Sleep and Comorbid Neurologic Disorders and... · Sleep medicine is neurology; all sleep disorders...
22
Sleep and Comorbid Neurologic Disorders Nathaniel F. Watson, MD, MSc; Mari Viola-Saltzman, DO ABSTRACT Purpose of Review: An understanding of the impact of sleep on neurologic disorders, and the impact of neurologic disorders on sleep, provides fresh opportunities for neurologists to improve the quality of life and functioning of their patients. Recent Findings: Sleep-disordered breathing (SDB) is a risk factor for cerebrovascular disease and should be considered in all TIA and stroke patients. Sleep disorders can amplify nociception and worsen headache disorders; and some headaches, including those related to SDB and hypnic headache, are sleep specific. REM sleep behavior disorder may be an early sign of neurodegenerative disease. Focal lesions of almost any etiology (eg, multiple sclerosis and CNS malignancies) in the hypothalamus, basal forebrain, or brainstem may result in sleep disturbance, sleepiness, and insomnia. Sleep-related hypoventilation and fatigue are common in neuromuscular disease. SDB and epilepsy are mutually facilitatory, and poor sleep can exacerbate epilepsy. Summary: Continued surveillance for sleep disorders by neurologists is rewarded by new treatment avenues in their patients with the possibility of improved clinical outcomes. Continuum (Minneap Minn) 2013;19(1):148–169. INTRODUCTION Sleep medicine is neurology; all sleep disorders emanate from or involve the central or peripheral nervous system. Even sleep-disordered breathing (SDB), considered by many a pulmonary or otolaryngologic disorder, is caused in large part by ineffective maintenance of oropharyngeal muscle tone in sleep. The intersection between sleep and neuro- logic disorders is broad and deep. Al- most every neurologic disorder affects or is affected by sleep. CEREBROVASCULAR DISEASE AND SLEEP-DISORDERED BREATHING Multiple well-adjusted, cross-sectional studies show a dose-response relation- ship between sleep-disordered breath- ing (SDB) severity and odds of prevalent stroke. 1,2 Longitudinal studies also dem- onstrate that increased SDB severity increases incident stroke risk. 2Y6 Even mild SDB is associated with increased incident stroke 5 and increased risk of composite stroke, TIA, or death. 6 The reverse is also true: incident cardiovas- cular disease is associated with worsen- ing of SDB over a 5-year period. 7 Incident stroke in particular increases central SDB, which is common following stroke, and may represent silent brain ischemia disturbing central respiratory mechanisms. 8 Table 8-1 presents a syn- opsis of epidemiologic studies assessing incident stroke in patients with SDB. Stroke timing favors a role for SDB. Awakening increases sympathetic nervous system activity and the renin- angiotensin-aldosterone axis, causing a sharp morning rise in arterial blood pressure and heart rate. Both ischemic and hemorrhagic stroke have a peak incidence in the morning hours, with ischemic stroke occurring about the time Address correspondence to Dr Nathaniel F. Watson, Harborview Medical Center, UW Medicine Sleep Center, 325 Ninth Ave, Box 359803, Seattle, WA, 98104, [email protected]. Relationship Disclosure: Dr Watson serves on the Board of Directors for the American Academy of Sleep Medicine and the American Sleep Medicine Foundation. Dr Viola-Saltzman reports no disclosure. Unlabeled Use of Products/Investigational Use Disclosure: Drs Watson and Viola-Saltzman report no disclosures. * 2013, American Academy of Neurology. Supplemental digital content: Videos accompanying this ar- ticle are cited in the text as Supplemental Digital Content. Videos may be accessed by clicking on links provided in the HTML, PDF, and iPad versions of this article; the URLs are provided in the print version. Video legends begin on page 165. 148 www.aan.com/continuum February 2013 Review Article Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Transcript of Sleep and Comorbid Neurologic Disorders and... · Sleep medicine is neurology; all sleep disorders...

Sleep and ComorbidNeurologic Disorders
Nathaniel F. Watson, MD, MSc; Mari Viola-Saltzman, DO
ABSTRACTPurpose of Review: An understanding of the impact of sleep on neurologicdisorders, and the impact of neurologic disorders on sleep, provides fresh opportunitiesfor neurologists to improve the quality of life and functioning of their patients.Recent Findings: Sleep-disordered breathing (SDB) is a risk factor for cerebrovasculardisease and should be considered in all TIA and stroke patients. Sleep disorders canamplify nociception and worsen headache disorders; and some headaches, includingthose related to SDB and hypnic headache, are sleep specific. REM sleep behaviordisorder may be an early sign of neurodegenerative disease. Focal lesions of almost anyetiology (eg, multiple sclerosis and CNS malignancies) in the hypothalamus, basalforebrain, or brainstem may result in sleep disturbance, sleepiness, and insomnia.Sleep-related hypoventilation and fatigue are common in neuromuscular disease. SDBand epilepsy are mutually facilitatory, and poor sleep can exacerbate epilepsy.Summary: Continued surveillance for sleep disorders by neurologists is rewarded by newtreatment avenues in their patients with the possibility of improved clinical outcomes.
Continuum (Minneap Minn) 2013;19(1):148–169.
INTRODUCTIONSleep medicine is neurology; all sleepdisorders emanate from or involve thecentral or peripheral nervous system.Even sleep-disordered breathing (SDB),considered by many a pulmonary orotolaryngologic disorder, is caused inlarge part by ineffective maintenance oforopharyngealmuscle tone in sleep. Theintersection between sleep and neuro-logic disorders is broad and deep. Al-most every neurologic disorder affectsor is affected by sleep.
CEREBROVASCULAR DISEASEAND SLEEP-DISORDEREDBREATHINGMultiple well-adjusted, cross-sectionalstudies show a dose-response relation-ship between sleep-disordered breath-ing (SDB) severity and odds of prevalentstroke.1,2 Longitudinal studies also dem-onstrate that increased SDB severity
increases incident stroke risk.2Y6 Evenmild SDB is associated with increasedincident stroke5 and increased risk ofcomposite stroke, TIA, or death.6 Thereverse is also true: incident cardiovas-cular disease is associated with worsen-ing of SDB over a 5-year period.7
Incident stroke in particular increasescentral SDB, which is common followingstroke, and may represent silent brainischemia disturbing central respiratorymechanisms.8 Table 8-1 presents a syn-opsis of epidemiologic studies assessingincident stroke in patients with SDB.
Stroke timing favors a role for SDB.Awakening increases sympatheticnervous system activity and the renin-angiotensin-aldosterone axis, causing asharp morning rise in arterial bloodpressure and heart rate. Both ischemicand hemorrhagic stroke have a peakincidence in the morning hours, withischemic stroke occurring about the time
Address correspondence toDr Nathaniel F. Watson,Harborview Medical Center,UW Medicine Sleep Center,325 Ninth Ave, Box 359803,Seattle, WA, 98104,[email protected].
Relationship Disclosure:
Dr Watson serves on theBoard of Directors for theAmerican Academy of SleepMedicine and the AmericanSleep Medicine Foundation.Dr Viola-Saltzman reports nodisclosure.
Unlabeled Use ofProducts/InvestigationalUse Disclosure: Drs Watsonand Viola-Saltzman report nodisclosures.
* 2013, American Academyof Neurology.
Supplemental digital content:Videos accompanying this ar-ticle are cited in the text asSupplemental Digital Content.Videos may be accessed byclicking on links provided inthe HTML, PDF, and iPadversions of this article; theURLs are provided in the printversion. Video legends beginon page 165.
148 www.aan.com/continuum February 2013
Review Article
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

most people are waking up to start theirday.9 Interestingly, none of the morecommon vascular risk factors or otheretiologic factors for stroke (includingpatient demographics, vascular distribu-tion, ischemic heart disease, previousmyocardial infarction, diabetes mellitus,hypertension, smoking, hyperlipidemia,stroke severity and recurrence, strokesubtype, and other clinical features) varyin a statistically significant manneraccording to the clock time of strokeonset.10 The temporal pattern of strokepoints to the impact of circadian factorson vascular tone, coagulative balance,and blood pressure. Perhaps most com-pellingly, a case-control study compar-ing subjects with wake-up stroke tothose without wake-up stroke foundthe wake-up stroke group had higherapnea-hypopnea and obstructive apnea
indices and lower mean oxygen sat-uration levels. The presence of severesleep apnea (apnea-hypopnea index[AHI] greater than 30 events/h) wasindependently associated with wake-upstroke.11
During healthy nocturnal sleep, bothsystolic and diastolic blood pressuresdrop by 10% to 20% from respectivedaytime mean levels. Some patients,referred to as nondippers, have less thana 10% decline in blood pressure relativeto respective daytime means. Nondip-ping, over time, likely contributes to leftventricular hypertrophy, renal pathol-ogy, and deleterious effects on brainvasculature such as atheromatous nar-rowing or occlusion of larger cerebralvessels, thickening of cerebral arteries bylipohyalinosis, and increased blood co-agulability. Nondipping blood pressure
TABLE 8-1 Synopsis of Studies Assessing Incident Stroke in Patients WithSleep-Disordered Breathing
Study N =
TimeFollowed(Years)
Numberof Events(Strokes)Observed
Fully AdjustedOdds Ratio orHazard Ratio P Value Comments
Arzt2 1189 4 21 OR: 3.08(95% CI; 0.74Y12.81)
.120 Unadjusted OR: 4.31(1.31Y14.15), P=.02
Munoz3 394 6 20 HR: 2.52(95% CI; 1.04Y6.01)
.040 HR presented for subjectswith severe obstructivesleep apnea (apnea-hypopneaindex [AHI] Q30 events/h)
Redline4 5422 ~8 193 HR: 2.86(95% CI; 1.10Y7.40)
.016 Incident stroke was notassociated with AHIquartiles in women
HR presented for highestAHI quartile (919 events/h);P value is for trend
Valham5 392 10 47 HR: 3.56(95% CI; 1.56Y8.16)
.011 HR presented for subjectswith moderate to severeobstructive sleep apnea(AHI Q15 events/h); P value isfor trend
Yaggi6 1022 ~3 88 HR: 1.97(95% CI; 1.12Y3.48)
.010 Outcome was incidentstroke and death
OR = odds ratio; CI = confidence interval; HR = hazard ratio.
149Continuum (Minneap Minn) 2013;19(1):148–169 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

