A prospective investigation of the development of borderline personality symptoms.pdf
description

Symptoms and Signsof Neuro-otologicDisorders
David E. Newman-Toker, MD, PhD, FAAN
ABSTRACTPurpose of Review: Symptoms and signs of neuro-otologic disorders are criticalcomponents in the diagnostic assessment of patients with vestibular symptoms suchas vertigo, dizziness, unsteadiness, and oscillopsia. Most diagnoses can be accom-plished at the bedside. An understanding of key diagnostic principles is essential forall practicing neurologists, who are often faced with determining whether suchpatients warrant urgent diagnostic testing or hospital admission. This article intro-duces readers to core concepts and recent advances in the understanding of di-rected history taking and physical examination in patients with vestibular symptomsor suspected neuro-otologic disorders.Recent Findings: International consensus definitions for vestibular symptoms haverecently been published. During the past 5 years, a growing body of scientific evi-dence has demonstrated that the traditional approach to bedside diagnosis of pa-tients with vertigo and dizziness is inadequate. Former teaching that history takingshould first rely on categorizing symptoms by type (eg, vertigo, presyncope, dis-equilibrium, nonspecific dizziness) has been replaced by an emphasis on catego-rizing timing and triggers for vestibular symptoms, which focuses the clinician’sattention on four key syndromic patterns: (1) acute, spontaneous, prolonged vestib-ular symptoms; (2) episodic, positional vestibular symptoms; (3) episodic, spontaneousvestibular symptoms; and (4) chronic unsteadiness (with or without oscillopsia). Eachof these categories delineates a relatively narrow differential diagnosis within which afocused examination distinguishes between benign common causes and dangerousuncommon ones.Summary: A focused approach to bedside assessment of patients with vestibularsymptoms is essential for accurate and efficient diagnosis. All neurologists should beaware of major recent advances.
Continuum Lifelong Learning Neurol 2012;18(5):1016–1040.
INTRODUCTIONPatients with neuro-otologic disorderstypically present with vertigo, dizziness,unsteadiness, or oscillopsia. Althoughmuch confusion and controversy existregarding these terms, internationalconsensus definitions have recentlybeen published (Box 2-1).1,2 This arti-cle will focus on key elements of thehistory and physical examination thathave important diagnostic value in the
assessment of patients with such symp-toms. While this article is not intendedto cover differential diagnosis per se, abrief discussion about general diagnos-tic approach is warranted, since theapproach influences the choice of whatis important in the history and physicalexamination.
In general, the role of the neurologistin vestibular diagnosis is often to dif-ferentiate central (ie, neurologic) from
Address correspondence toDr David E. Newman-Toker,Johns Hopkins Hospital,Department of Neurology,600 North Wolfe Street, Meyer8-154, Baltimore, MD 21287,[email protected].
Relationship Disclosure:
Dr Newman-Toker hasreceived honoraria forspeaking from JanssenPharmaceuticals, Inc., andconsulting fees from PierreFabre. He has receivedresearch support from theAgency for HealthcareResearch and Quality andthe NIH.Unlabeled Use ofProducts/InvestigationalUse Disclosure:
Dr Newman-Toker reports nodisclosure.* 2012, American Academy ofNeurology.
1016 www.aan.com/continuum October 2012
Review Article
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

peripheral (ie, otologic) causes for ves-tibular symptoms. Although some cen-tral causes (eg, multiple sclerosis) areless urgent, and some peripheral causes(eg, bacterial labyrinthitis) are quiteurgent, usually the reverse occurs; cen-tral causes (eg, stroke) are dangerousand urgent, and peripheral causes (eg,benign paroxysmal positional vertigo[BPPV] and Meniere disease) are benignor nonurgent. Thus, much of this arti-cle will focus on the utility of symptomsand signs for localizing vestibular le-sions as central versus peripheral. De-spite this focus, the neurologist mustalso remain vigilant about generalmedical disorders (especially cardiac),which, in aggregate, are actually morecommon causes of dizziness than areotologic or neurologic disorders.3 Thearticle will therefore also make refer-ence to circumstances in which symp-toms or signs can, or cannot, be usedto identify non-neurovestibular causes,particularly those that are dangerousand urgent (eg, cardiac arrhythmia).
RECENT TRENDSThe traditional approach to diagnosis ofpatients with vertigo or dizziness reliesheavily on the premise that the type ofvestibular symptom predicts the under-lying etiology. In this approach, thesymptom type is classified as (1) ver-tigo (spinning ormotion), (2) presyncope(impending faint), (3) disequilibrium(unsteadiness whenwalking), or (4) non-specific dizziness (any other balance-related sensation not fitting the priorthree categories).4 These traditional cat-egories direct subsequent diagnostic in-quiry, with vertigo prompting a searchfor vestibular causes, presyncope asearch for cardiovascular causes, un-steadiness a search for neurologiccauses, and nonspecific dizziness asearch for psychiatric or metaboliccauses.5 This approach, described in1972,6 continues to appear in high-impact medical journals, commonlyused medical texts, and Internet-basedresources. Recent studies confirm thatthis diagnostic method for assessing
BOX 2-1 International Consensus Definitions for CommonVestibular Symptomsa,b
Term Definition
Vertigo The sensation of self-motion when no self-motion is occurring orthe sensation of distorted self-motion during an otherwisenormal head movement.
Dizziness The sensation of disturbed or impaired spatial orientationwithout a false or distorted sense of motion.
Unsteadiness The feeling of being unstable while seated, standing, or walkingwithout a particular directional preference.
Oscillopsia The false sensation that the visual surround is oscillating.
Presyncope The sensation of impending loss of consciousness.
Syncope Transient loss of consciousness due to transient global cerebralhypoperfusion characterized by rapid onset, short duration, andspontaneous complete recovery.
a Data from Bisdorf A, et al, J Vestib Res.1 iospress.metapress.com/content/m127vq45v8l47052/.bData from Task Force for the Diagnosis and Management of Syncope, European Societyof Cardiology (ESC), European Heart Rhythm Association (EHRA), et al, Eur Heart J.2
eurheartj.oxfordjournals.org/content/30/21/2631.long.
1017Continuum Lifelong Learning Neurol 2012;18(5):1016–1040 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

patients with dizziness represents thecurrent standard of clinical practice infrontline care settings, such as the emer-gency department.7,8
Unfortunately, strong evidence nowindicates that the quality-of-symptomsapproach is neither valid nor reliable9Y13
and could be contributing to misdiag-nosis.4,8 Patients with dizziness fre-quently change their report of the typeof dizziness when they are asked todescribe it 5 to 10 minutes later, andtypes of dizziness are not valid indica-tors of the cause.9 Best available evi-dence instead suggests that a shift ofemphasis in clinical assessment awayfrom dizziness type and toward dizzi-ness timing (eg, episode duration) andtriggers (eg, changes in head position)will probably yield more accurate andreproducible diagnostic results.4 At itscore, this ‘‘timing-and-triggers’’ approachseeks to classify patients into one offour major clinical categories: (1) acute,spontaneous, prolonged vestibularsymptoms (often called the acute ves-tibular syndrome14,15), as seen withvestibular neuritis and posterior fossastroke; (2) episodic, positional vestibu-lar symptoms, as seen with BPPV andcentral mimics; (3) episodic, spontane-ous vestibular symptoms, as seen withvestibular migraine, Meniere disease,and TIA; and (4) chronic unsteadiness(with or without oscillopsia), as seenwith cerebellar degeneration, bilateralvestibular failure, and spinal cord com-pression. Each of these syndromes willbe covered in greater detail in laterarticles in this issue.
VESTIBULAR SYMPTOMS ANDHISTORY TAKINGAs with most other areas of neurology,history taking is paramount in patientspresenting with vestibular symptoms. Aswith other patient symptoms, it is gen-erally important to begin with an open-
ended question about the patient’ssymptoms and allow a narrative tounfold. Nevertheless, it is quite typicalwith vestibular patients that the criticalaspects of the history are not sponta-neously reported by the patient, anddirected historical questioning is re-quired. This section will describe eachmajor symptomdimension, such as typeand duration, and other key historicalelements, such as review of symptoms,emphasizing their diagnostic value andsome technical pearls about typical pa-tient responses.
Symptom TypeNeither patients9 nor physicians8,9,16 havea clear understanding of what the terms‘‘dizziness’’ and ‘‘vertigo’’ mean. In theUnited States, it is traditional for dizzi-ness to serve as an umbrella term thatincorporates different forms (eg, vertigo,presyncope, unsteadiness),5,8,10,11,17 andin Europe and Asia this has some-times,18Y20 but not always,1,21Y25 alsobeen the case. This discrepancy hasrecently been resolved by an interna-tional consensus group in favor of anonhierarchic approach that segregatesthe two terms entirely.1 This new ap-proach, however, has not yet fullypenetrated the scientific literature.12,13,26
Furthermore, despite an attempt toclarify that vertigo refers to any illusorysense of motion, whether spinning ornot,1 many practicing clinicians continueto identify vertigo as a ‘‘yes’’ answer tothe question, ‘‘Is the world spinning?’’
As suggested above, the traditionalapproach to diagnosis of vertigo ordizziness relies heavily on vestibularsymptom type. It remains standard fortextbooks andmost clinicians to suggestthat the first and most important ques-tion to ask a patient presenting withdizziness is, ‘‘What do you mean by‘dizzy’?’’ While this may be a reasonablequestion to ask as a conversation starter,
KEY POINTS
h Strong evidence nowindicates that thequality-of-symptomsapproach based oncategorizing dizzinesstype is neither valid norreliable and could becontributing tomisdiagnosis.
h Neither patients norphysicians have a clearunderstanding of whatthe terms ‘‘dizziness’’and ‘‘vertigo’’ mean.New consensusdefinitions have beenpublished.
1018 www.aan.com/continuum October 2012
Symptoms and Signs
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
little evidence suggests that the answerprovides much information of any realuse to the patient or physician. System-atic reviews have found no publishedstudies that support the predictive val-idity of symptom type.13,27 Small studieshave shown no association betweendizziness type and final clinical diagno-ses (eg, type of dizziness fails to differ-entiate central from peripheral causes12
or psychiatric from vestibular causes28).Furthermore, individual patients do notconsistently or reliably report their sub-jective dizziness experience as match-ing a single category, and differentpatients with the same condition expe-rience different types of dizziness.9
The exception may be in categoriz-ing patients whose primary symptom isunsteadiness or oscillopsia rather thanvertigo, dizziness, or presyncope. Al-though well-designed prospective stud-ies are lacking, unsteadiness andoscillopsia are likely associated with asomewhat different differential diagno-sis than vertigo, dizziness, and presyn-cope. This occurs partly because oftheir tendency to be reported as pri-mary complaints in patients withchronic rather than acute or episodicsymptoms. It may also reflect the factthat unilateral disorders, whether cen-tral or peripheral, are somewhat morelikely to produce vertigo, whereas thosethat are bilateral and symmetric do soonly infrequently. Unsteadiness withoutdizziness or vertigo is most commonlyseen in patients with sensory loss (eg,peripheral neuropathy), spinal cord dis-eases (eg, transverse myelitis, cordcompression), and slowly progressive,bilateral cerebellar or vestibular failure(eg, spinocerebellar ataxia syndromes;midline cerebellar neoplasm; bilateralvestibular schwannoma in neurofibro-matosis, type 2). Gait unsteadiness thatis present only with eyes closed andcompletely absent with eyes open ismore likely to be due to bilateral pe-
ripheral vestibular failure than a centralcause. Oscillopsia present at rest usuallyindicates the presence of nystagmus ofany type, but often vertical pendularnystagmus is present in the straight-ahead position of gaze, as seen inpatients with brainstem lesions causedby multiple sclerosis or stroke. Oscil-lopsia that occurs only during headmotion (eg, while walking) usually in-dicates bilateral vestibular failure (eg,post gentamicin toxicity).
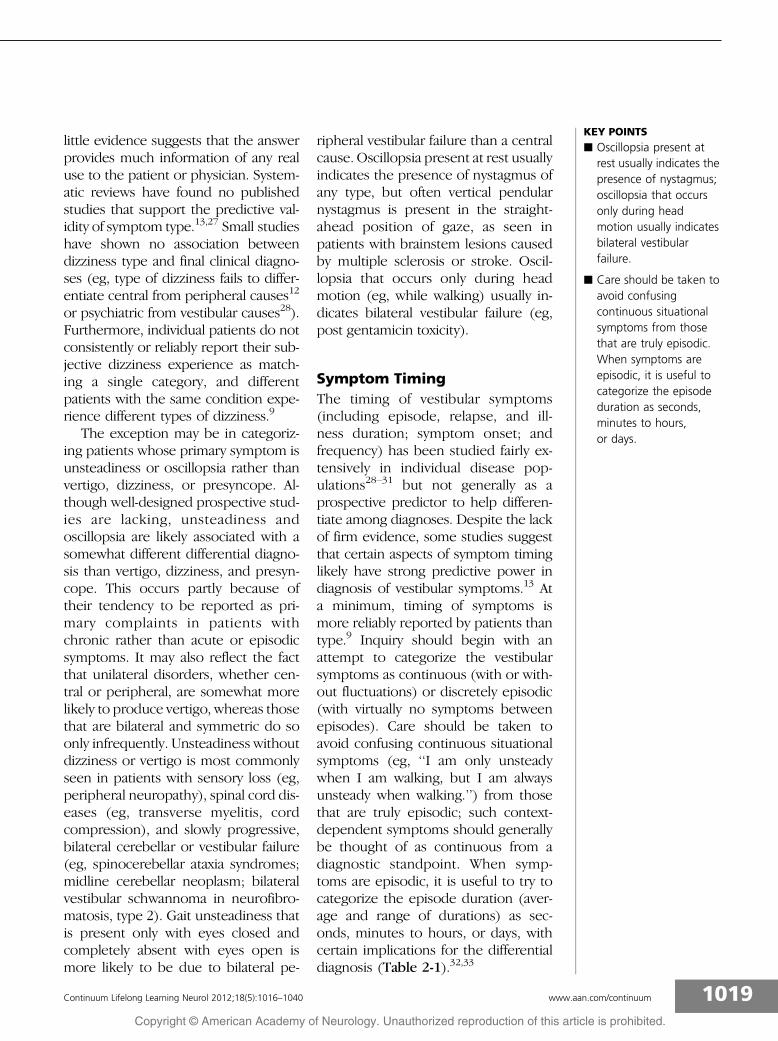
Symptom TimingThe timing of vestibular symptoms(including episode, relapse, and ill-ness duration; symptom onset; andfrequency) has been studied fairly ex-tensively in individual disease pop-ulations28Y31 but not generally as aprospective predictor to help differen-tiate among diagnoses. Despite the lackof firm evidence, some studies suggestthat certain aspects of symptom timinglikely have strong predictive power indiagnosis of vestibular symptoms.13 Ata minimum, timing of symptoms ismore reliably reported by patients thantype.9 Inquiry should begin with anattempt to categorize the vestibularsymptoms as continuous (with or with-out fluctuations) or discretely episodic(with virtually no symptoms betweenepisodes). Care should be taken toavoid confusing continuous situationalsymptoms (eg, ‘‘I am only unsteadywhen I am walking, but I am alwaysunsteady when walking.’’) from thosethat are truly episodic; such context-dependent symptoms should generallybe thought of as continuous from adiagnostic standpoint. When symp-toms are episodic, it is useful to try tocategorize the episode duration (aver-age and range of durations) as sec-onds, minutes to hours, or days, withcertain implications for the differentialdiagnosis (Table 2-1).32,33
KEY POINTS
h Oscillopsia present atrest usually indicates thepresence of nystagmus;oscillopsia that occursonly during headmotion usually indicatesbilateral vestibularfailure.
h Care should be taken toavoid confusingcontinuous situationalsymptoms from thosethat are truly episodic.When symptoms areepisodic, it is useful tocategorize the episodeduration as seconds,minutes to hours,or days.
1019Continuum Lifelong Learning Neurol 2012;18(5):1016–1040 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Three clinical nuances about epi-sode duration are worth noting:
1. If the clinician is not careful wheninquiring about duration, patientsmay initially report illness rather thanepisode duration. For example, inBPPV, episodes generally last sec-onds but occur repetitively during about or relapse for 1 to 2 weeks.
2. Patients may respond to an open-ended question about episode dura-tion with, ‘‘I don’t know’’ or ‘‘I wasn’tlooking at the clock’’; do not allowthem to escape answering the ques-tion. It is easy to reframe the question
for the patient by asking, ‘‘Was itseconds, minutes, hours, days, weeks,months, or years?’’ to help themunder-stand the level of precision required.
3. Patients may initially overestimateepisode duration, particularly forbrief episodes, either because timeseems to slow down during an attackof severe vertigo or dizziness or theyare reporting the duration of feelingslightly unwell (eg, nauseated) ormildly unsteady, rather than thecore duration of the main symptom.It may be necessary to push the pa-tient toward a shorter duration to test
TABLE 2-1 Common Causes of New Vertigo or Dizziness and Dangerous Mimics, By Durationa
Duration Common, Benignb Causes Principal Dangerous Mimics
Seconds to hours (episodic:transient or intermittent)
Benign paroxysmal positionalvertigo(s)
Benign orthostatic hypotension (eg,medications) (seconds to minutes)
Reflex syncope (seconds to minutes)
Panic attack (minutes to hours)
Meniere syndrome (minutes to hours)
Vestibular migraine (seconds to daysc)
TIA
Cardiac arrhythmia
Other cardiovascular disorders (eg,myocardial ischemia, aortic dissection,atrial myxoma, pulmonary embolus,occult gastrointestinal bleeding)
Neurohumoral neoplasm (eg,insulinomad, pheochromocytoma)
Days to weeks (nonepisodic:persistent or continuous)
Vestibular neuritis
Viral labyrinthitis
Medication toxicity(eg, anticonvulsants)
Brainstem, cerebellar, or labyrinthinestroke
Bacterial labyrinthitis/mastoiditis orherpes zoster oticus
Brainstem encephalitis (eg, Listeria,herpes simplex, paraneoplastic),
Miller-Fisher syndrome
Wernicke syndrome
Medication toxicitye (eg, lithium), drugwithdrawal (eg, alcohol), or toxicexposure (eg, carbon monoxide)
a Reprinted with permission from Newman-Toker DE, The neuro-ophthalmology virtual education library.32 novel.utah.edu/Newman-Toker/collection.php.
b Although they may be quite disabling during the acute illness phase, diseases classified here as common, benign causes rarely producesevere, irreversible morbidity or mortality, unlike their dangerous mimics counterparts.
c Vestibular migraine episodes may last longer than a day in about 25% of cases.33 Rigorous data on the duration of symptoms in thissubset of patients with vestibular migraine are lacking, but clinical experience suggests that such patients rarely experience true episodeslasting longer than 48 to 72 hours.
d Other causes of hypoglycemia (eg, excess exogenous insulin) are more common but usually simpler to diagnose.e The duration of medication toxicity depends on dosing and the half-life of the medication.
1020 www.aan.com/continuum October 2012
Symptoms and Signs
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

