Sleep Medicine on the Fly- What Every Physician Should Know \Integration of Psychiatry into Primary...
91
Sleep Medicine on the Fly- What Every Physician Should Know \Integration of Psychiatry into Primary Health Care Conference- January 2014 Deputy Psychiatrist in Chief- UHN Associate Professor Department of Psychiatry, University of Toronto Diplomate American Board of Psychiatry and Neurology Diplomate American Board of Sleep Medicine Raed Hawa MD, FRCP, DABSM, DABPN
-
Upload
itzel-finnie -
Category
Documents
-
view
219 -
download
5
Transcript of Sleep Medicine on the Fly- What Every Physician Should Know \Integration of Psychiatry into Primary...

Sleep Medicine on the Fly- What Every Physician Should Know
\Integration of Psychiatry into Primary Health Care Conference- January 2014
Sleep Medicine on the Fly- What Every Physician Should Know
\Integration of Psychiatry into Primary Health Care Conference- January 2014
Deputy Psychiatrist in Chief- UHNAssociate ProfessorDepartment of Psychiatry, University of TorontoDiplomate American Board of Psychiatry and NeurologyDiplomate American Board of Sleep MedicineSpecialty Certification in Psychosomatic MedicineSpecialty Certification in Sleep Medicine
Raed HawaMD, FRCP, DABSM, DABPN

Disclosure: Dr. Raed Hawa
Advisory board, speakers’ bureaus, grant, financial or research support
No conflict of interest and no financial interest or other affiliation to declare

A Road Map?
At the end of today's session participants are expected to:
1. improve their knowledge of sleep medicine as it pertains to their practice
2. become aware of the options that are available to treat these sleep disorders
3. appreciate the complexity and co-morbidity between psychiatric disorders and sleep disorders
*It is all about how it applies to your practice*

Why should physicians be interested in sleep disorders?
Sleep/tiredness/sleepiness complaints
Insomnia is often an early presentation of a psychiatric or medical illness
Many sleep disorders may mimic psychiatric illnesses ( sleep apnea and depression)
Medications affect sleep
Our patient population can benefit from basic sleep hygiene practices

QUESTION
What is Philagrypnia?

Clinical Vingette
David, a 48 yo married male, a banker, and a father of 2 ages 14 and 16.
Long history of recurrent major depressive episodes with multiple trials of SSRIs, SNRIs and Bupropion
Currently of Venlafaxine XR 225mg/day
Current complaints of increased irritability and missing work that he attributes to poor sleep
What might be the causes for David’s insomnia?

Tools to help us

SLEEPAwake – low voltage – random, fast
N1-Stage 1 – 3 to 7 cps – theta waves
Drowsy – 8 to 12 cps – alpha waves
N2-Stage 2 – 12 to 14 cps – sleep spindles and K complexes
N3 -Delta Sleep – 1 1/4 to 2 cps – delta waves > 75 mV
R-REM Sleep – low voltage – random fast with sawtooth waves

Normal Sleep Histogram
Hours of Recording
REM
W
N1
N3
N2
1 2 3 4 5 6 7

Is it a primary sleep disorder?
Obstructive sleep apnea (4-8%)
Restless leg syndrome (2-15%)
Insomnia (10-30%)
Parasomnia ( 5-10% )
EDS ( <5% )

OSAS
Cessation of breathing lasting at least 10 seconds with desaturations and arousals.
Some of the signs and symptoms:
Snoring, gasping for air, stopping breathing at night, memory complaints, irritability, depression, morning headaches, sexual problems, restless sleep, and sedation or tiredness during the day.