pattern is associated with stroke inde-pendent of sex and race.12 Stroke risk isincreased by 80% for every 5 mm Hgincrease in sleep-time blood pressure.13
Obstructive sleep apnea (OSA) is one ofthe most common causes of nondip-ping nocturnal blood pressure.
The effect of SDB on blood pressureis not confined only to the sleep period.Approximately 50% to 60% of patientswith OSA are hypertensive, while about30% to 40% of hypertensive patientshave OSA.14 Peppard and colleagues15
performed a 4-year, population-based,prospective cohort study of OSA andhypertension. After adjusting for multi-ple confounders, they found that evenpeople with few episodes of apnea orhypopnea (0.1 events/h to 4.9 events/h)at baseline had 42% greater odds ofhaving hypertension at follow-up thanpeople with no episodes. They alsofound those with mild SDB (AHI of 5.0events/h to 14.9 events/h) and thosewith more severe SDB (AHI of 15.0 ormore events/h) had approximately 2 and3 times, respectively, the odds of havinghypertension at follow-up than thosewith no episodes of apnea or hypo-pnea.15 Resistant hypertension is definedas blood pressure that requires four ormore antihypertensive medications.Stunningly, 80% to 90% of these patientshave OSA. Pathophysiologic mecha-nisms include activation of the renin-angiotensin-aldosterone system byintermittent hypoxia and aldosterone-related fluid retention causing para-pharyngeal edema.14 Thus, OSA is a riskfactor for hypertension and a major riskfactor for stroke.
Treatment of Obstructive SleepApnea to ImproveBloodPressureIn two meta-analyses reporting changesin blood pressure levels, patients ran-domized to continuous positive airwaypressure (CPAP) therapy compared withcontrols reduced systolic blood pressure
by approximately 1.5 mm Hg to 2.5mm Hg and diastolic blood pressure by1.5 mm Hg to 2.0 mm Hg.16,17 Inanother two meta-analyses reportingchanges in blood pressure obtained byambulatory monitoring, CPAP use wasassociated with an approximately 1.0mm Hg to 1.5 mm Hg reduction inboth 24-hour systolic and diastolic bloodpressure.18,19 In subgroup analyses,severe OSA (more than 30 events perhour), higher blood pressure levels, andgreater CPAP adherence were associ-ated with larger reductions in bloodpressure.16Y19
Additional Obstructive SleepApnea–Related Factors ThatIncrease Stroke RiskOSA increases systemic sympatheticnervous system activity and atrial size(through left ventricular hypertrophyand increased transmural pressure),which increases the risk of atrial fibrilla-tion, a major stroke risk factor.20 In ad-dition, cardioverted atrial fibrillation ismore likely to recur in untreated versustreated OSA patients.21 Sleep disrup-tion and chronic intermittent hypoxiain OSA increase oxidative stress andvascular inflammation, which results inendothelial dysfunction characterized byreduced vasodilatation and enhancedvasoconstriction, including chronic pro-thrombotic and procoagulant activity.22
Apneas are associated with reducedcerebral perfusion and delayed cere-brovascular compensatory response tochanges in blood pressure.23,24 CPAPtherapy has beneficial effects on vas-cular function and inflammatory andoxidative stress in these patients.25 OSAis associated with patent foramen ovale(PFO), an important cause of crypto-genic stroke. During an obstructive ap-nea, large intrathoracic pressure swingsand hypoxic pulmonary vasoconstric-tion act in concert to alter the interatrialpressure balance in favor of right to left
KEY POINTS
h Sleep-disorderedbreathing is a term thatencompasses allbreathing disturbancesin sleep, includingobstructive sleep apnea,central sleep apnea,Cheyne-Stokesrespirations, and upperairway resistancesyndrome.
h Sleep-disorderedbreathing is anindependent risk factorfor stroke.
150 www.aan.com/continuum February 2013
Comorbid Neurologic Disorders
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

PFO shunting,26 which may be pre-ventable with CPAP therapy.27 Thepresence of sleep apnea, including theduration and severity of disease, isassociated with carotid intima-mediathickness,28 some of which is reversi-ble with the application of CPAP ther-apy.29 SDB is also associated withdiabetes mellitus and insulin resist-ance, with the strength of association in-creasing as a function of OSA severity.30
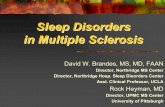
The effect of CPAP therapy on glucosemetabolism in patients with OSA hasyet to be established. Figure 8-1 dis-plays the complicated risk-factor rela-tionship between SDB and stroke.
Treatment of Sleep-DisorderedBreathing to Prevent StrokeIn patients with previous cardiovascularevents and moderate to severe OSA,those noncompliant with CPAP therapyhad an increased incidence of newischemic stroke compared to the com-
pliant group.31 Long-term CPAP treat-ment in moderate to severe OSA andischemic stroke is associated with a re-duction in excess risk of mortality.32
Treatment of OSA by CPAP in strokepatients undergoing rehabilitation im-proved functional and motor, but notneurocognitive, outcomes.33 Random-ized controlled trials are ongoing withthe goal of determining whether CPAPtherapy for OSA can prevent incidentcardiovascular disease and death.
Sleep-Disordered BreathingFollowing StrokeAcutely poststroke, over two-thirds of 161stroke patients had an AHI of more than10 events/h. After 3 months, both theAHI and central apnea index were signifi-cantly lower than in the acute phase,predominantly because of reductionsin central apneas, since the obstructiveapnea index remained unchanged. Inter-estingly, stroke location, type, or vascular
FIGURE 8-1 Interplay of risk factors for sleep-disordered breathing (SDB) and stroke. SDB influences stroke through shared riskfactors, facilitation of traditional stroke risk factors, and physiology unique to SDB. The latter likely explains whySDB is associated with incident stroke after adjustment for many of these other risk factors.
151Continuum (Minneap Minn) 2013;19(1):148–169 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

territory was not associated with SDB inthis study.34 This, along with the fact thatSDB frequency and severity are thesame for stroke and TIA patients,35
suggests that although stroke itself canworsen SDB through effects on orophar-yngeal musculature and brainstem respi-ratory centers, the SDB likely precedesthe vascular event in most cases.
Sleep Duration and StrokePathophysiologyA recent study found both short andlong sleep durations to be associatedwith stroke, independent of age, sex,bodymass index, physical activity, smok-ing, alcohol use, screen time (eg, timespent in front of TVs, computers, tablets,smart phones), country of birth, maritalstatus, education, and employment sta-tus. Compared with a sleep duration of7 hours (referent), the multivariate oddsratio (OR) of stroke for various sleepdurations was as follows: less than 6hours, OR = 1.54 (1.36Y1.75); 6 hours,OR = 1.25 (1.14Y1.38); 8 hours, OR =1.08 (1.00Y1.17); and 9 hours or more,OR = 1.50 (1.38Y1.62).36 The exactmechanism is unknown but likely re-lated to effects on metabolic, endo-crine, and autonomic nervous systems.
Conclusions. SDB is an indepen-dent risk factor for stroke. It meets thecriteria of biological plausibility, predic-tiveness, dose-responsiveness, and pre-stroke measurability. SDB is associatedwith many known stroke risk factors,including incident hypertension, endo-thelial dysfunction, oxidative stress,vascular inflammation, prothromboticand procoagulant factors, arrhythmias,diabetes, PFO, and carotid intima-media thickness. Treatment of SDBwith CPAP improves many stroke riskfactors, including reducing hyperten-sion and carotid intima-media thick-ness, reversing right to left shunting inPFO, and reducing recurrence of atrialfibrillation following cardioversion.
Unfortunately, despite the strength ofthe evidence, SDB is regularly unrecog-nized and undiagnosed in both primarycare and neurology/stroke clinics acrossthe country. Considering what is atstake, evaluation for SDB is essentialto the workup of any TIA or strokepatient. The identification and treat-ment of SDB in these patients providesa tremendous opportunity for neurolo-gists and stroke specialists to mitigatethe adverse effects of cerebrovasculardisease (Case 8-1).37
MOVEMENT DISORDERS ANDSLEEP IMPAIRMENTSleep andmovement disorders overlap ina number of important ways. This sectionfocuses on the sleep-related ramificationsof the dystonias, choreiform disorders,tremors, and tics. Other sections of thisarticle address othermovement disorder-related issues, including the relation-ship of sleep with Parkinson disease(PD) and dementia with Lewy bodies.
Sleep impairment and its secondarysymptoms have substantial quality of liferamifications for patients with dystonia.Cervical dystonia is associated with re-duced sleep quality and sleepiness, evenwhen compared to other focal move-ment disorders.38 A number of poly-somnographic abnormalities have beenreported, including problems with sleepinitiation and maintenance, reducedsleep efficiency, abnormal or reducedREM sleep, and changes in spindleactivity.39 Similar to other nonmotordystonia symptoms, the etiology ofsleep abnormalities includes primary ef-fects of dystonia and secondary effectsof pain and medications (eg, benzodia-zepines, anticholinergics). Some formsof dystonia, including blepharospasmand Meige syndrome, may persist dur-ing sleep, although frequency and se-verity are often decreased.
Sleep problems are present in nearly90% of patients with Huntington disease
KEY POINTS
h Sleep-disorderedbreathing should beconsidered in all strokeand TIA patients.
h Cervical dystonia isassociated with reducedsleep quality andsleepiness, even whencompared to patientswith other focalmovement disorders.
152 www.aan.com/continuum February 2013
Comorbid Neurologic Disorders
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

