SI Final Rule - White Paper
26
February 22, 2016 IT Supplement: 2016 Medicaid Program- Covered Outpatient Drug Final Rule Key Implementation Considerations for Manufacturers Confidential and Proprietary © 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
-
Upload
adam-kaufman -
Category
Documents
-
view
97 -
download
0
Transcript of SI Final Rule - White Paper

February 22, 2016
IT Supplement: 2016 Medicaid Program- Covered Outpatient Drug Final Rule Key Implementation Considerations for Manufacturers
Confidential and Proprietary © 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 2
Authors Ari Ilan, Susan Dunne, Gladys Arnold, Julian Barron, Jay Patel, Daniel Choi, Nicholas Torre, Matthew Schroyer, and Adam Kaufman

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 3
Table of Contents Introduction .................................................................................... 4 1.0 Master Data Considerations ................................................... 7 2.0 Monthly AMP Methodology Determination ........................... 10 3.0 Quarterly AMP Considerations ............................................. 12 4.0 Price Type Filters ................................................................. 16 5.0 Base Date AMP ................................................................... 20 6.0 Bundled Sales Arrangements............................................... 21 7.0 Authorized Generics ............................................................ 22 8.0 Medicaid Rebates ................................................................ 24

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 4
Introduction Intended Audience
The target audience for this guide is Government Pricing (GP) and Medicaid Rebates Business Technology professionals; however, we encourage all stakeholders impacted by the Final Rule to embrace these considerations. We believe this will provide crucial cross-functional insight into the Business Technology thought process, which may facilitate a more efficient implementation of changes.
Overview
On January 25, 2016, IMS Health distributed a white paper entitled “2016 Medicaid Program; Covered Outpatient Drug Final Rule Key Operational Considerations for Manufacturers” to assist manufacturers in analyzing the Center for Medicaid and Medicare Services (“CMS”) Covered Outpatient Drug Final Rule [CMS-2345-F].
This document is an IT supplement and serves to assist technology teams in understanding the business requirements that may need to be implemented in a manufacturer’s chosen software solution. While many of the provisions may appear straightforward from a business perspective, there are typically substantial and cumbersome SDLC requirements which must be met.
In this supplement IMS provides analysis of the Final Rule’s potentially broad reach on business processes, technology systems, reports, and other downstream enterprise integrations. We do not provide specific, prescriptive solutions because systems and processes are not identical among all manufacturers. Instead we offer a set of considerations for stakeholders to discuss when evaluating implementation options.
As we are always striving to enhance our understanding of issues that manufacturers face, we encourage you to provide detailed feedback. Please also reach out if you would like to discuss any questions, concerns, or for assistance with IT implementation of any specific provisions in the Final Rule. Contact information for your local IMS leadership can be found at the end of the document.

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 5
Notes
• This document is for informational purposes only. IMS does not engage in the practice of law and does not make any formal legal interpretation of statutes, regulations, and other government-issued guidance.
• The information contained herein is neither comprehensively exhaustive nor specific to any individual manufacturer. IMS recommends a full analysis and review of the Final Rule with your company’s relevant stakeholders and Legal Counsel.
• Most, if not all, of the considerations provided may have an impact on your business processes and associated documentation. Manufacturers should make updates to business processes and documentation in accordance with your company’s compliance policies and change management requirements.
• Our analysis of what constitutes a configuration change versus a core code change assumes newer versions of GP and Medicaid commercially available systems, which have configurable user interfaces (as opposed to back-end updates via SQL packs). Some recommendations may not be applicable to older versions of these software applications or homegrown systems solutions, which may require robust code changes.
• This document is vendor neutral. No software vendors participated in the creation of this document, which is strictly based on the IMS team’s experience with a wide variety of tools.
• The considerations in this guide may lead to system changes. Manufacturers will need to document and test all changes in accordance with their company’s SDLC.