whether temporal expansion may beat play. For example, if a patientinitially reports a 5-minute duration,ask, ‘‘Is it possible it might have beenjust a couple of minutes?’’ If thepatient says yes, consider asking,‘‘Might it have been less than a min-ute?’’ Follow-up questions such as,‘‘Did the bad vertigo you describedlast the whole time during the spell,or was the worst of it a lot shorter?’’may also get to the duration of coresymptoms.
Less is known about symptom onsetand frequency as predictors of under-lying disease. Some weak evidence sug-gests that abrupt-onset (instantaneousor nearly so) dizziness or vertigo may bemore likely to result from cerebrovas-cular than inflammatory causes,13 but itis common for many benign forms ofdizziness, such as BPPV, to begin fairlyabruptly. Also, in cases in which symp-toms were absent prior to sleep andpresent on awakening, the onset char-acteristics cannot be determined. Fre-quency of symptoms is an imprecisepredictor, except in cases inwhich symp-toms are frequent during a very long ill-ness duration, such as a decade orlonger, without permanent sequelae. Insuch cases, benign, recurrent disorders,such as vestibular migraine and Menieredisease, are highly likely. With an illnessduration of weeks or months, frequentor escalating symptoms may actually beharbingers of a dangerous underlyingetiology, such as TIA.13 Illness durationsof 1 to 5 years are intermediate in risk.
Symptom TriggersVestibular symptom triggers may in-clude positional change (head positionor body posture), Valsalva maneuver,and exertion, among others.1,10 Again,despite the lack of prospective stud-ies, some triggers clearly have strongpredictive power in diagnosis of neuro-
otologic aswell as cardiovascular disorderscausing episodic vestibular symptoms.10
Similar to timing, symptom triggers aremore consistently reported by patientsthan type.9 Clinicians must carefully dis-tinguish triggers (which provoke newsymptoms not present at baseline) fromexacerbating features (which worsen pre-existing baseline symptoms), since almostall forms of vestibular dizziness, whethercentral or peripheral, are exacerbatedby head movement, at least acutely.
The most common triggers arechanges in head position or body pos-ture, particularly rising from a recumbentor seated position.34 The most com-mon etiologies are orthostatic hypoten-sion and BPPV. Dangerous etiologiesinclude serious causes of orthostatichypotension, such as internal bleeding,and central mimics of BPPV, usually dueto posterior fossa structural lesions.35,36
BPPV may be confused with orthostatichypotension if patients report dizzinesson rising. The two can generally be dif-ferentiated by inquiring about symptomsthat occur on reclining or rolling over inbed, which should only be present inpatients with BPPV. Forms of BPPV andtheir diagnoses are described in other ar-ticles. However, triggers for symptomsare often canal specific (eg, posteriorcanal BPPV is triggered by tipping thehead back but not by turning the headto one side when upright), and theseissues will be alluded to in the ‘‘Signs’’section that follows ‘‘Symptoms’’ sincepositional testing and treatment maneu-vers are also canal specific.37 Vestibularmigraine can also produce BPPV-like po-sitional symptoms.38
Care should be taken to avoid con-fusing brief, triggered episodes (as withBPPV or orthostatic hypotension) withhead-motion dizziness (dizziness occur-ring only during head motion, ie, timelocked to the head movement)1 typi-cally seen in patients with chronic dizzi-ness after unilateral or bilateral vestibular
KEY POINTS
h With an illness durationof weeks or months,frequent or escalatingsymptoms may actuallybe harbingers of adangerous underlyingetiology such as TIA.
h Clinicians must carefullydistinguish triggers fromexacerbating features,since almost all forms ofvestibular dizziness,whether central orperipheral, areexacerbated by headmovement.
h Care should be taken toavoid confusing brief,triggered episodes withhead-motion dizziness,typically seen in patientswith chronic dizzinessafter unilateral orbilateral vestibular loss.
1021Continuum Lifelong Learning Neurol 2012;18(5):1016–1040 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

loss but also in vestibular migraine.Vestibular symptoms triggered by visualmotion with head still are commonly en-countered in vestibularmigraine andmaybe relatively specific for this condition.Some rare triggers, such as sound, some-times referred to as the Tullio phenom-enon, point to a narrow list of rare causes,such as superior canal dehiscence syn-drome, reflex epilepsy, and long QTsyndrome. A more thorough discussionof triggers is available elsewhere.10 Themost important message about trig-gered vestibular symptoms is thatmost patients with clear, reproducibletriggers for their symptoms have abenign underlying cause.10 Most dan-gerous causes for episodic symptoms,such as TIA and cardiac arrhythmia,usually occur spontaneously. A nota-ble exception is exertion, in which car-diac causes remain a serious concern.10
On rare occasions, far lateral head ro-tation can trigger posterior circulationTIA in the rotational vertebral arterysyndrome.39 These unusual cases mustbe distinguished from the more com-mon carotid sinus hypersensitivity syn-drome that also presents with dizzinesstriggered by lateral head rotation oranterior neck compression.
Review of SystemsAssociated symptoms are often impor-tant in the diagnostic assessment of pa-tients with a primary vestibular symptom.Theymay be divided into para-vestibular,otologic, cephalalgic, neurologic, andothermedical symptoms. Symptoms sponta-neously reported by the patient, as op-posed to elicited on symptom review,are perhaps more likely to be relevant,but it is common for diagnostically crit-ical symptoms to seem mild or irrele-vant to patients, eg, mild neck pain invertebral artery dissection presentingwith vertigo.40
The presence of vestibulo-vagal (nau-sea, vomiting) and vestibulo-spinal (gait
disturbance) symptoms is the rule ratherthan the exception in patients with acutevestibular pathology, whether new orrecurrent and episodic. These threepara-vestibular symptoms are oftenprominent in patients with a report ofvertigo, particularly if the vertigo issustained for more than a few seconds.Although these symptoms usually indi-cate a vestibular etiology, they do notassist in localization (ie, in distinguishingcentral from peripheral), except perhapsin cases in which the associated para-vestibular symptoms are disproportionalin severity to the primary vestibularsymptoms.13 With peripheral vestibularpathology, vertigo, nausea, and gait in-stability tend to be roughly propor-tional to one another in severity; withcentral lesions, this need not be so (eg,disproportionate vomiting or gait dis-turbance relative to dizziness or ver-tigo41,42). This disproportion mayexplain why acute dizziness dominatedby unsteadiness or ataxia is more likelyto have a central cause.12,43 Also, thereport of vertigo combined with nauseaor vomiting is not always due to pri-mary vestibular pathology and mayinstead be a sign of cardiovasculardisease, such as myocardial infarction44
or orthostatic hypotension.45
Otologic symptoms that may accom-pany vestibular symptoms include bothauditory (eg, tinnitus, hearing loss,hyperacusis) and aural (eg, ear fullnessor pressure, otalgia) symptoms. Thepresence of such symptoms substan-tially increases the odds of a peripherallocalization but does not confirm anonurgent cause except in cases whereauditory symptoms indicate clearMeniere disease, eg, episodic vertigolasting hours during several years, withepisodes routinely heralded by fluc-tuating, low-frequency tinnitus andreversible low-frequency hearing lossdocumented by audiometry. Otherwise,auditory symptoms may be peripheral
KEY POINTS
h Clear, reproducibletriggers for nonexertionalvestibular symptomsusually indicate a benignunderlying cause. Mostdangerous causes forepisodic symptoms,such as TIA and cardiacarrhythmia, usually occurspontaneously.
h Auditory symptoms maybe peripheral inlocalization butdangerous in cause.
1022 www.aan.com/continuum October 2012
Symptoms and Signs
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