OSAS
Why treat?High blood pressureHeart problems- 8 to 10 times more likely to have heart attacks or strokesMore health care money- 2.5 times more likely to visit a doctorMore likely to die in their sleep- 2.5 times more likelyPoor quality of life and 3 times more likely to be involved in car accidents

OSAS Rx
Didgeridoo!!
Weight loss/ Bariatric Surgery
EPAP
Surgery/ Pillar procedure/ Maxillofacial
Dental Device
CPAP – gold standard

If (s)he snores suspect apnea
ALSO CONSIDER STOPBANG & MALLAMPATI

STOP BANG questionnaire
S do you Snore
T do you feel Tired, fatigued or sleepy
O have you been Observed to stop breathing
P high blood Pressure
B BMI >35
A Age >50
N Neck circumference >40
G Gender: Male Anesthesiology 2008; 108:812-821

MALLAMPATI SCORE

Does the patient have apnea?
• Her BMI is 22. She is on methadone for prior heroin abuse. She denies sleep difficulties but has been complaining of sleepiness.
What would be your clinical concern?


What About This?
Restless leg syndrome
First described by Willis in 1672
Diagnostic Criteria ( strictly clinical ):
Desire to move limbs ( creepy crawly sensation, itchy and aching feeling, crampy and painful ) with
Motor restlessness
Worse at rest
Temporary relief by activity
Worse at night International RLS Study Group 2006
Periodic limb movements
PLMS: Diagnosis is based on PSG findings.
PLMD: PLMS plus sleep dysfunction.
80% of RLS patients have PLMS
Asymptomatic PLMS does not require treatment.

RLS
Rule out:
Iron deficiency, Uremia, RA, Peripheral neuropathy, Diabetes, Pregnancy, Spinal cord lesion, Medications.
“The Mimics”
Akathisia ( drug induced or positional ), peripheral neuropathy, nocturnal leg cramps, sleep starts, anxiety, and psychosis.

Pathophysiology RLS
SPECT/PET
Reduction of caudate and putamen D2 receptor binding
Brain Iron Transport
CSF ferritin low- abnormal iron transport
fMRI
Decreased thalamic blood flow during RLS symptoms
Treatment RLS
Dopamine Agonists
Ropinirole-- 0.25 to 3 mg (D2 agonist)
Pramipexole-- 0.125 to 1.5 mg (D2 and D3 agonist)
Cabergoline-- 1 to 4 mg
Pergolide-- 0.05 to 0.75 mg
Bromocriptine– 5 to 20 mg
Ldopa-carbodopa– 25 to 400 mg

Treatment RLS
Opioids:Codeine(15-120 mg),Oxycodone(2.5-20 mg), Methadone (5-
30 mg)
Benzodiazepines:
Clonazepam (0.5-2 mg), Temazepam (15-30mg)
Other treatments:Gabapentin, Carbamazepine, Clonidine, Baclofen, B12,
Folate

If your patient has RLS/PLMD?
R/O other causes
Check ferritin levels
If less than 50 – treat with Fe
Add vitamin C
If no help, try medications

B. Wayne Blount, MD, MPHProfessor, Emory S.O.M.
Insomnia- Scope of the Problem
Prevalence: 30% of general population have complaints of sleep disruption and 10% have associated functional impairment
Almost all major mental illness is associated with “some” sleep complaint
Insomnia can be the presenting complaint for anxiety, depression or a sign of abuse potential
Many medical problems can have sleep complaints as part of the presentation

Insomnia- Definitions
Global dissatisfaction with sleep and one of:
1.Difficulty initiating sleep
2. Difficulty maintaining sleep
3. Early morning awakening
With distress or impairment
3 nights/week for 3 months
3 months
Despite adequate opportunity for sleep
Episodic, persistent or recurrent

Pathophysiology of Insomnia
Disorder of hyperarousal - hypervigilance during day with difficulty initiating/maintaining sleep during the night
Cognitive model
Physiologic model
Neuroendocrine model
Increased autonomic activity in sleep ( HR, MR, BP,Temperature ,NE secretion, HPA
activation)
Increased beta/gamma and decreased delta EEG activity
Increased brain glucose metabolism Sleep Med Rev 2010 14(1):9-15

