

Single-Payer System: Is the Crystal Ball Any Clearer? March 14, 2006 Rick Mayes, Ph.D. Assistant...
36
Single-Payer System: Is the Crystal Ball Any Clearer? March 14, 2006 Rick Mayes, Ph.D. Assistant Professor of Public Policy
-
Upload
oscar-cunningham -
Category
Documents
-
view
213 -
download
0
Transcript of Single-Payer System: Is the Crystal Ball Any Clearer? March 14, 2006 Rick Mayes, Ph.D. Assistant...

Single-Payer System:Is the Crystal Ball Any Clearer?
March 14, 2006
Rick Mayes, Ph.D.Assistant Professor of Public Policy

2
Life’s Unavoidable TradeoffsIndividuals, families, organizations, companies, states,
nations constantly strike balances between:
Security and Freedom
Egalitarianism and Individualism
Every health care system has its strengths & weaknesses
(“problems”).

3
Life’s Unavoidable Tradeoffs

4
Life’s Unavoidable Tradeoffs

5

6

7

8
Health Care Spending as % of GDP, 2002(in purchasing power parity - U.S.$)
Source: OECD Data 2003

9
Why is the U.S. so Different from Other Countries?

10
Why is the U.S. so Different from Other Countries? “It’s primarily because of higher PRICES (less efficiency).”
Health Services Capacity & Use in U.S. and OECD, 2000
U.S.
U.S.
U.S.
U.S.
OECD
OECD
OECD
OECD
0
1
2
3
4
5
6
7
Acute care hospital beds per 1,000 pop.
Hospital admissionsper 10 pop.
Average length of hospital stay (days)
Acute care hospital stays per capita

11
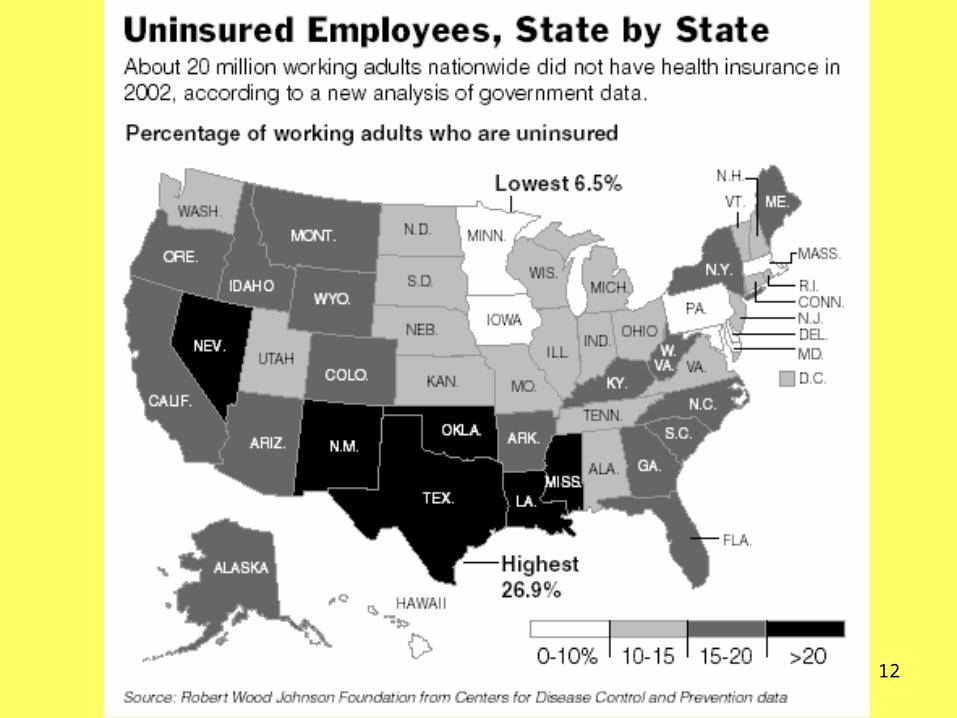
The Uninsured, 15.6% of the U.S. Population (Census, 2005)By Household Income
$50,000-$74,999
12%
$25,000-$49,999
20%
$75,000+8% Under
$25,000 24%
By Education
No High School
Diploma 24%
College Degree+
8%Associate
Degree 12%
High School
Graduate 19%
Some College
12%
By Race/Ethnicity
Asian 18%
African American
20%
Hispanic 32%
White11%
12

