Sickle Cell Disease: New Approaches and Guidelines Developed as part of a collaboration of CCNC, the...
35
Sickle Cell Disease: New Approaches and Guidelines Developed as part of a collaboration of Developed as part of a collaboration of CCNC, the NC Division of Public Health, CCNC, the NC Division of Public Health, the comprehensive sickle cell centers at the comprehensive sickle cell centers at Carolinas Health Care, Duke University, Carolinas Health Care, Duke University, East Carolina University, University of East Carolina University, University of North Carolina at Chapel Hill, Mission, North Carolina at Chapel Hill, Mission, and Wake Forest University and primary and Wake Forest University and primary care physicians across North Carolina. care physicians across North Carolina. Adapted from the NIHLBI guidelines Adapted from the NIHLBI guidelines
-
Upload
alvin-gilmore -
Category
Documents
-
view
218 -
download
0
Transcript of Sickle Cell Disease: New Approaches and Guidelines Developed as part of a collaboration of CCNC, the...

Sickle Cell Disease: New Approaches and
Guidelines
Developed as part of a collaboration of CCNC, Developed as part of a collaboration of CCNC, the NC Division of Public Health, the the NC Division of Public Health, the
comprehensive sickle cell centers at Carolinas comprehensive sickle cell centers at Carolinas Health Care, Duke University, East Carolina Health Care, Duke University, East Carolina University, University of North Carolina at University, University of North Carolina at
Chapel Hill, Mission, and Wake Forest Chapel Hill, Mission, and Wake Forest University and primary care physicians across University and primary care physicians across
North Carolina. Adapted from the NIHLBI North Carolina. Adapted from the NIHLBI guidelinesguidelines

ObjectivesObjectives
Provide basic overview of Sickle Cell Disease
Understand recommendations for care based on 2014 NHLBI guidelines Health Maintenance Acute Problems
Introduce tools to facilitate adoption of recommendations
Foster specialist and primary care collaboration in care of patients with sickle cell disease

Sickle Cell Disease (SCD)Sickle Cell Disease (SCD) SCD refers to a group of disorders SCD refers to a group of disorders
characterized by a predominance of characterized by a predominance of HbSHbS
SCD affects 1 in 375 African American SCD affects 1 in 375 African American live births, as well as other populationslive births, as well as other populations
Includes HbSS, HbSC, HbS/Includes HbSS, HbSC, HbS/thalassemia thalassemia ((00+)+), HbS/Other, HbS/Other
Sickle Cell Anemia (SCA) Sickle Cell Anemia (SCA) Subset of genotypes with often more clinical Subset of genotypes with often more clinical
severity and anemiaseverity and anemia Includes HbSS, HbS/Includes HbSS, HbS/00thalassemia thalassemia

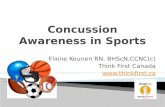
Brief PathophysiologyBrief Pathophysiology
Mutation at sixth position of beta Mutation at sixth position of beta globin chain changes glu → valglobin chain changes glu → val
With deoxygenation, the HbS With deoxygenation, the HbS molecule polymerizes within the molecule polymerizes within the RBC leading to characteristic RBC leading to characteristic shape changesshape changes
Sickled erythrocytes are rigid and Sickled erythrocytes are rigid and obstruct small blood vessels obstruct small blood vessels leading to tissue ischemialeading to tissue ischemia
Deformed sickle cells adhere to Deformed sickle cells adhere to endothelium & macrophagesendothelium & macrophages
induces hemolytic processinduces hemolytic process Inflammation and ongoing Inflammation and ongoing
adhesionadhesion

