Singer, however, -...
15
STUDIES WITH INAGGLUTINABLE ERYTHROCYTE COUNTS. VI. ACCELERATED DESTRUCTION OF NORMAL ADULT ERYTHROCYTES IN PERNICIOUS ANEMIA; CONTRI- BUTION OF HEMOLYSIS TO THE OLIGOCYTHEMIA 1, 2 By HENRY E. HAMILTON, ELMER L. DEGOWIN, RAYMOND F. SHEETS, CLINTON D. JANNEY, AND JASON A. ELLIS (From the Departments of Internal Medicine and Physiology, and the Radiation Research Laboratory, State University of Iowa, Iowa City, Iowa)' (Submitted for publication April 16, 1953; accepted October 7, 1953) The method of differential agglutination of Ashby has been employed by many workers in at- tempting to elucidate the mechanism of the oligo- cythemia in pernicious anemia. In 1921, Ashby (1) reported the first of these studies. In the first paragraph of her paper she stated, "Many of the older writers inclined to the idea that pernicious anemia is fundamentally a failure of erythrogene- sis, but in the light of recent investigations it is more generally assumed that increased blood de- struction is the important cause of the anemia in this disease." From her studies, however, she concluded that there was no hemolytic factor in the disorder, but it should be recalled that in 1921 highly specific and potent antisera for reagents were not available to her. In more recent studies with differential aggluti- nation Callender, Loutit, and Jope (2) found that the erythrocytes from patients in relapse from pernicious anemia, when transfused to normal re- cipients, survived only 20 to 60 days. Likewise, Singer, King, and Robin (3) reported similar ex- periments in which the patient's erythrocytes disap- peared from the normal subject's circulation at 28, 72, and 75 days. In the reverse experiment, sev- eral groups of workers (2, 4-6) have transfused normal adult erythrocytes to patients with un- treated pernicious anemia and observed normal survival times. Inspection of the data, however, 1 This investigation was supported in part by the Medi- cal Research and Development Board, Office of the Surgeon General, Departnent of the Army, under Contract No. DA-49-007-MD-485. 2 Portions of the material in this paper were presented before the American Society for Clinical Investigation at Atlantic City, May 5, 1952, and the Central Society for Clinical Research at Chicago, November 8, 1952. reveals that in some cases the conclusions were based on very few inagglutinable cell counts. Loutit (2) affirmed this paucity of data in a pub- lished discussion of his own studies. Acceptance of the conclusions that adult nor- mal erythrocytes survived normally in the cir- culation of the untreated patient with pernicious anemia, together with the curative effect of B12 on the disease and the demonstrated influence of B12 on the cells of the bone marrow, seem to have led to the concept that hemolysis plays but a minor role in the oligocythemia of the disorder. The purposes of the present studies were (a) to ascertain whether patients with untreated perni- cious anemia possess a hemolytic mechanism which acts upon normal adult erythrocytes, (b) to assess the effect of vitamin B12 upon such a mechanism, if present, and (c) to measure the rate of release of the patient's erythrocytes to the circulation in un- treated pernicious anemia. The experiments con- sisted of transfusing normal fresh adult erythro- cytes of group 0 to patients with pernicious anemia in relapse, or in various stages of treatment with B12, who belonged to blood groups A or B. The transfused cells were measured by the method of differential agglutination. In one case the eryth- rocytes from a patient with untreated pernicious anemia were transfused to a normal subject and similar measurements were made. With suitable assumptions, the rate of loss of transfused cells from the circulation was calculated. With these data as points of reference, the erythrocyte counts of the subject were employed to estimate the rate of release of the subject's own cells to the circula- tion, termed briefly rate of erythrocyte release. This rate is not necessarily equal to the rate of nu- 191
-
Upload
truongquynh -
Category
Documents
-
view
215 -
download
0
Transcript of Singer, however, -...

STUDIES WITH INAGGLUTINABLE ERYTHROCYTECOUNTS.VI. ACCELERATEDDESTRUCTIONOF NORMALADULTERYTHROCYTESIN PERNICIOUS ANEMIA; CONTRI-
BUTION OF HEMOLYSISTO THEOLIGOCYTHEMIA1, 2
By HENRYE. HAMILTON, ELMERL. DEGOWIN,RAYMONDF. SHEETS,CLINTON D. JANNEY, AND JASON A. ELLIS
(From the Departments of Internal Medicine and Physiology, and the Radiation ResearchLaboratory, State University of Iowa, Iowa City, Iowa)'
(Submitted for publication April 16, 1953; accepted October 7, 1953)
The method of differential agglutination ofAshby has been employed by many workers in at-tempting to elucidate the mechanism of the oligo-cythemia in pernicious anemia. In 1921, Ashby(1) reported the first of these studies. In thefirst paragraph of her paper she stated, "Many ofthe older writers inclined to the idea that perniciousanemia is fundamentally a failure of erythrogene-sis, but in the light of recent investigations it ismore generally assumed that increased blood de-struction is the important cause of the anemia inthis disease." From her studies, however, sheconcluded that there was no hemolytic factor inthe disorder, but it should be recalled that in 1921highly specific and potent antisera for reagentswere not available to her.
In more recent studies with differential aggluti-nation Callender, Loutit, and Jope (2) found thatthe erythrocytes from patients in relapse frompernicious anemia, when transfused to normal re-cipients, survived only 20 to 60 days. Likewise,Singer, King, and Robin (3) reported similar ex-periments in which the patient's erythrocytes disap-peared from the normal subject's circulation at 28,72, and 75 days. In the reverse experiment, sev-eral groups of workers (2, 4-6) have transfusednormal adult erythrocytes to patients with un-treated pernicious anemia and observed normalsurvival times. Inspection of the data, however,
1 This investigation was supported in part by the Medi-cal Research and Development Board, Office of theSurgeon General, Departnent of the Army, under ContractNo. DA-49-007-MD-485.
2 Portions of the material in this paper were presentedbefore the American Society for Clinical Investigation atAtlantic City, May 5, 1952, and the Central Society forClinical Research at Chicago, November 8, 1952.
reveals that in some cases the conclusions werebased on very few inagglutinable cell counts.Loutit (2) affirmed this paucity of data in a pub-lished discussion of his own studies.
Acceptance of the conclusions that adult nor-mal erythrocytes survived normally in the cir-culation of the untreated patient with perniciousanemia, together with the curative effect of B12 onthe disease and the demonstrated influence of B12on the cells of the bone marrow, seem to haveled to the concept that hemolysis plays but a minorrole in the oligocythemia of the disorder.
The purposes of the present studies were (a) toascertain whether patients with untreated perni-cious anemia possess a hemolytic mechanism whichacts upon normal adult erythrocytes, (b) to assessthe effect of vitamin B12 upon such a mechanism, ifpresent, and (c) to measure the rate of release ofthe patient's erythrocytes to the circulation in un-treated pernicious anemia. The experiments con-sisted of transfusing normal fresh adult erythro-cytes of group 0 to patients with pernicious anemiain relapse, or in various stages of treatment withB12, who belonged to blood groups A or B. Thetransfused cells were measured by the method ofdifferential agglutination. In one case the eryth-rocytes from a patient with untreated perniciousanemia were transfused to a normal subject andsimilar measurements were made. With suitableassumptions, the rate of loss of transfused cellsfrom the circulation was calculated. With thesedata as points of reference, the erythrocyte countsof the subject were employed to estimate the rateof release of the subject's own cells to the circula-tion, termed briefly rate of erythrocyte release.This rate is not necessarily equal to the rate of nu-
191

H. E. HAMILTON, E. L. DEGOWIN, k. P. SHEETS, C. fl. JANNEY, ANI J. A. ELLIS
4c 4
4-.1
a) 0 0E)
b~
rNA (A, _
4J 4-408 E
4
C) + t+0SEn cn
. a
+>@ Q +
c c
* + E
U.) Q2 0)
00 (AU C-.rA) \"00C 00cl ccaa a °.