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 6
Format and Structure Our analysis of each issue is presented using the following structure:
Metric Definitions
Complexity Relative level of difficulty to implement
Cost Relative level of costs to implement
Time Relative level of resource hours required to implement
Configuration Change Can be implemented using out-of-box system functionality
Code Change May require a patch/hotfix from the system vendor to implement
Customization Change Code change that is specific to one manufacturer (not applicable to all manufacturer deployments, as in the case of a patch/hotfix)
Reporting Change May require modifications to the application reporting layer
Interface Change May require modifications to inbound/outbound interfaces
Impacted Functionality Relevant system functionality or module to which the changes apply
1
2
7
8
3
4
5
6
9

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 7
1.0 Master Data Considerations
The provisions of the Final Rule may require manufacturers to make changes to Master Data tables, including elements of the Customer Master(s) and the Product Master(s).
1.1 Pediatric Indication Definition
The definition of “Pediatric Indication” was broadened. Drugs that were not previously considered “pediatric” may now qualify for the reduced 17.1% minimum rebate. Considerations:
• Does the Product Master have a way to flag drugs as “pediatric”?
o Is there a way to add additional related attributes (e.g. Effective Date) to the Product Master?
• If changes are made to the Product Master, do any interfaces need to be reconfigured?
• Does the Medicaid Rebates system allow for calculation of the 17.1% base rebate for these products?
1.2 Identification of a Line Extension that is an Oral Solid Dosage Form
Manufacturers are required to identify line extensions of S/I drugs that are an Oral Solid Dosage (OSD) form of the original drug. Line extensions that are an OSD form may be subject to the alternative Unit Rebate Amount (URA) calculation. OSD is defined to mean capsules, tablets, or similar drug products intended for oral use.
Considerations: • Does the Product Master have the ability to identify line
extensions? o Does the Product Master need to be modified to
identify the link(s) between the original S/I drug and the associated line extensions?
• Does the Product Master have a field to capture whether or not a drug is an OSD?
o Is this field populated manually or via an interface? • Does the Product Master require a field to identify corporate
relationship(s) between the S/I drug and the associated line
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Product Master
Medicaid
Section 1.1 Complexity: Low Cost: Low Time: Low Effective Date: 04/01/2016
Section 1.2 Complexity: High Cost: Medium Time: High Effective Date: 04/01/2016

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 8
extensions? • Does the URA formula need to be updated to account for
these changes to the Product Master?
1.3 Distinguishing Mail Order Pharmacies and RCPs
A distinction is drawn between an RCP that provides a home delivery service versus an entity that owns both a retail community pharmacy and a mail order pharmacy.
• Pharmacies that offer home delivery as a service, and do not offer prescriptions primarily through the mail, should be included in AMP.
o Manufacturers have latitude in how they determine whether or not an entity dispenses covered drugs primarily through the mail.
• If an entity owns both an RCP and a mail order pharmacy, the mail order pharmacy sales should be excluded when calculating AMP.
Considerations:
• How are parent-child relationships between RCPs and mail order pharmacies captured?
• Did the Business create new Classes of Trade or any other customer attributes to distinguish each of the following?:
o A) an entity that owns both an RCP and a mail order pharmacy
o B) a pharmacy that provides a home delivery service and does not dispense primarily through the mail
o C) a pharmacy that provides a home delivery service and does dispense primarily through the mail
• Did the Business make updates to the system price type policies to capture these changes?
o Are calculation filter configuration updates required?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Product Master
Medicaid
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Customer Master
Government Pricing
Section 1.3 Complexity: Low Cost: Low Time: Medium Effective Date: 04/01/2016

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 9
1.4 Covered Outpatient Drugs (“CODs”) CMS confirmed the multi-step process that manufacturers should use to determine when a drug is a COD. Notably, radiopharmaceuticals may be considered as CODs. Considerations:
• Are there any products that are now CODs, but were not previously consider CODs and vice versa?
• In the case of S/I drugs that are now CODs, is the necessary data available to perform base date AMP calculations and historical Best Price calculations?
• How will the required Government Pricing calculations be performed if they were not previously done so? How will Medicaid Rebate claims be received, validated, and paid?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
Section 1.4 Complexity: High Cost: High Time: High Effective Date: Retroactive to start of MDR program?

