Simultaneous Occurrence of Developmental Venous Anomalies ... · Simultaneous Occurrence of...
8
Simultaneous Occurrence of Developmental Venous Anomalies and Cavernous Angiomas G. Wilms, E. Bleus, P. Demaerel, G. Marchal, C. Plets , J. Goffin, and A. L. Baert PURPOSE: To stud y the clinical and radiol ogic findings in 15 p at ients presenting with both deve lopmental venous anomalies and cavernous angi omas and to determine which lesions caused the acute clini cal symptoms. METHODS: Les ions were infratentorial in 7 patients and supraten- torial in 7 other patients. In one patient the developmental venous anomaly was infratentor ial and the cavernous angioma supratentorial. In all 15 patients clinical exa min at ion and CT were per- formed . In 10 patients MR was performed at the time of th e initial CT scan. In 5 patients only late MR is available. RESULTS: Acute clinical signs were prese nt in 9 patients (ep ilepsy, hemip legia, meningeal signs, cranial nerve deficit ). On CT the cavernous angioma was missed in 9 patients, in 6 patients because of acute hemorrhage. On MR the cavernous angi oma was missed in 1 of 2 cases with acute hemorrhage but seen in all oth er patient s. On repeat MR all cavernous angiomas were correctly identifi ed. On CT, 11 developmental venous anomalies were seen. On MR all develop- mental venous anomalies were seen. CONCLUSIONS : Th e frequent association of developmental venous anomalies and cavernous angiomas is con firmed. MR is superior to CT in the detection of both cavernous angiomas and developmental venous anomalies. Furth ermore our data support the hypothesis that cavernous angiomas and not th e developmental venous anomalies cause the ac ute clinical symptoms because of hemorrhage. Index terms: Angioma ; Veins, abnormalities and anoma lies; Brain, comput ed tomography; Brain , magneti c resonan ce AJNR Am J Neurora.dio/15: 1247-1254 , Aug 1994 Developmental venous anomalies, the so- called venous angiomas, are diagnosed with in- creasing frequency on computed tomography (CT) and magnetic resonance (MR) (1-4). The lesions are considered normal variants of the venous drainage of the tectum and the white matter (5). Their clinical significance remains controversial, because in a minority of cases hematoma formation is found in the vicinity of the lesion (4, 5). Cavernous angiomas, on the other hand , are true vascular malformations which are much better demonstrated with MR than with CT Rece ived August 3, 1992 ; accepted after revision Apr il 27, 1993. Presented at the 30th annual meeting of the ASNR, May 31-June 5, 1992, St. Louis, Missouri. From the Departments of Radiology (G.W., E.B., P.D., G.M., A.L.B .) and Neurosurgery (C.P., J.G .), University Hospitals K.U. Leuven, Belgium. Address repri nt requests to Prof Dr G. Wilms , Department of Radiology, University Hospitals K.U. Leuven, Herestraat49 , B-3000, Leuven, Belgium. AJNR 15: 1247-1254, Aug 1994 0195 - 6108 / 94/ 1507-1247 © American Society of Neuroradiology (6, 7). Because the lesions produce no angie - graphic changes , they are also designated oc- cult cerebral vascular malformations (7). The association of developmental venous anomalies and cavernous angiomas was first described by Takamiya (8) and was later con - firmed by others (9, 10). It has been suggested that cavernous angiomas and not the venous anomalies cause the clinical symptoms and are a potential source of bleeding (5-9). We wish to report the clinica l, CT, and MR findings in 15 patients with combined venous anomalies and cavernous angiomas , complicated by hemor - rhage in seven cases. We more specifically studied whether the acute clinical symptoms or the hemorrhage was caused by the venous anomaly or the cavernous angioma . Material and Methods In a retrospective study of 65 venous anomalies, asso- ciated cavernous angiomas were found in 15 patients (23%). We reviewed the clinical and radiologic data of 1247
Transcript of Simultaneous Occurrence of Developmental Venous Anomalies ... · Simultaneous Occurrence of...

