Short and snappy topics off label prescribing, simplified lipid guidelines, type 1.5 diabetes
55
www.usask.ca Type 1.5 Diabetes What?
-
Upload
pasaskatchewan -
Category
Healthcare
-
view
664 -
download
0
Transcript of Short and snappy topics off label prescribing, simplified lipid guidelines, type 1.5 diabetes
www.usask.ca
Type 1.5 DiabetesWhat?

www.usask.ca
Conflict of InterestTerry Damm
I have no actual or potential conflict of interest in relation to this presentation.
www.usask.ca
www.usask.ca
What is Type 1.5 Diabetes? Latent Autoimmune Diabetes of the Adult (LADA)
Similar autoimmune characteristics of T1DM
Non-insulin dependant like T2DM
Often misdiagnosed as T2DM
www.usask.ca
Clinical features Ranges from diabetic ketoacidosis to mild controlled
with diet alone
No one diagnostic feature to distinguish LADA from T2DM
www.usask.ca
Clinical features Time until insulin varies
a) Based on metabolic changes
Worse glycemic control vs. T2DM
Microvascular complications similar to T2DM (less nephropathy)
Potentially less CV risk vs. T2DM
Auto-immune thyroid disease common comorbidity
www.usask.ca
Diagnosis Suspected if glycemic control issues later in life in a
healthy, leaner person
GADA testa) High GADA = more like T1DM and earlier need for insulinb) Low GADA = more like T2DMc) No GADA = could still have LADA
C-peptide levels
www.usask.ca
Diagnosis 3 criteria suggested:
1) Adult age onset (30)2) Presence of at least one circulating islet autoantibody
• GADA• IAA• IA2
3) Lack of insulin requirement for 6 months

www.usask.ca
How does LADA differ from T1DM? Insulin not required at diagnosis
a) >6 months before needing insulin = LADA
Less β-cell loss
Gene markers similar (HLA, INS VNTR, PTPN22)a) Also has markers seen in T2DM (TCF7L2)
Metabolically similara) Low TG, high HDL, lower BMI, good BPb) High HbA1C
www.usask.ca
How does it differ from T2DM? Between 5-10% of T2DM = LADA
Need for insulin sooner and more oftena) 84% LADA vs. 14% T2DM by six years
Higher insulin insensitivity
Less metabolic issues initially
Lower age of onset (34-44 years old)

www.usask.ca
Treatment Options Metformin
a) Little data, studies with methodological flawsb) Conflictingc) No safety issues expected
Sulfonylureas:a) vs. insulin: significantly worse, earlier insulin dependenceb) Plus insulin vs. insulin alone: no better
Thiazolidinediones plus insulin vs. insulin alonea) One small study combination better than insulin alone

www.usask.ca
Treatment Options DPP-4 inhibitors:
a) Saxagliptin vs. placebo: no decline in C-peptide; β-cell function improved
b) Saxagliptin + insulin vs. insulin alone: better C-peptide response
Insulina) Current first-line recommendation once glycemic control deterioratesb) Earlier use of insulin = better outcomes?
www.usask.ca
Treatment Options Non-pharmacologic
a) Diet: same recommendations as type 1 diabetesb) Physical activity and maintain healthy weight
www.usask.ca
Case Example HPI
a) 23 year old male diagnosed with T2D 6 months ago, placed on a sulfonylurea; poorly controlled
b) Presented in hospital with polyuria/dipsia, fatigue, and 6kg weight loss
Past medical historya) Nothing significant
Family historya) Father had T2DM

www.usask.ca
Case Example Physical findings – normal Metabolic findings
a) BMI: 20b) FG: 6 mmol/Lc) PG: 15 mmol/Ld) HbA1C: 9.1%
Lab findingsa) GADA antibodies positive

www.usask.ca
Case Example Management
a) Low saturated fat dietb) Limit intake of simple sugarsc) High-fiberd) Medium intensity physical activity 5x/weeke) Insulin 30/70, 20 units QAM and 16 units QHSf) 3 month follow up showed substantial improvement