Why care about insomnia?
Insomnia prevalence increases with greater medical comorbidity
There is increased prevalence of medical disorders in those with insomnia
Insomnia with objective short sleep duration is associated with high risk for hypertension
Insomnia with objective short sleep duration is associated with high risk for type 2 diabetes
Insomnia with objective short sleep duration is associated with neuropsychological deficits
Sleep 2009;32:491-497Sleep 2010;33:459-465
Sleep 2007;30920:213-218

Treatment Options
I. Behavioural and Cognitive therapies
II. Prescription medications

Behavioural and Cognitive TherapiesStandards of Practice
Stimulus control
Relaxation therapy
Cognitive behavioural therapy CBT-I
Stimulus control
Sleep restriction
Sleep hygiene
Sleep 2006;29:1415-1419

Clinical Practice Point
Most behavioural treatments studied are six one-hour sessions by trained therapists
There are a few basic principles that can be utilized in your practice
Establish a rapport with your patient, listen, instill hope and follow-up
Rely on principle of conditioning and good sleep hygiene practices
Self monitoring , treatment rationale, and homework
Psychological & Behavioural Treatments For Chronic Insomnia
Psychological / behavioural interventions
Stimulus control therapy
Relaxation training
Cognitive behaviour therapy ± relaxation
Sleep restriction
Multicomponent*
Paradoxical intention
Biofeedback
*stimulus control + relaxation + sleep hygiene OR stimulus control + sleep restriction + sleep hygiene.

FDA Approved Insomnia Treatment
Immediate Release benzodiazepines Dose (mg) T1/2 (hr)
Estazolam (ProSom®) 1,2 8-24
Flurazepam (Dalmane®) 15,30 48-120
Quazepam (Doral®) 7.5,15 48-120
Temazepam (Restoril®) 7.5-30 8-20
Triazolam (Halcion®) .125,.25 2-4
Immediate Release Non-benzodiazepines
Eszopiclone (Lunesta®) 1,2,3 5-7
Zaleplon (Sonata®) 5,10 1
Zopiclone (Imovane®*) 5,7.5 5-7
Zolpidem (Ambien®) (Sublinox *) 5,10 1.5-2.4
Selective Melatonin Receptor Agonist
Ramelteon (Rozerem®) 8 1-2.6Doxepin----3m and 6 mg(for maintenance insomnia)
* Available in Canada and not in USA

Benzodiazepine Receptor Agonists
All BDZ receptor agonists are GABA modulators at the GABAA receptor complex
GABAA-receptor: pentamer
Allows chloride ions to enter
Greater polarization and hence inhibitory
Non benzodiazepines have a higher degree of alpha1 subtype selectivity

Recommendations For the Management of Insomnia: Pharmacotherapies
Line of therapy
Class of medication Example medications
1st lineShort-intermediate acting benzodiazepinesMelatonin receptor agonist
Zolpidem, eszopiclone,* zaleplon,* temazepamEx: agomelatine*
2nd line Alternate short-intermediate acting benzodiazepines
Sedating antidepressantsTrazodone, amitriptyline, doxepin, mirtazapine
Insomnia + comorbid mood disorder
Combined benzodiazepine and sedating antidepressants
Anticonvulsants Gabapentin, tiagabine*
Atypical antipsychotics Quetiapine, olanzapine
*not available in Canada.





Insomnia and Depression
Up to 90% of MDE patients complain of insomnia
Up to 40% of patients complaining of insomnia could have a mood disorder
Subjective complaints of difficulty initiating, maintaining sleep or early awakening
Objective findings: decreased REM latency, increased % REM, increased first REM period and decreased SWS

Antidepressants and Sleep
SSRI
Venlafaxine
Duloxetine
BUPROPION
MIRTAZAPINE
TCA

SSRIs and Sleep
Idiosyncratic effects: can cause insomnia or agitation in any individual patient
Up to 60% of patients on SSRIs are also on a hypnotic
All SSRIs decrease SE, suppress REM, delay REM onset, and increase S1 sleep
There appears to be a trend where:
Fluvoxamine and paroxetine are more sedating
Fluoxetine is more stimulating
Sertraline, citalopram and escitalopram are neutral