13
Consequences: Care Postponed & Not Received

14
Extreme Consequences: Bankruptcy & Earlier Death• 50% of uninsured patients have debts from previous medical
care; a 1/3rd are being pursued by collection agencies
* Uninsured women with breast cancer are twice as likely to die as women with breast cancer who have health insurance.
(Kaiser Commission, 2002)
• Men without health insurance are nearly 50% more likely to be diagnosed with colon cancer at a later, more dangerous stage than men with insurance.
(Kaiser Commission, 2002)
* Upwards of 750,000 families are bankrupted by medical debt each year, even though 80% of them have some form of health insurance; single largest cause of bankruptcy (Health Affairs, 2005).

15
Arnold and Sharen Dorsett with their children, Dakota, Zachery and Jessica, back. Though they had insurance, health-care costs for Zachery led the Dorsetts to file for bankruptcy this year.
Nicole Bengiveno/The New York Times

16
Why no Universal Coverage in the U.S.?
Popular explanations:
-- it would be too expensive
-- American welfare policy is too stingy
-- traditional opposition by medical providers,
particularly physicians (the AMA)

17
America’s “Accidental” Health Care System
Critical Junctures & Tipping Points
↓Increasing Returns
↓Path Dependency

18
Critical Junctures & Tipping Pointsrare, often unpredictable, and hugely consequential for
what comes after
(e.g., QWERTY keyboard, VHS/Betamax, health epidemics)
personal examples (e.g., college major)

19
Increasing ReturnsEach subsequent step after a critical juncture reinforces the
initial event/decision due in part to large set-up or fixed costs
(e.g., frequent flier-programs, entitlement programs: Medicare/Social Security)
Momentum builds due to decreasing marginal costs and increasing benefits for continuing down the existing path.
At the same time, increasing penalties and costs for exiting from the current path.

20
Path DependencyThe benefits of sticking with a particular program or
decision ultimately increase to the point that they virtually outweigh any dramatic departure.
senior professors Vietnam Iraq

21
America’s “Accidental” Health Care System
Truman and NLRB ruling in 1948
regarding collective bargaining
famous GM-UAW 1948 contract

22
America’s “Accidental” Health Care System
0
10
20
30
40
50
60
70
80
1942 1946 1950 1954 1958 1962
Year
Per
cen
tag
e
Private HealthInsurance
PrivatePensions
23
One Problem with Employer-Provided Health Insurance
It creates gaps! . . . for the unemployed and the elderly (classic market failures).
Answer: build on the existing public social insurance program, Social Security…
Medicare & Medicaid, 1965
Still took:
(1.) the assassination of a President (JFK)
(2.) a landslide Democratic victory in ‘64 (thanks to Goldwater), and
(3.) a financial “deal” with the AMA and the AHA to pass Medicare.

24
One Problem With Medicare: Cost ($)
0
5
10
15
20
25
30
35
40
45
50
55
72 73 74 75 76 77 78 79 80 81 82
Year
enrollees(millions)
$ payments(billions)

25
America’s “Accidental” Health Care System

26
Path Dependency and America’s “Accidental” Health Care SystemClinton’s health reform effort in 1993-94 showed just how
entrenched our patchwork system of health care is.
Only 2 options available to Clinton:
large income tax increase or employer mandate
RESULT: health care in the U.S. is rationed ad hoc, person by person, child by child . . .

