
Shared Assessment? - Social Care...
108
Shared Assessment? An exploration of whether and in what ways the professional background of the assessor will influence the outcome of an assessment Submitted in part requirement for the MSc in Community Care The Robert Gordons University, School of Applied Social Studies. Charles McKerron, MSc. in Community Care, August 2001 15,624 Words 1
-
Upload
vuongtuong -
Category
Documents
-
view
217 -
download
2
Transcript of Shared Assessment? - Social Care...
Shared Assessment?
An exploration of whether and in what ways the professional background of the assessor will influence the outcome of an assessment
Submitted in part requirement for the MSc in Community Care
The Robert Gordons University, School of Applied Social Studies.
Charles McKerron, MSc. in Community Care, August 2001
15,624 Words
1

ACKNOWLEDGEMENTS I wish to thank all the people who assisted me with this study and who supported
this work in any way. In particular the people who took part in the questionnaire and those who helped with the pilot
I wish to thank Out of the Darkness Theatre Company, especially the company member who played the ‘client’ and all the members of the production crew for
their professionalism, their patience and their help in making the video of the assessment interview.
I wish to express my thanks the staff at Robert Gordons University, School of
Applied Social Studies and in particular, my Tutor, Rob MacKay for his knowledge and subtle guidance.
I wish to thank The Moray Council and the Moray LHCC.
Lastly I wish to thank my family for their patience and support.
2
STATEMENT OF AUTHENTICITY This dissertation is an original and authentic piece of work carried out by myself. I
have fully acknowledged and referenced all secondary sources of information. This
dissertation has not been presented in whole or in part for assessment elsewhere.
I have read the Examination regulations and am fully aware of the potential
consequences of any breach of them.
Signed_______________________________________________________________ Date_________________________________________________________________
3
CONFIDENTIALITY STATEMENT Permission was sought from and granted by the person who played the role of ‘client’
in the video. Formal permission was granted before the video recording was made.
All parties who participated in the making of the video, including and especially the
person who played the role of ‘client’ were made aware of how the video was to be
used and who might be permitted to see it.
In order to attempt to ensure full understanding, information was passed concerning
the purpose of this study and the use of the video within it. This ‘information giving’
was followed by discussion and debate within and between the members of Out of the
Darkness Theatre Company who participated in the project. This discussion and
debate led to informed choice to participate in the making of the video and permission
to use it for the purposes of this study.
Signed_______________________________________________________________
Date_________________________________________________________________
4
ABSTRACT
This is a two part study that questions whether and in what ways the professional
background of the assessor will influence the outcome of an assessment. The
objectives are; to highlight the differences found; to examine these differences from
the perspective of different professional backgrounds; and to explore how these
differences might influence the outcome of a community care assessment of need.
Part one, a review of literature indicates that there are different outcomes to
assessment that are related to the differing professional background of the assessors.
In part two, a small, qualitative study was conducted in an attempt to consider how
these differences manifest in practice.
The findings suggest that; a) Health based respondents assess the client as more
dependent than do the social work based respondents. b) Conversely, there is a
tendency for social work respondents to assess the client as more independent than do
the health based respondents. c) This tendency extends to social work based
respondents assessing the client as more able than he is, notably with regard to
personal care needs. d) Health based respondents identify more risks and a need for
more additional assessments than the social work based respondents. e) There is a
tendency from the health based respondents to form more assumptions about the
clients needs than do the social work based respondents.
There are indications of a degree of judgement made about the client especially in
terms of his emotional state and the best care setting for him. This is most noticeable
from health based respondents.
The study also raises questions about interpretation of assessment questions or
prompts by assessors from different professional backgrounds.
5
LIST OF CONTENTS
PAGE NUMBER
ACKNOWLEDGEMENTS 2
STATEMENT OF AUTHENTICITY 3
CONFIDENTIALITY STATEMENT 4
ABSTRACT 5
LIST OF CONTENTS 6
LIST OF APPENDICES TABLES & CHARTS 7
CHAPTER 1 INTRODUCTION 8
CHAPTER 2 REVIEW OF LITERATURE AND RESEARCH 11
CHAPTER 3 RESEARCH METHODOLOGY 23
CHAPTER 4 RESULTS 29
CHAPTER 5 ANALYSIS AND DISCUSSION 47
CHAPTER 6 CONCLUSIONS AND RECOMMENDATIONS 68
REFERENCES 88
BIBLIOGRAPHY 97
6
LIST OF APPENDICES TABLES & CHARTS
PAGE NUMBER
TABLE 1 31
TABLE 2 36
TABLE 3 38
TABLE 4 41
APPENDIX i Questionnaire 70
APPENDIX iia Questionnaire 71
APPENDIX iib Questionnaire 72
APPENDIX iic Questionnaire 73
APPENDIX iii Focus group questions 74
APPENDIX iv Respondent background information 76
APPENDIX v Raw data from part i of questionnaire 77
APPENDIX vi Raw data from part iia of questionnaire 80
APPENDIX vii Raw data from part iib of questionnaire 81
APPENDIX viii Raw data from part iic of questionnaire 82
APPENDIX ix Focus group comments 83
7
CHAPTER 1. INTRODUCTION 1.1. Assessment of need is seen as one of the key tasks in ensuring the development
of services which are needs-led and which are effective in meeting the needs of the
service user. ‘The aim of assessment should be to arrive at a decision on whether
services should be provided, and in what form. Assessment will therefore have to be
made against a background of stated objectives and priorities determined by the local
authority. Decisions on service provision will have to take account of what is
available and affordable. Priority must be given to those whose needs are greatest.
As part of its planning machinery, every local authority should monitor the outcomes
of its assessment process, and the implications of these outcomes for future
development of services.’ (Department of Health 1989, para 3.2.12)
Assessment of need was designed to be a joint activity, a partnership between assessor
and assessed. The policy guidelines however, firmly place the responsibility on to the
assessor. This responsibility has been shown to lead to a level of control over the
outcomes by the assessor. (Social Services Inspectorate 1991a, para 3.35) The
influence and ‘pressure’ stemming from limited resources tends to reinforce this
element of control. The effect of this is that assessors may have an ‘agenda’ greater
than that of fulfilling a needs-led assessment and which may well influence the
assessment.
A further complication arises from the extent to which assessors are able, because of
previous training, experience, conceptual models and so on, to effectively carry out
needs-led assessments. The focus of an assessment might therefore be influenced by
the application of professional models, ‘which attempt to slot problems into pre-
8
defined categories and fail to take account of the wider picture.’ (Nolan, Grant,
Caldock, Keady 1994, p14) Some work has been carried out with regard to this which
implied that different professional groups, given information via a three minute video
sequence, could identify need, but also missed obvious need and furthermore made a
number of value judgements about the client. (Runciman 1989)
Ellis describes a similar situation in which professionals were asked to determine who
was the most ‘deserving’ case, based on personality characteristics. The finding being
that the professionals used value judgements, ‘rooted in professional models and
dominated by a focus of physical needs.’ (Ellis, 1993 p 15, 16)
Recent governmental directives that health and social services must engage in joint
working and will use a single shared assessment document must inevitably bring to
the fore questions relating to assessment of need and the professional background of
the assessor. (Dept. of Health 2001, Scottish Executive 2000, Scottish Executive
2001).
The aim of this study is an exploration of whether and in what ways the professional
background of the assessor will influence the outcome of an assessment The
objectives are to highlight the differences found; to examine these differences from
the perspective of different professional backgrounds; and to explore how these
differences might influence the outcome of a community care assessment of need.
Two approaches have been utilised; the first part consists of a systematic review of
the literature using a selection of electronic data bases. This attempts to contextualise
9
the study through consideration of several questions: What is ‘need’? The meaning
of ‘assessment of need’? The historical, political and organisational influences upon
those professionals undertaking assessment of need? The second part consists of a
small scale qualitative study that attempts to build on existing knowledge. A
discussion of the findings placed in context against the literature search completes the
study.
10
CHAPTER 2. REVIEW OF LITERATURE AND RESEARCH
2.1. The word ‘need’ has a range of different meanings and uses depending upon who is
using it and for what purpose. The concept of ‘need’ is, ‘…personal, subjective, variable
and constantly changing…’. Kowley, Bergen, Young, Kavanagh, (2000 p127) Several
definitions of need have been proposed. Maslow (1954) set out a hierarchy of universal
needs as a model for understanding human actions. Bradshaw (1972) examined need from
a sociological perspective, and suggested four definitions of need; normative, felt,
expressed and comparative need. Changes in the concept of health service planning since
the 1960s have been described by Stevens & Gabbay (1991), who defined need as ‘the
ability to benefit in some way from health care’.
The Department of Health describes need as, ‘a dynamic concept, the definition of which
will vary over time in accordance with: changes in national legislation; changes in local
policy, the availability of resources; the patterns of local demand.’ (Department of Health
1991, p12)
When the word ‘assessment’ is linked to the word ‘need’, the phrase ‘needs assessment’ or
‘assessment of need’ is formed. At this point, the concept of some sort of process emerges.
This process then suggests or implies the use of a tool or instrument of assessment.
Lightfoot (1995)
‘Assessment of Need’ is used in several distinct ways. ‘…the terms ‘need’ and ‘needs
assessment’ encompass a wide range of meanings, and hold different connotations
according to the context in which they are found.’ (Kowley, Bergen, Young, Kavanagh,
2000 p128) The term is certainly used in the realms of education, housing, economics,
social science and psychology as well as health and social work. Indeed when using the
phrase ‘assessment of need’, (McWalter et al. 1994) suggest that you add the question, ‘for
11
what?’ In connection with both health and social work one can find a variety of meanings.
For the purposes of this study, a brief exploration of the main uses in both health and social
work will be of value.
From the perspective of the Health practitioner, Health Needs Assessment is about
assessing the health needs of a population. ‘The systematic assessment of need prior to any
form of health care intervention…lies at the heart of all research based professional
education and practice and since 1989, population health needs assessment has been
strongly endorsed by Government initiatives…’ (Robinson, Elkan, 1996 p1). Health
Needs Assessment can be described variously as, ‘a process of measuring ill health in a
population’ (Robinson, Elkan, 1996 p16) and measuring, ‘the capacity to benefit from
health care’. (Robinson, Elkan, 1996 p16) The data derived from the assessment is used
to define the objectives of a service, to identify the most efficient means of achieving those
objectives and to obtain information on which to base policy.
Another use of the term ‘Assessment of Need’ can be more accurately described as the
assessment or measurement of functional status using specific instruments such as the
‘Index of Independence in Activities of Daily Living Scale’ (IIADL). ‘Measuring
functional status using specific instruments is an important part of geriatric assessment.'
(Rubenstein, Schairer, Wieland, Kane, 1984 p686) These instruments make use of
measurable scoring systems and tend to be used by nursing and medical practitioners as
well as ‘Professions Allied to Medicine’ (PAM’s) such as occupational therapists, and
physiotherapists. They have a three-fold use. Firstly as an assessment of basic activities of
daily living where ability to manage is perceived as a major determinant of whether a
person can live independently. Secondly, knowledge of functional status is useful in
12
defining rehabilitation goals and programmes. Thirdly, these instruments can be used in
sequence to give a quantifiable record of functional status over time. As such they are seen
as indicators of improvement or deterioration in function (Rubenstein, Schairer, Wieland,
Kane, 1984 p686).
The third use of the term assessment of need is in connection with community care
assessment of need as defined by the 1990 NHS and Community Care Act. In this case,
need is seen as, ‘the requirements of individuals to enable them to achieve, maintain or
restore an acceptable level of social independence or quality of life, as defined by the
particular care agency or authority’ (Department of Health 1991, p12) and assessment is
to, ‘define, as precisely as possible, the cause of any difficulty’ (Department of Health
1991, p52). Many of these assessments are based on information gathered using structured
questionnaires, often in the form of checklists or prompts. Very often there is no attempt
to codify or ascribe value to the information through the assessment process. In some
cases, techniques to measure functional status, such as described above, are incorporated
into the process.
It might be argued that there is a fourth assessment of need type in the form of a
nursing needs assessment. Nurses have for many years carried out individual
assessment of patient need and have taken into consideration medical needs, health
care needs, mobility, dressing, independent living skills diet and social needs. Nurses
have included in this assessment basic medical tests such as blood pressure, certain
blood tests and so on. District nurses are required to:-
1. assess the health and health-related needs of patients, clients, their families and
other carers and identify and initiate appropriate steps for effective care for
13
individuals and groups;
2. assess, diagnose and treat specific diseases in accordance with agreed medical
protocols; and
3. assess, plan. Provide and evaluate specialist clinical nursing care to meet care needs of
individual patients in their own homes (UKCC 1994)
These assessments use a combination of techniques as described above and include
some medical assessments. The nursing assessment tends to happen over time and is
an ongoing process whereas the community care assessment is described as a one-off
event followed by care planning and review.
2.2. The Community Care form of assessment is linked to service commissioning through
the process of care management. The process is designed to be ‘needs led’ in that it
emphasises adapting services to needs rather than fitting people into existing services. The
NHS and Community Care Act firmly linked assessment of need to resources in three main
ways; firstly, as noted previously, ‘social independence or quality of life is ‘as defined by
the particular care agency or authority’ (Department of Health 1991, p12). Secondly, the
Act recognised that care management and assessment are to be seen as one integrated
process for identifying and addressing the needs of individuals ‘within available resources’
(Department of Health 1991, p9). Thirdly, the person doing the assessment was inevitably
also the person responsible for arranging the care package. Leat and Perkins argue that this
linking of assessment of need to resource, coupled with insufficient funding, led to
practitioners and managers adopting resource-led measures (Leat, Perkins 1998, p175).
The 1990 NHS and Community Care Act introduced other important changes. Notably
that the concept of health needs and of social needs are separated out and are the
14
responsibility of different agencies (Department of Health 1989a,b). The act also laid the
foundations for joint working in that it incorporated a statutory requirement for agencies to
co-ordinate the arrangements for the assessment of Community Care needs (Department
of Health 1990), (Social Services Inspectorate 1991).
The concept of joint working that was embedded in the 1990 legislation has been
developed by the subsequent Labour Government into a concept of partnership. The 1990
Conservative Government set in place the idea of a purchaser/provider split under the
ideology that competition would act as a spur to efficiency and customer orientation
(Mearns and Smith 1994). This concept was in direct tension with the concept of joint
working and collaboration (Hudson 1997) and served to set up a conflict between provider
agencies.
The ensuing Labour Government concluded that a partnership approach based on co-
operation not competition was the way ahead (Secretary of State for Scotland 1997 p2).
This partnership approach was in part fueled by the idea that collaboration is less costly
than competition. (Department of the Environment, Transport and the Regions 1999) The
concept of ‘partnership’ is to be enforced by new legal duties upon Local Authorities
(Secretary of State for Health 1998). The intention is that authorities should ‘…start
thinking more corporately about what will benefit their citizens…This will require close
partnership working…’ (Secretary of State for Health 1998 6.5). The concept of
partnership is also being promoted within the Health services (NHS Plan 7).
This concept of partnership, in particular between health and social services has manifested
today as an insistence upon, joint working. In England, the National Service Framework
15
for Older People outlined a single assessment process within which agencies should agree
joint working arrangements for assessment and care planning. Under the NHS bodies and
Local Authorities Partnership Arrangement Regulations 2000, provision has been made for
either NHS or Council professionals to legitimately carry out a full overview assessment
and in some instances, commit the resources and services of another agency to an
individuals care. By April 2002, agencies should comply and by April 2005 agencies must
comply or the Department of Health will ensure compliance (Department of Health 2001).
In Scotland, The White Paper, ‘Community Care: A Joint Future’ was produced at the end
of 2000. This calls for, amongst other reforms, a single, shared assessment for all client
groups by April 2002 (Scottish Executive 2000). This was followed in February 2001 by
the Report of the Chief Nursing Officer for Scotland’s group on Free Nursing Care who
recommended that a single shared assessment is carried out, preferably by one person, but
involving others if necessary (Scottish Executive 2001). These recommendations were
adopted by the Scottish Executive in January 2001.
Assessment is then an essential tool in the implementation of the community care policy
and proper assessment of need and good case management is ‘the cornerstone of high
quality care’ (Dept. of Health, 1989a 1.11). Considerable research has been undertaken
with a view to refining the assessment tools (Challis and Chesterman 1985), and to
consider the assessment procedures (Department of Health 1993). Investigation has been
carried out into the role of assessment in the avoidance of inappropriate placement (Stuck
et al., 1993), (Peet et al., 1994). Significant research has gone on to consider the link
between assessment and care planning (Caldock, 1994), (Lewis et al, 1995), (Parry-Jones
and Caldock, 1995). More recently, research has focussed on the development of multi-
16
disciplinary assessment involving health and social work agencies (Department of Health
1997). There appears however to be relatively little research that has looked at the
influence of professional background on the outcome of assessment of needs.
2.3. In 1984, Rubenstein et al considered the measurement of functional status in geriatric
assessment. They saw that the assessment instruments often relied on data sources that
differed from those with which they were originally validated. The experiment consisted
of assessing functional status of a group of elderly people using three different data
sources; a), direct patient interview; b), interview with a hospital nurse or nursing assistant
who was familiar with the patient (nurse proxy); c), interview with an individual from the
community who was familiar with the patient, usually the person closest to the patient and
who had visited in the previous two days (community proxy). The three assessments for
each patient were completed within a single day. The assessments used were the Lawton
Personal Self-Maintenance Scale, and Instrumental Activities of Daily Living. The
findings were that in a significant percentage of cases, patients rated themselves higher
than either the community proxy or the nurse proxy did. Also the discrepancy was greater
when the community proxy was a spouse rather than any other relative.
Rubenstein et al consider that there may be several reasons to explain these discrepancies.
These reasons include patient and community proxy perceptions and agendas as well as
influences on nursing staff.
The researchers conclude that care givers and case managers can make big decisions based
on functional capacity scores that are based on information gained from various observers
and reporters. The patient is often in an acute hospital at time of assessment and acute
illness often provokes functional deterioration that is reversible but may be interpreted as
permanent. Under these circumstances, the possibility of nursing staff and family
17
members viewing patients as more dysfunctional than the patients see themselves, ‘might
lead to tragic errors in discharge planning’ (Rubenstein L Z, Schairer C, Wieland G D,
Kane R 1984 p 686 – 691).
In 1985, Buckley and Runciman considered health assessment of the elderly at home.
They used video studies and questionnaires to examine the scope and content of health
assessment by different health professionals. They worked with seven professional groups,
including; health visitor students; experienced health visitors; district nurse students;
experienced district nurses; GP trainees; experienced GP’s; physiotherapy students;
occupational therapy students; social work students; home care organisers; elderly people.
In the study they showed a short video of an elderly lady with mobility problems. They
asked participants to note, 1) what they had observed of significance; 2) what problems
they perceived and 3) what areas of assessment would they wish to have covered.
Findings were interesting and included; ‘that individual professionals perceived the lady
and her circumstances in quite different and sometimes opposing ways’ (Buckley,
Runciman 1985) ‘there were interesting differences in detail which reflected different
professional perspectives’ (Buckley, Runciman 1985). They also noted major gaps in key
areas of assessment. Recommendations from the study included a need for training about
health assessment and a call for shared learning between professions.
Another 80’s study considered people who had already been placed in residential care.
530 assessments were considered over four different geographical areas using a variety of
different assessment tools. In order to achieve consistency of comparison, the Modified
Crighton Royal (MCR) Scale was also utilised to measure dependency. The assessments
were revisited by local social workers who categorised them into four groups to indicate
18
whether the person required care at time of placement and/or at time of re-assessment.
When the MCR Scale figures were considered, the figures showed that 40% of residents
who had been assessed by social workers as requiring residential care, had scorings that
placed them in the ‘mildly dependent’ section of the rating scale. This implied that they
were inappropriately placed.
The researchers concluded that social worker judgement had been affected by a variety of
social factors and that social worker judgement took into account the resources that were
locally available, and that ‘different people in different places make different judgements
about the same person’ (Gibbs, Bradshaw 1988).
As a part of the Duns pilot project, ‘Assessment of Social Care Needs’, comparisons were
made between assessors from different professions including; occupational therapists;
social workers; home care organisers; nurses; community psychiatric nurses. Of twelve
different needs recorded, different disciplines prioritised different needs and indeed there
was a significant spread of needs identified by workers from the same profession. As a
further part of the study, workers were invited to watch a 31 minute video of an interview
between an elderly lady and her GP. At the end of the process they were asked to
complete an assessment form and questionnaire. Once again there was a wide range of
needs identified, 15 in all, with considerable differences between disciplines. The
researchers concluded that, ‘…differences found…are as likely to be because of their
differing backgrounds…’ (Taylor 1993 p52). Recommendations included training for
assessors, including joint training with other professionals as well as written procedures
and guidelines for assessment completion (Taylor 1993).