(HD), with nearly two-thirds rating sleepdysfunction as either very or moderatelyimportant factors contributing to overallhealth impairment.40 As HD progresses,non-REM (NREM) sleep stages N1 andN2 are increased, and NREM sleep stageN3 and REM are decreased. In contrastto other neurodegenerative diseases,patients with HD show a higher densityof sleep spindles compared to healthycontrol subjects. Actigraphy studiesshow patients with HD have significantlymore movements and increased activityduring sleep compared with controls.With increasing HD severity, sleeplatency increases, sleep maintenancebecomes more difficult, sleep efficiencyreduces, wakefulness after sleep onsetincreases, circadian rhythmicity be-comes compromised, and sleepinessensues.41 SDB, narcolepsy, and restlesslegs syndrome are not more common inpatients with HD, as opposed to peri-odic limb movements of sleep (PLMS),
which are increased in HD and mayrepresent chorea rather than periodiclimb movement disorder.41 HD is asso-ciated with brainstem atrophy, evenbefore caudate atrophy and in one smallstudy, REM sleep behavior disorder(RBD) was observed in 12% of patientswith HD.42 In general, chorea anddyskinesias decrease and may even dis-appear during sleep, making these un-likely major sleep disrupters in HD, asopposed to dystonia, dementia, bodypain, and nocturia, which more likelyimpair sleep in this disorder. Atrophy inthe dorsolateral hypothalamus (site ofhypocretin/orexin production) and ante-rior ventral hypothalamus (site of thesuprachiasmatic nucleus) may explainsleepiness and circadian and other sleepdisruption in this disorder.
When compared to age- and sex-matched controls, patients with essentialtremor have poorer nocturnal sleep qual-ity but not increased daytime sleepiness.43
KEY POINT
h Sleep disturbance ispresent in nearly 90%of patients withHuntington disease,with most rating it asignificantly importantfactor in overall healthimpairment.
Case 8-1An obese 59-year-old hypertensive man presented to his primary carephysician because of a transient episode of difficulty speaking 2 days earlier.In the course of the examination, the physician found evidence for atrialfibrillation. Diagnostic testing included echocardiography significant forpatent foramen ovale (PFO) with a positive bubble test indicating right toleft shunting, and hypercholesterolemia. Carotid ultrasound was normal.The physician referred the patient to a cardiologist for cardioversion of hisatrial fibrillation, and prescribed warfarin, metoprolol, and simvastatin.The patient’s atrial fibrillation was successfully cardioverted 4 weeks afterwarfarin therapy, and warfarin was switched to aspirin 4 weeks aftercardioversion. Three weeks later, the patient presented to the emergencydepartment aphasic and hemiparetic from a large left middle cerebral arterydistribution stroke and was found to have recurrent atrial fibrillation.
Comment. This obese older man with hypertension, atrial fibrillation,and PFO is at high risk for having sleep-disordered breathing (SDB).Because no evaluation and management of the SDB was done, the patientwas at higher risk for recurrent atrial fibrillation following cardioversionand subsequent stroke. Although whether treatment of SDB withcontinuous positive airway pressure reduces incident stroke is unknown, it isclear that untreated sleep apnea increases the risk of recurrence of atrialfibrillation following cardioversion. PFO is also associated with SDB, butatrial fibrillation is a more likely explanation for the stroke mechanism inthis patient. Evaluation for SDB should be performed in TIA and strokepatients as part of their stroke workup.
153Continuum (Minneap Minn) 2013;19(1):148–169 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

However, pain and fatigue scores wereelevated among patients with essentialtremor, suggesting many misconstruesleepiness as fatigue. RBDdoes not appearto be associated with essential tremor.
Caregiver observations indicate sleepproblems in 20% to 50% of children andyoung adults with Tourette syndrome.Difficulties in falling and staying asleep,separation anxiety in the evening, andparasomnias were the most commonproblems.44 Children with tic disorderand Tourette syndrome have objectivesleep impairment indicated by reducedsleep efficiencies, prolonged sleeplatencies, and increased arousal indi-ces.44,45 The disturbed sleep of childrenwith Tourette syndrome is accompa-nied by increased short-lasting motoractivity in NREM sleep, which likelyrepresents tic activity during sleep.44
HEADACHE DISORDERSAND SLEEPSleep and headache have a complicatedinterrelationship. Although a history ofheadache upon awakening raises a con-cern for a space-occupying CNS lesion,this symptom is more likely to representSDB, especially in obese men withtension-type headache pain that dissi-pates during the course of the day. Insome instances, sleep improves head-ache, as exemplified by the typical pa-tient with migraine lying in a dark, quietroom. In other instances, such as hypnicheadache, sleep and specific sleep stagestrigger the headache. Headache pain, orpain of any kind, adversely affects sleeparchitecture, duration, and quality; andpatients with sleep disorders report over4 times more headaches than healthycontrols.46
Sleep disorders such as insomnia,SDB, sleep-related movement disor-ders, and circadian rhythm disordersare disproportionately observed in spe-cific headache patterns (eg, chronicdaily headache, awakening headache)
and diagnostic groups (eg,migraine, clus-ter, tension-type). Variations in circadiantiming of sleep and sleep duration out-side typical norms (ie, 7 to 9 hours pernight) are common headache triggers. Al-though sleep and headache associationsare diverse, sleep dysfunction influencesheadache threshold through effects onsleep regulatory processes.47 Relative to anage- and sex-matched chronic headacheYfree comparison group, headache pa-tients slept significantly shorter durations(6.7 versus 7.0 hours), reported longersleep latencies (31.4 versus 21.1 min-utes), and took longer to resume sleepfollowing nighttime awakening (28.5versus 14.6 minutes).48
Chronic morning headache occurs innearly 8% of the population, with sleepcomplaints more typical among thosewith tension-type than migraine head-ache.49 Of migraine patients, 24% de-scribe headache onset during sleep orupon awakening as opposed to 12% oftension-type headache patients.46 Head-ache is more common among peoplewith SDB than the general population,and habitual snoring is more typical ofchronic daily headache than episodicheadache. Morning headache is over 3times more common in snorers andapneics compared to healthy controls.Bruxism is another potential cause formorning headache. In a study of over1000 patients with migraine, sleep dis-turbance and oversleeping were recog-nized as headache precipitants by 50%and 37% of patients, respectively, while85% reported sleeping as a means torelieve headache. Many reported occa-sional sleep-onset (53%) and mainte-nance (61%) difficulties. Almost two-thirds reported morning headaches.50
Cluster headache patients have an eight-fold increase in OSA compared to age-and sex-matched controls, and a 24-foldincrease when overweight or obese.51
Treatment of OSA has been shown toimprove cluster headache control.46
KEY POINTS
h Sleep is impaired in20% to 50% ofchildren and youngadults with Tourettesyndrome.
h Obstructive sleep apneais a common cause forheadache uponawakening, particularlyif it dissipates during thecourse of the day.
h Bruxism should beconsidered as a potentialcause for headacheupon wakening.
h Patients with clusterheadache have aneightfold increasedrisk of obstructivesleep apnea whencompared to age- andsex-matched controls.
154 www.aan.com/continuum February 2013
Comorbid Neurologic Disorders
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Hypnic headache is a rare primaryheadache disorder in older adults char-acterized by moderate, throbbing, bilat-eral, or unilateral sleep-related headacheattacks with typical onset in REM sleep.Headache duration can be anywherefrom 15 minutes to 3 hours. In REM,dorsal raphe and locus coeruleus activityis absent and these areas, along withthe periaqueductal gray, are essentialcomponents of the human antinoci-ceptive system. Hypnic headache maytherefore represent REM-related mal-function of these neuroanatomic re-gions, although this may not be specificsince migraine and cluster headacheonset also commonly occur in REM.Because many patients with hypnicheadache experience headache onset ata consistent time of night, areas involvedin circadian rhythm generation, such asthe suprachiasmatic nucleus (SCN), alsomay be involved. The SCN has afferentand efferent connections with the peri-aqueductal gray, further strengtheningthis notion. Caffeine, either at bedtime orfollowing headache onset, is an effectivetreatment but concerns for sleeplessnesslimit its use. Lithium, indomethacin, andmelatonin are also helpful in some pa-tients, along with other headache med-ications on a case-by-case basis.52
Because sleep and headache are sotightly linked, diagnosing and treatingcomorbid sleep disorders afford anopportunity to improve the headacheproblem. Themost likely sleep disordersfor headache causality are SDB, sleepdeprivation, and circadian rhythm dis-turbances. A number of good screeninginstruments are available for clinical useto help identify headache patients thatmight benefit from consultation with asleep medicine specialist (Table 8-2).
EPILEPSY AND SLEEPSleep disorders and epilepsy are fre-quently comorbid. The relationship be-tween the two can be reciprocal; sleep
disorders can contribute to difficulty inmanaging seizures, and epilepsy candisrupt normal sleep, initiating or wor-sening sleep disorders. Patients withepilepsy commonly report poor sleepquality, increased nocturnal awakenings,early morning awakenings, difficulty ini-tiating sleep, and excessive daytimesleepiness. Nineteen percent of general-ized seizures occur during sleep, as com-pared to 51% of localization-relatedseizures. One in five patients with epi-lepsy has seizures exclusively duringsleep. Examples of focal-onset epilepsyoccurring predominantly during sleepinclude benign focal epilepsy with cen-trotemporal spikes, and nocturnal fron-tal lobe epilepsy. Many patients have‘‘awakening epilepsy,’’ occurring within2 hours of waking; juvenile myoclonicepilepsy is a classic example. Table 8-3provides a list of epilepsies with a pre-dilection for occurrence out of sleep.
Most sleep-related seizures occur outof NREM sleep, with NREM sleep stageN2 being the most common. This sleepstage likely facilitates focal spikes andepileptic activity through thalamocorti-cal hypersynchrony, as represented bycharacteristic sleep spindles and K com-plexes. Hypersynchronous delta activity
KEY POINTS
h Hypnic headache issleep specific, occurringrelative to REM sleep ata consistent time ofthe night.
h Epilepsy andsleep-disorderedbreathing are mutuallyfacilitatory, with higherrates of each disorderobserved in patientswith the other disorderwhen compared to thegeneral population.
h One in five patients withepilepsy has seizuresexclusively during sleep.
h Most sleep-relatedseizures occur out ofnon-REM sleep, mostoften non-REM sleepstage N2.
TABLE 8-2 Common ScreeningInstruments
b SleepinessEpworth Sleepiness ScaleStanford Sleepiness ScaleKarolinska Sleepiness Scale
b Sleep-Disordered BreathingBerlin QuestionnaireMultivariateApnea Prediction
IndexSTOP-BANG questionnaire
b InsomniaInsomnia Severity Index
b Sleep QualityPittsburgh SleepQuality Index
155Continuum (Minneap Minn) 2013;19(1):148–169 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