SS X CeqN
44
00 0
00I #) o44-
a )
If)
'0
4- 0
o 0U)
00
o qo 0 00 0
ei) u L)
'0
eq 0O g CS~e
O O
* .4. *I -~
0
00L
192
0
U)
4-)
4)
cC
u
co
C)
10
WI)
coUd
.Ei,le
4i
*b4
" kct3 ?,%m °)< o~
.Q
*t3
I
U)w
4-)
af)
Cd
CI
U
CIS
U)
0
I.M
0
U)
U)0
0
0
CC
CIS
00
C C O
0
CC
ai)
.0
4Ut
0
Sa)U)
C C d
u
Ut0n '-E0I.a)
0eCC 0I. CCC a
0
3C ,
EI.
.0Q
UtCCo
*
i
6r

VI. HEMOLYSIS IN PERNICIOUS ANEMIA
merical production of erythrocytes in the bonemarrow. The present study does not deal withthe rate of formation of hemoglobin nor any othererythrocyte components.
METHODS
Patients. All had proven Addisonian pernicious anemia.In each instance the diagnosis was made by the history,the physical findings, the demonstration of a hyperchromicanemia, the characteristic cytologic picture in the bonemarrow of pernicious anemia in relapse, and achlorhydriaafter stimulation with histamine intramuscularly. In allcases the injection of B12 intramuscularly resulted inprompt reticulocytosis and subsequent rise of erythrocytecounts to the normal range. These phenomena were ac-
companied by characteristic improvement in the clinicalpicture. Other features of pernicious anemia were usu-
ally present, such as leukopenia, thrombocytopenia,atrophic gastritis, elevated serum bilirubin level, and in-creased excretion of urobilinogen in the urine. Observa-tions of the patients for many months confirmed the ab-sence of neoplasms, sprue, gastrocolic fistulae, diseases ofthe liver, intestinal parasites, chronic hemorrhage, gener-alized infections, azotemia, and myxedema. The pertinentdata are found in Table I.
Donors. Blood was collected from healthy young men
of group 0 and transfused to patients of group A or Bwith compatible subtypes of Rh. Previously blood fromthe donors had been transfused to other recipients andnormal survival had been demonstrated.
Transfusions. Approximately 500 ml. of blood was em-
ployed for each transfusion. The donor's blood was col-lected in 3.2 per cent sodium citrate solution (Na,C.H,012 H2O) and stored at about 40 C. for less than 18 hours.The supernatant plasma was decanted and the cellswashed once with 0.9 per cent NaCl solution. Counts ofthe donor's erythrocytes were made and a measured vol-ume of blood was prepared and injected by gravity, as
described previously. During the first 24 hours aftertransfusion frequent samples of the recipient's plasmawere examined and found to contain no abnormal amountsof bilirubin or hemochromogens.
Erythrocyte counts. After transfusion the donor's cellcounts were estimated in the recipient's circulation by a
modification of the Ashby differential agglutination tech-nique previously described and evaluated by us (7, 8).The initial inagglutinable cell counts ranged from 405,-000 to 974,000 per mm.' Counts of the total erythrocytesin the recipient were made simultaneously with those ofthe inagglutinable cells. At each observation the average
was taken of six hemacytometer chamber counts; eachpair of chambers was filled from the contents of a sepa-
rate pipette. The counts of the recipient's own cells were
obtained by subtracting the observed value for the inag-glutinable cell count from the contemporaneous totalerythrocyte count.
LOSS OF NORMALADULT ERYTHROCYTESTRANS-
FUSEDTO PATIENTS WITH PERNICIOUS
ANEMIA
Method of Analysis
The observed values for the inagglutinable erythrocytecounts were employed to calculate NoQ values, which ineffect added to the observed values the number of cellsestimated to have been lost by normal aging. The NoQvalues, therefore, represent counts of cells with infinite po-tential life span which are only diminished by randomdestruction. These were calculated using equation 4, de-rived and discussed previously (9):
NNoQ= when 0 t T
T
where NoQ= the inagglutinable cell count adjusted tocompensate for cells lost by normal aging, N= the ob-served value for the inagglutinable cell count at time t,t = the day after transfusion when the cell count was ob-tained, T = the potential life span of the transfused eryth-rocytes (assumed to be 120 days in these studies, althoughthe assumption of 100 days does not affect the curves sig-nificantly). Values for NoQ were plotted on a verticallogarithmic scale and time t in days after transfusionon a rectangular scale of the abscissa. On such a graphN.Q values for cells lost solely by normal aging describea horizontal line with zero slope. Random destruction ofcells is indicated by a curve diverging downward fromthe horizontal and to the right. If the diverging curveis a straight line, the percentage rate of loss is constantand the slope indicates the percentage rate of random loss.When the diverging curve is curvilinear, the rate of lossis accelerating or decelerating, as the case may be.
Results
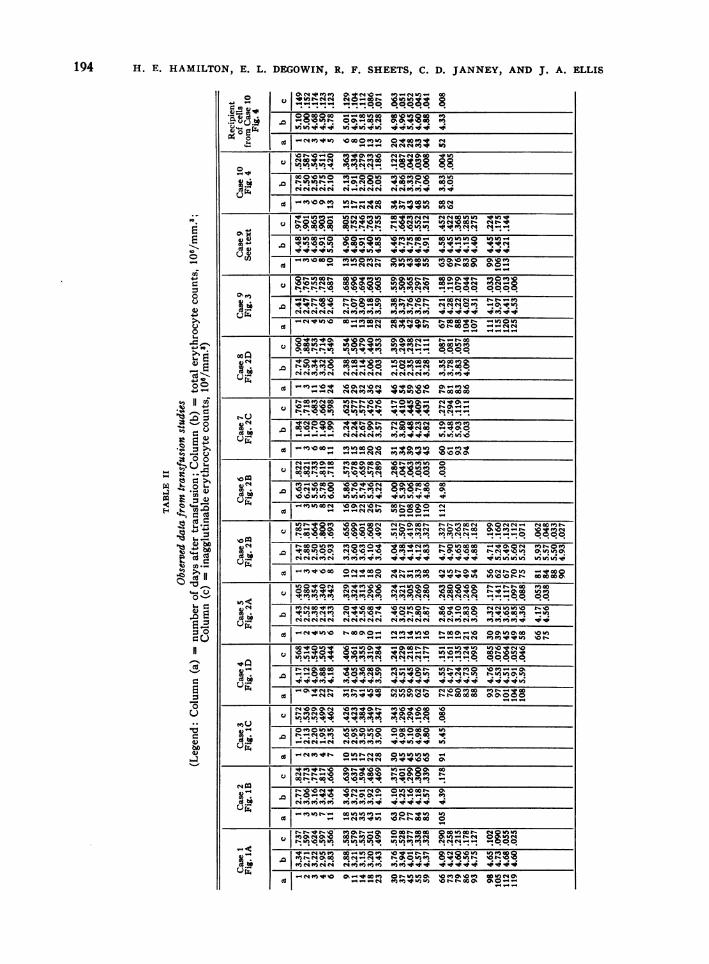
The observed values for the erythrocyte countsin these studies are presented in Table II, the quan-tities calculated from them are plotted in Figures 1,2, and 3.