in localization but dangerous in cause,14
eg, TIA or stroke due to ischemia in theanterior inferior cerebellar artery terri-tory.11,46 Auditory symptoms may evenoccur with dangerous cardiac disorders.44
Extra caution should be taken whendizziness or vertigo occurs in the con-text of ear or retroauricular pain absentsigns of ear disease (eg, erythema, dis-charge, tenderness), since ear pain is notalways due to local pathology, ie, re-ferred otalgia, and vertebral arterydissection is a recognized cause of suchpain.47 Vestibular migraine may causeeither auditory or aural symptoms.21
Cephalalgic symptoms, whetherman-ifest as headache, neck pain, eye pain,facial pain, or ear pain, are infrequentand, when present, usually not prom-inent in patients with benign peripheralvestibular diseases such as BPPV,Meniere disease, and vestibular neuritis.They are typical in vestibular migraine,but also frequent in dangerous centraldisorders that cause vestibular symp-toms, particularly posterior circulationstroke.13,48 When misdiagnosed, poste-rior circulation strokes are sometimesmistaken for migraine (Case 2-1).49
Pain that is sudden (abrupt onset), sus-tained (more than 72 hours), or severe,more likely indicates a dangerous cere-brovascular condition,13 although eventhe pain of vertebral artery dissectionmay be mild or intermittent.50 Dizzinessand headache are the two most com-mon symptoms of carbon monoxideexposure, and such exposure may beoccult. Not surprisingly, the mere pres-ence of headaches in patients withdizziness probably does not discrimi-nate those with central pathology fromthose with other etiologies.12
General neurologic symptoms (ie,other than audio-vestibular dysfunctionand craniocervical pain, described ear-lier) may be of any type, including bothlong tract (eg, hemiparesis, limb inco-ordination) and cranial nerve related
(eg, diplopia, dysarthria). Such ‘‘focal’’symptoms are rare in benign peripheralvestibular disorders and usually indicatea central cause, whether less urgent (eg,basilar migraine, cerebellar degenera-tion, multiple sclerosis, panic disorder)or more urgent (eg, TIA, stroke, brain-stem encephalitis).12,13 Peripheral causesassociated with neurologic symptomsare usually not benign and include in-fectious, infiltrative, or compressivecranial polyneuropathies (eg, herpeszoster oticus, Lyme disease, carcinom-atous meningitis, base of skull metas-tases) as well as local infections thatinvade the cranial vault and disseminate(eg, otitis media complicated by bacte-rial labyrinthitis and meningitis). Theabsence of general neurologic symp-toms is weak evidence, at best, in favorof a peripheral vestibular disorder, evenin patients with stroke as a cause fortheir vestibular symptoms.13
Almost any generalmedical symptommight potentially be relevant to diagno-sis of dizziness or vertigo (eg, dysuria asan indicator of urosepsis as the cause fordizziness in an older patient). Never-theless, some medical symptoms are ofparticular interest in the evaluation ofpatients with vestibular presentations.These include cardiorespiratory (eg,chest pain, dyspnea, orthopnea, palpita-tions, syncope) or hyperadrenergic (eg,fear, tremulousness, hyperventilation,pupillary dilatation, tachycardia) symp-toms. Cardiorespiratory symptoms, par-ticularly chest pain, dyspnea, or franksyncope, accompanying dizziness orvertigo could suggest an underlyingcardiac or other dangerous etiology,such as aortic dissection or pulmonaryembolus.10,51,52 Similar symptoms mayalso occur in nonurgent cardiovasculardisorders, such as reflex syncope,53 andpossibly a variety of other general med-ical disorders also diagnosed in patientswith dizziness.12 On occasion, syncopemay result from basilar migraine54 or
KEY POINTS
h Cephalalgic symptoms,whether manifest asheadache, neck pain,eye pain, facial pain, orear pain, are frequent indangerous centraldisorders that causevestibular symptoms,particularly posteriorcirculation stroke.
h The absence of generalneurologic symptoms isonly weak evidence infavor of a peripheralvestibular disorder, sincethe majority ofvestibular presentationscaused by stroke haveno associatedneurologic symptoms.
1023Continuum Lifelong Learning Neurol 2012;18(5):1016–1040 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

vertebrobasilar TIA and stroke,55,56
although generally not in associationwith chest pain or dyspnea, unless per-haps the source of a TIA or stroke iscardiac or a vascular dissection in thechest.57 The absence of cardiorespira-tory symptoms should not be used toexclude cardiovascular causes, sinceisolated dizziness or vertigo may some-times be the sole manifestation.11,58
The presence of chest pain or pressureaccompanying a primary symptom ofgait unsteadiness without other vestib-ular symptoms should specificallyprompt consideration of thoracic spinalcord compression.59 Hyperadrenergicsymptoms, with or without cardiores-piratory symptoms, accompanying diz-ziness or vertigo often indicate panicdisorder but can be difficult to distin-guish from less common causes suchas temporal lobe seizures,60 hypoglyce-
mia,61 and neuroendocrine malignancy,such as pheochromocytoma. Rarely,migraine62 or vertebrobasilar TIA andstroke63 may mimic panic disorder.
Medical HistoryMedical history is obviously importantin assessing known causes of recurrentvestibular symptoms (eg, Meniere dis-ease), conditions that may predisposeto vestibular conditions (eg, migraineheadaches or childhood motion sick-ness for vestibular migraine), or riskfactors for diseases that may causevestibular symptoms (eg, dyslipidemiaor diabetes for stroke12). It is generallywise to identify major, known, concur-rent illnesses (eg, multiple sclerosis,HIV/AIDS, metastatic cancer, severemalnutrition, and major depression)or potentially relevant exposures (eg,viral syndrome, ear surgery, bacterial
Case 2-1A 25-year-old woman presented with recent episodic dizziness andheadache. The episodes of dizziness occurred spontaneously once or twice aweek during the prior 6 weeks and lasted 5 to 10 minutes. No associatedneurologic symptoms, including diplopia, were present. The painwas locatedbehind the left ear and had been present throughout the period sincesymptoms began without substantial variation. She had a personal history ofmigraine headaches. No history of vascular risk factors was reported.
Comment. It is natural to assume that a 25-year-old woman with episodic,spontaneous dizziness and head pain, in the context of a personal historyof migraine headaches, is likely to have vestibular migraine as a cause forthe vestibular symptoms. In this case, however, the clue to a dangerousunderlying cause is the presence of continuous head pain. In patients withmigraine and auralike symptoms, both the pain and neurologic symptomsshould fluctuate. Here, the patient’s pain does not fluctuate, suggesting apersistent structural pathology, such as vertebral artery dissection, knownto mimic migraine in younger patients. The location of the pain (behind theear) is one of the common locations for referral of the pain of vertebraldissection. This symptom pattern prompted neuroimaging, and the patientwas found to have vertebral artery dissection. The vestibular symptoms wereattributed to TIAs in the cerebellum. When the diagnosis was made, thepatient disclosed that she had been bungee jumping shortly before the onsetof her symptoms. She had not disclosed this previously when asked aboutany recent injuries, because she did not wish to be blamed for taking the riskand causing her own symptoms. She was treated with anticoagulants for6 months and made a complete recovery.
1024 www.aan.com/continuum October 2012
Symptoms and Signs
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

otitis media, ototoxic medications[especially aminoglycoside antibioticsor chemotherapy agents], and toxins)in addition to assessing vascular riskfactors.13 No element of a patient’s his-tory can confidently predict whetherpresent symptoms are causally relatedto the prior condition or exposure, butthey can help establish a baselineprevalence (prior probability) for cer-tain diseases. Generally speaking, lessshould be inferred diagnostically fromcommon, nonspecific histories andexposures (eg, hypertension, multiplemedications, viral syndrome) than infre-quent, more specific ones (eg, recentear trauma,64 high-altitude travel, expo-sure to sources of carbon monoxide, orsevere systemic infection requiring hos-pitalization and intravenous antibiotics).Others in the household or workplaceaffected by similar symptoms shouldspark consideration of infectious,toxic,65 or heritable causes.66,67
VESTIBULAR SIGNS ANDPHYSICAL EXAMINATIONA thorough treatment of neurovestibu-lar signs and examination techniques isbeyond the scope of this article. Thissection emphasizes the most commonand most diagnostically useful bedsidesigns in neuro-otologic diagnosis, focus-ing on techniques that assist in local-ization, and discusses examination fornystagmus, assessment of the vestibulo-ocular reflex (VOR), and additionaloculomotor testing (alignment, sac-cades, smooth pursuits, and VOR can-cellation). The general neurologic andmedical examinations are briefly dis-cussed. Disease-oriented articles thatfollow emphasize and reinforce theprinciples described here.
NystagmusNystagmus is an involuntary, rapid,rhythmic, oscillatory eye movement
with at least one slow phase. Jerknystagmus has a slow phase and a fastphase (also called quick phase). Pendu-lar nystagmus has only slow phases. Thefinding may be normal or pathologic,depending on the type of nystagmusand the context in which it occurs.Normal forms of nystagmus includephysiologic end-gaze, optokinetic, per-rotatory, and postrotatory. Pathologicforms of nystagmus are varied in etiol-ogy but generally result from diseasesaffecting the brainstem, cerebellum, orperipheral vestibular apparatus. Asym-metric lesions of the vestibular system,central or peripheral, cause a slow-phase drift that is corrected by quickphases (vestibular nystagmus); otherforms of jerk nystagmus result insteadfrom failures of gaze-holding mecha-nisms. On occasion, cerebral disorderscan cause nystagmus, eg, epilepticnystagmus. Nystagmus differs from sac-cadic oscillations (eg, ocular flutter,opsoclonus) or other fast eye move-ment disorders (eg, superior obliquemyokymia) in that these disorders haveno slow phase of movement, ie, back-to-back saccades without an intersacca-dic interval. Certain eye movementsseen only in coma or reduced states ofconsciousness are given special names,eg, bobbing, dipping, and ping-ponggaze. Although classifications vary,some of these may be considered spe-cific forms of nystagmus.
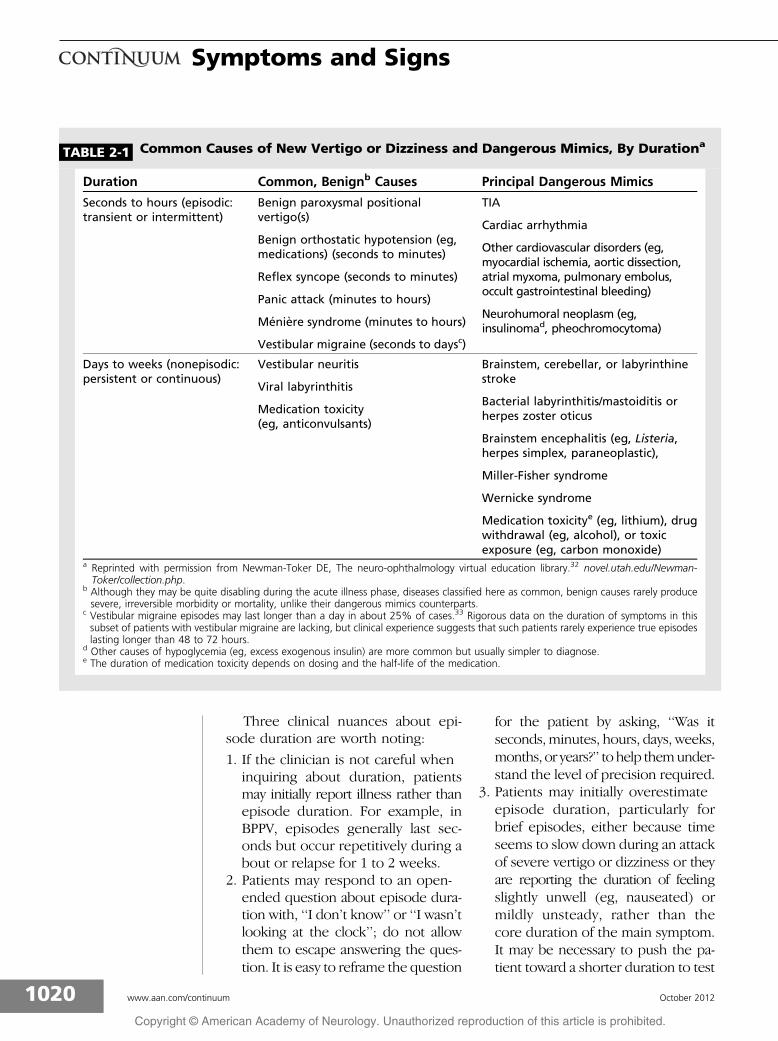
Several nystagmus attributes are typ-ically described either qualitatively atthe bedside or quantitatively using ocu-lographic equipment (Table 2-2). Thepattern of these attributes ultimatelydetermines the localizing value of thenystagmus. While dozens of nystagmustypes and subtypes have been identi-fied,35 only a handful are essential forall neurologists to be able to recognize.A provider who can confidently recog-nize physiologic nystagmus, nystagmusassociated with cerebellar degeneration,
KEY POINT
h Less should be inferreddiagnostically fromcommon, nonspecifichistories and exposures(eg, hypertension,multiple medications,viral syndrome) thanthose that areinfrequent and morespecific (eg, recent eartrauma).
1025Continuum Lifelong Learning Neurol 2012;18(5):1016–1040 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
vestibular neuritis, the direction-changinghorizontal nystagmus of acute stroke,and posterior canal BPPV is already wellon the way to successful diagnosis of thepatient with neurovestibular symptoms.
Nystagmus may be present contin-uously or only intermittently. If inter-mittent, it may be truly episodic andtriggered by particular maneuvers oronly present in certain gaze positionsor under particular viewing conditions(for the patient or the examiner).Thefirst step in assessment for nystagmusis to inspect the eyes carefully in dif-ferent gaze positions: primary position
(ie, looking straight ahead) plus sec-ondary gaze positions (right, left, up,and down). Tertiary gaze positions(up right, up left, down right, downleft) can also be tested, although it isunusual to find nystagmus in thesepositions if none is present in primaryor secondary gaze positions. Physio-logic end-gaze nystagmus to the rightand left is generally symmetric, non-sustained (lasting just a few beats), andabsent in all other gaze positions; theclassic nystagmus of cerebellar degen-eration looks similar but generally hasgreater intensity and is sustained. With
KEY POINT
h A provider who canconfidently recognizephysiologic nystagmus,nystagmus associatedwith cerebellardegeneration, vestibularneuritis, thedirection-changinghorizontal nystagmus ofacute stroke, andposterior canal benignparoxysmal positionalvertigo is already well onthe way to successfuldiagnosis of the patientwith neurovestibularsymptoms.
TABLE 2-2 Nystagmus Attributes Typically Described Duringa Neurovestibular Examination
b Baseline Attributes
Occurrence (eg, spontaneous [in primary gaze without provocation],gaze-evoked, positional)
Binocularity (monocular versus binocular)
Conjugacy (conjugate versus dysconjugate)
Waveform (jerk or pendular, the velocity profile of the slow phase [linear,increasing, decreasing])
Intensity (amplitude and frequency)
Plane or axis of rotation (in either head or eye coordinates)
Direction (by convention, the direction of jerk nystagmus is named for thefast-phase direction; for torsional quick phases, it is named for whetherthe top pole of the eye, ie, the 12 o’clock position, beats toward the rightor left ear)
Temporal profile of the nystagmus if it is nonsustained (eg, paroxysmalpositional nystagmus of a particular duration) or spontaneously varyingover time (eg, periodic alternating nystagmus)
Time since onset or age of first appearance if it is persistent (eg, infantile,adult-onset)
b Attributes Under Several Different Examination Conditions
Under different lighting or examiner viewing conditions (eg, eyes openversus closed, light versus dark, behind Frenzel lenses, with occlusiveophthalmoscopy)
In different gaze positions (ie, in all eight secondary and tertiary positionsof gaze; in different relative states of convergence or divergence)
Response of the nystagmus to various triggering or provocativemaneuvers (eg, shaking of the head, mastoid vibration, positioning)
1026 www.aan.com/continuum October 2012
Symptoms and Signs
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

