SHOCK. Intensive care of shock. Extreme conditions. Cardio –pulmonari resustication.
85
SHOCK. Intensive care of shock. Extreme conditions. Cardio –pulmonari resustication. L.Yu.Ivashchuk
-
Upload
karyn-sullivan -
Category
Documents
-
view
15 -
download
0
description
SHOCK. Intensive care of shock. Extreme conditions. Cardio –pulmonari resustication. L.Yu.Ivashchuk. Outline. Definition Epidemiology Physiology Classes of Shock Clinical Presentation Management Controversies. Definition. A physiologic state characterized by - PowerPoint PPT Presentation
Transcript of SHOCK. Intensive care of shock. Extreme conditions. Cardio –pulmonari resustication.

SHOCK. Intensive care of shock.
Extreme conditions. Cardio –pulmonari resustication.
L.Yu.Ivashchuk

Outline
Definition Epidemiology Physiology Classes of Shock Clinical Presentation Management Controversies


Definition
A physiologic state characterized by Inadequate tissue perfusion
Clinically manifested by Hemodynamic disturbances Organ dysfunction

Epidemiology
Mortality Septic shock – 35-40% (1 month mortality) Cardiogenic shock – 60-90% Hypovolemic shock – variable/mechanism

Pathophysiology
Imbalance in oxygen supply and demand Conversion from aerobic to anaerobic
metabolism Appropriate and inappropriate metabolic and
physiologic responses

Pathophysiology
Cellular physiology Cell membrane ion pump dysfunction Leakage of intracellular contents into the
extracellular space Intracellular pH dysregulation
Resultant systemic physiology Cell death and end organ dysfunction MSOF and death

Physiology
Characterized by three stages Preshock (warm shock, compensated shock) Shock End organ dysfunction

Physiology
Compensated shock Low preload shock – tachycardia,
vasoconstriction, mildly decreased BP Low afterload (distributive) shock – peripheral
vasodilation, hyperdynamic state

Pathophysiology
Shock Initial signs of end organ dysfunction
Tachycardia Tachypnea Metabolic acidosis Oliguria Cool and clammy skin

Physiology
End Organ Dysfunction Progressive irreversible dysfunction
Oliguria or anuria Progressive acidosis and decreased CO Agitation, obtundation, and coma Patient death

Classification
Schemes are designed to simplify complex physiology
Major classes of shock Hypovolemic Cardiogenic Distributive

Hypovolemic Shock
Results from decreased preload Etiologic classes
Hemorrhage - e.g. trauma, GI bleed, ruptured aneurysm
Fluid loss - e.g. diarrhea, vomiting, burns, third spacing, iatrogenic



Hypovolemic Shock
Hemorrhagic Shock
Parameter I II III IV
Blood loss (ml) <750 750–1500 1500–2000 >2000
Blood loss (%) <15% 15–30% 30–40% >40%
Pulse rate (beats/min) <100 >100 >120 >140
Blood pressure Normal Decreased Decreased Decreased
Respiratory rate (bpm) 14–20 20–30 30–40 >35
Urine output (ml/hour) >30 20–30 5–15 Negligible
CNS symptoms Normal Anxious Confused Lethargic
Crit Care. 2004; 8(5): 373–381.

Cardiogenic Shock
Results from pump failure Decreased systolic function Resultant decreased cardiac output
Etiologic categories Myopathic Arrhythmic Mechanical Extracardiac (obstructive)

Distributive Shock
Results from a severe decrease in SVR Vasodilation reduces afterload May be associated with increased CO
Etiologic categories Sepsis Neurogenic / spinal Other (next page)


Distributive Shock
Other causes Systemic inflammation – pancreatitis, burns Toxic shock syndrome Anaphylaxis and anaphylactoid reactions Toxin reactions – drugs, transfusions Addisonian crisis Myxedema coma

Distributive Shock
Septic Shock
SIRS 2 or more of the following: Temp >38 or <36 HR > 90 RR > 20 WBC > 20K >10% bands
Sepsis SIRS in the presence of suspected or documented infection
Severe Sepsis Sepsis with hypotension, hypoperfusion, or organ dysfunction
Septic Shock Sepsis with hyotension unresponsive to volume resuscitation, and evidence of hypoperfusion or organ dysfunction
MODS Dysfunction of more than one organ

Clinical Presentation
Clinical presentation varies with type and cause, but there are features in common
Hypotension (SBP<90 or Delta>40) Cool, clammy skin (exceptions – early
distributive, terminal shock) Oliguria Change in mental status Metabolic acidosis

Evaluation
Done in parallel with treatment! H&P – helpful to distinguish type of shock Full laboratory evaluation (including H&H,
cardiac enzymes, ABG) Basic studies – CxR, EKG, UA Basic monitoring – VS, UOP, CVP, A-line Imaging if appropriate – FAST, CT Echo vs. PA catheterization
CO, PAS/PAD/PAW, SVR, SvO2

Treatment
Manage the emergency Determine the underlying cause Definitive management or support

Manage the Emergency
Your patient is in extremis – tachycardic, hypotensive, obtunded
How long do you have to manage this?
Suggests that many things must be done at once
Draw in ancillary staff for support! What must be done?