Simultaneous Occurrence of Developmental Venous Anomalies and Cavernous Angiomas
G. Wilms, E. Bleus, P. Demaerel, G. Marchal , C. Plets, J . Goffin, and A . L. Baert
PURPOSE: To study the clinical and radiologic findings in 15 patients presenting with both
developmental venous anomalies and cavernous angiomas and to determine which lesions caused
the acute clinical symptoms. METHODS: Lesions were infratentorial in 7 patients and supraten
torial in 7 other patients . In one patient the developmental venous anomaly was infratentorial and
the cavernous angioma supratentorial. In all 15 patients clinical examination and CT were per
formed. In 10 patients MR was performed at the time of the initial CT scan. In 5 patients onl y late
MR is available. RESULTS: Acute clinical signs were present in 9 patients (epilepsy, hemiplegia,
meningeal signs, cranial nerve deficit). On CT the cavernous angioma was missed in 9 patients, in
6 patients because of acute hemorrhage. On MR the cavernous angioma was missed in 1 of 2 cases
with acute hemorrhage but seen in all other patients. On repeat MR all cavernous angiomas were
correctly identified . On CT, 11 developmental venous anomalies were seen. On MR all develop
mental venous anomalies were seen. CONCLUSIONS: The frequent association of developmental
venous anomalies and cavernous angiomas is confirmed. MR is superior to CT in the detection of
both cavernous angiomas and developmental venous anomalies. Furthermore our data support the
hypothesis that cavernous angiomas and not the developmental venous anomalies cause the acute
clinical symptoms because of hemorrhage.
Index terms: Angioma ; Veins, abnormalities and anomalies; Brain , computed tomography; Brain ,
magnetic resonance
AJNR Am J Neurora.dio/15: 1247-1254, Aug 1994
Developmental venous anomalies, the socalled venous angiomas, are diagnosed with increasing frequency on computed tomography (CT) and magnetic resonance (MR) (1-4). The lesions are considered normal variants of the venous drainage of the tectum and the white matter (5). Their clinical significance remains controversial, because in a minority of cases hematoma formation is found in the vicinity of the lesion (4, 5).
Cavernous angiomas, on the other hand, are true vascular malformations which are much better demonstrated with MR than with CT
Received August 3, 1992; accepted after revision April 27 , 1993.
Presented at the 30th annual meeting of the ASNR, May 31-June 5,
1992, St. Louis, Missouri.
From the Departments of Rad iology (G.W. , E.B., P.D., G.M., A.L.B.)
and Neurosurgery (C.P., J.G.), University Hospitals K.U . Leuven, Belgium.
Address reprint requests to Prof Dr G. Wilms, Department of Radiology,
University Hospitals K.U. Leuven , Herestraat49 , B-3000, Leuven, Belgium.
AJNR 15:1247-1254, Aug 1994 0195-6108/94/ 1507-1247
© American Society of Neuroradiology
(6, 7). Because the lesions produce no angiegraphic changes, they are also designated occult cerebral vascular malformations (7).
The association of developmental venous anomalies and cavernous angiomas was first described by Takamiya (8) and was later con firmed by others (9 , 10). It has been suggested that cavernous angiomas and not the venous anomalies cause the clinical symptoms and are a potential source of bleeding (5-9). We wish to report the clinica l, CT, and MR findings in 15 patients with combined venous anomalies and cavernous angiomas , complicated by hemorrhage in seven cases. We more specifically studied whether the acute clinical symptoms or the hemorrhage was caused by the venous anomaly or the cavernous angioma .
Material and Methods In a retrospective study of 65 venous anomalies, asso
ciated cavernous angiomas were found in 15 patients (23%) . We reviewed the clinical and radiologic data of
1247

1248 WILMS
these 15 patients. The patient population included 8 m en and 7 women, with a m ean age of 33.4 years. All patients were initially examined with CT; MR was performed for the confirmation of the diagnosis.
In 10 patients CT and MR were performed at the time of the initial symptoms. In 5 other patients initially only CT was performed. These patients all initially were diagnosed as having hemorrhagic developmental venous anomalies (y) . In these 5 and 2 other patients, repeat CT and MR was performed after a m ean of 16 ± 13 months. In 11 patients selective angiography of the internal carotid or vertebral artery was performed.
CT was done with a Somatom CR or Somatom DRH (Siemens, Germany). In all patients plain and contrastenhanced CT scans are available. MR was performed with a 1.5-T superconductive magnet (Magnetom, Siemens, Germ any) . In all patients T2-weighted images (2500/90/1 [repetition time/echo time/excitations]) were obtained. T1 -weighted spin-echo sequences (600/15/1) were performed before and after intravenous injection of gadopentetate dimeglumine (Magnevist, Schering, Germany) or gadopentatate-DOTA (Dotarem, Guerbet , France) at a dose of 0 .1 mmol/ kg. Angiography was performed with high-resolution digital angiography equipment with a 512 or 1024 matrix (Polytron, Siemens, Germany). None of the cases was surgically confirmed.