19
Of interest to this study are the findings of Petch et al 1994 who were funded by the
Scottish Office from 1991 onwards to look at the efficiency and effectiveness of the
delivery of community care in Scotland. Their 1994 work attempts to provide an overview
of four assessment and care management pilot projects in Scotland. The report draws on
the previous work by Taylor 1993, and comments that, ‘A further dimension of
significance is the influence of the background of the assessor on the needs that are
identified. From evidence in both Tayside and Borders it would appear that different
needs were being identified by different assessors’ (Petch, Stalker, Taylor, Taylor, 1994).
By 1996, it appears clear that professional perspectives are considered to have a bearing on
the outcome of assessment. Nolan and Caldock comment that, ‘…recent studies have
highlighted the fact that frameworks for assessment are often heavily influenced by
particular professional perspectives…’ (Nolan, Caldock, 1996 p77-85). Their paper
identifies contradictions in practice guidelines relating to assessment and attempts to create
a model to structure the assessment process.
International research has also been focused on this issue of professional background.
Slade (1996), reported on a survey of mental health professionals from cities in India,
Australia and England. The findings showed that similar priorities relating to individual
need were found at all survey sites, both from hospital and community staff. Differences
were found due to professional background. ‘This suggests that there is some cross-
cultural consistency in prioritising needs, but the choice of profession to assess need may
influence the way in which needs are assessed’ (Slade 1996 p1-9).
20
The issue of needs assessment for mentally disordered offenders was considered by Cohen
and Eastman in 1997. This work consisted of a literature review and a national survey of
agencies who were likely to be carrying out these assessments. The authors came to the
conclusion that needs assessment is value laden and that no single needs assessment
approach can address all the issues of importance. They suggest, ‘Substituting the term
‘perspective on needs’ for the term needs assessment would help reflect the lack of a single
‘truth’ about need…’ (Cohen, Eastman 1997).
A study done in 1998 is of interest in that it included subjects from different ethnic groups.
The study compared staff and patient assessment of need for people suffering from
psychotic disorders. 137 patients were assessed by both staff and patients using the
Camberwell Assessment of Need. The main difference was in the rating of unmet needs,
where staff rated 1.2 on average whereas patients rated 1.8 unmet needs. A group of the
patients were Black Caribbean. No significant differences were noted in terms of number
of needs identified when comparing Black Caribbean and White Caucasian patients
(Slade, Phelan, Thornicroft, 1998p 543-550).
The comparison of levels of perceived risk in people who have dementia formed the basis
of work done by Blanche in 1999. By using written vignettes and focus group work, a
comparison was undertaken using social workers, nurses and doctors drawn from two
multi-disciplinary teams. In a vignette presenting significant physical problems, nurses
were unanimous. In a vignette presenting potential carer abuse, the social work group
achieved near consensus. The findings were that each professional had some differences in
perceived risk compared to other members of the same profession and there were
differences between professions (Blanche 1999).
21
Work reported in 2000 by Cowley et al, attempts to create a descriptive taxonomy of needs
assessment. This work built on an earlier study that used data gained from observation of
recently qualified health visitors and district nurses (Bergen, Kowley, Young, Kavanagh
1996). The original study in part explored the tension between the concept of ‘health need’
and ‘social need’ and the strong emphasis on collaborative working found in the 1990 NHS
and Community Care Act. In particular, it looks at the changing educational needs of
workers who are required to operate within this contradiction and tension. The later study
was an attempt to describe different forms and levels of needs assessment and suggested a
taxonomy based on three elements; ideals, types and timing. The interesting finding is that
the holistic philosophy and the nursing idea of ‘wholeness’ was seen to underpin the idea
of needs assessment. ‘The extent to which such ideals were translated into practice varied,
but the holistic emphasis was ubiquitous in the data…’ (Cowley, Bergen, Young,
Kavanagh, 2000 p129). The practitioners used in the study recognised, ‘the complexity of
assessing the needs they encountered, acknowledging that their own perceptions and levels
of ability were some of the variables which helped to add to the confusing diversity’
(Cowley, Bergen, Young, Kavanagh, 2000 p133).
Summary
It appears clear from research findings that the professional background of the assessor
does influence the outcome of assessment. It appears that questions remain relating to how
and in what ways.
Given the clear political agenda to develop partnership arrangements and joint working
between social work and health and in particular a single shared assessment that can be
completed by a worker of either agency, the research question that has inspired this
dissertation becomes particularly relevant.
22
CHAPTER 3. RESEARCH METHODOLOGY
3.1. The aim of this study is; ‘to explore whether and in what ways the professional
background of the assessor will influence the outcome of an assessment’.
The objectives are to;
i. Highlight differences found.
ii. Examine these differences from the perspective of different professional
backgrounds.
iii. Explore how these differences might influence the outcome of an
assessment.
For this study, a short video, approximately 10 minutes, was prepared showing an
interview with a physically disabled man. This man also has a learning disability. In
the video, the man answers a series of questions relating to his physical needs. The
video was shown to groups of professionals who were then asked to complete a
questionnaire. The groups of respondents were then asked a series of questions in a
20 minute semi-structured focus group session. ‘A focus group is a discussion based
interview…that…involves the simultaneous use of multiple respondents to generate
data, it is… ‘focused’ (…on an external stimulus) and…staged (…by a moderator)’
(Millward 1995). The assumption of focus groups is that ‘people will become more
aware of their own perspective…and be prompted to analyse their views more
intensely than during individual interview’ (Millward 1995).
3.2. Design.
The use of video was an attempt to introduce a data source that was consistent for all
respondents and that would contain no experimenter bias. Video presentation of
23
client information has been used by previous researchers with an interest in
assessment e.g. (Buckley and Runciman 1985, Taylor 1995).
The study was designed so that the professional background of the respondent was an
independent variable. The assessment document used as questionnaire was the
dependent variable. This was a ‘within subject design’ study and as such the controls
were the subjects themselves. The sample size was thirty respondents.
The data gathering process was in three parts.
Part one was a questionnaire (appendix i.) that was designed to gather personal
information about the respondents in terms of their professional qualifications, length
of service and current job. This page also contained a confidentiality statement. The
data gathering would have been more precise if the questionnaire had asked for ‘post
qualifying’ employment history instead of just ‘employment history’.
Part two was a questionnaire (appendix ii a,b,c.) that used part of an assessment of
needs document. The assessment of needs document used was chosen because it is the
standard document used throughout the study area. All respondents had experience of
it in their working lives. The document is designed to gather data in two ways.
Firstly as pre-coded responses, secondly as open comments to these coded responses.
Three parts of the standard document were used. a) The personal profile page that is
designed to build up a picture of the client needs in terms of being either A)
independent, B) Requiring minimal assistance, C) Dependent. Space was available
for additional comments. b) A tick list of risk factors. c) A tick list of additional
(specialist) assessments that may be required with comments on reason for referral for
these additional assessments.
24
The use of the assessment document as questionnaire might have introduced a
variable into the study in as much as different workers have different working
knowledge and experience of using the assessment document. Some workers use it
daily whilst others encounter it seldom. Those workers who are less familiar with it
might interpret the sections differently or might miss out sections. This might bias the
findings.
Part three of the study was a series of six semi-structured questions used in a final
focus group session (appendix iii). The 3rd of the focus group questions was not well
formulated. It was designed to discover the theoretical and conceptual models that the
assessments were based on. The responses provided little useful information relating
to this. Other interesting comments given in response to this question have been
recorded. One of the sessions had only one respondent and cannot truly be termed a
focus group.
3.3. Pilot study
Prior to the final study, a pilot study was conducted using three respondents. The
respondents were all care officers, one of whom has an occupational therapy
background, one has a nursing background and one has a background in residential
care of the elderly. All have considerable experience in using the assessment
document. The three participated in two sessions. In one session, they ran through
the whole process from start to finish. In the second session, they acted as a focus
group to consider the overall process and in particular the wording of the focus group
questions to be used in the final study. As a result of the pilot study, the number of
elements of the assessment document used in the study was reduced from five to the
25
three described. The questions used in the focus group element of the process were
altered in an attempt create a mix of ‘stimulus structured and response free’ questions
and ‘stimulus free and response structured’ questions (Breakwell et al 1995). A
background information sheet was added giving additional information about the
client that was not available from the video (appendix iv.). This was considered to be
both useful information relating to the clients needs and contextual information about
the clients background.
3.4. Respondents.
The respondents were all drawn from the study area and were employed by either the
Local Authority, Community Services Department or the Local Health Care Co-
operative (LHCC). The respondents were self-selected. Several distinct groups were
approached and asked to participate in the study; a group of district nurses through the
local district nurses forum; a mixed group of care officers, care organisers and
occupational therapists (OT’s) through a social work, community care, area team; a
group of hospital nurses through the local community hospital; a group of professions
allied to medicine (PAM's) through the local community hospital.
This can be described as a stratified sample. However, the selection criteria were not
sufficiently clear and as a result the final mix of professions was unbalanced. Several
care officers/care organisers and community nurses participated but only two hospital
nurses, two physiotherapists and a small number of OT’s. If the respondent
population had been restricted to the group of community nurses and the group of care
officers/organisers, then a clearer comparison between these two groups would have
been possible. There was a high degree of co-operation and commitment from the
respondents.
26
3.5. Procedures.
Location was the usual meeting place of the group. A television/video was set up in
the room. The respondents were told the structure of the session and given verbal
reassurance regarding confidentiality. The respondents were asked to fill out part 1 of
the questionnaire but not to look at the rest of the document. The respondents were
asked not to write anything else until the video was over. The video was shown. The
respondents were invited to read the background information sheet then to complete
parts 2i-iii. of the questionnaire. The questionnaires were collected and a twenty
minute focus group session was held immediately afterwards. Notes on responses and
comments were recorded in writing during the focus group session and written up
immediately following. This note-taking had the effect of slowing interaction and
group process. A better method would have been to make an electronic recording of
the session for later transcription. As ending, the respondents were thanked for their
participation. The total process took approximately an hour.
3.6. Data Analysis.
This is a qualitative study however the use of the assessment document as
questionnaire provided some quantifiable data. The quantifiable data has been used to
compare the response to individual questions by professionals from different
backgrounds. The quantifiable data has been presented in percentage form to permit
easy comparison between numerically different groups. The groups represent a range
of different professions. For the presentation of quantifiable data, the respondents
have been grouped according to employer. This places them as either health or social
work employees. This decision has meant including OT’s and physiotherapists as
27
subsets of these larger groups and has not permitted a numerical analysis of them as
separate professional groups. Qualitative information about all professional groups is
available from focus group comments.
Because of the design of this study, statistical analysis has not been possible (Buaman,
1992 p192).
With regard to the information gathered via the focus groups, this has been
subjectively classified according to comment to illustrate particular themes or spreads
of meaning (Breakwell et al 1995). Representative comments have been used in the
text to illustrate particular themes. The subjective classification was carried out by
the writer of this study who is inevitably subject to a set of perceptual pre-dispositions
that are imposed by professional background and experience. There is a likelihood of
bias in this classification.
Consideration of the facilitation process of these focus groups would place it within
the quadrant of high control of both process and content (Breakwell et al 1995 p282).
Only twenty minutes were available for the focus group sessions. This was not long
enough to permit the level of interaction amongst participants needed for the most
effective focus groups. This time constraint was imposed because; a) it was
logistically impractical to arrange a follow up meeting with sufficient members of any
of the groups and b) many respondents could allow at most one hour to the task
because of their need to return to their own demanding work schedules.
28
CHAPTER 4. RESULTS
4.1. Summary of Respondent Background Details.
See appendix v.
There were thirty respondents in total, 29 female and one male. Of the 30, 17 people
are employed by or are on secondment to the LHCC. 13 people are employed by the
local Authority, Department of Community Services.
Of the LHCC staff, none noted any previous social work experience, of the
Community Service staff, one noted previous nursing experience.
The length of service ranged between. 9 months and 40 years with 28 (93%) of the
respondents having a length of service greater than 4 years. It should be noted that the
two student nurses quoted length of service as 9 month and 3 years respectively.
Neither of these had qualified. All the rest of the respondents quoted post-qualifying
length of service.
27 respondents were noted as having a professional qualification and 13 people
having more than one.
By Professional qualifications I have included RGN, RM, SCM, CQSW, CSS, HNC,
BSC.OT, Dip.OT, State Registered Physiotherapist. I have not included SVQ. (See
key to abbreviations in Appendix v.) A wide range of different service settings and
work experiences were noted.
24 respondents were community based. The others were hospital based.
29
4.2. Key findings.
The tables of findings are published in the appendices, listed as ‘Raw Data from Part
2,a,b,c.
See appendices vi – viii.
A brief pencil picture of the client as presented visually and verbally in the video will
be of use when considering the analysis of the findings of this study.
The client will be referred to as B. The video shows that B is male, probably in his
mid thirties. The view shows him sitting at a table. The picture does not extend to B’s
legs or feet. B has dark hair and wears spectacles. He is dressed in modern casual
clothes. He is clean and well dressed, his hair is neat and he appears to be well
nourished and in good health. B uses a wheelchair, the back and sides of the chair are
in evidence and the picture shows that the chair has a high, specially adapted backrest
to provide postural support and that B is strapped into the chair with a wide
restraining belt round his middle. Further consideration of the chair shows that it has
been well used, parts of the chair are ‘scuffed’ and worn, especially on the left armrest
and at the backrest where B places his head.
Physically, B holds his head at an angle and moves it constantly. He almost always
has a smile on his face. B’s left arm is held across his chest throughout the video and
his left hand is bent down at almost right angles to the arm. He does not move this
arm significantly. B’s right arm is more mobile but to a trained observer, it might
appear that B does not have full mobility in his right arm or hand.
B also has episodes of sudden movement when his whole body twitches.
B speaks slowly and his speech is quite slurred at times. In the video, he answers a
series of questions about his personal care needs. The questioner is a voice off
30
camera. B answers all questions, the questioner sometimes asks the same question
more than once or by using different wording before B answers. The questioner also
provides verbal prompts at times such as offering B two or more possible responses to
a question and inviting B to choose the most appropriate response.
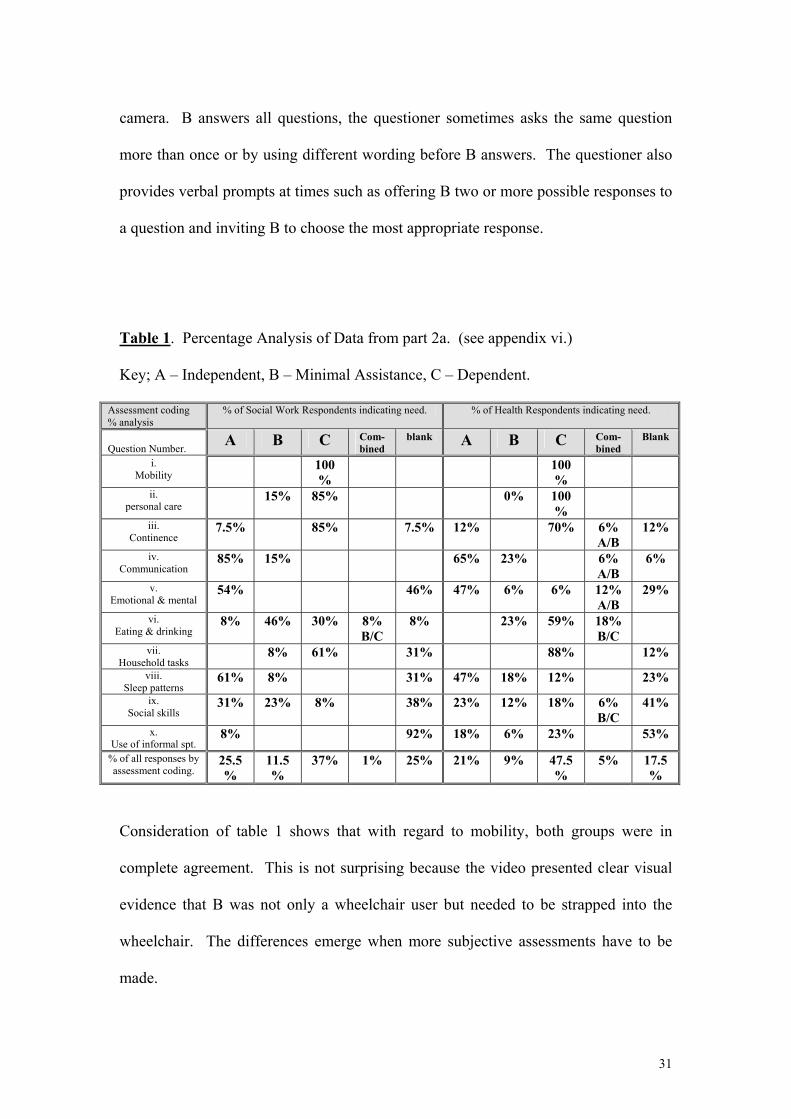
Table 1. Percentage Analysis of Data from part 2a. (see appendix vi.)
Key; A – Independent, B – Minimal Assistance, C – Dependent.
Assessment coding % analysis
% of Social Work Respondents indicating need. % of Health Respondents indicating need.
Question Number.
A B C Com-bined
blank A B C Com-bined
Blank
i. Mobility
100%
100%
ii. personal care
15% 85% 0% 100%
iii. Continence
7.5% 85% 7.5% 12% 70% 6% A/B
12%
iv. Communication
85% 15% 65% 23% 6% A/B
6%
v. Emotional & mental
54% 46% 47% 6% 6% 12% A/B
29%
vi. Eating & drinking
8% 46% 30% 8% B/C
8% 23% 59% 18% B/C
vii. Household tasks
8% 61% 31% 88% 12%
viii. Sleep patterns
61% 8% 31% 47% 18% 12% 23%
ix. Social skills
31% 23% 8% 38% 23% 12% 18% 6% B/C
41%
x. Use of informal spt.
8% 92% 18% 6% 23% 53%
% of all responses by assessment coding.
25.5%
11.5%
37% 1% 25% 21% 9% 47.5%
5% 17.5%
Consideration of table 1 shows that with regard to mobility, both groups were in
complete agreement. This is not surprising because the video presented clear visual
evidence that B was not only a wheelchair user but needed to be strapped into the
wheelchair. The differences emerge when more subjective assessments have to be
made.
31
Consideration of responses to ‘personal care’ indicate a large degree of agreement,
however, 15% of social work staff consider the client to require ‘minimal assistance’.
Visual evidence would suggest that this was not the case, the client is wheelchair
bound, requires to be strapped in, has apparently limited hand and arm movement.
Verbal evidence from B suggests that he is able to do a range of tasks independently.
This might suggest that a percentage of social work staff are inclined to believe what
the client says rather than what they see.
With regard to continence, B clearly states in the video that he can get to the toilet
himself but that he needs help when he is there. He provides contradictory verbal
evidence concerning the number of helpers he requires. There is no visual evidence
of continence needs but toileting needs might be assumed because of visual evidence
of poor mobility. 85% of social work staff against 70% of health staff score him as
dependent. It is impossible to know whether continence or toileting need is being
assessed.
The assessment of communication provides further evidence of differences between
social work based and health based staff. 85% of social work against 65% of health
based staff code him as independent. 15% of social work against 23% of health based
staff code him as requiring minimal assistance. The video provided both visual and
verbal evidence of B’s ability to communicate. Again, it is impossible to know
exactly what is being assessed. One worker might be assessing his speech ability
whilst another might be assessing his ability to get his message across.
32
The video provides no visual evidence of B’s emotional & mental state. At one point
the questioner says, “I’m right in saying that you have no mental health problems?” B
acknowledges that this is correct. At another point, there is an exploration of mood
and general emotional state. B indicates that he does not have high’s or low’s of
emotional state and says that he is “generally happy.” Social work respondents either
score him as independent or leave the question blank. In total 24% of health staff
code him as requiring some assistance. 6% assess him as dependent. The absence of
visual evidence and the positive verbal statements strongly suggest that a percentage
of health professionals are making assumptions at this point.
With regard to eating and drinking, visual evidence implies that B might have some
difficulties and therefore some need for assistance. B states that he can feed himself
but requires some food cut up. 8% of social work staff score him as independent
against no health staff. 46% of social work staff score him as requiring minimal
assistance compared with 23% of health based staff. 8% of social work staff score
him as dependent compared with 18% of health based staff. It would appear that
social work staff are tending to assess him as more able than he possibly is. Again
this could relate to his verbal evidence.
The video presents verbal information about B’s ability to prepare food. He indicates
that he can chop vegetables if they are placed on a table in front of him. There is no
specific information about any other household tasks. 8% of social work staff score B
as requiring minimal assistance with regard to household tasks against nil health
based staff. 61% of social work staff score him as dependent against 88% of health
based staff.
33
There is some verbal information in the video regarding B’s sleeping pattern. In the
context of questioning about his night time toilet needs he says that he sleeps all night.
61% of social work staff score him as independent against 47% of health staff. 23%
of social work staff consider that he requires minimal assistance against 12% of health
staff. 12% of health staff consider him to be dependent with regard to sleep pattern.
The evidence available from the video would suggest that there are no needs
associated with sleeping. It appears that assumptions are being made by some staff,
with health staff making more assumptions relating to his need.
