Silicone oiL emulsification in the anterior chamber after vitreoretinal ... · Silicone oiL...
4
Optometty (2006) 77, 446-449 Literatur-Nr.: 16 Standort: SIL- Ordner II Silicone oiL emulsification in the anterior chamber after vitreoretinal surgery Dennis J. Light, 0.0. Department of Veterans Affairs, Eastern Colorado Health Care System Eye Clinic, Pueblo, Colorado . • KEYWORDS Silicone oil; Endotamponade; Retinal detachmen~; Keratopathy; Glaucoma; Cataract Abstract BACKGROUND: The use of &iliconeoil as an endotamponade for the treatment of complicated retinaI detachment is common, hut lang-term complications can oceur if the oil is not removed later. This artic1e documents a case of emulsified silicone oil migration into the anterior chamber after vitreoretinaI surgery and provides a diseussion and review of comrnon anterior segment eomplieations trom this condition. CASE REPORT: A 59-year-old man reported to the eye clinic complaining of a "growth •• over bis right eye that had increased in size over the last month. Stit tamp examination found a "reverse pseudohy- popyon" iri the right eye, which was actuaIly emutsified silicone oil that had migrated from the posterior ehamber after a previous retinal detachrnent repair. Tbe patient was referred for surgical removal of this oily obstruetion. Although surgical treatment was delayed for 18 months, his vision improved and bis intraocular pressure was lowered through surgieal and medical management. CONCLUSIONS: The use of silicone oil as an endotamponade in cases of complex retina! detachment has become common, but it also may lead to postoperative complications if it is not surgically removed Iater. This case highlights possible complications from the migration of emuIsified silicone oil into the anterior chamber and illustrates the importance of follow-up care for every ophthalmie surgical procedure. Optometry 2006;77:446-449 The use of silicone oil in complex vitreoretinal surgery was first introduced in 1962.1 Its injection into the vitreous cavity.to serve as an endotamponade has become a standard technique and, when combined with vitreoretinal surgery, has been used sÜccessfully in the repair of proliferative vitreoretinopathy, prolifera,tive diabetic retinopathy, giant retinal tears, and ocular trauma. 2. Silicone oll has been known to emu1sify and migrate into various locations within the globe.3 Because this can lead to long-term cornplica- tions, such as cornea! decompensation, cataract, and glau- Correspondingauthor: Dennis J. Light, O.D., Departmentof Veterans Affairs,Eastern Colorado Henlth Care SystemEye Clinic, 4112 Outlook B1vd.,Pueblo, Colorado 81008. E-mail: [email protected] coma, it should be removed after adequate duration of endotamponade.4 (ase report A 59-year-old man reported to the eye clinic complaining of a "growth" over bis right eye that had increased in size over the last month according to his wife's observation. He denied any asthenopia but reported that he "had very little vision" in this eye and that Hit might have gotten a little worse:' His medical history included a '3S-year history of type 2 diabetes mellitus for which he had taken insulin for the last 15 years. His last Ale hemoglobin test, a measure of the 1529-1839/06/$ -see front matter © 2006 American Optometrie Association All rights reserved. doi:lO.l 016/j.optm.2006.04.l19
Transcript of Silicone oiL emulsification in the anterior chamber after vitreoretinal ... · Silicone oiL...

Optometty (2006) 77, 446-449
Literatur-Nr.: 16
Standort: SILOrdner II
Silicone oiL emulsification in the anterior chamber after
vitreoretinal surgery
Dennis J. Light, 0.0.
Department of Veterans Affairs, Eastern Colorado Health Care System Eye Clinic, Pueblo, Colorado .•
KEYWORDS
Silicone oil;
Endotamponade;Retinal detachmen~;Keratopathy;Glaucoma;Cataract
Abstract
BACKGROUND: The use of &iliconeoil as an endotamponade for the treatment of complicated retinaIdetachment is common, hut lang-term complications can oceur if the oil is not removed later. Thisartic1edocuments a case of emulsified silicone oil migration into the anterior chamber after vitreoretinaIsurgery and provides a diseussion and review of comrnon anterior segment eomplieations trom thiscondition.
