driven by alfred adler's paradigm- shifting rule- breaking ...

Shifting the Treatment Paradigm
for Multiple Sclerosis: Advances in
Pathophysiology and Emergence of
Novel Disease-Modifying Therapies
Moderator
Edward Fox, MD, PhD
Director, Multiple Sclerosis Clinic
Central Texas Neurology Consultants
Round Rock, Texas
Faculty
Stephen Krieger, MD
Associate Professor of Neurology
Icahn School of Medicine
Corinne Goldsmith Dickinson Center for MS
Mount Sinai Medical Center
New York, New York
Clyde Markowitz, MD
Associate Professor of Neurology
Director, Multiple Sclerosis Center
Perelman School of Medicine
University of Pennsylvania
Philadelphia, Pennsylvania

Learning Objectives
• Describe the pathophysiology of MS as it relates to T-
and B-cell behavior and mechanisms of action of MS
therapies
• Assess mechanisms of emerging MS DMTs and how
to integrate these therapies into treatment regimens to
enhance patient outcomes
• Discuss how advanced understanding of MS
pathophysiology may translate into new and emerging
therapeutic options for progressive forms of MS
Please review the faculty disclosures
and accreditation information on the
accompanying webpage.
2

Pathophysiologic
Mechanisms of MS

Paradigm Shifts in Understanding
of MS
• MS was thought to be primarily a T-cell disease;
we now recognize the importance of both B- and
T-cell mechanisms
• Recognition of a variety of immune cell types
involved in MS pathology offers potential for
more targeted treatments
• Understanding of immune-cell interaction in the
periphery and CNS suggests that triggering
activities may occur on both sides of the BBB
4
CNS = central nervous system; BBB = blood-brain barrier.

Unanswered Questions in MS
Pathology
• What is the inciting event that leads to the
immune cascade resulting in MS?
• Does this occur in the CNS or periphery?
• Rather than activated immune cells crossing the
BBB, could an event originating in the meninges
trigger a breach in the BBB that allows immune
cells to cross over and interact with antigens?
5

Activity of T Cells in Periphery and
CNS
DC = dendritic cell; Treg = regulatory T cell.
Fletcher JM, et al. Clin Exp Immunol. 2010;162(1):1-11. 6

T Cells in MS Pathogenesis
Th1 cells
• Promote cellular immunity directed against
intracellular pathogens
• Th1 ↑ during relapse (proinflammatory)
Th2 ↑ during remission (anti-inflammatory)
• T-cell subsets determine whether they will have
a helper or suppressor function
Amedei A, et al. Int J Mol Sci. 2012;13(10):13438-13460. 7

Th1 Mechanisms
IFN = interferon; Ig = immunoglobulin; IL = interleukin.
Mayer G, et al. Cell-mediated immunity: cell-cell interactions in specific immune responses. In: Hunt R.
(2011) Microbiology and Immunology. 8

T-Cell Subsets Driving Immune
Response
Th17 cells1:
• Distinct Th subset producing IL-17; critical role in autoimmune response
• Accumulation in MS vs controls: active MS lesions, CSF, peripheral circulation (esp. during acute relapse)
T-regulatory cells (Tregs)2:
• In non-MS: control autoreactive T cells; may have protective effect
• In MS: dysregulation or impaired maturation of Tregs
• Tregs, dendritic cells are potential therapeutic targets in MS
CSF = cerebrospinal fluid.
1. Amedei A, et al. Int J Mol Sci. 2012;13(10):13438-13460.
2. Zozulya AL, Wiendl H. Nat Clin Pract Neurol. 2008;4(7):384-398. 9

Personalized Medicine in MS
• Personalized medicine is desirable in MS
because it is a heterogeneous disease
• Expanding treatment armamentarium increases
opportunity to tailor therapy to patient
• Biomarkers are needed to better stratify patients
10 Derfuss T. BMC Medicine. 2012;10:116.