Clinical Practice Point
Trazodone, TCAs and mirtazapine are commonly used to help insomnia complaints in patients who suffer from depression or anxiety disorders
SSRI could be used alone or with a BDZ/hypnotic to help insomnia complaints in depression
Adjusting dose or timing can be helpful
Combining medication with CBT is an option

Are Antidepressants To Blame For Sleep Disturbances?
Data from placebo-controlled trials from respective product monographs; not for direct comparison between agents.Adapted from Lam et al. J Affect Disord 2009:17:S26-43 and Seroquel XR Product Monograph (2011).
0-9% 10-29% ≥30%
Are Antidepressants to Blame for Sleep Disturbances?
Role for Antipsychotics
A 45 year-old male was referred to see me for a sleep assessment
By the time I saw him he was already put on olanzapine 2.5mg po qhs and has been “doing great”. He was not sure why he needed to see me now
What are the effects of antipsychotics on sleep parameters?What is the evidence for use of antipsychotics in insomnia and in
complicated insomnia?

Antipsychotics and Sleep
Typical antipsychotics
Clozapine Risperidone Olanzapine Quetiapine Ziprasidone
Total Sleep Time
+ ++ ++ ++ ++ ++
Sleep Efficiency
+ ++ ++ ++ ++ ++
However consider:1.Weight gain and therefore worsening of apnea2.Increased leg restlessness3.Hyperlipidemia4.Glucose dysregulation5.QT prolongation

Important Quotes- NIH Chronic Insomnia Panel
“all (antipsychotics) agents have significant risks, and thus their use in the treatment of chronic insomnia cannot be recommended”
Eszopiclone and zolpidem extended release are not indicated for “short term” use
Intermittent vs regular prescription
Short term vs long term prescription
Clinical Practice Point
Antipsychotics are commonly used in patients who have psychosis and bipolar illness to help with sleep complaints
Antipsychotics are sometimes used in patients whose depression is successfully treated but still complain of their sleep
Potential effects on weight, lipids and glucose
Quetiapine is commonly used for “psychiatric insomnia”

Back to David
Is David’s insomnia most likely...
A primary sleep disorder? A residual symptom of depression?Medication-induced?Due to poor sleep hygiene?Due to something else?

David is exhibiting residual symptoms of depression and mild anxiety
His insomnia is affecting his work functioning
Would you change his treatment plan? If yes, how?
Back to David
Treatment of Insomnia
What is the most common prescribed medication for the treatment of insomnia
in the United States?
in Kuwait?

Clinical aspects of Insomnia
Treatment of insomnia is based upon the following principles:
A. Insomnia is always a symptom of a larger psychiatric disorder
B. Insomnia may lead to hypertension and diabetes
C. Reduction of depressive symptoms can improve insomnia
D. Sleep studies are always helpful in confirming the diagnosis of insomnia

Depression and sleep
Polysomnographic features of depression seen in 50% of patients diagnosed with depression include:
A. Abbreviated REM sleep onset
B. Increased REM amounts
C. Decreased slow wave sleep
D. Increased sleep fragmentation and arousals
E. Sleep studies are indicated in cases of suspected depression

Case of Mr. B
Mr. B is a healthy 20 yo male whom you have been seeing in therapy for treatment of anxiety. According to his roommate, the patient has been waking up screaming, with severe sweating and difficulty to communicate with during these episodes. The patient had severe nightmares as a child. The events typically occur after missing his normal amount of sleep because of social events or studying for tests.
Q: How would you treat these “nightmares”?

Events during sleep
Nightmares Night terrors Panic attacks (nocturnal) REM behaviour disorder Sleep walking Nocturnal seizures CONSIDER: prior history, age, dreaming episode,
time of occurrence, ability to console, autonomic arousability, and behaviours during episode.

