Simulation of acute myopericarditis by constrictive pericardial disease … · 2017. 1. 31. ·...
4
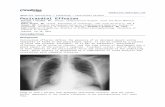
196 JACC Vol. 4. No. I July 1984:I%-9 Simulation of Acute Myopericarditis by Constrictive Pericardial Disease With Endomyocardial Fibrosis Due to Methysergide Therapy A. DANIEL HARBIN, MD,* MYRON C. GERSON, MD, FACC,*t JOHN B. O'CONNELL, MD, FACe!: Cincinnati, Ohio and Maywood, Illinois Methysergide (Sansert) has been associated with nu- merous fibrotic disorders. In particular, multiple car- diac lesions have been described in cases where methy- sergide was thought to have played a causative role. A patient is described who presented with cardiac findings suggestive of acute myopericarditis. An inflammatory myocarditis was subsequently excluded by endomyocar- Methysergide (Sansert) is an analog and antagonist of se- rotonin that has been used widely during more than two decades for the prophylaxis of migraine or cluster head- aches. Although methysergide may be the most effective agent available for prophylaxis against certain types of dis- abling headaches, its use has been marred by adverse effects in some patients. A small percent of patients using methy- sergide develop fibrotic disorders that may become life- threatening. Retroperitoneal fibrosis was initially recognized in 1961 (1), but methysergide-associated fibrotic processes in the cardiovascular system have included valvular fibrosis leading to aortic, mitral or tricuspid regurgitation (1-10), constrictive pericardial disease (11-13), cotonary artery dis- ease (1,3,5,14) and myocardial fibrosis (5,6,15). We report on a patient whose initial presentation mimicked acute viral myopericarditis, but who was later shown to have evidence of both endomyocardial fibrosis and pericardial disease as complications of methysergide therapy. Case Report Initial presentation. A 61 year old white male executive was in excellent health until December 1982, when he noted the onset of fatigue, night sweats, anorexia and occasional From the Division of Cardiology. Department of Internal Medicine, * and the E. L. Saenger Radioisotope Laboratory, Department of Radiol- ogy,t University of Cincinnati Medical Center, Cincinnati, Ohio, and the Division of Cardiology, Department of Internal Medicine.t Loyola Uni- versity School of Medicine, Maywood, Illinois. Manuscript received Oc- tober 4, 1983; revised manuscript received December 20. 1983, accepted December 28, 1983. Address for reprints: Myron C. Gerson, MD, University of Cincinnati, Division of Cardiology, Mail Location #542, Cincinnati, Ohio 45267. © 1984 by the American College of Cardiology dial biopsy. Hemodynamic findings suggested the pres- ence of constrictive pericarditis or restrictive cardio- myopathy, or both. Radiographic evidence of constrictive pericarditis and biopsy evidence of endocardial fibrosis were documented in this patient with a long history of interrupted methysergide therapy. chest pains. One month later while attending a business convention in the Virgin Islands, he required hospitalization for increasing chest pain accompanied by exertional dyspnea and pedal edema. In the hospital a pericardial friction rub was heard, and pedal edema, pulmonary rales and hepa- tomegaly were noted. Acute myocardial infarction was ex- cluded by serial measurement of cardiac serum enzymes and serial electrocardiograms. After symptomatic improvement with digoxin and diuretic drug therapy (furosemide), the patient returned home. Later evaluation. On the day of his return home, the patient presented for the first time to the University of Cin- cinnati Medical Center and was admitted for further eval- uation. On examination, bilateral rales, pedal edema and a pericardial friction rub were present. There was no abnormal jugular venous distension or cardiac gallop rhythm. The oral body temperature was 100°F (37.7°C). There was a history of renal calculi, and a past intravenous pyelogram suggested minor deviation in the course of the right ureter. Results of a treadmill exercise test performed I year earlier as part of an executive physical examination were normal. The only medication at the time of admission was methysergide, 2 mg twice daily, which the patient had taken for prophylaxis of vascular headaches for 10 years. The methysergide had been discontinued for a 2 week period every 6 months. There was roentgenographic evidence of bilateral pleural effusion with an enlarged cardiac silhouette. The electro- cardiogram revealed persistently inverted T waves in leads II, III and aVF, in association with intermittently inverted T waves in all precordial leads. There was echocardio- graphic evidence of pericardial effusion and mild left atrial dilation (5.0 ern) without evidence of other abnormalities. 0735-1097/84/$3.00
Transcript of Simulation of acute myopericarditis by constrictive pericardial disease … · 2017. 1. 31. ·...