Case 1 (Figure IA), G. Jam., an 83-year-old man wasadmitted to the hospital May 20, 1951 and discharged140 days later. Initially he was disoriented. There hadbeen no previous antianemic therapy. He belonged togroup A Rh. positive and was transfused with 500 ml. ofblood of the same group on the first hospital day. Vita-min B,, was given intramuscularly, 15 micrograms daily,for 59 days and then on the 66th, 73rd, 80th, 95th, 101st,115th, and 122nd day. A transfusion of normal freshgroup-O erythrocytes was given on the 12th day aftertherapy with B. was begun. The patient made a com-plete clinical recovery and was discharged mentallyhealthy and without other signs of the disease. The N.Qvalues for the donor's blood fit with reasonable exactnessa horizontal line, indicating no loss of transfused cells
193
I oz0W)a ooswo e.-coC,:~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~0okwoo0 .o e co***
. . . . . . . . . . . *r*)) ll )OW")q") q
I_ a- s o-4 0 *Chmo r- 40 1 'o02+o400-( 2m Wwe"N o!B"
'ID 0 'oo)VMo -8w :M OV
o ;0e°Cd S *NC4NC_CS N -4 N 04 N 04 M MVm
-4 -_qeeftNNMM VO) V)V_uW> '._ v>o W) m Mez ""WU)U) )va
t_c0L\0 0 0rorWoo"u*N__isU 0W0_o so_ou ~~~~~~~~~Oemw)_coW) ) )! & W) _
__m%oaot)o t,. v voW)W o 00c"fg41otO
cto m o V> U) _oso o- co o 0.
-_NoU O 1--900S NeorNO 0+k_V-tVItIttt10qp~~~~~~_C -.an "io n- luxl00ite! -- ": ttn
0oQ . . . . . . . .N . ..
X*~~~~~~~ VNee No00 e-cooei I
00W
.oe ""MM" ""N""s ""seso mmmv
IVN~~~~~~~~. ..OO t0N MMMV,1 NO OC,
a a0tt ORbeNOtl) W0i0 e ego. ___ C!"" C!t
0t i_ oN..0 ¢o o -" Noocogo N.
W)-148 NO\0% " 0 "N t CK 04t-t -M 0NaNNqNot
CNOO ll oq . .IR ql I Ileo:0lil io l!" :R
U)+Oa 0-Ntq08!oC',W 0sN Nt;I :'R i a tC0_o00 IRoo_O-NIel!or Ite-IR OeInCm m.mo v¢ ^ In>" in- o oooo.fW W@N b0ov)e e0e0~~~"Vw "t,"Mw No"t-oon_+VWOr0Zt0~~~~~~~~~~- --+0.o. "e_ o¢__0. "Ivotni I t -. co+omOk
W0W0N 0\+ea0D _UwOsNOco COOS,* -q a_
in MM, vovV+e-ow "sONn0t-"O0 Ma "Wlor+os v>¢
@N~~~~~~~~~~~rwa"eseMoovorw e.oo o no co.nou ooo r|~~~~~~~~~~~~~~..4.-D4-4">""+)o-.400.-4 " mmlolo. _
0.4! _n'OMN otIq inU> Csb_e^ 0ooomv
*:~~~~~~~~~~~~l ?l Il ,i " .. .... Ili. ... ... ... ........
oz. I ,lo ~"00_ vOOtcSVt SY>SPoV) krvNom rxOM-ed~~~~~~~~~~~enltlOtqI'rit tln0bPfnsfCtP+sn+*
Or~~~~~~~~~InICInICSI?-ns Ct+ CU>t. 01 0 Itr0 o
" rb_ oY 2mccol t- 0 "b'
ON.~~~~~~~~~l tttC t lI-iI MnmMSenene+enro ovV va _I mon-I0 i_ni en*o ini
I~~~~~~~~q m l 'I teOt- ep *o o.v)_o0
I_ v _v3 o_ eOo e o,/ er0
V 0NN)W"W0om S=Olnr OO)OMi"evlee ee**:)**ORa
**I ttt:*qnnt itl I I%I
;194 H. E. HAMILTON,9 E. L. DEC;OWIN, R. F. SHEETS, C. D. JANNEY, AND J. A. ELLIS
OcMvmm a ."^o-4 e-4")-4 0*es o mm 82w)o z o04i -4C: co 4)
.2=- ma 40 co
(Jr )I;o .-.i
v 0 stz.04 0w
11--14"MVW) .OWOMLn O*WMIO "
4..4-4 "NNMV "
.4-
E
4-
4)ecd
*0 0u D
..
-C;3d^ t. W
4XK o
Cd
°r.
4^O-
bo*
.r-t-r*tQS MCKr--& owtr00 o0woort "§W)W1- u) 'I u) *f &qSinz uq iv &ne a oee c4c (-- cOO
-"MV,40 0%-VWM ol-lnwo ~Omo%%O ww)""___"N MqMV'n& \01-0O, ONO"
4-

VI. HEMOLYSIS IN PERNICIOUS ANEMIA
I i/5,*P. 812
flhUlElEIN ~INIIIlUHI l I I I I I I IM1 E11|111-1-I 1-II
o 10 40 60 0 A 6MA4 TR TRAN&FUlON
A.
F I I
so __L__°1. +_1 0.7n0 I
-i ' I I1-lll l u 1- 1 -1 1 1120 SO 60 eV ao QV
MYSAVTEi T4A.4N5U30
C.
.900
*700.600 -
Who
.,~~~~~~~~B .9 .e bd
200- __5, 9d I~45/"y. B12
pi tllllIh I I I I I I I I./00 IL LI I
0 20 /00 AAV
B.
Celk
.700
.40
400
.00 -L20 40 00 /00
ACTArEA TMAW/UION
D.
FIG. 1. RANDOMLOSS OF FRESH NoRMALERYTHROCYTESTRANSFUSEDTO PATIENTS WITHPERNICIOUS ANEMIA TREATEDWITH B. AT VAious Tam
The data are plotted on semilogarithmic scales. The open circles are NoQ values calculatedfrom the observed inagglutinable cell counts in such a manner as to compensate for the cellslost by normal aging. By this method of calculation and plotting a horizontal straight line isformed when there is no random loss of cells. Deviations downward from the horizontal indi-cate random destruction. When the deviated curve is a straight line, there is a constant per-centage rate of random destruction and the slope of the line indicates the rate. Deviation fromthe straight line toward the horizontal occurs when the rate decelerates, whereas deviation fromthe straight line toward the vertical indicates acceleration.
In charts IA and 1B, when injections of B.2 were started 12 and 9 days before transfusion, therewas no loss of cells by random destruction. In chart 1C, when B, was started 3 days beforetransfusion, there was random loss of the donor's erythrocytes for the first 15 days; thereafterthe remaining cells survived normally. Mathematical considerations and facts established inthe following studies warrant the interpretation that only a few transfused cells were damagedand destroyed at random.
Cells transfused one day before B. therapy was begun are shown in chart 1D to have beenlost at random with the constant rate of 0.43 per cent.
&1hIl i0
-U-O-- 0-0- --
-1 -4--- -4-
- 0 0 ___i0
.700
.60
300
.200
.100
Celb
.200
.100 i
I JagSWAm3*pAwr
.4An'
--?.~~~4gIdyut,S*0-p
0"*0-0..
/..,* B,21III 111111 111111 III IIIIIIIIIII III III Hill
I
195
9
196 H. E. HAMILTON, E. L. DEGOWIN, R. F. SHEETS, C. D. JANNEY, AND J. A. ELLIS
I CI I IJdIb CieIII I1I I IllllII III 111111
200
.AW~~~~~~~'.
IncI..--O 20 i60 W a 10 40 160 UQ A0 /QVMYSTAFTfR TR4NSFUJON DAYS AFTER TRAWANSI
A. 8
Coft 1 ==7 scor atz w II_| zt 1.700 0 o0.0
.L00 1 10 11C. D4tv 0%.