www.usask.ca
References Latent autoimmune diabetes of the adult: current knowledge and uncertainty. Diabet Med. 2015 Jul;32(7):843-
52. doi: 10.1111/dme.12700. Epub 2015 Feb 7. Latent Autoimmune Diabetes in Adults: A Case Report Bermúdez, Valmore MD, MPH, PhD1*; Aparicio, Daniel BSc1;
Colmenares, Carlos BSc1; Peñaranda, Lianny BSc1; Luti, Yettana BSc1; Gotera, Daniela BSc1; Rojas, Joselyn MD1; Cabrera, Mayela MD, MPH, PhD1; Reyna, Nadia MgSc, PhD1; Velasco, Manuel MD, FRCP Edin2; Israili, Zafar H PhD2,3
Kobayashi T, Nakanishi K, Murase T, Kosaka K. Small doses of subcutaneous insulin as a strategy for preventing slowly progressive beta-cell failure in islet cell antibody-positive patients with clinical features of NIDDM. Diabetes 1996; 45: 622–626.
Maruyama T, Tanaka S, Shimada A, Funae O, Kasuga A, Kanatsuka A et al. Insulin intervention in slowly progressive insulin-dependent (type 1) diabetes mellitus. J Clin Endocrinol Metab 2008; 93: 2115–2121.
Yang Z, Zhou Z, Li X, Huang G, Lin J. Rosiglitazone preserves islet beta-cell function of adult-onset latent autoimmune diabetes in 3 years follow-up study. Diabetes Res Clin Pract 2009; 83: 54–60.
Interventions for latent autoimmune diabetes (LADA) in adults. [Review][Update of Cochrane Database Syst Rev. 2007;(3):CD006165; PMID: 17636829]
Saxagliptin improves glycaemic control and C-peptide secretion in latent autoimmune diabetes in adults (LADA) http://onlinelibrary.wiley.com/doi/10.1002/dmrr.2717/full
Huang, G., Yin, M., Xiang, Y., Li, X., Shen, W., Luo, S., Lin, J., Xie, Z., Zheng, P., and Zhou, Z. (2016)Persistence of glutamic acid decarboxylase antibody (GADA) is associated with clinical characteristics of latent autoimmune diabetes in adults: a prospective study with 3-year follow-up.Diabetes Metab Res Rev, doi: 10.1002/dmrr.2779.

www.usask.ca
Simplified Lipid GuidelinesAs easy as 1-2-3
www.usask.ca
I have no actual or potential conflict of interest in relation to this presentation.
Conflict of InterestCarmen Bell
www.usask.ca
Can Fam Phys 2015; 61(10):857-867
www.usask.ca
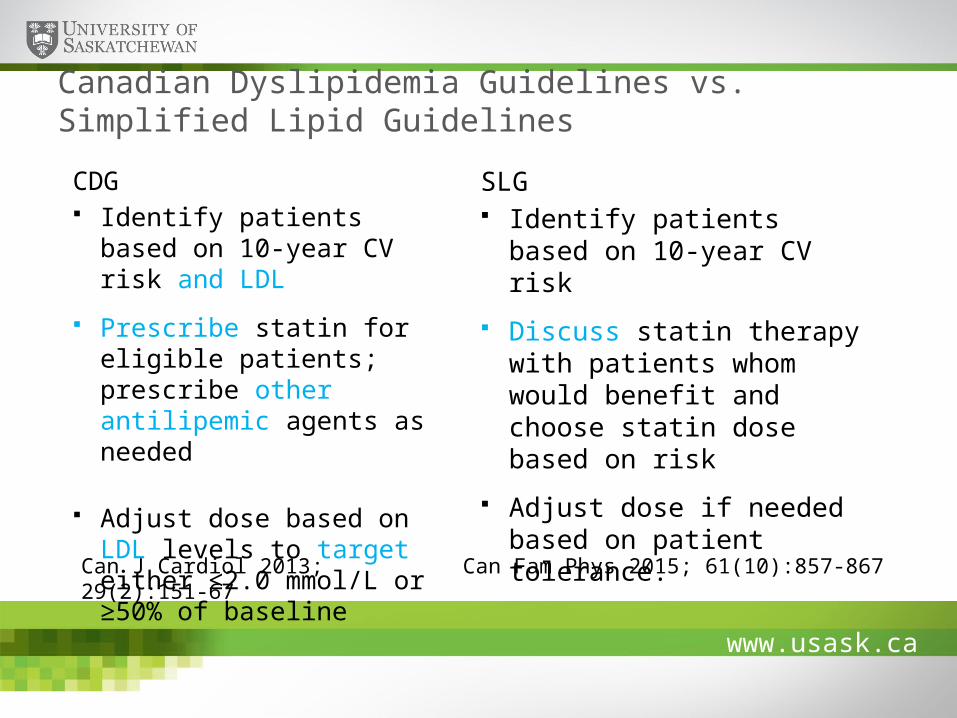
Canadian Dyslipidemia Guidelines vs. Simplified Lipid Guidelines
CDG Identify patients based on 10-
year CV risk and LDL
Prescribe statin for eligible patients; prescribe other antilipemic agents as needed
Adjust dose based on LDL levels to target either ≤2.0 mmol/L or ≥50% of baseline
SLG Identify patients based on 10-
year CV risk
Discuss statin therapy with patients whom would benefit and choose statin dose based on risk
Adjust dose if needed based on patient tolerance.
Can J Cardiol 2013; 29(2):151-67 Can Fam Phys 2015; 61(10):857-867