196 JACC Vol. 4. No. IJuly 1984:I%-9
Simulation of Acute Myopericarditis by Constrictive PericardialDisease With Endomyocardial Fibrosis Due to Methysergide Therapy
A. DANIEL HARBIN, MD,* MYRON C. GERSON, MD, FACC,*t JOHN B. O'CONNELL, MD, FACe!:
Cincinnati, Ohio and Maywood, Illinois
Methysergide (Sansert) has been associated with numerous fibrotic disorders. In particular, multiple cardiac lesions have been described in cases where methysergide was thought to have played a causative role. Apatient is described who presented with cardiac findingssuggestive of acute myopericarditis. An inflammatorymyocarditis was subsequently excluded by endomyocar-
Methysergide (Sansert) is an analog and antagonist of serotonin that has been used widely during more than twodecades for the prophylaxis of migraine or cluster headaches. Although methysergide may be the most effectiveagent available for prophylaxis against certain types of disabling headaches, its use has been marred by adverse effectsin some patients. A small percent of patients using methysergide develop fibrotic disorders that may become lifethreatening. Retroperitoneal fibrosis was initially recognizedin 1961 (1), but methysergide-associated fibrotic processesin the cardiovascular system have included valvular fibrosisleading to aortic, mitral or tricuspid regurgitation (1-10),constrictive pericardial disease (11-13), cotonary artery disease (1,3,5,14) and myocardial fibrosis (5,6,15). We reporton a patient whose initial presentation mimicked acute viralmyopericarditis, but who was later shown to have evidenceof both endomyocardial fibrosis and pericardial disease ascomplications of methysergide therapy.
Case ReportInitial presentation. A 61 year old white male executive
was in excellent health until December 1982, when he notedthe onset of fatigue, night sweats, anorexia and occasional
From the Division of Cardiology. Department of Internal Medicine,*and the E. L. Saenger Radioisotope Laboratory, Department of Radiology,t University of Cincinnati Medical Center, Cincinnati, Ohio, and theDivision of Cardiology, Department of Internal Medicine.t Loyola University School of Medicine, Maywood, Illinois. Manuscript received October 4, 1983; revised manuscript received December 20. 1983, acceptedDecember 28, 1983.
Address for reprints: Myron C. Gerson, MD, University of Cincinnati,Division of Cardiology, Mail Location #542, Cincinnati, Ohio 45267.
© 1984 by the American College of Cardiology
dial biopsy. Hemodynamic findings suggested the presence of constrictive pericarditis or restrictive cardiomyopathy, or both. Radiographic evidence of constrictivepericarditis and biopsy evidence of endocardial fibrosiswere documented in this patient with a long history ofinterrupted methysergide therapy.
chest pains. One month later while attending a businessconvention in the Virgin Islands, he required hospitalizationfor increasing chest pain accompanied by exertional dyspneaand pedal edema. In the hospital a pericardial friction rubwas heard, and pedal edema, pulmonary rales and hepatomegaly were noted. Acute myocardial infarction was excluded by serial measurement of cardiac serum enzymes andserial electrocardiograms. After symptomatic improvementwith digoxin and diuretic drug therapy (furosemide), thepatient returned home.
Later evaluation. On the day of his return home, thepatient presented for the first time to the University of Cincinnati Medical Center and was admitted for further evaluation. On examination, bilateral rales, pedal edema and apericardial friction rub were present. There was no abnormaljugular venous distension or cardiac gallop rhythm. The oralbody temperature was 100°F (37.7°C). There was a historyof renal calculi, and a past intravenous pyelogram suggestedminor deviation in the course of the right ureter. Results ofa treadmill exercise test performed I year earlier as part ofan executive physical examination were normal. The onlymedication at the time of admission was methysergide, 2mg twice daily, which the patient had taken for prophylaxisof vascular headaches for 10 years. The methysergide hadbeen discontinued for a 2 week period every 6 months.
There was roentgenographic evidence of bilateral pleuraleffusion with an enlarged cardiac silhouette. The electrocardiogram revealed persistently inverted T waves in leadsII, III and aVF, in association with intermittently invertedT waves in all precordial leads. There was echocardiographic evidence of pericardial effusion and mild left atrialdilation (5.0 ern) without evidence of other abnormalities.
0735-1097/84/$3.00

JACC V, J 4. No. IJuly 198'-:196- 9
HARBIN ET AL.COMPLICATIONS OF METHYSERGlDE THERAPY
197
M ,
E\
• J
Figure I. Photomicrographs of endomyocardial biopsy specimen .Hematoxylin-eosin stain at 4 x original magnification (left), andelastic tissue stain at 10x original magnification (right). Theendocard ium (E) demonstrates fibrosis and thickening , while themyocardium (M) is normal. The white arrow shows elastic tissue.
