
Shoulder clinical tests validity eleanor richardson
16
Clinical Assessment of the Shoulder: What the research says… Eleanor Richardson Senior MSK Physiotherapist 2015
-
Upload
lennard-funk -
Category
Health & Medicine
-
view
1.885 -
download
2
Transcript of Shoulder clinical tests validity eleanor richardson
Clinical Assessment of the
Shoulder:
What the research says…
Eleanor RichardsonSenior MSK Physiotherapist
2015
Are the Clinical Tests we use Valid?
Sensitivity
“SNOUT”:
➢ A sensitive test can rule out a disease when the result is negative
● A sensitive test = sensitivity > 80%, -LR < 0.20
Specificity
“SPIN”:
➢ A very specific test rules in a disease with a high degree of confidence
● A specific test = specificity > 80%, +LR > 5.0
SLAP lesions● Hegedus et al. (2012):
Passive Distraction and Active Compression = s:70% sp: 90%, +ve LR:7.0, –ve LR: 0.11 (Schlecter, 2009)
Compression-rotation AND Apprehension AND Speed = s: 25%, sp: 92%, +LR: 3.13, -LR: 0.82 for Type 2 only (Oh et al. 2008)
➢ Less optimism for Biceps load II than in Hegedus (2008)
● MRI may be helpful but anatomical variants and Buford complex are normal
● MRI and MR Arthrogram imaging have lower sensitivity than physical examination tests in diagnosing SLAP lesions
➢ in others words, both negative scans and negative cluster testing does NOT rule out a SLAP lesion
Labral Pathology (not exclusive to SLAP)
● Hegedus et al. (2012):
Anterior Slide AND Crank = s: 34%, sp: 91%, +LR: 3.75, -LR: 0.73 (Walsworth et al., 2008)
Apprehension AND Relocation = s: 38%, sp: 93%, +LR: 5.43, -LR: 0.67 (Gaunche & Jones, 2003)
➢ These combinations are good at ruling IN labral pathology but a negative test cannot confidently this rule out…
● Munro (2009):
Kim = s: 80%, sp: 93%, +LR: 12.6, -LR:0.21 (Kim, 2005)
Jerk = s: 73%, sp: 98%, +LR: 34.7, -LR: 0.21 (Kim, 2005)
IRRT (differentiate intra-articular pathology from impingement) = s: 88%, sp: 96%, +LR: 24.7, -LR: 0.12 (Zaslav, 2001)
Rotator Cuff Tears
● Hegedus et al. (2012):
Age ≥ 65 AND Weakness in ER (infraspinatus) AND night pain = s: 49%, sp: 95%, +LR: 9.84, -LR: 0.54 (Litaker, 2000)
Lift off and/or resisted IR (subscapularis) = s: 50%, sp: 95%, +LR: 10.0, -LR: 0.53 (Naredo, 2002)
● Hegedus (2008):
Recommend a combination of bear hug & belly press (s: 40-60%, sp: 88-98%)
● Miller et al. (2008):
ERLS for SSP & ISP, s: 46%, sp: 94%
➢ Tests here appear to be good at ruling in an RCT but a negative test does not mean a RCT/pathology does not exist
AC joint
● No clinical test met the criteria for recommendation by Hegedus (2012) due to high risk of bias from QUADAS 2 assessment
● Two studies looked at clinical tests for the AC joint: Jia et al. (2009) & Goyal et al. (2010)
● Jia et al. (2009) found:● AC resisted extension = s:
72%, sp: 85%, +ve LR:4.8 -LR: 0.33
● Active Compression for AC = s: 41%, sp: 95%, +LR: 8.2, -LR: 0.62
● Cross body for AC joint = s: 77%, sp: 79%, +LR: 3.67, -LR: 0.29
● Goyal et al. (2010) found:● Adductor stress = s: 57%, sp:
96%, +LR:15, -LR: 0.45
And now for the less well defined pathologies….
