Melinda Nugent, Derek Park, Priya Perumalsamy April 6, 2004 Vibrio cholerae.

0
2
4
6
8
10
12
14
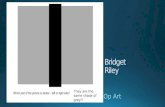
Figure 1. PCR ribotypes of C. difficile in external surroundings of four WA hospitals
1The University of Western Australia, School of Biomedical Sciences, Queen Elizabeth II Medical Centre, Nedlands, Western Australia; 2School of Veterinary and Life Sciences, Murdoch University,
Murdoch, Western Australia, Australia; 3PathWest Laboratory Medicine, Department of Microbiology, Queen Elizabeth II Medical Centre, Nedlands, Western Australia, Australia; 4School of Medical and
Health Sciences, Edith Cowan University, Joondalup, Western Australia, Australia.
• In 2018, a total of 145 samples consisting of soil, mulch, lawn and sand were collected
from the outdoor surroundings of four different old and new hospitals in Perth, WA.
• All samples were incubated in C. difficile selective enrichment broth (BHIB
supplemented with cycloserine and cefoxitin) for at least 5 days, followed by alcohol
shock and culture on C. difficile selective media (ChromID, bioMerieux).
• Any putative C. difficile colonies were sub-cultured onto pre-reduced blood agar to be
identified based on the distinctive horse dung odour, ground-glass colony morphology
and the characteristic chartreuse fluorescence under long-wave UV light (360nm).
• PCR toxin gene profiling and ribotyping was performed, and PCR ribotypes (RTs)
identified by comparing banding patterns to our reference library4,5,6 .
• C. difficile was isolated from 90 out of 145 (62.0%) samples (Table 1).
• Overall, 19.8% (20/101) of the isolates were toxigenic (A+B+CDT-, n=18; A-B+CDT-,
n=1; A+B-CDT-, n=1 [identified as a novel strain]).
• A total of 24 RTs were novel non-toxigenic strains followed by UK 010 (A-B-CDT-), UK
014/020 (A+B+CDT-), QX189 (A-B-CDT-), QX298 (A-B-CDT-), QX284 (A-B-CDT-) and
UK 051 (A+B+CDT-) (Figure 1).
• 24 different previously identified PCR ribotypes were found (Table 1).
• UK 017 (A-B+CDT-), a strain that is endemic to the Asia-Pacific region, was also found
from a newly laid lawn around one of the older hospitals.
• UK 027 and UK 078 (hypervirulent strains) were not isolated.
• This is the first study to identify C. difficile in outdoor environment of various hospitals.
• The presence of highly diverse strains in hospitalised patients suggests the possibility of
patients acquiring infections from sources/reservoirs external to the hospital (Table 1).
• Even though C. difficile is commonly found ubiquitously in soil, the presence of toxigenic
strains especially UK 014/020, UK 103 and the Asian strain of much interest, UK 017, is
of concern.
• It is possible that individuals from nearby Asian countries such as Thailand could have
imported the strain on the soles of their shoes. Another plausible means of transmission
might be vegetables imported from Asia.
• Despite this, the actual risk of disease remains unclear.
• Prominent ribotypes identified were UK 014/020 and 010 (Figure 1).
• UK 014/020 is a common strain identified among both CA and HA cases and the high
prevalence of this particular strain in this study (especially from the entrances of the
hospitals) further suggests the movement of C. difficile from community sources into the
hospital setting (Figure 1).
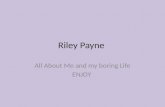
• Figure 2 illustrates the common sources of CA-CDI in WA.
• CDI is fast becoming a One Health issue that requires a comprehensive approach to
improving and safeguarding the health of human beings, animals and the environment
(external and internal to hospitals).
• It is prudent for healthcare professionals, policy makers, veterinarians and researchers
to be aware of the changing epidemiology of CDI.
• Checking for antimicrobial resistance in the C. difficile isolates and conducting
comparative genomic studies (such as WGS, MLST, SNV analysis) to determine strain
relatedness, between patients with CDI admitted in the respective hospitals included in
this study.
• Examining the prevalence of C. difficile on shoes of healthcare staff in old and new WA
hospitals
Table 1. Prevalence and toxin profile of C. difficile isolates
AcknowledgementsMany thanks to all members of
the Riley Clostridium difficile
research laboratory and
PathWest Media.
1. Slimings C, Mahé C, Riley TV. The epidemiology of C. difficile infection in Western Australia, 2011&2013;2012. Journal of Microbiology, Immunology and
Infection. 2015;48(2):S113.
2. Moono P, Lim SC, Riley TV. High prevalence of toxigenic Clostridium difficile in public space lawns in Western Australia. 2017;7:41196.
3. Lim SC, Foster NF, Elliott B, Riley TV. High prevalence of Clostridium difficile on retail root vegetables, Western Australia. Journal of Applied Microbiology.
2018;124(2):585-90.
4. Kato N, Ou CY, Kato H, Bartley SL, Brown VK, Dowell VR, et al. Identification of toxigenic Clostridium difficile by the polymerase chain reaction. Journal of
Clinical Microbiology. 1991;29(1):33-7.
5. Stubbs S, Rupnik M, Gibert M, Brazier J, Duerden B, Popoff M Production of actin-specific ADP-ribosyltransferase (binary toxin) by strains of Clostridium
difficile. FEMS Microbiol Lett. 2000;186:307–12
6. Stubbs SLJ, Brazier JS, O’Neill GL, Duerden BI. PCR Targeted to the 16S-23S rRNA Gene Intergenic Spacer Region of Clostridium difficile and
Construction of a Library Consisting of 116 Different PCR Ribotypes. Journal of Clinical Microbiology. 1999;37(2):461-3.
References
• Clostridium difficile is a Gram positive, anaerobic, spore forming enteropathogen that is
responsible for causing a wide spectrum of diseases from mild diarrhoea to toxic
megacolon and fulminant colitis.
• To prevent outbreaks, interventions commonly implemented include patient isolation,
environmental cleaning and disinfection in hospitals.
• Clostridium difficile infections (CDI) have been encountered in increasing numbers in
patients without previous healthcare contact, despite being a well established hospital
pathogen.
• Community-acquired CDI (CA-CDI) represents a significant proportion of CDI diagnosed
in WA hospitals. In 2011, CA-CDI cases comprised 26% of all hospital-acquired (HA)
CDI cases in Australia and the rates have increased consistently since then1.
• Non-human reservoirs of CDI include animals, food and the environment. Examples of
common environmental sources are contaminated soil, lawn, mulch, sand, compost and
water2,3.
Background
This study reports the prevalence of C. difficile in the immediate outdoor environment of
different hospitals, providing further insight into potential sources of CA-CDI.
Objective
Materials and methods
Results
Discussion and conclusions
Future studies
Nu
mb
er
of
iso
late
s
Figure 2. Common sources of CA-CDI transmission
Sicilia Perumalsamy¹, Papanin Putsathit2 and Thomas V Riley1,2,3,4
Sicilia Perumalsamy
Main collection sites
No. of samples
and prevalence
(%)
Toxin profiles of known RTs isolated
Front of hospital (main and
emergency entrances)
48 (33.1%) 16 0 7
Back of hospital 35 (24.1%) 7 1 2
Sides of hospital 23 (15.9%) 6 0 1
Parks and patient sitting areas 30 (20.7%) 13 0 7
Carparks 9 (6.2%) 5 0 1