
Shear lag sutures: Improved suture repair through the …web.mst.edu/~vbirman/papers/Shear lag...
11
Shear lag sutures: Improved suture repair through the use of adhesives Stephen W. Linderman a,b , Ioannis Kormpakis a , Richard H. Gelberman a , Victor Birman c , Ulrike G.K. Wegst d , Guy M. Genin e,⇑ , Stavros Thomopoulos a,b,e, * a Department of Orthopaedic Surgery, Washington University, St Louis, MO 63110, United States b Department of Biomedical Engineering, Washington University, St Louis, MO 63130, United States c Engineering Education Center, Missouri University of Science and Technology, St Louis, MO 63131, United States d Thayer School of Engineering, Dartmouth College, Hanover, NH 03755, United States e Department of Mechanical Engineering and Materials Science, Washington University, St Louis, MO 63130, United States article info Article history: Received 22 December 2014 Received in revised form 27 March 2015 Accepted 7 May 2015 Available online 25 May 2015 Keywords: Adhesive Suture Flexor tendon Shear lag Biomechanics abstract Suture materials and surgical knot tying techniques have improved dramatically since their first use over five millennia ago. However, the approach remains limited by the ability of the suture to transfer load to tissue at suture anchor points. Here, we predict that adhesive-coated sutures can improve mechanical load transfer beyond the range of performance of existing suture methods, thereby strengthening repairs and decreasing the risk of failure. The mechanical properties of suitable adhesives were identified using a shear lag model. Examination of the design space for an optimal adhesive demonstrated requirements for strong adhesion and low stiffness to maximize the strength of the adhesive-coated suture repair con- struct. To experimentally assess the model, we evaluated single strands of sutures coated with highly flexible cyanoacrylates (Loctite 4903 and 4902), cyanoacrylate (Loctite QuickTite Instant Adhesive Gel), rubber cement, rubber/gasket adhesive (1300 Scotch-Weld Neoprene High Performance Rubber & Gasket Adhesive), an albumin-glutaraldehyde adhesive (BioGlue), or poly(dopamine). As a clinically rel- evant proof-of-concept, cyanoacrylate-coated sutures were then used to perform a clinically relevant flexor digitorum tendon repair in cadaver tissue. The repair performed with adhesive-coated suture had significantly higher strength compared to the standard repair without adhesive. Notably, cyanoacry- late provides strong adhesion with high stiffness and brittle behavior, and is therefore not an ideal adhe- sive for enhancing suture repair. Nevertheless, the improvement in repair properties in a clinically relevant setting, even using a non-ideal adhesive, demonstrates the potential for the proposed approach to improve outcomes for treatments requiring suture fixation. Further study is necessary to develop a strongly adherent, compliant adhesive within the optimal design space described by the model. Ó 2015 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved. 1. Introduction Sutures are an age-old technology: they have been used for wound closure for over 5 millennia, dating back to sutures used in ancient Egypt, as described in the Edwin Smith Papyrus from 3000 to 1600 BC [1–3]. While many improvements in suture mate- rials and intricate knot tying techniques have been introduced over the years, the core method of directly sewing tissues together remains a crude mechanical solution. Sutures typically work in pure tension along most of their length. Tension is transferred to the tissue only at anchor points (Fig. 1). High stress concentrations at these anchor points can lead to sutures breaking or cutting through the surrounding tissue. This phenomenon limits the max- imum force that can be transferred across the repair site. While current suturing techniques are sufficient to maintain the integrity of many surgical repairs, musculoskeletal tissue reconstruction (e.g., tendon and ligament repair) typically demands strong biomechanical resilience to accommodate activities of daily living without risking rupture. For example, repair-site elongation and rupture rates of up to 48% have been described after flexor tendon repair, even with modern suturing and rehabilitation protocols [4–7]. Rotator cuff repairs, which require reattachment of materi- als with disparate mechanical properties (tendon and bone), have recently reported failure rates as high as 94% [8–10]. Improved suturing schemes would allow for the transfer of greater loads across the repair site, reducing rupture and gap formation between http://dx.doi.org/10.1016/j.actbio.2015.05.002 1742-7061/Ó 2015 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved. ⇑ Corresponding authors at: Department of Orthopaedic Surgery, Washington University, St Louis, MO 63110, United States (S. Thomopoulos), Department of Mechanical Engineering and Materials Science, Washington University, St Louis, MO 63130, United States (G. Genin). E-mail addresses: [email protected] (G.M. Genin), thomopouloss@wustl. edu (S. Thomopoulos). Acta Biomaterialia 23 (2015) 229–239 Contents lists available at ScienceDirect Acta Biomaterialia journal homepage: www.elsevier.com/locate/actabiomat
Transcript of Shear lag sutures: Improved suture repair through the …web.mst.edu/~vbirman/papers/Shear lag...

Acta Biomaterialia 23 (2015) 229–239
Contents lists available at ScienceDirect
Acta Biomaterialia
journal homepage: www.elsevier .com/locate /actabiomat
Shear lag sutures: Improved suture repair through the use of adhesives
http://dx.doi.org/10.1016/j.actbio.2015.05.0021742-7061/� 2015 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.
⇑ Corresponding authors at: Department of Orthopaedic Surgery, WashingtonUniversity, St Louis, MO 63110, United States (S. Thomopoulos), Department ofMechanical Engineering and Materials Science, Washington University, St Louis, MO63130, United States (G. Genin).
E-mail addresses: [email protected] (G.M. Genin), [email protected] (S. Thomopoulos).
Stephen W. Linderman a,b, Ioannis Kormpakis a, Richard H. Gelberman a, Victor Birman c,Ulrike G.K. Wegst d, Guy M. Genin e,⇑, Stavros Thomopoulos a,b,e,*
a Department of Orthopaedic Surgery, Washington University, St Louis, MO 63110, United Statesb Department of Biomedical Engineering, Washington University, St Louis, MO 63130, United Statesc Engineering Education Center, Missouri University of Science and Technology, St Louis, MO 63131, United Statesd Thayer School of Engineering, Dartmouth College, Hanover, NH 03755, United Statese Department of Mechanical Engineering and Materials Science, Washington University, St Louis, MO 63130, United States
a r t i c l e i n f o
Article history:Received 22 December 2014Received in revised form 27 March 2015Accepted 7 May 2015Available online 25 May 2015
Keywords:AdhesiveSutureFlexor tendonShear lagBiomechanics
a b s t r a c t
Suture materials and surgical knot tying techniques have improved dramatically since their first use overfive millennia ago. However, the approach remains limited by the ability of the suture to transfer load totissue at suture anchor points. Here, we predict that adhesive-coated sutures can improve mechanicalload transfer beyond the range of performance of existing suture methods, thereby strengthening repairsand decreasing the risk of failure. The mechanical properties of suitable adhesives were identified using ashear lag model. Examination of the design space for an optimal adhesive demonstrated requirements forstrong adhesion and low stiffness to maximize the strength of the adhesive-coated suture repair con-struct. To experimentally assess the model, we evaluated single strands of sutures coated with highlyflexible cyanoacrylates (Loctite 4903 and 4902), cyanoacrylate (Loctite QuickTite Instant Adhesive Gel),rubber cement, rubber/gasket adhesive (1300 Scotch-Weld Neoprene High Performance Rubber &Gasket Adhesive), an albumin-glutaraldehyde adhesive (BioGlue), or poly(dopamine). As a clinically rel-evant proof-of-concept, cyanoacrylate-coated sutures were then used to perform a clinically relevantflexor digitorum tendon repair in cadaver tissue. The repair performed with adhesive-coated suturehad significantly higher strength compared to the standard repair without adhesive. Notably, cyanoacry-late provides strong adhesion with high stiffness and brittle behavior, and is therefore not an ideal adhe-sive for enhancing suture repair. Nevertheless, the improvement in repair properties in a clinicallyrelevant setting, even using a non-ideal adhesive, demonstrates the potential for the proposed approachto improve outcomes for treatments requiring suture fixation. Further study is necessary to develop astrongly adherent, compliant adhesive within the optimal design space described by the model.
� 2015 Acta Materialia Inc. Published by Elsevier Ltd. All rights reserved.