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 10
2.0 Monthly AMP Methodology Determination The Final Rule requires manufacturers to determine whether a 5i drug is “not generally dispensed” by Retail Community Pharmacies (RCPs) using a 70% threshold (“70/30 test”).
Considerations: • Should the system perform the 70/30 test before or after
AMP calculations? o If after- 5i and RCP AMP both may need to be
calculated. o If before- only one AMP calculation may be
necessary. • What methodology and data should be used to calculate the
70/30 ratio? See Section 2.1 • How often should the ratio be calculated? See Section 2.2
2.1 Methodology and Data
Manufacturers have the option to perform the 70/30 test using a smoothing process. The application of a smoothing process should minimize the likelihood of “flip-flopping” between 5i/RCP designations. Manufacturers have latitude in determining the time span of historical data used for smoothing.
Considerations: • What data should be used to calculate the ratio?
o Transactional sales versus 3rd party data • What time span of historical data should be used when
calculating the ratio? • What, if any, smoothing methodology should be used when
calculating the ratio? • What filters should be applied to the data when calculating
the ratio?
2.2 Frequency of Calculations and Reporting
Manufacturers must perform the 70/30 test on a monthly basis and report which methodology was used and should therefore assess their GP and Master Data Management (MDM) system’s readiness to handle alternating 5i versus RCP designation
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
Section 2.1 Complexity: High Cost: Medium Time: Medium Effective Date: 04/01/2016
Section 2.2 Complexity: Medium Cost: Medium

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 11
changes.
Considerations: • How will the 70/30 ratio be calculated within the GP
system? • How will the ratio be used to automate the choice of
Average Manufacturer Price (AMP) methodology? • Where will the 5i designation be stored (e.g., MDM)? • How will historical 5i designation changes be stored and
maintained for restatements and auditing?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
MDM
Time: High Effective Date: 04/01/2016

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 12
3.0 Quarterly AMP Considerations
Provisions of the Final Rule may require manufacturers to reconfigure their quarterly AMP price type. Considerations:
• How does the 70/30 test requirement affect quarterly AMP? See Section 3.1
o How does the business interpret CMS’ expected method for calculating quarterly AMP?
• How does the interpretation impact quarterly AMP price type configuration? See Section 3.2
3.1 Impact of 70/30 Test to Quarterly AMP
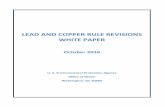
Monthly AMP methodologies may now switch between 5i and RCP within a single-quarter depending on the results of the monthly 70/30 test, and a single quarterly AMP calculation may include monthly AMPs calculated using both methodologies. See Figure 1 below for an illustration of a quarterly AMP calculation with “flip-flopping” monthly AMP methodologies.
Considerations: • How can the quarterly AMP price type be configured to
include 5i and RCP monthly AMP in the same reporting period?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
Section 2.0 Complexity: High Cost: High Time: High Effective Date: 04/01/2016
Section 3.1 Complexity: Medium Cost: Low Time: Low Effective Date: 04/01/2016

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 13
Figure 1: Monthly AMP Methodology Impact to Quarterly AMP Determination
Mon
th 1
Mon
th 2
Mon
th 3
qAM
P
RCP AMP
5i? Y 70/30?
N Y
5i AMPN
RCP AMP
5i? Y 70/30?
N Y
5i AMPN
RCP AMP
5i? Y 70/30?
N Y
5i AMPN
qAMP

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 14
3.2 Quarterly AMP Mechanics Considerations
Manufacturers are now expected to use the following calculation for quarterly AMP:
Quarterly AMP = (month 1 AMP × month 1 AMP units) + (month 2 AMP × month 2 AMP units) + (month 3 AMP × month 3 AMP units)
month 1 AMP units + month 2 AMP units + month 3 AMP units
If month 𝑛 AMP = month 𝑛 AMP $month 𝑛 AMP units
then the above is an exact mathematical transformation of the following formula:
Quarterly AMP = (month 1 AMP $ + month 2 AMP $ + month 3 AMP $)
month 1 AMP units + month 2 AMP units + month 3 AMP units
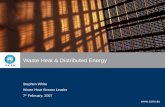
However, CMS clarifies that the second formula is inconsistent with their expectation of how manufacturers should calculate quarterly AMP. CMS’s comments imply that it expects manufacturers to use reported monthly AMP values when calculating quarterly AMP, which may be different than the manufacturer’s calculated values (e.g. when there are calculation exceptions).
See Figure 2 below for an illustration of the CMS expectation for the quarterly AMP calculation using reported monthly AMP values where the manufacturer data leads to calculation exceptions.
Considerations: • Are changes to the quarterly AMP price type configuration
required to reflect the expected quarterly AMP methodology?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
Section 3.2 Complexity: High Cost: High Time: High Effective Date: 04/01/2016