There are no specific statements about social skills in the video. Verbal clues and
visual clues might be drawn from observation of B answering the range of questions.
31% of social staff scored him as independent against 23% of health staff. 23% of
social work staff scored him as requiring minimal assistance against 12% of health
staff. 8% of social work staff scored him as dependent against 18% of health staff.
A further 6% of health staff scored him as B/C i.e. requiring minimal
assistance/dependent. Again it appears that certain workers are making assumptions
with health staff rating him as more dependent than social work staff.
There are no statements in the video about B’s use of informal support. Visual
evidence shows that he has limited mobility that might influence his use of informal
support. 8% of social work staff scored him as independent against 18% of health
staff. A total of 29% of health staff scored him as either dependent or requiring
minimal assistance compared with no social work staff. Once again it appears that
34

workers are making assumptions about his needs. Again, it appears that health staff
perceptions tend to place him at the more dependent end of the scale.
Consideration of the average scores show that social work staff score him as
independent 25.5% of the time against 21% health staff. Social work staff score as
requiring minimal assistance 11.5% of the time against 9% of health. Social work
score him as dependent 37% of the time compared to 47.5% of health.
Individual comparison of responses to each question indicate that social work staff
tend to score B as being independent a greater number of times than health staff do.
Conversely health staff tend to score B as being dependent a greater number of times
than social work staff do. The exceptions being in the question regarding mobility
when clear, unambiguous visual evidence was available and there was complete
agreement about scoring. In the question of continence, social work staff and health
staff reversed the usual pattern and social work staff scored B as being dependent a
greater percentage of times.
35
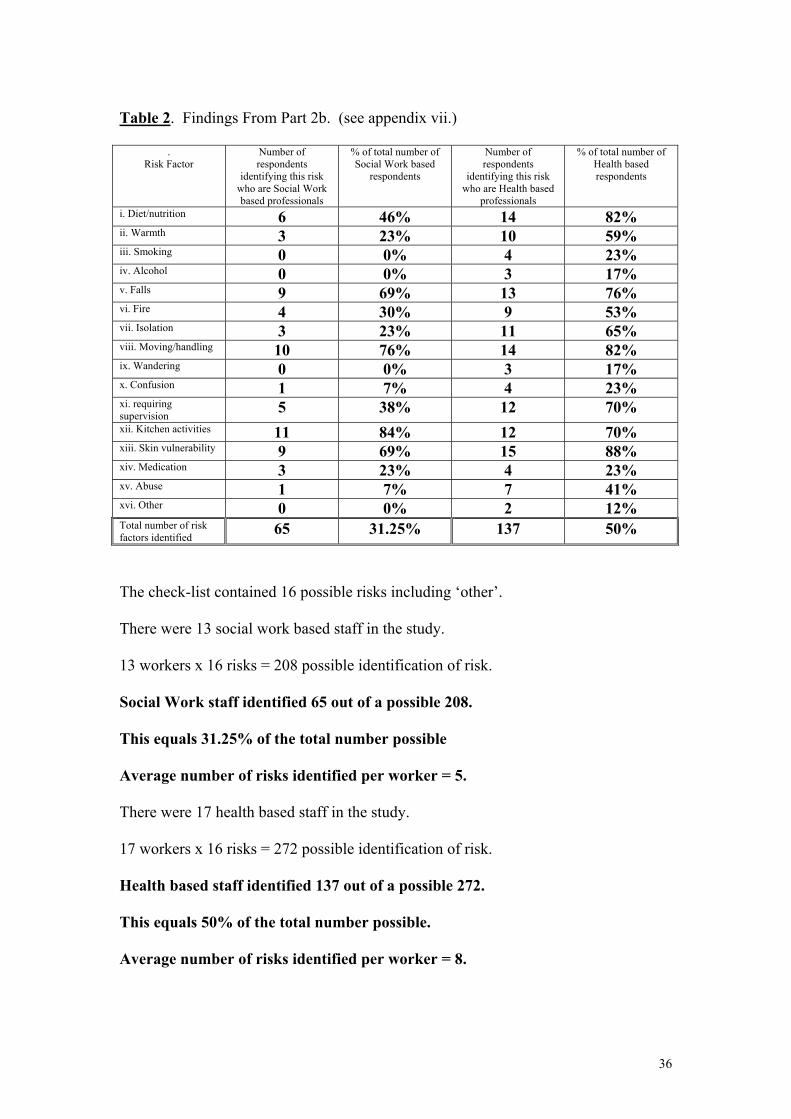
Table 2. Findings From Part 2b. (see appendix vii.)
. Risk Factor
Number of respondents
identifying this risk who are Social Work based professionals
% of total number of Social Work based
respondents
Number of respondents
identifying this risk who are Health based
professionals
% of total number of Health based respondents
i. Diet/nutrition 6 46% 14 82% ii. Warmth 3 23% 10 59% iii. Smoking 0 0% 4 23% iv. Alcohol 0 0% 3 17% v. Falls 9 69% 13 76% vi. Fire 4 30% 9 53% vii. Isolation 3 23% 11 65% viii. Moving/handling 10 76% 14 82% ix. Wandering 0 0% 3 17% x. Confusion 1 7% 4 23% xi. requiring supervision
5 38% 12 70% xii. Kitchen activities 11 84% 12 70% xiii. Skin vulnerability 9 69% 15 88% xiv. Medication 3 23% 4 23% xv. Abuse 1 7% 7 41% xvi. Other 0 0% 2 12% Total number of risk factors identified
65 31.25% 137 50%
The check-list contained 16 possible risks including ‘other’.
There were 13 social work based staff in the study.
13 workers x 16 risks = 208 possible identification of risk.
Social Work staff identified 65 out of a possible 208.
This equals 31.25% of the total number possible
Average number of risks identified per worker = 5.
There were 17 health based staff in the study.
17 workers x 16 risks = 272 possible identification of risk.
Health based staff identified 137 out of a possible 272.
This equals 50% of the total number possible.
Average number of risks identified per worker = 8.
36
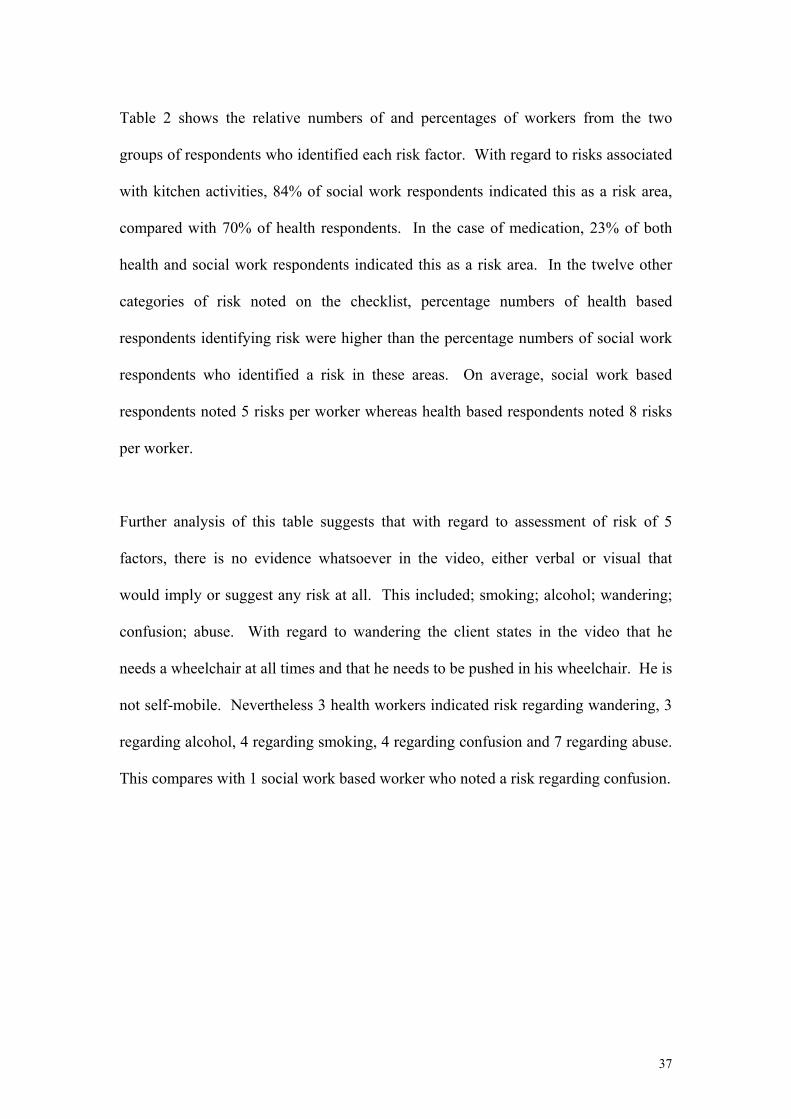
Table 2 shows the relative numbers of and percentages of workers from the two
groups of respondents who identified each risk factor. With regard to risks associated
with kitchen activities, 84% of social work respondents indicated this as a risk area,
compared with 70% of health respondents. In the case of medication, 23% of both
health and social work respondents indicated this as a risk area. In the twelve other
categories of risk noted on the checklist, percentage numbers of health based
respondents identifying risk were higher than the percentage numbers of social work
respondents who identified a risk in these areas. On average, social work based
respondents noted 5 risks per worker whereas health based respondents noted 8 risks
per worker.
Further analysis of this table suggests that with regard to assessment of risk of 5
factors, there is no evidence whatsoever in the video, either verbal or visual that
would imply or suggest any risk at all. This included; smoking; alcohol; wandering;
confusion; abuse. With regard to wandering the client states in the video that he
needs a wheelchair at all times and that he needs to be pushed in his wheelchair. He is
not self-mobile. Nevertheless 3 health workers indicated risk regarding wandering, 3
regarding alcohol, 4 regarding smoking, 4 regarding confusion and 7 regarding abuse.
This compares with 1 social work based worker who noted a risk regarding confusion.
37
Table 3. Findings From Part 2c. (see appendix viii.)
. Additional Assessment
Number of respondents requesting
this assessment who are Social Work based
professionals
% of total number of Social Work based
respondents
Number of respondents requesting
this assessment who are Health based
professionals
% of total number of Health based respondents
i. Carers assessment 4 31% 14 82% ii. Dementia team 0 0% 0 0% iii. Nursing – Community
6 46% 8 47% iv. Physiotherapist 4 31% 10 59% v. Speech/Language therapist
4 31% 7 41% vi. Chiropody 4 31% 9 53% vii. Dietician 1 8% 8 47% viii. Nursing – Hospital
0 0% 0 0% ix. Psychiatrist 0 0% 0 0% x. Other 1 8% 1 6% xi. Community Care 5 38% 8 47% xii. Learning Disability
2 15% 11 65% xiii. Occupational Therapist
9 69% 12 70% xiv. Psychologist 0 0% 0 0% Total number of additional assessments noted as required.
40 22% 88 37%
The check-list contained 14 possible additional assessments.
There were 13 social work based staff in the study.
13 workers x 14 additional assessments = 182 possible indication of need for additional assessment. 13 Social Work staff noted a need for 40 out of a possible 182 additional assessments. This equals 22% of the total number possible.
Average number of additional assessments noted per worker = 3.
There were 17 health based staff in the study.
17 workers x 14 additional assessments = 238 possible indication of need for additional assessment. 17 Health based staff noted a need for 88 out of a possible 238 additional assessments. This equals 37% of the total number possible.
Average number of additional assessments noted per worker = 5.
38
Table 3 shows the relative numbers of and percentages of workers from the two
groups of respondents who indicated a need for additional assessments. In the case of
seven of the additional assessment options, the percentage of the two groups was the
same or within 2%. These being dementia team; community nursing; hospital
nursing; psychiatry; other; occupational therapist; psychologist. With regard to the
other seven additional assessment options, a greater percentage of nursing based staff
than social work based staff indicated a need for additional assessments. On average,
social work based staff indicated a need for 3 additional assessments per worker.
Health based staff indicated a need for 5 additional assessments per worker.
It is interesting to note that no one indicated a need under the ‘other’ option for a
continence assessment despite high percentages of staff noting dependency in this
area. No one indicated a need for either psychiatrist or psychologist assessment,
despite 24% of health based workers scoring the client as requiring ‘minimal
assistance’ or as being ‘dependent’ in terms of emotional & mental state.
Considerably higher percentages of health based workers indicated a need for a
learning disability assessment than did their social work counterparts. Also of interest
is the relatively high awareness of carer needs shown by health workers compared
with social work staff.
The findings as presented in tables 1-3 indicate interesting divergences between social
work based staff and health based staff.
Differences in scoring could be because of a number of factors. Firstly, the group of
care officers in particular, have been using this type of assessment daily for some
time. Their health counterparts on the other hand use it less frequently. Secondly the
39
assessment does not indicate what specific aspect of a topic is being assessed.
Different assessors are likely to have different interpretations of the assessment
question or prompt. The meaning of the terms ‘independent’, ‘minimal assistance’
and ‘dependent’ might form a third factor. These are not precise terms and cannot be
measured. Meaning lies within a range of possibilities.
It is also important to remember that no interaction with the client or his carers was
possible.
There is evidence in the findings to suggest that; a) Health based respondents assess
the client as more dependent than do the social work based respondents. b)
Conversely, there is a tendency for social work respondents to assess the client as
more independent than do the health based respondents. c) This tendency extends to
social work based respondents assessing the client as more able than he is, notably
with regard to personal care needs. d) Health based respondents identify more risks
and a need for more additional assessments than the social work based respondents.
e) There is a tendency from the health based respondents to form more assumptions
about the clients needs than do the social work based respondents.
4.3. Focus Group Findings.
See appendix ix for comments.
The focus group findings might serve to assist in interpretation of some of the
questionnaire results.
40

A subjective consideration of all of the comments from question 1 permits a grouping
into; those prompted by visual clues and; those prompted by verbal clues. The
number of responses prompted by visual clues is more than three times higher than
the responses promoted by verbal clues.
Question 1 – What clues did you pick up from the video that indicated to you
what the persons possible needs were?
Table 4 – comparison of visual and verbal clues.
Number of Visual Clues Number of Verbal Clues
Facts 32 10
Generalisations 2 0
The two physiotherapists and the three OT’s noted fifteen of the visual clues between
them, an average of 3 clues each.
The remaining health based respondents, a group of 15 people noted 13 visual clues
between them, an average of 0.86 clues each. 2 of these were generalisations.
The remaining social work based respondents, a group of 10 people, noted six visual
clues between them, an average of 0.6 clues each.
These figures are not significant because some respondents are more talkative than
others in the focus groups and some did not make any comment at all.
Verbal clues were picked up equally by all professions.
Interestingly, the two generalisations came from nursing respondents one of whom
generated the statement, “looked as if he needed 24 hour care.” B clearly said that he
slept all night and had no night-time toileting needs.
41
Question 2. What did these clues mean for you?
The responses to question 2 were analysed by comment into five categories: care
planning assumptions; further information; specialist assessment; identification of
issue/problem/need; carer need:-
Care Planning Assumption;-
2 from District Nurses. 2 from Care Officers. Need for Further Information;-
3 from district nurses. 6 from Care Officers/Senior Care Officers. 1 from OT.
Need for Specialist Assessment: –
1 from District Nurse. 1 from Physiotherapist.
Identification of issue/problem/need.
5 from Physiotherapist. 1 from Hospital nurse. 1 from District Nurse. 1 from Senior
Care Officer. 1 from OT.
Carers Need: –
1 from physiotherapist.
With regard to question 2, the two district nurse comments imply assumptions about
the specific level of care required by B.
Many respondents indicate a need for further information.
With regard to identification of issue/problem/need, the physiotherapists generated
most comments. It is interesting to note that their comments are quite specific and
42
diagnostic. The hospital nurse comments are couched in terms of problems but are
also specific and diagnostic. The OT identified a need for equipment.
Only 1 respondent, a physiotherapist, gave any consideration to carers needs.
Question 3. From your professional background, what knowledge or ideas did
you relate to these clues?
Question 3 was designed to elicit theoretical concepts that informed the assessments.
This question was not well phrased in that only 4 comments suggested any model or
theoretical concept. The question elicited a wide range of other comments, some
about need, some about use of experience, some about assessment of emotional state.
Two comments relating to emotional state are worth highlighting;-
“Difficult to assess emotions by looking at video he may throw a tantrum at any
time.” There would appear to be an element of assumption and of judgement in this
statement by a district nurse.
“Assessment of emotional state – if not able to communicate needs – danger of people
interpreting for him.” – Senior Care Officer.
Both comments are concerned with the difficulty of assessing emotional state from
the video.
Question 4, Do you have any relevant personal experience in any part of your
life, that helped you arrive at your assessment and that you would like to share?
1 Care Officer is noted as having a relative who is, “fairly disabled”.
43
1 OT is noted as having a niece who has cerebral palsy.
None of the other respondents declared any relevant personal experience.
Question 5. What professional experiences have you had that helped you to
arrive at your assessment?
7 workers noted previous experience with people who have cerebral palsy and/or
learning disabilities:- 3 District Nurses; 1 Physiotherapist; 2 Care Officers; 1 Senior
Care Officer.
7 other workers noted overlapping experience e.g. working with people who have had
a stroke; working with elderly people.
Questions 4 and 5 were designed to gather information about personal or professional
experience of assessors with regard to this assessment. Relatively few workers
indicated either personal or professional experience. This suggests that many workers
were confronted with a relatively new assessment experience. This might be a factor
that has influenced the findings of this study.
Question 6. Given all the information that you have, should this person be living
on his own in the community?
This was analysed by comment into:- affirmative; qualified affirmative; questioning.
Qualified affirmative was further divided according to comments relating to i. Client
choice; ii. Care needs statement; iii. Finance.
Affirmative:
1 Health based and 5 social work based respondents gave an unqualified affirmative:-
1 District nurse; 3 Care Officers; 1 Care Organiser; 1 OT;
44
Qualified Affirmative:
7 health based and 3 social work based respondents gave qualified affirmatives
Qualified by:
i. Client choice:
2 health based and 2 social work based staff qualified re client choice:-
ii. Care needs statement:
6 health based and 1 social work based staff qualified re care needs
iii. Finance.
1 health based and 2 social work based staff qualified re finance.
Questioning comment:
3 health based workers made questioning comment.
Question 6 was designed to act as a means of checking out any underlying
assumptions about B and his needs. In total 23 comments relating to this question
were gathered. In general, social work staff gave more unqualified affirmatives than
did health based staff. Health based staff gave more qualified affirmatives than social
work staff. The total of qualified and unqualified affirmatives shows equal numbers
of comments from both groups.
Consideration of the ‘care needs statements’ contained within the qualified
affirmatives is of interest. 6 health based staff qualified their affirmative with a care
needs statement. Their statements appear to contain assumptions about the type of
care or the level of care that B requires. “In a group home would be OK, but not on
his own." "Independent with help, it is a possibility rather than institutional care.”
“Not without support he needs an intensive care package.” “Protection from certain
45
people, he is very vulnerable.” Interestingly, district nurses also made the 3
questioning comments. “Learning disability and psychiatric needs and choice, it’s a
huge problem.” “Did he ever live (on his own) before, would he be able to cope?”
“Has he mental understanding to make the choice?”
It has been acknowledged that the focus group part of this study contained flaws. It
can not be considered as a definitive study, however certain themes emerge from the
focus group information.
The information suggests that a) OT’s and physiotherapists appear to be especially
alert to visual clues. b) Health based respondents appear to be more prone to forming
assumptions about need and level of service provision required. These assumptions
appear to be based on limited information. The statements concerning level of service
provision required suggest that the nursing based assessor perceives the client as
relatively ‘dependent’.
The information available from the focus group study appears to support some of the
findings from the questionnaire.
46
CHAPTER 5. ANALYSIS AND DISCUSSION
5.1. The information gathered by part one of the questionnaire clearly shows that the
people who participated in this study as respondents all have significant levels of
educational qualifications and with the exceptions of the student nurses, considerable
post qualifying experience. They are all intelligent, able people who produce good
quality assessments. There are however differences in these assessments both within
profession and between profession. This part of the study considers some of the
subtle historical, political, organisational and cultural factors at work including factors
related to role and implicit knowledge that might influence the assessor and
consequently the outcome of an assessment No criticism is intended towards the
respondents in this study or any other worker. The focus is very much on the
assessment process and the work systems within which assessment is carried out.
It is apparent from this study that health based respondents identify more risks and a
need for more additional assessments than the social work based respondents. It
would appear that there is a tendency from the health based respondents to form more
assumptions about the clients needs and there appears to be a tendency for health
based respondents to see the client as more dependent than do the social work based
respondents. Also, some of the findings from the questionnaire and some focus group
comments generated by nurses imply a degree of judgement about the client in terms
of his emotional state and the best care setting for him. Conversely, the social work
staff appear to see the client as more independent than do the health based workers. A
contextual consideration of these differences will be of value.
