make the transi-tion without that kind of help, says Gunther, who opened her DPC office in June 2014. By scrimping and saving during the early months, she managed to break even in Janu-ary of this year.
“My business plan revolved around mak-ing it through the first three years,” says Gun-ther. “We put more personal finances into it than we planned but I’m definitely happier now because I can be the kind of physician I want to be.”
In addition, DPC offers savings over tra-ditional practice models that balance out some of the start-up costs, says Umbehr. For example, DPC practices do not need extra staff to handle third-party billing and they can eliminate the cost of pharmacy services by purchasing medications at wholesale rates and dispensing them from their of-fices.
Physicians are often hesitant at first to es-tablish an in-house pharmacy even though most states allow doctors to dispense con-trolled substances internally, he says. How-ever, negotiating wholesale prices with labs and drug companies and selling directly to patients are keys to staying profitable.
Wholesale discounts can be quite sub-
stantial—up to 95% off retail costs—making the cost to patients less than a typical insur-ance copayment, says Umbehr. For example, Atlas charges $4.60 for a complete metabolic panel compared with $52 retail, according to the price list posted on its website, and passes along wholesale discounts on pre-scription drugs to its patients.
“We get our medications from the same wholesalers as the pharmacies do,” he says. “Everything is transparent—our patients see all of our costs and prices and can decide for themselves whether to choose generic or brand-name medications.”
Physicians can also provide greater value to patients by performing common proce-dures in-house, says Umbehr. Atlas includes
Direct Primary Care Resources❚ DPC Frontier: an online resource maintained by healthcare
consultant Philip Eskew, DO, JD, MBA, also offers guidance and tips to physicians interested in starting a DPC practice.
❚ Direct Primary Care Journal: An online trade publication that publishes news and educational resources for physicians and patients.
❚ Direct Primary Care Coalition: An advocacy group that lobbies for policy changes favoring the DPC movement.
❚ The Docpreneur Institute: An Atlanta, Georgia-based mentoring and coaching facility run by Concierge Medicine Today. Offers meetings, classes, and educational materials.
❚ Atlas MD: Founder Josh Umbehr created an online curriculum that walks physicians through the steps of launching a DPC practice and answers many common questions.
One day I realized I was actually annoyed at a patient for talking too long and realized it wasn’t
really her I was annoyed with, but a healthcare system that gives me about 10 minutes with each patient.”
— JEFFREY GOLD, MD, OWNER, GOLD DIRECT CARE, MARBLEHEAD, MASSACHUSETTS

MedicalEconomics.com26 MEDICAL ECONOMICS ❚ JUNE 25, 2016
Operations Direct pay
procedures such as EKGs, spirometry, lesion removal and blood sugar testing, among others, in patients’ membership fees.
GROWING REVENUEOne of the toughest parts about getting started as a DPC practice is convincing cur-rent and prospective patients of its benefits. Consumers often assume that membership practices are more expensive than fee-for-service primary care and often equate DPC with concierge models.
It’s helpful to put the costs into per-spective when talking to prospective pa-tients, says Gold, noting that the price of DPC membership is roughly the same as a monthly cell phone bill. When paired with catastrophic insurance coverage for serious events and emergency department visits, membership can provide comprehensive primary care and full access to physicians at a cost that is often less than a traditional insurance plan, he says.
However, not all patients from his pre-vious employment were convinced by the value proposition of DPC, says Gold. Only about 100 out of 2,500 patients chose to join the new practice.
“It was very difficult emotionally,” he re-calls. “You feel rejected and abandoned by patients that you might have gone through a cancer diagnosis with. Despite all the finan-cial challenges of this transition, the hardest part was the emotional aspect of patients not sticking with me.”
Legislative issues also have slowed growth of the DPC movement. For example,
although the Affordable Care Act defines DPC as a primary care service, current IRS policy treats it as health insurance because of the monthly fee structure. That prevents patients from using their health savings accounts (HSAs) for DPC membership be-cause HSA funds cannot be used to pur-chase insurance.
However, changes are in the works. About a dozen states have adopted legislation that clearly defines DPCs as non-insurance ar-rangements that qualify as medical expens-es payable through HSAs. Similar legislation has been introduced at the federal level.
In addition, federal regulators have yet to define the criteria under which a DPC prac-tice would qualify as a primary care medi-cal home on state and federal healthcare exchanges. That uncertainty has prevented many large insurers from creating so-called wraparound plans for the exchanges, which would pair DPC with catastrophic coverage.
“Our goal is to have insurers start writ-ing policies that are true wraparounds with DPC,” says Gold. “Then I, as a DPC provider, could be on the state exchange as a product and insurers would save money by eliminat-ing spending on routine care.”
Another avenue for growth is market-ing to employers, says Umbehr. DPC can be an appealing option for companies looking to reduce healthcare costs by allowing em-ployees to pair DPC membership with high-deductible plans. “We can help an employer reduce its insurance premiums by 30%-60% in the first year,” says Umbehr. “Because we remove the cost of working with insurers.”
My business plan revolved around making it through the first three years.
We put more personal finances into it than we planned but I’m definitely happier now because I can be the kind of physician I want to be.”
—JULIE GUNTHER, MD, DIRECT FAMILY PHYSICIAN, BOISE, IDAHO

†*
Strong pain relief, without the dosing gap.
Recommend ALEVE®, with the strength of naproxen sodium. Give your patients all-day relief from minor OA pain with just 2 doses.
For patients with minor OA pain
A 6-hour dosing gap can be a painful experience.
* Reflects latest OTC label dosing for Extra Strength Tylenol for adults and children 12 years and older—maximum daily dose reduced from 8 pills (4000 mg) to 6 pills (3000 mg), with a dosing interval change from every 4 to 6 hours to every 6 hours, unless directed by a doctor.
† Each ALEVE tablet can last 12 hours.
Use as directed. ALEVE is indicated for minor arthritis pain.OA=osteoarthritis.
The Bayer Cross, ALEVE, and All Day Strong are registered trademarks of Bayer. Tylenol is a registered trademark of Johnson & Johnson.
© 2016 Bayer February 2016 61736-PP-AL-BASE-US-0908
Strong on pain. Long on relief.
7���'$��51/ ��1/$,&1'��6*$,-*® label warns about acetaminophen
overdose if patients take more than 4 g a day
7���-� ##/$00�1'(0� (002$�� (1�3-*2,1 /(*6� /$#2"$#� (10�# (*6�#-0$�
from 4 g to 3 g—so patients may experience a 6-hour gap
when pain persists for 24 hours

MedicalEconomics.com28
IN DEPTH
MEDICAL ECONOMICS ❚ JUNE 25, 2016
Amid rising deaths due to prescription painkillers, doctors are fi nding alternative ways to help patients manage chronic pain by JEFFREY BENDIX Senior Editor
GARY LEROY, MD, dreads the early-morning phone call from the coroner’s offi ce—the one where he learns that a patient who has been taking opioids has died in his sleep.
LeRoy, a family practitioner in Dayton, Ohio, prescribes opioids carefully. He orders them only in small quantities and for limited periods, and in-structs patients in how to use them. But patients don’t always tell him what medications they are get-ting from other prescribers. Nor can he stop them from getting drugs from friends and family mem-bers, or buying them on the street.
Th e result, if the drugs are used in the wrong combination, is the notifi cation from the coroner. “Th at kind of call really gnaws at you,” he says.
Experts agree opioid use in the U.S. is out of con-trol—and primary care doctors are writing most of the prescriptions. A study of 2013 Medicare Part D
claims found that internists and family practitio-ners accounted for over half of the 54.5 million pre-scriptions written for Schedule II opioids that year.
Like LeRoy, most primary care doctors take their prescribing responsibilities seriously. Indeed, 84% say they are “very” or “moderately” concerned about the possibility of opioid addiction among their patients, and 80% about the possibility of death, according to a 2015 survey.
Yet as the main providers of healthcare to most Americans, primary care doctors are who patients turn to fi rst when seeking relief from pain. Th e question now is, how do primary care providers be-come part of the solution? How do they minimize the number of opioids they dispense and reduce the number of people dependent on them, while still helping to ease the chronic pain millions of Ameri-cans experience?
D.C. CornerDoctors support legislation to help
slow the opioid epidemic—so
long as politicians don’t meddle
with treatment decisions [38]
How did we get here?The opioid crisis was caused in
part by a desire among providers
and drug manufacturers to
address patient pain [35]
CDC guidelinesNew recommendations for
primary care physicians on
how they should handle opioid
treatments [31]
PolicyIN
SIDE

MedicalEconomics.com 29MEDICAL ECONOMICS ❚ JUNE 25, 2016
PHYSICIANS WEIGH IN ON THE OPIOID CRISIS
Q:
Q:
Q:
Q:
Q:
EXCLUSIVE READER POLL
In your opinion, who is responsible for the increasing use of opioids?
Compared with five years ago, are you seeing
Do you ever refuse patient requests for opioid prescriptions?
Do you currently prescribe opioids to any of your patients?
What is (are) the main reason(s) why your patients request opioids?
If “yes,” is it due to:
Physicians
23%
52%
25%
The pharmaceutical industry
Patients
54%
13%
33%
More requests for opioid prescriptions?
Fewer requests?
About the same number?22%
18%
60%
concern that the patient is becoming dependent on opioids?
patient’s pain is not severe enough to require them?
patient can be treated more effectively using other medications or therapies not involving medication?
47% 12% 23% 18%
back pain headaches to relieve pain following surgery
or an accident
other
YES 97% NO 3%
YES 89% NO 11%
Source: Medical Economics reader poll
THE OPIOID CRISIS
OVERDOSE DEATHS ON THE RISETh e magnitude of the problem is diffi cult to overstate. According to the CDC:
❚ more than 165,000 Americans died from
overdoses related to prescription opioids
between 1999 and 2014, with 14,000 of those
deaths occurring in 2014 alone.
❚ Per-capita opioid prescriptions grew by 7.3%
between 2007 and 2012, with prescribing
rates among internists and family practitioners
rising faster than other specialties,
❚ In 2014 about two million people abused or
were dependent on prescription opioids
❚ More than one thousand people per day
are treated in emergency departments for
misusing prescription opioids
❚ Opioid dependence among primary care
patients receiving prescriptions for treating pain
not related to cancer may be as high as 26%.
Amid the sobering statistics, however, are signs that opioid use may be levelling off . A state-by-state survey of opioid use by IMS Health, a healthcare data company, found a 6.8% decline in the number of opioid prescrip-tions fi lled in the U.S. between 2014 and 2015.
Even so, the 2015 total—nearly 228 mil-lion, or an average of 0.7 per person—re-mains startlingly large.
Apart from the damage that opioids can infl ict on their own, they correlate strongly