www.usask.ca
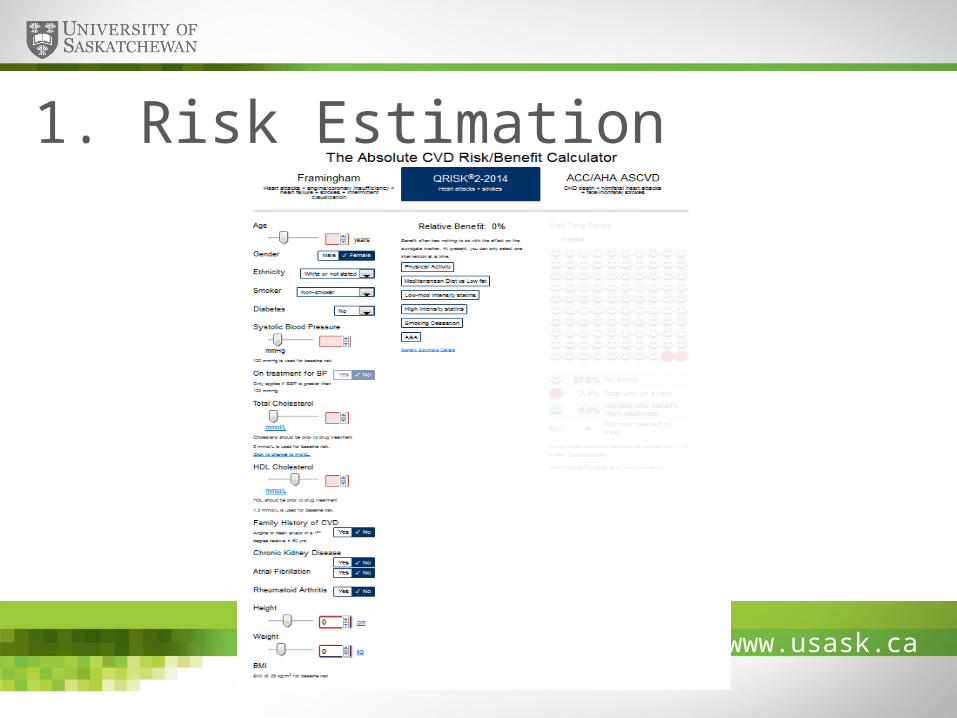
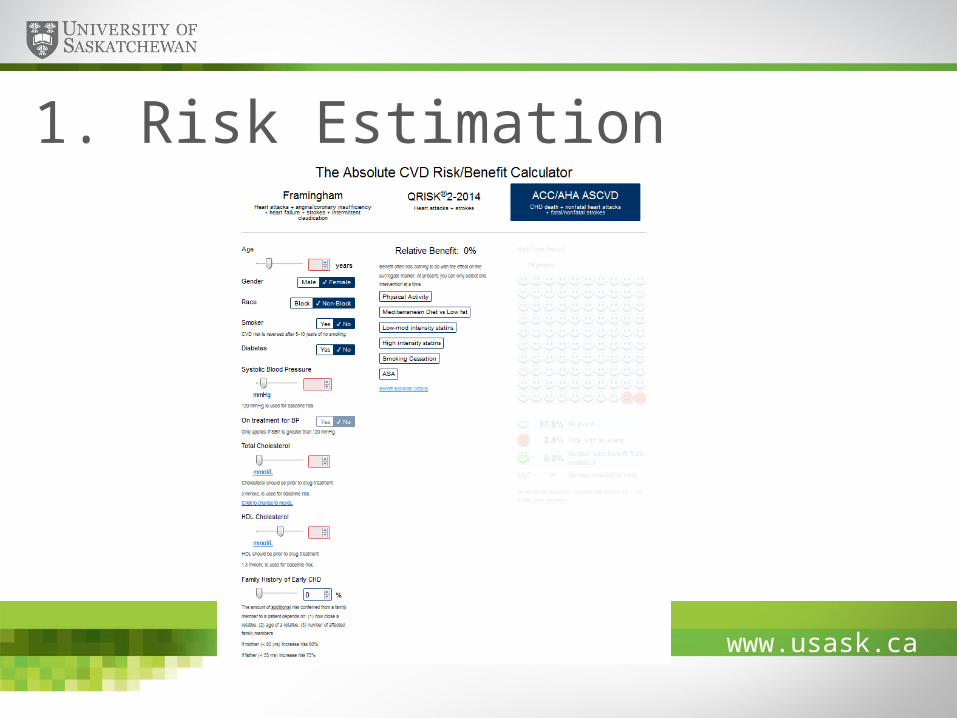
1. Risk Estimation
http://chd.bestsciencemedicine.com/calc2.html
www.usask.ca
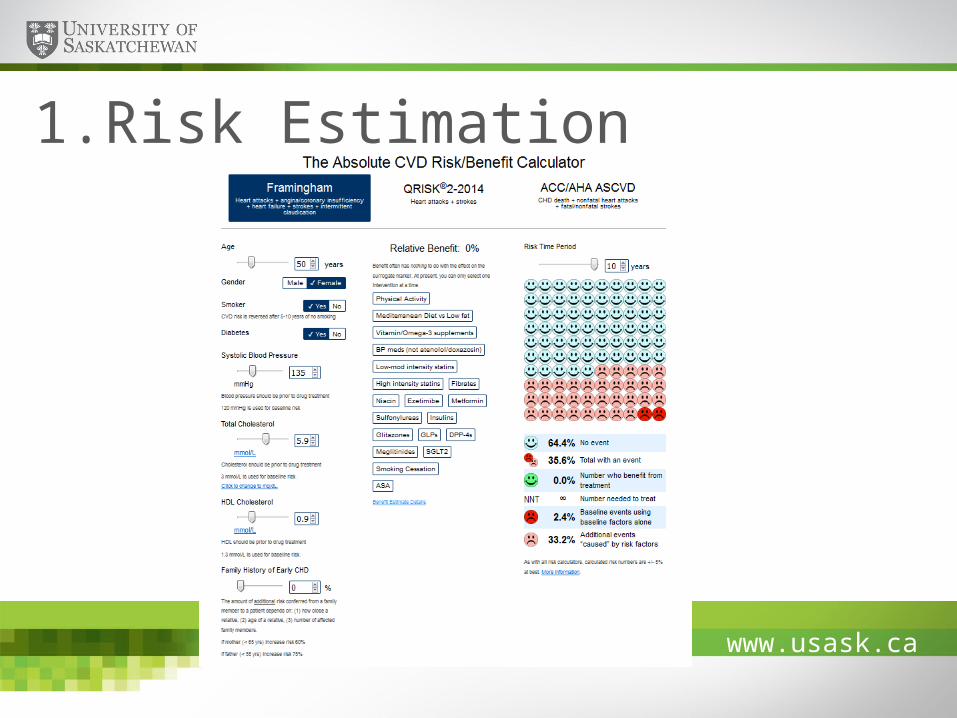