Role of B Cells in MS
Pathophysiology

B-Cell Mechanisms in MS
• Found mainly in active MS lesions
• Cytokine production:
– Activation/effector
– Proinflammatory, anti-inflammatory
– Regulatory
• Interaction with T cells:
– Presentation of antigen by B cells is necessary for
triggering autoimmunity against myelin
oligodendrocyte glycoprotein
von Büdingen HC, et al. Eur Neurol. 2015;73(3-4):238-246. 12

B-Cell Mechanisms in MS (cont’d)
BCR = B-cell receptor; LT = lymphotoxin; MHC = major histocompatibility complex; TCR = T-cell receptor;
TNF = tumor necrosis factor.
von Büdingen HC, et al. Eur Neurol. 2015;73(3-4):238-246. 13

Early Rituximab Data Established
Viability of B-Cell Depletion in MS
14 Hauser SL, et al. N Engl J Med. 2008;358(7):676-688.
0 4 8 12 16 20 24 28 32 36 40 44 48
Weeks
0.0
0.5
1.0
1.5
2.0
2.5
To
tal N
o. o
f L
esio
ns
P=0.78
P=0.003 P=0.001
Placebo
Rituximab
P<0.001
0 4 8 12 16 20 24 28 32 36 40 44 48
1.0
1.5
No
. o
f N
ew
Le
sio
ns
0.5
0.0
Weeks
Placebo
Rituximab
P<0.001
P=0.76 P=0.002
P<0.001
P values represent comparisons at baseline and 12, 16, 20, and 24 weeks

Does Depletion of B Cells “Reset”
Immune System in MS?
• Antigen presentation by B to T cells fosters
proinflammatory milieu associated with MS activity
• Bystander activation by B cells to T cells may
explain association between MS relapses and
systemic infections
• Goal of therapy is not just to reduce lymphocyte
counts but also to adjust immune balance
• Reset immune system toward an anti-inflammatory
environment by modulating B-cell activity
(“rebooting” immune system)
15

Measuring Response to B-Cell
Therapies
With recovery1,2:
• Immature B cells predominate in periphery
• Proinflammatory Th1, Th17 responses
decreased in periphery and CSF
• Repopulated B cells do not appear to have
increased IL-6 expression
1. Lehmann-Horn K, et al. Ther Adv Neurol Disord. 2013;6(3):161-173.
2. von Büdingen HC, et al. Eur Neurol. 2015;73(3-4):238-246. 16

“Resetting” the Immune System:
B-Cell Depletion
With recovery:
• Depleting peripheral B-cell population maintains
immune surveillance
• Pro-B cells and antibody-producing
plasmablasts/plasma cells are unaffected by
CD20 depletion
Lehmann-Horn K, et al. Ther Adv Neurol Disord. 2013;6(3):161-173. 17

Newer and Novel
Mechanisms of MS Disease-
Modifying Therapies

Anti-CD20 Monoclonal Antibodies
• B-lymphocyte antigen CD20: glycoprotein on
surface of all B cells1
• 3 anti-CD20 monoclonal antibodies (mAbs)
under study for treatment of MS2:
• Rituximab (chimeric human/mouse IgG1)
• Ocrelizumab (humanized IgG1)
• Ofatumumab (fully human IgG1)
1. Lehmann-Horn K, et al. Ther Adv Neurol Disord. 2013;6(3):161-173.
2. von Büdingen HC, et al. Eur Neurol. 2015;73(3-4):238-246. 19

What Are the Goals of Induction
Therapies in MS?
• Rapid onset of action
• Significant impact on disease activity
• Durable mechanism of action
• Long-term influence on immune
regulation/modulation
• Acceptable safety profile with respect to immune
activity (fighting infections, viruses)
20

Ocrelizumab Phase II Data
(Gd+ Lesions)
Gd+ = gadolinium-enhancing.
Kappos L, et al. Lancet. 2011;378(9805):1779-1787. 21
Placebo (n=54)
Ocrelizumab 600 mg (n=51)
Ocrelizumab 2000 mg (n=52)
Interferon-beta-1a (n=52)
0 4 8 12 16 20 24
Weeks
0
1
2
3
4
5
6
7
Mean T
1 g
adolin
ium
-enhancin
g lesio
ns
(95%
Cl)