MedicalEconomics.com30 MEDICAL ECONOMICS ❚ JUNE 25, 2016
with increased heroin use and addiction. Th is is because heroin is often cheaper and easier to acquire than opioids in many plac-es around the country. A 2013 study from the Center for Behavioral Health Statistics and Quality found “a strong association between prior nonmedical use of pain relievers [opi-oids] and the subsequent past year initiation of heroin use.”
Th e rapid increases in opioid use and ad-diction have drawn the attention of the pres-ident, Congress and policymakers. In Feb-ruary President Obama proposed adding $1.1 billion to address prescription opioid abuse. Meanwhile, by mid-May both houses of Congress had passed legislation designed to slow the spread of opioid and heroin ad-diction, and Washington insiders expected a unifi ed bill to go to the president for his signature shortly thereafter.
Perhaps most signifi cantly for physicians, in March the Centers for Disease Control and Prevention (CDC) issued a guideline for prescribing opioids. Intended mostly for pri-mary care providers, it consists of 12 specif-ic recommendations for when, how and to whom physicians should prescribe opioids other than for cancer treatment, and pallia-tive and end-of-life care.
“Th e guideline communicates that we shouldn’t be treating common conditions with opioids on a routine basis. And this is the fi rst time the medical community is get-ting that message from the federal govern-ment,” says Andrew Kolodny, MD, executive director of Physicians for Responsible Opi-oid Prescribing (PROP).
Even so, some physicians remain too quick to prescribe these powerful medica-tions, even if it’s for the right reasons, says Th omas Tape, MD, FACP, professor of inter-nal medicine at the University of Nebraska-Lincoln, chair of the American College of Physicians Board of Regents, and the Amer-ican College of Physician’s liaison to the CDC committee that wrote the guideline.
“I think there hasn’t been enough atten-tion paid to how easy it is to become depen-dent on opioids,” he says. “As a physician you naturally want to alleviate pain, so if you’re not sure exactly how long that patient will re-quire severe analgesic control you’re going to err on the side of being a little more generous.”
CHRONIC VS ACUTE PAINBalancing the desire to alleviate pain
against the dangers opioids pose is but one of the thorny issues PCPs must confront when considering whether to prescribe opi-oids, and why some providers are reluctant to treat patients who have been prescribed them previously. Challenges include fi nding eff ective alternative therapies for patients experiencing chronic pain, monitoring pa-tients who take opioids and fi nding success-ful tapering strategies for the users.
Like most physicians, Tape distinguish-es between acute and chronic pain when thinking about opioid prescribing. Th e for-mer, he says, generally is associated with severe tissue damage resulting from trauma, an accident or surgery and doesn’t require prolonged opioid use.
However, when pain is chronic—a con-dition that the CDC defi nes as lasting three months or more—the calculus changes. Th is type of pain is more likely to stem from a central nervous system issue, Tape says, and in such cases opioids are not as eff ective as they are in treating acute pain.
In Tape’s clinical practice, the vast ma-jority of patients requesting opioids began getting them from previous providers for conditions such as chronic headaches, fi -bromyalgia, and back pain. If they have been using them for years, he says, it’s often very diffi cult to taper them off the medications.
Th at diffi culty is why “the non-medicinal approach to pain should always be in the forefront of a doctor’s thinking,” says Jeff ry Lindenbaum, DO, a family physician who has practiced addiction medicine in Yard-ley, Pennsylvania for 39 years. “You want to try all the other modalities fi rst before you possibly sentence someone to a lifetime of opioid therapy.”
Time and money constraints also can play a role in the decision of whether to prescribe opioids. “In the primary care environment, if you’ve got a patient who spends more than 15 minutes in the room it starts to cost you a lot of money,” says Robert Twillman, PhD, FAMP, executive director of the American Academy of Pain Management (AAPM). “Th e fastest way to get them out of the room is to write a prescription. I’m not saying that’s a conscious decision, but I think it plays a role.”
PROP, along with others who have stud-ied the problem, believes that patient sat-isfaction surveys also have played a role in the opioid epidemic. Th e organization wrote recently to
THE OPIOID CRISIS
227MILLIONNumber of U.S. opioid prescriptions written in 2015Source: IMS Health
32

MedicalEconomics.com 31MEDICAL ECONOMICS ❚ JUNE 25, 2016
Source: Centers for Disease Control and Prevention
Determining When to Initiate or Continue Opioids for Chronic Pain
Nonpharmacologic therapy and nonopioid pharmacologic
therapy are preferred for chronic pain. Clinicians should
consider opioid therapy only if expected benefi ts for both
pain and function are anticipated to outweigh risks to the
patient. If opioids are used, they should be combined with
nonpharmacologic therapy and nonopioid pharmacologic
therapy, as appropriate.
Before starting opioid therapy for chronic pain, clinicians
should establish treatment goals with all patients,
including realistic goals for pain and function, and should
consider how therapy will be discontinued if benefi ts
do not outweigh risks. Clinicians should continue opioid
therapy only if there is clinically meaningful improvement
in pain and function that outweighs risks to patient safety.
Before starting and periodically during opioid therapy,
clinicians should discuss with patients known risks
and realistic benefi ts of opioid therapy and patient and
clinician responsibilities for managing therapy.
Opioid Selection, Dosage, Duration, Follow-Up, and Discontinuation
When starting opioid therapy for chronic pain, clinicians
should prescribe immediate-release opioids instead of
extended-release/long-acting (ER/LA) opioids.
When opioids are started, clinicians should prescribe the
lowest effective dosage. Clinicians should use caution
when prescribing opioids at any dosage, should carefully
reassess evidence of individual benefi ts and risks when
increasing dosage to ≥50 morphine milligram equivalents
(MME)/day, and should avoid increasing dosage to ≥90
MME/day or carefully justify a decision to titrate dosage
to ≥90 MME/day.
Long-term opioid use often begins with treatment of acute
pain. When opioids are used for acute pain, clinicians
should prescribe the lowest effective dose of immediate-
release opioids and should prescribe no greater quantity
than needed for the expected duration of pain severe
enough to require opioids. Three days or less will often be
suffi cient; more than seven days will rarely be needed.
Clinicians should evaluate benefi ts and harms with
patients within 1 to 4 weeks of starting opioid therapy
for chronic pain or of dose escalation. Clinicians should
evaluate benefi ts and harms of continued therapy with
patients every 3 months or more frequently. If benefi ts
do not outweigh harms of continued opioid therapy,
clinicians should optimize other therapies and work with
patients to taper opioids to lower dosages or to taper and
discontinue opioids.
Assessing Risk and Addressing Harms of Opioid Use
Before starting and periodically during continuation of
opioid therapy, clinicians should evaluate risk factors for
opioid-related harms. Clinicians should incorporate into
the management plan strategies to mitigate risk, including
considering offering naloxone when factors that increase
risk for opioid overdose, such as history of overdose,
history of substance use disorder, higher opioid dosages
(≥50 MME/day), or concurrent Benzodiazepine use, are
present.
Clinicians should review the patient’s history of controlled
substance prescriptions using state prescription drug
monitoring program (PDMP) data to determine whether
the patient is receiving opioid dosages or dangerous
combinations that put him or her at high risk for overdose.
Clinicians should review PDMP data when starting opioid
therapy for chronic pain and periodically during opioid
therapy for chronic pain, ranging from every prescription
to every 3 months.
When prescribing opioids for chronic pain, clinicians
should use urine drug testing before starting opioid
therapy and consider urine drug testing at least annually
to assess for prescribed medications as well as other
controlled prescription drugs and illicit drugs.
Clinicians should avoid prescribing opioid pain
medication and benzodiazepines concurrently whenever
possible.
Clinicians should offer or arrange evidence-based
treatment (usually medication-assisted treatment with
buprenorphine or methadone in combination with
behavioral therapies) for patients with opioid use disorder.
CDC recommendations for prescribing opioids for chronic pain outside of active cancer, palliative and end-of-life care
THE OPIOID CRISIS

MedicalEconomics.com32 MEDICAL ECONOMICS ❚ JUNE 25, 2016
LA
MS AL
SC
MI
KYWV
OKAR
TN
TOP 10 STATES
1. Alabama2. Tennessee3. West Virginia4. Arkansas5. Mississippi6. Louisiana7. Oklahoma8. Kentucky9. Michigan10. South Carolina
Source: IMS Health
most per capita opioid prescriptions, 2015
Andy Slavitt, acting adminis-trator of the Centers for Medi-
care & Medicaid Services, asking to have questions regarding pain management re-moved from the Hospital Consumer Assess-ment of Healthcare Providers and Systems (HCAHPS) survey.
Noting that hospitals are “fi nancially in-centivized” to score highly on the HCAHPS surveys, the letter—which was signed by 57 other organizations--says that questions re-garding pain treatment “have had the unin-tended consequence of encouraging aggres-sive opioid use in hospitalized patients and upon discharge.” It cites a 2014 study in the Journal of Hospital Medicine that found that doctors prescribe opioids in more than half of 1.14 million nonsurgical admissions.
PAIN MANAGEMENT SPECIALISTSSometimes PCPs will refer patients experi-encing chronic pain to pain management specialists. But doing so can be frustrating, notes Wanda Filer, MD, FAAFP, president of the American Academy of Family Physi-cians. Iff the specialist can’t perform an epi-dural or some other procedure, or the pro-cedure doesn’t work they send them back to the primary care doctor.
Filer’s assessment is “absolutely correct,” says David Craig, PharmD, a former board member of the American Pain Society. Th e problem for his members, he says, is fi nan-cial. Many pain specialists are highly-paid anesthesiologists. “Th ey go for training in this specialty in order to make more money. But writing scripts or talking to patients for an hour doesn’t pay a lot. So if you want to maintain that $400,000 salary you need to do something that’s procedure-based.”
IMPORTANCE OF COMPLETE MEDICAL PICTUREEven more than with most patients, treat-ing those who use opioids requires getting a comprehensive medical picture of the pa-tient, and especially all the medications he or she is using. Th at’s because patients ex-periencing chronic pain frequently also suf-fer from other conditions such as insomnia, depression and diabetes, notes Tape.
Often these patients are taking numer-ous medications prescribed by multiple pro-viders—not to mention those the patients acquire on their own. Th e wrong combina-tion, such as opioids and benzodiazepine,
can be lethal, says Leroy, because both act to suppress the body’s breathing refl ex—hence the many opioid-related deaths that occur during sleep. Th e eff ect is strengthened by alcohol use, he adds.
Th at danger makes it essential to review patient medications regularly, says Linden-baum. “Every time a patient comes in, the fi rst thing my medical assistant does is get a good history of what they are taking,” he says. “Th at includes over-the-counter medi-cations and the ones they ‘borrowed’ from their best friend and the drugs they stole from someone’s medicine cabinet.”
USER AGREEMENTSMost physicians who prescribe opioids re-quire patients to sign a contract, or user agreement, spelling out the patient’s respon-sibilities, such as undergoing random urine testing or getting their prescriptions fi lled at designated pharmacies, as well as the conse-quences of violating the agreement.
Patients in Tape’s clinical practice are re-quired as part of their agreement to attend a monthly class taught by a behavioral medi-cine specialist and a pharmacist. Th e former focuses on techniques for managing chronic pain, such as exercises and behavioral thera-py, that don’t involve medications. Th e latter educates patients on the addictive proper-ties of opioids and the eff ect of mixing them with other medications.
Th e consequences of violating a user agreement vary among practices. In some cases repeated violations may lead a physi-cian to dismiss the patient from his or her practice. But that is nearly always a last re-sort. More typical is the response of Filer, who practices in a federally qualifi ed health center in York, Pennsylvania. If a urine test on one of her patients comes back positive for drugs that shouldn’t be present (or nega-tive for drugs that should be there), she’ll stop prescribing the medication.
“Th e goal [of the user agreement] is for them to understand their role and my role,” she says. “And when we say we’re done [pre-scribing] there’s a reason for it. We’re trying to keep them safe and give them the best care while also protecting the health of the community.”
STATES LEND A HANDIn recent years states have been helping to reduce deaths from 35
THE OPIOID CRISIS
30