Manage the Emergency
One person runs the code! Control airway and breathing Maximize oxygen delivery Place lines, tubes, and monitors Get and run IVF on a pressure bag Get and run blood (if appropriate) Get and hang pressors Call your senior/fellow/attending

Determine the Cause
Often obvious based on history Trauma most often hypovolemic (hemorrhagic) Postoperative most often hypovolemic
(hemorrhagic or third spacing) Debilitated hospitalized pts most often septic
Must evaluate all pts for risk factors for MI and consider cardiogenic
Consider distributive (spinal) shock in trauma

Determine the Cause
What if you’re wrong?
85 y/o M 4 hours postop S/P sigmoid resection for perforated diverticulitis is hypotensive on a monitored bed at 70/40
Likely causes Best actions for the first 5 minutes?

Definitive Management
Hypovolemic – Fluid resuscitate (blood or crystalloid) and control ongoing loss
Cardiogenic - Restore blood pressure (chemical and mechanical) and prevent ongoing cardiac death
Distributive – Fluid resuscitate, pressors for maintenance, immediate abx/surgical control for infection, steroids for adrenocortical insufficiency

Controversies
IVF Resuscitation Limited resuscitation in penetrating trauma Use of hypertonic saline resuscitation in trauma Endpoints for prolonged resuscitation
Pressors Best pressors for distributive shock
Monitoring Most appropriate timing and use for PA
catheterization or intermittent echocardiogram

Three stages of ABC-reanimation. Algorithm of its realization by one and two medical men. Testimony to defibrillation and technique of its execution. Cardiac shock of feature of clinical dynamics, first aid. Acute respiratory insufficiency. Reasons of origin, types of hypoxia, degrees of heaviness. Medicinal therapy. Treatment of post-reanimating illness.

First aid at the terminal states. Concept about the terminal
states, purpose and task the first medical aid, first-aid and medical rescue.

General principles, legal, organizational, medical and deontological features of giving the first aid in extraordinary situation. Algorithm of primary inspection of the patient in the place of event.

BASIC CONCEPTS in REANIMATOLOGY
Reanimatology is science about the revival of organism, which studies etiology, pathogenesis, diagnostics and treatment of the terminal states.
A reanimation (abroad widespread is a term of rescucitation) is a process of replacement and proceeding in the functions of organism by the leadthrough of the special reanimation measures. It is proposed by V.Negovsky (1975). To these measures a pneumocardial reanimation belongs in particular (CLR).

Clinical death -| it is the state which circulation of blood and spontaneous breathing absent in the conditions of, but there yet were irrecurent changes in the human brain, when it is yet possible to return a patient to life without a clinically meaningful neurological deficit.

Why does attention apply exactly on a cerebrum? It is a structure of organism, which most sensible to the hypoxia or anoxia (clinical death), and in tissue of which above all things in case of stopping of circulation of blood there are irreversible changes. Maximally this period can last 3-б min, except of some states, above all things hypothermias, when vitability of cortex can be restored and through the greater interval of time.

Biological death is consisting of irreversible changes above all things of CNS, when to life turning a man is impossible. To the clinical signs of biological death take drying out and dimness of cornea, of a corpse spots and of a corpse.

Such concepts utillize in rescucitation, as a decortication (social death) is death of cortex (when somatic functions can recommence almost in full, but the function of cortex does not recommence) a that decerebration is death of cerebrum.
By the clinical signs of decortication ñ absence of свідо мості and purchased reflexes. There is a timber-toe by the dead bark of the brain on condition of valuable supervision can live yet long time. To set the exact diagnosis of decortication heavily, as there are events, when after the protracted comma a man came to consciousness.

A decerebration arises up after more protracted total ischemia of brain (20 min and anymore), sometimes can develop on a background a decortication in the case of progress of іschemical-reperfusion defeats.

The clinical signs of death of cerebrum is absence of electric activity of cerebrum during ЕЕG-decay, atony, areflexy, hypothermia, bradicardia, arterial hypotension, absence of the independent breathing. The vital functions of organism at decerebration may be supported of short duration time due to the leadthrough of AB and support of circulation of blood. Such organism can be utillized as a donor for transplantation of organs.

On condition of primary stop of circulation of blood the spontaneous rhythmic breathing stopping is not later than in 1 min as a result of exhaustion of respiratory center. But the terminal types of breathing are possible: Cheyn-Stoks, Biott, breathing by Husping.
After the stop of heart a man loses consciousness already through 10-15 s due to exhaustion of power substrates in the brain, first of all glucosum.