27
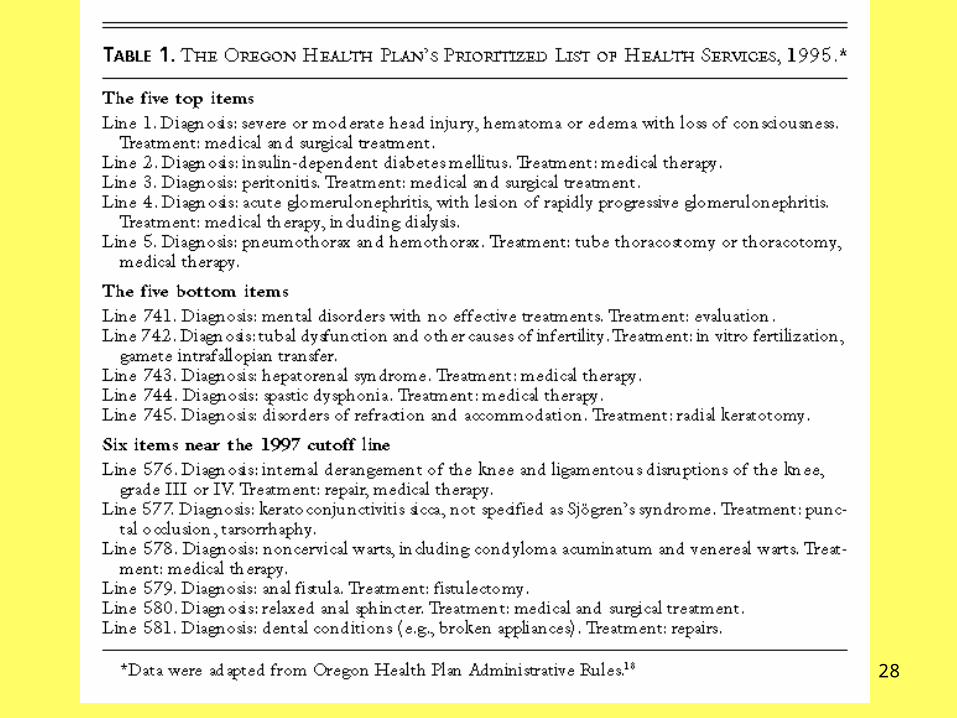
The Oregon Health Plan: Deliberative Rationing
1987: Death of 7-year old Coby Howard from leukemia
1989: Dr. John Kitzhaber, ER physician and President
of the Oregon Senate advocated changing Medicaid
1991: “Prioritized List” of diagnoses & treatments
1994: Oregon Health Plan begins operation, adds 100,000
2003: sliding-scale premiums increased and new co-pays

29
Two Major Developments Hindered Oregon’s Plan
(1.) 2001 recession
(2.) crystal-meth epidemic

30
State of U.S. Health Care System
Since 2000 . . .
health insurance premiums have increased 73%
(versus 14% in general inflation and avg. wage growth)
- avg. cost of single coverage ($4,000 annually in 2005)
- avg. cost of family coverage ($11,000 annually in 2005)
The percent of companies offering health insurance to their workers has fallen from 69% in 2000 to 60% in 2005
(5.5 million working Americans have lost their coverage since 2000)

31

32
Segmentation of U.S. Health Care Increasing: CONCIERGE MEDICINE
Patients like Ilse Kaplan, left, receive more personal attention from Dr. Bernard Kaminetsky in exchange for an annual fee of about $1,650.

34
Term used to describe the paradoxical fact that insurance can change behavior of the person insured.
example: employer-provided “donut” insurance or auto insurance
avg. annual amount spent on medical care (by uninsured person) = $934
avg. annual amount spent on medical care (by insured person) = $2,347
Conclusion I: co-pays, deductibles, utilization reviews make patients use health care more “efficiently” (frugally, wisely, sparingly, etc.)
Conclusion II: instead of expanding group health insurance, reduce it
The “Moral Hazard” Argument Against Expanding Health Insurance Coverage

35
The “Moral Hazard” Argument Against Expanding Health Insurance Coverage
Fallacy I: Moral-hazard argument only makes sense if we consume health care in the same way we consume donuts, car repairs or consumer goods.
Fallacy II: Having to pay for your own care does not automatically make ALL of your health care consumption more “efficient.” How could it?
example: wife’s appt. with dermatologist
Reality: cost-sharing is a very BLUNT instrument
example: RAND Corporation’s “Health Insurance Experiment” (1971-86)
BOTTOM-LINE: health insurance is moving in the “actuarial” direction and away from the “social insurance” model w/enormous consequences to come…

36
Alternative Model?


