CASE REPORT: A 59-year-old man reported to the eye clinic complaining of a "growth •• over bis righteye that had increased in size over the last month. Stit tamp examination found a "reverse pseudohypopyon" iri the right eye, which was actuaIly emutsified silicone oil that had migrated from the posteriorehamber after a previous retinal detachrnent repair. Tbe patient was referred for surgical removal of thisoily obstruetion. Although surgical treatment was delayed for 18 months, his vision improved and bisintraocular pressure was lowered through surgieal and medical management.CONCLUSIONS: The use of silicone oil as an endotamponade in cases of complex retina! detachmenthas become common, but it also may lead to postoperative complications if it is not surgically removedIater. This case highlights possible complications from the migration of emuIsified silicone oil into theanterior chamber and illustrates the importance of follow-up care for every ophthalmie surgicalprocedure.Optometry 2006;77:446-449
The use of silicone oil in complex vitreoretinal surgery
was first introduced in 1962.1 Its injection into the vitreouscavity.to serve as an endotamponade has become a standard
technique and, when combined with vitreoretinal surgery,
has been used sÜccessfully in the repair of proliferativevitreoretinopathy, prolifera,tive diabetic retinopathy, giantretinal tears, and ocular trauma. 2 .Silicone oll has been
known to emu1sify and migrate into various locations withinthe globe.3 Because this can lead to long-term cornplications, such as cornea! decompensation, cataract, and glau-
Correspondingauthor: DennisJ. Light, O.D., Departmentof VeteransAffairs,Eastern Colorado HenlthCare SystemEye Clinic, 4112 OutlookB1vd.,Pueblo,Colorado81008.
E-mail: [email protected]
coma, it should be removed after adequate duration ofendotamponade.4
(ase report
A 59-year-old man reported to the eye clinic complaining ofa "growth" over bis right eye that had increased in size overthe last month according to his wife's observation. Hedenied any asthenopia but reported that he "had very little
vision" in this eye and that Hit might have gotten a littleworse:'
His medical history included a '3S-year history of type 2diabetes mellitus for which he had taken insulin for the last
15 years. His last Ale hemoglobin test, a measure of the
1529-1839/06/$ -see front matter © 2006 American Optometrie Association All rights reserved.doi:lO.l 016/j.optm.2006.04.l19

Oenni" J. Light ClinicaL Ca,,,
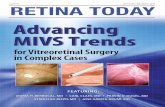
Figure 1 A "reverse pseudohypopyon" of emulsified silicone oil drop·
lets in the superior anterior chamber.
--""!1lilunt 01' glycnsylated h~moglobin in the blilod and a goodesrim;1lOr pI' htH\- \IcH the diabetes has been managed over
the pr~~\'ious 3 rnonlhs. \las 8.Y{;. He also had hypertension.
rhcumatniJ arthritis. hypcrlipidemia. duonie lower backpain. kidncy stones. gallbladder disea~c. and depression. Hismedications inc!uued insulin ntlvolin. rosiglitazone maleate.
and metarürmin HeL für his diabetes; Iisinopril. cycloben
l.aprine HeL hydrocblorothiazide. and metoprolol für his
hypertension; gemtlbr~nil for his hyperlipidemia: and amitrypliline Hel. for his depression. He reported no allergies.
His ocular hhtory was somcwhat sketchy but includedprevious "laser treatments for diabetö in bOlh eyes" and a
retinal detad111lCl1l repair 01' his right cye ! yeur previously.His uncorrccted visua! <lcuitics were 1/160 in the right eye(O.D.) amI 20170 2 in the !en eye (O.5.t Manifest refrac
lion was unable 10 improve the vision in his right eye whiiehis !efl eye was best conected to 20/60' 2. Pupils were 4mmand wund but with minimal reactiol1s in both eves (OU). A
~. ,.:rade ! + right relative afferent pupillary defect waspresent.