MOST WIDESPREAD REASONS OF UNEFFECTIVE CIRCULATION OF BLOOD
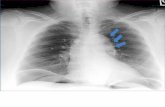
MYOCARDIAC ISCHEMIA
A myocardial ischemia more frequent all arises up as a result of violation of circulation of blood in coronarias (embolism, spasm). The extreme display of ischemia is a sharp heart attack of myocardium. As a result of complete absence of delivery oxygen there is a sharp deficit of power substrates to cardiac cells, above all things ATP.

Activity of cells membrane pumps and canals, foremost Na+, K+ and Ca++ is violated. The result of it is an accumulation in the myocardium Na and Ca with development of intracellular edema, there is a considerable intracellular deficit of K+. The finished goods of metabolism accumulate in myocardium, foremost C02 and lactat which results in heavy intracellular acidosis.

It does not follow to forget that the damage of cardiac cells (and also tissues of brain and other tissues of an organism) takes a place and after proceeding in perfusion, is the so-called syndrome of reperfusion. Its damaging factors are active free radicals (above all things, oxygen – super-oxides, peroxides, ions of hydroxide, peroxinitrate) on a background diminishing of activity of the antioxidant system.

Reflex stop of heart Takes a place foremost as a result of
n.vagus reflexes (from an eye is reflex of Ashner, trachea, carotis areas, root of lights, stomach, uterus). It should be noted that usually the stop of cardiac activity arises up on a background a myocardial ischemia, intact myocardium in default of hypoxia (it can be respiratory hypoxia, ischemia and others like that) quickly «avoids» influence of n.vagus.














TYPES OF STOP OF the HEART
Fibrillation of ventricles The most widespread type of uneffective
circulation of blood in not hospital terms is all of to 2/3 cases. Reason of фібриляції of ventricles is violation of leadthrough of impulses on myocardium of atrium and ventricles, and also increase of excitability of myocardium. To the factors which are instrumental in the origin of fibrilation of ventricles, take intracellular K+↓, total cooling of organism, mechanical irritations, during implementation of diagnostic and medical manipulations.

During fibrillation of ventricles there is a desynchronization of reductions of myo-fibriles myocardium with the loss of pumping function of the heart. On EKG fibrillation of ventricles shows up alike on a wave the curve of different amplitude in default of auricle and gastric complexes.

Unpulsive gastric tachycardia
The most widespread type of uneffective circulation of blood is in the conditions of permanent establishment. At unpulsive gastric tachycardia , without regard to frequent reduction of ventricles, the retractiveness of myocardium is considerably mionectic, that is accompanied uneffective circulation of blood.

Asystole
Practical absence of electric and mechanical activity of myocardium. On EKG appears as an almost straight line
The most frequent reason of asystole is ischemic heart (IKHS) trouble, it can develop on a background fibrilation of ventricles which are an unfavorable prognostic sign.

Electromechanic dissociation (EMD) and bradiarythmia with the uneffective mechanical activity of heart
At the transferred states electric activity of heart is stored, but it is not accompanied effective reductions of myocardium. On EKG discover typical and off type gastric complexes with a different rhythm. off type gastric complexes at
electromechanical dissociation

Diagnostics of uneffective circulation of blood
The element of pneumocardial reanimation is very important. On timely diagnostics of stop of circulation of blood a prognosis depends often.
If in the conditions of permanent establishment cardio-monitoring is conducted a patient during the stop of circulation of blood, on a monitor or on EKG find out the characteristic signs of stop of circulation of blood.

But more frequent all uneffective circulation of blood is diagnosed only after clinical signs. To them absence of pulse belongs, foremost, on central arteries (sleepy and thigh). The method of research of pulse is resulted the way of palpation. Research of pulse by means of
palpation on a. carotis

To the early signs of unefficiency of circulation of blood paralytic mydriasis belongs also: at raising of overhead eyelid a pupil remains wide and irresponsive on light

Research of pulse by palpation and estimation of the state of pupilla it is possible to perform simultaneously.
As already marked higher, the obligatory signs of uneffective circulation is absence of consciousness and rhythmic independent breathing.
Such symptoms, as cyanosys of skin, absence of tones of heart during auscultation, to the pulse on peripheral arteries, unnecessarily are the signs of stop of heart, but can be those symptoms which need immediate estimation of the state of circulation.

PNEUMOCARDIAL REANIMATION Complex of measures which are executed
during the leadthrough of CPR, it is possible to divide on three basic groups:
base sustentation - after the English letters of ABC:
A (airway ореn) providing of communicating of respiratory tracts
B (breeth) artificial respiration C (сirculation) a massage of heart

Must be conducted any man which is alongside; subsequent methods of CPR, the purpose of
which is proceeding in independent circulation of blood for a patient: electric defibrilation, medicinal therapy;
stabilizing of basic vitally important functions of organism sick, above all things it touches activity of cerebrum, heart and vessels, intensive therapy.