The CT criteria to make the diagnosis of cavernous angioma were the presence of a lesion with spontaneous high density or calcification, with moderate contrast enhancement. On MR cavernous angioma was diagnosed if a lesion was found with a complex internal structure, appearing as a rounded, multilobulated mass with septations, demarcating areas of varying intensity on both T1-and T2-weighted images and bounded by a low intensity rim that becomes darker on progressively T2-weighted sequences (7). The diagnosis of venous angioma or deve lopmental venous anomaly was made if an area of linear enhancem ent was seen with transcerebral or transcerebellar course possibly with visua lization of peripheral draining veins and mostly showing signal void on plain MR (4) .
Results
In seven patients the developmental venous anomalies and the cavernous angiomas were infratentorial: four lesions were located in the cerebellum, three in the pons. In seven patients the lesions were supratentorial: one occipital , two frontal, and four parietal lesions. In one patient the cavernous angioma was supratentorial in the parietal lobe, and the developmental venous anomaly was infratentorial , located in the cerebellum. In one patient, besides an infratentorial venous anomaly and cavernous angiomas, multiple other supratentorial cavernous angiomas were found. In one of the patients with
AJNR: 15, August 1994
supratentorial lesions , a huge contralateral meningioma was found .
Concerning the clinical symptoms, in six patients there were only nonspecific nonacute clinical signs. For the four infratentorial lesions these consisted of left-sided paresthesias, nystagmus, disturbance of vision, Meniere syndrome, and dizziness . A patient with supratentorial cavernous angioma and developmental venous anomaly reported disturbance of vision and emotional lability. In this patient there was a huge contralateral meningioma. The final patient reported headaches and paresthesias. In nine patients, there were acute clinical signs. In the three patients with infratentorial lesions, symptoms included headache, vomiting, gait disturbance, cranial nerve deficit, dizziness, nausea, and paresthesias. For the five patients with supratentorial lesions, these acute symptoms were epilepsy in two patients, headache and vomiting in two, and acute hemiplegia in one patient. The patient with a supratentorial cavernous angioma and an infratentorial developmental venous anomaly had a grand mal epileptic insult (Fig 1 ).
Concerning the radiologic diagnosis of cavernous angiomas (Table) with CT, on the initial CT scan the lesion was identified in six patients. In five of these patients the lesion had the typical CT characteristics of a cavernous angioma as described above (Fig 2) . In one patient the lesion showed signs of acute hemorrhage, but the presence of focal contrast enhancement allowed the correct diagnosis of an underlying cavernous angioma (Fig 3). In the remaining nine patients the cavernous angioma was not identified, in six because of acute hemorrhage obscuring the underlying cavernous angioma (Fig 4). Three small lesions were not seen on CT, because of either lack of calcification or enhancement or partial volume effects (Fig 5). On the repeat CT after resolution of the hematoma, four of the six lesions obscured by hemorrhage became visible on CT. The two other lesions remained equivocal.
At the time of the initial CT, MR was performed in 10 of these patients (see Table). The cavernous angioma was identified in 9 of the 10 cases, 1 of which was hemorrhagic. In this particular case, the underlying cavernous angioma was missed with CT. In 1 case the cavernous angioma was obscured by hemorrhage. In this particular case , on a repeat MR a few months later the cavernous angioma was correctly

AJNR: 15, August 1994
identified. In the remammg 5 patients, in whom the MR was not performed at the time of the initial CT, the cavernous angioma was correctly identified on MR performed later. In 1 patient, besides the cavernous angiomas in the direct vicinity of the developmental venous anomaly in the posterior fossa, 3 other supratentorial cavernous angiomas were present. Angiography, performed in 11 cases, only showed signs of mass effect caused by acute hematomas. None of the cavernous angiomas showed any particular angiographic finding.
Concerning the radiologic diagnosis of developmental venous anomaly on CT, the lesion was demonstrated in 11 patients. In 4 patients the lesion was missed because of obscuring hemorrhage. In all of these patients, the lesion was visible on repeat CT after resorption of a hematoma. On MR all developmental venous
Cavernous angioma: CT and MR diagnosis
Case Initial CT Late CT Initial MR Late MR
1 ID ID 2 OH ID ID 3 M ID 4 M ID 5 OH ID ID 6 OH M ID 7 OH M ID 8 ID ID ID 9 OH ID OH ID
10 ID ID ID ]] OH ID CA + H ID 12 M M ID 13 CA + H CA + H ID 14 ID ID 15 ID ID
Note.-ID indicates identified; M, missed; OH, obscured by hem-orrhage; CA + H, cavernous angioma and hemorrhage.