1. Introduction
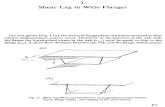
Sutures are an age-old technology: they have been used forwound closure for over 5 millennia, dating back to sutures usedin ancient Egypt, as described in the Edwin Smith Papyrus from3000 to 1600 BC [1–3]. While many improvements in suture mate-rials and intricate knot tying techniques have been introduced overthe years, the core method of directly sewing tissues togetherremains a crude mechanical solution. Sutures typically work inpure tension along most of their length. Tension is transferred to
the tissue only at anchor points (Fig. 1). High stress concentrationsat these anchor points can lead to sutures breaking or cuttingthrough the surrounding tissue. This phenomenon limits the max-imum force that can be transferred across the repair site. Whilecurrent suturing techniques are sufficient to maintain the integrityof many surgical repairs, musculoskeletal tissue reconstruction(e.g., tendon and ligament repair) typically demands strongbiomechanical resilience to accommodate activities of daily livingwithout risking rupture. For example, repair-site elongation andrupture rates of up to 48% have been described after flexor tendonrepair, even with modern suturing and rehabilitation protocols[4–7]. Rotator cuff repairs, which require reattachment of materi-als with disparate mechanical properties (tendon and bone), haverecently reported failure rates as high as 94% [8–10]. Improvedsuturing schemes would allow for the transfer of greater loadsacross the repair site, reducing rupture and gap formation between

Fig. 1. An 8-stranded Winters–Gelberman suture repair technique is shown forhuman flexor digitorum profundus tendon repair [11]. Red shading indicateslocation of load transfer. Current suturing techniques generate stress concentra-tions at anchor points where the suture bends within tissue. Adhesive-coatedsutures could distribute that load transfer along the entire length of the suture,reducing peak stresses and improving overall repair construct mechanics.
230 S.W. Linderman et al. / Acta Biomaterialia 23 (2015) 229–239
the repaired tissues and improving healing outcomes, not only bystrengthening repairs but also by enabling more aggressive reha-bilitation protocols. By holding the tissues together for longer timeintervals, mechanical solutions that prevent gap formation anddevelopment could provide more time for the biological healingresponse to generate a strong, organized tissue instead of disorga-nized scar [5,11,12].
Here, a new approach is proposed to augment standard suturingtechnology. Conventional sutures have a relatively large surfacearea passing through the tendon that is currently not utilized forload transfer. We envision a modified suture with an adsorbed orcovalently bound adhesive that tightly binds collagen along thesuture’s length, thereby reducing stress concentrations and betterdistributing load (Fig. 1). We hypothesized that adhesives alongthe length of the suture would transfer load more effectively thanconventional suture without adhesive. This improvement in loadtransfer is expected to result in an improvement in overall repairconstruct mechanical properties. Note that achieving the fullstrength of an uninjured tendon is unnecessary, as tendons areover-designed and are typically able to accommodate many timesmore load than is applied physiologically [13–15]. We aim to gen-erate functional repairs that are sufficient to accommodate in vivoloads and enhanced rehabilitation protocols. We focus here on sin-gle stranded sutures or pseudo-monofilament sutures, includingmultiple strands within an outer casing, because these are usedsurgically for flexor tendon repair [11].
In order to predict the ability of adhesive-coated sutures toimprove load transfer, we employed a shear lag model [16–19] ofsuture within a cylindrical tissue (e.g., a tendon). Using this model,we identified desirable adhesive mechanical properties to improveload transfer across a repair site. We then biomechanically testedsutures coated with adhesives to validate the model and experi-mentally assess the capacity to improve load transfer.
Table 1Abbreviations and variables used throughout the manuscript.
PBS Phosphate buffered salinesðxÞ Shear stress in the adhesive layersfail Failure shear stress of adhesive-coated sutureEs Suture elastic modulusEt Tendon elastic modulusG�a Adhesive shear modulus normalized by tendon elastic modulusL Suture purchase lengthPs Normal force in suture at the interface, x ¼ 0rs Suture radiusrt Tendon radiusta Adhesive thicknessbs Characteristic (inverse) length scale related to geometry and material propert
2. Materials and methods
2.1. Terminology
Throughout this paper, ‘‘suture’’ refers to the core strand ofsuture, ‘‘adhesive’’ refers to the adhesive layer, ‘‘assembly’’ and‘‘adhesive-coated suture’’ refer to the combination of suture withadhesive surrounding it, and ‘‘repair’’ refers to the complete tissuerepair, including several strands of adhesive-coated suture and aregion of tissue in which these are embedded. Abbreviations andvariables are described in Table 1.
2.2. Ex vivo surgical repair model
To experimentally assess the ability of adhesives to improve loadtransfer, a number of adhesive coatings were added to singlepseudo-monofilament polycaprolactam 4–0 suture strands(Supramid, S. Jackson, Inc., Alexandria, VA) and inserted into tendontissue prior to performing pullout tests. Single strands withoutknots were chosen to isolate the effects of the adhesive and mimicthe mathematical model as closely as possible. The following adhe-sives were examined: highly flexible cyanoacrylates (Loctite 4903and 4902, based on ethyl and octyl cyanoacrylate [20,21]; HenkelCorporation, Düsseldorf, Germany), cyanoacrylate (LoctiteQuickTite Instant Adhesive Gel, based on ethyl cyanoacrylate [22],Henkel Corporation, Düsseldorf, Germany), rubber cement(Elmer’s Rubber Cement; Elmer’s Products, Inc., Columbus, OH),rubber/gasket adhesive (1300 Scotch-Weld Neoprene HighPerformance Rubber & Gasket Adhesive; 3 M, St. Paul, MN),BioGlue (CryoLife Inc., Kennesaw, GA), and polydopamine [23,24](Sigma Aldrich, St. Louis, MO). Henkel does not release the exactchemical composition of their products. Of these adhesives, onlyBioGlue is FDA approved for use inside the body. These commer-cially available adhesives were chosen solely to assess the conceptproposed here, not to promote the use of any particular adhesiveclinically. Loctite 4903 and 4902 have shear moduli of 538 MPaand 399 MPa, respectively [25]. BioGlue, rubber cement, and rub-ber/gasket adhesives [26] have shear moduli on the order of 0.5–5 MPa [27–29]. Suture was passed through cadaveric canine hind-paw flexor digitorum profundus tendons using a French eye needle.All tendons tested in this study were from hindpaws of healthyfemale adult mongrel dogs 20–30 kg in weight (Covance Research,Princeton, NJ), taken postmortem from an unrelated project.Canine intrasynovial flexor tendons have been used extensively byour group and others since the early 1960s as a reliable model ofhuman tendon repair; we expect the results from this model to becomparable to those that would be obtained from human flexor ten-don reconstructions [5,30–36]. Tendons had elliptical cross sectionswith major and minor radii approximately 3 mm and 1 mm,
x Position along suturesave Average shear stress�rsðxÞ Normal stress in suture normalized by normal stress at x ¼ 0E�s Suture elastic modulus normalized by tendon elastic modulusGa Adhesive shear modulus
Lintersect Suture length where asymptotic limits for load transfer intersectPk Resultant normal force in suture at the anchor pointr�t Tendon radius normalized by suture radiusq�t Effective radius of tendon, normalized by suture radiust�a Adhesive thickness normalized by suture radius
ies v Variable related to geometry and material properties

S.W. Linderman et al. / Acta Biomaterialia 23 (2015) 229–239 231
respectively. The tendon was first dissected away from surroundingtissue and a complete transection was made in Zone II [37] perpen-dicular to the long axis of the tendon. Suture was passed from theside of the tendon 10 mm from the site of transection toward thelaceration interface. The suture was pulled through the tendon sothat only a single suture strand remained within the tendon. Inthe adhesive-coated suture tests, the adhesive was injected ontothe suture and the suture was pulled into place, dragging the adhe-sive into the tendon. Adhesive that accumulated on the side of thetendon was cleared with gauze soaked in phosphate buffered saline(PBS). The assembly within the tendon was wrapped in PBS-soakedgauze in an airtight tube and then allowed to cure overnight at 4 �Cbefore biomechanical testing. This curing procedure was chosen toensure that the postmortem tissue ex vivo would not rot ordeteriorate.
