Sibo and scleroderma handout
47
Small Intestine Bacterial Overgrowth and Scleroderma Dr Allison Siebecker 13th Annual Cheri Woo Education Seminar Saturday, March 8, 2014 Scleroderma Foundation, Portland Or www.siboinfo.com copyright Dr Allison Siebecker 2014
-
date post
14-Sep-2014 -
Category
Documents
-
view
1.210 -
download
5
description
Transcript of Sibo and scleroderma handout

Small Intestine Bacterial Overgrowth and Scleroderma Dr Allison Siebecker
13th Annual Cheri Woo Education Seminar Saturday, March 8, 2014 Scleroderma Foundation, Portland Or www.siboinfo.com
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4
SIBO Symptoms: GI & Systemic
• Bloating/ abdominal Gas
• Belching, flatulence
• Abdominal Pain, Cramps
• Constipation, Diarrhea, both
• Heartburn/ GERD
• Nausea
• Leaky Gut/SI Sx- any Systemic sx:
• food sensitivities, h/a, joint P, respiratory, skin, brain
• Malabsorption Sx- steatorrhea, anemia, weight loss
IBS

SIBO= Underlying Cause of IBS
• Drs Pimentel, Lin, Chow: 2000
• Tx’ed thousands of IBS pt’s successfully with SIBO protocol
• 84% IBS test+ SIBO • 75% of those whose
breath tests normalized after tx, had improvement in sx’s (Am J Gastroenterology 2003)
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

SIBO Associated Conditions & Risk Factors Study Links on www.siboinfo.com
Acne Acne Rosacea Acromegaly Alcohol Consumption (moderate intake) Anemia Atrophic Gastritis Autism Celiac Disease/ Tropical Sprue Chronic Fatigue Syndrome CLL (Chronic Lymphocytic Leukemia) Cystic Fibrosis Diabetes Diverticulitis Dyspepsia Elderly Age Erosive Esophagitis Fibromyalgia Gallstones Gastroparesis GERD Hepatic Encephalopathy (Minimal) H pylori Infection Hypochlorhydria Hypothyroid/ Hashimoto's Thyroiditis IBD (Crohn’s, Ulcerative Colitis)
IBS Interstitial Cystitis Lactose Intolerance Leaky Gut Liver Cirrhosis Lyme Malabsorption Syndrome Medications: Proton Pump Inhibitors, Opiates Muscular Dystrophy (myotonic Type 1) NASH /NAFLD (non-alcoholic:
steatohepatitis/fatty liver disease) Obesity Pancreatitis Parasites Parkinson's Prostatitis (chronic) Radiation Enteropathy Restless Leg Syndrome Rheumatoid Arthritis SCLERODERMA Surgery: Post-Gastrectomy
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

Prevalence of GI Involvement & SIBO in Scleroderma
• After the skin, the Gastrointestinal Tract is the 2nd most common target of symptoms (Marie ‘07)
• Esophagus = most common 70-95%
• Then the Anus/Rectum 70-95%
• Then the Small Intestine
• Though 100% have decreased SI motility w/in 5 yrs
• Then the Stomach 32%
• SIBO prevalence= 50% average
• 43% (Marie 2009), 46% (Savarino), 63% (Parodi)
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4
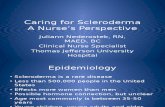
Gastrointestinal Anatomy

What is SIBO?
• Bacterial Colonization of the SI
• SI should have low Bacterial counts (101-2/duodenum)
• LI is the place for Bacterial colonization (1010-11)
• Protective measures keep bact low in SI
• Stomach Acid (HCl), Bile, Digestive Enzymes, GI Immune System (Galt), Migrating Motor Complex
• Deficient MMC= a 1° cause of SIBO
• SIBO= normal GIT bacteria, not pathogenic
• Problem= wrong place in wrong amounts
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

