Sham Berger

of 6
-
Upload
namkay-tenzyn -
Category
Documents
-
view
217 -
download
0
Transcript of Sham Berger
-
7/27/2019 Sham Berger
1/6
Introduction
Radiofrequency ablation (RFA) to treat tumors inadults has been widely reported [1]. With the exceptionof osteoid osteomas, there have been few reports inwhich RFA has been used to treat tumors in children [2,
3]. To our knowledge, there are no reports of RFA totreat pediatric renal tumors. In this case, RFA wasperformed to treat a progressive renal tumor that wasresistant to chemotherapy in a solitary kidney in a 5-year-old girl. This report details the case and relevanttechnical issues for performing RFA in children.
Stephen D. BrownEric vanSonnenbergPaul R. MorrisonLisa DillerRobert C. Shamberger
CT-guided radiofrequency ablationof pediatric Wilms tumor in a solitary kidney
Received: 27 October 2004Revised: 20 April 2005Accepted: 22 April 2005Published online: 1 June 2005
Springer-Verlag 2005
Abstract Although recent results ofpercutaneous imaging-guided radio-frequency ablation (RFA) of varioustumors in adults are promising,RFA of tumors in children has beenperformed in only a small number ofcases. We describe the treatment ofWilms tumor in a solitary kidney ina 5-year-old girl using percutaneousCT-guided RFA. The procedureprovided short-term palliation inthis child for whom partial or totalnephrectomy carried high risk andlow likelihood of success. Althoughit might only be useful ultimately asa temporizing measure, oncologistsand surgeons might wish to considerRFA in children who would other-wise require dialysis and renaltransplantation or who are poorsurgical candidates. Various specifictechnical issues differentiate pediat-ric from adult tumor ablation,including the amount of intra-abdominal fat, need for smallergrounding pads, and potential sys-temic effects of tissue heating.
Keywords Kidney neoplasms Radiofrequency ablation CT guidance Child
Pediatr Radiol (2005) 35: 923928DOI 10.1007/s00247-005-1510-y T E C H N I C A L I N N O V A T I O N
S. D. Brown (&)Department of Radiology,Childrens Hospital, 300 Longwood Ave.,Boston, MA 02115, USAE-mail:[email protected].: +1-617-3558259Fax: +1-617-7300573
E. vanSonnenberg P. R. MorrisonDepartments of Radiology, Dana FarberCancer Institute and Brigham andWomens Hospital, Boston, MA 02115,USA
L. DillerDepartments of Pediatric Oncology andMedicine, Dana Farber Cancer Instituteand Childrens Hospital, Boston, MA02115, USA
R. C. ShambergerDepartment of Surgery,Childrens Hospital, Boston, MA 02115,USA
Present address: E. vanSonnenbergDepartment of Radiology, St. JosephsHospital and Medical Center, Phoenix,AZ 85013, USA
-
7/27/2019 Sham Berger
2/6
Description
The patient is a developmentally delayed 5-year-old girlwith partial trisomy 1q mosaicism and multiple con-genital conditions, including congenital hydrocephalus,agenesis of the corpus callosum, bifrontal cortical dys-plasia, and seizure disorder. In 2000, she was found by
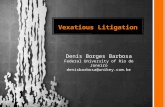
US and MRI to have bilateral renal nodules. Percuta-neous biopsy of two left kidney nodules revealedhyperplastic nephrogenic rests. At that time, a 1.41.2-cm lesion was present in the right kidney. During thenext 3 months, the right-sided lesion remained stable,but one left-sided nodule showed progressive growthand necrosis by CT and MRI, raising concern that thelesion had converted from a nephrogenic rest to a Wilmstumor (Fig. 1). Thus, she underwent left nephrectomy,with pathologic confirmation of multifocal Wilms tu-mors and quiescent and hyperplastic nephrogenic rests.The lesions were centered within the renal medulla.
About 2 years later, the mass in the right kidney
began to grow and failed to regress despite three cyclesof vincristine and dactinomycin. On MRI, it appeareddark on T1-weighted images, bright on T2-weightedsequences, and enhanced with intravenous gadopente-tate dimeglumine (Fig. 1). There were no metastases.Because the tumor did not shrink with chemotherapy,both the surgeon and oncologist considered the lesionclinically aggressive and likely to have transformed to aWilms tumor.