To assess the ability of adhesive to improve load transfer in aclinically relevant setting, cadaveric canine hindpaw flexor digito-rum profundus tendons with Zone II lacerations [37] were repairedusing 8-strand Winters–Gelberman repairs [11] (n ¼ 11; Supramid4–0 suture; S. Jackson Inc., Alexandria, VA), as diagrammed in Fig. 1and described previously [38]. Control repairs without adhesivewere compared to repairs with Loctite 4903-coated suture. Loctite4903 was chosen based on results of single suture pullout testsdescribed above. All surgeries were performed by IK, an orthopedichand surgeon. For adhesive-augmented repairs, sutures werepassed through the tendon following usual surgical technique, thenfor each suture pass, Loctite 4903 was injected onto the suturestrands using a syringe immediately prior to pulling theadhesive-coated suture into its final position. The outside of the ten-don was cleaned with PBS-soaked gauze to remove any excess adhe-sive. Repairs were completed with a continuous, nonlockingperipheral stitch using 5–0 nylon suture, as performed clinically[4,11,39,40]. The repaired tendon and distal phalangeal bone werewrapped in PBS-soaked gauze in an airtight tube and then allowedto cure overnight at 4 �C to prevent tissue deterioration beforebiomechanical testing.
2.3. Biomechanical testing
Samples were brought to 37 �C prior to biomechanical testing.For single suture strand pullout tests, any suture and adhesive out-side of the lateral tendon was first dissected away. This ensuredthat the effect was due to adhesive along the length of the sutureinstead of adhesive accumulated at the suture entrance point.Samples were then tested in uniaxial tension on a materials testingframe (ElectroPuls E1000; Instron Corp., Norwood, MA, chosenbecause of a low noise load cell suitable for distinguishingmilli-Newton level forces). The tendon was clamped in a stationarygrip so 15 mm of tendon length was exposed. Suture was carefullyplaced in a jig consisting of a low friction spool and a clamp grip,which was pulled upward at 0.3 mm/s to apply tension to thesuture. The gauge length between the tendon and suture gripswas 8.5 cm for all samples at the start of the test. Pullout (failure)force of single adhesive-coated suture strands within tendon tissuewere determined from the force–elongation curves.
Clinical repairs of cadaveric flexor digitorum profundus tendonswere tested as described previously [41–43,36]. After precondi-tioning, samples were pulled in uniaxial tension using a materialtesting machine (5866; Instron Corp., Norwood, MA, chosenbecause of a high capacity load cell) at 0.3 mm/s until failure.Strain was determined optically to determine when a physiologi-cally relevant 2 mm gap formed between the repaired tendon ends.Immediately prior to testing, tendons were stained with a specklepattern of freshly prepared Verhoeff stain to provide a surface tex-ture for optical tracking. Elongation measurements from the mate-rial testing machine were synced with optical recordings from a
high resolution camera at a frame rate of 4 Hz (illunis,Minnetonka, MN), similar to described previously [44]. Opticaltracking of points proximal and distal to the laceration interfaceenabled accurate determination of local tissue strain. From theforce–elongation curves, maximum force, required to create a2 mm gap in the repair (a clinically relevant measure of repairstrength [5]), and stiffness (slope of the linear region) were deter-mined. From the force–strain curves, strain at 20 N force (approx-imating strains at physiologically relevant load levels [45,46]) andresilience (area under the curve until yield) were determined.
2.4. Statistics
Statistical analysis for all experiments was performed bynon-parametric Wilcoxon rank-sum using MATLAB. Statistical sig-nificance was set at p < 0:05 unless otherwise noted.
3. Theory
3.1. Shear lag model
A shear lag model was studied to identify adhesives with desir-able properties for suture repair (Appendix A). The model pre-dicted load sharing between the sutures and an idealizedisotropic, homogeneous repaired tendon.
The load Ps on an assembly that would cause adhesive failurewas estimated from the following expression for the shear stresssðxÞ as a function of the position, x, along a suture (Fig. 2):
sðxÞsave
¼ bsLv sinhðbsLÞ
v� 1ð Þ cosh bsðx� LÞð Þ � Pk
Psv� 1
� �cosh bsxð Þ
� �ð1Þ
where save ¼ Ps2prsL is the average shear stress; L is the suture pur-
chase length (i.e., the length of the straight section of the suturewithin the connected section of the tendon); Pk is the resultant nor-mal force in the suture at the anchor point (the knot at x ¼ L); Ps isthe normal force in the suture at the interface (x ¼ 0); and v and thecharacteristic (inverse) length scale bs relate to the geometry andmaterial properties:
v ¼ 1þ q�2t
E�sð2Þ
b2s ¼
1r2
s
2G�at�a
1q�2tþ 1
E�s
� �ð3Þ
where q�2t ¼ r�2t � 1þ t�a� �2, in which r�t and t�a are, respectively, the
tendon radius and adhesive thickness normalized by the sutureradius rs; and E�s and G�a are, respectively, the suture elastic modulusand adhesive shear modulus normalized by the tendon elastic mod-ulus Et . The peak shear stress in the adhesive occurs at the interfacex ¼ 0 (Fig. 3). Equating this to the adhesive failure shear stress, sfail,and solving (1) for the case of Pk ¼ 0 yields:
Pmax
2pr2s
� �¼ sfail
Lrs
sinhðbsLÞbsL
vðv� 1Þ coshð�bsLÞ þ 1
ð4Þ
Note that sfail could be limited by failure at the interfaces withadherends (i.e., suture or surrounding tissue) or failure within theadherends themselves. This solution is nearly bilinear, with twoasymptotes (Figs. 4 and 5):
limL!1
Pmax
2pr2s
� �¼ sfail
E�s t�a2G�a
1þ E�sq�2t
� �� �12
ð5Þ
limGa!0
Pmax
2pr2s
� �¼ sfail
Lrs
ð6Þ

(A) (B)
Fig. 3. Shear stress vs. position along the length of a suture is shown. (A) The peak shear stress decreases as the adhesive shear modulus decreases because compliantadhesives distribute loads over a longer distance than stiffer adhesives. (B) A typical repair with Supramid or other sutures is unbalanced in the shear lag sense (i.e., q�2t > E�s ,orange line, Ga ¼ 1 GPa), resulting in higher peak stresses. If a 38x stiffer suture were available to balance the adherends (black line, still using Ga ¼ 1 GPa), the peak stresswould drop by a factor of 8.5. In these calculations Pk ¼ 0 N, so that all of the load carried by the suture was transferred to the surrounding tissue via the adhesive.
Fig. 2. Diagram of adhesive-coated suture assembly within a cylindrical tissue, such as tendon, used to conduct shear lag analysis. Ps is the tensile load carried by the suture atthe interface between repaired tissues (i.e., at x ¼ 0). Pk is the load at an anchor point or knot, where the suture bends within the tissue (x ¼ L). This load, when too high, leadsto the assembly cutting through surrounding tissue and to rupture of the repair.
232 S.W. Linderman et al. / Acta Biomaterialia 23 (2015) 229–239
For a given suture, the first limit (L!1) shows that the force asuture can carry increases monotonically with decreasing adhesiveshear modulus G�a. Below a critical adhesive shear modulus, how-ever, the second limit (Ga ! 0) shows that a cut-off exists thatdepends upon the suture length. Therefore, the optimum strengthinvolves as compliant of an adhesive as possible provided that thesuture length is sufficient:
L P Lintersect � rsE�s t�a2G�a
1þ E�sq�2t
� �� �12
ð7Þ
As a test case for a clinically relevant suture repair scenario, themodel was analyzed using realistic tendon and suture materialproperties and a variety of realistic suture lengths and adhesiveproperties for a typical flexor digitorum profundus clinical repair:L ¼ 13 mm; rt ¼ 2 mm; Et ¼ 200 MPa; ta ¼ 100 lm; rs ¼ 100 lm,and Es ¼ 2 GPa [38,47–52].