Etiology (Cause)
• Anything that allows bacteria to back up in the Small Intestine
1. Slowed motility in the SI (decreased MMC) • Ex: Dz- Acute Gastroenteritis, Diabetes, Scleroderma;
Opiate drugs; Surgical nerve damage/scarring
2. Obstruction of the SI
• Ex: tumors, strictures, adhesions, excess mucus
3. Non draining pockets/sections of SI • Ex: Small Intestine Diverticulitis, surgical Blind loops
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

Scleroderma SIBO Etiology= Impaired Motility • Thickening of intestinal connective tissue
(Savarino) GI smooth muscle atrophy & intestinal wall/sm musc fibrosis impairs motility(Recasens, Domsic)
• Decreased/Absent MMC (Marie ‘07, Ebert, Rees,
Graydanus)
• 1st vascular, 2nd nerve, 3rd muscle damage
• MMC depends on ICC – nerve cells
• Scleroderma must damage ICC
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

Pathophysiology
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4
SIBO Pathophysiology #1 Bacteria compete for & steal our Food
SI Bacterial Overgrowth
Bacteria Eat Our Food
Bacterial Gas GI Sx bloating, pain (Hydrogen/Methane) constipation/diarrhea GERD, nausea
Premature
Bacterial
Exposure to
Host’s Food
Fermentation
Food = Growth

co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4
Bacterial Gas Causes Abdominal Symptoms of IBS • Bloating/distention= physical swelling
• Pain= GIT sensitive to pressure, musc contract against gas, Visc Hypersens in IBS
• Eructation, flatulence= gas exiting
• GERD/Nausea= gas back pressure
• Altered BM’s
• Hydrogen= associated with diarrhea
• Methane = causes constipation

Problem: Carbohydrates
• Bacteria’s main food source is carbohydrate (CHO)
• Problem #1: CHO feed bacteria worsening overgrowth
• Problem #2: Bacteria ferment CHO > gas > symptoms
• Bacteria can ferment (eat) any and all CHO • All plant food can feed bacteria &
potentially worsen SIBO
cop
yrig
ht
Jan
20
14
Dr
Alli
son
Si
ebec
ker

co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4
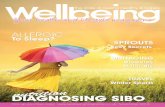
SIBO Pathophysiology #2 Damage= GI & Systemic Sx SI Bacterial Overgrowth
Disaccharidases (-) Carb Transporters Blunted Villi GI Sx’s Elongated Crypt Depth Intestinal Permeability Systemic Sx’s
Hydrogen, Methane Gas GI Sx’s: Bloating Constipation/ Diarrhea Pain , GERD, Nausea
Inflammatory cytokines Digest Brush Border Bile Deconjugation steatorrhea fat sol vit deficiency A, D, E, K
Bacterial Actions
Fermentation of
Unabsorbed Carbohydrate Damage the Brush Border
Bacterial Growth

Diagnosis/Testing
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4
When to consider SIBO?
• If the symptoms of IBS are present
• Bloating, constipation/diarrhea, abdominal pain
• If malabsorption is present
• Low weight, low ferritin/anemia, fatty stools (steatorrhea)
• It’s reasonable to screen all scleroderma patients for SIBO

Lactulose Breath Test
• Measures Gas produced only by Bacteria
• Challenge test- sx may occur during/after
• Positive Interpretations Vary by Dr/Lab
• H 20 ppm w/in 120min (w/in 100min best)
• M 3 ppm at any point in the test (Dr P)
• 3 hour test=best, 2 hr= sufficient
• Must test for both hydrogen & methane
• Locally: NCNM Clinic, OHSU, Emanuel
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