far lateral gaze, particularly outside thebinocular field of vision where the noseobscures the medially placed eye’s view,a small number of healthy patients willalso demonstrate sustained physiologicnystagmus; in such cases, the nystag-mus will typically disappear when theeyes are brought back into the binoc-ular field, ie, less extreme gaze.
Supraphysiologic nystagmus evokedby eccentric gaze positions and absentin the primary position is often calledgaze-evoked nystagmus. Typically thenystagmus beats in the direction ofattempted gaze (eg, rightward in rightgaze), although it may be exclusivelyhorizontal, exclusively vertical, or evenasymmetric. If it is exclusively horizon-tal and symmetric, pathologic gaze-evoked nystagmus must be distin-guished from physiologic end-gaze nys-tagmus; if it is present when the eyesare only partially displaced, eg, within30- of the primary gaze position, itis invariably pathologic. On occasion,pathologic and physiologic forms aredifficult to distinguish. Gaze-evokednystagmus most often results from fail-ure of the central gaze-holding path-ways that generate (or calibrate) theextraocular muscle force required tosustain the eyes eccentrically againstthe normal elastic restoring forces ofthe orbital tissues, which bring the eyespassively back to near the midposition.If gaze-evoked nystagmus is purely ver-tical (upbeat or downbeat) or changesdirections in different gaze positions (eg,supraphysiologic, direction-changinghorizontal nystagmus), the localizationis almost invariably central. The cause,if structural, is usually located in the pos-terior fossa (eg, cerebellar degeneration,neoplasm, or stroke), although the toxiceffects of medications such as alcohol orantiepileptic medications are more com-mon. If the nystagmus is horizontal,asymmetric, unidirectional, and elicitedonly by gaze in one horizontal direction
(ie, right-beat nystagmus in right gaze orleft-beat nystagmus in left gaze, but notboth, and without vertical nystagmus onvertical gaze), it may either be central orperipheral and additional assessmentsare necessary to localize the cause.
Unmasking techniques that blockvisual fixation, such as use of Frenzelgoggles,68 occlusive ophthalmoscopy,or the penlight cover test,69 may beused to elicit nystagmus that has beensufficiently suppressed by visual fixationas to be unapparent clinically. Visualfixation reliably damps spontaneous pe-ripheral vestibular nystagmus.70 Whensuch nystagmus is very mild, it may becompletely suppressed by normal vi-sion.69 It is generally the case that pe-ripheral nystagmus is more robustlysuppressed than central nystagmus,although the absence of fixation sup-pression, suggesting a central lesion, ismore helpful diagnostically than itspresence. For example, many patientswith stroke causing acute vestibularsyndrome have nystagmus that is onlyapparent when fixation is blocked.71
Magnification, such as with direct oph-thalmoscopy, may also be used to iden-tify subtler, low-amplitude nystagmus.However, very subtle nystagmus, partic-ularly that seen only with fixationblocked, is more nonspecific and maybe seen under unremarkable circum-stances, eg, after smoking a cigarette.Characteristics of several important ves-tibular nystagmus forms are described inTable 2-3.72Y79
Many maneuvers are used by special-ists to trigger or provoke nystagmus insearch of particular diseases. Most ofthese are beyond the scope of this ar-ticle, but all neurologists should famil-iarize themselves with the Dix-Hallpikemaneuver (also sometimes called theNylen-B"r"ny maneuver, or other per-mutations of these eponyms). TheDix-Hallpike maneuver is a bedsidetest designed to provoke symptoms
KEY POINTS
h Pathologic gaze-evokednystagmus must bedistinguished fromphysiologic end-gazenystagmus. If thenystagmus is vertical,asymmetric, or presentwhen the eyes are onlypartially displaced toone side, it is almostinvariably pathologic.
h If the nystagmus ishorizontal, asymmetric,unidirectional, andelicited only by gaze inone horizontal direction,it may be either centralor peripheral.
h Peripheral nystagmusis more robustlysuppressed than centralnystagmus, althoughthe absence of fixationsuppression, suggestinga central lesion, is morehelpful diagnosticallythan its presence.
1027Continuum Lifelong Learning Neurol 2012;18(5):1016–1040 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

TABLE 2-3 Nystagmus Characteristics in Key Peripheral and Central Vestibular Disordersa
Vestibular Condition Test ManeuverNystagmusDuration
Trajectory/Direction
Variation inDirection
Positional Vestibular Symptoms (Episodic Nystagmus Triggered by Specific Positional Maneuvers)
Posterior canal benignparoxysmal positionalvertigo (BPPV)(È80%Y90% of BPPV)
Head hanging with45- turn to each side(Dix-Hallpike37)
È5Y30 seconds29 Upbeat-torsionalb
(torsion towarddownfacing ear)29
Direction reversaltypical on arising fromDix-Hallpike72
Horizontal canal BPPV(È10% to 15% of BPPV)
Supine roll withhead neutral(Pagnini-McClure37)c
È30Y90seconds29
Horizontald
(towarddownfacing earmuch more thantowardup-facing ear)29
Direction reversaltypical during test(when switching sidesor spontaneously)73
Central paroxysmalpositional vertigo
Either test positionor midline headhanging
È5Y60+ seconds;sometimessustained (ie,remains whilehead position ismaintained)74
Downbeat orhorizontal muchmore often thanupbeat, torsional,or mixed74j77
More often directioninvariant; occasionallyshifts trajectory ordirection with headposition76
Acute Vestibular Syndrome (Spontaneous Nystagmus That May Be Exacerbated Nonspecifically by VariousHead Maneuvers)
Vestibular neuritisor neurectomy
Gaze testing(increases withgaze toward thefast phase70)
Persistent,increases whenvisual fixationis blocked70,e
Dominantlyhorizontal Tsmall vertical ortorsionalcomponent70
Direction fixed duringfirst 24Y72 hours13;occasionally switchesdirection duringrecovery phase
Central acutevestibular syndrome(usually stroke)
Gaze testing (mayincrease with gazetoward eitherdirection78)
Persistent, mayincrease whenvisual fixationis blocked71,f
Dominantlyhorizontal muchmore often thanvertical, torsional,or mixed15
Acutely È38% directionchanging withhorizontal gazeposition,13 (mixedvestibular/gaze holding)
a Reprinted with permission from Newman-Toker DE, The neuro-ophthalmology virtual education library.32 novel.utah.edu/Newman-Toker/collection.php.
b A mixed upbeat-torsional vector during the Dix-Hallpike test is a reliable predictor of posterior canal BPPV, since this pattern is highlyatypical in central paroxysmal positional vertigo.74
c The conventional supine roll test for horizontal canal BPPV may also provoke dizziness in disorders triggered by lateral neck rotation(eg, carotid sinus hypersensitivity, rotational vertebral artery occlusion). Characteristic nystagmus brought on during a modified, ‘‘en-bloc’’ (head and body together) supine roll test should exclude either mimic and confirm horizontal canal BPPV.79
d Horizontal nystagmus elicited by positional testing, even when transient and triggered by the supine roll test, is not a specificindicator of horizontal canal BPPV since it can occur in other peripheral vestibular disorders and those with central lesions.77 Inquestionable cases, response to treatment can be used as a diagnostic confirmation, since central paroxysmal positional vertigosymptoms should not improve with canalith repositioning, as would be expected for BPPV.36
e Peripheral vestibular nystagmus generally obeys ‘‘Alexander’s law.’’ It increases in intensity when gaze is directed toward the fastphase and decreases in intensity when gaze is directed toward the slow phase. The nystagmus may only be apparent in lateral gazeto one side (first degree); be apparent in lateral gaze toward the fast phase and in the primary position (second degree); or beapparent in all three gaze positions (third degree).
f Contrary to popular belief, spontaneous nystagmus due to acute central lesions can be suppressed by visual fixation and unmaskedby fixation-blocking maneuvers.71 Unmasking of nystagmus (ie, presence of fixation suppression of the nystagmus) should only beconsidered a peripheral sign in acute vestibular syndrome when accompanied by a ‘‘safe’’ HINTS result.
1028 www.aan.com/continuum October 2012
Symptoms and Signs
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

