Skeleton Excavation Manual Part 2

of 58
description
The second part of a manual about how to excavate human skeletons.
Transcript of Skeleton Excavation Manual Part 2
-
Poul
to
n Hu
man Remains Team
Skeleton Manual
Part 2 In the Laboratory
Editor: Ray Carpenter
Seventh Edition
First Revision - April 2013
-
Poulton Skeleton Manual -ii- 17-Aug-2013
Copyright Notice
Copyright 2013. This manual is the Copyright of Raymond Carpenter, Stephen Crane and Carla Burrell
who have asserted their right to be identified as the authors of the work in accordance with the Copyright,
Design and Patent Act 1988.
-
Poulton Skeleton Manual -iii- 17-Aug-2013
Table of Contents
List of Contributors 1
Editors Note 1
1 Introduction 3
1.1 Legal and Ethical Considerations 3
2 Post-Excavation Storage 5
2.1 Skeletons 5
2.2 Disarticulated Bones 5
2.3 Date Coding 6
3 Basic Post-Excavation Processes 7
3.1 Inventory Record 7
3.2 Basic Analysis 7
4 Advanced Post-Excavation Analysis 23
4.1 Overview 23
4.2 Other Ageing Methods 23
4.3 Other Sexual Dimorphism 23
4.4 Abnormalities 24
5 Disposal 27
6 References 29
7 Appendices 31
Appendix A Bones of the Adult Human Skeleton 33 Appendix B Bones of the Juvenile Human Skeleton 35 Appendix C Inventory: Worked example 37 Appendix D Post-Excavation Skeleton Analysis: Worked Example 41 Appendix E Descriptions of Pubic Symphyseal Surface Phases 45 Appendix F Descriptions of Auricular Surface Phases 47 Appendix G Stature Estimation: Worked example 49 Appendix H Notes on the Formulae used to Estimate Stature 51
-
Poulton Skeleton Manual -iv- 17-Aug-2013
-
Poulton Skeleton Manual 1 17-Aug-2013
List of Contributors Steve Crane, ex-Poulton Research Project
Carla Burrell, Liverpool John Moores University
Editors Note As Editor, I accept full responsibility for this document. Everything correct belongs to Steve and/or
Carla; the mistakes are all mine.
Ray Carpenter
March 2013
-
Poulton Skeleton Manual 2 17-Aug-2013
-
Poulton Skeleton Manual 3 17-Aug-2013
1 Introduction Ray Carpenter & Steve Crane
This Skeleton Manual is a stand-alone companion to the Poulton Research Project Site Manual [Emery,
2005]. It provides a detailed handbook for the treatment of human remains at all stages of the
archaeological process. It is in two parts: In the Field and In the Laboratory. This, Part 2, covers
storage, post-excavation analysis and disposal. It focuses on the types of human remains that have been
found to date at Poulton, together with the procedures developed by the Poulton Research Project to
handle these remains. It is not a general guide to the processing of human remains.
1.1 Legal and Ethical Considerations The overriding principle is that human remains must always be treated with respect, care and dignity.
It is a privilege to be allowed to excavate the remains of another human being. We adhere strictly to the
code of ethics published by the British Association for Biological Anthropology and Osteoarchaeology
[BABAO Code of Ethics, 2010].
There are important legal restrictions on the excavation and subsequent processing of human remains.
This is an area where the legal situation is currently under review by the Ministry of Justice (MoJ), and
may be subject to change in the near future [MoJ, 2011]. Excavation at Poulton is at present licensed by
the Ministry of Justice under the terms of the 1857 Burial Act.
-
Poulton Skeleton Manual 4 17-Aug-2013
-
Poulton Skeleton Manual 5 17-Aug-2013
2 Post-Excavation Storage Ray Carpenter & Steve Crane
Much of the material in this section comes from [Anderson, 1993] and [BABAO Code of Practice, 2010].
Excavated human bones need to be cleaned, both to prevent them from going mouldy and to aid post-
excavation analysis. Although some sources recommend dry brushing as a means of removing soil, this
is generally ineffective with the clay soil typical of Poulton: instead, the bones must be washed.
Bones must not be treated with any sort of chemicals. In certain circumstances, broken bones may be
glued together on a medium term basis using HMG acrylic adhesive B72. This adhesive may be safely
removed with solvents. For short term use (such as photography), 3M Scotch Magic Tape may be
used.
Note: Bones should only be glued for specific research purposes (for example, reconstruction of a fragmented
skull), and with the prior agreement of the Human Remains Team.
Gloves MUST be worn when cleaning a skeleton (and whenever else bones are handled), to
minimise contamination that might compromise future DNA analysis.
2.1 Skeletons On arrival in the bone cabin, the trays should be laid out on the drying racks. The drying process may
take several days depending on the conditions.
Once dry, the skeleton should be fully laid out and the full inventory and dental recording (Section 3.1)
completed. If time and resources permit, the full basic analysis (Section 3.2) should now be completed.
Otherwise, the dry bones should be placed back in the original bags (turned the right way out), or if the
bags are too dirty or damaged, in new bags. The site code, trench number, skeleton number, skeleton
context and description of bones should be written on the outside of the bag with an indelible marker.
All the bags for a single skeleton should be stored together. Normally one box per skeleton is sufficient
but additional boxes may be used if necessary. For example, if the skull is reasonably complete, or if
there are environmental samples, which should be kept with the skeleton at this stage. In this case, label
the boxes 1 of 2, 2 of 2, etc.
A standard label (below) should be stuck onto the end of the box(es) for each skeleton, giving the
skeleton number and context number, and its status in terms of post-excavation analysis. See Section 2.3
below regarding colour coding.
Finally, the box should be placed in the skeleton store, in the area allocated to skeletons awaiting post-
excavation analysis, with the label visible. Boxes should not be stacked too high, to avoid crushing.
Stacking directly on the floor should also be avoided as the boxes may become damp.
2.2 Disarticulated Bones Disarticulated bones are processed in basically the same way as articulated skeletons, but note the
following:
All the bones excavated at one time from a single context should be kept together. The Site Code and year of excavation (POU/CHF/yy), the description DISARTICULATED HUMAN BONE (or
DHB for short) and the context number should be identified on a label and/or by writing on the
bag. If the remains are unstratified, write U/S as the context number.
-
Poulton Skeleton Manual 6 17-Aug-2013
There may be several bags for each context, either because the bones were excavated at different times, or because of the sheer volume of material.
Disarticulated bone should be stored in separate boxes from articulated skeletons. It is quite acceptable to store disarticulated bone for different contexts as well as unstratified bone in a
single box, so as not to waste space. A standard label (below) should be stuck on the end of each
box. See Section 2.3 below regarding colour coding.
Finally, the boxes should be placed in the area allocated to disarticulated bones.
2.3 Date Coding From 2008 onwards, due to differing reburial requirements, the storage boxes for both articulated
skeletons and disarticulated bones are colour coded according to the year of excavation. The first style
was single colour stickers:
Red = 2008
Yellow = 2009
Green = 2010
Blue = 2011
From 2012 onwards, two coloured circles are printed on the labels. These colours represent the last two
digits of the year according the significant figure colours of the Electronic Colour Code [EN 60062:
2005], that is:
Brown & Red = 2012
Brown & Orange = 2013
Brown & Yellow = 2014
Brown & Green = 2015
-
Poulton Skeleton Manual 7 17-Aug-2013
3 Basic Post-Excavation Processes Ray Carpenter, Steve Crane & Carla Burrell
An inventory and a basic level of post-excavation analysis must be carried out on every excavated
skeleton.