Treatment
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14
SIBO Treatment Protocol
Variation of the Cedars-Sinai Protocol (Pimentel 2006)
Drs Siebecker & Sandberg-Lewis (2010)
SIBO Suspected
1. PE: ICV, Acid/Pancreas Reflex
2. Blood Test: CBC, ESR, thyroid, CV, KD
3. Stool Test (fat malabsorption)
4. String/Gastro-Test or Heidelberg
5. Celiac, Intestinal permeability,
Food allergy/sensitivity
6. Endo/Colonoscopy
Hx GI/Extra GI Sx, Meds, Dz
Antibio
tic
Elemental Diet x 2-3 wks
Diet SCD,
SCD + Fodmap 1. Rifaximin: Diarrhea/Alternating 550mg tid x 14 days
2a. Rifaximin + Neomycin: Constipation 550mg tid + 500mg bid x 14 days
or
2b. Rif + Metronidazole 250mg tid x 14 days
Optional: Probiotic, Antifungal
SIBO Lactulose Breath Test
Or: GBT, Organic Acid Test
SIBO Breath Re-Test
Feel Better- 90%
Partial Improvement/ Not Better
Re-Assess within 2 weeks
Prevention
1. Diet (SCD/Gaps, C-SD, Fodmap)
2. Prokinetic x 3 mo+
:Prucalopride .5-2mg hs
:Erythromycin 50mg hs
:LDN 2.5-5mg hs
Optional: Probiotic, HCl/bitters
Brush Border healing supplements Re-Treat
SIBO (+) SIBO (-)
Consider other Dx
Non-Dx/ other Tests
Treat SIBO
4 options
Hx
Antibiotic Antibiotic Herbal Antibiotics
1. Berberine Herbs
2. Allicin (methane)
3. Oregano
4. Neem
1-3 caps 2-3 x day x 4 weeks
Optional: Probiotic, Antifungal
Relapse

co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4
Key SIBO Tx Points for Success
• Test (LBT)
• Successive Tx Rounds (Abx/HAbx) needed
• If gas is above 35-45 ppm (avg gas dec from Abx/HAbx=25-35 ppm)
• Methane &/or constipation cases are harder to treat
• Double Abx Tx or Allicin needed for methane/constipation cases
• Vary tx method as needed (Abx, HAbx, ED)

Key SIBO Tx Points for Success
• Re-Test to assess results (if not 90% better)
• Both Prokinetic & Diet for prevention
• Diet must be customized to the individual through their own trial & error over time
• There’s no one “diet” that is perfect for anyone
• There’s no test to find one’s perfect diet
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

Prokinetics
• Commonly used in Scleroderma for improving esophagus/GI motility
• Most= cardiac /neurological side effects
• Prucalopride (Canada/Europe)= safe
• Recommended for Scleroderma (Ebert)
• Used for SIBO
• Mosapride (Asian)= ano-rectal ICC’s
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

Incurable SIBO
• With advanced/progressed Scleroderma or continuous PPI’s or Opiates
• Continuous Antimicrobials may be needed
• Rifaximin 550mg every other day • Monitor liver enzymes
• Rotating Herbal Antibiotics (Sandberg-Lewis)
• Berberine- 100mg 1-4x day
• Allicin- 450mg 2-3x day
• Neem 500mg 3x day
• Oregano- 50mg 3-4x day
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

Proton Pump Inhibitors (PPI’s)
• Commonly prescribed in scleroderma for esophagus protection or sx of GERD
• Problems • Risk Factor for SIBO (Lo)
• Acid kills bacteria
• Risk Factor for Bone Fracture (Geller, Gray)
• Acid helps Calcium/mineral absorption
• Many will need it but try removing it • Rebound reflux is common x 8-26 wks after
long term PPI use (Fossmark , Waldum)
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

Other Digestive Support
• Pancreatic Insufficiency in Scleroderma (Ebert)
• Enzymes: Prescription=Creon, OTC= Thorne Dipan
• Malabsorption may be due to:
• SIBO: bact stealing or damaged wall
• Thickened Wall, Poor Circulation • SIBO Leaky gut healers: L-Glutamine, Zinc
Carnosine, Colostrum, Vit D/A/Cod Liver Oil, Turmeric, Resveratrol, Glutathione
• Circulation improving remedies
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

Diet
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

Dietary Treatments for SIBO
• Specific Carbohydrate Diet (SCD) (Haas/Gottschall)
• Gut and Psychology Syndrome Diet (GAPS) (Campbell-McBride)
• Low FODMAP Diet (LFD) (Shepherd/Gibson)
• Cedars-Sinai Low Fermentation Diet (C-SLFD) (Pimentel)
• SCD + Low FODMAP Diet (SCD+LFD) (compiled by
Siebecker)
• All target & manipulate Carbohydrates
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