47
5.2. Social work – Historical and Political Context.
The unification of social services departments following the report of the Seebohm
Committee (1968) had an enormous influence upon social work in that it emphasised
community need. The underlying ideology was to meet social need through the fair
distribution of resources. Social work departments provided a ‘one door’ access for
local communities and social workers had the job of meeting those needs equitably.
These new arrangements had the effect of empowering social work as a profession in
that it was now a unified department within the Local Authority, an arrangement that
also supported professional status (Butrym 1989). Following this unification process
a number of studies were conducted to investigate how practice was affected by the
new arrangements. (Mayer and Timms 1970), (Hall 1974), (Blaxter 1976), (Rees
1978), (Smith 1980), (Lipsky 1980), (Satyamurti 1981), (Giller and Morris 1981).
Many of the researchers found that social workers were adopting a process of
informal decision making about clients in order to survive as workers in an
environment containing potentially overwhelming workloads. Lipsky seems to have
been credited with using the phrase ‘Street-level Bureaucracy’ to describe this process
and he used it as the title of his 1980 publication.
During this time, it can be argued that a fundamental tension lay at the heart of social
work practice. Firstly, there was the continuing debate on ‘what is social work’? On
the one hand was the concept of professionalised casework, on the other that of
community involvement and political action. (Brearley 1995). Secondly, the
ideology behind the Seebohm report was that of respect for the unique worth of the
individual. Social workers were trained to treat people differently according to their
48
individual and unique needs. Social work assessment, achieved through relationship
with an individual client, was the means of identifying need and developing an
appropriate response. The focus was on ‘process’ rather than ‘task’. In tension with
this lay what Ellis describes as, ‘the imperatives of rational administration.’ (Ellis et
al 1999 p264). Rational administration promoted selectivity through processes such
as eligibility criteria. Criteria that became increasingly selective as demand
outstripped supply of resources.
Alongside rising demand, the seventies and early eighties appear to have been a time
of ‘ill defined and ambiguous policy objectives’, (Ellis et al 1999 p 264) that left
workers without adequate operational guidelines. Coupled with this, the concept of
professional status of social workers meant relatively weak forms of bureaucratic
accountability and control. This cocktail of forces, Lipsky argues, meant that ‘street
level bureaucracy’ emerged because of worker need to make their work ‘more
predictable and hence controllable’ (Lipsky 1980 p86). The drive behind rational
administration coupled with increasing workload led workers to, ‘adopt simplifying
assumptions to categorise clients and respond in stereotyped ways to their situation’
(Ellis et al 1999 p 265). This is in line with findings by Rees who suggested that
social workers were guided by ‘practice based ideologies’ rather than by professional
principles (Rees 1978 p139,140). In practice this meant the categorisation of cases
according to ‘problem’ and the use of routinised responses by workers.
Come the White Paper, Caring for People, (Department of Health 1989) and the
(NHS and Community Care Act 1990). As previously noted, the NHS and
Community Care Act linked assessment of need to resources. Demand outstripped
available resources and yet Local Authorities were required to develop needs-led
49
services. The implementing Conservative Government presented Local Authorities
with prescriptive guidance papers and rational arguments that firmly ignored any
inherent contradiction and left little doubt about the ‘rationing’ element of the task in
hand. The ‘agenda, appeared to be to bring social security spending under control.
Couple this with a second agenda, firmly rooted in the ‘professionalised casework’
side of the social work debate. It can be argued that the NHS and Community Care
Act and corresponding process could be seen as an attempt to bring social work
practice firmly under managerial control. The process of care management and
assessment is highly prescriptive and because demand and resources are constantly
unmatched - to the detriment of Local Authority budgets - there is inevitably a high
degree of managerial control. This control manifests in policy and procedure
documents and increasing use of IT systems as monitoring tools. Indeed it might even
be argued that there exists a process of de-professionalisation. Systems that are
prescriptive do not require highly trained professionals to run them. ‘The NHS and
Community Care Act is a predominantly administrative rather than professional
model of community care’ (Hughes 1995).
Some similar conditions exist with this new model of social work and with Lipsky’s
street level bureaucracy. The new system of assessment and care management is
fundamentally linked to rationing and Ellis argues that the operation of it performs a
similar protective function to the informal rationing described by earlier writers. The
implication being that workers will ‘adopt simplifying assumptions to categorise
clients and respond in stereotyped ways to their situation’ (Ellis et al 1999 p 265).
‘Observation of practice suggests they (social workers) complied quite willingly with
formal procedures designed to ration their time and other resources…Where
50
informal judgements continued to shape decision making, these tended to reinforce
rather than challenge dominant rationing imperatives.’ (Ellis et al 1999 p277). One
might expect that this could lead to the categorisation of cases according to ‘problem’
and the use of routinised responses by workers. (Rees 1978 p139, 140).
5.3. Nursing – Historical and Political Context.
Binnie and Titchen identify three distinct styles of nursing practice; traditional,
individualised and patient centered (Binnie, Titchen 1999 p9). With regard to
traditional nursing, they argue that it has developed in its current role through the
influence of two historical figures, Florence Nightingale and Mrs. Bedford-Fenwick.
Nightingale focused on nursing as vocation and a calling to God. Bedford-Fenwick
attempted to establish nursing as a self-regulating profession. The two influences
manifested as an ethos towards humane, holistic caring with overtones of the
discipline, obedience and self-denial of religious life (Binnie, Titchen 1999 p10). The
influence of Bedford-Fenwick shifted the focus away from the spiritual towards the
scientific. Scientific at the time meant medical science and the medical model of
practice. The argument being that nursing placed itself in a hierarchical relationship
to medicine. Binnie and Titchen suggest that the style of nursing that emerged was
concerned with completion of practical tasks and borrowed from the industrial
production-line model of work organisation (Binnie, Titchen 1999). A 1950’s study
of nursing described the system as, ‘…an organised defence against stress and
anxiety’ (Menzies 1970) the system was routinised, task focused and hierarchical. It
was not until the seventies that this began to alter in Britain.
51
Individualised nursing can be seen as a move away from this earlier approach. In the
fifties, American nurses fought for professional status. An important aspect of their
struggle was to achieve university level training for nurses to establish nursing as a
credible scientific discipline in its own right. The prevailing philosophy sought to
temper ‘mechanistic’ scientific beliefs with the concept of ‘subjective human
experience’. This was attractive to nurses who had recognised the dehumanising
effects of the hospital system (Binnie, Titchen 1999 p12). The manifestation of these
ideas into practice resulted in the concept of individualised care plans. The attempt to
introduce this new concept of nursing was hampered by the prevalence of traditional
practices. In most cases the individualised care plans were completed in routinised
ways (Binnie, Titchen 1999 p13).
In the late seventies this ‘new’ system of individualised nursing was introduced into
Britain. Managers and academics in Britain had become aware of the ‘traditional’
systems inadequacies and introduced the ‘individualised’ system in an attempt to
promote positive change. Hospitals were placed under pressure to adopt the new
system and the process was hurried. ‘Emphasis was placed more upon producing the
visible, written care plan than on changing the way that patients were nursed’
(Binnie, Titchen 1999 p14). Again the suggestion was that the process became
routinised and heavily influenced by the prevailing and controlling traditional culture.
Patient-centered nursing emerged through the influence of the existentialist
philosophers who believed that people were not merely a product of environmental
factors or heredity but were in a continual process of growth and development that
was full of potential. Psychologists of the fifties and sixties found in this philosophy a
different basis for the study of human beings, one that incorporated subjective
52
experience and acknowledged uniqueness. Inevitably, nurse theorists were influenced
by this process and began to suggest changes in practice. ‘The patient’s status
changed from passive recipient, or object, of nursing care to active partner engaged
in improving his own situation’ (Binnie, Titchen 1999 p18). Patient centered nursing
also used individualised care plans and assessment techniques but now they were part
of a repertoire of techniques used for patient care. ‘Scientific methods were to be the
servants of a healing art’ (Campbell 1984). The writer acknowledges the existence of
other models of nursing such as team nursing, primary nursing and so on and suggests
that these are mainly organisational models within which different ideologies of
nursing care can operate (Manthey 1980).
The professional status of district nurses is not now in doubt, however, as recently as
the sixties it appears that district nurses were underused and under-acknowledged
(Hockey 1966, 1968) (Skeet 1970). It was not until 1960 that statutory training for
district nurses was imposed. The development of health centers in the sixties and
seventies appears to have created an environment where district nursing could
flourish. The traditional relationship with a doctor gave way to a relationship with
several members of a multi-disciplinary Primary Health Care team. The hierarchical
relationship between nurses and doctors appears to continue to be played out within
these teams however and district nurses operate in, ‘a more institutional and
hierarchical system alongside other grades…’ (Sweet, Ferguson 2000 p96). Changes
in hospital discharge procedures have had an influence on the recent development of
District nursing. Hospitals have reduced length of stay and District Nurses are much
more required to nurse patients at home. (DHSS 1993), (Timmins 1996). They
provide clinical nursing care and advice, health care consultations, nursing assessment
53
of both individual patients and community populations and they have a significant
role in health promotion and health education.
In more recent times, the health service reforms associated with the market economy
have had considerable influence upon nursing, especially district nursing. Between
1972 and 1987 the workload of district nurses increased four-fold with no additional
qualified staff (Ross 1987). The use of unqualified staff in community nursing roles
became the norm and the district nurse is usually required to supervise these staff.
The increase of patients at home coupled with the resource rationing aspects of the
1990 Act meant that district nurses, as gatekeepers to health care resources, were
faced with the dilemma of prioritisation of clients (Haughey 1995 p200). Laurent
argues that the service was becoming resource driven rather than needs led Laurent
(1993 p41-2). This inevitably created a tension with the emerging ‘patient centered’
approach to nursing. The creation of Local Health Trusts as a response to the
purchaser/provider split increased this tension. These local trusts fostered the
increasing use of business managers whose primary role was to ensure that the
Governments ‘rationing’ agenda was being fulfilled. The introduction of care
management also influenced the role of the district nurse because it moved them
away from a ‘maintenance’ role with dependent ‘social care’ patients. The new
caseload tended to consist of those who, ‘are severely disabled, acutely ill or dying’
(Lawton, Cantrell, Harris 2000, p 186).
5.4. Influence of Organisational Culture.
54
Culture has been described as ‘the way we get things done around here’ (Bower
1966). The concept of ‘culture’ is important to consider when looking at the
organisational influences upon workers. Handy (1985) describes four organisational
cultures; power, role, task and person culture. Power culture implies an organisation
where control is exercised by a central elite. There are few rules or procedures and
little bureaucracy. In an organisation based on role culture the processes tend towards
a high level of rules, procedures and bureaucracy. The task cultural organisation
emphasises getting the job done and making best use of skills and resources. People
are encouraged to take the lead when their skills match the needs of the goal rather
than because of their position within the hierarchy of the organisation. The ‘person
culture’ organisation is focused on the individual who takes precedence over the
needs of the organisation.
Consideration of the social work and health organisation, from which the respondents
for this study were drawn suggest the prevalent organisational cultures. The social
work organisation is part of the Local Authority provision. It has a director and senior
managers who report to a committee comprising local councilors, the organisation is
hierarchical. There appears to be a mix of power, role and task cultures. The Director
and senior staff represent a central elite who retain tight control over many aspects of
the organisation, in particular those relating to money. A high level of rules,
procedures and bureaucracy exists. These tend to relate to controls over spending and
include information gathering and monitoring both with regard to spending as well as
for quality assurance purposes. Some sub-groups can be described as task centered
such as pilot projects and so on. These tend to be short life groups formed for a
55
specific purpose. The main cultural styles would appear to lie in the domains of role
orientation and power orientation especially concerning finance and resource use.
The LHCC has a general manager at its head who is supported by a team of senior
management staff. This management team perceive themselves as ‘support to’ the
local primary care staff, community hospitals and PAM’s. In fact they have
considerable control over the activities of these groups through their control of the
budgets. An element of power culture is present as exercised by the central
management team but the main cultural theme is role based. Some elements of task
culture are present within specialist teams, pilot projects and some primary care
teams.
Harris (1975) argues that both power and role oriented organisations are slow to adapt
to change. He goes on to say that ‘The power and role-oriented organisations simply
do not provide for the development and utilisation of internal commitment, initiative
and independent judgement on the part of members at other than the highest levels’
(Harrison R, 1975).
It would seem likely that social work and health workers would describe themselves
as being ‘committed’ and in using ‘initiative’ and ‘independent judgement’. Research
findings suggest that there are other factors that influence the likelihood of these
‘ideals’ being present in the workplace.
Individualised nursing was introduced into Britain in relatively recent times. The
findings being that with the introduction of this style of nursing, routinised processes
became the norm. (Binnie, Titchen 1999 p14) The concept of patient centred nursing
56
has replaced individualised nursing however recent research suggests that professional
responses remain rooted in the previous culture. Binnie and Titchen found this in
their action research with ward nurses, and noted that ’We had to develop strategies
for helping the nurses to confront and challenge institutionalised attitudes and
behaviours’ (Binnie and Titchen 1999 p99).
Manthey (1980) argued that decentralised decision making permitted the best
organisational framework to achieve patient centered nursing. This means that
authority for decision making must be ‘devolved to nurses at the bedside’ (Binnie and
Titchen 1999 p62). What Binnie and Titchen found in practice was routinised
behaviour focused on the completion of practical tasks and with a hierarchical system
of decision making. This had the effect of stifling the ‘intelligent, alert questioning
and creativity necessary for decentralised decision making’ (Fretwell 1980).
The organisational arrangement of nursing tends to have a ‘role orientation’ as
described by Harrison. It is ‘rational, orderly, it has a strong emphasis on hierarchy
and status but is moderated by commitment to legitimacy and legality’ (Harrison 1975
p201). In this type of organisation, ‘The correct response tends to be more highly
valued than the effective one’ (Harrison 1975 p201).
Consideration of social work has shown that when resources are limited and control of
process is high, routinised responses are common (Rees 1978), (Lipsky 1980), (Ellis
et al 1999). Nurses too could be considered to be under similar pressure, in particular
district nurses who are gatekeepers to limited health resources. (Laurent 1993),
57
(Haughey 1995). A routinised response by nurses may well be to over estimate a
patients care needs. (Rubenstein et al 1984)
The concept of risk within the context of ‘Community Care’, carries the meaning of
‘probability of loss or harm’. (Unsworth, 2000, in Lawton, Cantrell, Harris, 2000
p120) Unsworth argues that this definition of risk has meant that health care
professionals in particular, view the concept of risk in a negative way (Unsworth
2000, p121).
Perhaps linked to this is the influence of the Law. In Law, each nursing practitioner is
accountable for his or her actions. (Lawton et al 2000) This means that, if a nurse
does not identify problems or symptoms during a nursing assessment and the patient
in some way highlighted the problem or symptom during the process, the nurse is
liable in law. (Lawton et al 2000 p122). This liability also extends to the employing
organisation through vicarious liability. This fact must drive the tendency towards
structure and bureaucracy and might also manifest as rigid policies and procedures
such as those found in the nursing profession and described by Harrison (1975).
It would seem possible that these influences might lead to nursing staff adopting a
‘cautious approach’ when carrying out an assessment of need. A cautious approach
coupled with a tendency towards routinised responses by nursing based respondents
appears to be consistent with the findings of this study.
58
The social workers in this study appear to operate within a mainly role oriented
organisation with aspects of power orientation relating in particular to resource and
finance issues. Harrison (1975) suggests that these orientations will tend towards lack
of commitment, initiative and independent judgement on behalf of workers.
There has been previous consideration of the increase in managerial control of social
work and how that has manifested in procedures and systems. Consideration has also
been given to how the system of care management and assessment coupled with this
increased managerial control has created similar conditions to those described by
Lipsky (1980). Ellis et al (1999) found that the response to these conditions was that
social work practices were based on stereotyped and routinised responses to client
situations. Ellis et al (1999) further found that social workers were content to accept
procedures ‘designed to ration their time and other resources’ (Ellis et al 1999 p277).
It is generally acknowledged that an element of the care management process is
concerned with the allocation of limited resources (Department of Health 1991). This
served to push practitioners towards adopting resource led measures (Leat, Perkins
1998). The adoption of resource led measures might impact on the assessment
process through over estimation of client ability. The more able the client is, the less
care and resources will be required.
One aspect of the power culture of the social work organisation from which the
respondents were drawn is the strict control of financial resources. The respondents
in this study have no authority whatsoever about allocation of finance. Back in 1986,
Davies and Challis found that if resources are too limited, assessors may be less
59
thorough. They go on to say ‘that resources are not available or are difficult to
obtain…deters workers from making assessments which are comprehensive, detailed
and precise’ (Davies, Challis 1986 p239). Routinised responses will also be likely
(Rees 1978), (Lipsky 1980), (Ellis et al 1999).
This study has highlighted a tendency for the social work based respondents to over
estimate the ability of the client. The influences described above leading to
simplification, routinisation and lack of precision coupled with the adoption of
resource led measures would be consistent with this.
5.5. Influence of professional models of disability.
There has been previous discussion about the nursing concept of ‘wholeness’ and
holistic assessment. There is another ‘model’ that lies in tension with this. Several
writers including Morris (1993) and Massie (1994) have commented upon the
‘medical’ model and the ‘social’ model of disability. There has been previous
discussion about the hierarchical relationship that exists between GP’s and nurses
(Sweet, Ferguson 2000). GP’s in general appear to prefer the medical model and
Unsworth (2000) argues that in recent years, the introduction of the internal market in
health care has given GP’s greater influence.
The findings from this study would be consistent with the predomination of the
medical model amongst the health based respondents.
5.6. Influence of Role.
60
Role theory suggests some ways that peoples perceptions about their occupations are
formed. Katz and Kahn (1966) describe the ‘role set’ as the group of people who
perform a similar role or have a vested interest in how an individual performs his or
her role. They go on to consider how each member of a ‘role set’ sends important
signals to the role holder about what they should do or how they should behave in
their role (Katz, Kahn, 1966 p190). Of particular interest is their consideration of
people who work in more than one organisational culture. They state that ‘Roles
become more complex when they require the focal person to be simultaneously
involved in two or more subsystems, since each is likely to have its own priorities and
culture’ (Katz, Kahn 1996 p197).
District nurses are currently being asked to be simultaneously involved in their own
role as well as the role of assessor of need for community care assessments. They
also appear to be very wary of the role of care manager and their professional
literature has described it as ‘short term’ and ‘finance led’, a ‘hit and run activity’
(Lawton et al 2000 p198). The same writers go on to warn that ‘district nurses are
likely to lose that nurse-patient intimacy…’ (Lawton et al 2000 p198).
Care management and community care assessment of need has been undertaken by
Local authority staff for eight years. Many of the study respondents had length of
service well in excess of this. Many of the social work respondents have been
carrying out community care assessment of needs for much of that time. It is likely
that they have successfully internalised this role and integrated it into their practice.
61
The concept of role conflict might be most appropriately applied to the nursing
respondents in this study who are relatively new to the task of community care
assessment. Research suggests that role conflict can occur when ‘the nurse is faced
with competing expectations of the various stakeholders’ (Bousfield 1997 p245).
5.7. Influence of Implicit Knowledge
Twigg and Atkin (1994) suggest two main influences upon workers when making an
assessment. The presence of clear and explicit policy and practice guidance and the
use of ‘implicit knowledge’. Implicit knowledge is based upon professional training
and values, the culture of the office and assumptive worlds.
By ‘assumptive worlds’, Twigg and Atkin mean the internal assumptions of an
assessor that often exists on a sub-conscious level (Twigg, Atkin, 1994). The idea of
workers being influenced by an internalised concept such as ‘medical model’ or
‘social model’ would exemplify this.
It should be noticed that in the case of the assessment process used in this study, there
exists no adequate clear and explicit policy and practice guidance. This will tend to
require the assessor to have to rely on their implicit knowledge.
The implicit knowledge and in particular the ‘assumptive world’ of some nursing
respondents in this study might be in part indicated by the concept of hospital setting.
All nurses have experience of working in hospital. Nursing perception of these
‘institutional’ settings is likely to be quite different from that of others. Binnie and
62
Titchen found with nursing staff that they ‘had to develop strategies for helping the
nurses to confront and challenge institutionalised attitudes and behaviours’ (Binnie
and Titchen 2000 p99). This implies that the institution of the hospital is a powerful
presence in nursing circles.
A number of focus group comments from the nursing respondents imply a need for
institutional care. These comments appear to be consistent with the idea of nursing
respondents having relative familiarity with the ‘institutional’ based care setting of
hospital and conversely might imply a relative unfamiliarity with community based
social care arrangements. They might also be seen to reinforce the idea that the
‘medical model’ of care is predominant.
The implicit knowledge of community nursing staff is also likely to be different.