in NREM sleep stage N3 also facilitatesepileptiform activity. Nighttime interic-tal activity is more suggestive of thelocation of the seizure focus than day-time interictal activity.53 Seizures areleast likely to occur out of REM sleep,but when they do, they can provide themost accurate seizure localization ofany sleep stage. Seizures and epilepti-form abnormalities are typically ob-served during sleep stage transitionsand unstable sleep characterized bycortical arousals. Temporal lobe epi-lepsy is the most common sleep-related epilepsy, not because of aparticular sleep-related predilection,but because of the common nature ofthis seizure type. Frontal lobe seizureshave the greatest penchant to occurout of sleep. Approximately 61% offrontal lobe seizures begin duringsleep, as opposed to 11% of temporallobe seizures. Temporal lobe seizuresare more likely to generalize when theyoriginate from sleep, and nocturnaltemporal lobe epilepsy is thought toportend a more favorable outcome fol-lowing epilepsy surgery.54
Autosomal dominant nocturnal fron-tal lobe epilepsy is a distinct clinical
syndrome (Table 8-4). These patientshave brief stereotyped hyperkinetic ortonic motor seizures that occur inclusters during sleep following suddenarousals. Kicking and movement of legs,arms, and trunk are seen. Patientstypically maintain consciousness duringthe seizures, which usually last less than60 seconds and are stereotyped innature. Seizures usually begin in child-hood and persist throughout life. Thedisorder demonstrates an autosomaldominant inheritance pattern with anapproximate penetrance of 70%. Seiz-ures involve deep mesial frontal gener-ators and may lack ictal and interictalEEG correlates. For all these reasons,nocturnal frontal lobe epilepsy can bedifficult to differentiate from NREMparasomnias (Table 8-5) (Case 8-2).55
Historically, sleep deprivation hasbeen used to provoke epileptic-relatedEEG activity. Sleep itself may activateinterictal activity in approximately one-third of patients with epilepsy and up to90% of people with sleep-wakeYrelated
KEY POINT
h Nocturnal frontal lobeepilepsy can be difficultto distinguish fromparasomnias, withstereotypia, minimalpostevent confusion,and shorter durationproviding clues that theevent was epileptic innature.
TABLE 8-3 CommonSleep-RelatedEpilepsies
b Nocturnal frontal lobeepilepsy
b Nocturnal temporal lobeepilepsy
b Benign focal epilepsy withcentrotemporal spikes
b Juvenile myoclonic epilepsy
b Continuous spike-wavedischarges during sleep
b Childhood epilepsy withoccipital paroxysms
b Generalized tonic-clonicseizures upon awakening
TABLE 8-4 Characteristics ofAutosomal
Dominant Nocturnal FrontalLobe Epilepsy
b Brief nocturnal seizures
b Prominent motor movements
b Little or no postictal confusion
b Frequent clusters
b Often misdiagnosed as sleepdisorder
b Involves the neuronal nicotinicacetylcholine receptor " 4(CHRNA4) subunit
b Two genetic loci identified(20q13.2-3 and 15q24)
b Mutations in neuronal nicotinicacetylcholine receptor genesCHRNA4 and CHRNB2
156 www.aan.com/continuum February 2013
Comorbid Neurologic Disorders
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

or state-dependent epilepsies. Sleepdeprivation activates epileptiform dis-charges on sleep-wake EEGs and is there-fore useful in evaluation of suspectedepilepsy. Although the exact mechanism
is unknown, sleep deprivation likelyactivates epileptiform dischargesthrough direct effects of sleep loss.Neurologists should be aware that sleepdeprivationYprovoked seizures may
TABLE 8-5 Pearls for Differentiating Non–REM Parasomnias FromNocturnal Frontal Lobe Epilepsy
Event CharacteristicNon–REMParasomnia
Nocturnal Frontal LobeEpilepsy
Timing in the sleep period Early Anytime
Sleep stage Non-REM N3 Any, but Non-REMN2 is most common
Epileptiform discharges seen onpolysomnography
No Yes or no
Stereotypia present No Yes
Awakening No Yes
Duration of event 30 seconds to30 minutes
30 seconds to2 minutes
Postevent confusion Yes Typically minor
Case 8-2A 28-year-old man was brought to clinic by his wife with the complaintthat he was waking up screaming and thrashing at night. This had begunabout 6 months earlier and occurred approximately every 2 weeks. Theevents would occur at any time of the night, but were slightly less likelyduring the final portion of the sleep period. The patient would awakenabruptly, thrashing and screaming incoherently. The events lasted about30 seconds and ended abruptly; the patient may or may not have anymemory of the event. The duration and characteristics of the event wereconsistent over time. Neither the patient nor his family had a history ofsleepwalking, head injury, encephalitis, or epilepsy. His neurologicexamination and routine EEG results were normal. He was admitted for7 days of inpatient EEG monitoring during which two typical events werecaptured, but no ictal EEG correlate was found. The events resolved with atreatment trial of carbamazepine.
Comment. This case of nocturnal frontal lobe epilepsy highlights thedifficulty in differentiating nocturnal seizures from parasomnias. In this case,the events are stereotypic, have no predilection for the first third of thenight (when non-REM sleep stage N3 is more prominent), are brief, and lacksubstantial postevent confusion, thereby arguing in favor of a diagnosis ofnocturnal frontal lobe epilepsy. The lack of a family history suggests this is notthe heritable type. Although events were captured on EEG monitoring, thelack of an ictal correlate does not obviate the diagnosis, as deepmesial frontalgenerators may insidiously trigger the events. The correct management inthis case is a treatment trial, which if successful, helps confirm the diagnosis.
157Continuum (Minneap Minn) 2013;19(1):148–169 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

alter seizure semiology and thereforenot confuse these as nonepileptic events.
Compared to the general popula-tion, patients with epilepsy experiencesubstantially more sleep disturbance,characterized by increased sleep latencyand number of awakenings during nightas well as alterations in normal sleeparchitecture due to seizures, interictalepileptiform discharges, or medicationside effects (Table 8-6).56 Nearly two-thirds of patients with epilepsy have ex-cessive daytime sleepiness as defined bythe Epworth Sleepiness Scale, and nightawakening is more common in patientswith epilepsy than in normal controls,with increased seizure frequency por-tending increased sleep disturbance.
Epilepsy is more prevalent in patientswith SDB than in the general popula-tion.57 Possible reasons include OSA
effects on sleep quality or duration andacute and chronic effects of intermittenthypoxia and sympathetic activationon epileptogenic regions of the brain.The reverse is also true: SDB is moreprevalent in patients with epilepsy thanin the general population.58 Dependingon epilepsy severity and SDB definition,between 20% and 80% of epilepsy pa-tients have been reported to havecomorbid SDB.59 In a study of refractoryepilepsy patients, 33% were found tohave OSA, with seizures more likely tooccur at night than during the day.Postulated reasons for this associationinclude antiepileptic drugYassociatedweight gain (eg, valproate, gabapentin),hypothyroidism, polycystic ovarian dis-ease, and the effect of chronic epilepsyon brainstem respiratory control centersand nuclei involved in airway patency.
KEY POINT
h Medication side effectsshould always beconsidered as a cause ofsleepiness in a patientwith epilepsy.
TABLE 8-6 Effect of Antiepileptic Drugs on Sleepa
Effects on SleepEffects on Sleep Disorders
Drug Efficiency LatencyStageN1
StageN2
StageN3 REM Improves/Treats Worsens
Phenobarbitol Y , Y j 0 , Sleep-onsetinsomnia
Obstructivesleep apnea(OSA)
Phenytoin 0 , j j , 0 or , None known None known
Carbamazepine 0 0 0 0 0 0 Restless legssyndrome (RLS)
RLS
Valproate Y 0 j , 0 0 None known OSA
Ethosuximide Y Y j Y , Y None known None known
Gabapentin 0 0 0 0 j j RLS OSA
Lamotrigine 0 0b 0 j , j None known None known
Topiramate 0 , 0 0 0 0 OSAc None known
Tiagabine Y Y Y Y j Y Insomnia None known
Levetiracetam Y Y Y Y j Y None known None known
Pregabalin j Y Y Y j Y None known OSA
REM = rapid eye movement; j = increase; , = reduction; Y = not reported; 0 = no change.a Reprinted with permission from Eriksson SH, Curr Opin Neurol.54 journals.lww.com/co-neurology/pages/articleviewer.aspx?year=2011&issue=04000&article=00014&type=abstract.
b Lamotrigine may be associated with insomnia.c Due to change in weight.
158 www.aan.com/continuum February 2013
Comorbid Neurologic Disorders
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Benzodiazepines and barbiturates maycause suppression in responsiveness ofcarbon dioxide and oxygen desaturationand increase upper airway musculaturerelaxation. Vagus nerve stimulation treat-ment for epilepsy has been reported toincrease airway disturbance during sleepin some patients.60 This therapy isthought to increase airway resistancefrom increasing lateral laryngeal musculartone or by interfering with the respira-tory sensory feedback.
Seizure control may improve withtreatment of OSA. In one study, treat-ment of OSA produced a 50% or greaterreduction of seizures, with some patientsbecoming seizure free. Excessive day-time sleepiness also improved, despiteno changes or higher doses of antiepi-leptic drugs.61 Another study showedthat children with epilepsy treated sur-gically for their SDB had a 53% medianseizure reduction, with about one-thirdbecoming seizure free.62 For all thesereasons, symptoms of daytime sleepi-ness and poor sleep should not neces-sarily be considered the result ofepilepsy until other causes have beenevaluated. Epilepsy patients should beroutinely asked about these symptomsand referred to a sleep specialist whenappropriate with the goal of improvingquality of life and seizure control.
NEURODEGENERATIVEDISEASES AND SLEEPNeurodegenerative diseases, such as Alz-heimer disease (AD) and PD, are com-monly associated with sleep disorderssuch as SDB, RBD, restless legs syndrome,insomnia, and circadian rhythm sleepdisorders (Table 8-7). Sleep disruptionin people with neurodegenerative diseasemay lead to worsened cognitive statusand functional ability, increased caregiverburden, and perhaps, most importantly,hastened institutionalization.
Persistent sleep disturbances arepresent in up to 44% of patients with
AD.63 Degeneration of cholinergic neu-rons in the SCN and ventrolateral pre-optic nucleus, critical for homeostaticmaintenance of the circadian rhythmand sleep initiation, leads to sleep-wakedisturbances in AD. Sundowning, char-acterized by confusion, wandering,hyperactivity, restlessness, and agitation,is common and typically occurs duringlow-light hours in the late afternoon andearly evening in these patients. Peoplewith mild to moderate dementia spend15% of the day napping, while thosewith severe dementia spend 29% of theday napping, which leads to furthersleep difficulty at night. Cholinergicmedications, the primary treatment forAD, can cause insomnia and dreamdisturbances. Sedative-hypnotic medica-tions, used for sleep induction orbehavioral modification in AD, can havesignificant side effects such as sleepdisruption and increased injury risk.Antipsychotic medications, if used foragitation or sleep induction, can causedaytime hypersomnia. Melatonin issometimes used to regulate circadianrhythms but may not be effective asmonotherapy for sleep disturbancesin these patients. Nonpharmacologictreatments, including light therapy, ex-ercise, and sleep-hygiene modification,are safe and effective alternatives.
In PD, muscle rigidity, tremors, anddystonia can lead to difficulty with sleepinitiation and maintenance. Carbidopa-levodopa, used to treat PD, may causenightmares and insomnia. Depressionand anxiety (and antidepressants such asselective serotonin reuptake inhibitors)may also perpetuate insomnia in thesepatients.
Cell loss in brainstem nuclei thatmodulate respiration, along with bulbarand diaphragmatic muscle dysfunction,increase the risk of SDB in neurodege-nerative disease. Patients with PD are atrisk of developing SDB due to hypoki-nesia and rigidity causing upper airway
KEY POINTS
h When approaching asleep problem in a patientwith neurodegenerativedisease, medication sideeffects should always beconsidered as a causativefactor, particularly withcholinergic, antipsychotic,and sedative hypnoticmedications.
h Sundowning is commonin patients withneurodegenerativediseases; treatment is bestfocused onnonpharmacologicmeasures, such asimproved sleep hygieneand a consistent daytimeschedule, that includelight exposure andregular physical activity.
159Continuum (Minneap Minn) 2013;19(1):148–169 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