4. Results
4.1. Shear lag model analysis
Shear lag modeling predicted that adhesive coatings on sutureswould improve load transfer compared to conventional sutures fora certain range of properties (white band, Fig. 4). Mechanicallydesirable adhesives would be compliant in shear while maintain-ing high binding and shear strengths. Compliant adhesives allowgreater deformation, thereby distributing loads over a larger lengththan stiff adhesives (Fig. 3a). This distribution reduces stress con-centrations at the suture anchor points, leading to anadhesive-coated suture assembly that carries greater load beforefailure. In addition to adhesive properties, the maximum shearstress in the adhesive is minimized by balancing the adherends[53] (i.e., tissue and suture) so that E�s ¼ q�2t (Appendix A). Theseadherends are not balanced with current Supramid surgical sutureand tendon. When adherends (tendon and suture) are balanced by

(A)
(B)
Fig. 5. Increasing suture length increases maximum load carried by assembly, i.e.,load causing adhesive to fail, only until a point. Above a transitional suture length,load capacity is governed by an asymptote independent of suture length. (A)Maximum load carried by an assembly, Pmax , as a function of suture length, L, withrespect to the length Lintersect . Maximum load is normalized by the maximum loadtransferred by an infinitely long suture, Pmaxð1Þ. At L ¼ Lintersect , the maximum loadis 76.0% of the asymptotic maximum load for an infinitely long suture. Note thatthis is an invariant curve that is true for any combination of ta;Ga; Es; rs; Et , and rt
that yields a particular value of Lintersect . (B) Maximum load carried by an assembly asa function of suture length for particular suture, tendon, and adhesive material andgeometric properties relevant to flexor tendon repair. Here the adhesive failureshear stress sfail ¼ 10 MPa, adhesive shear modulus Ga ¼ 100 kPa, adhesive thick-ness ta ¼ 0:1 mm, and Pk ¼ 0 N. Current suture length used in flexor tendon repairis 13 mm into each tendon end, as denoted by the dashed line.
Fig. 4. Contour map of maximum load transferred across the repair by an adhesive-coated suture strand, calculated from a wide array of theoretical adhesive shear moduliand adhesive failure shear stresses (i.e., strengths) given properties described in the methods, and overlaid with real material properties for several material types [25–28,54–56]. Maximum load transfer isoclines were normalized by the strength of healthy human flexor tendons (Ptendon � 1000 N) [57]. Maximum load transfer occurred with aninfinitely compliant and infinitely strong adhesive, toward the upper left corner of this contour plot. Current flexor tendon repairs carry approximately 10 N per suture strand,so relevant adhesive coatings would have failure loads above this level. Adhesive mechanical properties that are not expected to improve load transfer are shaded red (lowerportion). Note that the suture strand itself breaks above approximately 15.5 N for Supramid 4–0 or 23.5 N for Supramid 3–0 suture [38], so adhesive failure loads above thislevel would not further improve load transfer (shaded green, upper portion). Also note that shear modulus and failure shear stress are related for a given real material, so notall theoretical combinations are realistic.
S.W. Linderman et al. / Acta Biomaterialia 23 (2015) 229–239 233
assuming 38-fold stiffer suture, the peak stress is 8.5-fold lowerthan in conventional suture repair (Fig. 3b).
Shear lag modeling also predicted that maximum load transferwould increase with increasing adhesive-coated suture length.However, varying the ratio of suture length to Lintersect demonstratesthat adhesive-coated sutures approach the limit for maximum loadtransferred when the suture length, L, is 2–3 times Lintersect (Fig. 5a).The length of suture used is limited surgically by the particular tis-sue being repaired. Suture length of 13 mm was used in the modelto make results relevant to flexor digitorum profundus tendonrepair (Fig. 5b) [39]. A contour map of maximum load transfergiven various adhesive properties was generated using this length(Fig. 4). Properties of several real materials were then overlaid onthis contour map to identify promising candidate materials. Onlya small fraction of the material classes shown are relevant materi-als; the remainder are included for comparison, as is standard withan Ashby plot, and to highlight the importance of appropriateadhesive material selection. Assuming a compliant adhesive(Ga ¼ 100 kPa) with a strong shear strength (s ¼ 10 MPa) and thecurrent clinical suture length of 13 mm, maximum load transferper strand would approach 70 N of force. For the typical 4- and8-strand methods used in flexor tendon repair, this would resultin theoretical improvements of up to 280 N and 560 N, �4-foldand �8-fold improvements over current methods, respectively.
4.2. Ex vivo experimental results
Biomechanical tests of single strands of adhesive-coated suturewithin tendon tissue supported the model prediction that adhesivecoatings can increase force required to pull out a suture. Loctite4903, a ‘‘flexible’’ cyanoacrylate, improved the maximum load topull out a single suture strand in tendon from 0.076 N (±0.104 Nstandard deviation) without adhesive to 3.24 N (� 2.11 N;p ¼ 3:11 � 10�4) with an adhesive-coated suture strand (Fig. 6).

(A)
(B) (c)
Fig. 6. (A) Maximum loads resisted by single 4–0 Supramid suture strands coated with nothing (traditional suture), CryoLife BioGlue, Dopamine, Elmer’s rubber cement, 3 Mrubber and gasket adhesive 1300 (neoprene), Loctite Quicktite (cyanoacrylate), Loctite 4902 or Loctite 4903 (flexible cyanoacrylates) in cadaveric canine flexor digitorumprofundus tendon. The middle line within the box plots represents the median, the outer edges denote the 25 percentile and 75 percentile samples, and the whiskers extendto the extreme data points. Outliers are denoted by (+). Asterisks denote statistically significant differences compared to traditional suture (*p < 0:05, **p < 0:01). (B)Schematic of testing setup for single strand adhesive-coated suture pullout from tendon. (C) Representative force–elongation curve for Loctite 4903-coated suture pullout.
234 S.W. Linderman et al. / Acta Biomaterialia 23 (2015) 229–239
The more compliant adhesives tested did not meaningfullyincrease the maximum load necessary to pull out the suture, likelybecause of poor binding to suture and tissue.
The strongest single strands of adhesive-coated suture in tendonwere further evaluated in a clinically relevant 8-stranded cadavericcanine flexor tendon repair. Since the results for Quicktite, Loctite4902, and Loctite 4903 were comparable, the choice among themwas arbitrary from the mechanics perspective. In the clinically rele-vant ex vivo repairs, Loctite 4903-coated sutures increased maxi-mum load transfer by 17.0% (Control = 72.7 � 11.3 N; Loctite4903 = 85.0 � 8.6 N; p ¼ 0:009) and load to create a clinically rele-vant 2 mm gap by 17.5% (Control = 59.2 � 8.8 N; Loctite4903 = 69.5 � 11.2 N; p ¼ 0:032) compared to standard 8-strandedsuture repairs without adhesive coatings (Fig. 7; n ¼ 11 per group).Resilience, stiffness, and strain at 20 N applied force did not changesignificantly (Table 2).
5. Discussion
Although adhesives, especially cyanoacrylates [58], have beenused for decades in surgical repairs to replace or augment suturefor closing the skin and other tissues [59,60], their applicationhas been almost entirely limited to the interface between thealigned tissues. The application of adhesive to the lateral faces ofsutures has never been reported for a tissue that works in tension.To our knowledge, only one previous study used adhesive-soakedsutures, reporting an increase in re-bonding strength of repaired
meniscal tissue under compression compared to either suturealone or adhesive alone [61]. We hypothesized that the load distri-bution along sutures and the load tolerance of the repaired tissuescould be optimized using a mechanical model that predicts loadtransfer as a function of adhesive mechanical properties.Modeling and ex vivo experimental results demonstrated thatadhesive-coated sutures have the potential to improve thestrength of tensile tissue repairs, especially with the developmentof adhesives with optimal mechanical properties.
The modeling indicated that adhesives that are compliant toshear facilitate load transfer from the suture to the tendon by low-ering stress concentrations (Fig. 3). This strategy is somewhat anal-ogous to the tendon enthesis, where a compliant interfacial zonebetween tendon and bone [62–64] has been shown to optimizestress transfer and is hypothesized to toughen the interface [65].Similarly, a collagen-binding adhesive that directly attaches tothe suture via a small compliant layer in between the suture andthe collagen would be expected to better distribute load to mini-mize stress concentrations, enabling more effective load transferacross the repair. Finally, we note that compliant interfacesbetween fibers and matrix are associated with additional modesof toughening through crack deflection [66]; this can lead to tough-ening of the repair as a whole through decreased sensitivity toflaws that might otherwise lead to failure [67,68].