MedicalEconomics.com 35MEDICAL ECONOMICS ❚ JUNE 25, 2016
opioid combinations, as well as “doctor shopping,” by creat-
ing electronic databases of controlled sub-stances called prescription drug monitoring programs (PDMPs.) PDMPs enable doctors to get a picture of all the prescription drugs a patient is taking before writing (or refi lling) an opioid prescription, says Cynthia Reilly, director of the prescription drug abuse proj-ect of the Pew Charitable Trust.
Reilly says that consulting the PDMP be-fore prescribing opioids to a patient is one
of the most eff ective steps a PCP can take to protect the patient’s health. Still, she notes, even an up-to-date and comprehensive PDMP database will show only the medica-tions the patient has acquired legally, and only from that state. Moreover, time-pressed physicians don’t always remember to check PDMPs before writing a prescription.
To help address the latter problem, Reilly says, a majority of states now allow practic-es to delegate a non-physician to check the PDMP. “Th ey [the non-physician] can run a
32
HOW DID WE GET HERE? By Jeffrey Bendix, Senior Editor
espite the widespread—and
justifi ed--alarm about increased
opioid use and addiction, the med-
ications are not new to America.
According to a 2015 paper in the
Annual Review of Public Health, opium and
morphine use was common for much of the
19th century, largely because there were
few alternatives for treating pain.
By the early years of the 20th century,
however, opioid use had started to de-
cline, and with a few brief exceptions it
remained fairly low throughout the century.
So how did the U.S. get to the point where
259 million prescriptions were written for
opioid pain medications in 2012, and more
than 165,000 people died from opioid-re-
lated overdoses between 1999 and 2014?
Experts who have studied the problem,
as well as clinicians on the front lines of
treating opioid addiction, point to two
developments that led to the present situa-
tion. First was the American Pain Society’s
introduction in the mid-1990s of its “Pain
as the 5th Vital Sign” campaign, designed
to persuade doctors to pay more attention
to, and do more to alleviate, patient pain.
The concept was later adopted and ampli-
fi ed by The Joint Commission and by the
U.S. Department of Veterans Affairs, the
latter as part of its broader “National Pain
Management Strategy.”
“The idea was that when you assessed
a patient, in addition to checking blood
pressure and pulse and so forth, you were
to ask how much pain the patient was
in,” explains Thomas Tape, MD, FACP,
professor of internal medicine at the
University of Nebraska-Lincoln and chair of
the American College of Physicians Board
of Regents.
The problem, he says, was asking
about pain “created the expectation among
physicians and patients that zero pain was
an achievable goal. And unfortunately,
when it comes to chronic pain, 100% relief
may not be an achievable goal.”
Wanda Filer, MD, FAAFP, who has been
in family practice in York, Pennsylvania
for 28 years and is now president of the
American Academy of Family Physicians,
calls the fi fth vital sign campaign “well
intentioned,” but with unintended conse-
quences.
“Basically, physicians were being told
that we needed to be more aggressive
about managing pain, that opioids were
being underutilized and we needed to do
a better job,” she says. “My worry now is
that the pendulum has swung too far” in
the direction of over-prescribing, she adds.
The second, and more controversial,
development experts cite in explaining
the opioid crisis is the introduction and of
new and more powerful painkillers such as
OxyContin (oxycodone), and the aggressive
tactics used to market them. After several
states sued OxyContin manufacturer Pur-
due Pharma for claiming that OxyContin
was less addictive than other opioids, the
company paid a fi ne of $634 million, ac-
cording to the website drugwatch.com.
“The medical community started to pre-
scribe opioids more aggressively because
we were responding to a brilliant market-
ing campaign that minimized the risks of
opioids, especially the risk of addiction,
and exaggerated the benefi ts,” says
Andrew Kolodny, MD, executive director of
Physicians for Responsible Opioid Prescrib-
ing and a senior scientist at the Heller
School for Social Policy and Management
at Brandeis University in Massachusetts.
Moreover, OxyContin hit the market at
around the same time as the “Pain as the
5th Vital Sign” campaign was getting into
gear, Kolodny says, so the result was “if
you were a primary care provider you’re
hearing from every direction that if you’re
an enlightened, compassionate doctor you
would know that opioids can be prescribed
liberally with patients hardly ever getting
addicted.”
Others are less willing to blame the
pharmaceutical industry. Jeffry Linden-
baum, DO, a family practitioner and ad-
diction specialist in Yardley, Pennsylvania,
says pharmaceutical manufacturers have
done “a yeoman’s job” in making their
products safer. “Of course, they’re under
tremendous scrutiny from the FDA and the
public now, but I think they’re sincere in
trying to put out a product that has safety
as the number one goal and effi cacy as
number two.”
“Contrary to the idea that a phar-
maceutical rep can get a doc to write
whatever, most of the doctors I know
would not write for any medication until
it’s been out there a while,” says Sal Volpe,
MD, a Staten Island, New York internist
and Medical Economics editorial board
member. “Healthcare has a certain inertia
built into it, and that’s a good thing.”
D
THE OPIOID CRISIS

MedicalEconomics.com36 MEDICAL ECONOMICS ❚ JUNE 25, 2016
report so it’s ready for the prescriber to use when the patient is there in the examining room,” she says.
TAPERING STRATEGIESTh e ultimate goal, of course, is to get pa-tients who are taking opioids for chronic pain off of them entirely. Accomplishing that requires a two-part strategy, experts say. Th e fi rst is to fi nd an eff ective tapering strat-egy, and the second is to fi nd an alternative method for managing the patient’s pain.
Complicating the tapering challenge is the fact that long-term opioid use can in-duce opioid-induced hyperalgesia (OIH), in which the brain becomes more sensitive to pain. Consequently, Tape explains, “when you try to taper them down, they perceive their pain as actually getting worse because the opioids have made them more sensitive to pain in the fi rst place. It’s kind of like a drug withdrawal situation.”
Physicians in Tape’s clinical practice try to prepare patients for what they will likely experience when they begin reducing opioid use, including the possibility of OIH.
Physicians who treat opioid-dependent patients say there are no widely-accepted \tapering protocols. Each physician and patient have to develop a strategy geared to the patient’s circumstances. “Everyone has their own history as to how they got on it, why they got on it, what dose they take, and so on,” says Sameer V. Awsare, MD, FACP, associate executive director of the Oakland, California-based Permanente Medical Group and head of its opioid ini-tiative.
Awsare says that as part of its opioid initia-tive, Permanente regularly brings together a variety of specialists, including pharmacists, neurologists, psychiatrists and physical thera-pists, to help primary care providers navigate the complex process of weaning long-time opioid users off the medications and fi nd oth-er ways of managing the patient’s pain.
LeRoy sometimes uses celebrity deaths, notably that of Michael Jackson, to drive home the dangers of opioid use with his patients. “It becomes very real for patients when they see it happen to a high-profi le person,” he says.
Th e highly individualized nature of opioid dependence or addiction also means that alternative pain management techniques must be tailored to the patient’s individual
circumstances. “Every person has their own genetic makeup and psychological baggage,” notes Lindenbaum. “You can’t just say, ‘let’s follow this cookbook,’ because not every per-son is like that.”
Over his four decades of treating people with chronic pain, Lindenbaum has devel-oped a “toolbox” of alternatives to opioids. Among the approaches are physical therapy, massage therapy, acupuncture, water ther-apy, osteopathic manipulation and, for low back pain, the McKenzie Method.
Medications he tries with his patients include nonsteroidal anti-infl ammatory drugs, anti-depressants, and anti-seizure drugs such as Lyrica (Pregablin), which has been approved for treating the diff used pain caused by fi bromyalgia. It can also be eff ec-tive sometimes in treating migraines.
BARRIERS TO TREATMENTBut physicians looking for non-medicinal alternatives to pain management frequently bump up against other obstacles, namely, a lack of availability and/or insurance cover-age for such services.
For example, in 2010 a joint task force of the departments of defense and veterans af-fairs issued a study that identifi ed fi ve non-pharmacological therapies for chronic pain: chiropractic and osteopathic manipulation, massage therapy, acupuncture, biofeedback and yoga. But the APM’s Twillman points out that chiropractic/osteopathic manipu-lation is the only one covered by Medicare. Commercial payers are only slightly better in their coverage, he says.
As for the availability of such therapies, he notes that while in clinical practice in Kansas he saw patients who had come from hundreds of miles away for treatment, be-cause none was available where they lived. “So even for a well-informed physician who understands that using these methods can reduce the need for opioids, actually getting a patient access to these services and aff ord it is a real challenge.”
Th e ultimate solution, he believes, lies in developing multi-disciplinary pain clin-ics that can address all the issues facing patients who use opioids for chronic pain: physical, emotional, social and psycho-logical. “But again, it becomes a question of where the reimbursement comes from, and can you keep the doors open and the lights on with that sort of model?”
There hasn’t been enough attention paid to how easy it is to become dependent on opioids. As a physician you naturally want to alleviate pain, so ... you’re going to err on the side of being a little more generous.”— THOMAS TAPE, MD, ACP LIAISON TO THE CDC OPIOID GUIDELINES CORE EXPERT GROUP
THE OPIOID CRISIS

✔ Coding tips for better reimbursements
✔ Malpractice advice from the experts
✔ Practice management Q&As
✔ Strategies for optimal patient fl ow
✔ Practice makeovers to improve operational effi ciency
Visit MedicalEconomics.com/subscribe Enter priority code: MEHAW
Renew today!Online subscription renewal only takes a minute
Don’t miss an issue—renew your subscription now!