.soo -12 sder e(k r NO0
.200 ~ ~ ~ ~ ~ 2
.1000 I M - J 0 Ai &w /o20 MYA0if TRNFUIN 0 DAY AFeR RANSUSO
C. 1).
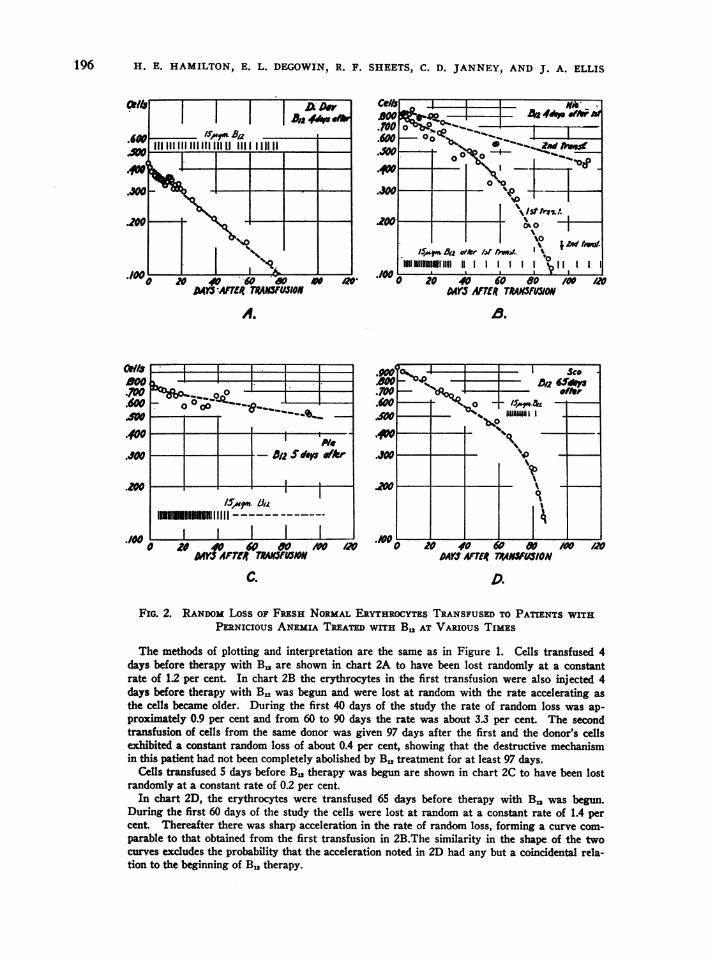
FIG. 2. RANDOMLOSS OF FRESH NORMALERYTHROCYTESTRANSFUSEDTO PATIENTS WITHPERNICIOUS ANEMIA TREATEDWITH B,, AT VARIOUS TIMES
The methods of plotting and interpretation are the same as in Figure 1. Cells transfused 4days before therapy with B. are shown in chart 2A to have been lost randomly at a constantrate of 1.2 per cent. In chart 2B the erythrocytes in the first transfusion were also injected 4days before therapy with B. was begun and were lost at random with the rate accelerating asthe cells became older. During the first 40 days of the study the rate of random loss was ap-proximately 0.9 per cent and from 60 to 90 days the rate was about 3.3 per cent. The secondtransfusion of cells from the same donor was given 97 days after the first and the donor's cellsexhibited a constant random loss of about 0.4 per cent, showing that the destructive mechanismin this patient had not been completely abolished by B1 treatment for at least 97 days.
Cells transfused 5 days before B. therapy was begun are shown in chart 2C to have been lostrandomly at a constant rate of 0.2 per cent.
In chart 2D, the erythrocytes were transfused 65 days before therapy with B1, was begun.During the first 60 days of the study the cells were lost at random at a constant rate of 1.4 percent. Thereafter there was sharp acceleration in the rate of random loss, forming a curve com-parable to that obtained from the first transfusion in 2B.The similarity in the shape of the twocurves excludes the probability that the acceleration noted in 2D had any but a coincidental rela-tion to the beginning of B. therapy.
_

VI. HEMOLYSIS IN PERNICIOUS ANEMIA
from random destruction and supporting the assumptionthat the majority of the cells of the transfused populationhad a potential life span of approximately 120 days.
Case 2 (Figure 1B), B. Wha., a 53-year-old womanwas admitted to the hospital with a mental depressionand anemia. She had been treated for pernicious anemiathree years before with blood transfusions and injectionsof liver extract. She had received no therapy whateverfor five months preceding admission. Vitamin B,, wasgiven intramuscularly in 15-microgram doses daily for17 days and on the 23rd, 30th, 37th, 44th, 51st, 58th, 65th,72nd, 80th, and 85th day. There was complete sympto-matic and hematologic recovery. The patient belonged togroup A Rh. positive and received a transfusion of nor-mal fresh erythrocytes of group 0 Rh. positive nine daysafter treatment with B,. was begun. The resulting N.Qvalues fit a horizontal line, prompting the conclusion thatthere was no random destruction of the transfused cellsand that their potential life span was approximately 120days.
Case 3 (Figure IC), W. Sau., a 63-year-old man was ad-mitted to the hospital September 30, 1952 because ofweakness incapacitating him for work. He had receivedno previous therapy for anemia. Vitamin B,1 was givenintramuscularly in 15-microgram doses daily for 34 daysand then every 14 days until the end of the study. Hemade a complete clinical and hematologic recovery andreturned to work. The patient belonged to group A Rh.
DAYS MERT7RSFUJIONFIG. 3. EFFECT OF INTERRUPTING B. THERPY ON
RANDOMLoss OF FRESH NORMALERYTHROCYTESTRANs-FUSEDTO A PATIENT WITH PERNICIOUs ANEMIA
The methods of plotting and interpretation are the sameas in Figures 1 and 2. Vitamin B,, was injected intra-muscularly in daily doses of 15 micrograms, from 9 daysbefore transfusion until 15 days afterward, when treatmentwas discontinued until the 62nd day after transfusion.The transfused cells survived normally until about 20 daysafter cessation of therapy when random loss at a constantrate of over 0.9 per cent occurred. This loss was main-tained despite resumption of B, therapy.
positive and, three days after the inception of B,,therapy, he was transfused with normal fresh erythrocytesof group 0 Rh. positive. For the first 15 days after trans-fusion the N.Q values described a sloping curve indicatingrandom loss of cells. Thereafter to the end of the ex-periment they fit a horizontal line, with no indication offurther random destruction. This curve is explained bythe fact that only a few of the transfused erythrocyteswere injured, irrespective of their ages, and were destroyedat random.
Case 4 (Figure ID), J. Dav., a 75-year-old man was ad-mitted June 25, 1949 with an infection of the urinary tractand inability to walk because of severe manifestations ofposterolateral sclerosis of the spinal cord. He had re-ceived no antianemic therapy previously. He was given15 micrograms of B,, intramuscularly on alternate daysfor a period of 94 days, and experienced considerablefunctional improvement. On discharge he could walkwith a spastic gait and had recovered control of hisbladder. He belonged to group A Rh. positive and on thefirst day of B. therapy he was transfused with fresh nor-mal erythrocytes of group 0 Rh. positive. The N.Qvalues for the resulting inagglutinable cell counts fit astraight line with a slope which indicates a random lossof 0.43 per cent of the remaining cells each day, in ad-dition to the loss by aging. The conclusion was drawnthat a hemolytic mechanism was present which injuredthe adult normal erythrocytes soon after transfusion sothat they were subsequently lost at random, despite con-comitant therapy with B,,.
Case 5 (Figure 2A), D. Dav., a 77-year-old man wasadmitted April 23, 1949 with anemia and cardiac insuffi-ciency. There had been no previous antianemic therapy.The patient was given 30 injections each of 15 microgramsof B., in the next 80 days on approximately alternate days.His blood was found to belong to group A Rh. positiveand, four days before therapy with B,, was begun, hewas transfused with fresh normal erythrocytes of groupO Rh. positive. The NoQ values for the resulting inag-glutinable cell counts fit a straight line with a slope indi-cating random destruction of the transfused erythrocytesat a rate of 1.2 per cent per day. Eight months after thestudy he was readmitted to the hospital in cardiac failurebut there had been no relapse of the pernicious anemiaunder treatment continued at home.