Adhesives with a broad range of physical properties areexpected to improve load repair strength. When the derived isocli-nes are plotted over the properties of real materials, as in a stan-dard Ashby plot [55,54,56], the model highlights a range of

Load creatinga 2mm gap
Maximum load0
20
40
60
80
100
Forc
e [N
]
Control repair (no adhesive)Repair with Loctite 4903-coated sutureOutliers
***(B)
bite length L = 12 mm
expo
sed
tend
on le
ngth
60 m
m
0.3 mm/s
Repaired
Distalphalynx
(A)
0 20 40 60 80 100 120Strain [%]
0
20
40
60
80
Forc
e [N
]
Loctite 4903-coated suture(C)
Fig. 7. Tendon repair load tolerance with and without adhesive. (A) Schematic of testing setup for clinically relevant repairs with adhesive-coated suture. (B) The plot showsload creating a 2 mm gap and maximum load for a cadaveric canine flexor digitorum profundus tendon repair using standard clinical surgical technique (8 stranded repairwith 4–0 Supramid suture, green) compared with the same repair style where suture was coated with Loctite 4903 (cyanoacrylate adhesive, blue with hash marks). Themiddle line within the box plots represents the median, the outer edges denote the 25 percentile and 75 percentile samples, and the whiskers extend to the extreme datapoints. Outliers are denoted by (+). Overbars and asterisks denote statistically significant differences (* p < 0:05, ** p < 0:01). (C) Representative force-strain curve for 8-stranded repair with Loctite 4903-coated suture.
Table 2Repair resilience, stiffness, and strain at 20 N load are shown for a cadaveric canine flexor digitorum profundus tendon repair using standard clinical surgical technique (8stranded repair with 4–0 Supramid suture) compared with the same repair style where suture was coated with Loctite 4903 (cyanoacrylate adhesive). Modified resilience shownhere is calculated from the force-strain curve.
Resilience Stiffness Strain at 20 N
Repair with Loctite 4903-coated suture 9.12 � 2.46 N 27.2 � 4.4 N/mm 8.00 � 1.36%Control repair (no adhesive) 7.39 � 2.22 N 24.0 � 7.0 N/mm 8.81 � 2.91%p-value 0.108 0.251 0.438
S.W. Linderman et al. / Acta Biomaterialia 23 (2015) 229–239 235
potential materials with appropriate mechanical properties(Fig. 4). Many of these are not biocompatible, but elastomers suchas polychloroprene, polyurethane rubber, and natural rubber dohave appropriate shear moduli and shear strength to be used asbase materials for adhesive development. Some biological materi-als, e.g., those based on elastin, could also be valuable for creatingbio-adhesives. Note that the shear strength used in this model maybe limited by either bulk failure within the adhesive material orinterfacial failure between the adhesive and adherends (i.e., sutureand tendon). Therefore, both the bulk adhesive mechanical proper-ties and the strength of adhesion are crucial factors for successfulapplication of this approach.
The proof-of-concept experiments performed here demonstratesubstantial improvements in load transfer across single strandpullout and clinically relevant tendon repairs, even thoughLoctite 4903 used in these tests is a stiff cyanoacrylate that is far
from ideal according to the shear lag model. The 3.24 N � 2.11 Nfailure load found experimentally for a single strand ofcyanoacrylate-coated suture within tendon tissue (Fig. 6) very clo-sely matches the predicted maximum load for cyanoacrylates fromthe shear lag model (Fig. 4). The 17% improvement in load toler-ance for a complete 8-stranded repair (Fig. 7), amounting toimprovement of 10–15 N, could substantially decrease rupture ratein flexor tendon repairs. The expected load transfer for clinicallyrelevant repairs comes partially from the shear lag load transferthrough adhesive and partially from the basal strength of a suturerepair with knots. This 17% improvement in load transfer across aclinically relevant repair represents 47% of the additive improve-ment expected for an 8-strand repair based on the single strandexperiments. We hypothesize that this discrepancy is due toimbalanced load sharing among strands in the surgical repair.Perfectly balanced repairs are not possible even for the highly

236 S.W. Linderman et al. / Acta Biomaterialia 23 (2015) 229–239
trained orthopaedic hand surgeons who performed the proceduresin this study because they require that (i) all strands have the exactsame tension applied to them when surgical knots are tied, (ii) thestrands be perfectly aligned with the longitudinal axis of the ten-don, and (iii) the tendon be loaded perfectly longitudinally.Therefore, some strands will carry more load than others in clini-cally relevant repairs, reducing the maximum load transfer.
The compliant adhesives tested here did not substantiallyimprove load transfer, as anticipated by overlaying their bulkmaterial properties on the shear lag model (Fig. 6). This discrep-ancy highlights the importance of compatibility between the dif-ferent materials (i.e., suture, adhesive, and tendon) and theresulting interfacial shear strengths. Overall shear strength couldbe limited by any of three factors: (i) the interfacial shear strengthbetween suture and adhesive, (ii) the interfacial shear strengthbetween adhesive and surrounding tissue, and (iii) the bulk shearstrength of the adhesive material. This study experimentally eval-uated the model using several commercially available adhesiveswithout prior knowledge of their binding strength to Supramid(polycaprolactam) sutures or tendon tissue. Notably, these com-mercially available adhesives were not optimized to adhere tosuture and tissue, whereas strength parameters used in the modelrepresented an optimal scenario where the interfacial shearstrengths were at least as strong as bulk shear strength of theadhesives. Poor binding strength of these commercially availableadhesives to suture or tissue might have limited the failure shearstress and efficacy for load transfer. While we tested Supramidsutures because of their surgical use in flexor tendon repair, differ-ent suture materials may have improved compatibility with partic-ular adhesives. In addition, multifilament sutures have increasedsurface area for adhesive integration and binding, serving as apotential mechanism to increase interfacial failure shear stress.
Since adhesives were simply injected onto the suture surfacebefore the suture was pulled into tissue, the compliant adhesivesmay have sheared off of the suture when pulled into place, beforeadequately curing could take place. One limitation of this experi-mental validation is the lack of suitable visualization of adhesivewithin the tissue along the length of the suture. We hope to over-come this limitation in future work. The modeling performed hereis applicable even for thin adhesive layers compared to the tissueand suture width. Furthermore, the methods described aboveensure that the effects seen experimentally were due to adhesivealong the length of the suture instead of adhesive at the entry pointinto tissue (Fig. 6).
Despite these limitations, the single-strand pullout results forcyanoacrylates were accurately predicted by the mathematicalmodel. This is possibly because Henkel publishes lap shearstrength for cyanoacrylates instead of block shear strength, sothe shear data includes interfacial adhesive strength.Additionally, cyanoacrylates are highly reactive compounds thatmay generate sufficient interfacial adhesive strength via covalentbonding with suture and with tendon that they were instead lim-ited by failure within the adhesive bulk.
The promising mechanical improvement seen in theseproof-of-concept studies with sub-optimal adhesives is still an orderof magnitude below the predicted improvement that could beachieved with an optimal adhesive. While current repairs are notstrong enough to sustain physiologic loading in all patients, evenmodest mechanical improvements are expected to make a substan-tial difference clinically. Therefore, we anticipate this technologywill be useful clinically even if we only see half of the maximumexpected improvement based on single-strand testing for a specifi-cally engineered compliant adhesive material. Note that we do notsuggest the specific adhesives tested in this proof-of-concept studybe used clinically. Rather, these results provide a foundation for thefurther development of adhesives with the desirable mechanical
properties predicted here, material compatibility with sutures andtissue, delivery methods that mitigate adhesives shearing off ofsuture, and appropriate biocompatibility for use in patients.
This shear lag model describes the importance of adhesivemechanical properties for creating a successful adhesive-coatedsuture; however, most currently used adhesives are not designedfor this purpose. Specifically engineering an adhesive material tobind suture and surrounding tissue tightly, while maintaining com-pliance to shear stress, could lead to substantially improvedadhesive-coated sutures. In addition to having appropriate mechan-ical properties once in place, an ideal adhesive-coated suture shouldbe inert for storage and surgical handling before it is placed into thebody. We envision several potential approaches to generate adhe-sive coatings that only activate when in place within tissue.
The shear lag model used in the current study employed severalsimplifying assumptions. First, shear lag models treat the displace-ment field as one-dimensional. Only displacements along the longaxis of the tendon/suture were considered. This approximation has,however, proven effective for a broad range of fibrous composites[17,69,70]. Second, the adhesive layer was considered to be verythin. For a thicker layer, deformation of the adhesive must be con-sidered explicitly, accounting for both axial displacements varyingthrough the thickness as well as radial displacements, especiallyfor highly compliant adhesives. Third, the stress field in the suturewas assumed to be independent of radial position, an approxima-tion valid only for relatively stiff sutures. Because non-absorbablesutures used in tendon repair can be assumed rigid in tension inthe range of the failure forces of the repair, this approximationshould be acceptable, especially for estimates of load transfer.Despite limitations listed above, this simplified model ofsuture-tendon interaction allows for adequate determination ofthe design space for an adhesive-coated suture for tissue repair.When used in combination with an Ashby plot showing real mate-rial properties [55], this model can identify promising base materi-als for adhesive-coated suture development.