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 15
Figure 2: Effects of Exceptions on Calculated and Reported Monthly AMP N
egat
ive
Dol
lars
Neg
ativ
e U
nits
Fals
e Po
sitiv
e
Calculated RCP AMP
Y 70/30?
N
N Calculated 5i AMP
Exception?
5i?Start
Y
Exception?
Y
N
Y
N RCP mAMP$/Units
Month 3
Prior Month AMP
Month 2
5i AMP$/Units
Month 1
Calculated RCP AMP
Y
70/30?
N
N Calculated 5i AMP
Exception?
5i?Start
Y
Exception?
Y
N
Y
N RCP mAMP$/Units
Month 3
Prior Month AMP
Month 2
5i AMP$/Units
Month 1
Calculated RCP AMP
Y 70/30?
N
N Calculated 5i AMP
Exception?
5i?Start
Y
Exception?
Y
N
Y
N RCP mAMP$/Units
Month 3
Prior Month AMP
Month 2
5i AMP$/Units
Month 1
When using calculated values (not reported values), monthly AMP is the same under both methods. Using reported values may yield different results when there are calculation exceptions.

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 16
4.0 Price Type Filters
Provisions of the Final Rule may require manufacturers to make various adjustments to price type calculation filters.
4.1 Sales and Price Concessions to U.S. Territories in AMP and Best Price
The definition of “United States” and “States” will include Puerto Rico and the U.S. territories (U.S. Virgin Islands, Guam, American Samoa, and the Northern Mariana Islands).
Many manufacturers’ IT systems may already be equipped to handle these configuration changes if their data for Puerto Rico and the U.S. territories is already included in Non-FAMP calculations. However, there may be instances where sales to these regions are excluded from Non-FAMP but included in AMP and Best Price (e.g. transfer prices from the U.S. parent to a foreign subsidiary for drugs dispensed in Puerto Rico and the U.S. territories).
Considerations: • Do the business circumstances require transactional data
for sales to Puerto Rico and the U.S. territories to be included in the calculations?
o Where is that data stored? Can it be accessed? • Do price type configurations require updates to include
these sales and discounts? o How will this data be included in applicable discount
reallocation, smoothing, and factoring processes? o Do reports need to be updated to reflect this
additional data?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
Section 4.1 Complexity: Medium Cost: Low Time: Medium Effective Dates: 04/01/2017

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 17
4.2 Returned Goods in AMP and Best Price
The AMP and Best Price definitions are modified with regard to what constitutes a return as follows: “reimbursement by the Manufacturers for recalled, damaged, expired, or otherwise unsalable returned goods, including (but not limited to) reimbursement for the cost of goods and any reimbursement of costs associated with return goods handling and processing, reverse logistics, and drug destruction, but only to the extent that such payment covers only these costs.”
Considerations: • Do the reason codes and transaction types in the data
contain the required specificity? • Do new reason codes and transaction types need to be
configured? • Are there any price type filter updates required? • Can the system maintain a history of reason code and
transaction type changes for restatement purposes?
4.3 Exclusion of Customary Prompt Pay Discounts (CPPDs) from AMP
The Final Rule confirms that CPPDs occur only between a Manufacturer and a Wholesaler (as narrowly defined in the regulation). CPPDs to Wholesalers only are excluded from AMP; CPPDs to non-Wholesalers are included.
Considerations: • Do the following attributes exist in the PPD transactional
data for calculation filtering? o PPD Type: Customary versus Non-customary o Customer Type: Wholesaler, RCP, and Non-RCP
• If the CPPD value is contained in the direct sales data, are any changes to the interface required?
• Do changes need to be made to monthly AMP calculation filters?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
Section 4.2 Complexity: Medium Cost: Low Time: Medium Effective Dates: 04/01/2016
Section 4.3 Complexity: Low Cost: Low Time: Low Effective Dates: 04/01/2016