Subacromial Impingement Syndrome (SIS)● Hegedus et al. (2012):
At least 3 or more positives of the following: Hawkins-Kennedy, Neer, Painful Arch, Empty Can, resisted ER = s: 75%, sp: 74%, +LR: 2.93 and –LR: 0.34 (Michener et al., 2009)
● Park et al. (2005) also recommend this cluster but without the arch sign
● Even with cluster testing adequate levels of sensitivity, specificity, positive & negative LRs are not reached for SIS
● However, consider relevance as would this inform clinical decision making?
● Structural Vs Patterning?
● Consider SSMP (Lewis, 2009) and neuromodulation/patterning re-education
Rotator Cuff Tendinopathy
● Hegedus et al. (2012):
Age > 39, Painful Arch, Self-report of popping or clicking (Chew et al. 2010):
➢ 2 or more positives= s: 75%, sp: 81%, +LR: 3.82 -LR: 0.32
➢ 3 positives = s: 38%, sp: 99%, +LR: 32.20, -LR: 0.63
Lift off and/or Resisted IR = s: 50%, sp: 84%, +LR: 3.13, -LR: 0.60 (Naredo et al, 2002)
However…
● Inadequate sensitivity means a negative test does not mean a tendinopathy doe not exist
● Large cross over with RCT and SIS
● Difficult to evaluate the use of cluster testing in light of Cook and Purdum’s (2009) tendinopathy continuum
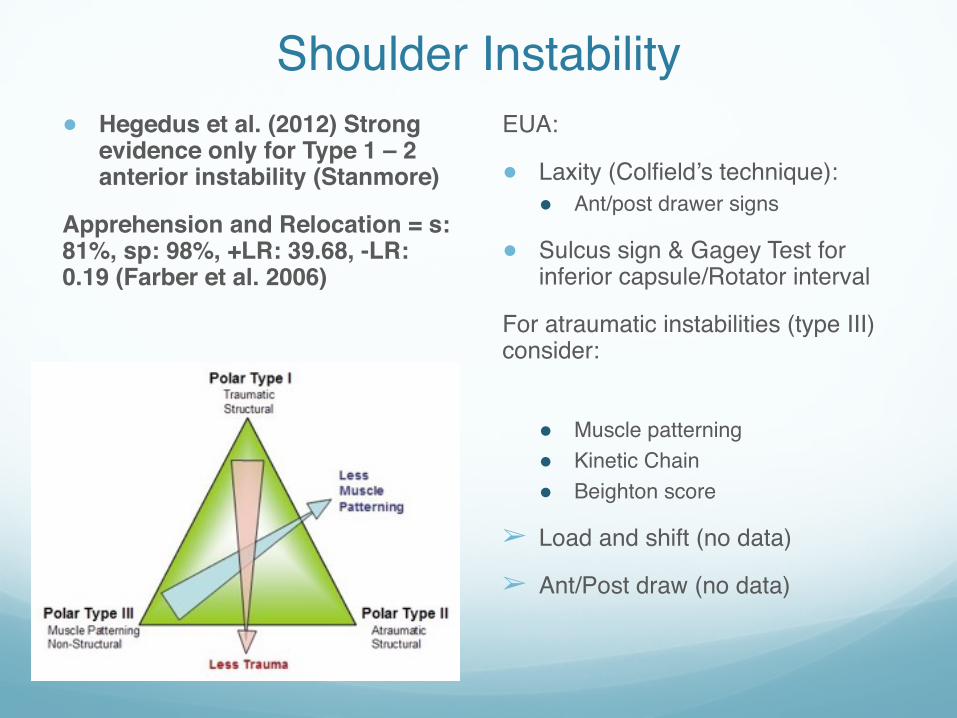
Shoulder Instability● Hegedus et al. (2012) Strong
evidence only for Type 1 – 2 anterior instability (Stanmore)
Apprehension and Relocation = s: 81%, sp: 98%, +LR: 39.68, -LR: 0.19 (Farber et al. 2006)
EUA:
● Laxity (Colfield’s technique):● Ant/post drawer signs
● Sulcus sign & Gagey Test for inferior capsule/Rotator interval
For atraumatic instabilities (type III) consider:
● Muscle patterning● Kinetic Chain● Beighton score
➢ Load and shift (no data)
➢ Ant/Post draw (no data)
Adhesive Capsulitis
● Not assessed as current diagnosis is clinical so no criterion standard
● Hegedus et al. (2012):
Shrug Sign appears sensitive for stiffness related disorders (OA and adhesive capsulitis)(Jia et al, 2008)
➢ Essential physical criteria for diagnosis is a marked and equal limitation of External rotation, both passively and actively
● Emig et al. (1995):
MR Arthrogram sensitivity of 70% and a specificity of 95%
➢ Difficult to interpret as etiology and histology is not fully understood
Osteoarthritis
● No data for sensitivity or specificity for clinical shoulder tests
● Based on clinical history, presentation and XRAY
● >50yrs, incidence increase with age
● Insidious and progressively worsening
● Pain: activity dependent, usually intermittent but can be at rest, dull generalised aching, night pain, reduced active and passive ROM all planes, esp. ER, disuse atrophy, possible grinding sensation with joint movements
● XRAYs:● Subchrondral sclerosis +/- cysts ● Osteophytes
● For the knee 24-56% of patients with OA X-ray findings have pain and higher grades of OA are linked with pain ?relevant to shoulder, a none weight bearing joint?