Billmicroscopy showed clear amI quiet conjlloctival tissues OU. The cornea was clear wilhollt ederna or endothe
baI strimions OU. In thc right eye. there was a globule of
silicone oil oceupying 40o/c of the superior anterio! chamberthat would O)ove sJightly with head tilt to either shoulder
(see Figure 1 ). Thc globulctilled the entire superior anteriorchamber and contacted the corneal endothelium amI the
amerior iris. 11 was composed 01' multiple, smalf, semi
opaque, nil droplets thm gave a "rock candy" appearance 10the globule. Gonioscopy llndings showed the angle open to
the ciliary body inferiorly 0.0.. but there was no view
through the globule 10 the superior angle. His irides werenormal, w1lh no rubcoslS 01' indotomy present in either eye.Grade 3+ l111clear sclerosis O.D. and grade 1+ nlldear
sclerosis O.S. were prescnt. lntn.lOClllar pressures by Gold·mann applan::.llion tonometry wert' 18 mmHg O.D. and 13
rnmHg O.S. at ]0:02 AM.
DiJared fundus examinariofl fj nJings were remarkabJe fordense vitreous debris and hall' 0.0. Because 01' the cloud-
447
iness 01' the media. a limiled view ur the fundus was
available O.D .. and unfortunately. fine retinal detail could
not be viewed. A red reflex was presenr in aH quadrants.B-scan ultrasonography. although indicalcd in cases in
which the retina cannol be visualized cleady to help determine the presence or absence of retina I detachment. was not
performed owing to unavailability 01' the instrument. Therewas 360-degree panretinal pholocoagulation 0.5. with flbrous vascular scarring temporal to thc rnacula.
This patient had emuJsified silicone oil in the anterior
chamber 01' the right eye after retinal detachment repair ! yearpreviously. He was referred to a vÜreoretinal specialist for
evaluation and surgical rem ova] of the emulsified silicone oil.
The decision to remove the emulsiflcd silicone oi! sllrgicallywas based on the patiem's des ire to improve his cosmetic
appearance (remove "thc grO\vth"), improve the reduction ofvisual acuity, decrease tbe elevated intraocular presslIre. rcmove the prescnee of comeal touch. and remove thc catamc!.
Unforlunately, this patient had unstablc angina associ
ared with poofly controlled hypel1cnsion causing him ro
canee! his surgical procedure. He returned for eare I yearlater. and a! thm time his vision had dccreased to lightperception 0.0..and his imraocular prcssure had risen to 28mmHg 0.0. He was prescribed O.2o/c brimonidine tartrate
twiee a day O.D., which lowered the intraocuJar pressure to18 mmHg O.D.
His SUHrcrv was delaved again after he suffered a tran-'-..' "' ..J ••••
sient ischemic aHack .that warranted flIrther cardiac and
carotid artery evaluations. Six months later, however. he
underwent successfuJ surgicaJ removal of the silicone oil0.0. with phacoemulsification and posterior charnber intraocular lens implantation. One day postoperative]y, visionhad improved to 4/1600.0. although there was consider
able comeal edema Iikely from endothelial cell los5 and
dysfunction from the silicone oil contact. His intraocular
pressure was 13 mmHg 0.0. Fundus examination tindingsshowed extensive panretinaJ photocoaglliation with areas offibrosis. auenuated vessels. ghost (sclerotic) vesseIs. andmoderate optic nerve pa]]or 0.0. believed to have resulted
from previous diabetic optic neuropathy.At his 6-monrh postoperative visit, vision had improved
to 20/] 50 0.0. The comea O.D. continued to show mild
edema without endothelial striation. The posterior eh amberintraocular lens implant O.D. was centered and elear. The
intraocular pressure was 16 mmHg O.D. on O.2'k brimonidinc tartrate bid.