Case 6 (Figure 2B), E. Nie., a 66-year-old woman wasadmitted January 7, 1950. Pallor had been noticed forsix years and progressive weakness had finally confinedher to bed. No therapy had been given for the anemia.Soon after admission she was transfused with 1,000 ml. ofblood of group A Rh. positive, the group to which she be-longed. At the beginning of this study she was trans-fused with fresh normal erythrocytes of group 0 Rh,positive. Four days later daily injections of 15 micro-grams of B., were begun and continued for 30 days;thereafter similar doses were given at weekly intervals.Gradual symptomatic improvement was noted and theabnormal neurologic signs disappeared in several months.Two years later the patient was in good health with con-
197

198 H. E. HAMILTON, E. L. DEGOWIN, R. F. SHEETS, C. D. JANNEY, AND J. A. ELLIS
tinued antianemic therapy and her hematologic findingswere normal. Ninety-seven days after the first trans-fusion of heterologous group a second transfusion oferythrocytes from the same donor was given. Duringthe first 24 days of the second study weekly injections of15 micrograms of B12 were given and thereafter injectionswere given every two weeks.
The N.Q values from the first tagged transfusion fita curve which indicates random destruction at an ac-celerating rate. Those from the second transfusion con-sist of only 13 counts which are probably insufficient todetermine a curve with any accuracy. However, the val-ues available fit a straight line with much less slope thanthat characterizing the first transfusion. This is cer-tainly evidence that the first curve could not have beenthe result of isosensitization to antigens in the trans-fused erythrocytes.
Case 7 (Figure 2C), M. Pla., a 74-year-old man, wasadmitted January 10, 1950. Sporadically he had receivedinjections of liver extract for anemia for several yearsbut not for the six months preceding admission. He hadbeen confined to bed because of signs of posterolateralsclerosis of the spinal cord. He was given B,,, intra-muscularly in 15-microgram doses for 36 consecutive'days, then on the 38th, 40th, 42nd, 44th, and 46th day, andthereafter at weekly intervals. He showed steady im-provement clinically and hematologically. Five days be-fore B. was begun he was transfused with fresh normalerythrocytes of group 0 Rh. positive (the patient be-longed to group A Rh. positive). The N0Q values de-rived from the inagglutinable cell counts fit well astraight line whose slope indicates a random loss of 0.2per cent of the remaining erythrocytes per day, in addi-tion to attrition from normal aging.
Case 8 (Figure 2D), M. Sco., a 75-year-old woman,was admitted December 12, 1950. She had received noprevious therapy for anemia. The patient belonged togroup A Rh. positive and she was transfused with freshnormal erythrocytes of group 0 Rh0 positive. On the65th day after transfusion daily injections of 15 micro-grams of B. were begun. She made a complete clinicaland hematologic recovery. The NoQ values for the inag-glutinable cell counts during the first 65 days fit a curveindicating a random loss of 1.4 per cent of the remainingerythrocytes daily. Thereafter the rate of loss accelerated.Although the acceleration coincided with the inception ofB. therapy, no causal relation is ascribed since a curveof similar form occurred in Figure 2B.
Case 9 (Figure 3), A. Joy., a 50-year-old woman, wasadmitted April 7, 1951 with weakness which confined herto bed. She had previously been known to have schizo-phrenia but had received no therapy for anemia. She wasgiven 15-microgram doses of B. for 23 consecutive days,therapy was discontinued for the next 48 days, and there-after injections were given about every four days duringthe remainder of the first transfusion experiment. Shemade a complete hematologic recovery and regainedgood physical health but the signs of schizophrenia werestill present 15 months later.
Nine days after inception of the first course of B.therapy she was transfused with fresh normal erythrocytesof group 0 Rh0 positive (she belonged to group B Rh0positive). The N0Q values for the inagglutinable cellcounts show practically no random loss of erythrocytesuntil about 20 days after cessation of therapy when thecurve suddenly dipped to fit a straight line with a slopeindicating a random loss of 0.9 per cent erythrocytes perday. The rate of loss was not influenced by resumptionof B. therapy on the 62nd day after transfusion.
After termination of the first transfusion experimentthe patient was treated with frequent injections of B,, for
.6oo I I
.600 M. 1. Ce//l -o Normel
.400 \
.300 I/ XNormiol Cc//s.4P-.PA
.200 I
NwoQx
'loI I I0 /0 20 30 40
AMTS 4ffR TP4AN/V3IONFIG. 4. RANDOMLOSS OF NoRMAL ADULT ERYTHRO-
CYTES IN PERNICIOUS ANEMIA COMPAREDWITH LOSS OFCELLS FROM PERNICIOUS ANEMIA PATIENT TRANSFUSEDTO NORMALSUBJECT
The N0Q values from the two transfusions are plottedon semilogarithmic scales. The open circles represent thevalues obtained when the erythrocytes from a patientwith untreated pernicious anemia were transfused to anormal subject. For the first 25 days after transfusionthe smoothed curve is straight with a slope indicating arandom loss of 3 per cent of the remaining erythrocytesper day. From the 25th to the 44th day apparently therewas no random loss of cells. Values obtained betweenthe 50th and 60th day were too small to be plotted on asingle cycle logarithmic scale and the inagglutinable cellcounts had become immeasurable by the 56th day. Thecause of the plateau is unknown.
The open crossed circles represent the values obtainedfrom the experiment in which normal adult erythrocyteswere transfused to the patient with pernicious anemiareferred to above. Both transfusions were performed onthe same day. The smoothed curve exactly parallels theother for 25 days, indicating also a rate of random loss of3 per cent of remaining erythrocytes per day. By the 30thday there was gradual acceleration of random destruction.Values below the scale of the chart indicate that the inag-glutinable cell counts became immeasurable by the 55thday.
j
so 60.

VI. HEMOLYSIS IN PERNICIOUS ANEMIA
several months. When complete hematologic and clini-cal recovery had occurred, a second transfusion of bloodfrom the same donor was given after a period of 18daily injections of 15 micrograms of B,,. Daily doseswere continued throughout the second study. The inag-glutinable cell counts showed no evidence of random lossof erythrocytes, excluding the possibility that the firsttransfusion curve could be ascribed to isosensitization toantigens in the donor's erythrocytes.
Summary
Normal adult erythrocytes survived normallywhen transfused to two patients with perniciousanemia who had been given injections of B12 for9 and 12 days, respectively, before the transfusedcells were exposed to the milieu of the patient(Figures 1A and 1B). In five other patients(Figures 1D, 2A, 2B, 2C, and 2D) normal adulterythrocytes were lost by random destruction whenB12 therapy was begun respectively 1, 4, 4, 5, and65 days after transfusion. In another patient(Figure 3) B12 therapy was begun 9 days beforetransfusion and the transfused normal erythro-cytes survived normally for approximately 20 daysafter cessation of therapy. Thereafter, however,the transfused erythrocytes were lost by randomdestruction. In none of the studies alluded towas the random loss of erythrocytes abated bysubsequent administration of B12. Finally, a tran-sition stage in this series of assays of B12 therapyseems to have been observed (Figure 1C) in a pa-tient who was treated with B12 for 3 days beforenormal adult erythrocytes were transfused. Thetransfused cells were lost at random for the first15 days or so, thereafter normal survival of theremainder occurred. This could be interpreted asdamage to only a few transfused cells, irrespectiveof their age.