Gloves MUST be worn when analysing a skeleton (and whenever else bones are handled), to
minimise contamination that might compromise future DNA analysis.
3.1 Inventory Record The inventory should be completed as soon as the skeleton can be safely handled after its arrival in the
bone cabin. On completion of the inventory, the skeleton may be put into its own box(es), clearly
labelled and placed in store pending further analysis.
There are a number of standards for inventories. The form used at Poulton (Appendix C) was created by
Carla Burrell and is derived from an inventory recording form for complete skeletons used in standards
[Buikstra, J. E., and Ubelaker, D. H., 1994] and the forensic data bank form [Burns, K. R., 2007]. It also
includes a dentition chart which should be completed. The data from this chart is used later in assessing
the age of the skeleton.
For the analysis of each skeleton, the inventory is the initial starting point. The skeleton is laid out in
the anatomical position. This view of the remains provides an accessible observation of the whole
skeleton. Each bone whether complete or fragmented is recorded in sequence from the cranium to the
metatarsals. The form used at Poulton provides a selection of tables, sectioning the skeleton into 6 areas;
cranial and post-cranial bones, vertebral column, long bones, the extremities (hands and feet) and the
dentition. Each table contains a list of the typical bones present of a complete skeleton, the side whether
left, right or medial and finally, further comments such as the condition of the bone and noticeable
pathologies. There is also a review section at the end of the form to record any anomalies that may have
arisen. This is an important process of any analysis in the archaeological context and even in the
forensic context. Any pathology or trauma noticed here could be missed at a later point in the
examination process; in turn these forms become a reference point throughout the rest of the analysis.
3.2 Basic Analysis This is the estimation of the age at death, sex, stature of the skeleton. An example of a completed form
used to record the results of this analysis is shown in Appendix D.
3.2.1 Age at Death Estimation In order to estimate sex and stature, it is necessary to establish an arbitrary age of adulthood. At
Poulton, that age is 18; below that, skeletons are classified as subadults without further distinction. All
techniques for determining age at death rely on relating changes in the skeleton to the age of the
individual concerned. Even where these relationships can be determined with some degree of accuracy
for modern populations, there is no guarantee that they will be equally applicable to the population
under study. Furthermore, individuals within a population can show great variability. It may
sometimes prove impossible to estimate the age at all, though it is usually possible to differentiate
between adult and sub-adult.
3.2.1.1 Adult/Subadult Differentiation A brief examination of the skeleton should be done to establish the approximate age of the skeleton
before undertaking any detailed analysis. In particular, overall bone size (length and diameter), the
state of epiphyseal fusion and/or dental development will normally allow adult/subadult categorisation.
Specifically, the skeleton is adult if:
One or more third molars are (or have been) fully erupted
All the epiphyses (except perhaps the sternal end of the clavicle) are fused.
In the case of doubt, treat the skeleton as a subadult and do a full dental development and/or a fusion
analysis and reclassify the skeleton as appropriate.
-
Poulton Skeleton Manual 8 17-Aug-2013
3.2.1.2 Adults Many methods have been proposed for estimating adult age at death but there is not one that is fully
satisfactory. It is only possible to assign skeletons to fairly wide age bands, for example the groups
defined by [Powers, 2008]:
Description Age Range
Young adult 18 25 years
Early middle adult 26 35 years
Later middle adult 36 45 years
Mature adult 46 years
The three techniques used at Poulton are:
dental attrition,
pubic symphysis degeneration, and
auricular surface degeneration.
We use all three techniques where possible to increase the accuracy of the overall age determination.
However, in some cases the relevant parts of the skeleton may not be available or may be in poor
condition.
Cranial suture closure is another widely used technique [White & Folkens, 2005: 369], but this requires
relatively complete and undamaged skulls; these are rare at Poulton. Similarly, we do not use the
technique based on metamorphosis of the sternal end of the fourth rib, because of the difficulty in
identifying this rib in incomplete skeletons and the damage that this area often suffers.
Dental Attrition
The diagram below [Brothwell, 1981: 72] shows the pattern of molar wear in Neolithic to Medieval
British skulls, which covers most of those expected to be found at Poulton.
-
Poulton Skeleton Manual 9 17-Aug-2013
Notes
1. The correlation between age and dental wear is greatest for first and second molars, and much lower
for third molars [Mays, 2010: 72].
2 . It is possible for the third molar to be present on the mandible but not on the maxilla (or vice-versa) or
even more confusingly, to vary from side to side of the maxilla or mandible. In this situation, there
would be minimal wear on the third molar, but this would give little or no indication of age. This
should be borne in mind particularly when you are missing the mandible or maxilla.
Pubic Symphysis Degeneration
The changes in the surfaces of the pubic symphysis at the front of the pelvis are considered to be one of
the most reliable criteria for estimating adult age [Buikstra & Ubelaker, 1994: 21]. The surfaces
degenerate with age from a distinctive ridge and furrow pattern to a smoother surface. However, be
aware that these bones are often damaged in the supine burials typical of Poulton, and also that the
technique does require knowledge of the sex of the skeleton.
We use the Suchey-Brooks scoring system ([Brooks & Suchey, 1990] and [Buikstra & Ubelaker, 1994: 21-
24]), in conjunction with:
the diagrams below
the detailed descriptions in Appendix E, and
the full set of acrylic casts.
The latter are preferred; they are an easier to use, more reliable aid to assessing the phase. Each side
should be scored separately.
-
Poulton Skeleton Manual 10 17-Aug-2013
The phase is converted to an age range (years, with 95% certainty) using the following table:
Phase Female Male
1 15 24 15 23
2 19 40 19 34
3 21 53 21 46
4 26 70 23 57
5 25 83 27 66
6 42 - 87 34 - 86
Auricular Surface Degeneration
Like the pubic symphysis, the auricular surface, where the os coxae meet the sacrum, also degenerates
from an undulating to a smooth surface. This area of the skeleton tends to survive burial well, and the
technique can be applied even where the sex of the skeleton is not known.
We use the technique described by [Lovejoy et al., 1985] and [Buikstra & Ubelaker, 1994: 24-32], using the
diagrams below and the detailed descriptions in Appendix F. Each side should be scored separately. The
photographs in [Buikstra & Ubelaker, 1994: 26-32] may also be useful.
-
Poulton Skeleton Manual 11 17-Aug-2013
3.2.1.3 Children and Young Adults Age at death is most accurately determined for children and young adults, as age-related changes to the
skeleton are most distinct at this stage of development. The most accurate method is dental
development. The teeth are relatively less affected by environmental influences such as poor diet or
disease during growth [Roberts, 2009: 130]. For older children and young adults, the fusion of the
epiphyses is also commonly used [Mays, 2010: 56] and [Bass, 1995: 194].
The dentition chart (see section 3.1) should be used in conjunction with the chart below, taken from
[Buikstra & Ubelaker, 1994: 51], to determine age based on overall development of the teeth:
-
Poulton Skeleton Manual 12 17-Aug-2013
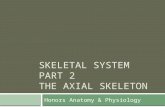
Epiphyseal Fusion
The diagram below [Mays, 2010: 58] with the addition of the ischiopubic ramus (o) from [Bass, 1995: 194]
shows the ages of epiphyseal fusion. Use the recording form (Appendix D) to record absence or presence
of fusion for each available epiphysis and then use the diagram to determine a bounding age for each
one. For example:
If the femur head (p) is fused in a male skeleton, then record age as 14.