The central location of the tumor within the solitarykidney made resection with renal salvage technicallydifficult. The patients oncologic and surgical specialiststhought there was a high likelihood she would require
nephrectomy and subsequent long-term dialysis andpossibly renal transplantation. Her limited developmentand multiple needs made her a poor candidate forcadaveric transplant. Further, the demands of dialysiswould likely be overwhelming for this particular child,whose developmental state was comparable to that of a1 year old. These issues prompted the surgeon and
oncologist to consider percutaneous RFA a reasonablealternative.
The ablation was undertaken as an innovativetherapy. A consent form conforming to the guidelinesof our Institutional Review Board for innovative ther-apy was discussed with the patients mother. Also, at therequest of our Institutional Review Board, the case was
reviewed with two outside experts in the field of adultRFA.
The patient was intubated, induced under generalanesthesia, and then placed prone and oblique on theCT table. Four pediatric grounding pads (ValleyLabE7510-25DB Infant Return Electrodes, Boulder, Colo.,USA) were placed on the proximal aspect of the childsthighs (one anteriorly and one posteriorly on eachthigh). An initial CT scan was performed with 2 cc/kg ofintravenous contrast medium (32 cc total in the 16-kgpatient) that demonstrated the solitary right kidney witha centrally located 1.81.61.5-cm solid, mildlyenhancing upper-pole lesion (Fig. 2).
The CT images also demonstrated the hepatic flexureof the colon to be directly abutting the medial-mostaspect of the tumor (Fig. 2). To diminish the risk ofcolonic injury, the distance between the colon and thetumor was widened by injecting sterile water betweenthem prior to commencing with the ablation. With CTguidance, a 22-g Chiba needle was directed into theminimal fat anterior to the kidney via a right lateraltranshepatic approach. Because the first needle was notin optimal position, two subsequent needles weremaneuvered using the standard tandem technique until a22-g needle tip was positioned precisely between thekidney and the colon. Sterile water (40 cc) was injected
into the perinephric space, providing 1.8 cm of dis-placement of the colon away from the tumor (Fig. 2).Subsequently, again with CT guidance, a 2-cm array-
type needle electrode (LeVeen Needle Electrode, BostonScientific CorporationOncology, Natick, Mass., USA)was inserted into the center of the lesion in tandem withtwo 22-g Chiba needles that had been placed from a
Fig. 1 Imaging prior to andafter left nephrectomy. A CTscan from 2.5 years prior toRFA showing the Wilms tumor
in the left kidney that wasresected (black arrow) and alesion in the right kidney (whitearrow). B T2-weighted axialMR 2 years after left nephrec-tomy shows an enlarging massin the right kidney (black arrow)
924
-
7/27/2019 Sham Berger
3/6
posterior approach. One of these two latter 22-g needleswas used to acquire a fine-needle biopsy specimen. Thepathology report later showed atypical cells consistentwith nephrogenic rests/nephroblastomatosis/Wilms tu-mor complex. The second needle was removed when theelectrode was well positioned within the lesion and priorto RFA. The electrode array was deployed (Fig. 2), andtreatment was started using an RF 3000 generator(Boston Scientific, Natick, Mass., USA.). Treatment wasinitiated with radiofrequency power set at 10 W and wasincreased by increments of 5 W per minute to a maxi-mum of 60 W. Repeat CT images through the regionwere acquired intermittently during the procedure tomonitor electrode position, colonic displacement, andthe effect of ablation.
Impedance roll-off (rapid increase from 70X to sev-eral 100X) was achieved at 19 min. A second phase oftreatment (booster burn) in the same location wasinitiated at 40 W and maintained for 6.5 min. A repeatCT scan showed that the water in the perinephric spacehad dissipated and that the colon was once againadjacent to the tumor. Rather than risk injuring thecolon, the radiofrequency treatment was terminatedprior to achieving a second impedance roll-off. Theimmediate post-ablation CT scan demonstrated low
attenuation within the lesion, indicating tumor necrosis(Fig. 3). There was a 1-cm crescent of high-densitymaterial posteriorly, likely a small perinephric hema-toma.