MEDICAL ECONOMICS��]��JUNE 25, 2016 MedicalEconomics.com38
READ MORE Doctors must be part of the solution to opioid abuse PAGE 4
ongress has taken what some are calling largely symbolic steps to address the issue of opioid abuse. Both the U.S. House and
Senate have passed opioid abuse legislation and were scheduled to con-ference in mid-May to come up with a fi nal bill both chambers would sup-port. However, neither chamber has authorized funding for the measures.
Th e White House called on Con-gress to appropriate $1.1 billion in emergency funding to address the issues of the overuse and abuse of opioid painkillers. Without funding allocations, “we’re back to where we were” says Kelly Brantley, MPH, a direc-tor at consulting fi rm Avalere Health in Washington, D.C. “I think this is feel-good legislation but it doesn’t neces-sarily do all that it could do.”
While generally supporting Con-gressional action, physician organiza-tions want whatever is enacted into law to avoid any mandates that would strip treatment decisions from indi-vidual providers.
Th e House in May passed 18 bills on the issue. One of those would mandate an interagency task force to review, modify and update best practices for pain management and prescribing pain medication. Another calls for treatment of pregnant women and in-fants born with opioid addiction, while
still another provides a framework for creating drug treatment programs for veterans.
Th e Senate already has passed the Comprehensive Addiction and Re-covery Act (CARA) with a wide range of provisions including education, addiction treatment and strengthening prescription monitoring programs. Th e Senate bill passed in March in an over-whelmingly bipartisan vote of 94 to 1.
Th e House, after consolidating its 18 bills into one so it could be con-ferenced with the Senate, approved the consolidated measure, also with a large, bipartisan majority.
Funding of any new programs could become an issue given that the Senate already has defeated a measure to pro-vide additional dollars for CARA.
But with Washington focused on the issue, as evidenced by the Centers for Disease Control and Prevention (CDC) opioid prescribing guideline published in March, and the National Rx Drug Abuse and Heroin Summit at the White House, expect some legislation before the end of the current session, Brantley and others agree.
“Th e president has made a lot of in-vestment in talking about opioids and prescription drug abuse,” notes Brant-ley. Pointing to the CDC guidelines, she says that “we’re seeing action in a way I don’t think we’ve ever seen before,” on the opioid abuse problem.
Physician groups say they support action on the issue, as long as whatever passes does not tie doctors’ hands when caring for patients.
Th e American College of Physicians (ACP) supports the CDC guidelines because they are guidelines rather than mandates, says Ryan Crowley, ACP senior associate for health policy. “We believe physicians should have discre-tion to provide care based on the needs of the patient,” he says.
Th e American Academy of Family Physicians (AAFP) has similar con-cerns. AAFP President Wanda Filer, MD, FAAFP, says that “clearly the pen-dulum has swung too far in terms of prescribing pain medications,” but any eff ort to impose treatment standards could go too far the other way.
Patrice A. Harris, MD, the Ameri-can Medical Association’s (AMA) board chairwoman-elect who chairs the group’s opioid abuse task force, notes that guidelines can have unin-tended consequences “which includes access and insurance coverage limitations for non-pharmacologic treatments, especially comprehensive care, and the potential eff ects of strict dosage and duration limits on patient care.”
John Frank is a contributing author. Do you think legislative action is needed to solve the opioid crisis? Tell us at [email protected].
C
Physicians don’t want hands tied by opioid reform
BY JOHN FRANK
D.C. CORNER
THE OPIOID CRISIS

MedicalEconomics.com MEDICAL ECONOMICS ❚ JUNE 25, 2016 39
Financial Strategies
PHYSICIANS CAN only
pass their business on to
another physician, natu-
rally limiting the number of
available potential buyers.
And this small pool grows
smaller still as a large num-
ber of younger doctors are
turning away from private
practice to work for large
healthcare providers.
At the same time, the
physician’s personal finances
and plans for retirement may
be inadequate. Doctors typi-
cally have a high level of stu-
dent debt that must be paid
off before retirement savings
can start, and the length of
schooling involved generally
means that doctors don’t
reach their peak earning age
until much later in life.
Between needing to
balance business finances
with personal retirement
priorities, many private
practice owners may em-
phasize the former, leaving
themselves vulnerable.
or voluntary withdrawal of
a physician from the group
practice.
Whether it involves a
solo or a group practice,
basic steps should be
considered in preparing
for the succession of the
practice ownership to try to
ensure that maximum value
is preserved:
Step 1 Plan early for
practice succession and
retirement. To help pre-
serve, enhance, and extract
maximum value from the
practice, succession plan-
ning should begin early,
preferably seven to 10 years
before retirement.
Step 2 Assemble a team of
competent advisers who
have in-depth knowledge
and experience work-
ing with physicians, their
practices, and their unique
planning needs. A qualified
tax advisor, attorney, and
wealth adviser should form
the core of the team.
Step 3 Implement a plan
to retain, recruit, and
reward key physician and
non-physician personnel to
shore up the practice and to
aggressively grow its gross
and net income, especially
For many physicians,
simply acknowledging these
obstacles is the first step
on the path to discussing
and creating a business
transition later in his or
her career, and, following
that, retirement. As with all
matters financial there can
be substantial advantages
to starting early. Below is
a road map to help you get
going.
Preparing for a saleEstablishing a succession
plan is one of the most
important business
decisions the owner of
a practice can make. The
succession plan should
provide for both ownership
transfer and management
continuation in the event
of disability, death or
retirement.
The structure of the
succession plan will de-
pend on the type of prac-
tice involved. A physician in
solo practice, for example,
will need to consider hiring
a junior physician who can
take over the practice, or
finding a potential buyer or
merger partner. As a last
resort, a solo practice may
need to wind down gradu-
ally if no other options are
available.
A group practice, in ad-
dition to the options noted
for solo practices, has the
possibility of a potential
physician partner buyout.
Another increasingly com-
mon scenario is to sell the
practice to a hospital or a
health system.
A formal buyout arrange-
ment, often referred to as a
buy-sell agreement, estab-
lishes how much the selling
or retiring physician partner
will receive for his/her inter-
est in the practice upon
the occurrence of certain
trigger events, such as the
death, disability, retirement
by JOHN CAMPBELL, JD Contributing author
Nearly 40% of doctors in the U.S. are aged 50 or older, and one in
four are 65 or older, according to the American Medical Association.
For these baby boomers, retirement is a fast-approaching reality.
As they ponder their next life phase, doctors who own private
practices face several challenges unique to the profession.
Succession planning for private practices

MEDICAL ECONOMICS ❚ JUNE 25, 2016 MedicalEconomics.com40
Financial Strategies
during the seven to 10 year
period prior to retirement.
Step 4 Approximately six
months prior to retirement,
engage a qualified appraiser
who specializes in medical
practices to ascertain the
value of the practice.
Step 5 Consider how a
practice’s underlying real
estate should be owned.
A practice that owns its
real estate may subject
that property to liability and
creditors’ claims flowing
from the practice. Proper
ownership of a practice’s
underlying real estate
(i.e., in a Limited Liability
Company), whether by the
solo physician or a group
of physicians, may provide
added protection of the
real estate and an addi-
tional source of potential
growth and income into
retirement.
Preparing yourself for retirementOn a parallel track to
planning for practice
succession, the practice
owner should develop
and implement a
complementary wealth
accumulation plan to
supplement the income
expected from the sale of
the practice.
This plan might include,
among other things,
taking full advantage of
tax-deductible contributions
to qualified plans (defined
contribution and defined
benefit plans), building up
an investment portfolio
outside of a qualified plan
and utilizing certain financial
instruments to provide tax-
advantaged income.
Structuring the transitionThere are many ways
to finance the sale of
a practice. Consider
early on how the
acquiring physician(s) will
compensate the retiring
doctor or doctors.
Different structures have
different tax consequences
and create different
demands on cash flow. Typi-
cally, the seller needs to be
compensated for a lifetime
of building equity in the
practice; the buyer needs
to have sufficient capital to
invest and grow.
John Campbell, JD, is a wealth strategist with the Private Client Reserve of U.S. Bank in Chicago. He has worked with physicians on wealth planning for more than 25 years. Send your financial questions to: [email protected].
SITUATIONS TO AVOIDThe sale of your practice may hit a variety of snags
EXAMPLE 1 Partners disagree Exit plans can go seriously awry if partners don’t agree in advance on how each of them will cash out. For example, one partner may want to be bought out and retire, whereas another partner may want to continue working but not purchase the first partner’s share. This scenario makes finding a third-party buyer difficult.
Disclosure: This information represents the opinion of U.S. Bank. It is not intended to be a forecast of future events or guarantee of future results.
The factual information provided has been obtained from sources believed to be reliable, but is not guaranteed as to accuracy or completeness
U.S. Bancorp Investments and its representatives do not provide tax or legal advice. Your tax and financial situation is unique. You should consult
your tax or legal advisor for advice and information concerning your particular situation.
EXAMPLE 2 No buyers in sight Another difficulty—and potentially a physician’s worst nightmare—is if potential buyers show little or no interest in the practice. Over the course of a career, competitive forces in a community can change, and not necessarily in a doctor’s favor. Some businesses, such as a specialist’s practice, may have so much local competition that similar practices may have no need to buy them.
For instance, a surgeon who is close to retirement is hoping to sell his busy practice to a group of younger surgeons located about 10 miles away. However, those surgeons know that the nearly retired surgeon’s patients probably will come to them anyway, so they aren’t interested in purchasing his practice.
This scenario illustrates how important it is for practice owners, like other professionals, to begin planning for retirement when they have plenty of time to save and invest their earnings. Regardless of specialty, physicians should not rely solely on their practice for future income.
EXAMPLE 3 Failure to plan for an internal succession If a doctor suddenly dies and has no business succession plan in place, his or her family can suffer financially. In one case, a doctor’s widow tried to sell the practice to younger partners and realized there was no agreement on who would take over and on what terms.
The younger partners—who were within their rights to start a new practice and take all the patients, leaving the owner’s family with nothing—did the ethical thing and bought the practice from the widow. However, the purchase price fell far short of what the owner could have gotten if he had planned for his exit ahead of time.
Source: Robert J. DiQuollo, CFP, CPA

MedicalEconomics.com MEDICAL ECONOMICS ❚ JUNE 25, 2016 41
Coding Insights
A: One of the incident-to
requirements is that the
“services rendered are part
of a course of treatment
during which the physician
personally performs the ini-
tial service and is actively
involved in the course of
treatment.” The key words
here, for your question, are
“actively involved.” What,
exactly, does that mean?
Many years ago there
were guidelines that
specified that the provider
needed to see the patient
him/herself every third
visit—and variations on
that theme. Those specific
guidelines are long gone,
and what we are left with is
this less specific language.
Other parts of the
incident-to guidelines bear
on this question. Was a
plan of care developed,
and is the problem being
addressed by the non-
were specific risk areas
identified–coding and billing
chief among them.
So if your provider’s
“own ways” do not align
with the general principles
of medical record documen-
tation, with correct coding
guidance or with current
guidance on cloning or
other EHR concerns, then
you may have an action-
able item with which to
approach him.
We all know folks who
are characters and gener-
ally ornery, but if there is
no actual rule or guideline
being breached, then it is
on your group to develop
internal policies for policing
such concerns.
physician provider (NPP)
part of the overall plan
of care developed by the
physician? Is the physician
treating or directing care for
the underlying condition for
which treatment is provided
today by the NPP?
So it’s not so much a
‘how long has it been’ since
the patient has been seen
by the physician, it is now
more of documenting the
physician’s involvement in
the plan. This is consistent
with the collaborative type
models of care that Medi-
care envisions for the future
of primary care and chronic
disease management.
As in the case of chronic
care management codes
and other services where
auxiliary or NPP staff par-
ticipate, let your electronic
health record reflect the
overall management of the
physician
Q: We have a physician
that does things his
own way, from notes
to codes to overriding
charges. One is enough,
but others see what he
does and want to do it
too. What can we do
rein him in?
A: This question is a
little outside the bounds
of coding—but could
fall into the compliance
category, depending on the
nature and extent of his
“variances.”
When compliance came
to the physician side of
healthcare, and the Office
of the Inspector General
produced its Compliance
Guidance for Physician
Practices, they made it clear
that compliance programs
were to detect and prevent
violations of the law. There
What active patient management means when billing incident-to
Bill Dacey, CPC, MBA, MHA, is principal of the Dacey Group, a billing, coding and compliance consulting firm. Send your billing and coding questions to: [email protected].
by BILL DACEY, CPC, MBA, MHA Contributing author
How often must the physician perform
subsequent services that reflect the
continued active management of a patient’s
care in order to bill incident-to?Q
Bundled payments: How they provide risk—and rewardPage 49
Why direct primary care may become the normPage 59
MORE AHEAD