1. Risk Estimation
www.usask.ca
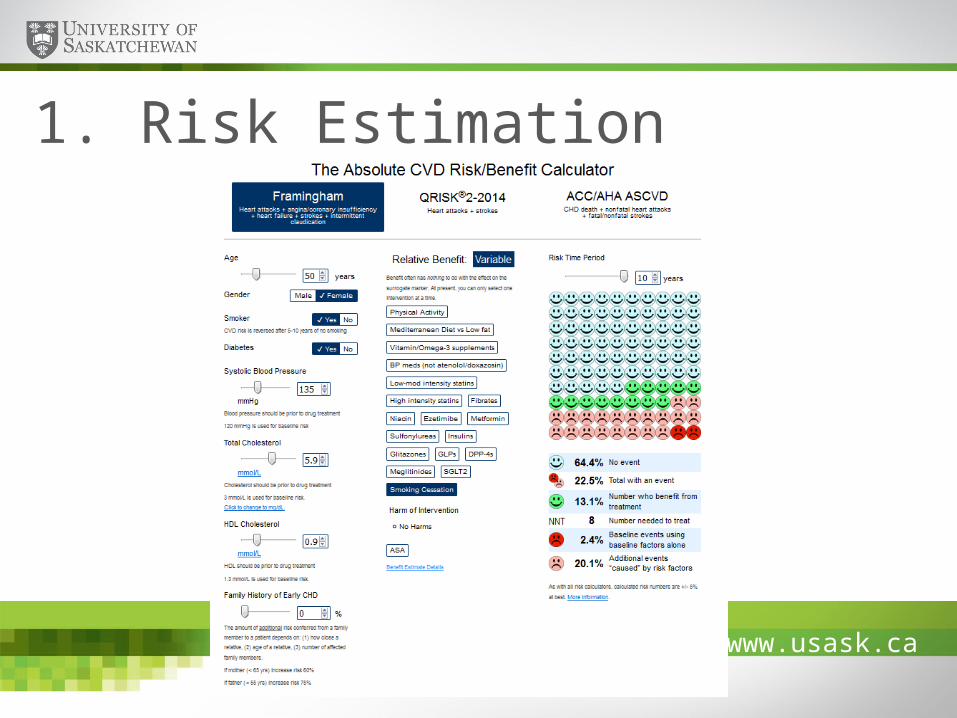
1. Risk Estimation
www.usask.ca
1.Risk Estimation
www.usask.ca
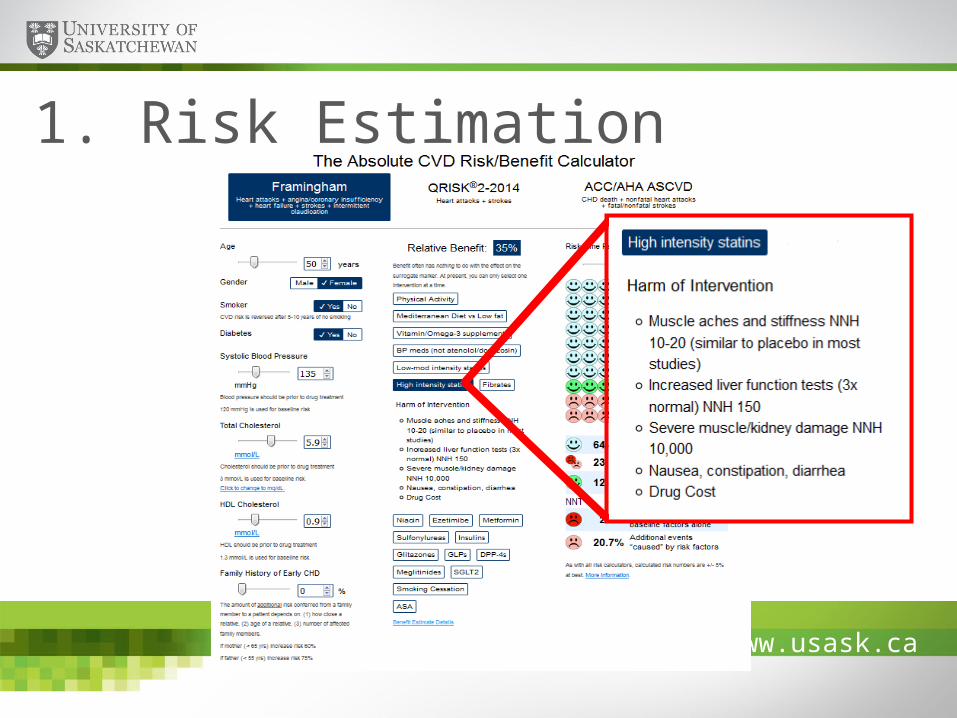
1. Risk Estimation
www.usask.ca
1. Risk Estimation