(Parsons et al., 2004)
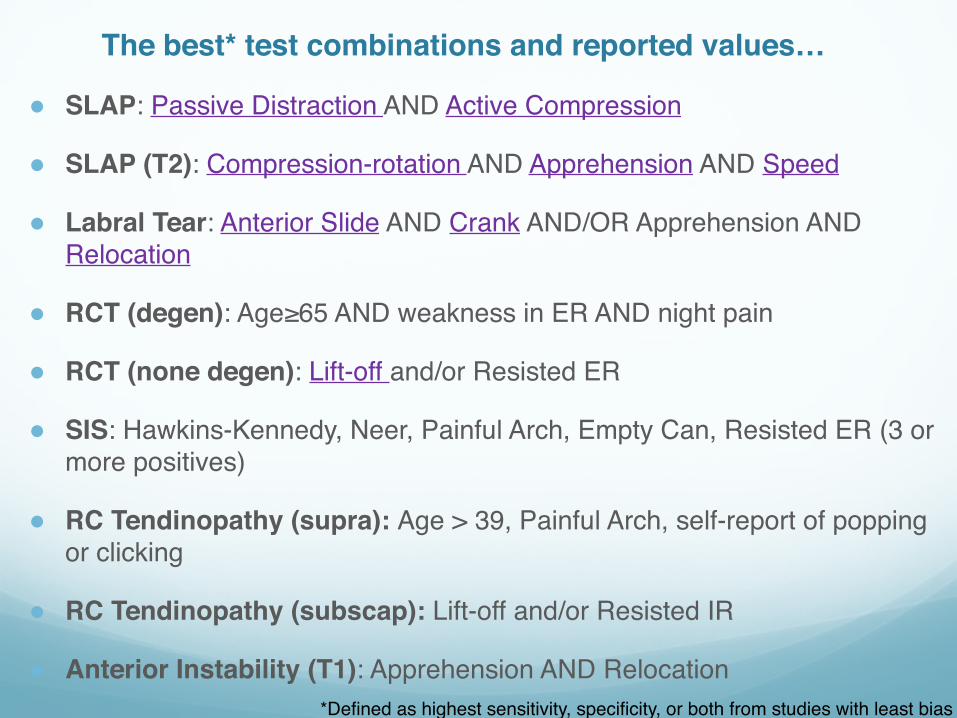
The best* test combinations and reported values…
● SLAP: Passive Distraction AND Active Compression
● SLAP (T2): Compression-rotation AND Apprehension AND Speed
● Labral Tear: Anterior Slide AND Crank AND/OR Apprehension AND Relocation
● RCT (degen): Age≥65 AND weakness in ER AND night pain
● RCT (none degen): Lift-off and/or Resisted ER
● SIS: Hawkins-Kennedy, Neer, Painful Arch, Empty Can, Resisted ER (3 or more positives)
● RC Tendinopathy (supra): Age > 39, Painful Arch, self-report of popping or clicking
● RC Tendinopathy (subscap): Lift-off and/or Resisted IR
● Anterior Instability (T1): Apprehension AND Relocation*Defined as highest sensitivity, specificity, or both from studies with least bias
References● Hegedus et al. (2012) Which physical examination tests provide clinicians with the most value when examining the
shoulder? Update of a systematic review with meta-analysis of individual tests. Br J Sports Med, Nov;46(14):964-78
● Hegedus et al. (2008) Physical examination tests of the shoulder: a systematic review with meta-analysis of individual tests. Br J Sports Med, 42: 80-92
● Oh et al. (2008) The Evaluation of various physical examinations for the diagnosis of type II superior labrum anterior and posterior lesion, Am J Sports Med, 36 (2): 353-359
● Walsworth et al. (2008) Reliability and diagnostic accuracy of history and physical examination for diagnosing glenoid labral tears, Am J Sports Med, 36: 162-8
● Guanche & Jones (2003) Clinical testing for tears of the glenoid labrum, Arthroscopy, 19: 517-23
● Munro & Healy (2009) The validity and accuracy of clinical tests used to detect labral pathology of the shoulder – a systematic review, Manual Therapy, 14:119-30
● Zaslav (2001) Internal rotation resistance strength test: a new diagnostic test to differentiate intra-articular pathology from outlet (Neer) impingement syndrome in the shoulder, Journal of Shoulder & Elbow Surgery, 10(1):23-7
● Litaker et al. (2000) Returning to the bedside: using the history and physical examination to identify rotator cuff tears. J Am Geriatric Soc, 48: 1633-7
● Naredo et al. (2002) Painful shoulder: comparison of physical examination and ultrasonographic findings. ANN Rheum Dis, 61: 132-6