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 18
4.4 Exclusion of Sales to Charitable or Not-for-Profit Pharmacies from AMP
Transactions to “charitable” and/or not-for-profit pharmacies are excluded from 5i and RCP AMP. Notably, these entity types are listed under the exclusions list for both Standard and 5i AMP.
Considerations: • Is there a way to determine “charitable” and/or not-for-profit
status? o How often should verification occur for “charitable”
and/or not-for-profit status? o Can this check be automated on a set schedule?
• Is the customer data granular enough to filter “charitable” and/or not-for-profit pharmacies?
• Is the system able to capture effective and expiration dates of entity designation?
4.5 Exclusion of Bona Fide Service Fees to Wholesalers and RCPs from 5i AMP
Bona Fide Service Fees (BFSFs) paid to Wholesalers and RCPs are excluded from 5i AMP calculations.
Considerations: • What is the company’s position on BFSFs to non-
wholesalers and non-RCPs? • Does the BFSF data contain attributes necessary to identify
payments to Wholesalers versus payments to RCPs versus payments to other customer types?
o Does the BFSF data contain attributes to identify the type of payment (e.g. data fees, inventory management fees, etc.)
• Do the 5i AMP calculation filters need to be updated to exclude BFSFs to Wholesalers and RCPs?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
Section 4.4 Complexity: Low Cost: Low Time: Low Effective Dates: 04/01/2016
Section 4.5 Complexity: Low Cost: Low Time: Low Effective Dates: 04/01/2016

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 19
4.6 Any Prices to Covered Entities Excluded from AMP and Best Price
Manufacturers are required to exclude “any prices” provided to 340B covered entities from AMP and Best Price.
Considerations: • How does the business define “any prices”? • Does the customer data contain filterable attributes
necessary to identify all purchases at all prices for eligible covered entities?
• If there is a business requirement to include prices to the expansion entities, does the data contain attributes to filter on covered entity type?
• How are these purchases excluded from AMP and Best Price?
4.7 Clarification of Nominal Sales Excluded from Best Price
All transactions that satisfy the “nominal sales” definition are excluded from Best Price.
Considerations: • Does the system have a way to flag Best Price excludable
nominal sales? • Does the system utilize price filters to exclude nominal sale
transactions from Best Price determination? • Are there any nominal sales reports that need to be updated?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
Section 4.6 Complexity: Medium Cost: Low Time: Medium Effective Dates: 04/01/2016
Section 4.7 Complexity: Low Cost: Low Time: Low Effective Dates: 04/01/2016

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 20
5.0 Base Date AMP
Base date AMP may be restated on a product-by-product basis if the necessary transaction data is available to do so. There may be application implementation considerations when deciding to restate base date AMP.
5.1 Base Date AMP Restatement
Manufacturers may recalculate base date AMP on a product-by-product basis. Considerations:
• Is the historical data required to restate base date AMP available?
o Do the COT definitions from that data align to the ACA definitions (e.g., wholesaler)?
• Can a new field for ACA base date AMP be added to the Product Master?
• Does the system allow for inflationary penalties to be calculated using more than one base date AMP field?
• Are there systems or interfaces accessing new fields? • Do adjustments need to be made to the reporting layer(s) to
account for the modification of existing fields or the addition of new fields to the Product Master?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Product Master
Section 5.1 Complexity: Medium Cost: Medium Time: Medium Effective Date: 04/01/2016

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 21
6.0 Bundled Sales Arrangements
Discounts in bundled sales arrangements may need to be reallocated in accordance with the regulation. Manufacturers may need to make changes to the way they are currently reallocating discounts in their software application. Many manufacturers may be using custom solutions for discount reallocation, and the associated system changes are likely more complex than User Interface (UI) configuration updates.
6.1 Discount Reallocation
All discounts in a bundled sale arrangement must be allocated proportionally to the total dollar value of the units of all products sold under the bundled arrangement.
CMS also added “or products” when referring to the total dollar value of the units in the bundled sale. This change means manufacturers should reconsider whether other products that are not Covered Outpatient Drugs (CODs) but are part of the bundled sale arrangement should be included in the unbundling process.
Considerations: • Will the business be making changes to its discount
reallocation methodology? • How will these changes be implemented in the system?
o Do contract attributes need to be created or modified?
o Does the unbundling logic need to be updated? o Are there devices that need to be unbundled with
drugs? o Are there any discount reallocation interfaces that
need to be updated?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Contracting
Discount Reallocation
Section 6.1 Complexity: High Cost: High Time: High Effective Date: 04/01/2016