Consideration of district nursing staff indicates that they are very familiar with and
competent at nursing patients in the community (Timmins 1996). Research findings
suggest however that their experience tends to be greater with patients who are
severely disabled, acutely ill or dying (Lawton et al 2000). Previous discussion has
highlighted that since the introduction of care management, community nursing staff
have lost their social-health care clients and consequently, although patients are
generally less dependent, they now require more skilled nursing input (Barrett,
Hudson 1977). This high degree of association with a group who undoubtedly have
multiple and complex needs may well influence the district nurses perception of need
(Ross 1987).
63
Although the rhetoric of patient centered nursing is well developed, the actuality is
often different ‘the cultural legacy of traditional nursing inhibited the kind of
independent thinking and behaviour required for patient-centered practice’ (Binnie
and Titchen 2000 p99). This finding is built upon previous work by the same authors
who found that ‘the system denied them (staff nurses) the opportunity to practice in
the way that they thought they should…they had not been fulfilling the roles they had
been prepared for…’ (Binnie and Titchen 1999 p63). This implies that the concepts
of holism and patient centered practice although possibly a part of the implicit
knowledge of the nursing respondents, are not as powerful an influence as the
organisational culture and role expectations.
The video used in this study was of a man who has physical disabilities and a learning
disability. There exists in social work a fairly strong theoretical base stemming from
such researchers as Wolfensberger (1972) Brandon (1988) and O’Brian (1989).
Whilst work with this client group has not been accorded especially high status, there
has been a slow introduction of theoretical concepts into the social work culture. This
theoretical base has tended to encourage perception of the client as someone able to
participate fully in all aspects of society through ‘the use of culturally valued means in
order to enable people to live culturally valued lives’ (Wolfensberger 1972). These
concepts are likely to have entered the implicit knowledge of the social work assessor.
It should be noted that few of the respondents noted any experience with people who
had similar conditions to the client. The local role developments had not included this
‘client group’. The presence of the concepts proposed by Wolfensberger and others,
and the concept of ‘social model’ as part of the implicit knowledge of the social work
64
based respondents would serve to provide them with a guiding theoretical base to
inform practice.
The quite different implicit knowledge of the health based respondents means that it is
possible that nursing respondents were struggling to complete a community care
assessment of need for this client.
Ellis (1993) highlighted that the more difficult the case, the more use of moral
judgements in the assessment process. This study suggests that there is a tendency for
health based respondents to form more judgmental assumptions about client need than
do the social work based respondents.
The extent to which the implicit knowledge of any of the respondents in this study is
influenced by ‘model’ of disability, training and other factors is not possible to
establish and might form the basis for future work.
5.8. Influence of Interpretation
Given that the role of assessor for a community care assessment of need is a new role
for the nursing respondents, it seems likely that they could be facing the sort of
difficulties with respect to community care assessment of needs that the social work
profession faced eight years ago i.e. that of distinguishing between an assessment of
need and a service response (Macdonald and Myers p26). Certainly, several of the
focus group comments in this study suggest level of service provision and these stem
mainly from nursing respondents.
65
There has been previous consideration of nursing staff concern about the role of care
manager. There is also some evidence to suggest that members of the nursing
community perceive the process of community care assessment of needs as quite
unsophisticated and possibly even unprofessional. ‘The documentation in care
management does appear to have more to do with a paperwork exercise than
assessment, in that although it is complex it is relatively limited in relation to the
philosophy of professional assessment’ (Lawton et al 2000 p197).
With regard to this study, it begins to seem possible that the nursing respondents were
making what amounts to a completely different type of assessment using the same
document. Their implicit knowledge, their experience and their assumptive worlds
are likely to be significantly different from social work based respondents. The same
assessment question or prompt is likely to generate a different set of associations or
conceptual links. An earlier example relating to the prompt of ‘communication’
questioned what was being assessed, speech ability or ability to get a message across.
The lack of clear guidelines will serve to exacerbate this sort of problem. An
interesting continuation of this study might be an examination of the implicit
knowledge and the assumptive world of the respondents.
5.9. Concept of Inter-professional working.
The literature search showed that there was an acknowledgement in the research
literature of different outcomes to the assessment process linked to assessors from
different professional backgrounds. This study supported this finding and went on to
66
explore specific differences. Many writers have turned to the concept of closer inter-
professional working as an important part of the solution to this fundamental problem,
in particular, the work of Ovretveit is often cited. Ovretveit describes a series of
models of team working based on; degree of integration; membership; process – in
particular the clients pathway through the team, and lastly; management (Ovretveit J
1997 p9).
The concept currently being promoted by government in both England and Scotland is
that of a single shared assessment that can be carried out by a worker from any agency
and shared with other workers as required. The motivating belief is that there is
duplication of effort that is both wasteful of resources and irksome to the client who
often experiences multiple assessors asking the same questions (NHS bodies and
Local Authorities Partnership Arrangement Regulations 2000), (Scottish Executive
2000), (Scottish Executive 2001). The Scottish Executive (2001) says that the
assessment should be ‘carried out, preferably by one person, but involving others if
necessary’ (Scottish Executive 2001). In practice, given that a significant part of the
agenda appears to be about duplication of effort and saving resources, it seems likely
that the assessment is likely to be carried out by one person, certainly in the first
instance. Given this assumption, then the organisation of multi-disciplinary working
arrangements becomes crucial.
Many current arrangements appear to be more appropriately described as a network
rather than a team. Given the findings from this study, then the levels of
communication within these networks and the mechanisms for problem solving and
67

conflict resolution are likely to be tested through the process of single shared
assessment.
68

CHAPTER 6. CONCLUSIONS AND RECOMMENDATIONS
6.1. Conclusions
Social Work based workers.
Resource rationing, increased managerial control, prescriptive systems of work,
organisational culture, model of disability and implicit knowledge influence practice. The
effects are a tendency for workers to assess their client as more able than their health based
counterparts. In some instances this has the effect of assessing the client as more able than
is in fact the case.
Health based workers.
Nursing style, organisational culture, resource rationing, concerns about risk, especially in
relation to the law, model of disability, role conflict and implicit knowledge influence
practice. The effects are a tendency to assess the client as more dependent and as having a
higher level of risk than their social work based counterparts. There is also a tendency
towards caution which manifests as request for additional assessments. This latter is
perhaps important at a time when duplication of effort is seen as a political agenda. It
further appears that this group are more likely to form assumptions and make a greater
degree of judgement about the client.
Finally, questions are raised about the interpretation of assessment questions by assessors
from different professional backgrounds.
69
6.2. Recommendations.
Recommendations for further study.
One key theme emerging from this study was the extent to which the implicit knowledge
of a practitioner might serve to set their conceptual framework and have an influence when
the practitioner is considering an assessment question or prompt.
Two approaches to this present themselves;-
1) An examination of the implicit knowledge and assumptive world of health based and
social work based practitioners, in particular with regard to concepts such as ‘holism’,
‘patient centered’, ‘person centred’ and model of disability.
2) A piece of action research to establish a process of community care assessment of need
that is not unduly influenced by differences relating to professional background.
Recommendations with regard to practice improvements.
1) Careful definition of key terms and concepts used in the community care
assessment of needs process.
2) Development of clear and explicit policy and practice guidance for community
care assessment of needs.
3) Shared training with regard to community care assessment of needs.
4) Development of appropriate organisational structure to facilitate effective multi-
disciplinary working.
70
Appendix i. Assessment of Need – Professional Background. Name: ____________________________________ Telephone Number______________ contact address:________________________________________________________ Current Professional title: _______________________________________________ Length of service in this professional capacity: _______________________________ 1. Details of previous service/experience that could enhance current professional
competence; (Please use back of sheet if more space is needed) Name of role Dates, from - To.
2. Professional qualifications held; (Please use back of sheet if more space is needed) Qualification Date of qualifying
3. Details of other appropriate training: (Please use back of sheet if more space is
needed) Confidentiality Statement Confidentiality will be maintained throughout this piece of work. At no time throughout the course of this work will any names or other means of identification of any participant in any of the groups be used in any public way, either verbally, or in writing. At no time will any of the participants have access to information about any of the other participants other than knowing who are the members of their own group and having awareness of the comments which might arise in the focus group element of the work.
71
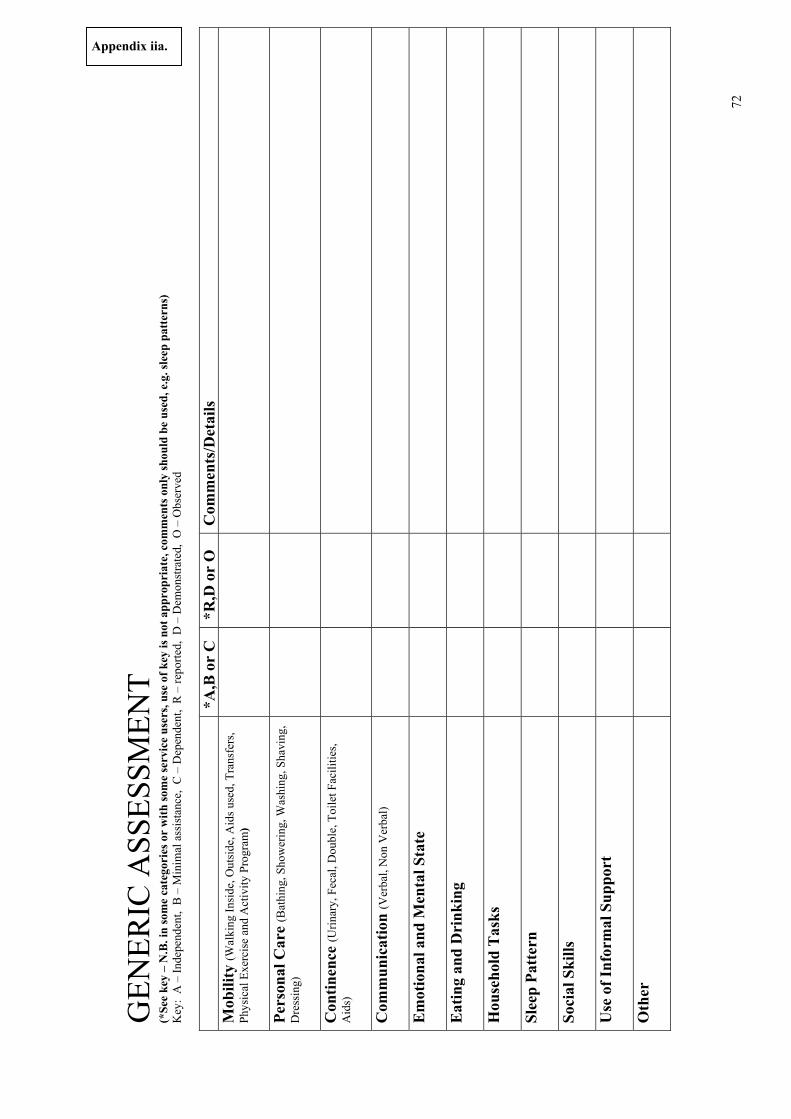
GEN
ERIC
ASS
ESSM
ENT
(*Se
e ke
y –
N.B
. in
som
e ca
tego
ries
or
with
som
e se
rvic
e us
ers,
use
of k
ey is
not
app
ropr
iate
, com
men
ts o
nly
shou
ld b
e us
ed, e
.g. s
leep
pat
tern
s)
Key
: A
– In
depe
nden
t, B
– M
inim
al a
ssis
tanc
e, C
– D
epen
dent
, R
– re
porte
d, D
– D
emon
stra
ted,
O –
Obs
erve
d
*A,B
or
C
*R,D
or
O
Com
men
ts/D
etai
ls
Mob
ility
(Wal
king
Insi
de, O
utsi
de, A
ids u
sed,
Tra
nsfe
rs,
Phys
ical
Exe
rcis
e an
d A
ctiv
ity P
rogr
am)
Pers
onal
Car
e (B
athi
ng, S
how
erin
g, W
ashi
ng, S
havi
ng,
Dre
ssin
g)
Con
tinen
ce (U
rinar
y, F
ecal
, Dou
ble,
Toi
let F
acili
ties,
Aid
s)
Com
mun
icat
ion
(Ver
bal,
Non
Ver
bal)
Em
otio
nal a
nd M
enta
l Sta
te
Eat
ing
and
Dri
nkin
g
Hou
seho
ld T
asks
Slee
p Pa
tter
n
Soci
al S
kills
Use
of I
nfor
mal
Sup
port
Oth
er
Appendix iia.
72
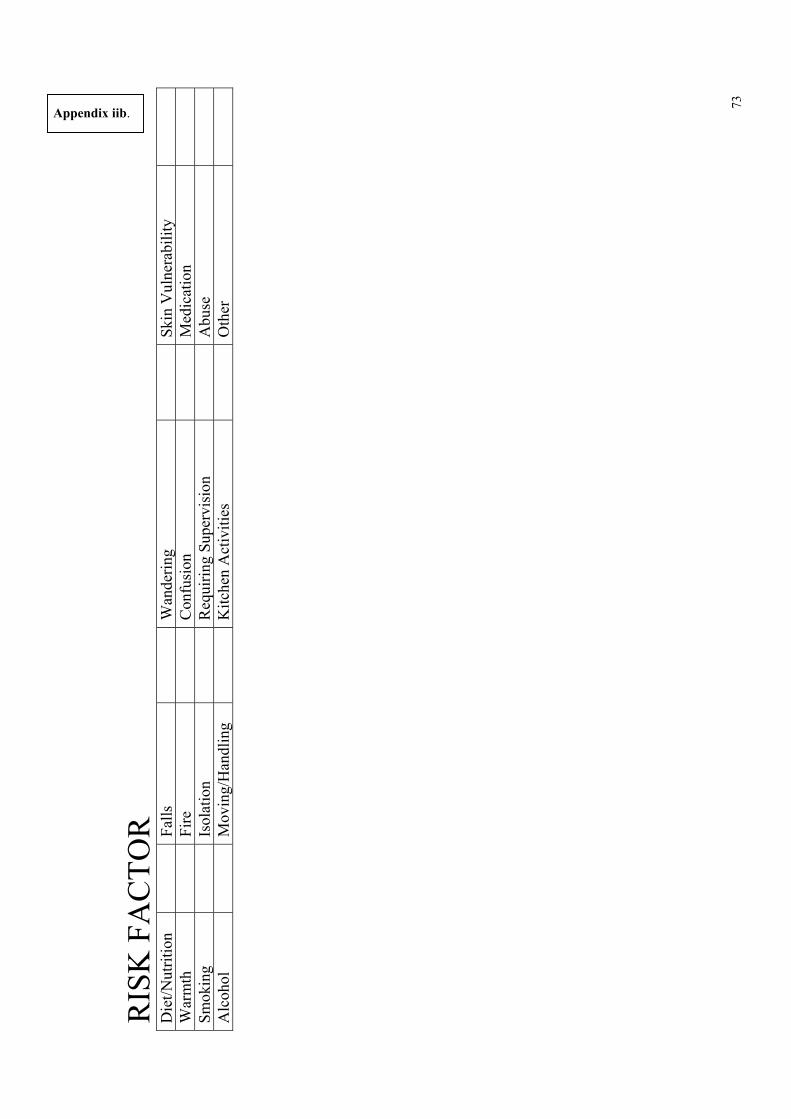
Appendix iib.
RIS
K F
AC
TOR
D
iet/N
utrit
ion
Falls
Wan
derin
gSk
in V
ulne
rabi
lity
War
mth
Fi
reC
onfu
sion
Med
icat
ion
Smok
ing
Is
olat
ion
Req
uirin
g Su
perv
isio
nA
buse
Alc
ohol
Mov
ing/
Han
dlin
gK
itche
n A
ctiv
ities
Oth
er
73
Appendix iic.
AD
DIT
ION
AL
ASS
ESS
ME
NT
S C
arer
s Ass
essm
ent
C
hiro
pody
Com
mun
ity C
are
Dem
entia
Tea
m
D
ietic
ian
Lear
ning
Dis
abili
ty
N
ursi
ng -
Com
mun
ity
N
ursi
ng -
Hos
pita
l
Occ
upat
iona
l The
rapi
st
Ph
ysio
ther
apis
t
Psyc
hiat
rist
Psyc
holo
gist
Sp
eech
/Lan
guag
e Th
erap
ist
O
ther
Rea
son
for
Ref
erra
l
74
Appendix iii. Assessment of Need – Professional Background Location___________ Date ________________ No. in group ____________ What clues did you pick up from the video that indicated to you what the persons possible needs were? What did these clues mean for you? From your professional background, what knowledge or ideas did you relate to these clues?
75
Do you have any relevant personal experiences in any part of your life, that helped you arrive at your assessment and that you would like to share? What professional experiences have you had that helped you to arrive at your assessment? Given all the information that you have, should this person be living on his own in the community?
76
Appendix iv. Background information sheet. Client moved into own tenancy from his parental home. He wished to be more independent. He has a rota of 4 helpers over a 24 hour period. His house is fully adapted for his needs. He uses a hoist plus helper to transfer. He does not require any medication. He has own car leased through Motability scheme, staff members are insured to drive it.
77
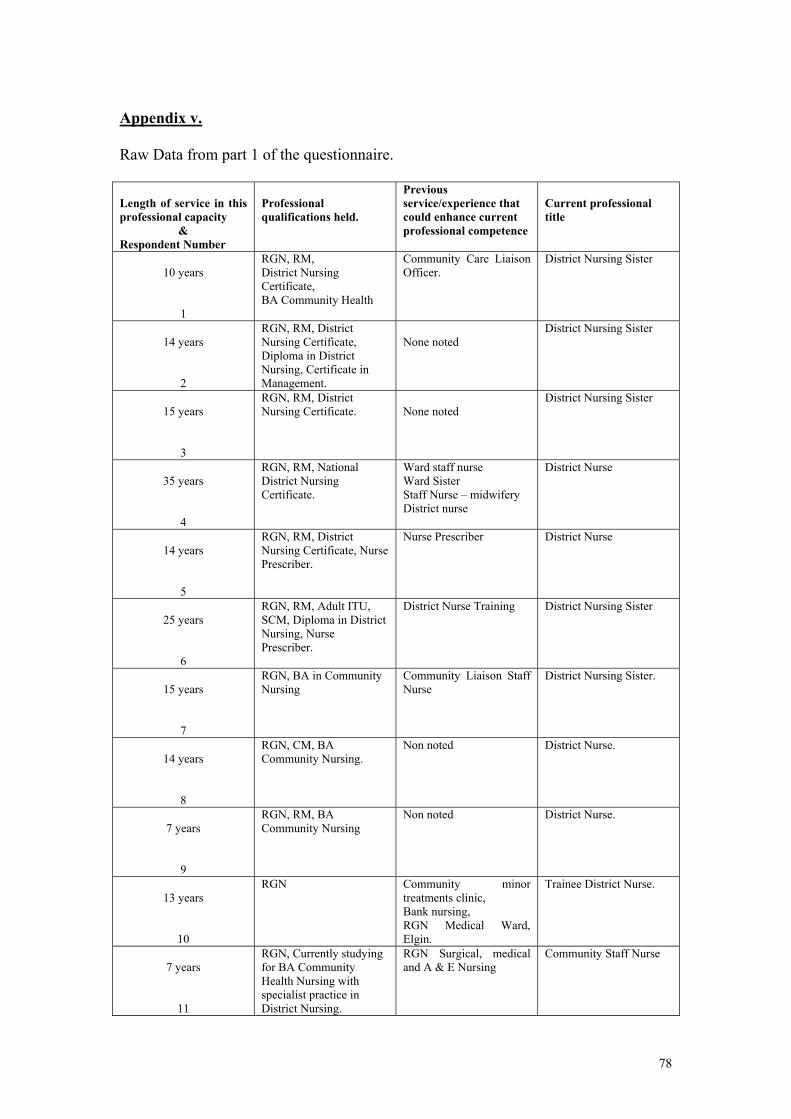
Appendix v. Raw Data from part 1 of the questionnaire. Length of service in this professional capacity
& Respondent Number
Professional qualifications held.
Previous service/experience that could enhance current professional competence
Current professional title
10 years
1
RGN, RM, District Nursing Certificate, BA Community Health
Community Care Liaison Officer.
District Nursing Sister
14 years
2
RGN, RM, District Nursing Certificate, Diploma in District Nursing, Certificate in Management.
None noted
District Nursing Sister
15 years
3
RGN, RM, District Nursing Certificate.
None noted
District Nursing Sister
35 years
4
RGN, RM, National District Nursing Certificate.
Ward staff nurse Ward Sister Staff Nurse – midwifery District nurse
District Nurse
14 years
5
RGN, RM, District Nursing Certificate, Nurse Prescriber.
Nurse Prescriber District Nurse
25 years
6
RGN, RM, Adult ITU, SCM, Diploma in District Nursing, Nurse Prescriber.
District Nurse Training District Nursing Sister
15 years
7
RGN, BA in Community Nursing
Community Liaison Staff Nurse
District Nursing Sister.
14 years
8
RGN, CM, BA Community Nursing.
Non noted District Nurse.
7 years
9
RGN, RM, BA Community Nursing
Non noted District Nurse.
13 years
10
RGN Community minor treatments clinic, Bank nursing, RGN Medical Ward, Elgin.