and signs, ie, nystagmus, in patientswith positional dizziness or vertigo(Figure 2-1). The modern form of thetest was first described in detail by Dixand Hallpike in 1952. With minor adjust-ments to technique, the Dix-Hallpiketest remains the gold standard diagnos-tic test for the condition now known asBPPV of the posterior semicircular canal(p-BPPV).36,37 Note that the Dix-Hallpiketest is best thought of as a specific diag-nostic test for p-BPPV, and a differentdiagnostic maneuver is needed to accu-rately diagnose horizontal canal BPPV(Table 2-3).37 A nuanced point is thatthe Dix-Hallpike test, particularly if notperformed with the head fully hanging,can also trigger the horizontal nys-tagmus of BPPV of the horizontal canal.
The test may also be used in thediagnosis of central positional vertigosyndromes, in which case the nystag-mus is typically persistent downbeat,and as a nonspecific provocative ma-neuver to elicit vestibular nystagmus.Under most circumstances, the rare
anterior canal variant of BPPV, whichalso presents with positional downbeatnystagmus, should only be seriouslyentertained after neuroimaging by MRIhas excluded a posterior fossa structurallesion. The Dix-Hallpike test should notgenerally be performed in patients withacute, continuous vestibular symptoms,such as vertigo, nausea, vomiting, orhead motion intolerance, ie, acute ves-tibular syndrome. Such patients almostinvariably have spontaneous nystagmusat baseline, and exacerbation of symp-toms or nystagmus by the Dix-Hallpiketest offers no further probative diagnos-tic information inmost cases, although itmay be mistakenly thought to.8 If thetest is applied in a patient with mild orrecovering vestibular neuritis with min-imal or no spontaneous or gaze-evokednystagmus, a unidirectional and non-paroxysmal, horizontal pattern of nys-tagmus can be elicited. A preferredmethod to provoke nystagmus in suchpatients, however, would be repetitiveside-to-side head shaking.
KEY POINTS
h The Dix-Hallpike test isthe gold standarddiagnostic test for thecommon, posteriorcanal variant of benignparoxysmal positionalvertigo and should bethought of as a specifictest for this disorder. Adifferent diagnosticmaneuver is needed toaccurately diagnose theuncommon horizontalcanal variant. Diagnosinganterior canal benignparoxysmal positionalvertigo withoutneuroimaging by MRI isusually ill advised, givenhow closely the signsmimic central disease.
h The Dix-Hallpike testshould generally not beperformed in patientswith severe, acutevestibular syndromewho already havespontaneous nystagmus.An exacerbation ofsymptoms or signs maybe misinterpreted assupport for a benignparoxysmal positionalvertigo diagnosis.
FIGURE 2-1 DixYHallpike maneuver for diagnosis of right posterior semicircular canal benignparoxysmal positional vertigo. Step 1: Seat the patient on a table positioned sohe or she may be taken back to the head-hanging position with the neck in slight
extension. Stabilize the head with your hands and move the head 45- toward the side you willtest. Move the head, neck, and shoulders en bloc to the head-hanging position. Step 2: Observethe eyes; hold them open if necessary.
Reprinted from Fife TD, et al, Neurology.37 B 2008, with permission from American Academy of Neurology.www.neurology.org/content/70/22/2067.full?sid=32955bc5-714f-40af-8024-8846a127a47e.
1029Continuum Lifelong Learning Neurol 2012;18(5):1016–1040 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

The test method was recently de-scribed in an AAN practice parameterderived from an evidence-based reviewof canalith repositioning maneuvers37
and is reproduced in Figure 2-1. Be-cause this is a provocative test, thenormal response is no response (nosymptoms, no nystagmus). A specificpositive response is the developmentof vertigo or dizziness in conjunctionwith the classic p-BPPV nystagmus(p-BPPN).72 The classic p-BPPN80,81
has a mixed vertical-torsional vectorwith the eyes in the primary position,often with the more dominant vectorbeing vertical in one eye and torsionalin the other. The direction of the fastphase is a combined upbeat (ie, to-ward the brow) and ipsitorsional (ie,toward the side of the affected ear);thus, the 12 o’clock ‘‘pole’’ of the eyesmoves up and toward the right ear ina right p-BPPV. This pattern of trig-gered nystagmus is highly localizing tothe posterior semicircular canal andessentially excludes a central cause. Ifthe eyes are deviated laterally duringthe test, the nystagmus may appearalmost purely torsional (looking to-ward the affected ear) or vertical (look-ing away from the affected ear), but thedirection of the nystagmus fast phasewill not change. If the test is performedin the light without Frenzel goggles68
or another method to block visual fix-ation, the patient’s brain may be ableto suppress the vertical vector of thep-BPPN using vision, so the nystagmusmay appear almost purely torsional.Beyond the nystagmus vector and di-rection are several other nystagmusfeatures said to help discriminate be-tween p-BPPN and central mimics thatare often assessed during or on re-peated trials of the Dix-Hallpike test,although central mimics can be almostindistinguishable on each of these var-iables. The nystagmus should (1) notbegin immediately but after a short
latency (1 to 15 seconds); (2) damp af-ter 5 to 30 seconds; (3) reverse direc-tion, but not change vector, on arisingfrom the Dix-Hallpike position; and(4) fatigue on repeated trials, ie, pro-gressively disappear on successive at-tempts of the Dix-Hallpike test.
Vestibuloocular ReflexAlthough there are many ways to eval-uate labyrinthine function, the mostdirect is to assess the VOR. The VORserves to maintain stable visual fixationwhile the head is moving, particularlywhen the head is moving too quickly forsmooth visual pursuit mechanisms tokeep up. Although the VOR can betested in a number of ways, the twoprincipal bedside tests of VOR functionare dynamic visual acuity and the hori-zontal head-impulse test (h-HIT). Eachof these tests involves moving the headrapidly and assessing whether eyemovements respond appropriately.For dynamic visual acuity, the normalresponse is stable visual acuity asreported by the patient while the headis moved; for the h-HIT, the normalresponse is stable fixation on a target aswitnessed by the examiner.
Dynamic visual acuity testing gen-erally involves asking the patient toread an eye chart while the examineroscillates the head rapidly, either ver-tically or horizontally. Loss of three ormore lines of visual acuity (head mov-ing versus head stationary) indicatessome degree of vestibular failure.82
This approach requires less examinerskill to perform and interpret than theh-HIT but also offers less diagnosticinformationVit does not lateralize thelesion and is often normal in patientswith unilateral or partial vestibularfailure. The test is probably most ef-fective in identifying bilateral vestibularfailure83 and can be used to monitorpatients for aminoglycoside vestibulartoxicity.84
KEY POINTS
h The classic nystagmusof posterior canalbenign paroxysmalpositional vertigohas a mixedvertical-torsional vectorwith the fast phasebeating upward andtoward the shoulder onthe side of the affectedear. This pattern ofnystagmus is highlylocalizing to theposterior semicircularcanal and essentiallyexcludes a central cause.
h The two principalbedside tests ofvestibuloocular reflexfunction are dynamicvisual acuity andthe horizontalhead-impulse test.
1030 www.aan.com/continuum October 2012
Symptoms and Signs
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

In 1988, the h-HIT was described byHalmagyi and Curthoys85 as a bedsidetest for peripheral vestibular disease.This high-acceleration maneuver (whichmight be thought of as a ‘‘doll’s eyemaneuver on steroids’’) proved to becapable of identifying patients with ves-tibular failure in a way that classicoculocephalic maneuvers could not.Moreover, the test is able to interrogateeach ear separately because of a quirk ofnormal vestibular physiology in whichexcitatory responses carry more weightthan inhibitory responses. Since its orig-inal description, an abnormal h-HIT hasconsistently been shown to correlatewith ipsilateral vestibular hypofunctionand, more specifically, deafferentationof the inputs from the ipsilateral hori-zontal semicircular canal.85Y87 Althoughnot described further here, the h-HIThas since been adapted for use tointerrogate function of the two verticalsemicircular canals (anterior and poste-rior).87 Similar tests using a linear headmotion (the head-heave and head-surge tests) have also been developedto interrogate function of the linear-acceleration-detecting otolith organs(utricle and saccule).
The h-HIT, as originally described, isa rapid, passive head rotation from acenter to lateral (10- to 20-) position asa subject fixates at a central target, suchas the examiner’s nose. Technique isimportant in conducting the h-HIT, andit is generally advisable to watch themaneuver being performed by an expe-rienced examiner before attempting it.Instructional videos are available on theInternet (novel.utah.edu/Newman-Toker/collection.php). Since theresponse is linked to high accelerationrather than high velocity or amplitudeof the head rotation, the technique isproperly conducted with a quick flickof the examiner’s wrists over a veryshort amplitude. The examiner mustwarn the patient that the head will be
rotated very rapidly, and it is generallyadvisable to rotate the head slowly sev-eral times before conducting the high-acceleration maneuver and preparingthe patient by asking him or her torelax the neck. The test must be per-formed passively by the examiner,rather than actively by the patient, andthe direction of the impulse should bedisguised, eg, by using an inconsistentpattern of directions such as left-left-left-right-left-left-right-right-left. Failureto do so may result in a false-negativetest result through the production of‘‘covert saccades,’’ in which an antici-patory fast eye movement is uncon-sciously substituted for the abnormalVOR during the head rotation,making itimpossible for the examiner to detectthe abnormality.
The normal VOR response to a rapid,passive head rotation as a subject fixateson a central target is an equal and op-posite eye movement that keeps theeyes stationary in space (normal h-HIT).This is sometimes referred to as a VORgain equal to 1.0 (ratio of head rotationto eye rotation 1:1). An abnormal re-sponse occurs when the head is rapidlyrotated toward the side of a vestibularlesion. The loss of vestibular afferentinput results in the inability to main-tain fixation during the head rotation(gain less than 1.0), requiring a correc-tive gaze shift (‘‘refixation saccade’’)once the head stops moving in order toreacquire visual fixation on the centraltarget (abnormal h-HIT). A large-amplitude refixation saccade indicatesa very low VOR gain and substantialvestibular hypofunction. The test is ab-normal with lesions affecting the laby-rinth (eg, labyrinthitis or aminoglycosideototoxicity), vestibular nerve (eg, ves-tibular neuritis or surgical section), andlateral pons (eg, anterior inferior cere-bellar artery stroke or multiple sclerosisplaque). Somewhat paradoxically, a nor-mal response points to a central lesion
KEY POINTS
h An abnormalhead-impulsevestibuloocular reflexresults fromdeafferentation of theinputs from theipsilateral horizontalsemicircular canal,which is most often theresult of peripheralvestibular pathology,although lateral pontinelesions may produce thesame sign.
h The head-impulse testmust be performedpassively by theexaminer, rather thanactively by the patient,and the direction of theimpulse should bedisguised. Failure to doso may result in afalse-negative test.
h A normal head-impulsevestibuloocular reflexresponse usually pointsto a dangerous centrallesion (typically stroke)in patients presentingwith acute vestibularsyndrome. Note that itis counterintuitive thatthe normal finding isconsidered a ‘‘bad’’ signin this clinical context.
1031Continuum Lifelong Learning Neurol 2012;18(5):1016–1040 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

(usually stroke) in patients presentingwith acute vestibular syndrome becausemost patients with peripheral causesof acute vestibular syndrome have anabnormal response, but most with cen-tral causes do not (Case 2-2).13,15,71
A common adaptation of the h-HITis to displace the head laterally first,then rotate the head back to the cen-ter position. Some examiners find themaneuver easier to conduct using thiscentripetal head motion, and, moreimportantly, the results are easier tointerpret, especially in the presence ofspontaneous nystagmus. Asymmetricnystagmus often varies in intensity withhorizontal gaze position. With the cen-tripetal rotation, the globes end in the
primary position in the orbit regard-less of the h-HIT direction of rotation(rather than a laterally displaced posi-tion either right or left of the midline).Because the end position is the sameon the right and left, the impact ofany nystagmus on interpreting theh-HIT result is equivalent regardless ofthe side tested. Using a centripetal headrotation also reduces any theoreticalrisk of vertebral artery injury with neckoverrotation by an overzealous, inex-perienced examiner.
For the test to be effective, the pa-tient must be able to fixate steadily on avisual target and the extraocularmusclesshould be working normally. If thepatient is visually impaired (eg, blind,
KEY POINT
h Using a centripetal headrotation for thehead-impulse testreduces any theoreticalrisk of vertebral arteryinjury with neckoverrotation by anoverzealous,inexperienced examiner.
Case 2-2A 45-year-old man presented to the emergency department with 24 hours of new continuous vertigo,nausea, vomiting, and unsteady gait. He preferred to lie motionless. He denied auditory or neurologicsymptoms, headache, neck pain, or recent trauma. He had no relevant medical or exposure history,including no cerebrovascular or vestibular disorders, no recent or remote ear surgery, and no smokingor other vascular risk factors. He took no medications. He had no family history of vestibular diseaseor recurrent dizziness. The patient’s general neurologic examination was normal, including no limbataxia or dysmetria, compatible with a peripheral cause. He felt unsteady when standing but wasable to sit with arms crossed unaided. Eye examination revealed direction-fixed, left-beat, horizontalnystagmus that was worse in left gaze and no skew deviation on alternate cover testing. The h-HITwas normal bilaterally. MRI with diffusion-weighted imaging revealed a large acute left posteriorinferior cerebellar artery infarction. A complete search for cerebrovascular risk factors identified aleft vertebral artery dissection as the underlying cause of stroke. The patient was observed in thehospital while antithrombotic agents were initiated and was discharged uneventfully after the critical3-day window had passed, during which complications related to swelling were most likely. He made acomplete neurologic recovery.
Comment. This patient presented with the acute vestibular syndrome (continuous vertigo ordizziness lasting more than 1 day, accompanied by nausea or vomiting, head-motion intolerance,nystagmus, and unstable gait). The most likely etiology is vestibular neuritis, but dangerous causessuch as cerebellar stroke must be considered. The absence of vascular risk factors and his age youngerthan 50 reduce the risk of vertebrobasilar atherosclerosis, but vertebral artery dissection remains aconcern, mitigated incompletely by the absence of craniocervical pain. No auditory symptoms werepresent to raise concerns about inner ear ischemia, all compatible with a leading potential diagnosisof vestibular neuritis. The presence of a normal general neurologic examination is compatible withvestibular neuritis but does not exclude the possibility of a cerebellar infarction, since roughly halfof strokes causing this clinical presentation produce no neurologic signs. His direction-fixed,predominantly horizontal nystagmus and absence of skew deviation are also compatible with thebenign diagnosis, but also do not exclude possible stroke since more than half of such patients havethese ‘‘benign’’ oculomotor signs. The normal head-impulse result in the setting of acute vestibularsyndrome, however, strongly favors a stroke, despite the lack of other symptoms, signs, or risk factors.
1032 www.aan.com/continuum October 2012
Symptoms and Signs
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