VENOUS ANOMALIES 1249
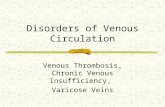
Fig 1. lnfratentorial developmental venous anom aly and supratentorial ca vernous angiom a (case 8) .
A, Plain Tl -weighted transverse image (600/1 5/l [repetition time/ echo time/ excitations]). Typica l cavernous angiom a in right ro landic reg ion. Notice heterotopic gray m atter in the neighborhood of the lesion .
B, Gadolinium-enhanced transverse MR image. Right cerebellar developmental venous anomaly.
anomalies were demonstrated. On angiography, performed in 11 patients, all the developmental venous anomalies were visualized with a typical umbrella shape. In 2 patients the devel opmental venous anomalies showed stenosis at the junction with the dural venous sinuses.
Discussion
Cerebral cavernous angiomas, or cavernomas, histologically are composed of large sinusoidal vascular spaces without intervening normal brain parenchyma (13) . They have a propensity for recurrent hemorrhage, but the bleeding is usually subclinical (6, 7, 12, 13). Because they are not seen on angiography, they are also called occult or cryptic arteriovenous malformations. On CT they are diagnosed by the presence of calcifications, cysts , or enhancement (8) . Because of the presence of hemorrhages of different ages, they are superbly demonstrated by MR (8). The reported cases of cavernous angiomas are mostly symptomatic. Seizures and neurologic symptoms related to the sudden or insidious enlargement of these lesions are the most common symptoms (6 , 7 , 9 , 12, 13). The risk for symptomatic acute hemorrhage could be as high as 29% (13).
Developmental venous anomalies , or the socalled venous angiomas, are composed neuropathologically of dilated medullary veins , located in the white matter and converging towards a central dilated draining vein ( 11) . They are easily identified on CT ( 1, 4) , but MR is superior in the demonstration of the medullary veins and the type of venous drainage (2-4, 14). The angiographic image typically demon-

1250 WILMS AJNR: 15, August 1994
A B c Fig 2. Typical combined cavernous angioma and developmental venous anomaly
(case 14) . A , Pla in CT. Right frontal paramedian , slightly calcified lesion. 8 , Contrast-enhanced CT. The cavernous angioma shows moderate contrast en
hancement. Notice strongly enhancing collector vein of developmental venous anomaly (arrow).
C. Transverse T2-weighted MR image (2500/90/1 ). Cavernous angioma demonstrates mixed intensities; developmental venous anomaly is seen by signal void.
D, Coronal gadolinium-enhanced Tl -weighted image. Cavernous angioma is strongly hyperintense; developmental venous anomaly is well shown, with better demonstration of medullary veins.
strates a radiating collection of medullary veins, draining centrally into a longer draining vein and terminating in a superficial cortical vein or a dural vein ( 1, 5). The clinical significance of developmental venous anomalies is controversial. Although most lesions are asymptomatic, they can appear with a variety of clinical symptoms, such as headache, vertigo, dizziness, tinnitus, dyplopia, nystagmus, and ataxia for the infratentorial lesions, and seizures and headaches as the most frequent symptoms of the supratentorial lesions ( 1-5). Because the correlation between the symptoms and the lesions is weak, they now are considered normal developmental variants of the cerebral venous drainage.