Trainee District Nurse.
7 years
11
RGN, Currently studying for BA Community Health Nursing with specialist practice in District Nursing.
RGN Surgical, medical and A & E Nursing
Community Staff Nurse
78
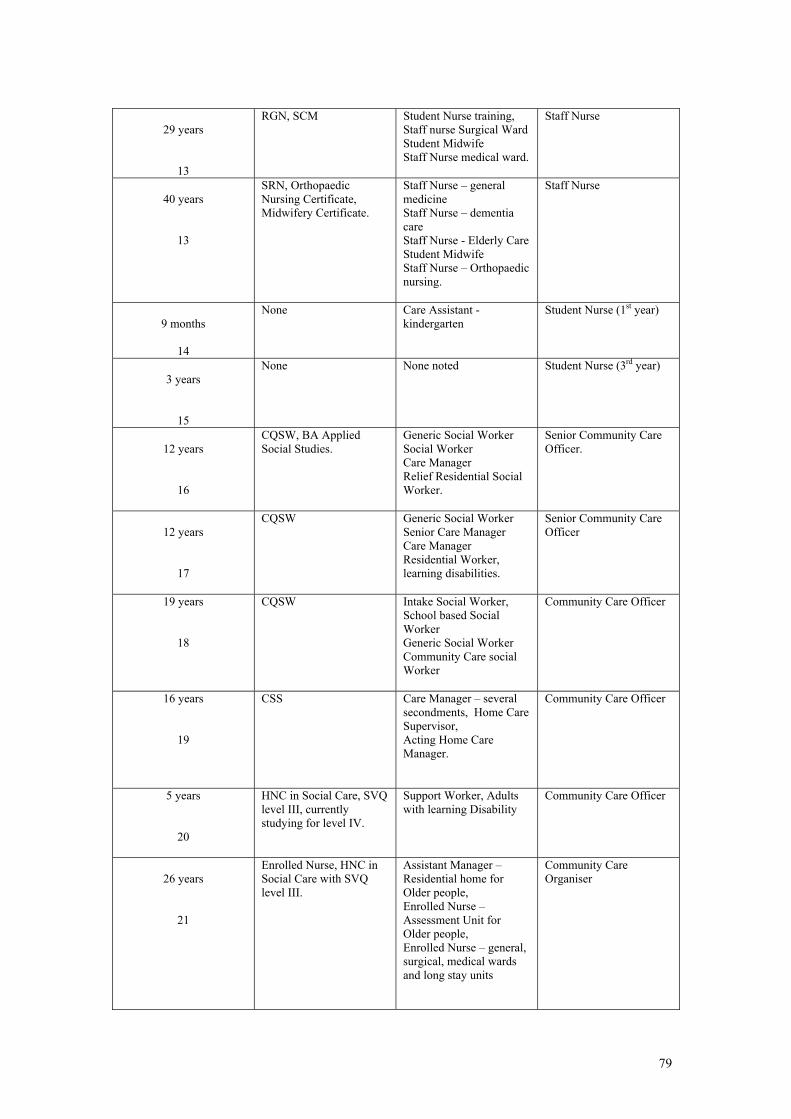
29 years
13
RGN, SCM Student Nurse training, Staff nurse Surgical Ward Student Midwife Staff Nurse medical ward.
Staff Nurse
40 years
13
SRN, Orthopaedic Nursing Certificate, Midwifery Certificate.
Staff Nurse – general medicine Staff Nurse – dementia care Staff Nurse - Elderly Care Student Midwife Staff Nurse – Orthopaedic nursing.
Staff Nurse
9 months
14
None Care Assistant - kindergarten
Student Nurse (1st year)
3 years
15
None None noted Student Nurse (3rd year)
12 years
16
CQSW, BA Applied Social Studies.
Generic Social Worker Social Worker Care Manager Relief Residential Social Worker.
Senior Community Care Officer.
12 years
17
CQSW Generic Social Worker Senior Care Manager Care Manager Residential Worker, learning disabilities.
Senior Community Care Officer
19 years
18
CQSW Intake Social Worker, School based Social Worker Generic Social Worker Community Care social Worker
Community Care Officer
16 years
19
CSS Care Manager – several secondments, Home Care Supervisor, Acting Home Care Manager.
Community Care Officer
5 years
20
HNC in Social Care, SVQ level III, currently studying for level IV.
Support Worker, Adults with learning Disability
Community Care Officer
26 years
21
Enrolled Nurse, HNC in Social Care with SVQ level III.
Assistant Manager – Residential home for Older people, Enrolled Nurse – Assessment Unit for Older people, Enrolled Nurse – general, surgical, medical wards and long stay units
Community Care Organiser
79
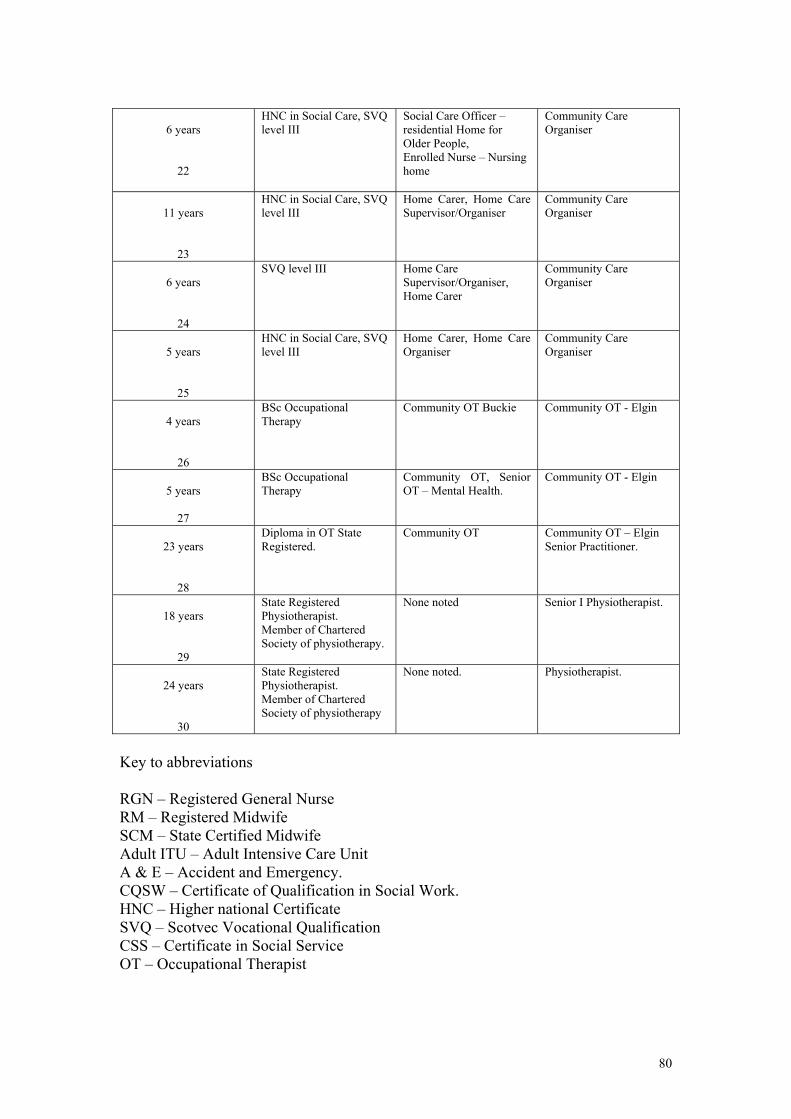
6 years
22
HNC in Social Care, SVQ level III
Social Care Officer – residential Home for Older People, Enrolled Nurse – Nursing home
Community Care Organiser
11 years
23
HNC in Social Care, SVQ level III
Home Carer, Home Care Supervisor/Organiser
Community Care Organiser
6 years
24
SVQ level III Home Care Supervisor/Organiser, Home Carer
Community Care Organiser
5 years
25
HNC in Social Care, SVQ level III
Home Carer, Home Care Organiser
Community Care Organiser
4 years
26
BSc Occupational Therapy
Community OT Buckie Community OT - Elgin
5 years
27
BSc Occupational Therapy
Community OT, Senior OT – Mental Health.
Community OT - Elgin
23 years
28
Diploma in OT State Registered.
Community OT Community OT – Elgin Senior Practitioner.
18 years
29
State Registered Physiotherapist. Member of Chartered Society of physiotherapy.
None noted Senior I Physiotherapist.
24 years
30
State Registered Physiotherapist. Member of Chartered Society of physiotherapy
None noted. Physiotherapist.
Key to abbreviations RGN – Registered General Nurse RM – Registered Midwife SCM – State Certified Midwife Adult ITU – Adult Intensive Care Unit A & E – Accident and Emergency. CQSW – Certificate of Qualification in Social Work. HNC – Higher national Certificate SVQ – Scotvec Vocational Qualification CSS – Certificate in Social Service OT – Occupational Therapist
80
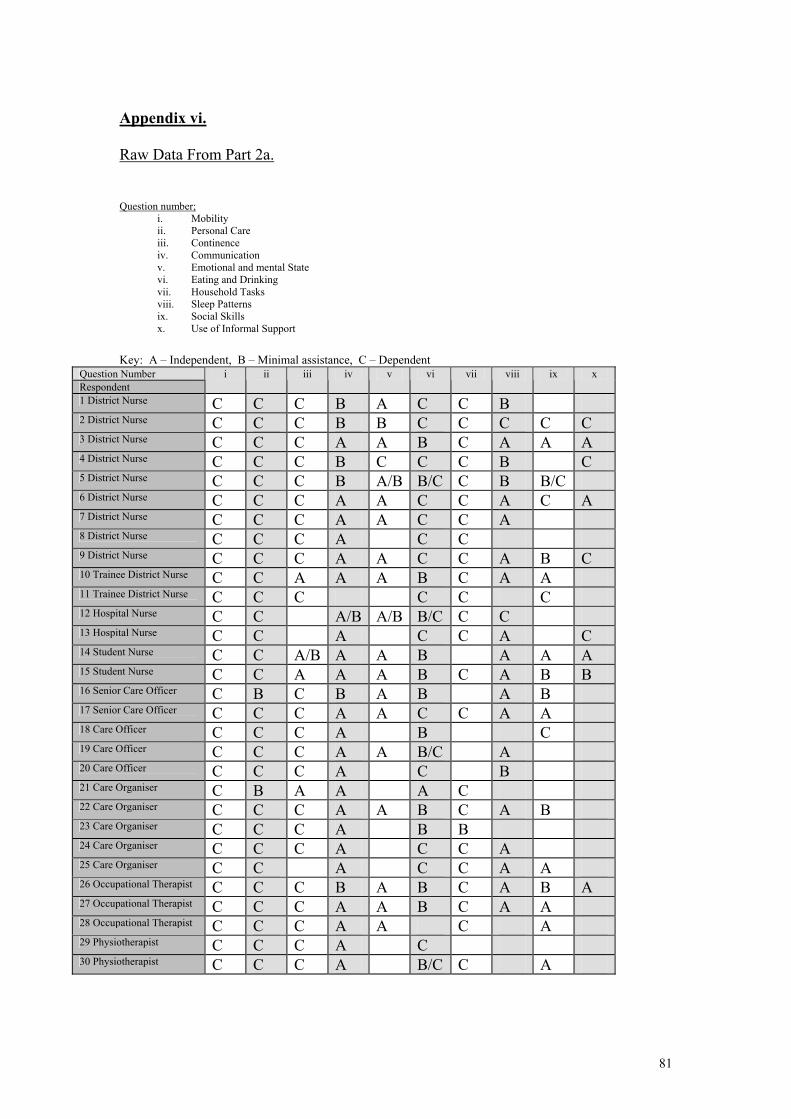
Appendix vi. Raw Data From Part 2a. Question number;
i. Mobility ii. Personal Care iii. Continence iv. Communication v. Emotional and mental State vi. Eating and Drinking vii. Household Tasks viii. Sleep Patterns ix. Social Skills x. Use of Informal Support
Key: A – Independent, B – Minimal assistance, C – Dependent
Question Number Respondent
i ii iii iv v vi vii viii ix x
1 District Nurse C C C B A C C B 2 District Nurse C C C B B C C C C C 3 District Nurse C C C A A B C A A A 4 District Nurse C C C B C C C B C 5 District Nurse C C C B A/B B/C C B B/C 6 District Nurse C C C A A C C A C A 7 District Nurse C C C A A C C A 8 District Nurse C C C A C C 9 District Nurse C C C A A C C A B C 10 Trainee District Nurse C C A A A B C A A 11 Trainee District Nurse C C C C C C 12 Hospital Nurse C C A/B A/B B/C C C 13 Hospital Nurse C C A C C A C 14 Student Nurse C C A/B A A B A A A 15 Student Nurse C C A A A B C A B B 16 Senior Care Officer C B C B A B A B 17 Senior Care Officer C C C A A C C A A 18 Care Officer C C C A B C 19 Care Officer C C C A A B/C A 20 Care Officer C C C A C B 21 Care Organiser C B A A A C 22 Care Organiser C C C A A B C A B 23 Care Organiser C C C A B B 24 Care Organiser C C C A C C A 25 Care Organiser C C A C C A A 26 Occupational Therapist C C C B A B C A B A 27 Occupational Therapist C C C A A B C A A 28 Occupational Therapist C C C A A C A 29 Physiotherapist C C C A C 30 Physiotherapist C C C A B/C C A
81
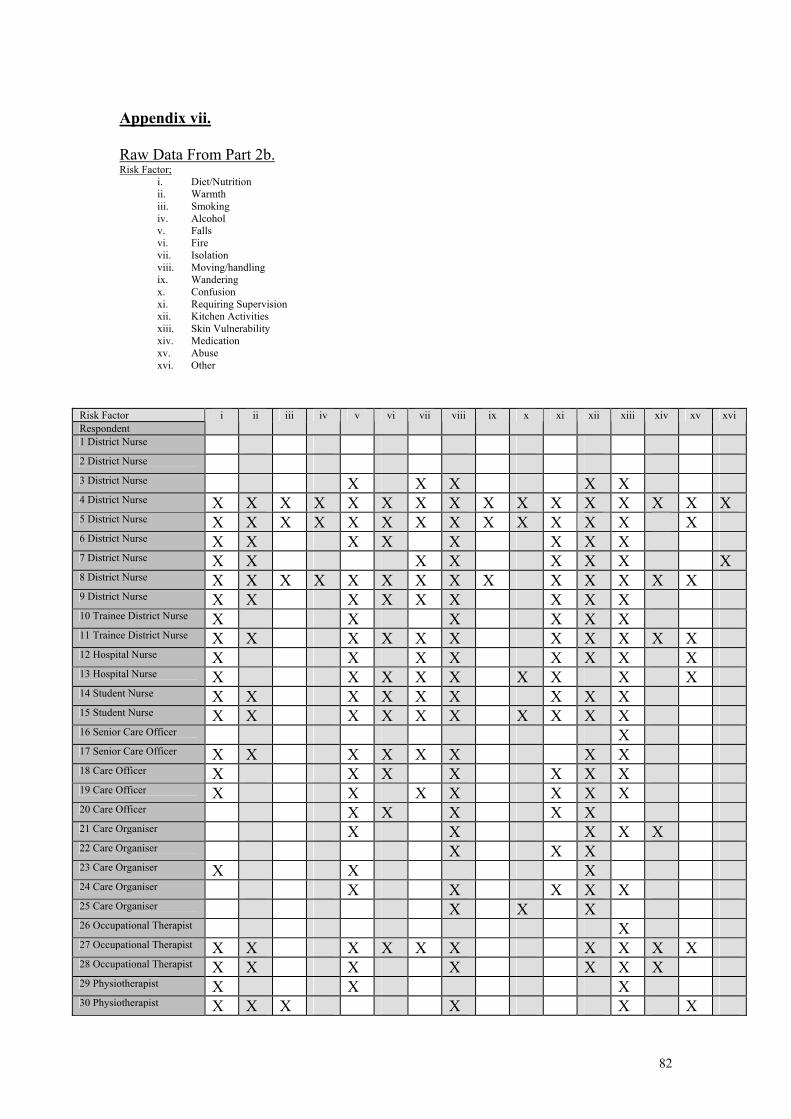
Appendix vii. Raw Data From Part 2b. Risk Factor;
i. Diet/Nutrition ii. Warmth iii. Smoking iv. Alcohol v. Falls vi. Fire vii. Isolation viii. Moving/handling ix. Wandering x. Confusion xi. Requiring Supervision xii. Kitchen Activities xiii. Skin Vulnerability xiv. Medication xv. Abuse xvi. Other
Risk Factor Respondent
i ii iii iv v vi vii viii ix x xi xii xiii xiv xv xvi
1 District Nurse 2 District Nurse 3 District Nurse X X X X X 4 District Nurse X X X X X X X X X X X X X X X X 5 District Nurse X X X X X X X X X X X X X X 6 District Nurse X X X X X X X X 7 District Nurse X X X X X X X X 8 District Nurse X X X X X X X X X X X X X X 9 District Nurse X X X X X X X X X 10 Trainee District Nurse X X X X X X 11 Trainee District Nurse X X X X X X X X X X X 12 Hospital Nurse X X X X X X X X 13 Hospital Nurse X X X X X X X X X 14 Student Nurse X X X X X X X X X 15 Student Nurse X X X X X X X X X X 16 Senior Care Officer X 17 Senior Care Officer X X X X X X X X 18 Care Officer X X X X X X X 19 Care Officer X X X X X X X 20 Care Officer X X X X X 21 Care Organiser X X X X X 22 Care Organiser X X X 23 Care Organiser X X X 24 Care Organiser X X X X X 25 Care Organiser X X X 26 Occupational Therapist X 27 Occupational Therapist X X X X X X X X X X 28 Occupational Therapist X X X X X X X 29 Physiotherapist X X X 30 Physiotherapist X X X X X X
X
82
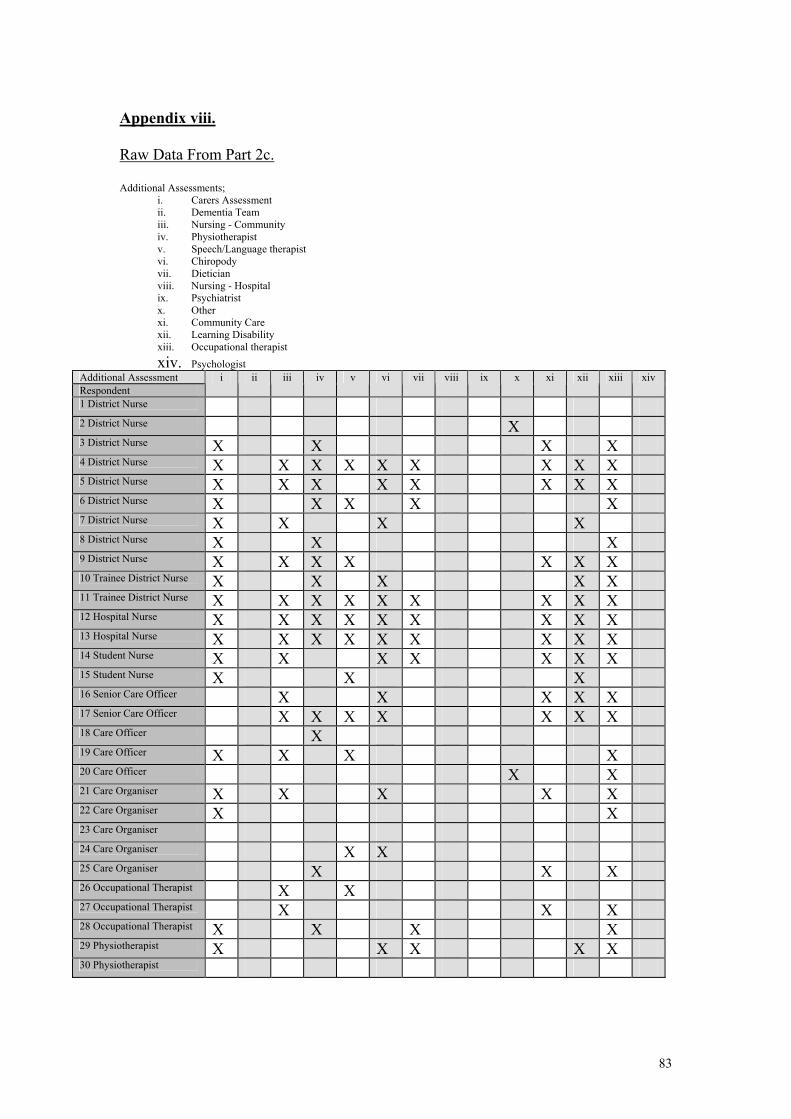
Appendix viii. Raw Data From Part 2c. Additional Assessments;
i. Carers Assessment ii. Dementia Team iii. Nursing - Community iv. Physiotherapist v. Speech/Language therapist vi. Chiropody vii. Dietician viii. Nursing - Hospital ix. Psychiatrist x. Other xi. Community Care xii. Learning Disability xiii. Occupational therapist xiv. Psychologist
Additional Assessment Respondent
i ii iii iv v vi vii viii ix x xi xii xiii xiv
1 District Nurse 2 District Nurse X 3 District Nurse X X X X 4 District Nurse X X X X X X X X X 5 District Nurse X X X X X X X X 6 District Nurse X X X X X 7 District Nurse X X X X 8 District Nurse X X X 9 District Nurse X X X X X X X 10 Trainee District Nurse X X X X X 11 Trainee District Nurse X X X X X X X X X 12 Hospital Nurse X X X X X X X X X 13 Hospital Nurse X X X X X X X X X 14 Student Nurse X X X X X X X 15 Student Nurse X X X 16 Senior Care Officer X X X X X 17 Senior Care Officer X X X X X X X 18 Care Officer X 19 Care Officer X X X X 20 Care Officer X X 21 Care Organiser X X X X X 22 Care Organiser X X 23 Care Organiser 24 Care Organiser X X 25 Care Organiser X X X 26 Occupational Therapist X X 27 Occupational Therapist X X X 28 Occupational Therapist X X X X 29 Physiotherapist X X X X X 30 Physiotherapist
83
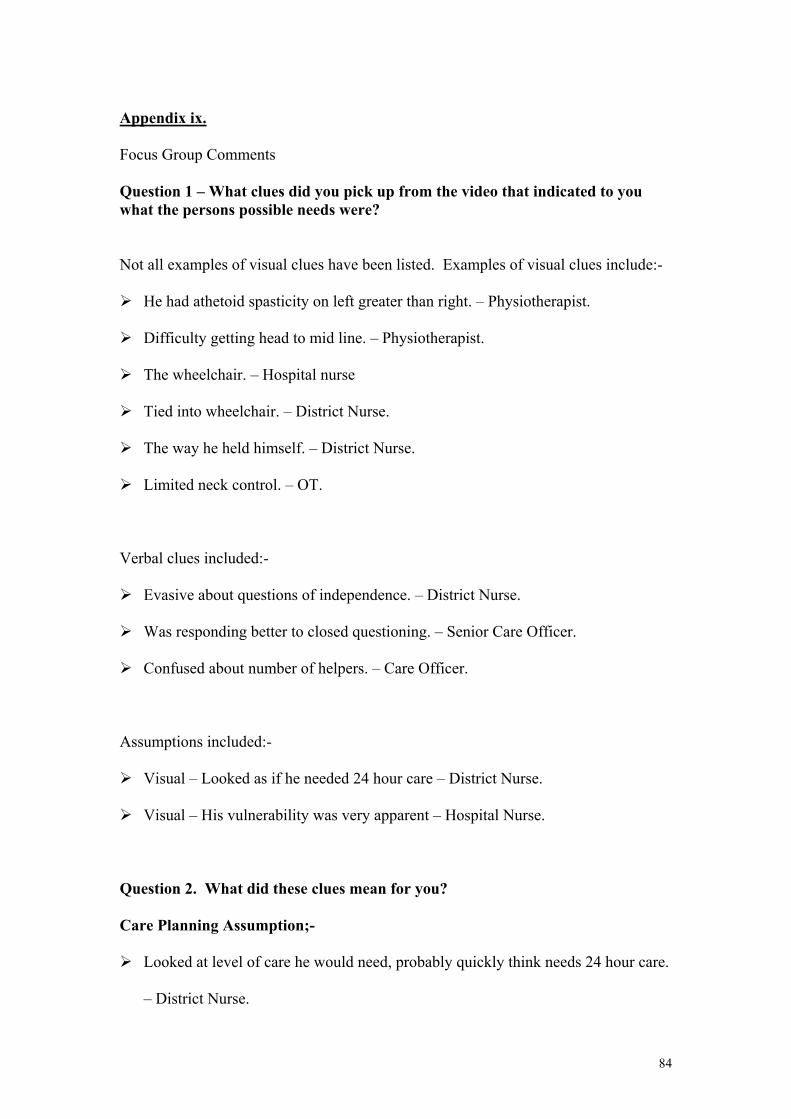
Appendix ix. Focus Group Comments
Question 1 – What clues did you pick up from the video that indicated to you what the persons possible needs were?