If a patient is in the swoon state (absence of reaction on asking and mechanical irritation), it is necessary to perform the followings actions:
To cause the brigade of medical first-aid, if there is possibility (it is better) - reanimation brigade.

Immediately to begin the leadthrough of reanimation measures:
1) to provide communicating of respiratory tracts; 2) to check up the presence of the independent
breathing; 3) if the independent breathing absents is a
leadthrough of AB; 4) to define a pulse on a carotid; if during 5 sec to
discover the pulse is impossible - immediately to begin the non-direct massage of the heart.
Reanimation specialized measures in obedience to algorithms are performed by reanimation brigade.

Providing of communicating of respiratory tracts
A patient at stop of circulation of blood has a presence of extraneous bodies reasons of violation of communicating of respiratory tracts in the cavity of mouth and swallow; supra-larynx and the root of tongue is recovered included in a larynx
Violation of communicating of overhead respiratory tracts in event of stopping of circulation of blood

For providing of communicating of respiratory tracts of patient inlay on a hard even surface, lying on the back. After it oral cavity of patient with a gauze tampon, serviette or handkerchief, release a finger from blood, vomit the masses, extraneous bodies (dentures and others like that). For the leadthrough of rest room of oral cavity it is possible to apply an aspirator.

The next stage is providing of communicating of larynx. As a result of that a tongue is anatomically related to the lower jaw, it is necessary to show out a lower jaw how it is indicated on a figure
Variants of leading-out of lower jaw for proceeding in communicating of overhead respiratory tracts

All of medical workers must own this reception. More simple and less effective, but made to order to application unmedical personnel, there is a reception of filling up of the head.
For this purpose reanimator lays the palm of one hand on the brow of patient, and palm of other hand underlays under a neck and unbends the head simultaneous motion of both hands (triple reception by Safar).

More professional methods of providing of communicating of respiratory tracts is intubation of trachea, use of laringeal mask or combined air-tube - combitube Laringeal mask

Intubation of trachea is the most reliable method of providing of communicating of respiratory tracts, but it must do it professional which will be able to execute manipulation in short period (30-40 s).

Urgent methods of artificial ventilation of lights
The methods of AB can be divided into 2
groups: inciter and expiration. Unfortunately, the inciter methods of AB, which almost reproduce the physiology mechanism of the spontaneous breathing, did not find the wide use in clinical practice through some inconveniences and difficult equipment for their leadthrough.

Today most widespread are expiration methods of AB (due to insufflation of gas mixture to lights), from urgent methods it above all things method «mouth to the mouth», which consists in insufflation of air in the respiratory tracts of patient under time of breathing out reanimator. For this purpose reanimator destroys the lower jaw of patient up to the top, whereupon densely takes by his lips the lip of patient and does exhalation, but necessarily here stops up the nose of patient.

If the leadthrough of AB is uneffective (what absence of excursion of thorax testifies to), it is needed to suspect the presence of extraneous body in lower respiratory tracts (below vocal connection). At that rate it follows to use reception by Geymlikh – under-diaphragmatic shove

MAINTENANCE OF CIRCULATION OF BLOOD
Except for providing of adequate receipt of oxygen in teethridges, it is needed to provide artificial circulation of blood. On condition of uneffective spontaneous circulation apply the indirect (external) and direct (internal) massage of heart to that end.

Indirect massage of heart A method is based on the
compression of ventricles of heart between sternum and and column.
Circulation the leadthrough of the external massage of heart provided due to two mechanisms: to the effect of pectoral pump and direct compression of ventricles of heart, that is why more expedient would be to talk about the massage of thorax.

Reanimator becomes from one side from a patient, places basis of one palm on middle part of sternum approximately on 2 fingers higher from to basis of sworden out-growth and along brest-bone disposes the second palm.
Then by direct hands, not bending them in elbow joints (it saves forces), reanimator executes pressure on sternum on a depth 4-6 sm for adults.

For children method of leadthrough of indirect massage of heart some other. It consists in pressure one or by two fingers on sternum with frequency for children junior in 1 over 100 times per 1 min.
The skilled conducted is closed the massage of heart enables keeping of systole BP at the level of 60-80 mm of Hg, although diastole BP leaves at low level which diminishes coronal and cerebral perfusion considerably, and it worsens a prognosis considerably.

Reasons of unefficiency of the closed massage of heart can be hypovolemy, hemopericarditis, anatomic defects of thorax.
It should be remembered that during the leadthrough of the closed massage of heart it is impossible to do the protracted (over 5-10 s) pauses.