obstruction, restrictive lung disease (ie,chest wall rigidity and postural abnor-malities), and autonomic dysfunction.However, patients with PD tend to havelower body weight, which reduces OSAoccurrence. SDB may also be worsenedby antianxiolytic and pain medicationsprescribed for these patients. In mild to
moderate AD, treatment of OSA withCPAP improves nocturnal sleep qual-ity and excessive daytime sleepiness.However, compliance with CPAP is achallenge in this population. Donepezilhas been shown to improve OSA in AD,likely by stimulating the neurochemicalregulation of breathing during sleep.64
TABLE 8-7 Prevalence Estimates of Sleep Disorders in Neurodegenerative Disorders
DisorderSleep-DisorderedBreathing Hypersomnia
REM SleepBehavior Disorder
Restless LegsSyndrome
Parkinson disease Obstructive sleep apnea(OSA): 27Y52%(apnea-hypopnea index[AHI] 95 events/h)
20Y50%(sleep attacks1Y20%)
25Y50% Up to 52%
21Y34% (AHI 915 events/h)
4Y15% (AHI 930 events/h)
Multiple systematrophy
OSA: 15Y37% 28Y50% 69Y90% 28%
Stridor: 30Y42%
Central sleep apnea(CSA): present
Cheyne-Stokesrespiration: present
Dementia withLewy bodies
Not characterized Present 950% No knownassociation
Alzheimer disease OSA: 70Y80% (AHI 95events/h)
Up to 69% Case reports supportthis association
No knownassociation
Up to 53% (AHI 910 events/h)
38Y48% (AHI 920 events/h)
Spinocerebellarataxia (SCA)
Stridor (SCA types 1and 3): present
SCA type 3:45%
SCA type 2: 80% SCA type 3:30Y55%
OSA (SCA type 3):20Y25%
SCA type 3: 46% SCA types 1and 6: 23%
SCA type 2:18%
ALS Sleep-disorderedbreathing: 17Y76%
23% No knownassociation
19Y25%
Hypoventilation(most common)
CSA
OSA
REM = rapid eye movement.
160 www.aan.com/continuum February 2013
Comorbid Neurologic Disorders
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Central sleep apnea and Cheyne-Stokes breathing pattern can be observedin neurodegenerative diseases and arerelated to degeneration of the ventralarcuate nucleus and the pre-Botzingercomplex of the medulla (neural areasresponsible for respiratory chemosensi-tivity and rhythmogenesis).65 Stridor inpatients with multiple system atrophy orcertain spinal cerebellar ataxias andnocturnal hypoventilation in ALS areassociated with increased mortality.66
Excessive daytime sleepiness is fre-quent in patients with neurodegenerativedisorders. The degree of excessive day-time sleepiness correlates with theseverity of AD.67 Sleep attacks can occurin patients with PD and dementia withLewy bodies.68 Dopamine agonists, usedto treat symptoms such as tremor in PD,may also induce sudden sleep attacks.69
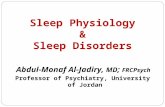
RBD (Supplemental Digital Content8-1, links.lww.com/CONT/A19) is asso-ciated with disruption of the normalparalysis-inducing mechanisms of REMsleep and may herald the onset of PDor other synucleinopathies by 20 yearsor more (Figure 8-2).70 Dream-enactingbehaviors can lead to injury to the pa-tient or bed partner and are typicallytreated with clonazepam or melatonin(Case 8-3). In PD, an increased fre-quency of restless legs syndrome andperiodic limb movement disorder maybe present, especially in patients nottreated with levodopa.71
NEUROMUSCULAR DISEASEAND SLEEPIn general, sleep disorders from neuro-muscular diseases occur because ofsleep-related ventilatory difficulties (andrespiratory failure), particularly in laterstages of the disease. Respiratory com-promisemay be related to diaphragmaticweakness, restrictive lung disease fromintercostal muscle weakness, kyphosco-liosis, or pulmonary microatelectasisfrom chronic hypoventilation. Contribu-
ting factors specific to SDB in myopa-thies include weakness of oropharyngealmuscles, tonsillar hypertrophy, obesity,and craniofacial dysmorphias. Breathingalterations become particularly evidentduring REM sleep when respirationbecomes diaphragm dependent. Centralapneas due to alterations in central re-spiratory drive may be present. Frequentnocturnal awakenings, daytime sleepi-ness and fatigue, morning headaches,and difficulty concentrating should cuethe practitioner to perform an over-night polysomnogram and check forlaboratory evidence of hypoxia andhypercapnia. Diurnal hypercapnia isindicated by a PaCO2 greater than 45mm Hg. Nocturnal hypoventilation isdefined as a PaCO2 greater than 55 mmHg for 10 minutes or more or a 10 mmHg or greater increase in PaCO2 duringsleep (in comparison to an awake su-pine value) to a value exceeding 50 mmHg for 10 minutes or more. Nocturnalhypoxia can be indicated by a low meansaturation, high desaturation index, and
KEY POINTS
h REM sleep behaviordisorder canherald preclinicalsynucleinopathies, andas such patients withREM sleep behaviordisorder should befollowed for signs andsymptoms of thesediseases over time.
h Indicators ofsleep-disorderedbreathing in patientswith neuromusculardisorders includedisrupted nocturnalsleep, daytime sleepinessand fatigue, morningheadache, and troubleconcentrating.
FIGURE 8-2 Survival curve of patients with idiopathic REMsleep behavior disorder. At 5 years’ survivaltime, 17% of patients went on to develop a
neurodegenerative disorder, and at 10 years’ survival time,40% of patients developed a neurodegenerative disorder.
Modified from Postuma RB, et al, Neurology.68 B 2009, with permissionfrom American Academy of Neurology. www.neurology.org/content/72/15/1296.abstract.
161Continuum (Minneap Minn) 2013;19(1):148–169 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