MedicalEconomics.com 43
IN DEPTH
MEDICAL ECONOMICS ❚ JUNE 25, 2016
Technology
by MARY K. PRATT Contributing author
Data thieves are getting craftier with their methods—and are actively targeting healthcare records
How cyberattacks can impact physicians
TO CRIMINALS, your practice’s most valu-able asset isn’t a high-tech medical device or a pricey piece of diagnostic equipment. It’s your patient records.
Th ose records are the asset most vulner-able to theft, too.
What does that mean for physicians? Plenty. In an increasingly interconnected in-dustry, an attack on one could aff ect many. Every player in the system—from the largest hospital system down to rural solo practitio-ners—is facing a heightened risk.
“Th ere could be a consequence upstream if there’s a breach. A breakage or disrup-tion at one site can have that cascading ef-fect,” says Lee Kim, JD, FHIMSS, director of privacy and security at the Healthcare Information and Management Systems So-ciety, a nonprofi t organization focused on improving healthcare through information technology.
Consider the fi ndings from the Ponemon Institute, a public policy think tank. Its re-cent report, “Th e State of Cybersecurity in Healthcare Organizations in 2016,” found that the 535 healthcare organizations sur-
veyed averaged almost one cyberattack per month over the past 12 months. Moreover, 48% of the IT and IT security practitioners polled said that their organizations experi-enced an incident involving the loss or expo-sure of patient information during this same 12 months.
Perhaps more telling is how respondents, who come from various healthcare organi-zations and government agencies, feel about their ability to protect and respond: Just one-third said they’d rate the cybersecurity at their organization as very eff ective.
A more chilling observation comes from the Institute for Critical Infrastructure Tech-nology and its report, Hacking Healthcare IT in 2016. It pegged the industry as the most targeted, yet least prepared for, cybersecu-rity threats.
Th e impact of the healthcare industry’s cybersecurity stance is signifi cant: Ac-cording to the Offi ce of Civil Rights (OCR), 2015 saw 253 healthcare data breaches af-fecting 500 or more individuals. Together, those breaches aff ected more than 112 mil-lion records. Meanwhile, the Bitglass 2016
HIGHLIGHTS
The cybersecurity
threats impacting the
healthcare sector
aren’t much different
than the ones affecting
other industries. In
nearly all cases, the
cybercriminals are
looking to make money.
Hackers attacking
healthcare aren’t after
credit card numbers;
they’re looking for data-
rich electronic health
records (EHRs).

MedicalEconomics.com44 MEDICAL ECONOMICS ❚ JUNE 25, 2016
Technology Cyber attacks
Healthcare Breach Report has found that one in three Americans have been victims of healthcare data breaches.
Tom Stafford, PMP, vice president and CIO of Halifax Health, a hospital system headquartered in Port Orange, Florida, says the recent rash of cyberattacks against healthcare institutions is prompting execu-tives—board members, upper management, IT leaders and cybersecurity experts—to put even more attention on security measures.
“It is amazing how much the waves of at-tacks have increased ... but we should have all seen this coming. There’s been enough discussions around cybersecurity in the past few years. So it was just a matter of time be-fore hackers came after healthcare,” he says.
SHOW ME THE MONEYThe cybersecurity threats impacting the healthcare sector aren’t much different than the ones affecting other industries. In nearly all cases, the cyber criminals are look-ing to make money, says Mark Ford, CISSP, principal at Deloitte & Touche LLP and Life Sciences & Health Care Cyber Risk Services leader with Deloitte Advisory.
The February attack on Hollywood Pres-byterian Medical Center is a case in point. Hackers used malware to lock up the insti-tution’s computers and then demanded 40 bitcoin, about $17,000, to free the system. (The hospital paid the ransom.)
Although ransom attacks are making news now, cybercrimi- 46
Feds focus on healthcare ransomware attacksBy Dava Stewart Contributing author
t the direction of the
White House and the U.S.
Department of Health and
Human Services (HHS), the
federal Office of Civil Rights
(OCR) has begun to focus on the
threats to the healthcare community
of malware--software designed to do
harm. They are specifically focusing
on ransomware, malware that blocks
access to a computer system until a
sum of money is paid.
This shift in focus is the result of
research conducted by HHS to better
understand the requirements of the
Health Insurance Portability and
Accountability Act (HIPAA) in light of
known security threats. During the
second half of 2015 and the early part
of 2016, there has been a dramatic
increase in the incidences of malware
attacks, not only in the healthcare
industry but in the financial services
and retail sectors.
The FBI, along with the OCR and
various other agencies, have been
issuing warnings all year in an effort
to encourage IT departments to take
precautions and be aware of the rise
in criminal activity.
One result of that focus is a
monthly educational newsletter,
launched by the OCR in February.
The newsletter highlight threats,
including information on ransomware
and technical support scams. Dave
Peterson, senior vice president and
chief information officer at Erlanger
Health System in Chattanooga,
Tennessee, told Medical Economics
the newsletters can be beneficial to
healthcare IT departments, adding
that he doesn’t rely on this guidance
completely, but finds them a useful
supplement.
A report released by the Ponemon
Institute and ID Experts in May 2015
shows a 125% increase in criminal
cyberattacks over the last five years,
making these incidents the leading
cause of data breach. Another report
is set to be published on May 12, 2016,
and Rick Kam, president of ID Experts
said “some areas have gotten worse
since the last report, and there hasn’t
been any improvement.”
Much of the rise in cyber attacks
is attributable to ransomware. In a
ransomware attack, the criminals,
often referred to by authorities
as “bad actors,” infiltrate an
organization’s IT system through
one of a variety of methods, and
install malicious software. Malicious
email attachments are common, but
tech support scams also are on the
increase.
In a tech support scam, a user
receives a phone call, email or website
popup with a warning that their
system is infected. Then, a criminal
masquerading as a tech support
person offers to clear the infection.
Instead, they install malware.
The ransomware in use today,
according to Kam, is far more
sophisticated than it has been in
the past. The current version of
ransomware locks up the information,
and destroys log files and backups.
The criminals then demand a financial
ransom to release the system.
“It’s become the shortest path to
the money for crooks,” says Kam.
A

MedicalEconomics.com46 MEDICAL ECONOMICS ❚ JUNE 25, 2016
Technology Cyber attacks
nals are much more likely to go after the data that computer
systems hold—just as they do when attack-ing stores and financial institutions and oth-er types of businesses, Ford and others say.
However, hackers attacking healthcare aren’t after credit card numbers; they’re looking for data-rich electronic health re-cords (EHRs), security and healthcare ex-perts say. “The reality is it’s profitable,” Peter B. Nichol, PMP, CSSMBB, a healthcare expert with PA Consulting Group, says of these at-tacks.
A former chief information officer and former head of IT for Connecticut’s Health Insurance Exchange, Nichol says a credit
card number sells for $2 on the black market while a health record goes for $20 or more.
Credit card numbers, and other finan-cial data such as bank account numbers, have short shelf lives on the black market. But EHRs contain multiple types of data that can be used fraudulently but are diffi-cult, if not impossible, to change. A typical health record has a patient’s name, address, age, employer, Social Security number and spouse’s information—all of which can be used for identity theft.
A typical record also includes health in-surance information as well as prescription drug data, which thieves can use to seek medical care at the expense of someone else and/or obtain drugs that they can either use themselves or sell on the black market.
“Banks have such great analytics and they can spot an erroneous transaction and can in seconds notify you and shut down a stolen credit card number. And [hackers] know the bank can turn one off right away, which is the exact opposite of medical infor-mation,” says Ryan Witt, who, as vice presi-dent and managing director of Healthcare Industry Practice at Fortinet is working with the nonprofit organization WEDI to develop cybersecurity material for healthcare.
CONNECTIONS HEIGHTEN RISKSOne of the challenges of this increasingly networked world is enabling necessary con-nections while blocking the unauthorized or dangerous ones. “It’s a balance between how much you protect yourself vs. how much you’re obstructing a team member,” Stafford says.
Healthcare IT and cybersecurity experts say the sophistication of attacks has been in-creasing and that most cybercriminals aim to stay undetected for as long as possible, giving them more time to find as much data to exploit as they can.
Hackers do that by finding weak spots in computer systems. An office administrator could fall for an email phishing scheme. A doctor could unwittingly download a mali-cious app. A researcher could lose a laptop with weak password and encryption pro-tection. Hackers working in a waiting room could get in via an unsecured Wi-Fi connec-tion, or they could drop USB flash drives near workstations to trick employees into thinking they’re authorized for use when in fact they contain malware.
44
❚ Hollywood Presbyterian Medical Center, Los Angeles
434-bed hospital ransomware attack, systems later recovered $17,000 (40 bitcoin) ransom paid
❚ Methodist Hospital in Henderson, Kentucky
217-bed hospital ransomware attack, systems later recovered no ransom paid
❚ MedStar Health System, Columbia, Maryland
10 hospitals ransomware attack, systems later recovered no ransom paid
❚ Alvarado Hospital Medical Center, San Diego
306-bed hospital
ransomware attack, systems later recovered no ransom paid
❚ Chino Valley Medical Center, California
126-bed hospital ransomware attack, systems later recovered no ransom paid
❚ Desert Valley Hospital, Victorville, California
83-bed hospital ransomware attack, systems later recovered no ransom paid
❚ King’s Daughters’ Health, Madison Indiana
77-bed hospital malware attack, systems replaced
HOSPITAL HIT LISTHere’s a list of reported ransomware and malware attacks on U.S. hospitals. According to a recent survey from the Healthcare Information and Management Systems Society (HIMSS), as many as 75% of hospitals responding said they could have been hit with such an attack in the last year.
Source: information compiled through various media reports