● Miller et al. (2008) The validity of the lag sing in diagnosing full thickness tears of the rotator cuff: a preliminary investigation. Archives of Physical Medicine & Rehabilitation, 89(6): 1162-1168
References cont…● Michener et al. (2009) Reliability and diagnostic accuracy of 5 physical examination tests for subacromial
impingement. Arch Phys Med & Rehabilitation, 90: 1898-903
● Park et al. (2005) Diagnostic accuracy of clinical tests for different degrees if impingement, JBJS American, 87: 1446-1455
● Lewis JS. Rotator cuff tendinopathy. Br J Sports Med. 2009 Apr;43(4):236-41.
● Lewis, J. S. (2009) Rotator cuff tendinopathy/subacromial impingement syndrome: is it time for a new method of assessment? British Journal of Sports Medicine, Vol 43, pp. 259-264
● Lewis JS. Rotator cuff tendinopathy: a model for the continuum of pathology and related management. Br J Sports Med. 2010 Oct;44(13):918-23. http://bjsm.bmj.com/content/44/13/918
● Lewis JS, Tennent TD. How effective are diagnostic tests for the assessment of rotator cuff disease of the shoulder? In: MacAuley D, Best TM, editors. Evidenced Based Sports Medicine. 2nd ed. London: Blackwell Publishing; 2007.
● Farber et al. (2006) Clinical assessment of three common tests for traumatic anterior shoulder instability, J Bone Joint Surg Am, 88: 1467-74
● Emig et al. (1995) Adhesive capsulitis of the shoulder: MR diagnosis, Am J Roenthenol, 164(6): 1457-9
● Parsons et al. (2004) Glenohumeral arthritis and its management, Physical Medicine and Rehab Clinics of North America, 15: 447-474
References cont…● Jia et al. (2009) Examination of the shoulder: the past, the present and the future. J Bone Joint surg Am,
91(6): 10-8
● Jia et al. (2008) Clinical evaluation of the shrug sign. Clin Orthop Relap Res, 466:2813-9
● Goyal et al. (2010) High resolution sonographic evaluation of the painful shoulder. Internat J Radiology. 12:22
● Chew et al, (2010) Cinical predictions for the diagnosis of supraspinatus pathology, Physiotherapy Singapore, 13: 12-17
● Cook & Purdum (2009) Is tendon pathology a continuum? A pathology model to explain the clinical presentation of load-induced tendinopathy. Br J Sports Med, 43(6): 406-16


