Screening for Parasomnias
1. do you or your bed partner believe that you move your arms, legs, or body too much or have unusual behaviour during sleep?
2. do you move while dreaming as though you are attempting to carry out a dream?
3. have you ever hurt yourself or your partner while asleep?
4. do you eat or drink without full awareness during the night?
5. review medication(hypnotic) list/alcohol intake
Events during the night
Fuseli’s

Nightmares vs Night terrors
Nightmares REM related
Last 1/3 of night
Scared
Little movement
Remember dream
Consolable
Delayed back to sleep
Night terrors Non REM related
First half of night
Confused
Active
Amnesia in morning
Not consolable
Easy back to sleep

Nightmares
REM related events
Last third of the night
Vivid dreams
Dreams are remembered
Autonomic hyperarousability- mild
No confusion or disorientation

Nightmares- cont’d
Treatment to be directed for culprit- medications, withdrawal, sleep disorder, sleep deprivation
No harm results from awakenings- Reassurance
Imagery rehearsal treatment
Prazosin in cases of PTSD related n/m
Tryptophan?

Night terrors

Night terrors- cont’d
May be triggered by: febrile illness, alcohol, sleep deprivation, stress.
Medications can induce such events- hypnotics/neuroleptics/stimulants/anti-histamines and antiarrhythmic meds
R/O brain insult, brain glioma, epilepsy, cardiac insufficiency.

Night terrors- cont’d
Treatment of NREM Parasomnia
Education and reassurance
Safety precautions- if sleep walking
BDZ/ TCA
Relaxation
Hypnosis

Unusual dreams
A 66 yo male who you see for depression presented to your office with bruises to his hands and feet after falling off the bed few days earlier. He recalls having a dream where he had to defend himself from a snake. On further inquiry he indicated that his wife has been scared to sleep with him in the same bed due to his excessive movements at night. His sleep record epoch shows the following:

Unusual dreams

Unusual dreams
A 66 yo male who you see for depression presented to your office with bruises to his hands and feet after falling off the bed few days earlier. He recalls having a dream where he had to defend himself from a snake. On further inquiry he indicated that his wife has been scared to sleep with him in the same bed due to his excessive movements at night.This man likely:
A. Has loss of muscle atonia during his REM sleep
B. Has REM sleep behaviour disorder (RBD)
C. Would benefit from an SSRI
D. Will develop neuropathy with Guillain Barre-like illness
E. Will benefit from Clonazepam

ONE LAST, VERY EFFECTIVE TREATMENT OPTION
For apnea, RLS, Insomnia, parasomnias with com0rbid depression and anxiety is:

ONE LAST, VERY EFFECTIVE TREATMENT OPTION

EXTRAs
If we have time we can cover: Excessive Daytime Sleepiness
Excessive Daytime Sleepiness

Sleepy!

The "switch" for sleep is considered to be the ventrolateral preoptic nucleus (VLPO) of the anterior hypothalamus.
VLPO uses GABA and galanin to initiate sleep by inhibiting the arousal regions of the brain.
VLPO inhibits the wake-promoting regions of the brain including the tuberomammillary nucleus, lateral hypothalamus, locus coeruleus, dorsal raphe, laterodorsal tegmental nucleus, and pedunculopontine tegmental nucleus.
Hypocretin (orexin) neurons in the lateral hypothalamus help to stabilize this switch
Sleepy!

EDS
A 45 yo female has been referred to a sleep clinic for assessment of day time sleepiness and fatigue.
How do you differentiate between EDS and fatigue?
Is there a role for a sleep study? MSLT? MWT?
What are the causes for EDS?