www.usask.ca
CDG - Management
www.usask.ca
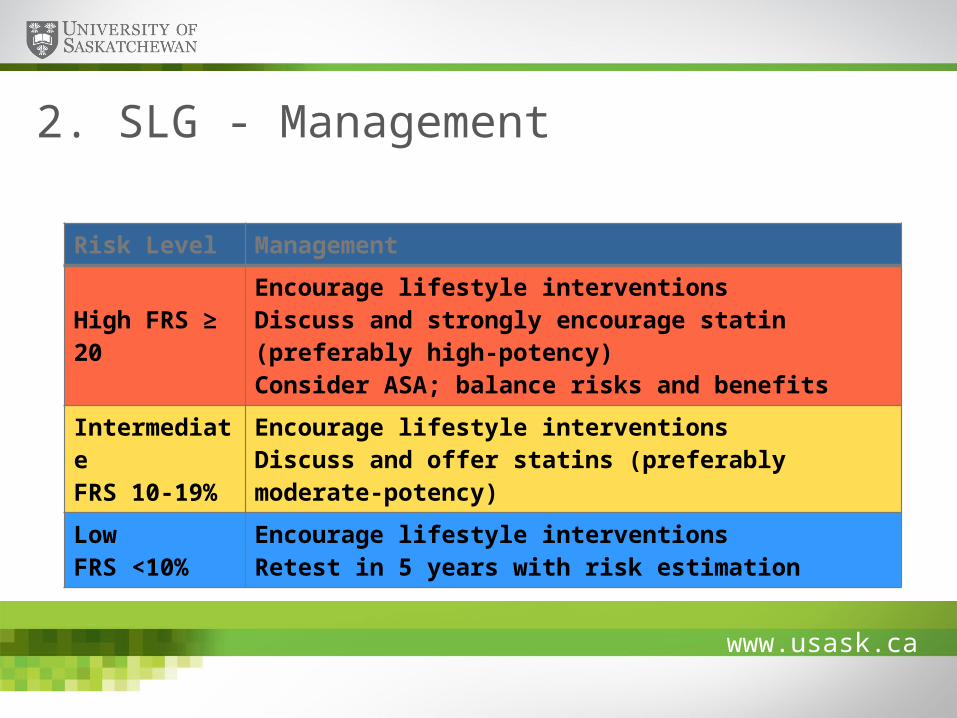
2. SLG - Management
Risk Level Management
High FRS ≥ 20Encourage lifestyle interventionsDiscuss and strongly encourage statin (preferably high-potency)Consider ASA; balance risks and benefits
IntermediateFRS 10-19%
Encourage lifestyle interventionsDiscuss and offer statins (preferably moderate-potency)
LowFRS <10%
Encourage lifestyle interventionsRetest in 5 years with risk estimation