severe refractive error without glasses orcontact lenses), cognitively impaired(eg, comatose, inattentive), or other-wise unable to consistently follow di-rections (eg, 2 years old or with alanguage barrier and no interpreter),the test cannot be performed. Evenawake, alert, and attentive patientsmust often be reminded to maintainvisual fixation during the testing; in-termittent inattentiveness can resultin extraneous refixation saccades thatcan bemisinterpreted, ie, false-positives.If the patient has extraocular muscleweakness, such as sixth nerve palsy, in-ternuclear ophthalmoplegia, or prioroculomotor surgery, h-HIT VOR testresults should be interpreted withcaution.
Additional Oculomotor TestingIn addition to a search for nystagmusand VOR testing, several other oculo-motor tests are typically performed inthe assessment of patients with vestib-ular symptoms. A search for ocularmisalignment by alternate cover testingis often warranted, particularly in pur-suit of skew deviation, ie, vertical ocularmisalignment of vestibular cause.Although skew deviation can resultfrom peripheral vestibular disease, it ismost often a central vestibular sign,particularly in patients with acute ves-tibular syndrome.15 If saccades (ie, fasteye movements) are abnormal in pa-tients with vestibular symptoms, thecause is usually central rather than pe-ripheral. The classic finding is saccadicdysmetria (ie, hypometric or hyper-metric saccades), which usually resultsfrom lesions of the cerebellum or itsconnections in the brainstem. Smoothpursuit eye movements may be choppyrather than smooth, often known assaccadic breakdown of smooth pursuit.This finding is somewhat nonspecific,but, when combined with direction-changing, gaze-evoked nystagmus, ver-
tical nystagmus, or failure of VORcancellation, it typically indicates cere-bellar or brainstem disease.35
The VOR is essential for maintainingstable vision on a target when the head ismoving, but the brain requires a mech-anism for suppressing the VOR duringcombined eye-head tracking, as in visu-ally pursuing a target in the distancemoving slowly from right to left, wherethe head and eyes rotate together, ratherthan in opposition. VOR cancellation ismanaged by the vestibulocerebellumand, in particular, the flocculus andparaflocculus. However, the task isaccomplished by a distributed networkof neurons that likely include contribu-tions from the parietal and frontal eyefields, as well as the dorsal pontinenuclei. Although many bedside tests ofcerebellar function are available, onlythree are typically abnormal in diseasespredominantly affecting the flocculusand paraflocculus (eg, Chiari I malfor-mation): (1) eccentric gaze holding;(2) visual smooth pursuit tracking; and(3) VOR cancellation.
The VOR cancellation test, alsoknown as the VOR suppression test,involves a combined eye-head trackingtask. It is typically accomplished asfollows: (1) While seated, the patient isasked to extend the arms directly infront of the body and clasp the handstogether with thumbs abducted andpointed toward the ceiling. (2) The pa-tient is then asked to visually fixate onthe thumbs and maintain that fixation.(3) The patient’s entire body is thenrotated en bloc from side to side. Therotation should cover an angle sweepof roughly 30- to either side of thestarting position with each 60- passlasting approximately 1.5 to 6 seconds(rotational velocity 10- to 40- per sec-ond). Several passes of increasing ve-locity should be examined to establishthe range within which the VOR can-celling system is able to compensate.
KEY POINT
h Although skewdeviation can resultfrom peripheralvestibular disease, it ismost often a centralvestibular sign,particularly in patientswith acute vestibularsyndrome.
1033Continuum Lifelong Learning Neurol 2012;18(5):1016–1040 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

This whole-body rotation is most easilyaccomplished using a swivel chair, al-though it can also be approximatedby asking the patient to twist at thewaist from a stationary seat. Particularlyin the latter case, the patient must beinstructed to keep the head, neck, andshoulders moving together as a unitand the thumbs straight in front of thebody and pointed toward the ceiling.Some physical instruction and assis-tance from the examiner are often re-quired. The test can be adapted for usein interrogating cancellation of the ver-tical VOR by using the same fixationtarget (outstretched thumbs) and as-sisting the patient through severalcycles of trunk flexion and extension.The normal response to the VORcancellation test is that the eyes remainstationary and motionless in the pri-mary position of gaze (midpositionwithin the orbits) throughout the mid-dle of each side-to-side pass. It is com-mon for normal subjects to slip offthe target and demonstrate a few jerksof what looks like nystagmus at the‘‘turns,’’ ie, during peak decelerationand acceleration. Patients with an abnor-mal response will develop vestibularnystagmus during the middle of eachrotational pass (fixed-velocity segment).This will occur at lower velocities and bemore pronounced in cases with moresevere failure of cancellation. For thetest be effective, the patient must beable to fixate steadily on a visual target(as with the tests of VOR functiondiscussed earlier) and should not havebaseline primary position nystagmus.Furthermore, the test is not meaningfulin patients who have completely lostVOR function (eg, aminoglycoside tox-icity), since there is nothing to suppress.
Additional Neurologic andGeneral ExaminationsSeveral aspects of the neurologic andgeneral examinations are typically rele-
vant in patients with vestibular symp-toms. As with general neurologicsymptoms, neurologic signs other thanaudiovestibular dysfunction and gaitimbalance are rare in benign periph-eral vestibular disorders. Long tract orcranial nerve signs almost always indi-cate a central cause, whether less ur-gent, such as multiple sclerosis, ormore urgent, such as stroke and brain-stem encephalitis.12,13 Many patientswith central causes, however, includingdangerous ones such as stroke, haveno such signs.13
Almost any general examination find-ing might prove to be diagnostic, eg, atender, swollen calf suggesting deep veinthrombosis leading to pulmonary embo-lism as a cause for dizziness, but somefindings should be sought routinely inpatients with vestibular symptoms.Aspects of the general examinationthat are of particular relevance in thosewith vertigo or dizziness include thefollowing: (1) measurement of heartrate and blood pressure, particularlyorthostatic vital signs in patients withsymptoms on arising or comparison ofblood pressures in the two arms incases of suspected subclavian steal88
or other upper thoracic vascular path-ology; (2) cardiac auscultation forsignificant valvular murmurs; and(3) inspection of the ear (pinna, mas-toid) and otic fundus by otoscopy forsigns of trauma, infection, or neoplasm.
Syndrome-Specific Approachesto ExaminationIn aggregate, a focused examinationapproach is usually warranted basedon the vestibular syndrome in question.Patients with spontaneous, episodicsymptoms usually have no obvioussigns, but those with episodic positional,acute prolonged, or chronic persistentsymptoms may have examination cluesto the underlying localization or diagno-sis. For positional vestibular symptoms,
KEY POINT
h Long tract or cranialnerve signsaccompanyingvestibular symptomsindicate a central cause.Many patients withcentral causes, however,including dangerousones such as stroke,have no such signs.
1034 www.aan.com/continuum October 2012
Symptoms and Signs
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
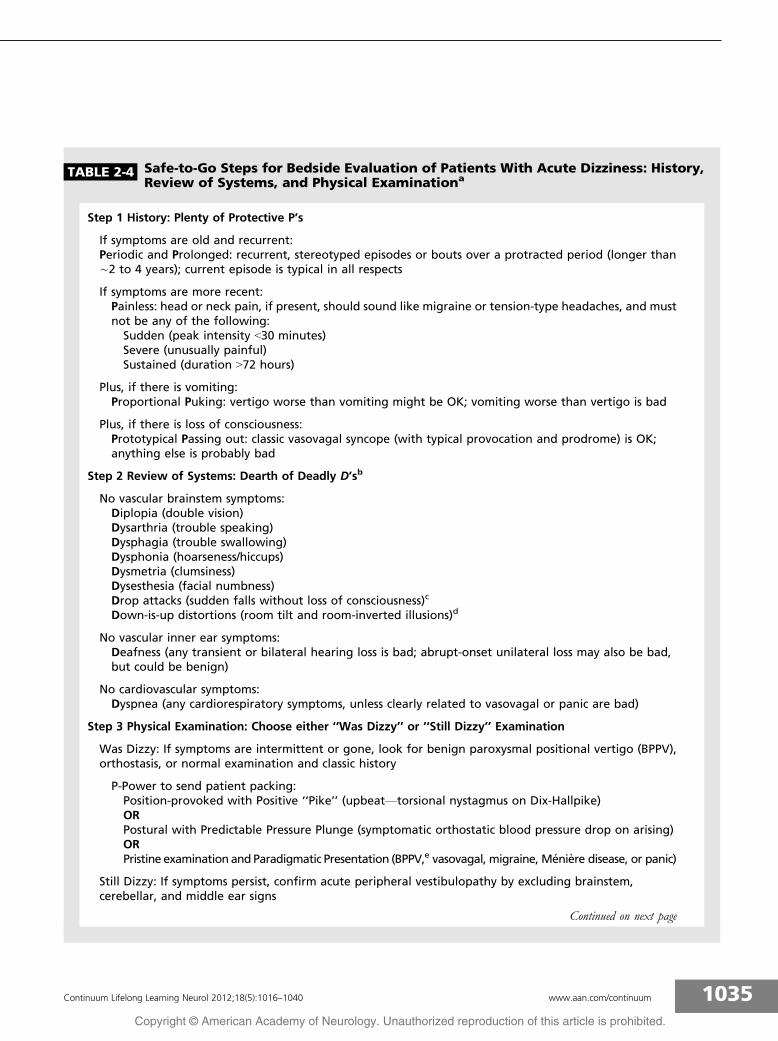
TABLE 2-4 Safe-to-Go Steps for Bedside Evaluation of Patients With Acute Dizziness: History,Review of Systems, and Physical Examinationa
Step 1 History: Plenty of Protective P’s
If symptoms are old and recurrent:Periodic and Prolonged: recurrent, stereotyped episodes or bouts over a protracted period (longer thanÈ2 to 4 years); current episode is typical in all respects
If symptoms are more recent:Painless: head or neck pain, if present, should sound like migraine or tension-type headaches, and mustnot be any of the following:Sudden (peak intensity G30 minutes)Severe (unusually painful)Sustained (duration 972 hours)
Plus, if there is vomiting:Proportional Puking: vertigo worse than vomiting might be OK; vomiting worse than vertigo is bad
Plus, if there is loss of consciousness:Prototypical Passing out: classic vasovagal syncope (with typical provocation and prodrome) is OK;anything else is probably bad
Step 2 Review of Systems: Dearth of Deadly D’sb
No vascular brainstem symptoms:Diplopia (double vision)Dysarthria (trouble speaking)Dysphagia (trouble swallowing)Dysphonia (hoarseness/hiccups)Dysmetria (clumsiness)Dysesthesia (facial numbness)Drop attacks (sudden falls without loss of consciousness)c
Down-is-up distortions (room tilt and room-inverted illusions)d
No vascular inner ear symptoms:Deafness (any transient or bilateral hearing loss is bad; abrupt-onset unilateral loss may also be bad,but could be benign)
No cardiovascular symptoms:Dyspnea (any cardiorespiratory symptoms, unless clearly related to vasovagal or panic are bad)
Step 3 Physical Examination: Choose either ‘‘Was Dizzy’’ or ‘‘Still Dizzy’’ Examination
Was Dizzy: If symptoms are intermittent or gone, look for benign paroxysmal positional vertigo (BPPV),orthostasis, or normal examination and classic history
P-Power to send patient packing:Position-provoked with Positive ‘‘Pike’’ (upbeatVtorsional nystagmus on Dix-Hallpike)ORPostural with Predictable Pressure Plunge (symptomatic orthostatic blood pressure drop on arising)ORPristine examination and Paradigmatic Presentation (BPPV,e vasovagal, migraine, Meniere disease, or panic)
Still Dizzy: If symptoms persist, confirm acute peripheral vestibulopathy by excluding brainstem,cerebellar, and middle ear signs
Continued on next page
1035Continuum Lifelong Learning Neurol 2012;18(5):1016–1040 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