6. Conclusion
Strengthening surgical repairs should lead to improved healingoutcomes for mechanically sensitive tissues, such as tendon. Ourmodels and proof-of-concept experiments suggest that coatingsutures with adhesives that are appropriately designed hold promisefor achieving repairs that have higher levels of resistance to gap for-mation and catastrophic failure. While Loctite 4903 shows promisingresults that would be valuable clinically, it is far from an ideal adhe-sive according to the model due to its high shear modulus. We intendto develop biocompatible adhesives with optimized mechanical andchemical properties to further increase load transfer and improveclinical repairs for tendon, ligament, and other tissue injuries.
Author contributions
SWL derived the shear lag model with help from VB and GMG.SWL designed and performed all experiments with guidance fromST, RHG, VB, and GMG. IK performed the surgeries and providedinput into how to apply adhesives to sutures during surgeries.UGKW provided input and data comparing model results to realmaterial properties. SWL wrote the manuscript, and ST, GMG, IK,RHG, VB, and UGKW provided edits.
Acknowledgements
This study was supported by the National Institutes of Health(NIH): U01 EB016422 (to ST and GMG), R01 AR062947 (to ST andRHG), T32 AR060719 (to SWL) and T32 GM007200 (to Medical

Fig. 8. Free body diagram showing an axisymmetric model of adhesive-coated suture within a cylindrical tendon tissue. Simultaneously analyzing a section of the repair (left)and each component independently (i.e., suture, adhesive, and tendon; right) allows derivation of a shear lag model to estimate shear stress within the adhesive. Note thatthis model reduces to a one-dimensional set of equations along the x-axis.
S.W. Linderman et al. / Acta Biomaterialia 23 (2015) 229–239 237
Scientist Training Program, Washington University in St. Louis).Loctite 4902 and 4903 were gifts from Henkel Corporation(Düsseldorf, Germany).
Appendix A. Shear lag analysis of an adhesive suture
The shear lag model applied was analogous to the [16,17] dou-ble lap joint solutions, and to the [18] axisymmetric solution (cf.Appendix B). We present a derivation here to highlight ourapproximations and how adhesive properties arise in the finalexpression.
The model was based upon the free body diagram in Fig. 8) andthe following assumptions: (a) the suture, adhesive, and tendonare linear elastic materials; (b) viscous effects are negligible; and(c) radial displacements, strains, and stresses are small. The latteris appropriate for a thin adhesive layer. The validity of theseassumptions has been established in composites with short[69,17] and long fibers (e.g., [70]), and by comparison to solutionsin which these assumptions were not made [71,72]. We note aswell that, although adhesives often exhibit nonlinearity and vis-coelasticity, the linear analysis is adequate and useful for the targetdesign range in which the adhesive is not close to failure.
The differential equation governing the normal stress in thesuture at position x is [17,18]:
d2 �rsðxÞdx2 � b2
s�rsðxÞ þ
b2s
v ¼ 0 ðA:1Þ
where �rðxÞ is normal stress in the suture normalized by the stressPs=pr2
s at x ¼ 0, and bs and v are defined in the main text. Solvingand applying the boundary condition �rsð0Þ ¼ 1 at the interfacebetween repaired tendon ends and �rsðLÞ ¼ Pk=Ps at the anchor orknot yields:
�rsðxÞ ¼1vþ 1� 1
v
� �cosh bsxð Þ
þ sinh bsxð ÞsinhðbsLÞ
Pk
Ps� 1
vþ1v� 1� �
cosh bsLð Þ� �
ðA:2Þ
Inserting this into the equilibrium equation yields an expression forthe shear stress sðxÞ (Eq. (1)).
Note that, as with lap joints (e.g. [53]), parametric analysis ofEq. (1) confirmed that peak stress is minimized if the inner andouter adherends (tendon and suture) are ‘‘balanced’’ so thatE�s ¼ q�2t (Fig. 3b). This is not the case for current Supramid surgicalsuture and tendon. Balancing requires a 38-fold stiffer suture, andwould reduce the peak stress by a factor of 8.5 (assuming geometryand material properties used in the main text).
Appendix B. Derivation from Nairn’s (1997) general, optimizedshear lag solution
[18] presented a general shear lag solution for n concentric,transversely isotropic cylinders that sustain an average axial stressof r0. We verify in this appendix that, for the case of n ¼ 3 anexpression analogous to that of Appendix A can be derived fromthis solution. Nairn’s governing equation for the interfacial shearstress srzðrÞ at suture/adhesive interface is:
2 �srzðrsÞ1E�sþ 1
E�aðt�2a þ2t�aÞ
!þð1þ t�aÞsrzðrsþ taÞ
E�aðt�2a þ2t�aÞ
" #
¼�s00rzðrsÞ1
4G�sþ ð1þ t�aÞ
2
2G�aðt�2a þ2t�aÞð1þ t�aÞ
2
t�2a þ2t�alnð1þ t�aÞ�1þ t�2a þ2t�a
2ð1þ t�aÞ2
!" #
þð1þ t�aÞ3s00rzðrsþ taÞ
2G�aðt�2a þ2t�aÞ1
t�2a þ2t�alnð1þ t�aÞ�1þ t�2a þ2t�a
2ð1þ t�aÞ2
!
ðB:1Þ
where G�s is the shear modulus of the suture normalized by the elas-tic modulus of the tendon and all other variables are as defined inAppendix A. For the adhesive/tendon interface,
2srzðrsÞ
E�aðt�2a þ2taÞ�ð1þ t�aÞsrzðrsþ taÞ
1E�aðt�2a þ2taÞ
þ 1q�2t
!" #
¼ s00rzðrsÞ2G�aðt�2a þ2t�aÞ
ð1þ t�aÞ2
t�2a þ2t�alnð1þ t�aÞ�1þ t�2a þ2t�a
2
!
�ð1þ t�aÞs00rzðrsþ taÞ1
2G�aðt�2a þ2t�aÞ1
t�2a þ2t�alnð1þ t�aÞ�1þ t�2a þ2t�a
2
!"
þ r�2t
2G�t q�2t
r�2t
q�2tln
r�2t
ð1þ t�aÞ2�1þ q�2t
2r�2t
!#ðB:2Þ
where G�t is the shear modulus of the tendon normalized by theelastic modulus of the tendon.
We model the case of a thin adhesive layer (t�a � 1) that is com-pliant compared to the suture and tendon (G�a � G�s and G�a � G�t ).We also assume that the shear stress to be uniform throughoutthe adhesive layer, as is reasonable for a thin layer. Thus,srzðrsÞ � srzðrs þ taÞ and s00rzðrsÞ � s00rzðrs þ taÞ.
Making the two assumptions noted above and rewriting theabove equations in the form
s00rz � b2Nsrz ¼ 0
yields:
b2N �
1r2
s
2G�at�a
1þ t�aq�2t
þ 1E�s
� �ðB:3Þ
which is equal to the expression in Eq. (2) for t�a � 1.

238 S.W. Linderman et al. / Acta Biomaterialia 23 (2015) 229–239
Appendix C. Figures with essential colour discrimination
Certain figures in this article, particularly Figs. 1 and 4, are dif-ficult to interpret in black and white. The full colour images can befound in the on-line version, at http://dx.doi.org/10.1016/j.actbio.2015.05.002.
References
[1] J.H. Breasted, The Edwin Smith Surgical Papyrus (Facsimile and HieroglyphicTransliteration with Translation and Commentary, in Two Volumes), TheUniversity of Chicago Press, Chicago, Illinois, 1930.
[2] J.P. Allen, The Art of Medicine in Ancient Egypt, The Metropolitan Museum ofArt, New York, NY, 2005.
[3] Unknown, Possibly Imhotep (Egyptian Physician); 3000–1600 B.C.; EdwinSmith Papyrus. URL:<http://archive.nlm.nih.gov/proj/ttp/flash/smith/smith.html>. URL Accessed URL:12/08/2014
[4] H.M. Kim, G. Nelson, S. Thomopoulos, M.J. Silva, R. Das, R.H. Gelberman,Technical and biological modifications for enhanced flexor tendon repair, J.Hand. Surg. Am. 35 (6) (2010) 1031–1037.