It should be emphasized that the observed ratesof loss from random destruction were slow,ranging from 0.2 per cent to 1.4 per cent of theremaining erythrocytes per day. This is a muchslower rate than has been observed in the case ofproven hemolysis from isosensitization in trans-fusion. Furthermore, in Cases 6 and 9 subsequentstudies were made after adequate treatment ofthe patients with B12. Erythrocytes from the samedonors were retransfused and found to survivenormally in Case 9 and to be lost randomly at amuch slower rate than before in Case 6.
LOSS IN NORMALSUBJECTOF ERYTHROCYTESFROM
PERNICIOUS ANEMIA COMPAREDTO LOSS OF
NORMALCELLS IN THE PATIENT
Case 10 (Figure 4), L. Ben., a 79-year-old man, wasadmitted to the hospital February 20, 1953. On March 2,blood was collected from him (group 0 MNRh. posi-tive) and the erythrocytes were transfused to a normalrecipient (group A MN Rh. positive). The patient'scells were subsequently identified in the subject's circu-lation by differential agglutination using anti-A serum.The patient was transfused on the same day with freshnormal erythrocytes of group 0 N Rh. positive, and thedifferential agglutination on his blood samples was per-formed with anti-M serum. Therapy was withheld untilthe 28th post-transfusion day when daily injections of30 micrograms of B1. were given until his discharge 53days later. At the termination of his hospitalization hehad improved clinically and hematologically although theerythrocyte level had not yet attained the normal value.
When the NoQ values resulting from the two trans-fusions were plotted on the same graph, the fitted curvesshowed remarkable correspondence in rate of loss forthe first 25 days. For each the rate of random loss wasabout 3.0 per cent of the remaining erythrocytes per day.After the 25th day the rate of loss of the normal erythro-cytes in the pernicious anemia patient accelerated rapidlyand the inagglutinable cells were immeasurable after the55th day. In contrast, the rate of random loss of thepatient's cells in the normal subject was zero from the25th to sometime after the 44th day; but by the 52nd day,they too were immeasurable. This suggests that the hemo-lytic mechanism acts on normal cells at approximatelythe same rate as it does on the erythrocytes of the patient.
RANDOMERYTHROCYTEDESTRUCTIONAS A FACTOR
IN THE OLIGOCYTHEMIAOF PERNICIOUS
ANEMIA
Method of analysis
In a previous paper (10) graphic analyses were derivedand described in detail by which the expected erythro-cyte counts can be computed from the demonstrated rateof loss of transfused cells. The expected erythrocytecounts can then be compared with the observed values andcertain conclusions can be made regarding the rate ofrelease of the patient's own erythrocytes to the circu-lation. For this purpose only two measurements are re-quired: the inagglutinable cell counts and the total eryth-rocyte counts over a long period of time, so that smoothedcurves can be constructed with some validity.
When the conditions of the experiment indicate that thesubject is in the steady state of random destruction oferythrocytes, the resulting expected level of erythrocytecounts can be computed on the assumptions: (a) The rateof cell release to the circulation continues to be normal;(b) the rate of random destruction of transfused eryth-rocytes is the same as that of the subject's cells; (c) the
199

H. E. HAMILTON, E. L. DEGOWIN, R. F. SHEETS, C. D. JANNEY, AND J. A. ELLIS
B
A4
FIG. 5., PATIENTS WITH UNTREATEDPERNIcIOus ANEMIA DEMONSTRATINGTHE EFFECT OF
MATURATIONARRESTON ERYTHROCYTELEvELs
The data are plotted on Cartesian coordinates. On the upper scales are the values for cellcounts of the patient. The lower scale pertains to data from the inagglutinable cell counts offresh normal transfused blood.
In the lower section the solid circles are the observed values for the inagglutinable cell countsof the donor's erythrocytes. The open circles in this section represent the corresponding NoQvalues, calculated from the inagglutinable cell counts to compensate for the loss of cells by nor-
mal aging. The curves formed by the NoQ values are straight horizontal lines when there is no
random loss of cells. Deviations from the horizontal indicate random loss.The solid circles in the upper section are the observed values for the patient's erythrocyte
counts, obtained by subtracting the inagglutinable cell count from the total cell count takensimultaneously. The solid horizontal line indicates the observed erythrocyte level of the patientduring the steady state of random destruction, before B1, therapy. The broken horizontal linerepresents the expected erythrocyte level, estimated for the steady state of random destruction,assuming a normal rate of erythropoiesis, and assuming the rate of random destruction to be thesame as that of the transfused cells. It was previously shown that once the transfused cells are
damaged in the milieu of the patient with B., deficiency, their rate of random loss is unaltered bysubsequent treatment. The open circles, connected by broken lines, are the expected cell countsof the patient during the recovery phase of random destruction, assuming a normal rate of cellrelease beginning shortly after inception of B., therapy, and assuming that the pre-existing crops
of the patient's erythrocytes continue to be lost at random as in the steady state of randomdestruction.
In chart 5A the expected level of the patient's erythrocytes during the untreated state was esti-mated at 3.77 millions per mm.', as compared with the observed level of 1.00 million. The dis-crepancy can be explained as the result of maturation arrest. B., therapy was started 5 days af-ter transfusion. The patient's erythrocyte counts increased faster than was expected and therate of cell release attained a maximum of twice the normal 25 days after the inception of treatment
Therapy with B,. was initiated 9 days before transfusion in the study in 5B. But treatmentwas discontinued 15 days after transfusion, and resumed on the 62nd day after transfusion.The expected level of the patient's erythrocytes before treatment was estimated to be 2.31 millionsper mm.', compared with the observed value of 1.70 millions. This is probably a significant
200

VI. HEMOLYSIS IN PERNICIOUS ANEMIA
potential life spans of cells of both populations are es-sentially the same. The N.Q values were plotted onCartesian coordinates according to the construction inFigure 6 of the paper (10). Then equation 15 of the samepaper was employed:
RI = Ro y+It)
where R'=the expected cell count of the subject in thesteady state of random erythrocyte destruction, R. = thenormal cell level of the subject, Y = the area under thecurve of the N.Q values, Y + Y' = the area of the en-closing rectangle in Figure 6 (10).
After treatment of the patient having pernicious anemiawith B., the expected curve of the erythrocyte countsduring the recovery phase can be computed on the assump-tions: (a) The rate of cell release continues to be nor-mal; (b) crops of the patient's cells, formed beforetherapy, continue to be lost at random whereas cropsformed during B,, therapy survive normally; (c) therate of random destruction of the patient's cells is thesame as that of transfused cells corrected for loss by aging;(d) the potential life spans of the two cell populations areessentially the same. The N.Q values were plotted onCartesian coordinates, as in Figure 10 (10). The heightof the rectangle was determined by the value No CO, where
N. is the point at which the N.Q curve intersects thevertical axis, a. is the expected cell count in the steadystate of random destruction of erythrocytes and a' is theobserved level of erythrocytes at the same time. Thevalues R,., for the expected erythrocyte counts duringthe recovery phase were computed from equation 28 (10):
Rr.c = Ro( w')where R. is the normal eythrocyte level, Wis the stippledarea in Figure 10 (10), and W+W'=the area of theenclosing rectangle.
The expected values R' and R,.r were then comparedwith the observed values for the recipient's cell counts(total erythrocyte count minus contemporaneous inag-glutinable cell count) and significant discrepancies wereinterpreted as acceleration or deceleration in the normalrate of erythrocyte release to the circulation.
Results
Data from 6 of the 10 cases (Table II) wereavailable for this part of the study because randomdestruction of normal transfused erythrocytes hadbeen demonstrated and the rate of random loss
estimated. The evidence obtained from the crosstransfusion experiment in Case 10 supported theassumption that the erythrocytes of the patient withpernicious anemia were destroyed at random atleast as fast as the normal adult erythrocytes trans-fused to the patient with untreated, or inadequatelytreated, pernicious anemia. Since the disappear-ance curves of normal erythrocytes, transfusedbefore adequate B12 therapy had been given, werenot altered by subsequent administration of thevitamin, it was thought to be a safe assumption thatthe rate of loss from curves obtained during ther-apy were at least not less than the rate beforetherapy was begun. Any calculations resultingfrom the use of these disappearance curves would,therefore, be on the conservative side when the con-tribution of hemolysis to the erythrocyte level wasestimated.