Ocrelizumab: Phase III Trials
OPERA I and II1
• Relapsing-remitting MS (N=800 each)
• Ocrelizumab 2 x 300 mg IV, followed by 600 mg IV every 24
weeks vs
• IFN-beta-1a 44 mcg SC 3 x weekly
• Primary outcome: annualized relapse rate at 96 weeks
ORATORIO2
• Primary progressive MS (N=732)
• Ocrelizumab 600 mg IV every 24 weeks vs placebo
• Age 18-55 years; EDSS 3.0-6.5, abnormal CSF
• Primary outcome: time to sustained progression
EDSS = Expanded Disability Status Scale.
1. Hauser S, et al. 31st ECTRIMS, 7-10 Oct., 2015. Barcelona, Spain. Abst. 190.
2. Montalban X, et al. 31st ECTRIMS, 7-10 Oct., 2015. Barcelona, Spain. Abst. 228. 22

Ocrelizumab Phase III Results
PPMS (ORATORIO)2 Reduced proportion of patients with:
• Confirmed disability progression at 12 weeks by 24% vs placebo (25% by 24 weeks, P=0.0365)
• Worsening on Timed 25-Foot Walk Test by 29% vs placebo (P=0.0404)
• Whole-brain volume loss over 120 weeks, by 17.5% vs placebo (P=0.0206)
PPMS = primary progressive MS; RRMS = relapsing-remitting MS.
1. Hauser SL, et al. Presented at ECTRIMS 2015; abstract 190 (OPERA).
2. Montalban X, et al. Presented at ECTRIMS 2015; abstract 228 (ORATORIO). 23
Study Interferon-β-1a Ocrelizumab Reduction P Value
Annualized relapse rate
OPERA I OPERA II
0.292 0.290
0.156 0.155
46% 47%
<0.0001 <0.0001
Gadolinium-enhancing lesions
OPERA I OPERA II
0.286 0.416
0.016 0.021
94% 95%
<0.0001 <0.0001
RRMS (OPERA I and II)1

Goals for Long-Term Follow-Up
Studies of CD20 Therapies
• Crossover trials will move patients into most
effective treatment group
• No long-term IFN comparator group
• Sustained benefits over time:
– Brain atrophy
– New lesion acquisition
– Relapse activity
– EDSS progression
24

NEDA (“No Evidence of Disease
Activity”)
• Is NEDA an aspirational outcome?
• Useful outcome in clinical trials to show the
maximum potential efficacy of a therapy
• Percentage of patients achieving NEDA in a
real-world setting is unknown
Imitola K, Racke ML, JAMA Neurol. 2015;72:145-147. 25

Ofatumumab: Phase II Data
MIRROR Study
• RRMS, N=232
Subcutaneous dosing:
• Phase II study compared every 12 weeks and every 4 weeks
Overall Objective:
• Determine MRI efficacy and tolerability/safety of SC ofatumumab doses of 3, 30, and 60 mg vs placebo
Primary Endpoint:
• Cumulative number of new T1 Gd+ brain lesions over 12 weeks, vs placebo
Bar-Or A, et al. Neurology. 2014;82(10 Suppl):S23.006. 26

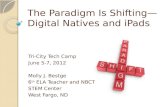
Ofatumumab: Cumulative T1
Lesions (Phase II)
Bar-Or A, et al. Neurology. 2014;82(10 Suppl):S23.006. 27
Wk 4 Wk 8 Wk 12 Wk 16 Screening Wk 20 Wk 24 Wk 36 Wk 48
0
1
2
Me
an
Nu
mb
er
of C
um
ula
tive
Le
sio
ns
3
4
5
6
7
8
9 Placebo (N=67)
Ofatumumab 3 mg q12w (N=32)
Ofatumumab 30 mg q12w (N=32)
Ofatumumab 60 mg q12w (N=32)
Ofatumumab 60 mg q4w (N=63)

Alemtuzumab: Anti-CD52
• CD52: glycoprotein present on surface of normal
T and B lymphocytes, monocytes, dendritic cells
• Alemtuzumab: humanized mAb directed against
CD52 cell-surface protein
• Depletes mainly T and B lymphocytes
• To a lesser degree, depletes monocytes,
macrophages, dendritic cells, NK cells
NK cells = natural killer cells.
Zhang X, et al. J Immunol. 2013;191(12):5867-5874. 28