provocative positional testing to elicitnystagmus (eg, Dix-Hallpike) and ortho-static cardiovascular assessment are war-ranted. For acute vestibular syndrome,VOR assessment by h-HIT, a search fordirection-changing nystagmus, and alter-nate cover testing for skew deviation arethe signs most likely to discriminatecentral from peripheral causes.13 Thisthree-test oculomotor battery has beengiven the acronym HINTS (head
impulse, nystagmus, test of skew) withthe findings predicting stroke given theacronym INFARCT (impulse normal,fast-phase alternating, refixation oncover test).15 For chronic persistent ves-tibular symptoms, VOR testing by h-HITor dynamic visual acuity combined withassessments for cerebellar-type oc-ulomotor abnormalities, such as gaze-evoked horizontal nystagmus, verticalnystagmus, impaired smooth pursuit,
TABLE 2-4 Continued
IF SAFE AND CLEAR THEN I’LL SEND HIM ON HOMEf
Intact Fields (no visual field cut)Stands Alone (able to stand unassisted)Face Even (no weakness, droop, or ptosis)CLear Enunciation (no slurred or hoarse speech)Accurate Reaching (no drift; normal reaching, rapid alternating movements)THErmal Normal (equal thermal or sharp sense)Isocoria in Low Light (equal pupils in dim light)g
Straight Eyes (normal ocular alignment, especially vertical)h
No Deafness (no moderate to severe hearing loss)Head Impulse Misses (abnormal h-HIT)i
One-way Nystagmus (unidirectional, horizontal)j
HealthyOtic andMastoid Examination (pearly; no pimples, pus, perforation, or pain on palpation of mastoid)a Modified with permission from Newman-Toker DE, The neuro-ophthalmology virtual education library.32 novel.utah.edu/Newman-Toker/collection.php.
b Deadly D’s should be excluded both by review of systems and corresponding examination, eg, diplopia and ocular misalignment.c Drop attacks are common in patients with Meniere disease and occasionally seen in patients with other inner ear diseases.89
However, in the absence of a clear Meniere disease history, they should spark concern for an underlying cerebrovascular orcardiovascular90 etiology for dizziness/vertigo. Although drop attacks are also seen in epilepsy and narcolepsy-cataplexy, in suchcases, they are generally not associated with dizziness.
d Room tilt illusions have been reported in patients with Meniere and other inner ear diseases, but, in the absence of a convincinghistory pointing to otic involvement (eg, fluctuating tinnitus with recurrent attacks, symptoms provoked by noise, progressive low-frequency hearing loss), a cerebrovascular cause should be surmised.
e Since BPPV may resolve on its own, a typical history alone is sometimes considered sufficient for diagnosis. However, care shouldbe taken to ensure that episodes were reliably triggered by adopting the head positions, rather than exacerbated by headmovement after a spontaneous, episodic onset of symptoms (more typical of TIA).
f The ‘‘IF SAFE&CLEAR THEN I’LL SENDHIMONHOME’’ acronym can be abridged to ‘‘SENDHIMONHOME’’ bymandating that a thoroughgeneral neurologic examination be normal. ‘‘SEND HIM ON HOME’’ is ‘‘HINTS’’ plus normal hearing and a normal ear examination.
g Pupils must be examined in dim light, since the anisocoria of Horner syndrome (suggesting brainstem pathology in this clinicalcontext) is usually only apparent in dim light or darkness. Note that even in low light, the amount of anisocoria is typically less than2 mm, and any associated ptosis or anhidrosis is also subtle.
h Clinically evident skew deviation (vertical misalignment of vestibular cause) has been reported in occasional patients with peripheralvestibular lesions, but, in the context of acute vestibular syndrome, skew is a strong predictor of stroke.13 Unfortunately, the converse isnot true, since most strokes presenting with acute vestibular syndrome have normal vertical ocular alignment clinically.13 Thus, normalvertical ocular alignment is necessary but not sufficient for a safe-to-go departure.
i An abnormal h-HIT is seen in most cases of vestibular neuritis but also in some stroke patients (particularly those with lateralpontine involvement). Therefore, in patients with acute vestibular syndrome, the abnormal impulse is necessary but not sufficientfor a safe-to-go departure.
j In acute vestibular syndrome, peripheral nystagmus should be predominantly horizontal and direction-fixed, regardless of gazeposition. Direction-changing, gaze-evoked nystagmus is highly suggestive of brainstem or cerebellar stroke.13 Unfortunately, theconverse is not true, since most strokes presenting with acute vestibular syndrome have unidirectional nystagmus mimickingvestibular neuritis.15,41,71,91Y93 So unidirectional nystagmus is necessary but not sufficient for a safe-to-go departure.
1036 www.aan.com/continuum October 2012
Symptoms and Signs
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
VOR cancellation failure, and saccadicdysmetria, is likely to be the most ef-fective strategy.
CONCLUSIONSA careful history and physical exam-ination will generally permit accuratediagnosis of patients presenting withvestibular symptoms. Patients with con-ditions producing vestibular symptomslasting seconds to hours are rarelysymptomatic at the time of initial as-sessment. If they are still symptomatic,it is generally with intermittent symp-toms triggered by certain actions, suchas head movement and standing upquickly. By contrast, patients with con-ditions producing vestibular symptomslasting for days to weeks are usuallysymptomatic at the time of initial as-sessment. This clinical distinction iscrucial, since the expected bedsideexamination findings differ dramaticallybetween the two groups. In the formergroup, with transient or intermittentsymptoms, the physician should usephysical examination maneuvers toprovoke symptoms and signs butshould not be surprised to find acompletely normal examinationVhere,often the history offers the only clueto differentiate between common,benign causes and their dangerousmimics. In the latter group, with persis-tent and continuous symptoms, thephysician should expect the physicalexamination findings to distinguishbetween benign causes and dangerouscauses and should be surprised if theydo not. More importantly, distinguish-ing the ‘‘were dizzy’’ from the ‘‘stilldizzy’’ patients allows the examiner torapidly and confidently determine whois at risk of serious underlying dis-ease. Table 2-4 89Y93 shows a compositesummary of the critical history and ex-amination techniques necessary to de-termine a benign cause under these twocrucial scenarios.
REFERENCES1. Bisdorff A, Von Brevern M, Lempert T,
Newman-Toker DE. Classification ofvestibular symptoms: towards aninternational classification of vestibulardisorders. J Vestib Res 2009;19(1Y2):1Y13.
2. Task Force for theDiagnosis andManagementof Syncope, European Society of Cardiology(ESC), European Heart Rhythm Association(EHRA), et al. Guidelines for the diagnosisand management of syncope (version 2009).Eur Heart J 2009;30(21):2631Y2671.
3. Newman-Toker DE, Hsieh YH, Camargo CAJr, et al. Spectrum of dizziness visits to USemergency departments: cross-sectionalanalysis from a nationally representativesample. Mayo Clin Proc 2008;83(7):765Y775.
4. Newman-Toker DE. ProQuest: Dissertations &Theses. Diagnosing dizziness in the emergencydepartment: why ‘‘What do you mean by‘dizzy’?’’ should not be the first question youask, gateway.proquest.com/openurl?url_ver=Z39.88-2004&res_dat=xri:pqdiss&rft_val_fmt=info:ofi/fmt:kev:mtx:dissertation&rft_dat=xri:pqdiss:3267879. Published 2007.Accessed April 18, 2012.
5. DrachmanDA.A 69-year-oldmanwith chronicdizziness. JAMA 1998;280(24):2111Y2118.
6. Drachman DA, Hart CW. An approach tothe dizzy patient. Neurology 1972;22(4):323Y334.
7. Newman-Toker DE. Charted records of dizzypatients suggest emergency physiciansemphasize symptom quality in diagnosticassessment. Ann Emerg Med 2007;50(2):204Y205.
8. Stanton VA, Hsieh YH, Camargo CA Jr, et al.Overreliance on symptom quality indiagnosing dizziness: results of a multicentersurvey of emergency physicians. Mayo ClinProc 2007;82(11):1319Y1328.
9. Newman-Toker DE, Cannon LM, StofferahnME, et al. Imprecision in patient reports ofdizziness symptom quality: a cross-sectionalstudy conducted in an acute care setting.Mayo Clin Proc 2007;82(11):1329Y1340.
10. Newman-Toker DE, Camargo CA Jr.‘Cardiogenic vertigo’Vtrue vertigo as thepresenting manifestation of primary cardiacdisease. Nat Clin Pract Neurol 2006;2(3):167Y172; quiz 173.
11. Newman-Toker DE, Dy FJ, Stanton VA, et al.How often is dizziness from primarycardiovascular disease true vertigo? Asystematic review. J Gen Intern Med 2008;23(12):2087Y2094.
12. Cheung CS, Mak PS, Manley KV, et al.Predictors of important neurological causes
KEY POINTS
h A safe (benign) HINTSresult in acute vestibularsyndrome is a unilaterallyabnormal horizontalhead-impulse testplus direction-fixed,predominantly horizontalnystagmus plus normalvertical ocular alignmenton alternate cover test.The nystagmus mustbeat away from the sideof the abnormal impulseand should not changedirection in different gazepositions or duringprovocative testing (eg,positional maneuvers orhead shaking).
h For spontaneous, episodicvestibular symptoms,emphasize the historyover the examination. Forpositional symptoms, usethe Dix-Hallpikemaneuverand orthostatic vital signs.For acute vestibularsyndrome, test for HINTSto INFARCT. For chronic,persistent vestibularsymptoms, focus oncerebellar eye signs.
h With transient orintermittent symptoms,the physician shoulduse physical examinationmaneuvers to provokesymptoms and signs butshould not be surprisedto find a completelynormal examination.With persistent andcontinuous symptoms,the physician shouldexpect that the physicalexamination findingswill usually distinguishbetween benign causesand dangerous causesand be surprised if theydo not.
1037Continuum Lifelong Learning Neurol 2012;18(5):1016–1040 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

of dizziness among patients presenting tothe emergency department. Emerg Med J2010;27(7):517Y521.
13. Tarnutzer AA, Berkowitz AL, Robinson KA,et al. Does my dizzy patient have a stroke?A systematic review of bedside diagnosis inacute vestibular syndrome. CMAJ 2011;183(9):E571YE592.
14. Hotson JR, Baloh RW. Acute vestibularsyndrome. N Engl JMed 1998;339(10):680Y685.
15. Kattah JC, Talkad AV, Wang DZ, et al. HINTSto diagnose stroke in the acute vestibularsyndrome: three-step bedside oculomotorexamination more sensitive than early MRIdiffusion-weighted imaging. Stroke 2009;40(11):3504Y3510.
16. Blakley BW, Goebel J. The meaning of theword ‘‘vertigo’’. Otolaryngol Head NeckSurg 2001;125(3):147Y150.
17. Delaney KA. Bedside diagnosis of vertigo:value of the history and neurologicalexamination. Acad Emerg Med 2003;10(12):1388Y1395.
18. Cappello M, di Blasi U, di Piazza L, et al.Dizziness and vertigo in a department ofemergency medicine. Eur J Emerg Med1995;2(4):201Y211.
19. Yardley L, Owen N, Nazareth I, Luxon L.Panic disorder with agoraphobia associatedwith dizziness: characteristic symptoms andpsychosocial sequelae. J Nerv Ment Dis2001;189(5):321Y327.
20. Hsu LC. Isolated dizziness/vertigo, vascularrisk factors and stroke. Acta Neurol Taiwan2011;20(2):75Y76.
21. Kayan A, Hood JD. Neuro-otologicalmanifestations of migraine. Brain 1984;107(pt 4):1123Y1142.
22. Vukovic V, Plavec D, Galinovic I, et al.Prevalence of vertigo, dizziness, andmigrainous vertigo in patients withmigraine. Headache 2007;47(10):1427Y1435.
23. Neuhauser HK, Lempert T. Vertigo:epidemiologic aspects. Semin Neurol 2009;29(5):473Y481.
24. Radtke A, Lempert T, von Brevern M, et al.Prevalence and complications of orthostaticdizziness in the general population. ClinAuton Res 2011;21(3):161Y168.
25. Nozawa I, Imamura S, Hashimoto K,Murakami Y. Psychosomatic aspects ofpatients complaining of dizziness or vertigowith orthostatic dysregulation. Auris NasusLarynx 1998;25(1):33Y38.
26. Anagnostou E, Spengos K, Vassilopoulou S,et al. Incidence of rotational vertigo in
supratentorial stroke: a prospective analysisof 112 consecutive patients. J Neurol Sci2010;290(1Y2):33Y36.
27. Kerber KA, Fendrick AM. The evidence basefor the evaluation and management ofdizziness. J Eval Clin Pract 2010;16(1):186Y191.
28. Clark MR, Sullivan MD, Fischl M, et al.Symptoms as a clue to otologic and psychiatricdiagnosis in patients with dizziness. JPsychosom Res 1994;38(5):461Y470.
29. Aw ST, Todd MJ, Aw GE, et al. Benignpositional nystagmus: a study of itsthree-dimensional spatio-temporalcharacteristics. Neurology 2005;64(11):1897Y1905.
30. Neuhauser H, Leopold M, von Brevern M,et al. The interrelations of migraine, vertigo,and migrainous vertigo. Neurology 2001;56(4):436Y441.
31. Havia M, Kentala E. Progression ofsymptoms of dizziness in Meniere’s disease.Arch Otolaryngol Head Neck Surg 2004;130(4):431Y435.
32. Newman-Toker DE. The David Newman-Tokerneuro-ophthalmology collection. TheNeuro-ophthalmology Virtual EducationLibrary. novel.utah.edu/Newman-Toker/collection.php. Accessed April 18, 2012.
33. Furman JM, Marcus DA, Balaban CD.Migrainous vertigo: development of apathogenetic model and structureddiagnostic interview. Curr Opin Neurol2003;16(1):5Y13.
34. Tinetti ME, Williams CS, Gill TM. Dizzinessamong older adults: a possible geriatricsyndrome. Ann Intern Med 2000;132(5):337Y344.
35. Leigh RJ, Zee DS. The neurology of eyemovements. 4th ed. New York, NY: OxfordUniversity Press, 2006.
36. Bhattacharyya N, Baugh RF, Orvidas L, et al.Clinical practice guideline: benign paroxysmalpositional vertigo. Otolaryngol Head NeckSurg 2008;139(5 suppl 4):S47YS81.
37. Fife TD, Iverson DJ, Lempert T, et al. Practiceparameter: therapies for benign paroxysmalpositional vertigo (an evidence-based review):report of the Quality StandardsSubcommittee of the American Academyof Neurology. Neurology 2008;70(22):2067Y2074.
38. von Brevern M, Radtke A, Clarke AH,Lempert T. Migrainous vertigo presenting asepisodic positional vertigo. Neurology 2004;62(3):469Y472.
39. Vilela MD, Goodkin R, Lundin DA, Newell DW.Rotational vertebrobasilar ischemia:
1038 www.aan.com/continuum October 2012
Symptoms and Signs
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