Case 8-3A 68-year-old, right-handed man presented with symptoms of loud snoring and nocturnal awakeningsrelated to nocturia and dreams in which he is fighting off an animal such as a lion or an ape. He wouldawaken from these dreams swinging his arms and yelling and in the past had struck his wife in bed.He found these behaviors embarrassing since they had occurred on long plane flights and tour busrides. His medical history included lumbar stenosis, prostate carcinoma status-post resection, anddiverticulosis. He took a baby aspirin, multivitamin, and calcium daily. He had no family history ofneurodegenerative disease, but two brothers also had undiagnosed dream-enacting behaviors.
His vital signs were within normal range, he was not orthostatic, body mass index was 24 kg/m2, andgeneral examination was nonrevealing. His MiniYMental State Examination score was 29/30. No signsof dysarthria, hypophonia, or ataxic speech were present, and the remainder of the neurologic
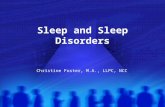
FIGURE 8-3 Thirty-second polysomnogram fragment showing increased chin tone in REM sleep and limb movements.Channels are as follows: electrooculogram (left: LOC-A2, right: ROC-A1); chin EMG (Chin1-Chin2); EEG (leftcentral [C3-A2], right central [C4-A1], left occipital [O1-A2], right occipital [O2-A1]), two ECG channels; limb
EMG (LAT1-LAT2); snore channel; nasal-oral airflow (N/O); respiratory effort (thoracic [THOR], abdominal [ABD]); andoxygen saturation (SpO2). Tonic EMG activity is consistent with REM sleep behavior disorder when present in more than50% of the total 30-second epoch duration with an amplitude of at least twice the background EMG muscle tone or morethan 10 6V. Phasic EMG activity includes any burst of activity lasting between 0.1 and 5.0 seconds with an amplitudeexceeding twice the background EMG activity irrespective of its morphology. The green arrow points to increased muscletone in the chin EMG lead while the blue arrow points to increased muscle tone in the limb EMG lead.
Figure courtesy of Alon Y. Avidan, MD, MPH, FAASM.
Continued on page 163
162 www.aan.com/continuum February 2013
Comorbid Neurologic Disorders
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

high hypoxemic burden such as anoxygen saturation of 88% or less for 5consecutive minutes. Other indicatorsof SDB in neuromuscular disease in-clude a maximal inspiratory pressure ofless than 60-cm water and a forced vitalcapacity of less than 50% predicted.72
Daytime predictors of sleep hypoventi-lation in Duchenne muscular dystro-phy are a forced expiratory volume ofless than 40% and a base excess greaterthan 4 mmol per liter.73
Noninvasive positive-pressure ventila-tion (NPPV) is the most common initialtreatment for SDB in neuromusculardisorders and improves survival andquality of life in patients with ALS.74 Thismay involve bilevel positive airway pres-sure with expiratory pressure set to pre-vent airway obstruction and inspiratorypressure set for ventilation purposes.Ventilation is often a greater concernthan airway obstruction and may nec-essitate pressure-support windows aslarge as 10-cm water or more. In manycases, the presence of central apneasnecessitates a back-up rate to deliver abreath if the patient fails to trigger aninspiratory effort. Another NPPV option
is average volume-assured pressure sup-port, which automatically adjusts pres-sure support to maintain a target tidalvolume. Regardless of NPPV type or set-tings, supplemental oxygen may also berequired and tracheostomy becomes aconsideration in advanced disease.
Myotonic dystrophy type 1 (DM1) isthe most common adult-onset form ofmuscular dystrophy, and hypersomniais a key clinical feature of the disease.Subjective and objective sleepiness (as-sessed by the Epworth Sleepiness Scaleand multiple sleep latency test, respec-tively) is present in 70% of patients withDM1.75 Excessive daytime sleepiness inDM1 is frequently persistent and unaf-fected by napping, unlike that of patientswith narcolepsy, who tend to feelrefreshed after naps. Patients with DM1frequently meet diagnostic criteria fornarcolepsy, and methylphenidate andmodafinil are effective treatments forsleepiness in these patients. Regardingmyasthenia gravis, 40% to 60% ofclinically stable patients have SDB.76
Insomnia is associated with neuro-muscular diseases and often induced bysteroids for treatment of disorders such
KEY POINT
h Objective tests indicatingnocturnal hypoventilationin neuromuscular diseaseinclude daytime PaCO2
greater than 45 mm Hg,nocturnal oximetryshowing oxygensaturation of 88% or lessfor 5 consecutiveminutes, nocturnalPaCO2 of greater than55 mm Hg for 10minutes or more or a 10mm Hg or greaterincrease in PaCO2 duringsleep (compared towake) to a valueexceeding 50 mm Hg for10 minutes or more,maximal inspiratorypressure of less than60-cm water, and forcedvital capacity of less than50% predicted.
examination results were normal. Overnight polysomnography showed minimal sleep-disorderedbreathing, oxygen desaturation nadir of 91%, and increased muscle tone during REM sleep (Figure 8-3).No epileptiform discharges were seen.
Clonazepam 0.5 mg nightly was prescribed, and the patient was ensured a safe sleepingenvironment. He tolerated the medication, and the dream-enacting behaviors ceased. During thenext 2 years, no signs of tremor, gait impairment, or dementia were apparent.
Comment. This case of REM sleep behavior disorder (RBD) highlights protean aspects of the disease.This disorder typically involves older men, can precede the onset of synucleinopathies such asdementia with Lewy bodies in some but not all patients, and may result in substantial injury topatients or their bed partners. Increased chin EMG tone in REM sleep is the polysomnographichallmark of the disease. Exposure to selective serotonin reuptake inhibitors or tricyclic antidepressantscan provoke the disorder. Treatment focuses on creating a safe sleeping environment (eg, removesharp furniture edges and mirrors, lock bedroom doors, close windows) and benzodiazepines, mostcommonly clonazepam. Melatonin and dopamine agonists have also been used with some success. Allpatients with RBD should undergo a thorough neurologic examination and be followed over time forevidence of parkinsonism. In the event of focal findings, neuroimaging is recommended since RBDcan also be precipitated by brainstem lesions of almost any cause.
Continued from page 162
163Continuum (Minneap Minn) 2013;19(1):148–169 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

as inflammatory myopathies. PLMS areincreased in DM1 compared to controlsand associated with sleep disturbance.77
Lastly, restless legs syndrome is increasedin ALS and associated with increasedsleep complaints.78
DEMYELINATING DISEASEAND SLEEPAs with stroke or tumor, lesion locationin multiple sclerosis (MS) is critical tothe presence or absence of sleepiness,insomnia, or specific sleep disorders.Hypothalamic lesions involving the tuber-omammillary nucleus or hypocretin/orexin production can cause sleepiness.Pontine lesions involving areas such asthe sublaterodorsal tegmental nucleuscan precipitate RBD. Lesions involvingthe ventrolateral preoptic nucleus canpredispose to insomnia. For these rea-sons, attention to lesion location onneuroimaging can prove insightful whenaddressing sleep concerns in MS.
Fatigue and sleepiness are commoncomplaints in MS and are frequentlyintertwined. In a cross-sectional surveyof 1063 people with MS, those with MShad more sleep disturbances (and day-time somnolence) compared to a groupof chronically ill patients and a group ofhealthy individuals.79 Conversely, multi-ple studies dispute sleepiness as an MSsymptom.80,81 Fatigue may be relatedto sleepiness, as sleep disruption cancause or worsen fatigue through CNSactivation and increased inflammation.When focusing on fatigued subsets ofMS patients, those with fatigue are sig-nificantly sleepier than nonfatiguedpatients with MS,82,83 although this isdisputed by other studies showingnormal Epworth Sleepiness Scale scoresand sleep latencies on the multiplesleep latency test between the twogroups.84,85 SDB is more frequent infatigued (27.0%) versus nonfatigued MSpatients (2.5%), and the presence of asleep disorder is associated with an
increased risk of fatigue in MS. Sleepi-ness and fatigue in MS are commonlytreated with modafinil, although its ef-fectiveness is uncertain.
Narcolepsy and RBD occur morefrequently in patients with MS. Casereports suggest an association betweenacute disseminated encephalomyelitisand neuromyelitis optica with hyper-somnia and secondary narcolepsy.Insomnia is common in MS, present inup to 40% of patients. Common MSsymptoms, such as pain, spasticity, blad-der dysfunction, depression, anxiety,and medications (ie, immunomodula-tors, such as interferon and corticoste-roids) all likely contribute to difficultyfalling and staying asleep. Restless legssyndrome may be seen in MS patientsand is associated with greater disabil-ity,86 although these symptoms may beconfused with other frequent MS com-plaints such as paresthesias, dysesthe-sias, pain, and spasticity. PLMS are alsohighly prevalent in MS.84 Intrathecalbaclofen, for treatment of spasticity,reduces PLMS but increases obstructiveand central respiratory events, especiallyin patients receiving bolus compared tocontinuous intrathecal administration.87
Generally speaking, poor sleep in MS isan independent predictor of quality oflife.88
CNS MALIGNANCIES AND SLEEPMalignancies disrupt sleep through bothdirect and indirect effects. Cerebral tu-mors, especially those located in thesellar or suprasellar regions (ie, cranio-pharyngioma, pilocytic astrocytoma, andpituitary adenoma) can induce sleepi-ness through direct neoplastic involve-ment or pressure exertion on thehypothalamus, with a correspondingreduction in hypocretin (orexin) as thelikely causative factor. Sellar or supra-sellar tumors may also cause endo-crine dysfunction, indirectly producingsleepiness and sleep disturbances by
KEY POINTS
h When treating patientswith neuromusculardisorders with bilevelpositive airway pressure,improving ventilation isoften more importantthan relieving airwayobstruction, and widepressure-support windowsmay be necessary.
h Multiple sclerosis lesionsin brain areassubserving sleep onset,alertness, and REMsleep paralysis canprecipitate insomnia,sleepiness, and REMsleep behavior disorder.
h Insomnia is common inmultiple sclerosis andlikely due to manydisease-related factors,such as pain, spasticity,bladder dysfunction,depression, anxiety, andmedication side effects.
h Sellar or suprasellarmalignancies canindirectly causesleep-disorderedbreathing byendocrinologicdysfunction causingobesity.
164 www.aan.com/continuum February 2013
Comorbid Neurologic Disorders
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