www.usask.ca
2. SLG - Management
StatinIntensity
Low Moderate HighRosuvastatin 2.5 mg 5-10 mg 20-40 mgAtorvastatin 5 mg 10-20 mg 40-80 mgSimvastatin 5-10 mg 20-40 mg -Lovastatin 10-20 mg 40-80 mg -Pravastatin 10-20 mg 40-80 mg
Potency

www.usask.ca
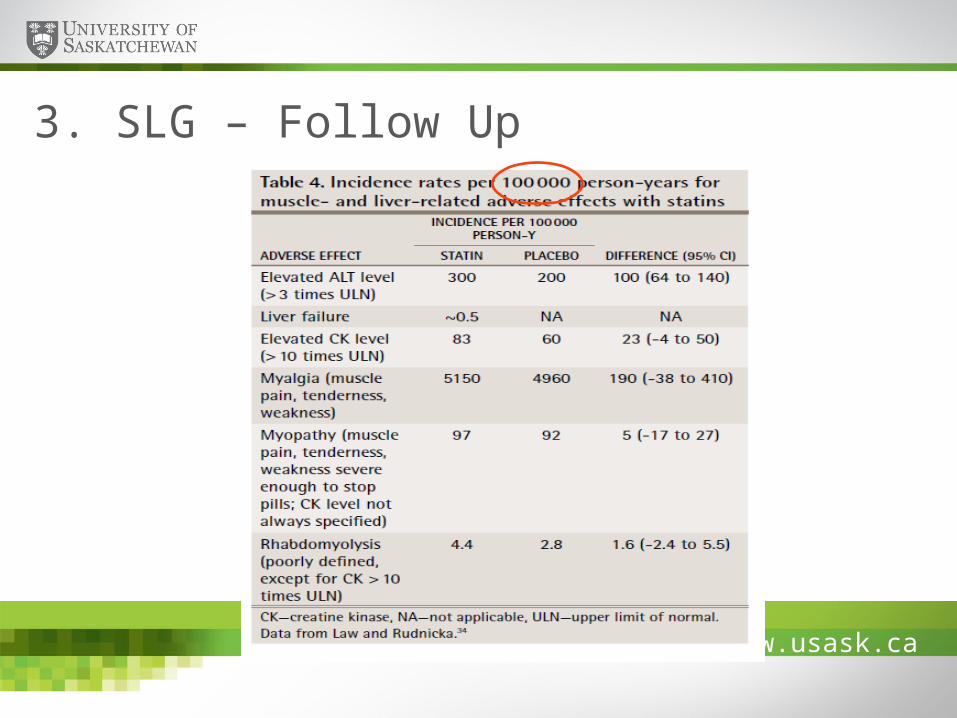
3. SLG – Follow Up Lipid levels Liver enzymes CK How are you feeling? Continue to encourage lifestyle interventions
www.usask.ca
3. SLG – Follow Up
www.usask.ca
4. SLG -Non-Statin Drugs
FibratesEzetimibe
NiacinBile acid sequestrants
As easy as 1-2-3