[5] R.H. Gelberman, M.I. Boyer, M.D. Brodt, S.C. Winters, M.J. Silva, The effect ofgap formation at the repair site on the strength and excursion of intrasynovialflexor tendons, J. Bone Joint Surg. Am. 81-A (7) (1999) 975–982.
[6] D.T. Fufa, D.A. Osei, R.P. Calfee, M.J. Silva, S. Thomopoulos, R.H. Gelberman, Theeffect of core and epitendinous suture modifications on repair of intrasynovialflexor tendons in an in vivo canine model, J. Hand Surg. Am. 37 (12) (2012)2526–2531.
[7] C. Xu, J. Zhao, D. Li, Meta-analysis comparing single-row and double-row repairtechniques in the arthroscopic treatment of rotator cuff tears, J. ShoulderElbow Surg. 23 (2) (2013) 1–7.
[8] L.M. Galatz, C.M. Ball, S.A. Teefey, W.D. Middleton, K. Yamaguchi, The outcomeand repair integrity of completely arthroscopically repaired large and massiverotator cuff tears, J. Bone Joint Surg. Am. 86-A (2) (2004) 219–224.
[9] D.T. Harryman II, L.A. Mack, K.Y. Wang, S.E. Jackins, M.L. Richardson, F.A.Matsen III, Repairs of the rotator cuff. Correlation of functional results withintegrity of the cuff, J. Bone Joint Surg. Am. 73 (7) (1991) 982–989.
[10] K. Yamaguchi, W.N. Levine, G. Marra, L.M. Galatz, S. Klepps, E.L. Flatow,Transitioning to arthroscopic rotator cuff repair: the pros and cons, Instr.Course Lect. 52 (1) (2003) 81–92.
[11] S.C. Winters, R.H. Gelberman, S.L.Y. Woo, S.S. Chan, R. Grewal, J.G. Seiler III, Theeffects of multiple-strand suture methods on the strength and excursion ofrepaired intrasynovial flexor tendons: a biomechanical study in dogs, J. HandSurg. Am. 23 (1) (1998) 97–104.
[12] M.L. Killian, L. Cavinatto, S.A. Shah, E.J. Sato, S.R. Ward, N. Havlioglu, et al., Theeffects of chronic unloading and gap formation on tendon-to-bone healing in arat model of massive rotator cuff tears, J. Orthop. Res. 32 (3) (2014) 439–447.
[13] D.L. Butler, S.a. Goldstein, F. Guilak, Functional tissue engineering: the role ofbiomechanics, J. Biomech. Eng. 122 (6) (2000) 570–575.
[14] D.L. Korvick, J.F. Cummings, E.S. Grood, J.P. Holden, S.M. Feder, D.L. Butler, Theuse of an implantable force transducer to measure patellar tendon forces ingoats, J. Biomech. 29 (4) (1996) 557–561.
[15] N. Juncosa, J.R. West, M.T. Galloway, G.P. Boivin, D.L. Butler, In vivo forces usedto develop design parameters for tissue engineered implants for rabbit patellartendon repair, J. Biomech. 36 (2003) 483–488.
[16] V. Volkersen, Die Nietkraftverteilung in zugbeanspruchten Nievtverbindungenmit konstanten Laschenquerschnitten, Luftfahrforschung 15 (1938) 41–47.
[17] H. Cox, The elasticity and strength of paper and other fibrous materials, Br. J.Appl. Phys. 3 (3) (1952) 72.
[18] J.A. Nairn, On the use of shear-lag methods for analysis of stress transfer inunidirectional composites, Mech. Mater. 26 (2) (1997) 63–80.
[19] J.A. Nairn, D.A. Mendels, On the use of planar shear-lag methods for stress-transfer analysis of multilayered composites, Mech. Mater. 33 (2001) 335–362.
[20] Henkel Corporation; 2014;Technical Data Sheet: Loctite 4902. URL: https://tds.us.henkel.com/NA/UT/HNAUTTDS.nsf/web/41BCEE769DD0931C85257CF5004876E3/$File/4902-EN.pdf. URL AccessedURL:03/25/2015.
[21] Henkel Corporation; 2014;Technical Data Sheet: Loctite 4903. URL: https://tds.us.henkel.com/NA/UT/HNAUTTDS.nsf/web/0192ED8CF7AABF1685257CF50048CB6A/$File/4903-EN.pdf. URL Accessed URL:03/25/2015
[22] Henkel Corporation; 2005;Technical Data Sheet: Loctite Quicktite InstantAdhesive Gel. URL: https://tds.us.henkel.com/NA/UT/HNAUTTDS.nsf/web/A7685691D5C6B064882571870000DC0D/File/Quicktite Gel-EN.pdf. URLAccessed URL:03/25/2015.
[23] H. Lee, S.M. Dellatore, W.M. Miller, P.B. Messersmith, Mussel-inspired surfacechemistry for multifunctional coatings, Science 318 (5849) (2007) 426–430.
[24] H. Lee, B.P. Lee, P.B. Messersmith, A reversible wet/dry adhesive inspired bymussels and geckos, Nature 448 (7151) (2007) 338–341.
[25] Henkel Corporation; 2014;Loctite Highly Flexible Instant Adhesives.URL:<http://www.henkelna.com/us/structureimages/11839LT6864CHART507316338984web563W.jpg>. URL Accessed URL:10/06/2014.
[26] 3M Industrial Adhesives and Tapes Division; 2012;3M Scotch-Weld NeopreneHigh Performance Rubber & Gasket Adhesives – 1300 and 1300L TechnicalData. URL: http://multimedia.3m.com/mws/mediawebserver?mwsId=
66666Ugx GCuNyXTtnxfVNXz6EVtQEcuZgVs6EVs6E666666–&fn=1300 and1300L DataPageR2.pdf. URL Accessed URL:10/14/2014.
[27] R.O. Babitt, Vanderbilt Rubber Handbook, thirteen ed.; R T Vanderbilt, 1990.[28] C.A. Harper, Handbook of Plastics, Elastomers, and Composites, 3 ed., McGraw
Hill, 1996.[29] A.N. Azadani, P.B. Matthews, L. Ge, Y. Shen, C.S. Jhun, T.S. Guy, et al.,
Mechanical properties of surgical glues used in aortic root replacement, Ann.Thorac. Surg. 87 (4) (2009) 1154–1160.
[30] A.D. Potenza, Detailed evaluation of healing processes in canine flexor digitaltendons, Mil Med. 127 (1962) 34–47.
[31] A.D. Potenza, Tendon healing within the flexor digital sheath in the dog, J. BoneJoint Surg. 44-A (1) (1962) 49–64.
[32] R.H. Gelberman, J. Menon, M. Gonsalves, W.H. Akeson, The effects ofmobilization on the vascularization of healing flexor tendons in dogs, Clin.Orthop. Relat. Res. 153 (1980) 283–289.
[33] R.H. Gelberman, S.L. Woo, K. Lothringer, W.H. Akeson, D. Amiel, Effects of earlyintermittent passive mobilization on healing canine flexor tendons, J. Hand.Surg. Am. 7 (2) (1982) 170–175.
[34] R.H. Gelberman, P.R. Manske, J.S. Vande Berg, P.a. Lesker, W.H. Akeson, Flexortendon repair in vitro: a comparative histologic study of the rabbit, chicken,dog, and monkey, J. Orthop. Res. 2 (9) (1984) 39–48.
[35] S.L.Y. Woo, R.H. Gelberman, N.G. Cobb, D. Amiel, K. Lothringer, W.H. Akeson,The importance of controlled passive mobilization on flexor tendon healing,Acta Orthop. Scand. 52 (6) (1981) 615–622.
[36] R.H. Gelberman, S. Thomopoulos, S.E. Sakiyama-elbert, R. Das, M.J. Silva, Theearly effects of sustained platelet-derived functional and structural propertiesof repaired intrasynovial flexor tendons: an in vivo biomechanic study at 3weeks in canines, J. Hand. Surg. Am. 32A (3) (2007) 373–379.
[37] H.E. Kleinert, C. Verdan, Report of the committee on tendon injuries, J. Hand.Surg. Am. 8 (5) (1983) 794–798.
[38] D.A. Osei, J.G. Stepan, R.P. Calfee, S. Thomopoulos, M.I. Boyer, R. Potter, et al.,The effect of suture caliber and number of core suture strands on zone ii flexortendon repair: a study in human cadavers, J. Hand. Surg. Am. 39 (2) (2014)262–268.