Several authors reported the association of developmental venous anomalies and cavernous venous anomalies (6, 8-10) . This frequent association was present in 23% of our cases of venous angioma. In most series the clinical
D
symptoms are attributed to the cavernous angiomas, either by direct compression or by hemorrhage (9, 10). In our series hemorrhagic complications were noted in 7 of the 15 patients and in 7 of 9 patients with acute clinical symptoms. In these patients with hemorrhage, on CT the venous angioma was always clearly identified as a separate lesion and was located a certain distance from the hematoma. In one of the seven hemorrhagic lesions (case 13), the cavernous angioma was recognized within the area of acute hemorrhage as a focus of contrast enhancement. In another patient (case 11), MR could show the cavernous angioma immediately adjacent to the hemorrhage, whereas the venous angioma was at a distance. In the five other cases, on late CT or MR it was obvious that the hemorrhage had occurred at the site where later the cavernous angioma was found, at a distance from the developmental venous anomaly. Therefore we concluded that the hem-

AJNR: 15, August 1994
A B
c D
orrhage was caused by the cavernous angioma and not the developmental venous anomaly. For the patients with nonacute symptoms, it is difficult to evaluate which lesion is responsible for the symptoms, considering the vicinity of the developmental venous anomalies and the cavernous angiomas. Unlike in other series, in ours there were no clinical symptoms related to the mass effect of brain stem or hemispheric cavernomas. It is known that MR is superior to CT in the demonstration of both developmental venous anomalies and cavernous angiomas ( 4 , 6) . This is confirmed in our series: seven cavernous angiomas were obscured by hemorrhage. After resolution of the hemorrhage, the CT findings remained equivocal in 3 patients, probably because of insufficient calcification of the lesion. Here it has to be stressed that MR was able to show a cavernous angiomas within a large subacute hematoma. In 3 patients small lesions were missed on CT because of partial volume effects, lack of calcification, or insuffi cient enhancement. For the diagnosis of the
VENOUS ANOMALIES 1251
Fig 3. Hem orrhag ic cavernous angioma and developmental venous anomaly (case 13).
A, Plain CT. Right cerebellar hematom a. B, Contrast-enhanced CT. Contrast en
hancement is evident within cavernous angiomas; Collector vein (arrow) of developmental venous anomalies (y) is well shown.
C, Frontal T1-weighted MR image (600/ 15/1) performed 9 m onths later. Cavernous
' angioma is strongly hyperintense. Hemosiderin is present as a rim around the lesion. Streaks in the right cerebellar hemisphere probably represent portions of the venous angioma.
D, Gadolinium-enhanced MR, sam e level. Strong enhancement of developmenta l venous anomaly (arrow).
developmental venous anomalies, adjacent hemorrhage was responsible for the four falsenegative results on CT, whereas MR was positive in all cases.
Recently Dillon et al (Dillon WP, Wilson CB, Hieshima GB, Rosenau W, Hemorrhagic Venous Malformations: The Role of Venous Restriction , presented at the 30th annual meeting of the ASNR, St. Louis , June 1992) found stenosis of the collector vein in 13 of 16 patients with angiographically demonstrated developmental venous anomalies , in a series of 27 patients with occult cryptic vascular malformations or acute hemorrhage in close association with venous malformations. They hypothesize that an elevated pressure within the venous malformation results in hemorrhage, leading to the development of cavernomas. This hypothesis was sustained by direct intraoperative venous pressure measurements, documenting a 15-mm pressure gradient across the venous stenosis. In our opinion this hypothesis is very attractive. We carefully examined all the possible argu-

1252 WILMS AJNR: 15, August 1994
A 8 c Fig 4 . A cute hemorrhage within cavernous angioma (case 11) . A, Plain CT. Right frontal hemorrhage with the appearance of multiple bleeds of
different ages into the lesion with a central subacute part. B, Sagittal T2-weighted MR image (2500/ 90/ 1 [repetition time/ echo time/ excita
tions]) . Cavernous angioma (arrow) is identified superior to subacute hemorrhage. C, Sagittal Tl -weighted MR image (60/1 5/1 ). Same observations . A rrow points to
cavernous angioma . D, Sagittal T1-weighted MR image, 10 m onths later. Cavernous angioma is seen at
sam e site. Hemorrhage is no longer visible. Note: venous angioma was present on other sections (not illustrated) .
ments against this theory but were unable to contradict it. A first objection against this hypothesis could be that in most patients there are no signs of acute hemorrhage in the medical history. This argument is easily contradicted because it is known that hemorrhage within cavernous angiomas is not always clinically relevant (9 , 12, 13). Moreover, the authors examined a patient with a craniopharyngioma who had a fortuitous finding of a developmental venous anomaly in the left basal ganglia. One year later, without apparent clinical signs, a repeat MR demonstrated a cavernous angioma next to the known developmental venous anomaly. Second, it is obvious that not all hemorrhagic developmental venous anomalies have stenoses near their site of drainage. Here it must be underlined that the stenoses in their series are found in a majority of the cases on routine angiograms. If additional oblique views would be performed, one might expect to find stenoses in an even higher percentage of cases. Third, it is obvious that not every cavernous angioma
is accompanied by a developmental venous anomaly. In these cases it is logical to suggest that the cavernous angioma itself is at the base of a possible hemorrhage. Nevertheless, it is also possible that the developmental venous anomaly could thrombose after hemorrhage and become invisible on MR. A final argument is that in 1 of our 2 patients with a clinically evident acute hemorrhage in the neighborhood of a developmental venous anomaly, a cavernous angioma could be identified within the acute bleeding. Of course this does not exclude that an earlier smaller hemorrhage could have been clinically silent.