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 22
7.0 Authorized Generics The business requirements for including sales of authorized generics in AMP calculations are complex and may require manufacturers to make system changes. Detailed analysis should be performed to determine the necessary transactional data and price type calculation logic.
7.1 Sales from Primary Manufacturers to Secondary Manufacturers
Manufacturers are required to include sales of authorized generic drugs from a Primary Manufacturer to a Secondary Manufacturer (both as defined in the regulation) in its AMP calculation, if the Secondary Manufacturer engages in wholesale distribution of drugs to RCPs. The Primary Manufacturer is to include sales of authorized generics in its Best Price determination of the branded product, provided the authorized generic drug is sold by the Primary Manufacturer.
Considerations: • Is the company a Primary Manufacturer of a drug for which
there is also an authorized generic drug in the marketplace?
o If so, is it also selling the authorized generic version through a related legal entity? How can it be determined if the related entity is
functioning as a wholesaler to RCPs? Can a quantitative analysis be performed to
make this determination? • What data should be used?
Can the determination be made on a product-by-product basis?
How frequently should this determination be made?
o Should the Secondary Manufacturer’s lagged exempt sales, price concessions, and royalty payments be included in the GP calculations for the branded AMP? Should there be combined or separate
smoothing ratios? o What changes need to be made to the price type
filters and calculation logic?
Section 7.1 Complexity: High Cost: High Time: High Effective Date: 04/01/2016

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 23
o Do any changes need to be made to the Master Data to account for Secondary Manufacturers that act as wholesalers to RCPs for some authorized generics, but not others?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Government Pricing
Master Data

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 24
8.0 Medicaid Rebates
Provisions of the Final Rule may require manufacturers to make changes to their Medicaid Rebate system. Considerations:
• How will the inclusion of Puerto Rico and the U.S. Territories impact the system? See Section 8.1
• How will the system calculate alternative URA for line extensions? See Section 8.2
• Can the system effectively validate Medicaid MCO rebate claims? See Section 8.3
8.1 Inclusion of Puerto Rico and U.S. Territories for Medicaid Rebate Processing
As noted above in Section 4.1, the definition of “States” is expanded to include Puerto Rico and the U.S. Territories (Virgin Islands, Guam, Northern Mariana Islands, and American Samoa). Manufacturers will need to pay rebates to the additional States for the associated Medicaid rebate claims.
Considerations: • How will claims from the additional States be received and
validated? • Does the Medicaid Rebate system allow for payment of
claims to the additional States? • Can the system handle supplemental rebate contracts with
the additional States?
8.2 Alternative Unit Rebate Amount (“URA”) for Line Extension Drugs
As noted above in Section 1.2, manufacturers are required to calculate an alternative URA for line extensions that are an Oral Solid Dosage form of the original S/I drug.
This alternative URA is the product of the AMP of the line extension drug and the highest additional rebate (calculated as a percentage of AMP) for any strength of the original S/I drug.
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Medicaid
Section 8.2 Complexity: Low Cost: Medium Time: Medium Effective Dates: 04/01/2016
Section 8.1 Complexity: Medium Cost: Medium Time: High Effective Dates: 04/01/2017

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 25
Considerations: • Does the system have the ability to calculate alternative
URA? • Can the system compare alternative URA to “standard”
URA?
8.3 Managed Care Organizations (“MCO”) Utilization – Date of Service
States that have participating Medicaid MCOs must provide utilization data with rebate claims based on the date dispensed (i.e. date of service) as opposed to the claim paid date.
Considerations: • Can the system validate that invoices received from Medicaid
MCOs are processed based on the date dispensed (date of service)?
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Medicaid
Configuration Change
Code Change
Customization Change
Reporting Change
Interface Change
Medicaid
Section 8.3 Complexity: Medium Cost: Low Time: Medium Effective Dates: 04/01/2016

© 2016 IMS Health Incorporated and its affiliates. All rights reserved. Trademarks are registered in the United States and in various other countries.
Page 26
Practice Leadership New York
Ari Ilan [email protected]
Los Angeles
Cynthia Hwang [email protected]
Washington, DC
Susan Dunne [email protected]
San Francisco
David Chan [email protected]
Chicago
Jeremy Docken [email protected]
Philadelphia
Kathleen Kulp [email protected]