[39] G.N. Nelson, R. Potter, E. Ntouvali, M.J. Silva, M.I. Boyer, R.H. Gelberman, et al.,Intrasynovial flexor tendon repair: a biomechanical study of variations insuture application in human cadavera, J. Orthop. Res. 30 (10) (2012) 1652–1659.
[40] E. Diao, S. Hariharan, O. Soejima, J.C. Lotz, S. Francisco, Effect of peripheralsuture depth on strength of tendon repairs, J. Hand. Surg. Am. 21 (2) (1996)234–239.
[41] S. Thomopoulos, H.M. Kim, M.J. Silva, E. Ntouvali, C.N. Manning, R. Potter, et al.,Effect of bone morphogenetic protein 2 on tendon-to-bone healing in a canineflexor tendon model, J. Orthop. Res. 30 (11) (2012) 1702–1709.
[42] M.J. Silva, S. Thomopoulos, N. Kusano, M.A. Zaegel, F.L. Harwood, H. Matsuzaki,et al., Early healing of flexor tendon insertion site injuries: tunnel repair ismechanically and histologically inferior to surface repair in a canine model, J.Orthop. Res. 24 (5) (2006) 990–1000.
[43] S. Thomopoulos, E. Zampiakis, R. Das, H.M. Kim, M.J. Silva, N. Havlioglu, et al.,Use of a magnesium-based bone adhesive for flexor tendon-to-bone healing, J.Hand. Surg. Am. 34 (6) (2009) 1066–1073.
[44] M.J. Silva, M.I. Boyer, K. Ditsios, M.E. Burns, F.L. Harwood, D. Amiel, et al., Theinsertion site of the canine flexor digitorum profundus tendon heals slowlyfollowing injury and structure repair, J. Orthop. Res. 20 (2002)447–453.
[45] R.L. Lieber, D. Amiel, K.R. Kaufman, J. Whitney, R.H. Gelberman, Relationshipbetween joint motion and flexor tendon force in the canine forelimb, J. Hand.Surg. Am. 21 (6) (1996) 957–962.
[46] R.L. Lieber, M.J. Silva, D. Amiel, R.H. Gelberman, Wrist and digital joint motionproduce unique flexor tendon force and excursion in the canine forelimb, J.Biomech. 32 (2) (1999) 175–181.
[47] C.N. Maganaris, J.P. Paul, In vivo human tendon mechanical properties, J.Physiol. 1999 (521 Pt 1) (1999) 307–313.
[48] S.S. Raghavan, C.Y.L. Woon, A. Kraus, K. Megerle, M.S.S. Choi, B.C. Pridgen, et al.,Human flexor tendon tissue engineering: decellularisation of human flexortendons reduces immunogenicity in vivo, Tissue Eng. Part A 18 (2012) 796–805.
[49] J. Kondratko-Mittnacht, S. Duenwald-Kuehl, R. Lakes, R. Vanderby, Shear loadtransfer in high and low stress tendons, J. Mech. Behav. Biomed. Mater. 45(2015) 109–120.
[50] D. Casey, O. Lewis, Absorbable and nonabsorbable sutures, in: Handbook ofBiomaterials Evaluation: Scientific, Technical and Clinical Testing of ImplantMaterials, chap. 7., Macmillan Publishers Limited, New York, NY, 1986, pp. 86–94.
[51] C.C. Chu, J.A. Von Fraunhofer, H.P. Greisler, Wound Closure Biomaterials andDevices, CRC Press, 1996.
[52] S. Jackson Inc., Supramid Product Information Sheet. 2015. URL:<http://www.supramid.com/content/SUPRAMIDEXTRAIIProductInformation.pdf>
[53] D.A. Dillard, Fundamentals of Stress Transfer in Bonded Systems. AdhesionScience and Engineering, in: A.V. Pocius (Ed.), first ed., Elsevier, Amsterdam,The Netherlands, 2002.
[54] M.F. Ashby, Overview No. 80: on the engineering properties of materials, ActaMetall. 37 (5) (1989) 1273–1293.
[55] M.F. Ashby, L.J. Gibson, U. Wegst, R. Olive, The mechanical properties of naturalmaterials. I. Material property charts, Proc. R. Soc. A 450 (1938) (1995) 123–140.

S.W. Linderman et al. / Acta Biomaterialia 23 (2015) 229–239 239
[56] U.G.K. Wegst, M.F. Ashby, The mechanical efficiency of natural materials,Philos. Mag. 84 (21) (2004) 2167–2186.
[57] D.J. Pring, A.A. Amis, R.R. Coombs, The mechanical properties of human flexortendons in relation to artificial tendons, J. Hand Surg. Eur. 10 (1985) 331–336.
[58] P.J. Bouten, M. Zonjee, J. Bender, S.T. Yauw, H. van Goor, J.C. van Hest, et al., Thechemistry of tissue adhesive materials, Prog. Polym. Sci. 39 (2014) 1375–1405.
[59] I.A. Trail, E.S. Powell, J. Noble, S. Crank, The role of an adhesive (Histoacryl) intendon repair, J. Hand Surg-Br. Eur. 17 (5) (1992) 544–549.
[60] A.C. Nassif, An adhesive for repair of tissues: experiments with canine tendon,bone, lung, blood vessels and skin, using a methyl 2-cyanoacrylate adhesive, J.Surg. Res. 5 (3) (1965) 108–115.
[61] T. Inoue, T. Taguchi, S. Imade, N. Kumahashi, Y. Uchio, Effectiveness andbiocompatibility of a novel biological adhesive application for repair of meniscaltear on the avascular zone, Sci. Tech. Adv. Mater. 13 (6) (2012) 064219.
[62] S. Thomopoulos, G.R. Williams, J.A. Gimbel, M. Favata, L.J. Soslowsky, Variationof biomechanical, structural, and compositional properties along the tendon tobone insertion site, J. Orthop. Res. 21 (3) (2003) 413–419.
[63] G.M. Genin, A. Kent, V. Birman, B. Wopenka, J.D. Pasteris, P.J. Marquez, et al.,Functional grading of mineral and collagen in the attachment of tendon tobone, Biophys. J. 97 (4) (2009) 976–985.
[64] Y. Liu, S. Thomopoulos, C. Chen, V. Birman, M.J. Buehler, G.M. Genin, Modellingthe mechanics of partially mineralized collagen fibrils, fibres and tissue, J. R.Soc. Interface 11 (92) (2014) 20130835.
[65] Y. Liu, S. Thomopoulos, V. Birman, Bi-material attachment through a compliantinterfacial system at the tendon-to-bone insertion site, Mech. Mater. 44 (2012)83–92.
[66] H. Ming-Yuan, J.W. Hutchinson, Crack deflection at an interfacebetween dissimilar elastic materials, Int. J. Solids Struct. 25 (9) (1989) 1053–1067.
[67] G.M. Genin, J.W. Hutchinson, Composite laminates in plane stress: constitutivemodeling and stress redistribution due to matrix cracking, J. Am. Ceram. Soc.80 (5) (1997) 1245–1255.
[68] J.C. McNulty, F.W. Zok, G.M. Genin, A.G. Evans, Notch-sensitivity of fiber-reinforced ceramic-matrix composites: effects of inelastic strainingand volume-dependent strength, J. Am. Ceram. Soc. 82 (5) (1999)1217–1228.
[69] A. Kelly, W.R. Tyson, Tensile properties of fibre-reinforced metals:copper/tungsten and copper/molybdenum, J. Mech. Phys. Solids 13 (6)(1965) 329–350.
[70] R.F. Gibson, Principles of Composite Material Mechanics, 3 ed., CRC Press,2011.
[71] S. Lekhnitskii, Theory of Elasticity of an Anisotropic Elastic Body, Holden-Day,San Francisco, CA, 1963.
[72] V. Birman, Mechanics and energy absorption of a functionally graded cylindersubjected to axial loading, Int. J. Eng. Sci. 78 (2014) 18–26.






![Electromechanical Impedance Response of a Cracked ......considered the shear lag effect of the bond layer [23]. Suresh Bhalla et al. [24] incorporated the shear lag effect into the](https://static.fdocuments.us/doc/165x107/60b9eac572ee7d3d394ef187/electromechanical-impedance-response-of-a-cracked-considered-the-shear-lag.jpg)