www.usask.ca
Off-Label Drug Use:Mitigating the RisksKaren Jensen BSP, MSc medSask; Your Medication Information Service
www.usask.ca
No affiliation with pharmaceutical or medical device organization
Article published in Pharmacy Practice Journal July 2014;1:17-21
a) Payment from Roger’s Publishing Healthcare Group
Conflict of InterestKaren Jensen

www.usask.ca
Drug labeling regulations
Benefits of off-label drug use
Concerns with off-label drug use
Liability issues
Minimizing risk
Presentation Outline

www.usask.ca
Drug company must obtain approval from Health Canada to sell drugs in Canada
a) the company has to submit proof the drug is safe & effective for the “labeled uses” …for which trials have been conducted
Researchers & clinicians may discover other “off-label” uses after drug is approved
Drug Labeling

www.usask.ca
Prescribing and dispensing of drugs for off-label use is legal
• But NOT for research or experimentation
• Health Canada has no jurisdiction over prescribing practice
• Decision to prescribe or dispense is between healthcare professional and patient
Drug Regulation
www.usask.ca
Prohibited from promoting off-label uses for their products in Canada and USA but can respond to unsolicited questions about off-label use.
Billions paid out to settle False Claim law suits settlements in the US.
Regulation of Drug Companies

www.usask.ca
Brand name Approved for: Off-label use (s) promoted:Abilify Schizophrenia, bipolar disorder,
depression (adj.)Dementia –related psychosis in elderly
Geodon(Zeldox)
Schizophrenia, bipolar disorder Dementia –related psychosis in elderly
Neurontin Epilepsy (adjunctive) Bipolar disorder, pain disorders, ALS, ADHD, migraine, and more
Seroquel Schizophrenia, bipolar disorder Dementia –related psychosis in elderly
Topamax Epilepsy (adj.), migraine prophylaxis
Variety of psychiatric conditions
Zyprexa Schizophrenia, bipolar disorder Dementia –related psychosis in elderly
Examples of off-label law suits
www.usask.ca
Amarin Wins Off-Label Ruling Against FDA – August 2015
Promotion of unapproved use of Vascepa (omega-3 fatty acid derivative)
Ruling - products can be promoted if information is truthful and “not misleading” — whether or not product has been approved for that particular use
Open door to increased company marketing to physicians??
www.usask.ca
Quebec study (2012)*
a) 11 % of Rx’s ( 1 in every 9) were for off-label indicationsb) 79 % of these not based on scientific evidence
American data – up to 40 % of Rx’s off-label Higher use of off-label drugs in
a) Children – 25 % in community; up to 60 % in hospital.b) Older adultsc) Pregnancy and lactation
*Arch Intern Med. 2012 May 28;172(10):781-8.
How often are drugs used off-label?
www.usask.ca
Option when approved medication is ineffective
Option when no drugs are approved for condition
May be drug of choice
May advance medical knowledgea) New therapeutic uses for currently marketed drugsb) Previously unidentified ADR’s – important to report to
Health Canada
Benefits of off-label drug use

www.usask.ca
Patient safety• Use often not based on scientific evidence
• Lack reliable evidence on• Effectiveness• Adverse effects
Cost to patient • May not be on drug plan formularies• May not qualify for insurance coverage
Cost to healthcare system• Cost of coverage for potentially ineffective drug treatment• Cost to treat serious adverse effects
Potential Problems
www.usask.ca
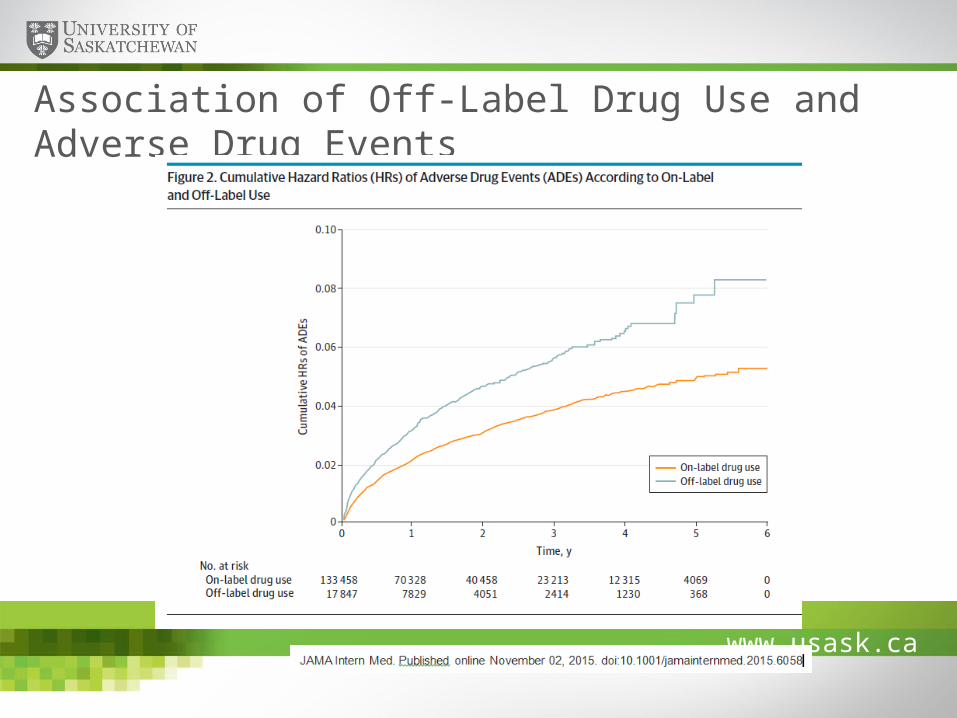
Association of Off-Label Drug Use and Adverse Drug Events