Erythrocyte levels attributable partially tomaturation arrest. The data from two patientscan be interpreted as demonstrating the effect ofmaturation arrest on the erythrocyte levels. InCase 7 (Figure 5A) the observed erythrocyte levelin the steady state of random destruction of eryth-rocytes was approximately 1.00 million per mm.8Assuming that the patient's cells were destroyedat the same rate as the transfused erythrocytes, andassuming the rate of random destruction deter-mined by transfusion obtained also before trans-fusion, the expected level of the patient's cellcounts was 3.77 millions per mm.8 The discrep-ancy between observed and expected levels couldbe attributed to maturation arrest, but the differ-ence between the expected and the normal levelis ascribed to the hemolytic mechanism. Therapywith B12 caused a rapid increase in the erythro-cyte counts of the patient, which in 25 days oftreatment doubly exceeded the number expectedif the hemolytic mechanism had merely been in-hibited and the rate of erythrocyte release to thecirculation had continued normal. This findingis ascribed to an actual acceleration of the rate ofcell release to twice the normal rate.
The data in Case 9 (Figure 5B) were obtained
difference and may be attributed to maturation arrest. The erythrocyte counts of the patientincreased up to 1.7 times the normal rate of cell release for the 15 days of therapy after trans-fusion. The rate of cell production approximated the normal during 47 days without treatment,despite the supervention of random destruction of normal transfused cells. This suggests thatthe destructive effect of B1. deficiency occurs at concentrations of the vitamin which permit cellsstill to be produced by the bone marrow.
201

H. E. HAMILTON, E. L. DEGOWIN, R. F. SHEETS, C. D. JANNEY, AND J. A. ELLIS
CeXli I I I!.
I0 00
40 0 0 A~w
009 -0
I
.1~~~~~~~~~~.,0 £ hsredIvl(wIo
'4
4°°[1 0W_*; t8125Z 00 0-.Jg4.00 1 *** r( 0'& ' - t
0- 1-%- 'D0 f,MeedectWC0S#wqLeOW.3.04 (J'CI,e )
.600
.2
0 JOv 40 60 VW AN"VS diTR TA'A#IF /ON
0
40' 0*
0
o 0"
tL+2: :7xdml4 Ohsere'd Le,vl(N'ie')I I I I
Zm, Ia
0
400
I.&3.00
C
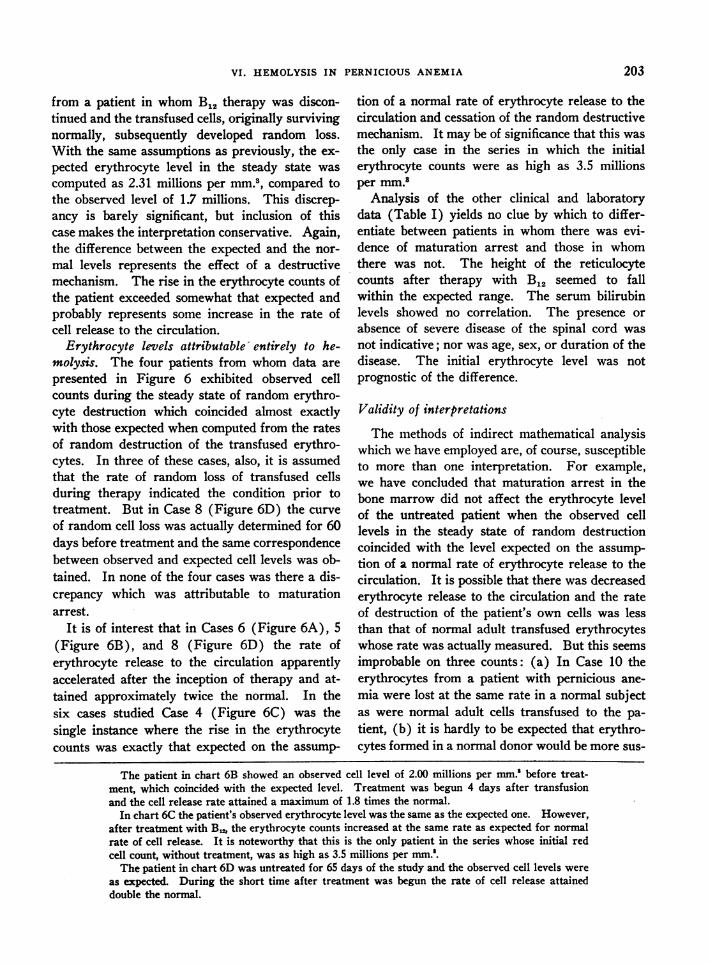
FIG. 6. PATIENTS WITH UNTREATEDPERNICIOUS ANEMIA DEMONSTRATINGNo EFFECT OFMATURATIONARRESTON ERYTHROCYTELEVELS
The methods of plotting and interpretation are the same as in Figure 5. The bone marrow ofall patients exhibited the cytologic findings of maturation arrest. The coincidence of observederythrocyte levels and those expected on the assumption of normal erythropoietic rates can be ex-
plained either on the basis of a sufficient number of cells being produced by overactivity of bonemarrow of normal mass, or by an increase in the total mass of hypoactive marrow sufficientto compensate.
In chart 6A the observed erythrocyte level of 2.09 millions per mm.' coincided with that ex-
pected from a normal rate of cell production and a rate of random destruction similar to that bywhich the transfused cells were lost. Treatment with B. was begun 4 days after transfusion andthe rate of cell release accelerated to a maximum of nearly twice the normal. A cell countof 5.5 millions was attained about 60 days after the beginning of therapy.
202
I~
00
.
00eA0 40 60 so a
MY5AfTER TRANJFU3ON
W~
Cells
0 -
".0
0*+ I 1n~~~~~~~~~~
soso.. I
w o ".%.. 0~0 0
* ...2o oQ_>°Oa-o!LQ000 -0- -O oo0 -
*I.0 1
0...
0 00.I 0~~00,.
-1L
4zA
I
1 I1x'
A Aff
0 a
140-a I.
VI. HEMOLYSIS IN PERNICIOUS-ANEMIA
from a patient in whom B,2 therapy was discon-tinued and the transfused cells, originally survivingnormally, subsequently developed random loss.With the same assumptions as previously, the ex-pected erythrocyte level in the steady state wascomputed as 2.31 millions per mm.8, compared tothe observed level of 1.7 millions. This discrep-ancy is barely significant, but inclusion of thiscase makes the interpretation conservative. Again,the difference between the expected and the nor-mal levels represents the effect of a destructivemechanism. The rise in the erythrocyte counts ofthe patient exceeded somewhat that expected andprobably represents some increase in the rate ofcell release to the circulation.
Erythrocyte levels attributable' entirely to he-molysis. The four patients from whom data arepresented in Figure 6 exhibited observed cellcounts during the steady state of random erythro-cyte destruction which coincided almost exactlywith those expected when computed from the ratesof random destruction of the transfused erythro-cytes. In three of these cases, also, it is assumedthat the rate of random loss of transfused cellsduring therapy indicated the condition prior totreatment. But in Case 8 (Figure 6D) the curveof random cell loss was actually determined for 60days before treatment and the same correspondencebetween observed and expected cell levels was ob-tained. In none of the four cases was there a dis-crepancy which was attributable to maturationarrest.