Alemtuzumab: Anti-CD52 (cont’d)
• Rapid depletion of peripheral lymphocytes and
monocytes1
• Alemtuzumab depletes CD52-bearing T cells,
but does not affect hematopoietic stem cells2
• Monocytes return to pre-treatment levels within
1 month; B cells recover in 3 months1
• Potential for reconstitution of immune response
is preserved2
1. Freedman MS, et al. J Clin Cell Immunol. 2013;4(4).
2. Zhang X, et al. J Immunol. 2013;191(12):5867-5874 29

Months after alemtuzumab
T- and B-Cell Reconstitution After
Alemtuzumab
Thompson SA, et al. J Clin Immunol. 2010;30(1):99-105.
Months after alemtuzumab
30
*P<0.05; **P<0.01.

6-month SAD defined as EDSS score increase ≥1.0 point for ≥6 months (or ≥1.5 points when baseline EDSS = 0).
1. Freedman M, et al. Presented at AAN 2013; abstract PO7.1111. 2. Coles AJ, et al. Lancet. 2012;380(9856):1829-1839. 31
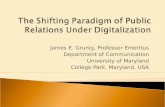
Alemtuzumab Efficacy in MS
Alemtuzumab significantly reduced clinical disease activity in
patients who relapsed on prior therapy
• Alemtuzumab significantly reduced annualized relapse rate (ARR)1 and risk of 6-month sustained accumulation of disability (SAD)2 by an additional 49.4% and 42% beyond SC IFN-β-1a, respectively, in patients who relapsed on prior therapy
• Benefits on clinical disease activity were similar regardless of type, duration, or number of prior treatments1
alemtuzumab
IFN-β-1a

Targeting Therapeutic Selection
in MS
• How can we determine appropriate patient
selection for B-cell‒depleting therapies?
• Are there groups of patients who do not benefit
from these treatment strategies?
• Should we be treating earlier with more
aggressive therapies?
• Does stopping immune system activity early in
disease prevent long-term progression?
32

ACR/EULAR Definition of Remission
in Rheumatoid Arthritis
• Boolean-based definition: At any time point, a
patient must satisfy all of the following:
– Tender joint count ≤1
– Swollen joint count ≤1
– CRP ≤1 mg/dL
– Patient Global Assessment ≤1
• Index-based definition: At any time point, a
patient must have:
– Simplified Disease Activity Index (SDAI) ≤3.3
ACR/EULAR = American College of Rheumatology/European League Against Rheumatism; CRP = C-reactive protein.
Bykerk VP, Massarotti EM. Rheumatology (Oxford). 2012;51(Suppl 6):vi16-vi20. 33

Treating Progressive
Forms of MS: Impact of
Newer Mechanisms

Active Disease Relapses, new/increasing neurologic
dysfunction, full or partial recovery
Progressive Disease Steadily increasing dysfunction or
disability without unequivocal recovery
Worsening Disease Documented increase in neurologic
dysfunction due to relapses or
progressive disease
Confirmed Progression or
Worsening
Increase of neurologic dysfunction
confirmed through a defined time interval
(eg, 3, 6, 12 months)
Revised Phenotype Classification
(Lublin 2013)
Lublin FD, et al. Neurology. 2014;83(3):278-286. 35

Determining Active vs Inactive
Inflammation in Progressive MS
• Disease burden may continue to advance in some people with MS despite lack of Gd+ lesion activity
• Some patients with progressive forms of MS have continued inflammatory activity
• This subpopulation of patients showed benefit from rituximab in early trials
• New data on B-cell therapies in patients with progressive MS will elucidate the role of lymphocyte depletion in these phenotypes
36

Educating Patients About
Disease Mechanisms and
Management

Role of Patient Education on
Therapeutic Mechanisms
• Many MS patients are well informed; discussing pathophysiology/mechanism of action is increasingly important
• Risks of particular mechanisms are important part of discussion: – Importance of adherence to monitoring protocols
– Importance of follow-up to therapies
• Therapeutic decisions may be based on response to previous treatments and on individual perceptions of risk vs benefit
38

This completes this activity, “Shifting the
Treatment Paradigm for Multiple Sclerosis:
Advances in Pathophysiology and Emergence
of Novel Disease-Modifying Therapies.”
Thank you for joining us. Please complete the
post-test and program evaluation to receive
Continuing Medical Education credit.
39