In conclusion we can confirm the frequent association of developmental venous anomalies and cavernous angiomas. Our study demonstrates that MR is superior to CT in the detection of both developmental venous anomalies and cavernous angiomas in the acute as well as in the chronic phase. Furthermore our data support the hypothesis that the cavernous angioma and not the developmental venous anomaly is

AJNR: 15, August 1994
Fig 5. Cavernous angioma, missed with CT (case 4) . A, Plain CT. No lesion visible, especially on the midline.
E
VENOUS ANOMALIES 1253
8, Contrast-enhanced CT. Enhancing draining vein (arrow) of developmental venous anomaly. C. T2-weighted (2500/9/1 [repetition time/echo time/excitations]) transverse image, same level. Midline cavernous angioma seen at
the floor of the fourth ventricle (arrow) . Draining vein of cavernous angiomas is seen as a hyperintense structure (arrowheads). D, Sagittal T1-weighted image on the midlinE' (600/15/1 ). Small midline cavernous angioma. E, Gadolinium-enhanced image, same level. Dem onstration of part of venous angioma (arrowheads).
the cause of the acute clinical symptoms, most frequently because of hemorrhage. Finally we could not find any solid argument to contradict the hypothesis of Dillon et al that stenosis within the developmental venous anomaly results in hemorrhage, leading to the development of cavernous angioma .
References
1. Valavanis A, Wellaver J, Yasargil MG. The radiological diagnosis of cerebral venous angioma: cerebral angiography and computed tomography. Neuroradiology 1982;24: 193-199
2. Augustijn GT, Scott JA, Olson E, Gilmor RL, Edwards MK. Cerebral venous angiomas: MR imaging. Radiology 1985;156:391-395
3. Cammarata C, Han JS, Haaga JR, Alfidi RJA, Kaufman B. Cerebral venous angiomas imaged by MR. Radiology 1985; 155:639-643
4 . Wilms G, Marchal G, Van Heeke P, Van fraeyenhoven L, Decrop E, Baert AL. Cerebral venous angiomas. Neuroradiology 1990;32: 81-85
5. Lasjaunias P, Burrows P, Plante Chantal. Developmental venous anomalies (DVA): the so-called venous angioma. Neurosurg Rev 1986;9:233-244
6. Gomori JM, Grossman Rl , Goldberg HI, Hackney DB, Zimmerman RA, Bilaniuk LT. Occult cerebral vascular malformations: highfield MR imaging. Radiology 1986;158:707-713
7. Rapacki TFX, Brantley MJ, Furlow TW, Geyer CA, Toro VE, George ED. Heterogeneity of cerebral cavernous hemangiomas diagnosed by MR imaging. J Comput Assist Tomogr 1990;14: 18-25

1254 WILMS
8. Takamiya Y, Takayama H, Kobayashi K, Mine T, Suzuki K. Familiar occurrence of multiple vascular malformations of the brain. Neuro/ Med Chir (Tokyo) 1984;24:271-277
9. Goulao A, Alvarez H, Monaco RG , Pruvost P, Lasjaunias P. Venous anomalies and abnormalities of the posterior fossa. Neuroradiology 1990;31 :476-482
10. Rigamonti D, Spetzler RF. The association of venous and cavernous malformations: report of four cases and discussion of the pathophysiological , diagnostic, and therapeutic implications. A cta Neurochir 1988;92:100-105
11. McCormick WF. The pathology of vascular (arteriovenous) malformations. J Neurosurg 1966;24:807-816
AJNR: 15, August 1994
12. Voigt K , Yasargil MG. Cerebral cavernous hemangiomas or cavernomas: incidence, pathology, localization, diagnosis, clinical features and treatment: review of the literature and report of an unusual case. Neurochirurgia 1976; 19:59-68
13. Simard JM, Garci-Bengocheat F, Ballinger WE, Mickle JM, Quisling RC. Cavernous angioma: a review of 126 collected and 12 new clinical cases. Neurosurgery 1986; 18:162-172
14. Wilms G, Marchal G, Baert AL, Plets C. Gadolinium-enhanced MR imaging of cerebral venous angiomas with emphasis on their
drainage. J Comput Assist Tomogr 1991 ;15:199-206
Please see the commentary on page 1255 in this issue.