promoting obesity and subsequent OSA.Insomnia in these patients may resultfrom alterations in melatonin productionby the pineal gland. Brainstem gliomasand hemispheric tumors (ie, thosewith bilateral hemisphere invasion oredema causing increased intracranialpressure and/or cerebral herniation)have also demonstrated somnogeniccapabilities, with disruption of the re-ticular activating system as the likelycause. In addition, paraneoplastic dis-orders such as anti-Ma2 encephalitisare associated with sleepiness.89 Nu-merous case reports document secon-dary narcolepsy and sleepiness relatedto treatment of cerebral tumors withradiation and surgical instrumentationand/or resection. Radiation therapy hasbeen implicated in ‘‘somnolence syn-drome,’’ a poorly described hypersomniain children receiving cranial irradiationfor acute lymphocytic leukemia. Chemo-therapeutics and immunomodulatorsused to treat cerebral tumors mayinduce insomnia or somnolence. Meth-ylphenidate, amphetamines, and modafi-nil are effective in the treatment ofsleepiness in children with brain tumors.
SDB may be caused by tumors in-volving the brainstem leading to dys-function of the respiratory centers andnuclei involved in diaphragmatic andbulbar muscle control. RBD may pre-sent when a brainstem lesion disruptsthe normal paralysis-inducing mecha-nisms of REM sleep. Restless legs syn-drome has been described as the initialcomplaint in a patient with a foramenmagnum tumor,90 and PLMS have beenobserved in patients with thoracic spi-nal cord tumors.91
CONCLUSIONSSleep dysfunction and neurologic disor-ders are deeply intertwined, and theneurologist is well served to considerthe interaction of sleep with almostevery patient entering the clinic. SDB is
a risk factor for stroke and, as with allstroke risk factors, its investigationshould be considered in every TIA andstroke patient for secondary prevention.Whether diagnosing and treating SDB isa good stroke primary prevention strat-egy is yet to be definitively determined,but in the meantime it is probablyreasonable and safe to assume thattreating SDB will positively affect futurerisk of cerebrovascular disease. Sleepaffects all headache disorders, and twodisorders (hypnic and sleep apnea head-ache) are sleep specific and may occurupon awakening. Neurodegenerativediseases, MS, and CNS malignanciescan influence sleep quality, continuity,and sleepiness and precipitate SDB orRBD by involving nuclei and pathwaysinvolved in automatic control of respira-tion, dream-related paralysis, alertness,and circadian rhythmicity.
VIDEO LEGENDSupplemental Digital Content 8-1
REM sleep behavior disorder. Video montageof REM sleep behavior disorder demonstratingvigorous, aggressive, and violent behaviors duringREM sleep in an older adult male patient. Noteviolent and aggressive dream enactment correlat-ing with dream sequence, placing both the pa-tient and the bed partner at risk for injury.links.lww.com/CONT/A19
B 2013 Carlos Schenk, MD. Used with permission.
REFERENCES1. Shahar E, Whitney CW, Redline S, et al.
Sleep-disordered breathing andcardiovascular disease: cross-sectional resultsof the sleep heart health study. Am J RespirCrit Care Med 2001;163(1):19Y25.
2. Arzt M, Young T, Finn L, et al. Association ofsleep-disordered breathing and theoccurrence of stroke. Am J Respir Crit CareMed 2005;172(11):1447Y1451.
3. Munoz R, Duran-Cantolla J, Martinez-Vila E,et al. Severe sleep apnea and risk of ischemicstroke in the elderly. Stroke 2006;37(9):2317Y2321.
4. Redline S, Yenokyan G, Gottlieb DJ, et al.Obstructive sleep apnea-hypopnea and incidentstroke: the sleep heart health study. Am JRespir Crit Care Med 2010;182(2):269Y277.
KEY POINT
h Secondary narcolepsycan occur fromtreatment of CNSmalignancies withsurgical resection orradiation therapy in theperihypothalamic region.
165Continuum (Minneap Minn) 2013;19(1):148–169 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

5. Valham F, Mooe T, Rabben T, et al. Increasedrisk of stroke in patients with coronaryartery disease and sleep apnea: a 10-yearfollow-up. Circulation 2008;118(9):955Y960.
6. Yaggi HK, Concato J, Kernan WN, et al.Obstructive sleep apnea as a risk factor forstroke and death. N Engl J Med 2005;353(19):2034Y2041.
7. Chami HA, Resnick HE, Quan SF, Gottlieb DJ.Association of incident cardiovasculardisease with progression of sleep-disorderedbreathing. Circulation 2011;123(12):1280Y1286.
8. Munoz R, Duran-Cantolla J, Martinez-Vila E,et al. Central sleep apnea is associated withincreased risk of ischemic stroke in theelderly. Acta Neurol Scand 2012;126(3):183Y188.
9. Manfredini R, Boari B, Smolensky MH, et al.Circadian variation in stroke onset: identicaltemporal pattern in ischemic andhemorrhagic events. Chronobiol Int 2005;22(3):417Y453.
10. Casetta I, Granieri E, Fallica E, et al. Patientdemographic and clinical features andcircadian variation in onset of ischemicstroke. Arch Neurol 2002;59(1):48Y53.
11. Hsieh SW, Lai CL, Liu CK, et al. Obstructivesleep apnea linked to wake-up strokes.J Neurol 2012;259(7):1433Y1439.
12. Phillips RA, Sheinart KF, Godbold JH, et al.The association of blunted nocturnal bloodpressure dip and stroke in a multiethnicpopulation. Am J Hypertens 2000;13(12):1250Y1255.
13. Pringle E, Phillips C, Thijs L, et al. Systolicblood pressure variability as a risk factor forstroke and cardiovascular mortality in theelderly hypertensive population. J Hypertens2003;21(12):2251Y2257.
14. Dudenbostel T, Calhoun DA. Resistanthypertension, obstructive sleep apnoea andaldosterone. J Hum Hypertens 2012;26(5):281Y287.
15. Peppard PE, Young T, Palta M, Skatrud J.Prospective study of the associationbetween sleep-disordered breathing andhypertension. N Engl J Med 2000;342(19):1378Y1384.
16. Alajmi M, Mulgrew AT, Fox J, et al. Impactof continuous positive airway pressuretherapy on blood pressure in patients withobstructive sleep apnea hypopnea: ameta-analysis of randomized controlledtrials. Lung 2007;185(2):67Y72.
17. Bazzano LA, Khan Z, Reynolds K, He J. Effectof nocturnal nasal continuous positiveairway pressure on blood pressure in
obstructive sleep apnea. Hypertension 2007;50(2):417Y423.
18. Haentjens P, Van Meerhaeghe A,Moscariello A, et al. The impact ofcontinuous positive airway pressure onblood pressure in patients with obstructivesleep apnea syndrome: evidence from ameta-analysis of placebo-controlledrandomized trials. Arch Intern Med 2007;167(8):757Y764.
19. Mo L, Gai J, He QY. The effect of chronicintermittent hypoxia caused by obstructivesleep apnea hypopnea syndrome on bloodpressure [in Chinese]. Zhonghua Jie He HeHu Xi Za Zhi 2007;30(12):898Y903.
20. Kohli P, Balachandran JS, Malhotra A.Obstructive sleep apnea and the risk forcardiovascular disease. Curr Atheroscler Rep2011;13(2):138Y146.
21. Kanagala R, Murali NS, Friedman PA, et al.Obstructive sleep apnea and the recurrenceof atrial fibrillation. Circulation 2003;107(20):2589Y2594.
22. Lurie A. Endothelial dysfunction in adultswith obstructive sleep apnea. Adv Cardiol2011;46:139Y170.
23. Balfors EM, Franklin KA. Impairment ofcerebral perfusion during obstructive sleepapneas. Am J Respir Crit Care Med 1994;150(6 pt 1):1587Y1591.
24. Urbano F, Roux F, Schindler J, Mohsenin V.Impaired cerebral autoregulation inobstructive sleep apnea. J Appl Physiol2008;105(6):1852Y1857.
25. Oyama J, Yamamoto H, Maeda T, et al.Continuous positive airway pressure therapyimproves vascular dysfunction and decreasesoxidative stress in patients with the metabolicsyndrome and obstructive sleep apneasyndrome. Clin Cardiol 2012;35(4):231Y236.
26. Lau EM, Yee BJ, Grunstein RR, CelermajerDS. Patent foramen ovale and obstructivesleep apnea: a new association? Sleep MedRev 2010;14(6):391Y395.
27. Pinet C, Orehek J. CPAP suppression ofawake right-to-left shunting through patentforamen ovale in a patient with obstructivesleep apnoea. Thorax 2005;60(10):880Y881.
28. Ciccone MM, Scicchitano P, Mitacchione G,et al. Is there a correlation between osasduration/severity and carotid intima-mediathickness? Respir Med 2012;106(5):740Y746.
29. Hui DS, Shang Q, Ko FW, et al. A prospectivecohort study of the long-term effects ofCPAP on carotid artery intima-mediathickness in obstructive sleep apneasyndrome. Respir Res 2012;13:22.
166 www.aan.com/continuum February 2013
Comorbid Neurologic Disorders
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