If the radius distal epiphysis (f) is unfused in a female skeleton, then record age as 20.
In cases where it is not possible to determine the sex, check the figures for both males and females and
use the least restrictive condition. For example:
If the femur head is fused, it implies 14 (male) or 13 (female). Record age as 13.
If the radius distal epiphysis is unfused, it implies 23 (male) or 20 (female). Record age as 23.
-
Poulton Skeleton Manual 13 17-Aug-2013
Finally, use the data for all available epiphyses to determine an overall age range. A Visual Basic
program is available which performs all these calculations.
Note: Newborn infants do not have any epiphyses. However, the absence of epiphyses should not be used as a
guide to age determination, as these small and less-mineralised bones often do not survive anyway or
are lost during excavation.
-
Poulton Skeleton Manual 14 17-Aug-2013
Key Description
a Clavicle: sternal
b Humerus: head
c Humerus: distal
d Humerus: medial epicondyle
e Radius: proximal
f Radius: distal
g Ulna: proximal
h Ulna: distal
i Metacarpals: proximal
j Metacarpals: distal
k Phalanges: first and second
l Phalanges: third
m Pelvis: iliac crest
n Pelvis: triradiate
o Pelvis: ischiopubic ramus
p Femur: head
q Femur: greater trochanter
r Femur: distal
s Tibia: proximal
t Tibia: distal
u Fibula: proximal
v Fibula: distal
w Tarsal
x Metatarsals
y Phalanges
Diaphyseal and Epiphyseal Length
For subadults, there is obviously a relationship between age and height, and thus between age and the
length of the long bones. This technique is particularly useful where insufficient material is available to
assess age based on dental development and/or epiphyseal fusion. However, it does tend to produce a
lower estimate of age than these other methods (at least for the Poulton skeletons). This matches the
results found at Wharram Percy [Mays, 2010: 134-137], where medieval children were found to be
significantly shorter than modern children of the same age, lagging in growth by about 1-2 years.
The table below (taken from [Schaefer, Black & Scheuer, 2009: 267; 286; 302; 174; 191; 207] and by taking
the mean of the male and female measurements) can be used to estimate the age of subadults based on
the length of the long bones. For bones where the epiphyses have not yet fused, this is the diaphyseal
length (Di in the table below), that is, the length of the diaphysis or shaft of the bone. For bones where
the epiphyses have fused, this is the epiphyseal length (Epi in the table below). The bones should be
measured to the nearest mm using an osteometric board, and the lengths and derived ages recorded on
the form (Appendix D) under the Height Determination section.
-
Poulton Skeleton Manual 15 17-Aug-2013
Age (Yrs) Femur Tibia Fibula Humerus Radius Ulna
Di Epi Di Epi Di Epi Di Epi Di Epi Di Epi
1 13.6 10.9 10.6 10.5 8.1 9.1
2 17.2 13.9 13.7 12.9 9.7 10.8
3 19.9 16.2 16.1 14.6 11.0 12.2
4 22.4 18.2 18.1 16.2 12.1 13.4
5 24.7 20.1 20.0 17.7 13.2 14.6
6 26.9 21.8 21.7 19.0 14.2 15.6
7 29.0 23.5 23.3 20.3 15.1 16.6
8 31.1 26.8 25.0 21.7 16.1 17.6
9 33.0 26.7 26.5 22.8 16.9 18.5
10 34.9 38.4 28.5 32.1 28.0 30.9 24.0 25.7 17.9 19.1 19.5 20.3
11 36.7 40.4 30.0 33.9 29.5 32.5 25.2 27.0 18.7 20.1 20.5 21.4
12 38.7 42.7 31.7 35.9 31.1 34.4 26.4 28.5 19.7 21.3 21.5 22.7
13 44.7 37.6 35.9 29.9 22.4 23.9
14 46.5 39.1 37.4 31.3 23.4 25.0
15 47.7 39.9 38.3 32.2 24.2 25.8
16 48.5 40.5 38.9 32.9 24.6 26.4
17 48.6 40.4 38.9 33.1 24.8 26.5
Note: All bone lengths in cm.
For other methods of ageing children, see Section 4.
3.2.1.4 Infants and Foetuses Diaphyseal bone length is a good indicator of age in infants and foetuses. Bone growth is less affected by
external factors (for example, malnutrition) than after birth, and the skeleton grows rapidly during this
stage. Age can be estimated from long-bone length to an accuracy of approximately 2 weeks. The data in
the table below is from [Schaefer, Black & Scheuer, 2009: 264; 284; 300; 171; 188; 204]. For foetuses younger
than 20 weeks, see Section 4.
The bones should be measured using an osteometric board or sliding callipers and the lengths recorded
on the form (Appendix D) under the Height Determination section.
For other methods of ageing infants, see Section 4.
Foetal Age (weeks) Femur Tibia Fibula Humerus Radius Ulna
20 3.26 2.85 2.78 3.18 2.62 2.94
22 3.57 3.26 3.11 3.45 2.889 3.16
24 4.03 3.58 3.43 3.76 3.16 3.51
26 4.19 3.79 3.65 3.99 3.34 3.71
28 4.70 4.20 4.00 4.42 3.56 4.02
30 4.87 4.39 4.28 4.58 3.81 4.28
32 5.55 4.82 4.68 5.04 4.08 4.67
34 5.98 5.27 5.05 5.31 4.33 4.91
36 6.25 5.48 5.16 5.55 4.57 5.10
38 6.89 5.99 5.76 6.13 4.88 5.59
40 7.43 6.51 6.23 6.49 5.18 5.93
Note: All bone lengths in cm.
-
Poulton Skeleton Manual 16 17-Aug-2013
3.2.2 Sex Estimation Within any human population, adult male and female skeletons differ in general size and shape and this
is the basis for determining their sex. There are currently no generally agreed standards for
determining sex in juveniles (apart from DNA analysis which we are unlikely to use at Poulton).
This can lead to problems with adolescent skeletons [Buikstra & Ubelaker, 1994]:
Pelvis Immature pelvises tend to follow the male pattern. Hence female features are a reasonable indicator of sex, but male features are ambiguous, since they may represent either a
male or an immature female.
Skull Conversely, immature skulls tend to follow the female pattern. Hence male features are a reasonable indicator of sex, but female features are ambiguous since they may represent
either a female or an immature male
The estimation of sex should always be done after that of age (see Section 3.2.1) and when the skeleton is
believed to be an adult. Occasionally, skeletons classified as subadult display sufficient sexual
dimorphism to estimate the sex. In that case, do the sex estimation and record the results.
The two primary bones for determining sex are the pelvis and skull. The accuracy which can be
achieved has been estimated as follows [Dunn, 2002]:
Skull alone 80%
Pelvis alone 95%
Both skull and pelvis 98%
Many different attributes of the pelvis and skull have been proposed as a means of sex estimation. A
number of the most commonly used have been taken from [Brothwell, 1981: 60], [Buikstra & Ubelaker,
1994: 17-20], [Sutherland and Suchey, 1991: 502] and [Mays, 2010: 41]. As many as possible of these
attributes should be used for each skeleton; this increases the accuracy of sex determination. Sometimes
the skull or pelvis may not be available or may be in poor condition, that it is not possible to determine
the sex. In this case, record the sex as indeterminate. Equally, sometimes the indicators may be
contradictory. If the pelvis and skull are self-consistent but contradictory, score the sex according to the
pelvis. If the pelvis is not self-consistent, review the balance of stronger and weaker indicators and
consider recording the sex as Ambiguous.