A radionuclide-determined left ventricular ejection fractionwas OA8 with generalized mild left ventricular hypokinesia.The erythrocyte sedimentation rate was 82 mm in I hour.Antinuclear, antimitochondrial , antismooth muscle, antiparietal cell and antithyroid antibodies were absent. Thethird component of complement C3 was slightly elevated at220 (normal 83 to 177) with a normal C4 and total hemolyticcomplement (CH lOo) . Double and single-stranded deoxyribonucleic acid (DNA) binding, antiDNAase-B and antistreptolysin 0 were normal. Serologic titers for Histoplasmacapsulatum and Coxsackie B virus were less than 1:8 dilutions. An indium-Ill white blood cell scan was negativefor evidence of myocardial inflammation.
Methysergide therapy was discontinued on admission .After I week the patient was discharged receiving no medication except for aspirin, which controlled his headaches .One week later , a repeat blood pool radionuclide scan demonstrated a decrease in the left ventricular ejection fractionto 0.40.
Clinical deterioration. Within I week after hospital discharge , exertional dyspnea and pedal edema returned andfurosemide therapy was resumed . A repeat left ventricularejection fraction determination I week later demonstrated afurther decrease to 0.33. With the documentation of progression in left ventricular dysfunction in the setting of arecent illness suggestive of a viral infection , the patient wasreferred to Loyola University Medical Center for endomyocardial biopsy with a presumptive diagnosis of acutemyopericarditis.
At the time ofendomyocardial biopsy , hemodynamic determinations were found to be supportive of constrictive orrestrictive physiology. Blood pressure values (nun Hg) were:
Figure 2. Computed tomogram of the chest demonstrates marked pericardial thickening (white arrows) .

198 HARBIN ET AL.COMPLICATIONS OF METHYSERGlD E THERAPY
JACC Vol. 4. No. 1July 1984:1% - 9
Figure 3. Simultaneous recording of leftventricular (LV) and right ventricular (RV)pressures. Diastolic pressure equalization inthese chambers is demonstrated, in additionto the dip-plateau pattern characteristic of restrictive or constrictive hemodynamics.
mean right atrial 15, right ventricular end-diastolic 18, pulmonary artery 28/18 , mean pulmonary capillary wedge 17,and left ventricular end-diastolic 18. After intravenous infusion of 500 cc of normal saline solution over a 20 minuteperiod , the right atrial pressure was 17 and the pulmonarycapillary wedge pressure was 19.
Six endomyocardial biopsy specimens were obtained fromthe right ventricle and demon strated marked endocardialfibrosis (Fig. 1) . Minimal elastosis was seen with elastictissue staining. No histologic evidence for myocardial inflammation was found . Myocardial cultures were negativefor virus. Computed tomograph y of the chest was performedand a markedly thickened pericardium (maximal width 0 .55
ern) was documented (Fig. 2). A gallium-76 scan of theheart was negative for evidence of myocardial inflammation .
Repeat hemodynamic evaluation. While the patient wasnot receiving methysergide , his headaches remained mildand were easily controlled with aspirin. Two months afterhis initial hospitalization , he began to note progressive exertional chest pain . Coronary angiography demonstratednormal coronary arteries . Repeat hemodynamic determinations suggested possible improvement in the previouslyobserved constrictive/restricti ve hemodynamics (Fig. 3).Pressures (mm Hg) were as follows: mean right atrial 10,right ventricular 24/12 , pulmonary artery 24/12; pulmonarycapillary wedge 12 and left ventricular end-diastolic 12.
Figure 4. Computed tomogram of thechest obtained 5 months after discontinuation of methysergide. In comparison with the earlier study (Fig. 2),decreased pericardial thickness isdemonstrated.

JACC YO'. 4, No.1July 1984 196- 9
HARBI N ET AL.COMPLICATIONS OF METIIYSERGIDE THERAPY
199
Thermodilution cardiac output was 4.54 liters/min. Afterintravenous infusion of 500 cc of normal saline solutionover 20 minutes, the mean right atrial pressure increased toII , right ventricular end-diastolic pressure to 15, pulmonaryartery diastolic pressure to 14 and left ventricular end-diastolic pressure to 15.
Subsequent clinical course. Currentl y, the patient hasreturned to full employment without cardiac symptoms ondiuretic drug therapy (furosemide, 40 mg daily). He hasbeen advised not to resume methysergide use. A follow-up ,radionuclide ventriculogram at rest demonstrated an increasein the left ventricular ejection fraction to 0.44. Computedtomography of the chest repeated 5 months after discontinuation of methysergide demonstrated a decrease in thepericardial thickness, with a maximal width of 0.30 em(Fig. 4) .