MedicalEconomics.com 47 MEDICAL ECONOMICS ❚ JUNE 25, 2016
TechnologyCyber attacks
And once into a practice’s system, cyber-criminals may be able to go far, using it as a gateway into the vendors and partners connected to the computer system that was first hacked. “It’s a real concern and not far-fetched at all, this machine-to machine type of attack,” Witt says.
COST AND CONSEQUENCESThe consequences of a data breach range from costly to catastrophic. In its 2015 Cost of Data Breach Study: Global Analysis, the Ponemon Institute put the average cost of a healthcare breach in the United States at $398 per exposed personally identifiable record. (That’s significantly higher than the $217 average per exposed records across various industry sectors.) The investigation, remediation, notification, credit monitoring and other possible costs, such as fines and legal bills, add up quickly.
“The implications to a practice are very, very significant,” says Lee Barrett, executive director of the Electronic Healthcare Net-work Accreditation Commission (EHNAC). “When you look at stakeholder level of trust, what patients think of doctors, if their infor-mation is compromised, the patients will go somewhere else, regardless if the patient has a long-standing relationship with that doctor. The practice would have to report [the breach] to Office of Civil Rights, which can fine the practice. And it will be in the newspapers. A practice could easily go out of business.”
Others see even more serious conse-quences, with breaches crippling an organi-zation’s ability to provide care. Ford, for ex-ample, says a hacker could launch an attack like the one that hit Hollywood Presbyterian Medical Center.
“That’s really scary because that changes the game a bit. People’s lives can be at stake if you lock up a system like that,” he says, adding that some have voiced concerns that terrorists looking to inflict harm could carry out similar types of attacks aimed at dis-rupting the nation’s ability to provide criti-cal healthcare.
Think that’s far-fetched? Consider the 2014 cyberattacks on Boston Children’s Hospital that disrupted patient and hospital personnel access to certain files. The attack was allegedly carried out by the infamous computer hacker network known as Anony-mous over a highly-publicized 2013 case in
which hospital officials accused the parents of a sick teenager of medical child abuse.
PROTECT YOURSELFMany IT professionals are hesitant to talk about the cybersecurity measures they have in place or the challenges they face. As one security consultant explains: If they say they’re doing well, it’s like a issuing a chal-lenge to would-be hackers. If they say they need work, it’s like painting a target on their systems.
Still, there’s widespread agreement that the healthcare industry needs to strengthen its security measures.
“To be resilient, you need to plan and think about your controls and structure and be able to adapt quickly,” Ford says. He adds that organizations must start by under-standing what data they have, what they’re connected to, what protections they have and what risks they face as well as what would happen if an attack occurred.
“You have to go through some compre-hensive analysis to understand what your risks are and whether you have the proper structures in place to respond,” he says.
In addition to employing standard best practices such as regular cybersecurity training for staff, Barrett says he recom-mends that organizations hire an outsider to review and test their security strategies as well as earn an industry accreditation or certification that shows they meet cyberse-curity standards.
Stafford noted that among the best prac-tices in cybersecurity is to require anyone connecting to your network—vendors, sup-pliers, insurers, medical partners—to prove that they, too, have in place appropriate cy-bersecurity measures.
“You have to do the due diligence, so whomever you’re working with you know they’re doing cybersecurity audits and risk assessments, too,” he says.
Barrett, Ford and others cybersecurity experts concur, saying every organization should have in their agreements with other entities—medical facilities, vendors, insur-ers, etc.—provisions that specify the mini-mum cybersecurity measures they must have in place.
“The industry is putting the onus on those who have data to do their due diligence and make sure their systems are secure,” Ford says.

MEDICAL ECONOMICS ❚ JUNE 25, 2016 MedicalEconomics.com48
Legally Speaking
Discharging problem patients the right wayby RODNEY K. ADAMS, JD and LUCIEN W. ROBERTS, I I I Contributing authors
Discharging patients is not pleasant, but it is often
prudent and necessary. Because of the legal and ethical
implications of patient dismissal, it is helpful to get
practical guidance on how to correctly terminate a patient.
have a right to know
why they are being
discharged.
More and more
patients are being dis-
charged because they are
unable to pay their bills.
It’s unfortunate, but it is a
reality and there is noth-
ing illegal about doing so.
Just as patients who do
not show up for appoint-
ments are violating the
physician-patient relation-
ship, so too are patients
who receive care but do
not pay for it.
Finally, patients have
a right to a copy of their
medical records. Your
letter should offer to
make a copy of these
records available to the
patient or their new
physician. You do not
need to provide a copy
of your medical records
with the termination
letter.
❚ the notification itself,
❚ the effective date,
❚ the reason for the
termination, and
❚ an offer to provide a
copy of the records
to the physician
assuming the patient’s
care.
Notification and effective dateBegin with a straightforward
sentence stating that the
patient is being discharged
from the practice. The letter
should include an effective
date that is at least 30 days
beyond the date the letter
is mailed. We recommend
that this period be extended
45 days to 60 days if you
practice in a specialty or
geographic area where it
may take patients longer to
find another physician, or if
you are currently providing
care for an ongoing
condition.
During the period
WE FIND THAT most
patient terminations fall into
one of four categories:
❚ patients who are
verbally abusive
or threatening to
providers or staff;
❚ patients who are
noncompliant with
their care—missing
appointments and/
or recommended
testing;
❚ patients who “doctor
shop” and often are
most interested in
obtaining medications;
and
❚ patients who do not
pay for the care you
provide.
Regardless of why
the patient is being
terminated, the
termination letter itself
should be straightforward
and contain four
elements:
between your letter and the
patient termination date,
offer to provide emergency
care only. Our practice
refills necessary prescrip-
tions but otherwise avoids
providing non-acute care
during this period.
You are not required
to suggest alternative
providers in your letter, nor
do we recommend doing
so. We do not like it when
other groups refer their
“problem” patients to us,
so we do not recommend
that our problem patients
contact specific physicians
or groups. Our discharge
letters simply say we are
providing ample time for
the patient to find another
provider.
TransparencyWe think it is appropriate
to provide a reason for
the patient’s discharge.
Even if the patient does
not like the reason, they
Rodney K. Adams, JD, is a healthcare attorney with LeClairRyan in Richmond, Virginia.
Lucien W. Roberts, III, is administrator of Gastrointestinal Specialists, Inc., in central Virginia. This article was first published in our partner publication Physicians Practice. Send your legal ques-tions to: [email protected].

MedicalEconomics.com 49
IN DEPTH
MEDICAL ECONOMICS ❚ JUNE 25, 2016
Money
by NICOLE LEWIS Contributing author
Many experts view bundled payments as a critical part of cutting costs and reforming healthcare
Bundled pay brings physicians greater risks and rewards
AS PHYSICIANS deepen their involvement in the shift to value-based care, they are begin-ning to grapple with the sweeping changes that bundled payment initiatives will bring to the way they practice medicine.
David Galetto, MD, is an internist and one of fi ve members of a private practice in Vineland, New Jersey. Galetto commits 25% of his time to Inspira Health Network, which has three acute care hospitals in southern New Jersey. Th ere he serves on the commit-tee overseeing care redesign and attends to Medicare benefi ciaries who are part of a bundled payment initiative. He spends the rest of his time seeing patients at his group practice, which is also involved in a patient-centered medical home initiative.
“Am I working harder than I used to? Oh my God, yes,” says Galetto.
He says that at Inspira Health, the bun-dled payment program has increased his workload, adding tasks from meeting with peers to discuss implementing best prac-tices for care design to following up with doctors, specialists, case managers, social workers and surgeons—all in an eff ort to make sure patients don’t stay in the hospital longer than necessary.
“It takes time and eff ort to keep ev-erything under control, and you’ve got to count on a lot of stakeholders to do the job,” Galetto says.
As the bundled payments model evolves, it will also provide an opportunity for phy-sicians in independent practice to take the lead in establishing a direct relationship with the payer, predicts Tom Campanella, JD, associate professor of health econom-ics and director of the Health Care MBA program at Baldwin Wallace University in Berea, Ohio. He adds that the practice would then negotiate a facility fee with the hospital (if applicable) and the other provider stake-holders.
Th ere will be more risks and rewards for physicians under this approach, Campan-ella says, but the long-run payoff —which includes enhancing their ability to stay inde-pendent—would make it worthwhile.
“As they drive quality metrics and cost-eff ective initiatives, physicians will soon re-alize that they’ve never had such a golden opportunity to take a leadership role in im-proving healthcare across the board. Th at’s a great position to be in,” Campanella says
Galetto agrees, noting that the model
HIGHLIGHTS
New initiatives help
small practices earn
funds to pay for higher
offi ce expenses that
come with the demands
of monitoring patients
more closely, employing
additional medical
assistants and paying
to upgrade and maintain
technology.

MedicalEconomics.com50 MEDICAL ECONOMICS ❚ JUNE 25, 2016
CMS bundled payment modelsCMS’ Bundled Payments for Care Improvement initiative is comprised of four broadly defined models of care that link payments for multiple services beneficiaries receive during an episode of care.
Model 1 Model 2 Model 3 Model 4
Episode All diagnosis-related
groups (DRGs); all acute
patients
Selected DRGs; hospital
plus post-acute period
Selected DRGs; post-
acute period only
Selected DRGs;
hospital plus
readmissions
Services included in the bundle
All Part A services paid
as part of the MS-DRG
payment
All non-hospice Part A
and B services during
the initial inpatient
stay, post-acute period
and readmissions
All non-hospice Part A
and B services during
the post-acute period
and readmissions
All non-hospice Part
A and B services
(including the hospital
and physician) during
initial inpatient stay
and readmissions
Payment Retrospective Retrospective Retrospective Prospective
Money
will be critical in shaping the way doctors approach their jobs because it allows their opinions to carry greater weight in the deci-sion-making process.
“Over the years, doctors have been frus-trated because when we wanted to make changes in a particular care process, and if we failed to effect change, in some instances it was because stakeholders were not all at the table to come to a consensus, or individ-ual stakeholder interests were not aligned,” Galetto says.
Even while there is the burden of addition-al work, many physicians at small practices are actively engaged in new initiatives to boost revenues. All five physicians at Galetto’s pri-vate practice are involved in Inspira Health’s bundled payment initiative.
April Venable, director of Population Health Decision Support at Inspira Health Network, who invited Galetto to join the hos-pital’s bundled payment efforts, says once physicians attended a series of open sessions to learn more about the program, it was easy to get them to enroll. “Their billing and pay-ment processes do not change–it’s just an ex-tra payment to them every six months if their cost has improved,” says Venable.
Another advantage to the new payment initiatives is they can help small practices earn income to pay for higher office expens-es that come with the need to monitor pa-tients more closely, such as additional medi-cal assistants and upgrades to technology, Galetto says.
FACING THE FUTUREAs a result of new bundled payment initia-tives, physicians will encounter the follow-ing, according to Campanella:
❚ The need for better care coordination among
stakeholders involved with the bundled
payments.
❚ The challenge of improving patient compliance
so as to improve the quality/outcome aspect to
most bundled payment methodologies.
❚ Greater financial risks and rewards, especially
as bundled payments continue to evolve.
❚ The need to understand the details of the
bundled payment contractual relationship
with the payer or the hospital if the physician
is sub-contracting with them, especially as it
relates to risks, rewards and quality/outcome
requirements.
Bundled payments