30. Bulcun E, Ekici M, Ekici A. Disorders ofglucose metabolism and insulin resistance inpatients with obstructive sleep apnoeasyndrome. Int J Clin Pract 2012;66(1):91Y97.
31. Martinez-Garcia MA, Campos-Rodriguez F,Soler-Cataluna JJ, et al. Increased incidenceof nonfatal cardiovascular events in strokepatients with sleep apnoea: effect of CPAPtreatment. Eur Respir J 2012;39(4):906Y912.
32. Martinez-Garcia MA, Soler-Cataluna JJ,Ejarque-Martinez L, et al. Continuouspositive airway pressure treatment reducesmortality in patients with ischemic strokeand obstructive sleep apnea: a 5-yearfollow-up study. Am J Respir Crit Care Med2009;180(1):36Y41.
33. Ryan CM, Bayley M, Green R, et al. Influenceof continuous positive airway pressure onoutcomes of rehabilitation in stroke patientswith obstructive sleep apnea. Stroke 2011;42(4):1062Y1067.
34. Parra O, Arboix A, Bechich S, et al. Timecourse of sleep-related breathing disordersin first-ever stroke or transient ischemicattack. Am J Respir Crit Care Med 2000;161(2 pt 1):375Y380.
35. Bassetti C, Aldrich MS. Sleep apnea in acutecerebrovascular diseases: final report on128 patients. Sleep 1999;22(2):217Y223.
36. Magee CA, Kritharides L, Attia J, et al.Short and long sleep duration are associatedwith prevalent cardiovascular disease inAustralian adults. J Sleep Res 2012;21(4):441Y447.
37. Watson NF. Stroke and sleep specialists: anopportunity to intervene? J Clin Sleep Med2010;6(2):138Y139.
38. Trotti LM, Esper CD, Feustel PJ, et al.Excessive daytime sleepiness in cervicaldystonia. Parkinsonism Relat Disord 2009;15(10):784Y786.
39. Kuyper DJ, Parra V, Aerts S, et al. Nonmotormanifestations of dystonia: a systematicreview. Mov Disord 2011;26(7):1206Y1217.
40. Taylor N, Bramble D. Sleep disturbance andHuntingdon’s disease. Br J Psychiatry 1997;171:393.
41. Goodman AO, Barker RA. How vital is sleepin Huntington’s disease? J Neurol 2010;257(6):882Y897.
42. Arnulf I, Nielsen J, Lohmann E, et al. Rapideye movement sleep disturbances inHuntington disease. Arch Neurol 2008;65(4):482Y488.
43. Chandran V, Pal PK, Reddy JY, et al.Non-motor features in essential tremor.Acta Neurol Scand 2012;125(5):332Y337.
44. Kostanecka-Endress T, Banaschewski T,Kinkelbur J, et al. Disturbed sleep inchildren with Tourette syndrome: apolysomnographic study. J Psychosom Res2003;55(1):23Y29.
45. Kirov R, Kinkelbur J, Banaschewski T,Rothenberger A. Sleep patterns in childrenwith attention deficit hyperactivity disorder,tic disorder, and comorbidity. J ChildPsychol Psychiatry 2007;48(6):561Y570.
46. Rains JC, Poceta JS. Headache and sleepdisorders: review and clinical implicationsfor headache management. Headache 2006;46(9):1344Y1363.
47. Rains JC, Poceta JS. Sleep and headachedisorders: clinical recommendations forheadache management. Headache 2006;46(suppl 3):S147YS148.
48. Spierings EL, van Hoof MJ. Fatigue and sleepin chronic headache sufferers: an age- andsex-controlled questionnaire study.Headache 1997;37(9):549Y552.
49. Ohayon MM. Prevalence and risk factors ofmorning headaches in the general population.Arch Intern Med 2004;164(1):97Y102.
50. Kelman L, Rains JC. Headache and sleep:examination of sleep patterns andcomplaints in a large clinical sample ofmigraineurs. Headache 2005;45(7):904Y910.
51. Nobre ME, Leal AJ, Filho PM. Investigationinto sleep disturbance of patients sufferingfrom cluster headache. Cephalalgia 2005;25(7):488Y492.
52. Evers S. Sleep and headache: the biologicalbasis. Headache 2010;50(7):1246Y1251.
53. Buechler RD. Rodriguez AJ, Lahr BD, So EL.Ictal scalp EEG recording during sleep andwakefulness: diagnostic implications forseizure localization and lateralization.Epilepsia 2008;49(2):340Y342.
54. Sinha S, Brady M, Scott CA, Walker MC. Doseizures in patients with refractory epilepsyvary between wakefulness and sleep?J Neurol Neurosurg Psychiatry 2006;77(9):1076Y1078.
55. Derry CP. The sleep manifestations of frontallobe epilepsy. Curr Neurol Neurosci Rep2011;11(2):218Y226.
56. Eriksson SF. Epilepsy and sleep. Curr OpinNeurol 2011;24(2):171Y176.
57. Sonka K, Juklickova M, Pretl M, et al.Seizures in sleep apnea patients: occurrenceand time distribution. Sb Lek 2000;101(3):229Y232.
58. Malow BA, Levy K, Maturen K, Bowes R.Obstructive sleep apnea is common in
167Continuum (Minneap Minn) 2013;19(1):148–169 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

medically refractory epilepsy patients.Neurology 2000;55(7):1002Y1007.
59. van Golde EG, Gutter T, de Weerd AW. Sleepdisturbances in people with epilepsy;prevalence, impact and treatment. SleepMed Rev 2011;15(6):357Y368.
60. Parhizgar F, Nugent K, Raj R. Obstructivesleep apnea and respiratory complicationsassociated with vagus nerve simulators.J Clin Sleep Med 2011;7(4):401Y407.
61. Beran RG, Holland GJ, Yan KY. The use ofCPAP in patients with refractory epilepsy.Seizure 1997;6(4):323Y325.
62. Segal E, Vendrame M, Gregas M, et al. Effectof treatment of obstructive sleep apnea onseizure outcomes in children with epilepsy.Pediatr Neurol 2012;46(6):359Y362.
63. Vitiello MV, Borson S. Sleep disturbancesin patients with Alzheimer’s disease:epidemiology, pathophysiology andtreatment. CNS Drugs 2001;15(10):777Y796.
64. Sukys-Claudino L, Moraes W, GuilleminaultC, et al. Beneficial effect of donepezil onobstructive sleep apnea: a double-blind,placebo-controlled clinical trial. Sleep Med2012;13(3):290Y296.
65. Benarroch EE, Schmeichel AM, Low PA,Parisi JE. Depletion of putative chemosensitiverespiratory neurons in the ventral medullarysurface in multiple system atrophy. Brain2007;130(pt 2):469Y475.
66. Gaig C, Iranzo A. Sleep-disordered breathingin neurodegenerative diseases. Curr NeurolNeurosci Rep 2012;12(2):205Y217.
67. Bonanni E,MaestriM, TognoniG, et al. Daytimesleepiness in mild and moderate Alzheimer’sdisease and its relationship with cognitiveimpairment. J Sleep Res 2005;14(3):311Y317.
68. Bhatt MH, Podder N, Chokroverty S. Sleepand neurodegenerative diseases. SeminNeurol 2005;25(1):39Y51.
69. Comella CL. Sleep disturbances inparkinson’s disease. Curr Neurol NeurosciRep 2003;3(2):173Y180.
70. Postuma RB, Gagnon JF, Vendette M, et al.Quantifying the risk of neurodegenerativedisease in idiopathic REM sleep behaviordisorder. Neurology 2009;72(15):1296Y1300.
71. Bliwise DL, Trotti LM, Yesavage JA, Rye DB.Periodic leg movements in sleep in elderlypatients with Parkinsonism and Alzheimer’sdisease. Eur J Neurol. 2012;19(6):918Y923.
72. Benditt JO. Initiating noninvasivemanagement of respiratory insufficiency inneuromuscular disease. Pediatrics 2009;123(suppl 4):S236YS238.
73. Hukins CA, Hillman DR. Daytime predictorsof sleep hypoventilation in Duchennemuscular dystrophy. Am J Respir Crit CareMed 2000;161(1):166Y170.
74. Bourke SC, Bullock RE, Williams TL, et al.Noninvasive ventilation in ALS: indicationsand effect on quality of life. Neurology2003;61(2):171Y177.
75. Laberge L, Begin P, Dauvilliers Y, et al. Apolysomnographic study of daytime sleepinessin myotonic dystrophy type 1. J NeurolNeurosurg Psychiatry 2009;80(6):642Y646.
76. Prudlo J, Koenig J, Ermert S, et al. Sleepdisordered breathing in medically stablepatients with myasthenia gravis. Eur JNeurol 2007;14(3):321Y326.
77. Romigi A, Izzi F, Pisani V, et al. Sleepdisorders in adult-onset myotonic dystrophytype 1: a controlled polysomnographicstudy. Eur J Neurol 2011;18(9):1139Y1145.
78. Lo Coco D, Piccoli F, La Bella V. Restless legssyndrome in patients with amyotrophiclateral sclerosis. Mov Disord 2010;25(15):2658Y2661.
79. Bamer AM, Johnson KL, Amtmann D,Kraft GH. Prevalence of sleep problems inindividuals with multiple sclerosis. Mult Scler2008;14(8):1127Y1130.
80. Rammohan KW, Rosenberg JH, Lynn DJ,et al. Efficacy and safety of modafinil(Provigil) for the treatment of fatigue inmultiple sclerosis: a two centre phase 2study. J Neurol Neurosurg Psychiatry 2002;72(2):179Y183.
81. Zifko UA, Rupp M, Schwarz S, et al.Modafinil in treatment of fatigue inmultiple sclerosis. Results of an open-labelstudy. J Neurol 2002;249(8):983Y987.
82. Heesen C, Nawrath L, Reich C, et al. Fatiguein multiple sclerosis: an example of cytokinemediated sickness behaviour? J NeurolNeurosurg Psychiatry 2006;77(1):34Y39.
83. Stanton BR, Barnes F, Silber E. Sleep andfatigue in multiple sclerosis. Mult Scler 2006;12(4):481Y486.
84. Kaynak H, Altintas A, Kaynak D, et al.Fatigue and sleep disturbance in multiplesclerosis. Eur J Neurol 2006;13(12):1333Y1339.
85. Vetrugno R, Stecchi S, Scandellari C, et al.SleepVwake and body core temperaturerhythms in multiple sclerosis with fatigue.Clin Neurophysiol 2007;118(1):228Y234.
86. Manconi M, Fabbrini M, Bonanni E, et al.High prevalence of restless legs syndrome inmultiple sclerosis. Eur J Neurol 2007;14(5):534Y539.
168 www.aan.com/continuum February 2013
Comorbid Neurologic Disorders
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

87. Bensmail D, Marquer A, Roche N, et al.Pilot study assessing the impact ofintrathecal baclofen administration modeon sleep-related respiratory parameters.Arch Phys Med Rehabil 2012;93(1):96Y99.
88. Merlino G, Fratticci L, Lenchig C, et al.Prevalence of ‘poor sleep’ among patientswith multiple sclerosis: an independentpredictor of mental and physical status.Sleep Med 2009;10(1):26Y34.
89. Dalmau J, Graus F, Villarejo A, et al. Clinicalanalysis of anti-Ma2-associated encephalitis.Brain 2004;127(pt 2):1831Y1844.
90. Glasauer FE, Egnatchick JE. Restless legssyndrome: an unusual cause for a perplexingsyndrome. Spinal Cord 1999;37(12):862Y865.
91. Lee MS, Choi YC, Lee SH, Lee SB.Sleep-related periodic leg movementsassociated with spinal cord lesions. MovDisord 1996;11(6):719Y722.
169Continuum (Minneap Minn) 2013;19(1):148–169 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.