The Epworth Sleepiness Scale
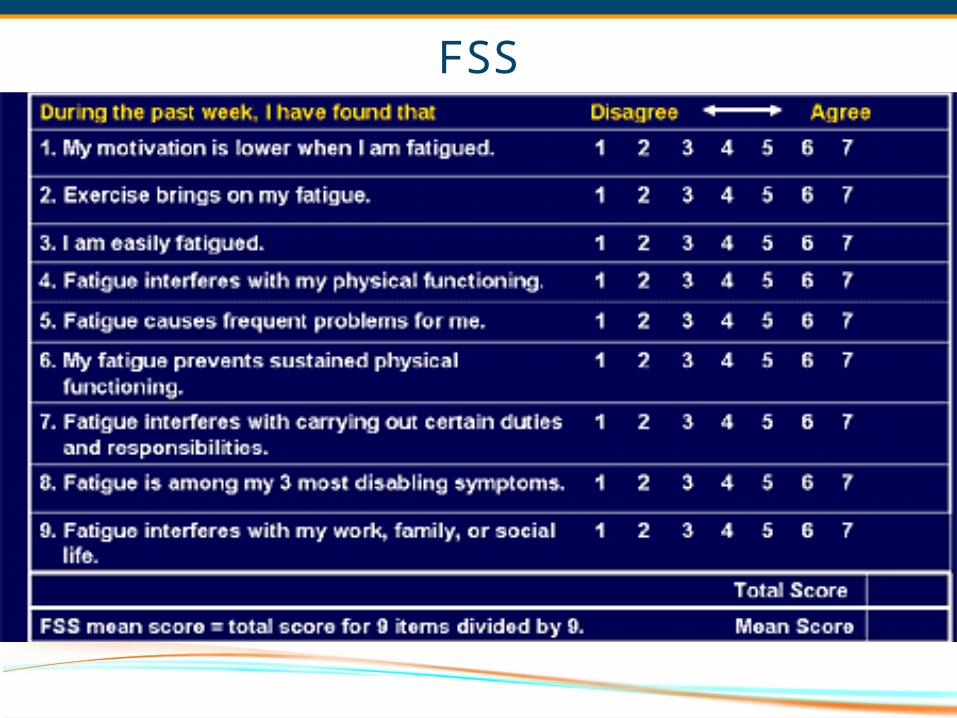
FSS

Date of download: 2/16/2013
Copyright © American College of Chest Physicians. All rights reserved.
From: Multiple Sleep Latency Test and Maintenance of Wakefulness Test
CHEST. 2008;134(4):854-861. doi:10.1378/chest.08-0822
MSLT protocol. Adapted from Littner et al.1
Figure Legend:

Excessive Daytime Sleepiness

Final question
Of the following which is the most specific finding in a patient who is known to have narcolepsy?
A.MSLT with average sleep onset of 6 minutes
B.Improvement of EDS when drinking coffee
C.Sleep paralysis
D.Hypnagogic Hallucinations
E.Cataplexy

BibliographyAn update on the dopaminergic treatment of restless legs syndrome and periodic limb
movement disorder. Sleep 2004:27(3):560-583
Brower KJ. Alcohol’s effects on sleep in alcoholics. Alcohol Research and Health 2001;25(2):110-125
Kushida CA,Littner MR,Hirshkowitz M etal. Practice parameters for the use of continuous and bilevel positive airway pressure devices to treat adult patients with sleep related breathing disorders. Sleep 2006:29(3):375-380
Morgenthaler T,Kapen S,Lee-Chiong T etal. Practice parameters for the medical therapy of obstructive sleep apnea. Sleep 2006;29(8):1031-1035
Morin CM,Bootzin RR,Buysse DJ etal. Psychological and behavioural treatment of insomnia. Update of the recent evidence. Sleep 2006;29(11):1398-1414
Neubauer DN. The evolution and development of insomnia pharmacotherapies. JCSM 2007;3(5): S11-S15
Peterson MJ and Benca RM. Sleep in mood disorders. Psychiatr Clin N 2006;29:1009-1032
Roth T. Insomnia: Definition, prevalence, etiology, and consequences. JCSM 2007;3(5): S7-S10
Schenck C, Mahowald M. Parasomnias. Post Med 2000;107(3):145-156
Silber MH. Chronic insomnia. NEJM. 2005;353:803-10