On the recording form (Appendix D), each attribute is scored using a range of 1 (most female) to 5 (most
male), using as a guide the diagrams given below.
Where diagrams are only given for values of 1 and 5, interpolate for the intermediate values.
Attributes more extreme than 1 and 5 should be scored as 1 and 5 respectively.
If it is not possible to assess the attribute (for example, because of damage to the bone), then assign a score of 0.
Finally, make an overall assessment based on all the available data and taking into account the varying
reliability of the different indicators (That is, dont simply average the scores!)
3.2.2.1 Pelvis The Grea ter Scia tic No tch tends to be broad in females and narrow in males. Hold the os coxae
(innominate) about 15cm above the figure below [Buikstra and Ubelaker, 1994: 18] and align it as closely
as possible with the diagram (which shows the left side).
As a rule of thumb, place your thumb in the notch. If the notch is filled or only limited side-to-side
movement is possible, it is male. If considerable side-to-side movement is possible, it is female.
-
Poulton Skeleton Manual 17 17-Aug-2013
The Sub-P ubic Angle , the dotted line in figure [after Mays, 2010: 41] below, tends to be wider and more U-
shaped in females, narrower (generally less than 90) and more V-shaped in males.
1 5
The P rea uricula r Sulcus (location shown in the left figure [Buikstra and Ubelaker, 1994: 19] and the
details in the right figure by one of the authors, C. Burrell, below) is more consistently present in
females, although sometimes poorly developed, or present on one side only or not present at all.
1 5
-
Poulton Skeleton Manual 18 17-Aug-2013
There are three main attributes of the subpubic region, the area indicated in the figure below (the right
side is shown):
The Ventra l Arc is a slightly elevated ridge of bone across the ventral surface of the pubis, which tends
to be present in the female (diagram shows view from front):
1 5
The Subpubic Co nca vity (diagram shows left side viewed from rear):
1 5 1 5
-
Poulton Skeleton Manual 19 17-Aug-2013
The I schio pubic R a mus Rid ge (diagram shows left side viewed end-on):
1 5
3.2.2.2 Skull Males tend to have larger, more robust skulls than females, but the differences can be difficult to
interpret. Four key aspects have been chosen, based on the parts of the skull which tend to survive
reasonably intact at Poulton, and are illustrated below (originally from [Buikstra and Ubelaker, 1994]
but also in [White and Foulkens, 2005: 391]).
Nuchal Crest: Hold the cranium (or relevant part of it) at arms length a few inches above the
appropriate part of the figure, oriented as closely as possible to the diagram.
Mastoid Process: The most important variable to consider is the volume, not the length.
Supra-Orbital Margin: Hold the edge of the orbit between your fingers to determine its thickness. To
score 1, the edge should feel sharp, like the edge of a slightly dulled knife. To score 5, the edge should feel
thick and rounded like a pencil.
-
Poulton Skeleton Manual 20 17-Aug-2013
Supra-Orbital Ridge/Glabella: Hold the cranium (or relevant part of it) at arms length a few inches
above the appropriate part of the figure, oriented as closely as possible to the diagram.
3.2.3 Stature Estimation For adults, the most reliable method of estimating stature is from the long bones [Brickley & McKinley,
2004: 33]. Formulae can then be applied to calculate height from the length of these bones. This technique
can only be applied to mature individuals (that is, those with fused epiphyses) because the relative sizes
of the bones change during development. There is currently no generally agreed method for estimating
height in subadults.
Use the following procedure for an adult skeleton:
Back of bone placed face
downward on board,
rotate bone to find
maximum length.
Back of bone placed face
downward on board, long
axis of bone parallel to
long axis of board.
Head placed against fixed vertical, distal
end against movable upright. Bone moved
up & down and side to side until maximum
length obtained.
(Ulna and fibula are also measured in the
same way).
-
Poulton Skeleton Manual 21 17-Aug-2013
Measure the lengths of all available bones to the nearest mm using an osteometric board. The diagrams above [Brothwell, 1981] show how the bones should be positioned. Horizontal arrows
denote movement from side to side, curved arrows circular movement.
Broken bones can generally be re-assembled and measured, provided that the breaks are clean and all pieces are present. The pieces should be held together by hand and not glued or fixed in
any way other than by the minimal use of 3M Scotch Magic Tape [BABAO Code of Practice,
2010]. This may require two people, one to hold the bone and the other to operate the osteometric
board.
The measurements are recorded on the form (Appendix D).
Also record on the form the number of pieces of each bone and whether or not it is complete.
Calculate the stature using the appropriate set of equations, Male American White or Female American White, depending on sex (stature can only be determined if the sex is known).
Each formula should be calculated separately for left- and right-side bones and the results are normally averaged where both values are available. However, when clear pathology causes the
left and right values to differ significantly (>0.3cm), consider ignoring the affected side.
Examine and compare the various estimates and consider rejecting any outliers which appear too different from the rest (for example, might a bone from a different skeleton have been
measured?). Also carefully (re-)examine the bones for pathology that might explain the
difference. A common cause is a healed fracture.
The stature estimate based on the equation with the lowest standard error should be taken as the best estimate, rather than averaging the estimates from all the available equations.
A spreadsheet is available which performs all these calculations (see Appendix G).
Record the estimated stature and the standard error of the corresponding equation on the Post-Excavation recording form (Appendix D). The stature should be recorded to a precision of 0.1cm
and ", and the standard error to a precision of 0.1cm.
Detailed notes on the formulae used are in Appendix H.
-
Poulton Skeleton Manual 22 17-Aug-2013
-
Poulton Skeleton Manual 23 17-Aug-2013
4 Advanced Post-Excavation Analysis Ray Carpenter & Carla Burrell
4.1 Overview This section firstly describes methods and techniques that have been used at Poulton when those
described in Section 3 cannot be applied. Note that in all cases the results will be less reliable than those
obtained from the methods described in Section 3.
Secondly, it describes bone abnormalities and anomalies not covered at all in Section 3.
It is intended for people with experience in human ostoeology. There are no illustrations or diagrams
but there are references to standard text-books. The reader is expected to have (access to) a copy.
4.2 Other Ageing Methods Although dental development remains the best method for ageing subadults, the dentition is not always
available. The long bone measurements in Section 3 may be used (with the caveat that long bone age
and dental development age may not agree for Poulton specimens). The relevant chapters of [Schaefer,
Black & Scheuer, 2009] contain alternative sets of measurements and extended ranges of the
measurements quoted.
There are also other age indicators which been used successfully at Poulton when the dentition is not
available and the long bones are in a poor state.
In some cases, age estimation using the ribs may be possible [Iscan, Loth, & Wright, 1984] and [Iscan,
Loth, & Wright, 1985].
4.2.1 Other Fusions As well as the epiphyseal fusions identified in Section 3, there are other sites of fusion in the subadult
skeleton that we commonly use at Poulton to give an (albeit poorer) estimate of the age at death. There
are also many other fusion sites across the subadult skeleton that can be reviewed if required.
Vertebral Fusion
Most vertebrae are in three pieces at birth and fuse to a single entity by the age of 5. [Schaefer, Black &
Scheuer, 2009: 114] shows the age of fusion on the posterior arch and of the arch to the centrum.