Prior to beginning ablation, mild hypothermia wasinduced by leaving the patient exposed without blankets.Her core body temperature was allowed to fall to 33.2Cunder close observation by the anesthesiologist. Thepatients temperature rose to 34.1C during the ablationtreatment itself. She remained intubated for approxi-mately 1 h after the procedure while she was coveredwith blankets to allow her body temperature to nor-malize. She was discharged home the next morning withno complications.
The patient remained well as an outpatient. Threeweeks post-RFA, an MRI demonstrated no change inthe size of the treated tumor. It became bright on T1-weighted images, dark on T2-weighted images, andlacked enhancement (Fig. 3). At the 2-month follow-up,MRI showed continued lack of enhancement and notumor growth; the lesion remained T1 bright and T2dark, although she developed mild upper-pole hydro-nephrosis. The US performed 1 month later showed nochange in the hydronephrosis or size of the tumor. Thehydronephrosis remained stable at the 7-month follow-
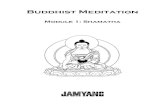
Fig. 2 The RFA procedure.A Access route problemproneoblique preprocedure CT scanshows right colon immediatelyanterior to the renal tumor(arrowheads). This poses apotentially dangerous risk forcolonic perforation from RFA.B, C Solution to access prob-
lemhydrodisplacement. A 22-g needle (small arrowheads) hasbeen placed in the anteriorpararenal space. Distilled water(40 cc) has been injected todisplace the colon away fromthe renal lesion. Note the 22-gneedle (arrow) and the 1.8-cmdisplacement of the colon bythe water (large arrowheads).D Radiofrequency electrodedeploymentthe radiofrequen-cy probe has been placed from aposterior approach into thetumor. Note that the fluid con-tinues to displace the colon
anteriorly
925
-
7/27/2019 Sham Berger
4/6
up, both on US and MRI, while the lesion decreased insize from 1.8 to 1.3 cm by measurements taken withboth modalities. At this time, the lesion demonstratedintermediate signal intensity on T1-weighted images,and higher signal on T2-weighted sequences with faintrim enhancement. Centrally, it lacked enhancement. Thepatients creatinine remained unchanged.
The US performed at 10 months post-treatmentshowed no change in the size of the lesion. However,MRI at 14 months post-treatment showed that the tu-mor grew considerably (3.91.61.5 cm) and extendedbeyond the renal capsule (Fig. 4). It became isointenseon both T1-weighted and T2-weighted images, withinhomogeneous enhancement centrally (Fig. 4). Inaddition, a new enlarged retroperitoneal lymph nodeappeared (Fig. 4). The decision was then made to havethe patient undergo an attempt at partial nephrectomy,preceded by chemotherapy. It was conceded that if acomplete nephrectomy were necessary at the time ofsurgery, she would undergo dialysis with subsequent
consideration as a transplant candidate. She thusunderwent an additional cycle of chemotherapy, fol-lowed by a successful upper-pole nephrectomy. Thepathology report showed multiple microscopic residualfoci of viable nephrogenic blastemal cells, presenting insmall clusters associated with a nodular renal medullaarea of necrosis, granulation tissue, and scarring. Thelymph node demonstrated reactive hyperplasia with noevidence of tumor.
Discussion
Several reports on the use of percutaneous RFA to treatrenal cancers in adults have demonstrated promisingresults with low morbidity [1, 4, 5], but this is the firstreport to describe RFA to treat a renal tumor in a child.
The patient had an aggressive lesion in a solitary kidney,as well as challenging chronic developmental and med-ical comorbidities. The decision to treat with RFA was,in part, based on the patients history of proven Wilmstumor in the contralateral kidney, the continued growthof the current ipsilateral tumor despite chemotherapy,and the demonstration of new contrast enhancement onMRI. Partial nephrectomy would have been the treat-ment of choice after chemotherapy failed to contain thegrowth of the lesion. However, partial nephrectomy wasconsidered to have a low likelihood for technical successand was thought to carry a high potential morbidity. Itwas hoped that RFA as an alternative to partial
nephrectomy could obviate or delay the need for bothnephrectomy and dialysis. Delaying dialysis, even if tu-mor recurrence occurred, was believed by the patientssurgeon and oncologist to be acceptable. In this case,RFA was successful in abating the growth of the tumorand halting contrast enhancement on MRI for approx-imately 1 year after chemotherapy had failed.