Not all examples of visual clues have been listed. Examples of visual clues include:-
He had athetoid spasticity on left greater than right. – Physiotherapist.
Difficulty getting head to mid line. – Physiotherapist.
The wheelchair. – Hospital nurse
Tied into wheelchair. – District Nurse.
The way he held himself. – District Nurse.
Limited neck control. – OT.
Verbal clues included:-
Evasive about questions of independence. – District Nurse.
Was responding better to closed questioning. – Senior Care Officer.
Confused about number of helpers. – Care Officer.
Assumptions included:-
Visual – Looked as if he needed 24 hour care – District Nurse.
Visual – His vulnerability was very apparent – Hospital Nurse.
Question 2. What did these clues mean for you?
Care Planning Assumption;-
Looked at level of care he would need, probably quickly think needs 24 hour care.
– District Nurse.
84
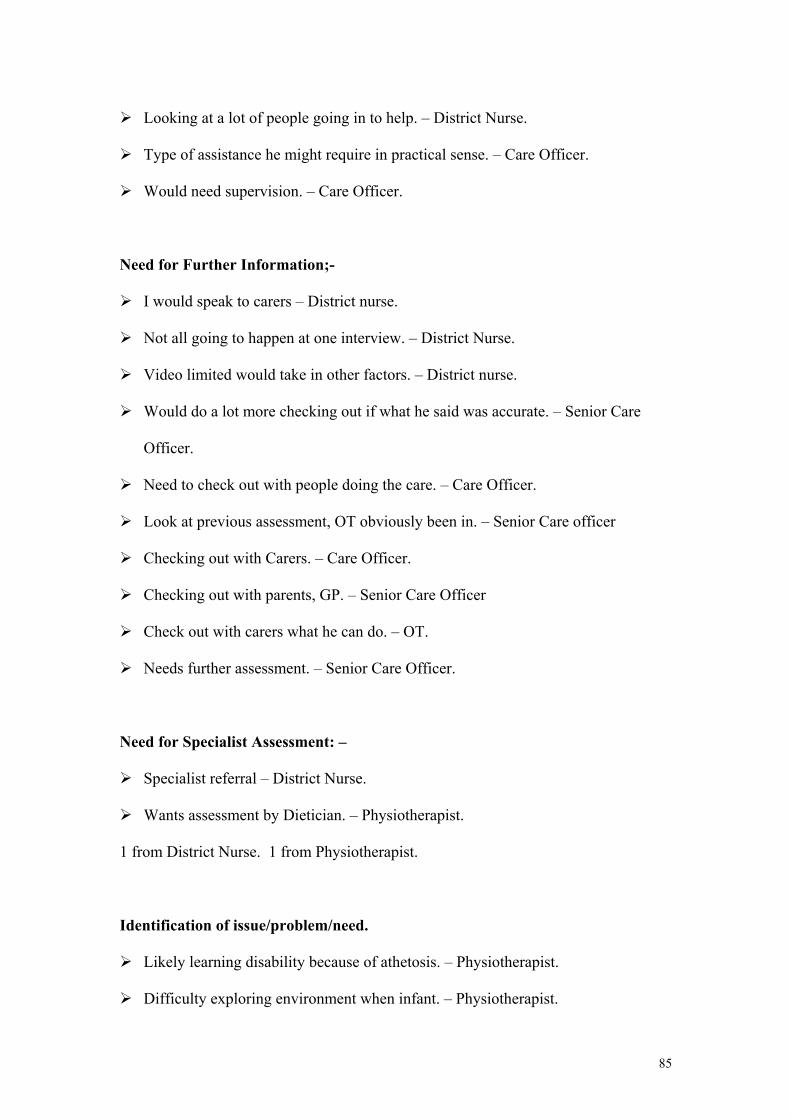
Looking at a lot of people going in to help. – District Nurse.
Type of assistance he might require in practical sense. – Care Officer.
Would need supervision. – Care Officer.
Need for Further Information;-
I would speak to carers – District nurse.
Not all going to happen at one interview. – District Nurse.
Video limited would take in other factors. – District nurse.
Would do a lot more checking out if what he said was accurate. – Senior Care
Officer.
Need to check out with people doing the care. – Care Officer.
Look at previous assessment, OT obviously been in. – Senior Care officer
Checking out with Carers. – Care Officer.
Checking out with parents, GP. – Senior Care Officer
Check out with carers what he can do. – OT.
Needs further assessment. – Senior Care Officer.
Need for Specialist Assessment: –
Specialist referral – District Nurse.
Wants assessment by Dietician. – Physiotherapist.
1 from District Nurse. 1 from Physiotherapist.
Identification of issue/problem/need.
Likely learning disability because of athetosis. – Physiotherapist.
Difficulty exploring environment when infant. – Physiotherapist.
85
Possible educational difficulties. – Physiotherapist.
Could see all sorts of problems – pressure sores, continence problems, feeding,
choking. – Hospital nurse.
He is disabled. – District Nurse.
Did he have a learning disability? Indicators were yes. Senior Care Officer.
Would need equipment. – OT.
Possible problems with skin care – pressure areas. – Physiotherapist.
Can he get to toilet? Can he use a bottle? – Physiotherapist.
Carers Need: –
How carers manage and protect themselves. – Physiotherapist.
Question 3, From your professional background, what knowledge or ideas did
you relate to these clues?
Activities of living model of assessment – Roper, Logan & Tierney. – 2 x District
Nurses.
Most social work training related to developing self awareness. – Senior Care Officer.
Would use a functional tool. – Physiotherapist.
Other statements made in response to this question but not pertaining to the
question.
Manual handling – obviously needs someone to help. – District nurse.
Co-ordination for chopping veg is doubtful. – District nurse.
Concentration possibly poor. – District nurse.
Difficult to assess emotions by looking at video he may throw a tantrum at any time. –
District nurse.
86
Never assessed anyone with cerebral palsy. – District nurse.
Use experience, similar assessments, rely on OT or others. – Care Officer.
Suspicion of cerebral palsy. – OT.
Know kinds of problems sufferer of cerebral palsy would have – look for these things.
– OT.
Physical problems quite obvious, difficulty assessing cognitive skills. – Care Officer.
Assessment of emotional state – if not able to communicate needs – danger of people
interpreting for him. – Senior Care Officer.
Question 6, Given all the information that you have, should this person be living
on his own in the community?
This was analysed by comment into:- affirmative; qualified affirmative; questioning
statement.
Qualified affirmative was further divided according to statements relating to i. Client
choice; ii. Care needs statement; iii. Finance.
Affirmative:
1 Health based and 5 social work based respondents gave an unqualified affirmative:-
1 District nurse; 3 Care Officers; 1 Care Organiser; 1 OT;
Qualified Affirmative:
7 health based and 3 social work based respondents gave qualified affirmatives
Qualified by:
i. Client choice:
2 health based and 2 social work based staff qualified re client choice:-
1 District Nurse; 1 Physiotherapist; 1 Senior Care Officer; 1 Care Organiser.
ii. Care needs statement:
87
6 health based and 1 social work based staff qualified re care needs
.In group home he would be OK, but not on his own. – District Nurse.
Independent with help – it is a possibility rather than institutional care. – District
Nurse.
Not without support he needs an intensive care package. – Hospital Nurse.
Protection from Certain people, he is very vulnerable. – Hospital Nurse.
Depends on the support he has got. As long as he has the professional support
that he needs. – District Nurse.
Providing services are there. – Care Officer.
With the right sort of back up I don’t see why not. – Physiotherapist.
iii. Finance.
1 health based and 2 social work based staff qualified re finance.
Depends on budget. – District Nurse.
As long as it’s not more than £300 per week. – Care Organiser.
He would be on ILF (Independent Living Fund). – Care Officer.
Questioning statement:
3 health based workers gave questioning statements.
Learning Disability and psychiatric needs and choice, it’s a huge problem.
District nurse.
Did he ever live before – would he be able to cope? – District Nurse.
Has he mental understanding to make the choice? – District Nurse.
88
REFERENCES
Baldwin M, 1995, Is assessment working? – Policy and practice in Care management,
Practice, vol. 8, no 4.
Barrett G. Hudson M. 1997, Changes in District Nursing Workload, Journal of
Community Nursing, 11(3).
Bauman Z., 1992, Intimations of Post-Modernity, Routledge, London.
Bergen A., Cowley S., Young K., Kavanagh A., 1996, An Investigation into the
Changing Educational Needs of Community Nurses with Regard to Needs
Assessment and Quality of Care in the Context of the NHS and Community Care Act,
1990. English National Board for Nursing, Midwifery and Health Visiting, London.
Binnie A., Titchen A., 1998, Patient Centred Nursing. An Action Research Study of
Practice Development in an Acute medical Unit. Report No. 18, Oxford: RCN
Institute.
Binnie A., Titchen A., 1999, Freedom To Practice The Development of Patient
Centred Practice, Butterworth Heinemann, Oxford.
Blanche R, 1999, Attitudes to Risk Taking in Community Multi-Disciplinary teams
Working With people Who Have Dementia. Robert Gordons University, School of
Applied Social Studies, Aberdeen.
Blaxter M, 1976, The Meaning of Disability, Heinemann, London
Bousfield C. 1997, A phenomenological investigation into the role of the clinical nurse
specialist, Journal of Advanced Nursing, 25.
Bower M, 1966, The will to manage. McGraw Hill, New York
89
Bradshaw, J. (1972) A taxonomy of social need. In Problems and Progress in Medical
Care: Essays on Current Research (ed. G. McLachlan) (7th series). Oxford University
Press. London.
Brandon D. Brandon A, 1988, Putting People First, A handbook on the Practical
Application of Ordinary Living Principles, Good Impressions Publishing, London.
Breakwell G.M., Hammond S., Fife-Schaw C., 1995, Research Methods in
Psychology, Sage Publications, London.
Buckley E.G., Runciman P.J., 1985, Health Assessment of the Elderly at Home.
University of Edinburgh, Edinburgh.
Butyrm Z. T. 1989, “Health Care and Social Work, What Kind of Relationship”, in
Social Work and Health Care, Jessica Kingsley, Bristol.
Caldock K, 1994, The new assessment: moving towards holism or new roads to
fragmentation? In Community Care: New Agendas and Challenges from the UK and
Overseas. (Challis D, Davies B, Traske K, eds.) Arena Ashgate, Aldershot.
Campbell A. V., 1984, Moderated Love: A Theology of Professional Care. SPCK,
London.
Challis D. J., Chesterman J. F., 1985, A system for monitoring social work activity
with the frail elderly. British Journal of Social Work. 15.
Cohen A, Eastman N, 1997, Needs assessment for mentally disordered offenders and
others requiring similar services. British Journal of Psychiatry, London. 171.
Cowley S, Bergen A, Young K, Kavanagh A, 2000. A taxonomy of needs
assessment, elicited from a multiple case study of community nursing education and
practice. Journal of Advanced Nursing, 31(1).
Davies B. Challis D, 1986 Matching Resources to Needs in Community Care, Gower,
Aldershot.
90
Department of the Environment, Transport and the Regions, 1999, Achieving Best
Value Through Competition, Benchmarking and Performance Networks.
Department of Health 1989a, Caring for people Cmnd. 849, HMSO, London.
Department of Health 1989b, Working for Patients Cmnd. 555, HMSO, London.
Department of Health 1990, Caring for People: Implementation Document-
Assessment & Case Management. HMSO, London.
Department of Health, Social Services Inspectorate, Scottish Office, Social Work
Services Group, 1991, Care management and Assessment, Practitioners’ Guide.
HMSO, London.
Department of Health, 1993, Monitoring and Development: Assessment Special
Study. HMSO, London.
Department of Health, 1997, Better Services for Vulnerable People. Department of
Health, London
Department of Health, 2000, NHS bodies and Local Authorities Partnership
Arrangement Regulations 2000, HMSO, London.
Department of Health, 2001, The Single Assessment Process, HMSO, London.
Department of Health and Social Services Inspectorate, 1993, Regional Health
Authority Community Care Monitoring national summary. HMSO, London.
Dewing J, 1991, Primary nursing – implications for the nurse. In, Primary Nursing in
Perspective, Ersser S., Tutton E (eds.) Scutari Press, London.
Ellis K. 1993, Squaring the Circle: User and Carer Participation in Needs
Assessment, Joseph Rowntree Foundation, York.
Ellis K, Davis A, Rummery K, 1999, Needs Assessment, Street-level Bureaucracy
and the New Community Care. Social Policy & Administration, 33 (3).
91
Fretwell J.E., 1980 Hospital Ward Routine – Friend or foe? Journal of Advanced
Nursing, 5, 625-636.
Gibbs I, Bradshaw J, 1988, Dependency and its Relationship to the Assessment of
Care Needs of Elderly People. British Association of Social Workers, University of
York, York.
Giller H, Morris A, 1981, What type of case is this? Social workers’ decisions about
children who offend. In Adler M, Asquith S, 1981, Discretion and Power,
Heinemann, London.
Hall A.S. 1974, The Point of Entry: A Study of Client Reception in the Social
Services, George Allen and Unwin, London.
Harrison R, 1975, The 1975 Annual handbook for Group Facilitators, University
Associates Publishers Inc., USA.
Haughey A, 1995, Contemporary District Nursing Practice. In Sines D, 1995,
Community Health Care Nursing, Blackwell Science, Oxford.
Hockey L, 1966, Feeling the Pulse. Queens Institute of District Nursing, Edinburgh.
Hockey L, 1968, Care in the Balance. Queens Institute of District Nursing, Edinburgh.
Hudson R., 1997, Caring Sharing, Community Care Magazine, 25/9/97.
Hughes B, 1995, Older People and Community Care: Critical Theory and Practice,
Open University Press, Buckingham-Laurent C, 1993, Out in Force, Nursing Times,
89(3)
Katz D., Kahn R.L. 1996, The social psychology of organisations, John Wiley, New
York.
Kaye L.W., 1987, Assessing the Community Care Needs of the Functionally
Impaired Elderly: The Gerontological Worker’s Perspective, Home Health Care
Services Quarterly, 8(4).
92
Lawton S, Cantrell J, Harris J. eds., 2000, District Nursing Providing Care in a
Supportive Context, Churchill Livingstone, Edinburgh.
Leat D, Perkins E, 1998, Juggling and Dealing: The Creative Work of Care Package
Purchasing, Social Policy and Administration, Vol. 32,(2).
Lewis J, Bernstock P, Bovell V, 1995, The community Care Changes: unresolved
tensions in policy and issues in implementation. Journal of social Policy, 24.
Lightfoot J. 1995, Identifying needs and setting priorities. Issues of theory, policy
and practice. Health and Social Care in the Community 3, 105-114.
Lipsky M. 1980, Street-Level Bureaucracy, Russell Sage, New York.
MacDonald C. Myers F. 1995, Assessment and Care Management: The Practitioner
Speaks, Community Care in Scotland Discussion Paper 5, University of Stirling, Stirling.
Manthey M, 1980, The Practice of Primary Nursing, Blackwell Scientific publications,
Oxford
Maslow, A. H. (1954) Motivation and Personality. Harper & Row, New York.
Mayer J.E., Timms N. 1970, The Client Speaks: Working Class Impressions of
Casework, Routledge and Keegan Paul, London.
McWalter G, Toner H, Corser A, et al (1994) Needs and needs assessment: their
components and definitions with reference to dementia. Health and Social Care in
the Community, Vol. 2.
Means R and Smith R., 1994, Community Care Policy and Practice, Macmillan, London.
Millward L, 1995, Focus Groups, in Research Methods in Psychology, 1995, in
Breakwell G.M., Hammond S, Fife-Schaw C, eds., Sage Publications, London.
Morris J. 1993, Community Care or Independent Living? Joseph Rowntree, York.
Nolan M, Caldock K, 1996, Assessment: identifying the barriers to good practice.
Health and Social Care in the Community, 4(2).
93
O’Brian J, Mount B, O’Brian C, 1989, Framework For Accomplishment, Responsive
Systems Associates, Georgia.
Oliver M, 1989, Disability and Dependency: A Creation of Industrial Societies? in
Barton L (editor), 1989, Disability and Dependency, The Falmer Press, London.
Ovretveit J, 1997, Inter-professional working for Health and Social Care, Mathias P.
Thomson (eds.), Macmillan, London.
Parry-Jones B, Caldock K, 1995, Assessment and practice after reforms: a view from
the workshops, a report of the CSPRD Second annual Conference. CSPRD
Newsletter. CSPRD, University of Wales, Bangor.
Peet S. M., Castleden C. M., Potter J. F., Jagger C. 1994, the outcome of a medical
examination for applicants to Leicestershire homes for older people. Age and
Ageing. 23.
Petch A, Stalker K, Taylor C, Taylor J, 1994, Assessment and Care Management
Pilot Projects in Scotland: An Overview. University of Stirling, Social Work
Research Centre, Stirling.