Hemolysis
Vaso-Occlusion
ACS pain
asplenia stroke
anemia
pulmonary HTN
gall- stones
leg ulcers
nephropathy
AVN
Manifestations of Manifestations of Sickle Cell DiseaseSickle Cell Disease
Chronic anemiaChronic anemia HemolysisHemolysis JaundiceJaundice Cholelithiasis (bilirubinate)Cholelithiasis (bilirubinate)
Acute complicationsAcute complications Pain, priapism, strokePain, priapism, stroke Acute chest syndrome Acute chest syndrome
(ACS)(ACS) Splenic sequestrationSplenic sequestration infectioninfection
Chronic organ damageChronic organ damage Spleen, brainSpleen, brain Kidneys, lung, bones, eyesKidneys, lung, bones, eyes


Recommendations and Recommendations and ToolsTools
Health MaintenanceHealth Maintenance Pediatric and AdultPediatric and Adult
Problem-focused– Acute and ChronicProblem-focused– Acute and Chronic FeverFever Respiratory Symptoms/HypoxiaRespiratory Symptoms/Hypoxia AnemiaAnemia Neurological Neurological PainPain
Tip Sheet - New Recommendations Tip Sheet - New Recommendations and Clinical Pearlsand Clinical Pearls

Health MaintenanceHealth Maintenance

Routine Health Routine Health MaintenanceMaintenance
General co-morbidities to address and control Asthma Obstructive Sleep Apnea Dental Caries
Screen for retinopathy/retinal infarctScreen for retinopathy/retinal infarct By history (age 0-2 yrs)By history (age 0-2 yrs) By vision screen (3-10yrs)By vision screen (3-10yrs) By comprehensive eye exam (10 yrs+)By comprehensive eye exam (10 yrs+)
Screen for renal disease Screen for renal disease Proteinuria starting age 10yProteinuria starting age 10y

Routine Health Routine Health MaintenanceMaintenance
Screen for CNS problems (strokes, moyamoya)Screen for CNS problems (strokes, moyamoya) Annual Trans-Cranial Doppler (2-16y) for Annual Trans-Cranial Doppler (2-16y) for
HbSS/HbSHbSS/HbS0 0
By specialistBy specialist History of neurocognitive symptoms/decline History of neurocognitive symptoms/decline
(headaches, changes in school or work (headaches, changes in school or work performance)performance)
No longer routine Pulmonary Hypertension Screen (EKG, ECHO, CXR)
Anticipatory guidance to include risk of priapism

Routine Health Routine Health MaintenanceMaintenance PenVK 125mg BID <3y; 250mg BID >3y
Until age 5 yrs for HbSS/S0, if no splenectomy or invasive bacterial infection
Typically to age 3 yrs for other genotypes, but weak recommendation to consider no prophylaxis
13-valent pneumococcal vaccine (Prevnar) as 13-valent pneumococcal vaccine (Prevnar) as per recommendations for general populationper recommendations for general population
23-valent pneumococcal age 2 and 7 years23-valent pneumococcal age 2 and 7 years MenHibRix or Menveo at 2, 4, 6, and 12-15 MenHibRix or Menveo at 2, 4, 6, and 12-15
months months MCV4/Menactra – 2 dose primer at age 2, MCV4/Menactra – 2 dose primer at age 2,
booster at age 5, and then every 5 yearsbooster at age 5, and then every 5 years

Routine Health Routine Health Maintenance Maintenance
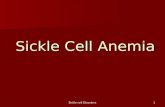
Hydroxyurea (HU) Original use – anti-cancer drugOriginal use – anti-cancer drug Increases fetal hemoglobin in the bloodIncreases fetal hemoglobin in the blood
Prevents sickling of red cellsPrevents sickling of red cells RBCs survive longer in the bloodstreamRBCs survive longer in the bloodstream
Daily doses reduce:Daily doses reduce: Frequency of painful crisesFrequency of painful crises Frequency of acute chest syndromeFrequency of acute chest syndrome Need for blood transfusions/severe anemiaNeed for blood transfusions/severe anemia MortalityMortality