What the Diets were Formulated to Treat • Formulated for active SIBO, as a treatment
• SCD, GAPS, SCD+ Fodmaps • SCD= IBD/diarrheal dz
• GAPS= GI + brain/mood symptoms (autism)
• SCD+LFD= more severe SIBO
• Formulated for IBS, not SIBO specifically
• Low FODMAP Diet
• Formulated for SIBO Prevention • Cedars-Sinai Low Fermentability Diet
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

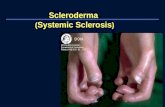
Continuum of Diet Tolerance in SIBO
SCD+LFD SCD/GAPS Low Fodmap Diet No Starch, Low Fiber Fermentable Gluten Free Grains(Starch, Fiber) No Beans at 1st Fruit/Veg Beans, Sugar
Low Fermentable Fruits/Veg C-S Low Fermentation Diet Refined Grains (Starch, Gluten) Sugar
No Beans
cop
yrig
ht
Jan
20
14
Dr
Alli
son
Si
ebec
ker
Less Tolerance/More Severe Case More Tolerance/Less Sever Case

Key Points of SIBO Treatment Diets
• Decrease Fermentable Food (Carbs) for bacteria
• Avoid Grains, Starch, Starchy Veggies, some Beans, Sugar/most sweeteners, Lactose, Fiber/Prebiotics
• Allow monosaccharides= glucose/fructose as honey
• Intro Diet (SCD/GAPS) to decrease bacteria/sx
• SCD+LFD = Intro is optional since Abx/HAbx/ED will decrease bacteria
• Progressive- easier to digest foods at 1st
• no raw fruit or veg, nuts or beans at 1st
• fruit & veg= peel, de-seed, cook & puree at 1st
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

SIBO Diets Match Scleroderma Diets for Esophagus/GI (Recasens)
• Liquid/pureed/soft food
• Soup/broth. Bone broth healing to tissue but wait till SIBO is gone (mucopolysacc)
• Yogurt
• Low Fiber/Fermentable Carbs
• Except meal timing
• Scleroderma= small freq meals for esoph
• SIBO= 4-5 hrs between meals to allow MMC
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

Cons of SIBO Diets
• Weight Loss (5-15#)- not good for underweight
• Difficult
• removal of common/favorite foods
• more home cooking required
• lack of portable snacks
• difficulty participating in food events (weddings, holidays, dinner parties, ‘other people’s food’)
• traveling
• eating out
• Psychologically Difficult: feeling different, out of synch with society, like an outsider, not normal
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker

How to gain weight? • Reduce bacteria with tx: Abx, HAbx
• Caution: Elemental Diet can cause wgt loss
• Eat more food, more often: set a timer (it’s a job)
• Eat more allowed CHO: honey, squash, fruit, nuts, beans
• Eat Lactose free dairy
• Shakes: HM 24 hr ½ & ½ ygt/lactose-free whole milk/coconut milk; nut butter; egg yolks, fruit; fruit juice; honey; cinnamon
(ingredients as tolerated)
• Eat refined CHO (white- rice/potato/bread/pasta)
or Whole CHO if tolerated (whole grains/tubers/beans)
• Heal brush border (abs), take Enzymes (dig)
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker

Diet Pro’s: Benefits Beyond GI Sx (SCD+LFD, SCD, GAPS)
• Weight Loss (inches off waist)
• Stabilization of blood sugar; high & low, stops sugar cravings
• Decrease in chronic infection and inflammation: arthritis, chronic gingivitis
• Improved immunity: decreased seasonal colds/flu/allergies
• Improved skin, mood, sleep, energy and overall well-being
• IBD: off all medicines, normal colonoscopy
• Removes ‘obstacles to cure’, repairs the gut, tx’s other pt complaints
• “I’ll never go back to the way I was eating before”, “I got my life back”
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker

Diet Points
• Gluten (wheat,barley,rye) correlated with AI Dz
• Best avoided by anyone with AI Dz
• Or Test= Cyrex Array III (Wheat/Gluten)
• Lactose Free Dairy= many w/ SIBO tolerate it & do better with it
• Increased energy, stabilize weight loss, helps digestion (ygt-Pbx), increases food pleasure
• But casein can cross-react with Gluten, test via IgG/A blood & correlate w/ TTG (+)
• Cyrex Array IV= cross reactive
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

Lactose Free Dairy Foods
• Homemade 24 hr yogurt/sour cream
• Aged cheese, Dry Curd Cottage Cheese
• Ghee/butter
• Lactase enzyme treated cream in sm amts
• Commercial lactose-free dairy
• Lactaid Milk- SCD Illegal but if tolerated=OK
• Pectin is in “lactose-free” (Green Valley) yogurt, but if tolerated= OK
• True Greek yogurt (no pectin)= low lactose
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

Scleroderma SIBO Case 1
• CC: osteoporosis/malabsorption
• Current Meds: Nexium
• Sx: diarrhea tendency x 1 yr (previously constipated), bloated feeling, esophagus irritation, low weight
• Test: LBT (+) Hydrogen 78ppm Methane 4ppm
• After 2 courses Abx given by other Dr’s
• Rifaximin for SIBO & ? For Gastroenteritis/ER
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

Scleroderma SIBO Case 1
• Treatment • Consider removal of Nexium (referral)
• Berberine Complex (Integrative Therapeutics)
• 5 grams/11 pills per day x 4 weeks
• Specific Carbohydrate Diet
• Result: neg test H 4ppm/M 0ppm • Test- H dec 74ppm, M dec 4ppm
• Sx: still low weight, BM’s improved, bloated/esophagus feelings gone, feels better overall
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

Scleroderma SIBO Case 1
• Prevention Treatment
• SCD/C-SD (rice, potatoes)
• Prokinetic: LDN 2.5mg at bed long term
• 3 months out= treatment is holding
• Notes:
• GI sx were not major a complaint
• Qi-Shen/Vitality-Glow is much improved!
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

Summary
• SIBO is common in Scleroderma
• Symptoms are the same as IBS
• Bacteria ferment carbs into gas> GI sx
• Diagnosis= Lactulose Breath Test
• Treatment= 4 options, 3=quick killing & Diet
• Prevention= Diet + Prokinetics
• Diet= SCD, Gaps, Fodmaps, SCD+LFD, C-SD
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

Resources
See www.siboinfo.com under:
• ‘Resources’ for:
• Testing Laboratories -Books
• Website Resources -Cookbooks
• MMC videos -You tubes
• ‘Treatment’: ‘Diet’= for more diet info
co
pyrig
ht D
r A
lliso
n
Sie
be
cke
r 2
01
4

References
• Marie I, Ducrotté P, Denis P, Menard JF, Levesque H. Small intestinal bacterial overgrowth in systemic sclerosis. Rheumatology (Oxford). 2009 Oct;48(10):1314-9. doi: 10.1093/rheumatology/kep226. PMID: 19696066
• Marie I, Ducrotté P, Denis P, Hellot MF, Levesque H. Outcome of small-bowel motor impairment in systemic sclerosis--a prospective manometric 5-yr follow-up. Rheumatology (Oxford). 2007 Jan;46(1):150-3. PMID:16782730
• Parodi A, Sessarego M, Greco A, Bazzica M, Filaci G, Setti M, Savarino E, Indiveri F, Savarino V, Ghio M. Small intestinal bacterial overgrowth in patients suffering from scleroderma: clinical effectiveness of its eradication. Am J Gastroenterol. 2008 May;103(5):1257-62. doi: 10.1111/j.1572-0241.2007.01758.x. PMID: 18422815
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