Discussion
Silicone oil often is placed in the vitreoretinal cavily as an
aid in the repair of proliferative vitreoretinopathy, prolifcrative cliabetic rctinopathy, reCllrrent retinal dClachmenh.giant retinal tears. macular hole. viral retinitis. and lTaumatic
retinal injuries. 5 Ir has a densily lower than water and Illuch
greater surface tensions. making it an dfective intraocubr

448
tamponade. When injected into the vitreal cavity, its buoyancy mechanically pushes the retina back into its properanatomie position, while its surface tension helps keep itthere. This also keeps vitreal fluid from entering through aretinal break into the subretinal space, thus allowing for astrong chorioretinal adhesion to take place.6
The use of silicone oll as a tamponade has a fewadvantages compared with long-lasting gases used for similar purposes. Unlike the gas-filled eye, which leaves thepatient with no useful vision, silicone oil is transparent (itdoes not mix with intraocular fluids or blood) and perrnitsthe patient to see after proper refraction.7 The use of siliconeoil eliminates the need for facedown positioning duringhealing, and it allows for high altitude and air travel (gasexpands at higher altitudes). Perhaps its biggest advantage isthat it does not dissolve, allowing for longer-acting tamponade in the repair of very complicated retinal detachments.8
This permanence of silicbne oil in ocular tissue hasc;sociated risks. Over time, silicone oil bas a tendency to
•.•mulsify and break into smaller oil droplets, which have apropensity to leak through very small openings.9 The droplets may egress surgical incision sites or rnigrate throughanatomically compromised areas such as through brokenzonules.10 Migration has been observed in phakic, aphakic,and pseudophakic eyes, and has been documented from
eyelidJ1•12 to optic nerveY·J4 Emulsification of silicone oilto some degree has been reported to occur in 56% tO.1 00%of cases over aperiod of months· to years.3.10 Multiplefactors may contribute to silicone oil emulsification, inc1uding the use oflow viscosity silicone oils (higher viscosityoils restriet mechanical emul sificati on),9 residual fluid in thevitreous cavity, and hemorrhage or leakage of other bloodconstituents from the breakdown of the blood-aqueousbarrier after surgery.J5.J6 Anterior segment complicationsassociated with the use of silicone oil include alterations ofcorneal structure or integrity,17 increased intraocular pres-
----'lre,18and development or progression of cataract.4Silicone oil is toxic to the cornea. Specular microscopic
studies have shown the main corneal complication to beendothelial cell darnage inc1uding decreased cell density,pleomorphism, and necrosis. If allowed to enter the anteriorchamber, silicone oll will eventually lead to corneal endothelialcell damage, edema, or band keratopathy.19 Rates ofkeratopathy after silicone oil injection have been reported torange from 4.5% to 63%.2 As seen in this case report,corneal edema may riot always be present on initial presentation, even if there is significant corneal touch and presumed endothelial damage. Silicone oil in the anteriorchamber may act as a physical barrier and interfere withcorneal homeostasis.20 When the oi! is removed later dam
aged endothelium may allow for excess stromal hydrationand lead to corneal edema.
The prevalence of elevated intraocular press ure aftersilicone oil injection has been reported to range from 1.5%~o.48%,21 Silicone oil in the vitreous cavity may push thems or lens forward resulting in pupillary block or directangle obstruction. Emulsified silicone oil also may fill the
Optometry, Vol 77, No 9, September 2006
anterior chamber, infiltrate the trabecular meshwork, anddecrease the aqueous outflow.22 Outflow in this case isaffected initially through direct obstruction, aIthough histologie studies have shown that silicone damages the outftowpathway with a loss of cellularity and fibrosis. Foreign bodygranuloma containing macrophages laden with oil also maydevelop.22.23 Clinically significant increased intraocularpressure after silicone oil injection usually can be controlledby topical antiglaucoma medications and is reversible inmost patients after oil removal.23
By preventing the anterior migration cf silicone oil fromthe vitreous cavity, the risk of damage to the cornea anddevelopment of elevated intraocular pressure can be re·duced?4 A prophylactic inferior peripheral iridotomy maybe placed at the time of silicone injection. The buoyancy ofthe silicone oil coupled with the inferior placement of theiridotomy encourages a natural flow of aqueous from theposterior chamber into the anterior ehamber. This helpsprevent pupillary block and indirectly limits the access andmigration of silicone oil into the anterior chamber.25
Cataracts can develop in nearly all eyes in wh ich silicone .oil remains in situ for a few months, and up to 60% of lensesthat appear relative1y clear at the time of silicone oil removal will also develop a clinically significant cataraet after2 years?6 Obstruction of normal metabolie exchange at thesilicone-Iens interface results in cataract fonnationP Cat
aract formation may be delayed by the early removal ofsilicone oil,28but it is considered to be almost unavoidable.