The atlas and axis (C1 & C2) also follow a documented fusion process which can be used.
Sacral Fusion
[Schaefer, Black & Scheuer, 2009: 121] gives an outline of sacral fusion by age.
Occipital Fusion
The two pars lateralis and the pars basilaris often seem to survive intact at Poulton. The morphology
and age as these (and the pars supra-occipitalis) fuse to encircle the foramen magna is documented in
[Schaefer, Black & Scheuer, 2009: 15]
4.2.2 Bone Metrics As well as the long bones, metrics of other parts of the subadult skeleton which survive at Poulton have
been used to estimate the age at death.
Bone Reference
Pars basilaris [Schaefer, Black & Scheuer, 2009: 11; 13]
Pars lateralis [Schaefer, Black & Scheuer, 2009: 11]
Maximum iliac length & width [Schaefer, Black & Scheuer, 2009: 241-242]
4.3 Other Sexual Dimorphism Although not as reliable or accurate as those described in Section 3, there are other techniques for
estimating the sex of a skeleton. These may be helpful when the previously described methods cannot be
used.
-
Poulton Skeleton Manual 24 17-Aug-2013
Humeral and femoral head diameters
The femoral and/or humeral head is measured using a sliding calliper according to [Stewart, 1979]
Diagnostic categories are [Stewart, 1979]:
Femoral head: 47.5mm = Male
Humeral head: 47mm = Male
[Berrizbeitia, 1989] provides similar data for the radial head:
21mm = Female
22 - 23mm = Ambiguous
24mm = Male
Curvature of the sacrum
Sacral curvature is an additional observation. [Bass, 1995] indicates that the sacrum is generally more
curved in males than females. [Mishra, Singh, Agrawal & Gupta, 2003] have also reported more detailed
results based on the sacral curvature.
Dentition
A number of authors have proposed methods of sex estimation based on dentition. These include:
The mandibular canines [Mays, 2010]
General sexing of permanent dentition: [Ditch and Rose, 1972]
Immature skeletons [Rosing 1983]
Gonial Angle
The gonial angle has been proposed as sex determinant. However, to date the evidence is contradictory.
[Karoshah, Almadani, Ghaleb, Zaki & Fattah, 2010] suggest (using CT scans rather than the dry
mandible itself) that such a metric is viable; [Ayoub, Rizk, Yehya, Cassia, Chartouni, Atiyeh & Maizoub,
2009] suggest the contrary. Considerably more work needs to be performed using the Poulton
assemblage before this metric could become a reliable sex determinant.
4.4 Abnormalities Any abnormality in the skeleton must be identified as either taphonomy or pathology. Taphonomy
occurs to the bone after death (post-mortem); pathology occurs before death (ante-mortem). There are
some around death (peri-mortem) anomalies but they can be difficult to identify.
Taphonomic abnormalities such as root marks, rodent gnawing, deformation through soil pressure, and
soil erosion. These should be noted on the recording form (Appendix D), for possible further
investigation.
Pathological anomalies are more common and potentially more interesting. Definite abnormalities
should be recorded. The following information should be recorded for each abnormality:
Which bone/tooth is affected (including side)?
Which part of the bone/tooth (for example, proximal shaft)?
What is the nature of the change has additional bone been formed (most common), has bone been destroyed, or has the bone changed shape (least common)?
If bone has been formed, is it disorganised (indicating active disease at the time of death) or organised (indicating a healed lesion)?
If bone has been destroyed, is there any sign of healing, for example, rounding of the edges of the lesion?
What is the distribution pattern if more than one tooth/bone is affected?
Can the abnormality be measured and compared with a normal tooth/bone?
-
Poulton Skeleton Manual 25 17-Aug-2013
Photographs should be taken and noted on the recording form. A scale bar and label showing the site
code and skeleton number should be included in each photograph. Where appropriate, a normal bone or
tooth should be included for comparison.
4.4.1 Types of Pathological Abnormality The following list summarises the major types of pathological abnormality which should be recorded,
with the most common type first.
Type Description & Examples
Arthropathy (joint diseases) Osteoarthritis (formation of new bone on and around joints) is most
common. In severe cases, the cartilage is totally destroyed and bones
directly abrade each other; this can lead to joint surface polishing
(eburnation).
Dental Disease Wear on teeth can lead loss of teeth.
Gum (periodontal) disease is common and leads to abscesses and to
loosening or loss of teeth.
Trauma Broken bones note whether any healing has occurred (can help to
determine if damage is post-mortem).
Healed fractures.
Trephining or trepanning.
Injury from weapons (for example, an arrow head), tools or
implements.
Scoliosis
Osteophytes
Stress Indicators Horizontal striations on teeth (dental enamel hypoplasia).
Harris lines in long bones (visible only in radiographs).
Cribra orbitalia (pitting in the tops of the orbits, due to anaemia).
Rickets.
Osteoporosis (thinning of walls of long bones and loss of bone mass
difficult to identify).
Infection Generally leaves little evidence on the skeleton.
TB causes centres of vertebrae to collapse, leading to curvature of
spine.
Syphilis causes a gnawed effect on many bones, with rough edges.
Leprosy bone is lost on the palate, front of maxilla, etc., with
smooth edges.
Pagets disease bone assumes a distorted and enlarged character
Osteomyelitis pitting and irregularity of the bone surface and
possibly cavity formation within the bone interior.
Congenital/Developmental Cleft palate.
Hip dislocation due to shallow acetabulum.
Hydrocephalus (indicated by enlarged skull).
Sacralisation of 5th lumbar vertebra.
Supernumerary vertebrae
Unusual formation of teeth.
Cancerous Growths Erosion of normal bones and growth of other bone.
[Roberts and Manchester, 1995] and/or [Waldron, 2009] give a comprehensive description of the most
common diseases and traumas which affect bone.
In exceptional circumstances where the skeleton is of special interest or importance, it may be
necessary to call upon the services of an external expert to carry out a professional examination of the
remains.
It is essential that all basic post-excavation recording and analysis has been completed before any
destructive analysis is performed (such as 14C dating).
-
Poulton Skeleton Manual 26 17-Aug-2013
-
Poulton Skeleton Manual 27 17-Aug-2013
5 Disposal Ray Carpenter
Ultimately the remains will be re-interred in a duly authorised burial ground.
Previously we arranged for our human remains to be re-buried at Mount St. Bernard monastery, near
Loughborough in Leicestershire. This is particularly appropriate as this is a Cistercian monastery,
maintaining the link with the chapels past history. However, recently that route has become
unavailable to us. At the time of writing, the terms of our MoJ licence require all the human remains
excavated by the Project to be re-interred during 2015. We plan to apply for an extension of that licence
in due course. However, as precautionary measure, the Trustees have drawn up outline plans to re-inter
all the remains on specially dedicated land at Chapel House Farm, close to the original burial grounds.
The Trustees will decide the exact form and procedure of the re-burial closer to the event.
-
Poulton Skeleton Manual 28 17-Aug-2013
-
Poulton Skeleton Manual 29 17-Aug-2013
6 References Anderson, S., 1993 Digging Up People: Guidelines for Excavation and Processing of
Human Skeletal Remains.
http://www.spoilheap.co.uk/pdfs/digbone.pdf. Date accessed 26-
Jan-2013.
Ayoub, F., Rizk, A., Yehya, M.,
Cassia., A, Chartouni, S., Atiyeh, F.