It is of interest that in Cases 6 (Figure 6A), 5(Figure 6B), and 8 (Figure 6D) the rate oferythrocyte release to the circulation apparentlyaccelerated after the inception of therapy and at-tained approximately twice the normal. In thesix cases studied Case 4 (Figure 6C) was thesingle instance where the rise in the erythrocytecounts was exactly that expected on the assump-
tion of a normal rate of erythrocyte release to thecirculation and cessation of the random destructivemechanism. It may be of significance that this wasthe only case in the series in which the initialerythrocyte counts were as high as 3.5 millionsper mm."
Analysis of the other clinical and laboratorydata (Table I) yields no clue by which to differ-entiate between patients in whom there was evi-dence of maturation arrest and those in whomthere was not. The height of the reticulocytecounts after therapy with B12 seemed to fallwithin the expected range. The serum bilirubinlevels showed no correlation. The presence orabsence of severe disease of the spinal cord wasnot indicative; nor was age, sex, or duration of thedisease. The initial erythrocyte level was notprognostic of the difference.
Validity of interpretations
The methods of indirect mathematical analysiswhich we have employed are, of course, susceptibleto more than one interpretation. For example,we have concluded that maturation arrest in thebone marrow did not affect the erythrocyte levelof the untreated patient when the observed celllevels in the steady state of random destructioncoincided with the level expected on the assump-tion of a normal rate of erythrocyte release to thecirculation. It is possible that there was decreasederythrocyte release to the circulation and the rateof destruction of the patient's own cells was lessthan that of normal adult transfused erythrocyteswhose rate was actually measured. But this seemsimprobable on three counts: (a) In Case 10 theerythrocytes from a patient with pernicious ane-mia were lost at the same rate in a normal subjectas were normal adult cells transfused to the pa-tient, (b) it is hardly to be expected that erythro-cytes formed in a normal donor would be more sus-
The patient in chart 6B showed an observed cell level of 2.00 millions per mm.' before treat-ment, which coincided with the expected level. Treatment was begun 4 days after transfusionand the cell release rate attained a maximum of 1.8 times the normal.
In chart 6C the patient's observed erythrocyte level was the same as the expected one. However,after treatment with B,,, the erythrocyte counts increased at the same rate as expected for normalrate of cell release. It is noteworthy that this is the only patient in the series whose initial redcell count, without treatment, was as high as 3.5 millions per mm.'.
The patient in chart 6D was untreated for 65 days of the study and the observed cell levels wereas expected. During the short time after treatment was begun the rate of cell release attaineddouble the normal.
203

H. E. HAMILTON, E. L. DEGOWIN, R. F. SHEETS, C. D. JANNEY, AND J. A. ELLIS
ceptible to destruction than those formed in amilieu of B12 deficiency, (c) it seems highly un-likely to encounter four out of six cases in whichsuch an equilibrium between an abnormally slowrate of erythrocyte release and destruction wouldexactly coincide with the condition expected un-der the assumption of a normal rate of cell release.
The data presented, however, show a possibleeffect of maturation arrest in that there is no evi-dence that the rate of erythrocyte release, and pre-sumably the rate of cell production, ever acceleratedduring the untreated phase of the disease in re-sponse to the stimulus of the oligocythemia. Thisis in decided contrast to the reaction of the hemato-poietic system in carcinoma and X radiation (9)and in many other types of hemolytic anemia.Apparently B12 deficiency precludes this "accelera-tion response" of the bone marrow beyond per-mitting a normal rate of erythrocyte release.
CONCLUSIONS
1. Normal adult erythrocytes transfused to eightpatients with untreated Addisonian perniciousanemia were destroyed at random, irrespective oftheir ages. After adequate therapy with B12 twoof the patients were retransfused with erythrocytesfrom the same donors and the rate of random losswas zero in one and much less than previously inthe other, excluding the possibility of isosensitiza-tion to antigens in the donor's cells as a cause forthe random destruction.
2. The erythrocytes from a patient with un-treated pernicious anemia were destroyed at ran-dom in the circulation of a normal subject at thesame rate as normal adult erythrocytes transfusedto the patient.
3. The action of the hemolytic mechanism caus-ing random destruction of normal adult erythro-cytes in patients with pernicious anemia was pre-vented by the administration of 15 micrograms ofvitamin B12 daily for 9, but not for 3 days, beforetransfusion.
4. Once normal adult erythrocytes were dam-aged by exposure to the milieu of B12 deficiencyfor only a few hours, subsequent therapy of thepatient-recipient did not reverse the effect. Theadministration of 15 micrograms of B12 daily for23 days to one patient protected normal adult
transfused erythrocytes from random destructionfor only 20 days after cessation of therapy.
5. The experiments suggest a noxious influenceof B12 deficiency on normal adult erythrocytes inthe circulation.
6. In four of six patients with untreated per-nicious anemia the oligocythemia could be entirelyaccounted for by the random destruction of eryth-rocytes, as measured by the loss of normal trans-fused cells in the circulation.
7. In two other patients maturation arrest in thebone marrow could be ascribed as a factor in theoligocythemia. But part of the depressed erythro-cyte level could be attributed to abnormally rapiddestruction of erythrocytes.
8. Five of six patients responded to vitamin B12therapy by acceleration of the rate of erythrocyterelease to the circulation at approximately twicenormal. In contrast, the single patient, with aninitial erythrocyte count of 3.5 millions per mm.",exhibited only a normal rate of erythrocyte re-lease during treatment.
9. During the untrea^ted state of pernicious ane-mia, the milieu of B12 deficiency seems to inhibitacceleration of the rate of erythrocyte release abovethe normal in response to oligocythemia. This isin contrast to many other types of hemolyticanemia.
REFERENCES
1. Ashby, W. J., Study of transfused blood: II. Blooddestruction in pernicious anemia. J. Exper. Med.,1921, 34, 147.
2. Callender, S. T., Loutit, J. F., and Jope, E. M., Dis-cussion on the life and death of the red blood cor-puscle. Proc. Royal Soc. Med., 1946, 39, 755, 757,760.
3. Singer, K., King, J. C., and Robin, S., The life spanof the megalocyte and the hemolytic syndrome ofpernicious anemia. J. Lab. & Clin. Med., 1948, 33,1068.
4. Brown, G. M., Hayward, 0. C., Powell, E. O., andWitts, L. J., The destruction of transfused erythro-cytes in anaemia. J. Path. & Bact., 1944, 56, 81.
5. Mollison, P. L., The survival of transfused erythro-cytes, with special reference to cases of acquiredhaemolytic anaemia. Clin. Sc., 1947, 6, 137.
6. Wearn, J. T., Warren, S., and Ames, O., The lengthof life of transfused erythrocytes in patients withprinary and secondary anemia. Arch. Int. Med.,1922, 29, 527.
204

VI. HEMOLYSIS IN PERNICIOUS ANEMIA
7. DeGowin, E. L., Sheets, R. F., and Hamilton, H. E.,Studies with inagglutinable erythrocyte counts.I. A method for measurement of net gain or deficitof red cells in the human subject. J. Clin. Invest.,1950, 29, 693.
8. Sheets, R. F., Janney, C. D., Hamilton, H. E., andDeGowin, E. L., Studies with inagglutinableerythrocyte counts. III. Kinetics of erythrocytedestruction in human beings. J. Clin. Invest., 1951,30, 1272.
9. Sheets, R. F., Hamilton, H. E., DeGowin, E. L., andJanney, C. D., Studies with inagglutinable eryth-rocyte counts. V. Spontaneous and X-ray-in-duced hemolysis in malignancy. J. Clin. Invest.,1954, 33, 179.
10. DeGowin, E. L., Ellis, J. A., Sheets, R. F., Hamilton,H. E., and Janney, C. D., Studies with inag-glutinable erythrocyte counts. IV. Graphic analysisof rates of production and destruction of humanerythrocytes. J. Clin. Invest., 1954, 33, 163.
205