Plummer S, 2000, Management of Change, in Lawton S, Cantrell J, Harris J. eds.,
2000, District Nursing Providing Care in a Supportive Context, Churchill
Livingstone, Edinburgh.
Rees S, 1978, Social Work Face to Face, Edward Arnold, London.
Reynolds T, Thornicroft G, Abas M, Woods B, Hoe J, Leese M, Orrell M, 2000,
Camberwell Assessment of Need for the Elderly (CANE): Development, validity and
reliability. The British Journal of Psychiatry, London. 176.
Robinson J, Elkan R, 1996, Health Needs Assessment, Theory and Practice,
Churchill Livingstone, London.
94
Ross F, 1987, District Nursing. In Recent Advances in Nursing (15), Community
Nursing, Littlewood J (ed.). Churchill Livingstone, Edinburgh.
Rubenstein L.Z, Schairer C, Wieland G.D, Kane R, 1984, Systematic Biases in
functional Status Assessment of Elderly Adults: Effects of Different Data Sources.
Journal of Gerontology, 39(6).
Runciman P, 1989, Health assessment of the elderly at home: the case for shared
learning. Journal of Advanced Nursing, 14.
Satyamurti C, 1981, Occupational Survival, Blackwell, Oxford.
Scottish Executive Health Department, 2000, Community Care: A Joint Future, The
Stationery Office, Edinburgh.
Scottish Executive Health Department, 2001, Report of the Chief Nursing Officer for
Scotland’s Group on Free Nursing Care, The Stationery Office, Edinburgh.
Secretary of State for Health, 1998, Modern Local Government: In touch with the
People, HMSO, London.
Secretary of State for Health, 2000, The NHS Plan, HMSO, London.
Secretary of State for Scotland, 1997, Designed to Care, Renewing the National
Health Service in Scotland. The Stationery Office, Edinburgh.
Seebhom Committee 1968, Report of the Committee on Local Authority and Allied
Personas Social Services, Cmnd 3703, HMSO, London.
Skeet M.H., 1970, Home From Hospital. Dan Mason Research Committee. In Baly
M, 1973, Nursing and Social change. Heinemann, London.
Slade M, 1996, Assessing the needs of the severely mentally ill: cultural and
professional differences. International Journal of Social Psychiatry. 42(1).
95
Slade M, Phelan M, Thornicroft G, 1998, A comparison of needs assessed by staff
and by an epidemiologically representative sample of patients with psychosis.
Section of Community Psychiatry, Institute of Psychiatry, London.
Smith G, 1980, Social Need, Policy, Practice and Research, Routledge and Kegan Paul,
London.
Social Services Inspectorate 1991, Care Management and Assessment: Practitioners
Guide. HMSO, London.
Stevens, A. & Gabbay, J. (1991) Needs assessment needs assessment. Health Trends, 23,
Sweet H, Ferguson R, 2000, District Nursing History. In District Nursing Providing
Care in a Supportive Context, 2000, Lawton S, Cantrell J, Harris J. (eds.). Churchill
Livingstone, Edinburgh.
Taylor C, 1993, An evaluation of a multi-disciplinary pilot project ‘Assessment of
Social Care Needs’ for elderly people in Borders Region. Social Work Research
Centre, University of Stirling, Stirling.
Timmins A, 1996, Dilemmas of Discharge: the case of district nursing. Department
of Nursing and Midwifery Studies, University of Nottingham, Nottingham.
Twigg J. Atkin K., 1994, Carers of elderly people: Models for analysis, in Janieson
A. Illsey R (eds.) Contrasting European Policies for the Care of Older people, Gower,
Aldershot.
UKCC, 1992b, The Code of Professional Conduct. UKCC, London.
UKCC, 1994, The Future of Professional Practice: The Council’s Standards for
Education and Practice Following Registration, UKCC, London.
Unsworth J. 2000, Developing roles which enhance patient care, in Lawton S,
Cantrell J, Harris J. (eds.), 2000, District Nursing Providing Care in a Supportive
Context, Churchill Livingstone, Edinburgh.
96

Wolfensberger W, 1972, The Principles of Normalisation in Human Services, Toronto
National Institute on mental Retardation, Toronto.
97
BIBLIOGRAPHY
Baldwin M, 1995, Is assessment working? – Policy and practice in Care management,
Practice, vol. 8, no 4.
Barrett G. Hudson M. 1997, Changes in District Nursing Workload, Journal of
Community Nursing, 11(3).
Bauman Z., 1992, Intimations of Post-Modernity, Routledge, London.
Bergen A., Cowley S., Young K., Kavanagh A., 1996, An Investigation into the
Changing Educational Needs of Community Nurses with Regard to Needs
Assessment and Quality of Care in the Context of the NHS and Community Care Act,
1990. English National Board for Nursing, Midwifery and Health Visiting, London.
Beyea S.C. Nicoll L.H., 1999, A survey does not equal research, AORN Journal,
69(1).
Binnie A., Titchen A., 1998, Patient Centred Nursing. An Action Research Study of
Practice Development in an Acute medical Unit. Report No. 18, Oxford: RCN
Institute.
Binnie A., Titchen A., 1999, Freedom To Practice The Development of Patient
Centred Practice, Butterworth Heinemann, Oxford.
Blanche R, 1999, Attitudes to Risk Taking in Community Multi-Disciplinary teams
Working With people Who Have Dementia. Robert Gordons University, School of
Applied Social Studies, Aberdeen.
Blaxter M, 1976, The Meaning of Disability, Heinemann, London
Bousfield C. 1997, A phenomenological investigation into the role of the clinical nurse
specialist, Journal of Advanced Nursing, 25.
Bower M, 1966, The will to manage. McGraw Hill, New York
98
Bradshaw, J. (1972) A taxonomy of social need. In Problems and Progress in Medical
Care: Essays on Current Research (ed. G. McLachlan) (7th series). Oxford University
Press. London.
Brandon D. Brandon A, 1988, Putting People First, A handbook on the Practical
Application of Ordinary Living Principles, Good Impressions Publishing, London.
Breakwell G.M., Hammond S., Fife-Schaw C., 1995, Research Methods in
Psychology, Sage Publications, London.
Buckley E.G., Runciman P.J., 1985, Health Assessment of the Elderly at Home.
University of Edinburgh, Edinburgh.
Buglass D, 1993, Assessment and Care Management: A Scottish Overview of
Impending Change, Community Care in Scotland Discussion Paper No 2, University
of Stirling, Stirling.
Butyrm Z. T. 1989, “Health Care and Social Work, What Kind of Relationship”, in
Social Work and Health Care, Jessica Kingsley, Bristol.
Caldock K, 1994, Policy and Practice: fundamental contradictions in the
conceptualisation of community care for elderly people? Health and Social Care in
the Community, 2(3).
Caldock K, 1994, The new assessment: moving towards holism or new roads to
fragmentation? In Community Care: New Agendas and Challenges from the UK and
Overseas. (Challis D, Davies B, Traske K, eds.) Arena Ashgate, Aldershot.
Caldwell P, 1996, Getting in touch Ways of working with people with severe learning
disabilities and extensive support needs, Joseph Rowntree Foundation, Pavilion
Publications, Brighton.
Campbell A. V., 1984, Moderated Love: A Theology of Professional Care. SPCK,
London.
99
Challis D. J., Chesterman J. F., 1985, A system for monitoring social work activity
with the frail elderly. British Journal of Social Work. 15.
Cohen A, Eastman N, 1997, Needs assessment for mentally disordered offenders and
others requiring similar services. British Journal of Psychiatry, London. 171.
Cowley S, Bergen A, Young K, Kavanagh A, 2000. A taxonomy of needs
assessment, elicited from a multiple case study of community nursing education and
practice. Journal of Advanced Nursing, 31(1).
Davies B. Challis D, 1986 Matching Resources to Needs in Community Care, Gower,
Aldershot.
Davidson H. Capewell S. Macnaughton J. Murray S. Hanlon P. McEwen J., 1999,
Community-oriented medical education in Glasgow: developing a community
diagnosis exercise, Medical Education, 33.
Department of the Environment, Transport and the Regions, 1999, Achieving Best
Value Through Competition, Benchmarking and Performance Networks.
Department of Health 1989a, Caring for people Cmnd. 849, HMSO, London.
Department of Health 1989b, Working for Patients Cmnd. 555, HMSO, London.
Department of Health 1990, Caring for People: Implementation Document-
Assessment & Case Management. HMSO, London.
Department of Health, Social Services Inspectorate, Scottish Office, Social Work
Services Group, 1991, Care management and Assessment, Practitioners’ Guide.
HMSO, London.
Department of Health, Social Services Inspectorate, Scottish Office, Social Work
Services Group, 1991, Care management and Assessment, Managers’ Guide.
HMSO, London.
100
Department of Health, 1993, Monitoring and Development: Assessment Special
Study. HMSO, London.
Department of Health, 1997, Better Services for Vulnerable People. Department of
Health, CL(97)24, London
Department of Health, 2000, NHS bodies and Local Authorities Partnership
Arrangement Regulations 2000, HMSO, London.
Department of Health, 2000, The NHS Plan the Government’s Response to the Royal
Commission on Long Term Care, HMSO, London.
Department of Health, 2001, Older People, National Service Framework for Older
People, Department of Health, London.
Department of Health, 2001, The Single Assessment Process, HMSO, London.
Department of Health and Social Services Inspectorate, 1993, Regional Health
Authority Community Care Monitoring national summary. HMSO, London.
Dewing J, 1991, Primary nursing – implications for the nurse. In, Primary Nursing in
Perspective, Ersser S., Tutton E (eds.) Scutari Press, London.
Ellis K. 1993, Squaring the Circle: User and Carer Participation in Needs
Assessment, Joseph Rowntree Foundation, York.
Ellis K, Davis A, Rummery K, 1999, Needs Assessment, Street-level Bureaucracy
and the New Community Care. Social Policy & Administration, 33 (3).
Finlay L, 2000, in Brechin, Brown, Eby, Critical Practice in Health and Social Care,
Sage, London.
Fretwell J.E., 1980 Hospital Ward Routine – Friend or foe? Journal of Advanced
Nursing, 5, 625-636.
101
Gibbs I, Bradshaw J, 1988, Dependency and its Relationship to the Assessment of
Care Needs of Elderly People. British Association of Social Workers, University of
York, York.
Giller H, Morris A, 1981, What type of case is this? Social workers’ decisions about
children who offend. In Adler M, Asquith S, 1981, Discretion and Power,
Heinemann, London.
Hall A.S. 1974, The Point of Entry: A Study of Client Reception in the Social
Services, George Allen and Unwin, London.
Harding K. Baldwin S. Baser C, 1987, Towards Multi-level Needs Assessment,
Behavioural Psychotherapy, 15.
Harrison R, 1975, The 1975 Annual handbook for Group Facilitators, University
Associates Publishers Inc., USA.
Haughey A, 1995, Contemporary District Nursing Practice. In Sines D, 1995,
Community Health Care Nursing, Blackwell Science, Oxford.
Hicks C. Hennesey D., 1998, A triangulation approach to the identification of acute
sector nurses’ training needs for formal nurse practitioner status, Journal of Advanced
Nursing, 27(1).
Hockey L, 1966, Feeling the Pulse. Queens Institute of District Nursing, Edinburgh.
Hockey L, 1968, Care in the Balance. Queens Institute of District Nursing, Edinburgh.
Hudson R., 1997, Caring Sharing, Community Care Magazine, 25/9/97.
Hughes B, 1995, Older People and Community Care: Critical Theory and Practice,
Open University Press, Buckingham.Laurent C, 1993, Out in Force, Nursing Times,
89(3)
Katz D., Kahn R.L. 1996, The social psychology of organisations, John Wiley, New
York.
102
Kaye L.W., 1987, Assessing the Community Care Needs of the Functionally
Impaired Elderly: The Gerontological Worker’s Perspective, Home Health Care
Services Quarterly, 8(4).
Kennerley T, 1992, Professional values in Health Care, Health Services Management,
88(3).
Laing B, 1995, Discharge Planning A Management Challenge, Social Care:
Perspectives & Practice Critical Studies, University of Warwick, Coventry.
Lawton S, Cantrell J, Harris J. eds., 2000, District Nursing Providing Care in a
Supportive Context, Churchill Livingstone, Edinburgh.
Leat D, Perkins E, 1998, Juggling and Dealing: The Creative Work of Care Package
Purchasing, Social Policy and Administration, Vol. 32,(2).
Lewis J, Bernstock P, Bovell V, 1995, The community Care Changes: unresolved
tensions in policy and issues in implementation. Journal of social Policy, 24.
Lewis J, Bernstock P, Bovell V, Wookey F, 1997, Implementing Care Management:
Issues in Relation to the New community Care, British journal of Social Work, 27.
Lightfoot J. 1995, Identifying needs and setting priorities. Issues of theory, policy
and practice. Health and Social Care in the Community 3, 105-114.
Lipsky M. 1980, Street-Level Bureaucracy, Russell Sage, New York.
MacDonald C. Myers F. 1995, Assessment and Care Management: The Practitioner
Speaks, Community Care in Scotland Discussion Paper 5, University of Stirling, Stirling.
Macdonald G, Macdonald K, 1995, Ethical issues in social work research, in Social Work,
Hugman R., Smith D. (eds.), Routledge London.
Manthey M, 1980, The Practice of Primary Nursing, Blackwell Scientific publications,
Oxford
Maslow, A. H. (1954) Motivation and Personality. Harper & Row, New York.
103
Mayer J.E., Timms N. 1970, The Client Speaks: Working Class Impressions of
Casework, Routledge and Keegan Paul, London.
McWalter G, Toner H, Corser A, et al (1994) Needs and needs assessment: their
components and definitions with reference to dementia. Health and Social Care in
the Community, Vol. 2.
Means R and Smith R., 1994, Community Care Policy and Practice, Macmillan, London.
Millward L, 1995, Focus Groups, in Research Methods in Psychology, 1995, in
Breakwell G.M., Hammond S, Fife-Schaw C, eds., Sage Publications, London.
Morris J. 1993, Community Care or Independent Living? Joseph Rowntree, York.
Morrow-Howell N, Proctor E.K., Dore P, 1998, Adequacy of Care: the Concept and
its Measurement, Research on Social Work Practice, 8(1).
Nazarko L, 1997, Educating Elsie, Nursing times, 93(43).
Neill J, 1989, Assessing Elderly People For Residential Care: A Practical Guide,
National Institute for Social Work Research Unit, London.
Nolan M, Grant G, Caldock K, Keady J, 1994, A framework for assessing the needs
of family carers: a multi-disciplinary guide, BASE Publications, Bangor.
Nolan M, Caldock K, 1996, Assessment: identifying the barriers to good practice.
Health and Social Care in the Community, 4(2).
O’Brian J, Mount B, O’Brian C, 1989, Framework For Accomplishment, Responsive
Systems Associates, Georgia.
Oliver M, 1989, Disability and Dependency: A Creation of Industrial Societies? in
Barton L (editor), 1989, Disability and Dependency, The Falmer Press, London.
Olover M, 1990, the Politics of Disablement, Palgrave publishers, Basingstoke.
Ovretveit J, 1997, Inter-professional working for Health and Social Care, Mathias P.
Thomson (eds.), Macmillan, London.
104
Parry-Jones B, Caldock K, 1995, Assessment and practice after reforms: a view from
the workshops, a report of the CSPRD Second annual Conference. CSPRD
Newsletter. CSPRD, University of Wales, Bangor.
Peet S. M., Castleden C. M., Potter J. F., Jagger C. 1994, the outcome of a medical
examination for applicants to Leicestershire homes for older people. Age and
Ageing. 23.
Petch A, Stalker K, Taylor C, Taylor J, 1994, Assessment and Care Management
Pilot Projects in Scotland: An Overview. University of Stirling, Social Work
Research Centre, Stirling.
Plummer S, 2000, Management of Change, in Lawton S, Cantrell J, Harris J. eds.,
2000, District Nursing Providing Care in a Supportive Context, Churchill
Livingstone, Edinburgh.
Rees S, 1978, Social Work Face to Face, Edward Arnold, London.
Reynolds T, Thornicroft G, Abas M, Woods B, Hoe J, Leese M, Orrell M, 2000,
Camberwell Assessment of Need for the Elderly (CANE): Development, validity and
reliability. The British Journal of Psychiatry, London. 176.
Robinson J, Elkan R, 1996, Health Needs Assessment, Theory and Practice,
Churchill Livingstone, London.
Ross F, 1987, District Nursing. In Recent Advances in Nursing (15), Community
Nursing, Littlewood J (ed). Churchill Livingstone, Edinburgh.
Rubenstein L.Z, Schairer C, Wieland G.D, Kane R, 1984, Systematic Biases in
functional Status Assessment of Elderly Adults: Effects of Different Data Sources.
Journal of Gerontology, 39(6).
Runciman P, 1989, Health assessment of the elderly at home: the case for shared
learning. Journal of Advanced Nursing, 14.
105
Satyamurti C, 1981, Occupational Survival, Blackwell, Oxford.
Scottish Executive Health Department, 2000, Community Care: A Joint Future, The
Stationery Office, Edinburgh.
Scottish Executive Health Department, 2001, Report of the Chief Nursing Officer for
Scotland’s Group on Free Nursing Care, The Stationery Office, Edinburgh.
Scottish Executive Health Department, 2001, Progress on Implementing The Joint
Future Group’s Recommendations. Scottish Executive, Edinburgh.
Secretary of State for Health, 1998, Modern Local Government: In touch with the
People, HMSO, London.
Secretary of State for Health, 2000, The NHS Plan, HMSO, London.
Secretary of State for Scotland, 1997, Designed to Care, Renewing the National
Health Service in Scotland. The Stationery Office, Edinburgh.
Seebhom Committee 1968, Report of the Committee on Local Authority and Allied
Personas Social Services, Cmnd 3703, HMSO, London.
Sim A. Milner J. Love J. Lishman J., 1998, Definitions of need: can disabled people
and care professionals agree? Disability & Society, 13(1).
Sines D,1995, Community Health Care Nursing, Blackwell Science, Oxford.
Skeet M.H., 1970, Home From Hospital. Dan Mason Research Committee. In Baly
M, 1973, Nursing and Social change. Heinemann, London.
Slade M, 1996, Assessing the needs of the severely mentally ill: cultural and
professional differences. International Journal of Social Psychiatry. 42(1).
Slade M, Phelan M, Thornicroft G, 1998, A comparison of needs assessed by staff
and by an epidemiologically representative sample of patients with psychosis.
Section of Community Psychiatry, Institute of Psychiatry, London.
106
Smith G, 1980, Social Need, Policy, Practice and Research, Routledge and Kegan Paul,
London.
Social Work Services Inspectorate 1991, Care Management and Assessment:
Practitioners Guide. HMSO, London.
Social Work Services Inspectorate, 1994, Community Care Assessment and Care
Management Progress to Date, HMSO, London.
Stevens, A. & Gabbay, J. (1991) Needs assessment, Health Trends, 23.
Stevenson J, 1999, Comprehensive Assessment of Older People, King’s Fund
Rehabilitation Programme Developing Rehabilitation Opportunities For Older People,
Briefing Paper 2.
Stewart K, Challis D, Carpenter I, Dickinson E, 1999, Assessment approaches for Older
People Receiving Social Care: Content And Coverage, International Journal of Geriatric
Psychiatry, 14.
Sweet H, Ferguson R, 2000, District Nursing History. In District Nursing Providing
Care in a Supportive Context, 2000, Lawton S, Cantrell J, Harris J. (eds.). Churchill
Livingstone, Edinburgh.
Taylor C, 1993, An evaluation of a multi-disciplinary pilot project ‘Assessment of
Social Care Needs’ for elderly people in Borders Region. Social Work Research
Centre, University of Stirling, Stirling.
Timmins A, 1996, Dilemmas of Discharge: the case of district nursing. Department
of Nursing and Midwifery Studies, University of Nottingham, Nottingham.
The Scottish Office, 1993, Process and Preference: Assessment of Older People For
Institutional Care, Central research Unit Papers, Edinburgh.
107
Toner H.L., Keith D., Corser A., Turvey T., 1996, Assessing Continuing Care Needs:
Findings from the Fife Healthcare Assessment for Placement Project for Elderly
People, Health Bulletin 54 (2).
Twigg J. Atkin K., 1994, Carers of elderly people: Models for analysis, in Janieson
A. Illsey R (eds.) Contrasting European Policies for the Care of Older people, Gower,
Aldershot.
UKCC, 1992b, The Code of Professional Conduct. UKCC, London.
UKCC, 1994, The Future of Professional Practice: The Council’s Standards for
Education and Practice Following Registration, UKCC, London.
Unsworth J. 2000, Developing roles which enhance patient care, in Lawton S,
Cantrell J, Harris J. (eds.), 2000, District Nursing Providing Care in a Supportive
Context, Churchill Livingstone, Edinburgh.
Wolfensberger W, 1972, The Principles of Normalisation in Human Services, Toronto
National Institute on mental Retardation, Toronto.
108


