& Maizoub, Z., 2009
Sexual dimorphism of mandibular angle in a Lebanese sample,
Journal of Forensic and Legal Medicine 16- 3:121-124.
BABAO Code of Ethics, 2010 2010 BABAO Code of Ethics. British Association for Biological
Anthropology and Osteoarchaeology and
http://www.babao.org.uk/index/ethics-and-standards. Date
accessed 26-Jan-2013.
BABAO Code of Practice, 2010 2010 BABAO Code of Practice. British Association for Biological
Anthropology and Osteoarchaeology and
http://www.babao.org.uk/index/ethics-and-standards. Date
accessed 26-Jan-2013
Bass, W.M., 1995 Human Osteology: A Laboratory and Field Manual (4th ed.). Special
Publication No. 2 of the Missouri Archaeological Society.
Bedford M.E. , Russell K.F. &
Lovejoy C.O., 1989
Poster presented at the 58th Annual Meeting of the American
Association of Physical Anthropologists, San Diego, CA. 7 April
1989
Berrizbeitia, E.L., 1989 Sex determination with the head of the radius. Journal of
Forensic Sciences. 34: 1207-1213.
Brickley, M. and McKinley, J.I.
(eds.), 2004
Guidelines to the Standards for Recording Human Remains. IFA
Paper No. 7, Reading.
Brooks, S. and Suchey, J.M., 1990 Skeletal Age Determination Based on the Os Pubis: A
Comparison of the Acsdi-Nemeskri and Suchey-Brooks
Methods. Human Evolution, 5: 227-238.
Brothwell, D., 1981 Digging Up Bones (3rd ed.). British Museum (Natural History),
London/Oxford University Press, Oxford.
Buikstra, J.E. and Ubelaker, D.H.
(eds.), 1994
Standards for Data Collection from Human Skeletal Remains.
Arkansas Archaeological Survey Research Series, No. 44.
Burns, K. R. (2007) Forensic Anthropology Training Manual (2nd Eds.) Pearson
Education, Pearson Practice Hall.
Ditch, L. E., and Rose, J. C. (1972). A multivariate dental sexing technique. American Journal of
Physical Anthropology, 37: 61-64
Dunn, G., 2002 Personal Communication
Emery, M., 2005 Poulton Research Project Site Manual (v0.2). Poulton.
EN 60062:2005 BS EN 60062 :2005: Marking codes for resistors and capacitors
http://shop.bsigroup.com/en/ProductDetail/?pid=0000000000301
61717 Date accessed 26-Jan-2013
Iscan, M. Y., Loth, S. R., and Wright,
R. K., 1984.
Age estimation from the ribs by phase analysis: White males.
Journal of Forensic Sciences 29: 1094-1104
Iscan, M. Y., Loth, S. R., and Wright,
R. K., 1985.
Age estimation from the ribs by phase analysis: White females.
Journal of Forensic Sciences 30: 853-863
Karoshah, M., Almadani, O., Ghaleb,
S., Zaki, M. & Fattah, Y., 2010
Sexual dimorphism of the mandible in a modern Egyptian
population, Journal of Forensic and Legal medicine 17- 4: 213-215.
Lovejoy, C.O., Meindl, R.S.,
Pryzbeck, T.R. and Mensforth, R.P.,
1985
Chronological Metamorphosis of the Auricular Surface of the
Ilium: A New Method for the Determination of Adult Skeletal
Age at Death. American Journal of Physical Anthropology, 68: 15-
28.
Mays, S., 2010. The Archaeology of Human Bones (2nd ed). Routledge, London.
-
Poulton Skeleton Manual 30 17-Aug-2013
McKinley, J.I. and Roberts, C., 1993 Excavation and Post-Excavation Treatment of Cremated and
Inhumed Human Remains. IFA Technical Paper No. 13,
Birmingham.
Mishra, S.R., Singh, P.J., Agrawal,
A.K., Gupta, R.N., 2003
Identification Of Sex Of Sacrum Of Agra Region. Journal of
Anatomical Society of India, 52(2): 132-136
MoJ, 2011 Statement on the exhumation of human remains for archaeological
purposes http://www.justice.gov.uk/downloads/burials-and-
coroners/statement-exhumation-human-remains-
archaeological.pdf. Date accessed 26-Jan-2013
Powers, N. (ed.), 2008 Human Osteology Method Statement. Museum of London and
http://www.museumoflondon.org.uk/NR/rdonlyres/2D513AFA-
EB45-43C2-AEAC-
30B256245FD6/0/MicrosoftWordOsteologyMethodStatementMar
ch2008.pdf. Date accessed 26-Jan-2013.
Roberts, C. and Manchester, K., 1995 The Archaeology of Disease (2nd ed.). Sutton Publishing, Stroud.
Roberts, C., 1998 Report on Skeletal Remains of One Individual from Poulton Chapel,
Cheshire. http://www.poultonproject.org/skel.shtml. Date
accessed 26-Jan-2013.
Roberts, C.A., 2009 Human Remains in Archaeology: A Handbook (Practical
Handbooks in Archaeology No. 19). Council for British
Archaeology, York.
Rosing, F. M. (1983). Sexing immature skeletons. Journal of Human Evolution, 12: 149-
155.
Schaefer, M., Black, S. & Scheuer, L.,
2009
Juvenile Osteology: A Laboratory and Field Manual. Academic
Press, London.
Stewart, T.D., 1979 Essentials of Forensic Anthropology. Springfield, IL: Charles C.
Thomas.
Stirland, A., 1999 Human Bones in Archaeology. Shire, Princes Risborough.
Sutherland, L.D. and Suchey, J.M.,
1991
Use of the Ventral Arc in Pubic Sex Determination. Journal of
Forensic Sciences, 36(2): 501-511.
Trotter, M. and Gleser, G.C., 1952 Estimation of Stature from Long Bones of American Whites and
Negroes. American Journal of Physical Anthropology 10: 463-514.
Trotter, M. and Gleser, G.C., 1958 A Re-Evaluation of estimation of stature based on measurements
of stature taken during life and of long bones after death.
American Journal of Physical Anthropology 16: 79-123.
Trotter, M. and Gleser, G.C., 1977 Corrigenda to estimation of stature from long limb bones of
American Whites and Negroes. American Journal Physical
Anthropology (1952). American Journal of Physical Anthropology
47: 355-6.
Trotter, M., 1970 Estimation of Stature from Intact Long Bones. In TD Stewart
Personal Identification in Mass Disasters. Washington:
Smithsonian Institution 71-83.
Waldron, T., 2009 Paleopathology. Cambridge University Press, Cambridge.
Western, A.G. and Kausmally, T.,
2005
A Field Guide to the Excavation of Inhumated Human Remains.
http://www.ossafreelance.co.uk/PastProjects/FieldGuidetotheE
xcavationofHumanInhumatedRemains.pdf. Date accessed 26-
Jan-2013.
White, T.O. and Folkens, P.A., 2005 The Human Bone Manual. Elsevier, London.
-
Poulton Skeleton Manual 31 17-Aug-2013
7 Appendices A Bones of the human skeleton
B Inventory: Worked example
C Post-excavation Skeleton Analysis: Worked example
D Descriptions of Pubic Symphyseal Surface phases
E Descriptions of Auricular Surface phases
F Stature Estimation: Worked example
G Notes on the Formulae used to Estimate Stature
Note: The pro-forma sheets are always being revised and those in current use may differ slightly from those
shown in these appendices.