MedicalEconomics.com 51 MEDICAL ECONOMICS ❚ JUNE 25, 2016
MoneyBundled payments
The growth of bundled payments coin-cides with the Centers for Medicare & Med-icaid Services’ (CMS) looming Merit-based Incentive Payment System (MIPS) and Al-ternative Payment Models (APMs), designed to replace Medicare’s Sustainable Growth Rate physician payment formula.
Campanella says the goal of bundled payment initiatives and MIPS/APMs is to encourage physicians to provide better care, not just more care.
The bundled payment model is being applied to more episodes of care, as the traditional practice of charging separately for services such as a surgical procedure, post-operative care, and physical therapy— which generates multiple claims from multi-ple providers—is replaced with a model that compensates care teams with a fixed dollar amount under one bundled payment.
For example, Horizon Blue Cross Blue Shield of New Jersey recently announced a bundled payment initiative with University Hospital of Newark for pregnancy and de-livery. In another example, St. Vincent Char-ity Medical Center in Cleveland, Ohio, will participate in the Pacific Business Group on Health Employers Center of Excellence network to provide a bundled payment pro-gram for bariatric surgery.
CMS is experimenting with four bun-dled payment initiatives under its Bundled Payments for Care Improvement (BPCI) program. In April it launched the Compre-hensive Care for Joint Replacement model, which is the agency’s first mandatory bun-dled payment initiative. It requires that acute care hospitals be held accountable for the cost and quality of care for Medicare beneficiaries that have hip and knee re-placement, from surgery to recovery.
BPCI MODEL 1Since April, 2013, Inspira Health Network has participated in BPCI Model 1. Under this initiative, an episode of care is defined as the inpatient stay in an acute care hospi-tal. Medicare pays the hospital a discount-ed amount based on the payment rates es-tablished under the Inpatient Prospective Payment System (IPPS), a system of pay-ment for the operating costs of acute care hospital inpatient stays. (Under the IPPS, each case is categorized into a diagnosis-related group [DRG] and each DRG has a payment weight assigned to it, based on
the average resources used to treat Medi-care patients in that DRG.)
Another feature of BPCI Model 1 is that Medicare continues to pay physicians sepa-rately for their services according to the Medicare Physician Fee Schedule.
While Galetto is not employed by Inspi-ra Health, he credits the efforts of its care teams in aligning provider incentives with rewards for measures that cut costs while improving patient outcomes as the catalyst for cost reductions ranging from 7% to 11% per admission, depending on the time pe-riod being calculated.
The initiatives include performing fewer unnecessary tests, collaborating with care teams to follow up with patient care, in-cluding more information related to the patient’s care in the patient’s electronic health record, and educating staff mem-bers on the latest recommendations from the American Board of Internal Medicine’s Choosing Wisely initiative.
Between April 2013 and June 2015, Galetto says, the hospital has realized sav-ings of $9 million. Part of that is attributed to the decline in length of stay and reduced use of the intensive care unit ($2.6 million), a reduction in the general length of stay at the hospital’s acute care unit ($2.6 million) and emergency department cost reductions ($610,000).
“Many of the cost-cutting practices that we’ve implemented would never have oc-curred had it not been for our involvement in the BPCI initiative,” Galetto says.
He adds that a lesson Inspira has learned from using the bundled payment model is that change comes with a price. “If there’s going to be a change in the way the health-care system delivers care, those changes must be aligned with financial incentives,” Galetto says.
He notes also that the goals are twofold: physicians can earn dollars based on achiev-ing either: 1) performing better than they did in the prior year on a similar case ( for example, heart failure last year compared to heart failure this year), or 2) reaching the best practice level for that DRG which is the lowest 25th percentile in the state of New Jersey.
“Physicians who have enrolled in the BPCI program at Inspira Health have re-ceived payments every six months depend-ing on how many patients they treat and
[Bundled payments take] time and effort to keep everything under control, and you’ve got to count on a lot of stakeholders to do the job.”— DAVID GALETTO, MD, INTERNIST, VINELAND, NEW JERSEY

MedicalEconomics.com52 MEDICAL ECONOMICS ❚ JUNE 25, 2016
Money Bundled payments
whether they reduced costs without com-promising quality,” Galetto says.
Most physicians receive between $1,000 and $10,000 each payment period. The larg-est payment to an individual physician has been $13,000 in a given six-month time pe-riod. “That’s enough to make doctors want to improve their practices and contribute to better outcomes for their patients,” Galetto says.
As CMS continues to promote cost cut-ting measures, the agency views bundled payments as a critical part of healthcare re-form. In 2015, for the first time in the history of the Medicare program, the U.S. Depart-ment of Health and Human Services set ex-plicit targets for alternative payment models and value-based payments. These included a goal of tying 30% of fee-for-service (FFS) Medicare payments to quality or value through alternative payment models such as accountable care organizations (ACOs) or bundled payment arrangements by the end of 2016, and tying 50% of payments to these models by the end of 2018.
BPCI MODEL 2Like many orthopedic surgeons, Michael Fehm, MD, who is one of eight private prac-tice physicians at Excel Orthopaedic Spe-cialists in Boston, Massachusetts, says he was attracted to the idea of participating in the BPCI Model 2 program because he saw clinical and financial opportunities and wanted to experiment with new care plans and protocols before a bundled payment model became mandatory.
While continuing to see patients at Excel, in 2014 Fehm joined Ortho New England Group LLC, which includes four orthope-dic surgeons who are participating in BPCI Model 2.
Under Model 2, Medicare continues to make fee-for-service payments to providers and suppliers furnishing services to benefi-ciaries in care episodes. The total expendi-tures for a beneficiary’s episode is later rec-onciled against a bundled payment amount (the target price) determined by CMS. Medi-care payments reflect the aggregate perfor-mance compared to the target price.
Fehm likes that the arrangement en-ables Ortho New England to receive critical patient data from Medicare, including the cost of care during an episode. For exam-ple, Fehm has access to information that
shows how many days the patient spent in rehab, the rehab charges and how many visits the patient received from a visiting nurse or secondary consultations from other providers.
“The data helps me feel empowered to make better decisions to improve patient care,” says Fehm. He has performed roughly 100 surgeries, including joint replacements and hip fracture repairs, during the past 12 months on Medicare patients who are in-cluded in the BPCI Model 2 initiative.
Fehm says he’s learned that the model enables surgeons to keep tight control over a patient’s care. As a result, he and his part-ners now are paying more attention to dis-charge planning, and referral patterns are starting to change as additional data be-comes available.
Understanding how his patients are treated after surgery is critical, because Ortho New England is responsible for the Medicare beneficiary’s inpatient stay in an acute care hospital, as well as their post-acute care and all related services during the episode of care, which ends 30 days after hospital discharge.
“The data allows us to look at our own performance and the performance of sec-ondary providers such as rehabilitation facilities and home therapy and nursing groups,” Fehm says. “Having that data helps us work to raise the bar on performance and quality from all angles. It has empowered us to better advocate and care for our patients.”
The risk of failing to improve patient care is real, but sometimes a patient’s health is beyond the control of physicians. For ex-ample, last year one of Fehm’s hip replace-ment patients developed a post-operative GI bleed following the surgery. The patient required a 10-day ICU stay and multiple up-per endoscopies.
While the patient’s hip replacement was straightforward, Fehm says, his overall med-ical course was complicated, and with the complications came higher costs.
“A large percentage of these costs are as-sumed by the provider participating in the BPCI. There is a large risk, and not all factors can be controlled” Fehm says. “It’s hard to imagine taking care of a patient and then ending up having to pay.”
Fehm adds that most hip fractures oc-cur in patients with multiple medical con-ditions, and these patients require more
There is a large risk, and not all factors can be controlled. It’s hard to imagine taking care of a patient and then ending up having to pay.”— MICHAEL FEHM, MD, EXCEL ORTHOPAEDIC SPECIALISTS, BOSTON, MASSACHUSETTS

MedicalEconomics.com 53 MEDICAL ECONOMICS ❚ JUNE 25, 2016
MoneyBundled payments
in-hospital and post-discharge care. “On av-erage every hip fracture episode that we’ve attended to has cost this program several thousand dollars, money that must be made up by taking good care of our healthy elec-tive patients and having excellent outcomes in that population,” Fehm says.
Knowing that there’s a financial penalty if patients have complications or are readmit-ted to the hospital motivates Fehm to watch patients more closely. “I care specifically that patients are better educated to mini-mize risks post-operatively, such as deep vein thrombosis, infection, constipation and urinary retention,” Fehm says.
He adds that preventing readmissions and avoiding complications will make this Medicare initiative a success, both in its ef-fort to improve care and to cut costs. “The financial implications are real, and in this real-world scenario it has helped us better improve the delivery of care we provide for patients. This is the primary objective set forth by Medicare and I believe we are better now at fulfilling that goal,” Fehm says.
BUNDLED PAYMENTS FOR DIALYSIS PATIENTSGurdev Singh, MD, an internist and ne-phrologist is participating in yet another bundled payment model. In October, 2015, Southwest Kidney Institute, a private prac-tice with 53 nephrologists based in Phoe-nix, Arizona, teamed with dialysis services provider Davita HealthCare Partners Inc., and Banner Health, a nonprofit health care system, to launch an End Stage Renal Dis-ease Seamless Care Organization (ESCO) in Phoenix and Tucson.
Designed by the Center for Medicare & Medicaid Innovation (CMMI) the ESCO is a kidney disease-specific ACO. As part of the ESCO pilot, CMS tracks both cost and qual-ity of care, and benchmarks it against aver-age cost per patient for prior years, explains Singh, who is vice president of finance at Southwest Kidney Institute.
“There is a great amount of risk involved in this bundled payment model,” says Singh, who is spearheading the bundled payment initiative. Any savings generated compared to the fixed benchmark will be shared be-tween CMS and the ESCO participants. However, at the end of the year, if the cost to treat a patient is higher than the CMS benchmark, ESCO participants will pay a
penalty. Noting that the current FFS-based health-
care delivery model is not sustainable, Singh says bundled payments for dialysis patients prompts nephrologists to find ways to im-prove quality and reduce patient expenses through optimal use of medical services, dialysis services, drugs and hospitalizations. This requires creative solutions to promote patient engagement and education.
“Bundled payments have changed the way physicians approach care delivery. For example, physicians have to increase resources to enhance patient education around their care, coordinate care delivery among patients and providers and impress upon patients the importance of controlling comorbidities to improve their outcomes,” Singh says.
Medication adherence and consistent attendance at dialysis sessions are top con-cerns because skipping medications and delaying dialysis treatments could worsen a patient’s condition, leading to hospitaliza-tion and higher care expenses. Finding ways to address these issues is important. Re-search shows that a dialysis patient can cost anywhere from $72,000 to $100,000 per year.
Another challenge involves the timing of payments. To support the initiative, the organization has had to invest time and money in infrastructure and support ser-vices. Singh says Southwest Kidney’s costs have increased 10% since the ACO began. However, any reimbursement related to the success of the program is delayed by about 15 to 18 months.
Although Singh says it’s too early to tell what lessons he’s learned from the program, he predicts that the bundled payment mod-el is here to stay and will get better over time.
“We believe that the quality of care will improve and the cost will go down with bun-dled payment models as long as physicians are reimbursed adequately for additional time and costs associated with achieving the goals,” Singh says. “This will create a win-win for all parties involved – patients, pro-viders and payers.”
Exclusive report: Physician income is actually improvingbit.ly/MEphysicianreport
MORE ONLINE