www.usask.ca
Off-label use with/without strong evidence
www.usask.ca
Include indication on the prescription
Inform patient of off-label use
Facilitate access to Canada Vigilance Adverse Reaction online reporting form
a) Include indication in report
Better access to drug comparison resources
CIHR, CADTH to evaluate and research off-label drug use
Facilitate research in drug therapy for pediatrics, seniors, pregnant and lactating women
Senate Committee Recommendations 2014

www.usask.ca
23 year old woman given the anticonvulsant valproic acid for “irritability” (unapproved use). She developed a kidney cyst and nervous system disorder; kidneys failed and she died.
85 year old man received antipsychotic quetiapine for insomnia (unapproved use). He subsequently developed diarrhea and nausea, then died of a heart attack.
www.usask.ca
Off-label prescribing and dispensing is not illegal – may in some circumstances be the best choice for the patient.
Liability insurance should cover healthcare providers who prescribe and dispense drugs off-label unless:
a) there is insufficient evidence supporting the off-label use b) evidence of negligence
Provider Liability
www.usask.ca
Be aware of drug labeling a) Check Canadian drug monographs
Be able to justify off-label usea) Medications should offer clear benefit vs the riskb) Comparison with approved options?
Communicationa) What is the indication?b) Inform patient – consent?
Documentation Follow-up Report ADRs
Risk Mitigation

www.usask.ca
Drug Off-label use supported by evidence, guideline recommendations
Limited or no evidence of effectiveness and/or safety
Amitriptyline Neuropathic pain, migraine prophylaxis
Insomnia (esp. in elderly)
Clonazepam Benzodiazepine withdrawal, panic disorder
Insomnia, essential tremor, tinnitus
Divalproex Bipolar disorder maintenance, migraine prophylaxis, SSRI induced headache
Dementia
Gabapentin Neuropathic pain, hot flashes ADHD, migraine, restless leg syndrome, bipolar
Metformin PCOS Weight loss in nondiabetic patients
Examples:
www.usask.ca
Approved indications for drugs• CPS (e-cps via SHIRP – www.shirp.ca )• Drug Product Database -
http://webprod5.hc-sc.gc.ca/dpd-bdpp/index-eng.jsp
Off-label usesa) Lexi-Compb) Drugs.com (free on-line)c) NICE Evidence summaries: unlicensed or off-label
medicines http://www.nice.org.uk/about/what-we-do/our-programmes/nice-advice/evidence-summaries-unlicensed-or-off-label-medicines
d) Medical literature search – PubMed, Scopus etc
Resources

www.usask.ca
Drug comparisonsa) RxFiles www.rxfiles.cab) RxTx (Therapeutic Choices) – available through SHIRP (
www.shirp.ca)c) Dynamed (by subscription)
Resources (continued)
www.usask.ca
medSask: Your Medication Information Service
Evidence-based information about prescriptions, over-the-counter medications and herbal products, including:
a) INDICATIONS – APPROVED /OFF-LABELb) DRUG OF CHOICEc) Dose / administrationd) Drug use during pregnancy / lactatione) Drug interactions and adverse drug reactions
Questions researched and information provided by licensed pharmacists
Respond within 24 hours to 90 % of calls

www.usask.ca
Available: 365 days a year8am – midnight, Monday to Friday
5pm – midnight, weekends / holidays
Contact us byTelephone: 1-800-667-3425 (toll-free)
306-966-6340 (Saskatoon)Email: [email protected]
Website: www.medsask.usask.ca
medSask: Your Medication Information Service