References cont.
• Savarino E, Mei F, Parodi A, Ghio M, Furnari M, Gentile A, Berdini M, Di Sario A, Bendia E, Bonazzi P, Scarpellini E, Laterza L, Savarino V, Gasbarrini A. Gastrointestinal motility disorder assessment in systemic sclerosis. Rheumatology (Oxford). 2013 Jun;52(6):1095-100. doi: 10.1093/rheumatology/kes429. PMID: 23382360
• Soudah HC, Hasler WL, Owyang C. Effect of octreotide on intestinal motility and bacterial overgrowth in scleroderma.N Engl J Med. 1991 Nov 21;325(21):1461-7. PMID: 1944424
• Rees WDW, Leigh RJ, Christofides ND, Bloom SR, Turnberg LA. Interdigestive motor activity in patients with systemic sclerosis . Gastroenterology 1982;83:575–80.
• Greydanus MP, Camilleri M. Abnormal postcibal antral and small bowel motility due to neuropathy or myopathy in systemic sclerosis . Gastroenterology 1989;96:110–5.
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

References cont.
• Recasens MA, Puig C, Ortiz-Santamaria V. Nutrition in systemic sclerosis. Reumatol Clin. 2012 May-Jun;8(3):135-40. doi: 10.1016/j.reuma.2011.09.006. PMID: 22197834
• PPI: • Proton pump inhibitor therapy and hip fracture risk. Geller JL,
Adams JS.JAMA. 2007 Apr 4;297(13):1429; author reply 1429-30. PMID: 17405964
• Proton pump inhibitor use, hip fracture, and change in bone mineral density in postmenopausal women: results from the Women's Health Initiative.Gray SL, LaCroix AZ, Larson J, Robbins J, Cauley JA, Manson JE, Chen Z. Arch Intern Med. 2010 May 10;170(9):765-71. doi: 10.1001/archinternmed.2010.94. PMID: 20458083
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

References cont. PPI
• Rebound acid hypersecretion after long-term inhibition of gastric acid secretion. Fossmark R, Johnsen G, Johanessen E, Waldum HL. Aliment Pharmacol Ther. 2005 Jan 15;21(2):149-54. PMID: 15679764
• Rebound acid hypersecretion from a physiological, pathophysiological and clinical viewpoint. Waldum HL, Qvigstad G, Fossmark R, Kleveland PM, Sandvik AK. Scand J Gastroenterol. 2010 Apr;45(4):389-94. doi: 10.3109/00365520903477348. Review. PMID: 20001749
• Proton pump inhibitor use and the risk of small intestinal bacterial overgrowth: a meta-analysis. Lo WK, Chan WW. Clin Gastroenterol Hepatol. 2013 May;11(5):483-90. doi: 10.1016/j.cgh.2012.12.011. PMID: 23270866
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14

References: Gluten
• [Antigliadin antibodies in the absence of celiac disease]. Kamaeva OI, Reznikov IuP, Pimenova NS, Dobritsyna LV. Klin Med (Mosk). 1998;76(2):33-5. Russian. PMID: 9553358
• High incidence of celiac disease in patients with systemic sclerosis. Rosato E, De Nitto D, Rossi C, Libanori V, Donato G, Di Tola M, Pisarri S, Salsano F, Picarelli A. J Rheumatol. 2009 May;36(5):965-9. doi: 10.3899/jrheum.081000. PMID: 19332639
• [Celiac disease associated with systemic sclerosis]. Trucco Aguirre E, Olano Gossweiler C, Méndez Pereira C, Isasi Capelo ME, Isasi Capelo ES, Rondan Olivera M.Gastroenterol Hepatol. 2007 Nov;30(9):538-40. Review. Spanish. PMID: 17980132
• Low prevalence of coeliac disease in patients with systemic sclerosis: a cross-sectional study of a registry cohort. Forbess LJ, Gordon JK, Doobay K, Bosworth BP, Lyman S, Davids ML, Spiera RF. Rheumatology (Oxford). 2013 May;52(5):939-43. doi: 10.1093/rheumatology/kes390. PMID: 23335635
cop
yrig
ht
Dr
Alli
son
Sie
bec
ker
20
14