85
Fun Websites The sleep IQ test:
http://www.sleepfoundation.org/nsaw/sleepiq99i.cfm
Sleep meditation quilt square: A couple of simple things to remember and a cool site. http://www.irvingstudios.com/child_abuse_survivor_monument/Water_files/water14_help_with_sleep/help_with_sleep.html
Practice parameters for treating chronic primary insomnia in the elderly. Nat’l. Guideline Clearinghouse; www.guidelines.gov
http://cks.library.nhs.uk/insomnia/view_whole_guidance

QUESTIONS
If you have any questions I could be reached at the following address:
Raed Hawa MD FRCPC DABPN DABSM
Associate Professor, Department of Psychiatry
Deputy Psychiatrist in Chief, University Health Network
Deputy Clerkship Director, UME, University of Toronto
Director, Undergraduate Psychiatry Program, UME, University of Toronto

Extra Slides

Agomelatine and Sleep
Kasper et al. J Clin Psychiatry 2010:71:109-20.
Double-blind, randomized, controlled clinical trial of agomelatine 25-50 mg/d (n=154) vs. sertraline 50-100 mg/d (n=159) over 6 weeks.
7071727374757677787980
0 1 2 3 4 5 6
ASLEEP EFFICIENCY
77.2
78.3 78.278.8 78.9
78.4 78.9
76.5
74.8
76.475.8
75.1 75.275.7
Slee
p Effi
cien
cy (%
)
Week
AgomelatineSertaline
P value – <.0001 .018 .001 <.001 .007 .001Agomelatine n 117 117 112 112 105 99 88Sertraline n 114 113 101 93 87 79 71
B
SLEEP LATENCY
AgomelatineSertaline
Week0 1 2 3 4 5 6
10
15
20
25
30
23.5
28.426.7 28.1
29.7 29.927.8
22.5
19.5 18.8 18.8 19.6 20.218.9
P value – <.001 <.001 <.001 <.001 .003 .005Agomelatine n 117 117 112 112 105 99 88Sertraline n 114 113 101 93 87 79 71

Efficacy of Adjunctive Modafinil In Partial Responders To SSRIs With Persistent Fatigue & Sleepiness
• Other significant improvements for adjunctive modafinil vs. placebo:
• ↑ CGI-I scores• ↓ fatigue
Fava et al. J Clin Psychiatry 2005:66:85-93.
Double-blind, randomized, placebo-controlled clinical trial of 60 depressed, insomniac outpatients receiving open-label fluoxetine plus add-on eszopiclone 3 mg or placebo at bedtime for 8 weeks. CGI-I: Clinical Global Impression – Improvement.*P=0.07; † p=0.06; ‡p<0.08.
Modafinil Placebo
6
8
10
12
14
16
18
Mea
n =
SEM
HAM
-D-1
7 Sc
ore
*† ‡
Week1
Week2
Week4
Week6
Week6
Final VisitaBaseline

Quetiapine XR: Significant Effect On Sleep In Patients With MDD
Weisler et al. Int Clin Psychopharmacol 2012; 27: 27-39.
Pooled analysis of two 8 week†, RCTs of quetiapine XR in patients with MDD (n=968) Pooled analysis of two 8 week†, RCTs of quetiapine XR in patients with MDD (n=968)
*p<0.001; †6 week randomization phase, 2 week discontinuation phase; results shown are at week 6.PSQI: Pittsburg Sleep Quality Index.
*p<0.001; †6 week randomization phase, 2 week discontinuation phase; results shown are at week 6.PSQI: Pittsburg Sleep Quality Index.

ZOPICLONEZALEPLONESZOPICLONETRAZADONERAMELTEONMODAFANILSODIUMOXYBURATETEMAZEPAM
**************ZOLPIDEM AGOMELATIN