Discussion
Previous reports. Fibrotic disorders in association withmethysergide therapy have long been recognized . Pathologic demonstration of the fibrotic cardiac process was reported in 1966 (I ). A 36 year old woman recei ving longterm methysergide therapy developed significant aortic insufficiency and sustained a myocardial infarction. After aortic valve replacement, the excised tissue demonstrated athickened and fibrotic ring involving the root of the aortaand the left coronary artery orifice, with fibrosis lining theaortic valve leaflets (l,3). Subsequent histopathologic studies (3,5,9) have confirmed that in methysergide-related cardiac involvement, as in the carcinoid syndrome, the cardiacvalve structure itself is not significantly affected. There isan orderly deposition of overlying fibrous tissue on the cardiac valve.
In addition to cardiac valvular lesions, pericardial involvement (I 1-13), including a case with constrictive hemodynamics (13), has been documented. A difference betweenour pat lent and the patient described by Orlando et al. (13)is that our patient was complying with a regimen of interrupted methysergide therapy. Furthermore, our patient demonstrated radiographic evidence of regression of pericardialthicken ing along with some objective hemodynamic evidence of improvement on discontinuation of methysergide ,whereas the patient of Orlando et al. required pericardiectomy.
Myocardialfibrosis in association with methysergide usehas also been documented by right ventricular endomyocardial biopsy (6) and autops y (15). The patient of Masonet a!. (til represents the only other reported case of cardiaccompli cations in association with appropriately interruptedrnethysergide therapy. No suggestion of pericardial diseasewas reported in the patient of Mason et al. (6).
Myopericarditis simulation. Our patient represents aunique and interesting case because his initial clinical pre-
sentation was suggestive of an acute viral myopericarditis .Endomyocardial biopsy was helpful in excluding an inflammatory myocardial process and confirming the presence ofendom yocardial fibrosis apparently related to chronic interrupted methysergide therap y. The computed tomograms ofthe chest demonstrated pericardial thickening. In associationwith the hemodynamic abnormalities described, the findingssupport a diagnosis of constrictive pericardial disease , although restrictive physiology is not excluded. Both pericardial and endomyocardial fibrosis were documented-twoknown compl ications of methysergide therapy that have notpreviously been reported in the same patient.
Implications. Patients using methysergide, even on aninterrupted program, should be closely observed by theirphysicians for signs of cardiac disease. A patient with chroniccomplications of methysergide therapy , such as pericardialand endomyocardial fibrosis, can have an initial clinicalpresentation that may mimic unrelated acute disease andotherwise delay correct diagnosis.
ReferencesI . Graham JR, Suby HI, LeCompte PR, Sadowsky NL. Fibrotic disorders
associated with methysergide therapy for headache . N Engl J Med1966;274:359-68.
2. Parnes LR, Graham JR . Possible cardiac and renovascular complications of Sansert therapy. In: Headache Rounds No. 36. Boston:Headache Research Foundat ion . 1965:5.
3. Graham JR. Cardiac and pulmonary fibrosis during methysergide therapy for headache . Trans Am Clin Climatol Assoc 1967;78:79-92.
4. Slugg PH, Kunkel RS. Complications of methysergide therapy: retroperitoneal fibrosis , mitral regurgitat ion . edema and hemolytic anemia. JAMA 1970;213:297-8 .
5. Graham JR. Cardiac and pulmonary fibrosis during methysergide therapy for headache. Am J Med Sci 1967;254:1-12.
6 . Mason JW, Billingham ME. Friedman JP . Methysergide-induced heartdisease: a case of multivalvular and myocardial fibrosis. Circulat ion1977 :56:889-90.
7. Salner AL, Mullany LD, Cole SR. Methysergide induced mitral valvular insufficiency. Conn Med 1980;44:6-8.
8. Munroe OS, Allen P. Cox AR. Mitral regurgitation occurring duringmethysergide (Sansert) therapy. Can Med Assoc J 1969;101:62-5 .
9. Misch KA. Development of heart valve lesions during methysergidetherapy. Br Med J 1974;2:365-6.
10. Barrillon A. Baragan J . Methysergide and tricuspid valve lesions (letter). Circulation 1978;58:578.
II . Greenberg BH, Suros J, Nunn SL. McGoon DC. Partial pericardialdefect with constrictive pericarditis . Chest 1970;57:383-6.
12. Meeran MK, Ahmed AH , Parsons FM, Anderson CK . Constrictivepericarditis due to methysergide therapy. S Afr Med J 1976;50:1595-7.
13. Orlando RC, Moyer P, Barnell TB . Methysergide therapy and constrictive pericarditis. Ann Intern Med 1978;88:213-4 .
14. Hudgson P, Foster lB, Walton IN . Methysergide and corona ry arterydisease . Am Heart J 1967;74:854-5 .
15. Bana OS, MacNeal PS. LeCompte PM, Shah Y, Graham JR. Cardiacmurmurs and endocardial fibrosis assoc iated with methysergide therapy. Am Heart J 1974;88:640-55 .