The reported incidence of alterations to the cornealstructure or integrity, increased intraocular pressure, andcataract progression show a varied range of occurrence.This variation can be attributed to a number of factors
including sampIe size, viscosity of silicone oi! used, theduration of silicone oil endotamponade, the presence ofinferior iridotomy, and previous surgical history.
Surgical removal of silicone oil significantly increasesthe likelihood of improved visual acuity and reduces the riskof keratopathy, secondary glaucoma, and cataract progression.4 The timing of silicone oil removal remains contcoversial,29.3obut in most cases, removal is recommended 2 to3 months after surgery31 or as soon as a stable retinalsituation is achieved. This can be difficult to assess. Clinicalsigns include a quieting of inflammation, a whitening of anyepiretinal membrane formation, and, most important, a lackof change in the appearance or configuration of the retina.32Contraindications for removal are unclear but include the
presenee of profound hypotony,33 In any case, there is anincreased risk of retinal detachment after oil removal. Mostretinal redetachments occur within the first 3 months afterremoval of silicone oil. Six months after oiI removal, aretinal redetachment becomes unlikely. 34
Summary
The use of silicone oil as an endotamponade in cases ofcomplicated retina! detachment has become increasingly

Dennis J. Light Clinical Care
common, but it is has been associated with alterations to the
corneal structure or integrity, increased intraoeular pressure,and cataraet progression. Surgical removal of the siliconeoil reduces the risk of these eomplications and signifieantlyincreases the likelihood of improved visual aeuity. Removalis reeommended as soon as the tamponade effect is nolonger needed. This case shows the importanee of follow-upcare for every ophthalmie surgical procedure. The optometrist should be familiar with the technique and materialsused during ophthalmie surgery and be aware ofthe clinicalsigns of potential eomplications.
Acknowledgments
The author acknowledges Robert Newcomb, O.D., GregoFy__Kiracofe, O.D., and Wilbur Meiklejohn, O.D., for their
.ontributions to this case report.
References
I. Cibis PA. Becker B. Okun E. el al. The use of liquid silicone in retinaldetnchment surgery. Arch Ophthalmol ]962;68:590-9.
2. Falkner CI, Binder S, Kruger A. Oukome after silicone ~it removal.Br J OphthalmoI200];85:1324-7.
3. Fedetman JL. Scbubert HD. Complications associated witb the use ofsilicone oil in 150 eyes after retina-vitreous surgery. Ophtha/mology1988;95:870-6.
4. Hutton WL, Azen SP, Blumenkranz MS, et al. Tbe effects of silicone
oil removal. Silicone Study Report 6. Arch Ophthalmoll994;112:77885.
5. Jonas JB, Knorr HL, Rank RM, et al. Retinal redetachment afterremoval of introocular silicone oil tamponade. Br J Ophthalmol2001;85:1203-7.
S. Gallemore RP. McCuen BW 11.Silicone oil in vitreoretinal surgery. In:
Ryan 5J, ed. Retina, Vol. 4. Sr. Louis, MO: Mosby; 2000:22] 1-34.7. Lane JL. Wat..<;onRE Jr, Wille RJ, et al. Retinal detachment: imaging
of surgical treatments and cornplications. Radiographies 2003;23:98394.
8. Yamamoto S, Takeuchi S. Silicone oil and fluorosilicone. SeminOphthalmoI2000;15:15-24.
9. Nakamura K. Refojo MF. Crabtree DV. Factors contributing to theemulsification of intraocular silicone and ftuorosilicone oils. /nvest
Ophthalmol Vis Sei 1990;31 :647-56.
10. Donahue SP, Friberg TR, Johnson BL. Intraconjunctival cavltaryinclusions of silicone oil complicating retinal detachrnent repair. Am JOphthalmol 1992;114:639-40.
11. Donker DL, Paridaens D, Mooy CM, et al. Blepharoptosis and uppereyelid swelling due to lipogranulomatous inflammation caused bysilicone oil. AmJ OphthalmoI2005;140:934-6.