hemodynamic assessment and surgicaltreatment. Neurosurgery 2005;56(1):36Y43;discussion 43Y45.
40. Rane NJ, McAuley D. Vertebral arterydissection presenting as isolated vertigo.Emerg Med J 2007;24(10):732.
41. Kase CS, Norrving B, Levine SR, et al.Cerebellar infarction. Clinical and anatomicobservations in 66 cases. Stroke 1993;24(1):76Y83.
42. Fisher CM. Vomiting out of proportion todizziness in ischemic brainstem strokes.Neurology 1996;46(1):267.
43. Kerber KA, Brown DL, Lisabeth LD, et al.Stroke among patients with dizziness,vertigo, and imbalance in the emergencydepartment: a population-based study.Stroke 2006;37(10):2484Y2487.
44. Culic V, Miric D, Eterovic D. Correlationbetween symptomatology and site of acutemyocardial infarction. Int J Cardiol 2001;77(2Y3):163Y168.
45. Low PA, Opfer-Gehrking TL, McPhee BR,et al. Prospective evaluation of clinicalcharacteristics of orthostatic hypotension.Mayo Clin Proc 1995;70(7):617Y622.
46. Newman-Toker DE, Reich SG. Wrong-Waynystagmus in the AICA syndrome.Laryngoscope 2008;118(2):378Y379.
47. Silbert PL, Mokri B, Schievink WI. Headacheand neck pain in spontaneous internalcarotid and vertebral artery dissections.Neurology 1995;45(8):1517Y1522.
48. Edlow JA, Newman-Toker DE, Savitz SI.Diagnosis and initial management ofcerebellar infarction. Lancet Neurol 2008;7(10):951Y964.
49. Savitz SI, Caplan LR, Edlow JA. Pitfalls in thediagnosis of cerebellar infarction. AcadEmerg Med 2007;14(1):63Y68.
50. de Sousa JE, Halfon MJ, Bonardo P, et al.Different pain patterns in patients withvertebral artery dissections. Neurology 2005;64(5):925Y926.
51. Quinn JV, Stiell IG, McDermott DA, et al.Derivation of the San Francisco Syncope Ruleto predict patients with short-term seriousoutcomes. Ann Emerg Med 2004;43(2):224Y232.
52. Kung SW, Ng WS, Ng MH. Aortic dissectionin an accident and emergency departmentin Hong Kong. Hong Kong Med J 2007;13(2):122Y130.
53. Romme JJ, van Dijk N, Boer KR, et al.Influence of age and gender on the
occurrence and presentation of reflexsyncope. Clin Auton Res 2008;18(3):127Y133.
54. Kirchmann M, Thomsen LL, Olesen J.Basilar-type migraine: clinical, epidemiologic,and genetic features. Neurology 2006;66(6):880Y886.
55. Grad A, Baloh RW. Vertigo of vascularorigin. Clinical and electronystagmographicfeatures in 84 cases. Arch Neurol 1989;46(3):281Y284.
56. Schwarz S, Egelhof T, Schwab S, Hacke W.Basilar artery embolism. Clinical syndromeand neuroradiologic patterns in patientswithout permanent occlusion of the basilarartery. Neurology 1997;49(5):1346Y1352.
57. Garewal M, Selhorst JB. Subclavian arterydissection and triple infarction of the nervoussystem. Arch Neurol 2005;62(12):1917Y1919.
58. Demiryoguran NS, Karcioglu O, TopacogluH, Aksakalli S. Painless aortic dissection withbilateral carotid involvement presentingwith vertigo as the chief complaint. EmergMed J 2006;23(2):e15.
59. Kelly PJ, Toker DE, Boyer P, et al.Granulomatous compressive thoracicmyelopathy as the initial manifestation ofWegener’s granulomatosis. Neurology 1998;51(6):1769Y1770.
60. Kanner AM. Ictal panic and interictal panicattacks: diagnostic and therapeutic principles.Neurol Clin 2011;29(1):163Y175, ix.
61. Jaap AJ, Jones GC, McCrimmon RJ, et al.Perceived symptoms of hypoglycaemia inelderly type 2 diabetic patients treated withinsulin. Diabet Med 1998;15(5):398Y401.
62. Ossipova VV, Kolosova OA, Vein AM.Migraine associated with panic attacks.Cephalalgia 1999;19(8):728Y731.
63. Yen JC, Chan L, Lai YJ. Vertebral arterydissection presented as lateral medullarysyndrome in a patient with migraine: a casereport. Acta Neurol Taiwan 2010;19(4):275Y280.
64. Megerian CA, Hadlock TA. Case records ofthe Massachusetts General; Hospital. Weeklyclinicopathological exercises. Case 40-2001.An eight-year-old boy with fever, headache,and vertigo two days after aural trauma. NEngl J Med 2001;345(26):1901Y1907.
65. Juntunen J. Neurotoxic syndromes andoccupational exposure to solvents. EnvironRes 1993;60(1):98Y111.
66. Lee H, Jen JC, Cha YH, et al. Phenotypicand genetic analysis of a large family withmigraine-associated vertigo. Headache 2008;48(10):1460Y1467.
1039Continuum Lifelong Learning Neurol 2012;18(5):1016–1040 www.aan.com/continuum
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.

67. Jen JC. Recent advances in the genetics ofrecurrent vertigo and vestibulopathy. CurrOpin Neurol 2008;21(1):3Y7.
68. Hain TC. Frenzel goggles and relateddevices. www.dizziness-and-balance.com/practice/images/equipment/frenzels.htm.Modified November 21, 2009. Accessed April18, 2012.
69. Newman-Toker DE, Sharma P, ChowdhuryM, et al. Penlight-cover test: a new bedsidemethod to unmask nystagmus. J NeurolNeurosurg Psychiatry 2009;80(8):900Y903.
70. Bohmer A, Straumann D, Fetter M.Three-dimensional analysis of spontaneousnystagmus in peripheral vestibularlesions. AnnOtol Rhinol Laryngol 1997;106(1):61Y68.
71. Newman-Toker DE, Kattah JC, Alvernia JE,Wang DZ. Normal head impulse testdifferentiates acute cerebellar strokes fromvestibular neuritis. Neurology 2008;70(24 pt 2):2378Y2385.
72. Baloh RW, Honrubia V, Jacobson K. Benignpositional vertigo: clinical and oculographicfeatures in 240 cases. Neurology 1987;37(3):371Y378.
73. Nuti D, Mandala M, Salerni L. Lateral canalparoxysmal positional vertigo revisited.Ann N Y Acad Sci 2009;1164:316Y323.
74. Lawson J, Bamiou DE, Cohen HS, Newton J.Positional vertigo in a Falls Service. AgeAgeing 2008;37(5):585Y589.
75. Chang MB, Bath AP, Rutka JA. Are allatypical positional nystagmus patternsreflective of central pathology?J Otolaryngol 2001;30(5):280Y282.
76. Bertholon P, Tringali S, Faye MB, et al.Prospective study of positional nystagmus in100 consecutive patients. Ann Otol RhinolLaryngol 2006;115(8):587Y594.
77. Johkura K. Central paroxysmal positionalvertigo: isolated dizziness caused by smallcerebellar hemorrhage. Stroke 2007;38(6):e26Ye27; author reply e28.
78. Morita S, Suzuki M, Iizuka K. False-negativediffusion-weighted MRI in acute cerebellarstroke. Auris Nasus Larynx 2011;38(5):577Y582.
79. Heidenreich KD, Carender WJ, HeidenreichMJ, Telian SA. Strategies to distinguishbenign paroxysmal positional vertigo fromrotational vertebrobasilar ischemia. AnnVasc Surg 2010;24(4):553.e1Y553.e5.
80. Fetter M, Sievering F. Three-dimensional(3-D) eye movement analysis in patients with
positioning nystagmus. Acta OtolaryngolSuppl 1995;520(pt 2):369Y371.
81. Cremer PD, Migliaccio AA, Pohl DV, et al.Posterior semicircular canal nystagmus isconjugate and its axis is parallel to that of thecanal. Neurology 2000;54(10):2016Y2020.
82. Longridge NS, Mallinson AI. A discussion ofthe dynamic illegible ‘‘E’’ test: a newmethod of screening for aminoglycosidevestibulotoxicity. Otolaryngol Head NeckSurg 1984;92(6):671Y677.
83. Zingler VC, Cnyrim C, Jahn K, et al. Causativefactors and epidemiology of bilateralvestibulopathy in 255 patients. Ann Neurol2007;61(6):524Y532.
84. Ariano RE, Zelenitsky SA, Kassum DA.Aminoglycoside-induced vestibular injury:maintaining a sense of balance. AnnPharmacother 2008;42(9):1282Y1289.
85. Halmagyi GM, Curthoys IS. A clinical signof canal paresis. Arch Neurol 1988;45(7):737Y739.
86. Aw ST, Fetter M, Cremer PD, et al. Individualsemicircular canal function in superior andinferior vestibular neuritis. Neurology2001;57(5):768Y774.
87. Halmagyi GM, Aw ST, Cremer PD, et al.Impulsive testing of individual semicircularcanal function. Ann N Y Acad Sci 2001;942:192Y200.
88. Smith JM, Koury HI, Hafner CD, Welling RE.Subclavian steal syndrome. A review of 59consecutive cases. J Cardiovasc Surg (Torino)1994;35(1):11Y14.
89. Brantberg K, Ishiyama A, Baloh RW. Dropattacks secondary to superior canaldehiscence syndrome. Neurology 2005;64(12):2126Y2128.
90. Parry SW, Kenny RA. Drop attacks in olderadults: systematic assessment has a highdiagnostic yield. J Am Geriatr Soc 2005;53(1):74Y78.
91. Norrving B, Magnusson M, Holtas S. Isolatedacute vertigo in the elderly; vestibular orvascular disease? Acta Neurol Scand 1995;91(1):43Y48.
92. Lee H, Sohn SI, Cho YW, et al. Cerebellarinfarction presenting isolated vertigo:frequency and vascular topographicalpatterns. Neurology 2006;67(7):1178Y1183.
93. Cnyrim CD, Newman-Toker D, Karch C, et al.Bedside differentiation of vestibular neuritisfrom central ‘‘vestibular pseudoneuritis’’.J Neurol Neurosurg Psychiatry 2008;79(4):458Y460.
1040 www.aan.com/continuum October 2012
Symptoms and Signs
Copyright @ American Academy of Neurology. Unauthorized reproduction of this article is prohibited.