Effects of Hydroxyurea in Effects of Hydroxyurea in SCASCA

Expanded Expanded Recommendations for Recommendations for
HydroxyureaHydroxyurea ALL children > 9 months with SCA (HbSS, ALL children > 9 months with SCA (HbSS, HbSHbS00thal)thal)
Adults with SCA:Adults with SCA: 3+ painful crises in 12 months3+ painful crises in 12 months Sickle cell pain or severe symptomatic chronic Sickle cell pain or severe symptomatic chronic
anemia that interferes with daily activities or anemia that interferes with daily activities or quality of lifequality of life
History of ACSHistory of ACS Consider in other populations (e.g. SCD and Consider in other populations (e.g. SCD and
chronic kidney disease, HbSchronic kidney disease, HbSββ+thal/HbSC +thal/HbSC and recurrent painful crises)and recurrent painful crises)

Initiation and Initiation and MonitoringMonitoring Starting dose Starting dose
Children - 20 mg/kg/dayChildren - 20 mg/kg/day Adults - 15 mg/kd/day (5-10 mg/kg/day if Adults - 15 mg/kd/day (5-10 mg/kg/day if
CKD)CKD) Increase by 5 mg/kg/day q8w to maximal Increase by 5 mg/kg/day q8w to maximal
tolerated dose (max 30-35 mg/kg/day)tolerated dose (max 30-35 mg/kg/day) Monitor CBC, reticulocyte count every 4 Monitor CBC, reticulocyte count every 4
weeks during initiation and every 3 months weeks during initiation and every 3 months while on a stable dosewhile on a stable dose
Maximum tolerated dose to keepMaximum tolerated dose to keep ANC ANC >>2,000/µL– 4,000/µL2,000/µL– 4,000/µL Platelets Platelets >>80,00080,000 ARC ARC >>80,00080,000

Initiation and Initiation and MonitoringMonitoring
Initiation and titrating typically done Initiation and titrating typically done by specialistby specialist
Monitoring could be done in Monitoring could be done in collaboration with PCP, if more collaboration with PCP, if more accessible for the patientaccessible for the patient
Similar to anti-convulsant levels and Similar to anti-convulsant levels and titratingtitrating

Reproductive CounselingReproductive Counseling Discuss importance of knowing partners’
hemoglobin genotype for genetic counseling
Hydroxyurea (HU) is a teratogen
Long Acting Reversible Contraceptive (LARC) is recommended while on HU
Progesterone-only contraception may be preferable
Current recommendation is to discontinue HU before pregnancy and while breastfeeding



Acute and Chronic Acute and Chronic ProblemsProblems
FeverFever
Respiratory SymptomsRespiratory Symptoms
AnemiaAnemia
Neurological SymptomsNeurological Symptoms
PainPain

Management of Fever in Management of Fever in SCDSCD Prompt evaluation for any fever > 38.5°C (101.3°F)Prompt evaluation for any fever > 38.5°C (101.3°F)
Age < 1 year (any fever > 38°C (100.5°F)Age < 1 year (any fever > 38°C (100.5°F) CBC, Blood Culture, retic, ± CXR ± UcxCBC, Blood Culture, retic, ± CXR ± Ucx Immediate administration of IV/IM CeftriaxoneImmediate administration of IV/IM Ceftriaxone
Recommend hospital admission for:Recommend hospital admission for: Age < 1 year Age < 1 year Temp > 39.5°C, 103.1°FTemp > 39.5°C, 103.1°F Allergy to CephalosporinsAllergy to Cephalosporins Surgical splenectomy/history of pneumococcal Surgical splenectomy/history of pneumococcal
sepsissepsis Unsure follow-upUnsure follow-up Toxic appearance, low BPToxic appearance, low BP Infiltrate on CXRInfiltrate on CXR WBC < 2000, > 30,000 x 10WBC < 2000, > 30,000 x 1099/L/L Hb < 2 g/dl from baseline or < 6g/dlHb < 2 g/dl from baseline or < 6g/dl