449
12. Quintyn JC, Genevois 0, Ranty ML, el al. Silicone oil migration in theeyelid after vitrectomy for retinal detachment Am J Ophthalmol2003;136:540-2.
13. Ni C, Wang WJ, Albert DM, et aI. Intravitreous silicone injection.Histopathologie findings in a human eye after ]2 years. Arch Ophthalmol 1983;10]:1399-1401.
14. Fangtian D, Rongping D, Lin Z, et a1.Migration of silicone oil into the
cerebral ventricIes. Am J Ophthalmol 2005;140:156-8.15. Bartov E, Pennarola F, Savion N. et al. A quantitative in vitro model
for silicone, oil emulsification. Role of blood constituents. Retina] 992;12:S23-7.
16. Heidenkummer HP. Kampik A, Thierfelder S. Emulsification of sili
cone oils with specific physico-chemical characteristics. Graefes ArchClin Exp OhthalmoI1991;229:88-94.
17. Abrams GW. Azen SP, Barr CC, et al. Tbe incidence of corneal
abnormalities in the Silicone Study report 7. Arch Ophthalmol1995;13:764-9.
18. Bare CC, Lai MY, Lean JS, et al. Postoperative intraocular pressureabnormalities in the Silicone Study. Silicone Study report 4. Ophthalmology 1993;100:1629-35.
19. Gao RL, Neubaurer 1, Tang S, et al. Silicone oil in the anteriorchamber. Graefes Arch CUn Exp OphthalmoI1989;227(2):106-9 .
20. Stemberg P, Hatchell DL, Foulks GN, et aI. Tbe effect of silicone oilon tlJe cornea. Arcll Ophrha/molI985; 103:90-4.
21. Nguyen QH, Lloyd MA, Heuer DK, et al. Incidence and managementof glaucoma after intravitreal silicone oi! injection for complicaledretinal detachments. Ophthalmology 1992;99:1520-6.
22. Valone J Jr, McCarthy M. Emulsified anterior chamber oil and glaucoma. OphthaZmology 1994;101:1908-12.
23. Jonas JB, Knorr m.... Rank RM, et al. Intraocular pressure and silicone
oil endotnmponade. J Glaucoma 200];10:102-8 ..24. Friberg TR. Guibord NM. Comeal endothelial cell ]oss. after multiple
vitreoretinal procedures aT'.l the !Jse of silicone oil. Ophthalmie: SurgLasers 1990;30:528-34.
25. Madreperla SA; McCuen MW 2nd. Inferior peripheral iridectomy inpatients receiving silicone oil. Rates of postoperative c10sure andeffect on oil position. Retina 1995;15:87"90.
26. Assi A, Woodruff S, Gotzardis E. el al. Combined phacoemulsificationand transpupillary drainage of silicone oil: results and complications.Br J OphthalmoI2001;85:942-5.
27. Leaver PK, Grey RH, Gamet' A. Silicone oil injection in the treatmentof massive pre-retinal retraction. L Late complications in 93 eyes. Br J
Ophthalmol1979;63:361-7 ..28. Franks WA, Leaver PK. Removal of silicone oil-rewards and pen
alties. Eye 1991;5(Pt 3):333-7.29. Caswell AG, Gregor zr. Silicone oil removal. I. The effect on the
cornplications of silicone oil. Br J Ophthalmo11987;71:893-7.
30. Caswell AG. Gregor zr. Silicone oil removal. II. Operative andpostoperative complications. Br J OphthalmoI1987;71:898-902.
31. Laroche L, Pavalski C. Saraux H, et al. Ocular findings followingintrovitreal silicone injection. Arch OphthalmoI1983;101:1422-5.
32. Unlu N. Kocaoglan H, Acar MA, et al. Outcome of complex retinaldetnchment surgery after silicone oil removal. /nt Ophthalmol 2004;25:33-6.
33. Zillis JD, McCuen II BW, de luan E, et al. Results of silicone oil
removal in advanced proliferative vitreoretinopathy. Am J Ophthalmol1989;108:15-21.
34. Lesnoni G, Rosi T, Nistri A, et al. Long-term prognosis after removalof silicone oil. Eur J Ophthalmol 2000;10:60-5.