-
Poulton Skeleton Manual 32 17-Aug-2013
-
Poulton Skeleton Manual 33 17-Aug-2013
Appendix A Bones of the Adult Human Skeleton
-
Poulton Skeleton Manual 34 17-Aug-2013
Bones of the Adult Skeleton
from [Mays, 2010: 2-3]
Skull: Including mandible & ossicles 28
Hyoid 1
Spinal column: Vertebrae Cervical 7
Thoracic 12
Lumbar 5
Sacrum 1
Coccyx 1
Thoracic cage: Rib 12 pairs 24
Sternum 1
Pectoral girdle: Clavicle 2
Scapula 2
Pelvic girdle: Pelvic bone 2
Limb bones: Arm bones: Humerus 2
Radius 2
Ulna 2
Wrist/hand: Carpal 16
Metacarpal 10
Phalanx 28
Leg bones: Femur 2
Patella 2
Tibia 2
Fibula 2
Ankle/foot: Tarsal 14
Metatarsal 10
Phalanx 28
Total 206
In addition, there are a variable number of small bones (sesamoids) embedded in the tendons of the
hands and feet.
Although this list shows the standard number of bones in an adult skeleton, extra bones are not
uncommon, for example, 13 rather than 12 thoracic vertebrae, or 6 rather than 5 lumbar vertebrae.
Detailed descriptions and photographs of all the bones can be found in [White & Folkens, 2005].
-
Poulton Skeleton Manual 35 17-Aug-2013
Appendix B Bones of the Juvenile Human Skeleton
-
Poulton Skeleton Manual 36 17-Aug-2013
Bones of the Juvenile Skeleton
from [Mays, 2010: 2-3] with additonal data from [Schaefer, Black & Scheuer, 2009]
Skull: Including mandible & ear ossicles 39-28
Hyoid 3-1
Spinal column: Vertebrae Cervical 22-7
Thoracic 36-12
Lumbar 15-5
Sacrum 15-5-1
Coccyx 1-1
Thoracic cage: Rib 12 pairs 24
Sternum 5-2-1
Pectoral girdle: Clavicle 4-2
Scapula 4-2
Pelvic girdle: Pelvic bone 10-2
Limb bones: Arm bones: Humerus 8-2
Radius 6-2
Ulna 6-2
Wrist/hand: Carpal 16-16
Metacarpal 20-10
Phalanx 56-28
Leg bones: Femur 8-2
Patella 2-2
Tibia 6-2
Fibula 6-2
Ankle/foot: Tarsal 16-14
Metatarsal 20-10
Phalanx 56-28
Total 404-206
This shows the total number of elements in the juvenile skeleton against that of an adult. For example,
the mandible can be in 1 or 2 pieces depending on the age of the juvenile.
-
Poulton Skeleton Manual 37 17-Aug-2013
Appendix C Inventory: Worked example
-
Poulton Skeleton Manual 38 17-Aug-2013
-
Poulton Skeleton Manual 39 17-Aug-2013
-
Poulton Skeleton Manual 40 17-Aug-2013
-
Poulton Skeleton Manual 41 17-Aug-2013
Appendix D Post-Excavation Skeleton Analysis: Worked Example
-
Poulton Skeleton Manual 42 17-Aug-2013
-
Poulton Skeleton Manual 43 17-Aug-2013
-
Poulton Skeleton Manual 44 17-Aug-2013
-
Poulton Skeleton Manual 45 17-Aug-2013
Appendix E Descriptions of Pubic Symphyseal Surface Phases The following descriptions are taken from [Brooks & Suchey, 1990], and should be read in conjunction
with the sub-section Pubic Symphysis Degeneration in Section 3.2.1.2
Phase 1: Symphyseal face has a billowing surface (ridges and furrows), which usually extends to
include the pubic tubercle. The horizontal ridges are well-marked, and ventral bevelling may be
commencing. Although ossific nodules may occur on the upper extremity, a key to the recognition of this
phase is the lack of delimitation of either extremity (upper or lower).
Phase 2: The symphyseal face may still show ridge development. The face has commencing delimitation of
lower and/or upper extremities occurring with or without ossific nodules. The ventral rampart may be in
beginning phases as an extension of the bony activity at either or both extremities.
Phase 3: Symphyseal face shows lower extremity and ventral rampart in process of completion. There can
be a continuation of fusing ossific nodules forming the upper extremity and along the ventral border.
Symphyseal face is smooth or can continue to show distinct ridges. Dorsal plateau is complete. Absence
of lipping of symphyseal dorsal margin; no bony ligamentous outgrowths.
Phase 4: Symphyseal face is generally fine grained although remnants of the old ridge and furrow
system may still remain. Usually the oval outline is complete at this stage, but a hiatus can occur in upper
ventral rim. Pubic tubercle is fully separated from the symphyseal face by definition of upper extremity.
The symphyseal face may have a distinct rim. Ventrally, bony ligamentous outgrowths may occur on
inferior portion of pubic bone adjacent to symphyseal face. If any lipping occurs, it will be slight and
located on the dorsal border.
Phase 5: Symphyseal face is completely rimmed with some slight depression of the face itself, relative to the rim.
Moderate lipping is usually found on the dorsal border with more prominent ligamentous outgrowths
on the ventral border. There is little or no rim erosion. Breakdown may occur on superior ventral
border.
Phase 6: Symphyseal face may show ongoing depression as rim erodes. Ventral ligamentous attachments
are marked. In many individuals the pubic tubercle appears as a separate bony knob. The face may be
pitted or porous, giving an appearance of disfigurement with the ongoing process of erratic ossification.
Crenulations may occur. The shape of the face is often irregular at this stage.
-
Poulton Skeleton Manual 46 17-Aug-2013
-
Poulton Skeleton Manual 47 17-Aug-2013
Appendix F Descriptions of Auricular Surface Phases The following descriptions are taken from [Buikstra & Ubelaker, 1994: 25], and should be read in
conjunction with the sub-section Auricular Surface Degeneration in Section 3.2.1.2
Phase 1. Transverse billowing and very fine granularity. Articular surface displays fine granular texture
and marked transverse organization. There is no porosity, retroauricular or apical activity. The surface
appears youthful because of broad and well-organized billows, which impart the definitive transverse
organization. Raised transverse billows are well-defined and cover most of the surface. Any subchondral
defects are smooth-edged and rounded. (Age, 20 -24)
Phase 2. Reduction of billowing but retention of youthful appearance. Changes from the previous phase are
not marked and are mostly reflected in slight to moderate loss of billowing, with replacement by striae.
There is no apical activity, porosity, or retroauricular activity. The surface still appears youthful owing
to marked transverse organization. Granulation is slightly more coarse. (Age, 25 -29 )
Phase 3. General loss of billowing, replacement by striae, and distinct coarsening of granularity. Both
demifaces are largely quiescent with some loss of transverse organization. Billowing is much reduced
and replaced by striae. The surface is more coarsely and recognizably granular than in the previous
phase, with no significant changes at apex. Small areas of microporosity may appear. Slight
retroauricular activity may occasionally be present. In general, coarse granulation supersedes and
replaces billowing. Note smoothing of surface by replacement of billows with fine striae, but distinct
retention of slight billowing. Loss of transverse organization and coarsening of granularity is evident.
(Age, 30 -34)
Phase 4. Uniform, coarse granularity. Both faces are coarsely and uniformly granulated, with marked
reduction of both billowing and striae, but striae may still be present. Transverse organization is
present but poorly defined. There is some activity in the retroauricular area, but this is usually slight.