MEDICAL ECONOMICS ❚ JUNE 25, 2016 MedicalEconomics.com54
Practical Matters
Independent doctors find success with physician-led ACOsby TOM GIANNULLI, MD, MS Contributing author
There are over 600 accountable care organizations (ACOs)
in the United States—and half of them are physician-led.
practice needs to be up to
date and support the risk
stratification, care manage-
ment and quality report-
ing needed to support a
diverse set of payment
models.
Technology is needed
as well to support
improved patient engage-
ment through visit remind-
er, post visit surveys, and
other tools. But both pro-
viders still find that some
work remains manual, and
as Bee mentioned, this
is where some additional
cost can come in to play.
As technology continues
to grow to meet the needs
of providers participating in
value-based programs such
as virtual ACOs, the process
will only get easier. This will
help the providers continue
to be more efficient, im-
prove outcomes and reduce
costs. As a result, their
incentives will grow. There
is a lot of potential when
independent physicians
band together to achieve
improved results as a group
instead of standing alone.
al approach, and testing
new models on a smaller
scale, a practice can offset
the costs involved in fully
transitioning to a single
payment model, includ-
ing staff downtime and
reduced patient load.
Joining a physician-led
ACO, as one piece of a
bigger practice picture, has
worked well for primary
care physician Lee Peter
Bee, DO, an internist in
Sesser, Illinois, who says
there were virtually no ad-
ditional set-up costs.
“There were some
indirect costs with staff
performing additional data
entry for tracking the quality
measures,” he says. “But
there were no direct costs,
and we have saved money
and increased reimburse-
ment through the group’s
negotiating power.”
His ACO also has been
successful in achieving the
quality measures required
to receive an incentive,
so he has been receiving
shared savings payments
quarterly. In addition, Bee
THIS APPROACH is only
gaining momentum, as
the majority of physicians
say they would prefer to
stay in private practice
and not sell to a larger
entity. Providers are seeing
that these programs are
positioning them to better
meet the changing expec-
tations of patients.
Because physician-led
ACOs are more flexible,
providers can not only stay
independent but maintain
control over their mix of
payers and the payment
models they choose to
support. Thus, an agile
medical practice can
manage risk and revenue
potential by supporting a
population of patients from
a virtual ACO as well as a
group of patients that are
fee-for-service or even a
direct primary care panel
of patients.
A shift towards a value-
based and patient-centric
practice will improve
patient satisfaction and op-
erational performance. By
using a gradual, transition-
has tested a telemedicine
model in his practice. So far,
he has had the flexibility to
keep the models and op-
tions that work and let go of
those that don’t.
Family physician Doug-
las Hansen, MD, also has
seen the benefits of partic-
ipating in a large physician-
led ACO and testing other
reimbursement options
at his practice in Littleton,
Colorado.
“The focus is on
certain high-risk groups
of patients and previously
uninsured patients,” he
explains. “The payments
coming in from the virtual
ACO are small, but we
are seeing that percent-
age grow and we are
participating in some other
value-based programs
and receiving incentives
through those as well.” He
has also been trying some
direct primary care options
in his practice for patients
with high-deductible plans.
To make these changes
successful, the technol-
ogy used to manage the
Tom Giannulli, MD, MS, is the chief medical information officer at Kareo. Send your practice management questions to: [email protected].

Products & Serv ices SHOWCASE
MedicalEconomics.com 55 MEDICAL ECONOMICS ❚ JUNE 25, 2016
Search for the company name you see in each of the ads in this section for FREE INFORMATION!
SKIN HEALTH REFERRALS
Skin ConditionsAcne Scars
Birthmarks
Hyperhidrosis
Surgical and Trauma Scars
Varicose VeinsAmbulatory Phlebectomy
Sclerotherapy
Trust us with your patientsWhen patients inquire about their skin health, you can be
comfortable you are making the right choice when you refer
them to members of the American Society for Dermatologic Surgery.
You’ll know your patients are in the right hands for the right procedures.
8LIWI�FSEVH�GIVXM½�IH�HIVQEXSPSKMWXW�¯�[LS�TMSRIIVIH�QER]�SJ�XSHE] W�GSWQIXMG�QIHMGEP�XVIEXQIRXW�¯�YWI�GYXXMRK�IHKI�XIGLRSPSKMIW�XS�TVSZMHI�GSWX�IJJIGXMZI��UYEPMX]�SYXGSQIW�MR�SJ½�GI�FEWIH�WIXXMRKW�
Please think of members of the
American Society for Dermatologic Surgery –
the experts in skin health and
beauty – when your patients
need a referral for:
Performing more than 3 million skin cancer and 6 million cosmetic treatments each year, ASDS members combine their training and expertise to offer the widest range of options available. Visit www.asds.net/refer
Skin CancerMohs Micrographic Surgery
Wide Local Excision
Electrodesiccation and Curettage
Cryosurgery
Photodynamic Therapy
For information, call Wright’s Media at 877.652.5295 or visit our website at www.wrightsmedia.com
Leverage branded content from Medical Economics to create a more powerful and sophisticated
statement about your product, service, or company in your next marketing campaign. Contact Wright’s
Media to find out more about how we can customize your acknowledgements and recognitions to
enhance your marketing strategies.
Content Licensing for Every Marketing Strategy
Marketing solutions fit for:
Outdoor | Direct Mail | Print Advertising | Tradeshow/POP Displays | Social Media | Radio & TV

MedicalEconomics.com56 MEDICAL ECONOMICS ❚ JUNE 25, 2016
M A R K E T P L AC E
P R O D U C T S & S E R V I C E S
M E D I C A L E Q U I P M E N T
Mark J. Nelson MD
FACC, MPH
E-mail: [email protected]
Advertising in Medical
Economics has
accelerated the growth
of our program and
business by putting me
in contact with Health
Care Professionals
around the country
who are the creators
and innovators in their
field. It has allowed
me to help both my
colleagues and their
patients.
Contact me today to place your ad.
Tod McCloskey, Sales Manager440-891-2739
Reach your target audience.
Our audience.

MedicalEconomics.com 57 MEDICAL ECONOMICS ❚ JUNE 25, 2016
M A R K E T P L AC E
O N C A L L S U P P O R T
P R O D U C T S & S E R V I C E S
TRANSC R I PT ION SE RVIC ES
REST ASSURED — WE WORK NIGHTS AND WEEKENDS SO YOU DON’T HAVE TO.
������������� ����
����������������
����������
��� ���������� �����
������ ������ ����
����� ���������� ���� ��
FaceSheet App
Call 888-502-2268www. FacesheetMD.com
Transcription ServiceScribe into EMR
Visit: AAAMT.COM
Call: 888 50-AAAMT Email: [email protected]
Less than a Dollar per dictation.
One week free trial. No obligation.
No Start-up costs, no contracts.
Transcribe in your EMR.
Same day turn around guaranteed.
Transcripts to referral doctors same day.
AAAMTdictate iPhone/Android App.
Physicians can use from nursing homes
will send transcript by fax same day.
Highly customized.
Capture visit and send info to biller
Forward patients to another provider
with signoff note. HIPAA compliant.
Web interface access for provider & Biller
to check reports. 14% increased revenue.
No lost Facesheets. No more paper.
Available as FaceSheet in App store.
all in 5 seconds.
Reach your target audience.
Our
audience.
Contact me today to place your ad.
Tod McCloskeySales Manager
440-891-2739

MARKETPLACE
MedicalEconomics.com58 MEDICAL ECONOMICS ❚ JUNE 25, 2016
Advertiser IndexBayer AGAleve . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27
Commonwealth LaboratoriesIBSchek . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7
Janssen Pharmaceuticals, Inc.Invokana . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16a – 16h*, 17*, Back cover
Kareo . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
TevaProAir RespiClick . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 – 23
* Indicates a demographic advertisement.
It’s as if job candidates are delivered to your door.Place a recruitment ad in Medical Economics.
Joanna ShippoliNational Account ManagerHealthcare Careers(440) [email protected]
C A R E E R S

MedicalEconomics.com MEDICAL ECONOMICS��]��JUNE 25, 2016 59
THE LAST WORD
raditional primary care is failing, and physicians are burning out at a high rate for two main reasons: Insurance payments in fee-
for-service practice do not reimburse primary care well, forcing physicians to care for large numbers of patients; and the work of primary care has become more complex, with comprehensive prevention and chronic illness man-agement in an aging society, such that brief visits are no longer eff ective.
Garrison Bliss, MD, a general inter-nist in Seattle, Washington is a found-er of concierge medicine. Concierge practice, with a very small patient panel and a high cost to patients—gen-erally more than $1,500 per year—be-came popular in the previous decade with primary care physicians wanting to get off the treadmill of traditional practice. But concierge practice has limited potential in most communities due to its high cost.
Recognizing this, Bliss turned his interest to founding “direct primary care.” Here, the patient pays a monthly fee—typically about $75—for all the services provided in a primary care practice. Th e primary care physician can do well fi nancially with panels of patients of 1,000 or fewer. More time and attention can be given to meeting the needs of each patient. Th e physi-cian and patients are much happier,
and the model is aff ordable for more of the population.
A variation on direct primary care’s global fee is a hybrid payment model. Patients pay a “membership fee” of about $50 per month for all non-visit services such as online communica-tion, telephone visits and better care coordination and then the patient’s insurance is billed for visits. Th is com-
bination pays enough for physicians to employ team members to help with pa-tient care, such as physician assistants, nurse practitioners, heath coaches and more activated medical assistants do-ing more advanced care coordination such as tracking referrals. Patient visits are longer, typically 30 to 60 minutes for routine new and follow-up care.
A major development is that research shows that more compre-hensive primary care, such as with direct primary care, improves quality
and lowers overall healthcare costs. Commercial insurance companies, Medicare and even Medicaid are starting to provide contracts to direct primary care physicians for popula-tions of patients.
Direct primary care saves money by reducing the need for emergency de-partment visits and hospital stays. Th e population served becomes healthier
through more comprehensive care. With advanced information system tools, secure online communication and team practice, direct primary care mod-els are likely to become the traditional primary care of the 21st century.
Joseph E. Scherger, MD, MPH, is a family physician in La Quinta, California, and a member of the Medical Economics editorial advisory board. Do you think Direct Primary Care can replace traditional fee-for-service care? Tell us at [email protected].
READ MORE Innovations in practicing direct primary care PAGE 18
T
Direct primary care may become the norm
BY JOSEPH E. SCHERGER, MD, MPH
“A major development is that research shows that more comprehensive primary care, such as with direct primary care, improves quality and lowers overall healthcare costs.”

MO
RE THAN
8 MILLIO
N
PRESCRIPTION
S TO DATE 1
*
© Janssen Pharmaceuticals, Inc. 2016 April 2016 049570-160318
Janssen Pharmaceuticals, Inc.Canaglifl ozin is licensed from Mitsubishi Tanabe Pharma Corporation.
Learn more and register for updates
at INVOKANAhcp.com
* Data on fi le. Based on TRx data sourced from IMS NPA Database, weekly data through 4/8/16.† Coverage that makes brand-name medications available at a lower co-payment than Tier 3 brand-name drugs. Tier 1 medications are usually generics with low co-payments.
Reference: 1. Data on fi le. Janssen Pharmaceuticals, Inc., Titusville, NJ.
PREFERRED COVERAGE† FOR MOST COMMERCIAL ANDMEDICARE PART D PATIENTS1