Respiratory Symptoms Respiratory Symptoms Biggest worry-Acute Chest Biggest worry-Acute Chest
SyndromeSyndrome Number One cause of deathNumber One cause of death Any new infiltrate with Any new infiltrate with
clinical symptoms (e.g. clinical symptoms (e.g. fever, dyspnea, chest pain, fever, dyspnea, chest pain, hypoxia, increased WBC)hypoxia, increased WBC)
CXR may be negative in CXR may be negative in first 24 hours first 24 hours
Lower lobes most Lower lobes most commonly involved; 1/3 commonly involved; 1/3 bilateralbilateral
May be caused by infection, May be caused by infection, sickling, fat embolism, sickling, fat embolism, atelectasisatelectasis



Neurological SymptomsNeurological Symptoms
Acute focal neurological deficits Risk of acute stroke Immediate, emergency evaluation and
treatment
Headaches Risk of Moyamoya - Stenotic arteries in
Circle of Willis/basal ganglia with network of collaterals (“puff of smoke”)
Referral to specialist

Neurological SymptomsNeurological Symptoms“Silent” Cerebral “Silent” Cerebral
InfarctsInfarcts Cerebral ischemia on MRI without focal Cerebral ischemia on MRI without focal neurological symptomsneurological symptoms
20-30% patients with HbSS20-30% patients with HbSS Associated with neurocognitive Associated with neurocognitive
deficits/declinedeficits/decline Increased risk of overt strokeIncreased risk of overt stroke Progression shown to be decreased with Progression shown to be decreased with
chronic transfusion therapychronic transfusion therapy Consider referrals for Consider referrals for
neuro/neuropsych/sickle cell neuro/neuropsych/sickle cell specialist/learning eval/IEPspecialist/learning eval/IEP
Pegelow Blood, 2002; Kwiatkowski BJH 2009; DeBaun Blood, 2012


PainPainAcuteAcute
ChronicChronic

Acute Painful/Acute Painful/Vaso-occlusive ‘crisis’Vaso-occlusive ‘crisis’
Most prominent manifestationMost prominent manifestation
Variable frequency (none to daily)Variable frequency (none to daily)
May be precipitated by illnesses, May be precipitated by illnesses, stress, dehydrationstress, dehydration
Pain in the extremities, Headache, Pain in the extremities, Headache, Chest, AbdomenChest, Abdomen
Abdominal pain may mimic surgical Abdominal pain may mimic surgical conditioncondition

Acute/Vaso-occlusiveAcute/Vaso-occlusive
Assess for other complications (e.g. Assess for other complications (e.g. aplastic crisis, neuro event, priapism, aplastic crisis, neuro event, priapism, sepsis, fever, ACSD, abdominal, ortho, sepsis, fever, ACSD, abdominal, ortho, etc)etc)
Keep warm, hydratedKeep warm, hydrated
Assure following home pain planAssure following home pain plan
Home plan fails → emergency Home plan fails → emergency treatmenttreatment

Chronic PainChronic Pain Major Causes – Avascular necrosis of Major Causes – Avascular necrosis of
hips/shoulders, leg ulcers, chronic bony pain, hips/shoulders, leg ulcers, chronic bony pain, priapism, neuropathic pain/hyperalgesiapriapism, neuropathic pain/hyperalgesia
Assess effect on activity, functional status, Assess effect on activity, functional status, quality of life, depressionquality of life, depression
Involve pain management specialist, sickle cell Involve pain management specialist, sickle cell provider, ortho as indicatedprovider, ortho as indicated
Controlled, coordinated pain management Controlled, coordinated pain management Best if one provider manages chronic pain Best if one provider manages chronic pain
medicationsmedications Pain AgreementPain Agreement Check CSRS/Provider Portal for Check CSRS/Provider Portal for
medication/prescriber historymedication/prescriber history


Thank youThank you
Acknowledgment for part of slide content: Acknowledgment for part of slide content:
Jennifer Rothman, MDJennifer Rothman, MD
Director, Pediatric Comprehensive Sickle Cell Director, Pediatric Comprehensive Sickle Cell Program, Duke University Medical CenterProgram, Duke University Medical Center