Minimal changes are seen at the apex, microporosity is slight, and there is no macroporosity. (Age, 35 -
39)
Phase 5. Transition from coarse granularity to dense surface. No billowing is seen. Striae may be present
but are very vague. The face is still partially (coarsely) granular and there is a marked loss of transverse
organization. Partial densification of the surface with commensurate loss of granularity. Slight to
moderate activity in the retroauricular area. Occasional macroporosity is seen, but this is not typical.
Slight changes are usually present at the apex. Some increase in macroporosity, depending on degree of
densification. (Age, 40 -44)
Phase 6. Completion of densification with complete loss of granularity. Significant loss of granulation is
seen in most specimens, with replacement by dense bone. No billows or striae are present. Changes at
apex are slight to moderate but are almost always present. There is a distinct tendency for the surface to
become dense. No transverse organization is evident. Most or all of the microporosity is lost to
densification. There is increased irregularity of margins with moderate retroauricular activity and
little or no macroporosity. (Age, 45 -49)
Phase 7. Dense irregular surface of rugged topography and moderate to marked activity in periauricular
areas. This is a further elaboration of the previous morphology, in which marked surface irregularity
becomes the paramount feature. Topography, however, shows no transverse or other form of
organization. Moderate granulation is only occasionally retained. The inferior face generally is lipped at
the inferior terminus. Apical changes are almost invariable and may be marked. Increasing irregularity
of margins is seen. Macroporosity is present in some cases. Retroauricular activity is moderate to
marked in most cases. (Age, 50 -59)
Phase 8. Breakdown with marginal lipping, macroporosity, increased irregularity, and marked activity in
periauricular areas. The paramount feature is a nongranular, irregular surface, with distinct signs of
subchondral destruction. No transverse organization is seen and there is a distinct absence of any
youthful criteria. Macroporosity is present in about one-third of all cases. Apical activity is usually
marked but it is not requisite. Margins become dramatically irregular and lipped, with typical
degenerative joint change. Rctroauricular area becomes well defined with profuse osteophytes of low to
moderate relief. There is clear destruction of subchondral bone, absence of transverse organization, and
increased irregularity. (Age, 60+)
-
Poulton Skeleton Manual 48 17-Aug-2013
The following is from [Bedford, Russell. & Lovejoy, 1989]
Age Transverse 1 Organisation
Texture Retroauricular Activity
Apical Activity
Porosity
20
21
22 billowing fine
23 (20-24) granularity
24
25
26
27 decr. billowing slight coarse
28 incr. striae granularity
29 (25-29) (25-29)
30
31
32 decr. transv incr. coarse slight retro. micropor.
33 striae evident granularity possible possible
34 (30-34) (30-34) (30-34) (30-34)
35
36
37 last striae uniform coarse slight retro. minimal apical micropor.
38 (35-39) granularity activity change often slight
39 (35-3.9) (35-39) (35-39) (35-39)
40
41
42 vague transv. coarse granularity slight/moder. slight apical micropor.
43 (40-44) to dense (Islands) retro. activity changes occas.
macropor. 44 (40-44) (40-44) (40-44) (40-44)
45
46
47 no transv. decr. granularity moderate retro. apical change micropor. to
48 (45-49) incr. density activity irreg. margins densification
49 (45-49) (45-49) (45-49) possib.
macropor. 50 (45--49)
51
52
53
54
55 irregular
surface
dense mod/severe more apical possib.
macropor. 56 (50-60) possib. residual retro. activity change (50-60)
57 granularity (50-60) irreg. margins
58 (50-60) (50-60)
59
60 irregular
surface
dense, with severe retro. more apical macropor.
61 (60+) subchondral activity change (60+)
62 destruction (60+) margin lipping
63 (60+) osteophytes
64 (60+)
65
1 Terms used here are defined in Lovejoy et al. (1985) Chronological Metamorphosis of the Auricular Surface of the
Ilium: A New Method for the Determination of Adult Skeletal Age at Death. Amer. J. Phys. Anth. 68:15-28.
-
Poulton Skeleton Manual 49 17-Aug-2013
Appendix G Stature Estimation: Worked example
-
Poulton Skeleton Manual 50 17-Aug-2013
-
Poulton Skeleton Manual 51 17-Aug-2013
Appendix H Notes on the Formulae used to Estimate Stature The process used to calculate stature for the Poulton skeletons is as defined in [Brickley and McKinley,
2004: 33]. That document includes both the formulae (which are quoted in full, including the
corresponding standard error estimates) and their method of application, for example the use of the
single formula with the lowest standard error. We only use the sets of formulae for white males and
white females, and ignore those for black males and females as unapplicable for the medieval population
of Poulton.
Source Papers
The formulae are taken from four well-known sources: [Trotter & Gleser, 1952], [Trotter & Gleser, 1958],
[Trotter, 1970] and [Trotter & Gleser, 1977]. However, the way in which formulae have been selected from
the source papers is not straightforward, and is certainly not explained. This Appendix attempts to
clarify the origin of the sets of formulae we use.
The four source papers can be briefly summarised as follows, in chronological order:
[Trotter & Gleser, 1952] male formulae based on WW II data, female formulae based on the
Terry skeletal collection (at that time located at the Washington University Medical School, St.
Louis).
[Trotter & Gleser, 1958] male formulae revised, based on Korean War data.
[Trotter, 1970] just repeats some (but not all) of the formulae from the 1952 paper. It prefers
these to the formulae from the 1958 paper, on the grounds that the differences are of not
statistical significance and that the 1952 set have slightly smaller standard errors.
[Trotter & Gleser, 1977] corrections to some of the black female formulae. These are not
relevant for Poulton.
Males
The white male formulae recommended by [Brickley & McKinley, 2004:33] are listed in the table below:
Formula (in cm) Std Error Source
1.30 (XLF + LCT) + 63.29 2.99 1952
2.38 XLF + 61.41 3.27 1952
2.68 XLG + 71.78 3.29 1952
2.52 LCT + 78.62 3.37 1952
1.31 (XLF + XLG) + 63.05 3.62 1958
3.08 XLH + 70.45 4.05 1952
1.82 (XLH + XLR) + 67.97 4.31 1958
3.70 XLU + 74.05 4.32 1952
3.78 XLR + 79.01 4.32 1952
These are taken primarily from the 1952 paper, with the exception of two formulae from the 1958 paper
(highlighted in the Source column). The logic behind the selection is not clear.
-
Poulton Skeleton Manual 52 17-Aug-2013
Females
The white female formulae recommended by [Brickley & McKinley, 2004:33] are listed in the table below:
Formula (in cm) Std Error Source
0.68 XLH + 1.17 XLF + 1.15 LCT + 50.12 3.51 1952
1.48 XLF + 1.28 LCT + 53.07 3.55 1952
1.39 (XLF + LCT) + 53.20 3.55 1952
2.93 XLG + 59.61 3.57 1952
2.90 LCT + 61.53 3.66 1952
1.35 XLH + 1.95 LCT + 52.77 3.67 1952
2.47 XLF + 54.10 3.72 1952
4.74 XLR + 54.93 4.24 1952
4.27 XLU + 57.76 4.30 1952
3.36 XLH + 57.97 4.45 1952
This is the full set of formulae from the 1952 paper. In this case the logic is clear, as there are no other
formulae for white females in the source documents.