Numerous technical issues arose with respect to per-forming ablation in children. The position of the colon
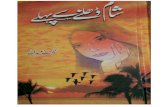
Fig. 3 Post-ablation imaging.A Immediate postprocedurecontrast-enhanced axial CTimage shows nonenhancinglesion (arrow) with a tiny airbubble centrally. Coronalinversion recovery (B) andT1-weighted (C) MRI 3 weekspost-ablation demonstrate the
T2 hypointense and T1 hyper-intense ablated tumor. T1 darkcentral focus (arrow) representseither a residual air bubble orsmall focus of necrosis. D Therewas no enhancement withintravenous contrast medium
926
-
7/27/2019 Sham Berger
5/6
adjacent to the tumor in this case presented a challenge,not only because of the proximity of the bowel to thetumor, but also because the patient, like many children,had minimal retroperitoneal fat. Complications fromthermal injury, including death, have been reported incases of RFA in tumors adjacent to bowel in adult pa-tients [6]. Indeed, one of our outside consultants believedthat this presented a relative contraindication to per-forming the case percutaneously. He suggested usingintraoperative laparoscopic assistance, which has beenadvocated when percutaneous access is particularly dif-ficult or dangerous [7]. Some have employed carbondioxide dissection and angiographic balloon distractionto protect the bowel [8]. Such a maneuver might betechnically easier in adults, who tend to have more fat intheir perirenal space than young children. Farrell et al.[6] successfully instilled sterile water into the perinephricspace (hydrodisplacement) to displace bowel fromrenal tumors in two adult patients who underwent RFA.In our patient, hydrodisplacement was performed withsterile water, and successful displacement of the colon
from the tumor with protection of the bowel wasachieved. A second burn was terminated prematurelybecause of concern that the colon had regained prox-imity to the lesion. It is likely that secondary thermalinjury was responsible for the delayed development ofupper-pole hydronephrosis. Some suggest cold salineinfusion into the collecting system of the kidney toprevent such injury, particularly when performing RFAfor centrally located renal tumors [9].
The placement of the grounding electrodes in smallerchildren and infants presents a challenge because stan-dard pads might be too large. For the 16-kg child in ourcase, four infant grounding pads adequately covered thethighs without overlapping. Because pediatric groundingpads have less cross-sectional area than adult pads, themaximum wattage (60 W) was maintained below themanufacturers instruction-for-use (90 W) to reduce thepossibility of creating skin burns at the pad sites. Theinitial ablation was terminated when impedance roll-offwas achieved. This is the clinical endpoint for therapywith the device used in this procedure. The power for thesecond application of energy was maintained at 40 W inaccordance with the manufacturers instructions for use.
Hyperthermia in a child undergoing RFA of pulmo-nary metastases has been reported [2]. This has not beenreported in adults and might be related to higher heatdelivery relative to body volume in children compared toadults. More experience is needed to ascertain whetherhyperthermia is of practical concern in children. Con-founding issues include larger tumors in smaller chil-
dren, the specific organ system involved, and theproximity of the tumor to the central vasculature. Untilmore data are available, it might be prudent to provide amechanism to monitor and control core body tempera-ture closely in pediatric patients. One might inducehypothermia prior to the onset of heating, as we did.Although induced mild-to-moderate hypothermia (3135C) has been used therapeutically for acute neuro-protection in adults and children in intensive care units
Fig. 4 Fourteen months post-ablation. The treated tumor(arrowheads) now demonstratesintermediate signal intensity onaxial fat-saturated FSE T2-weighted (A) and coronal T1-weighted (B) sequences, andinhomogeneous central contrastenhancement on coronal T1-
weighted fat-saturated images(C) (arrowsT2 bright, T1dark upper-pole hydronephro-sis). D Coronal inversionrecovery image shows a newretroperitoneal lymph node(arrow) that was subsequentlydemonstrated to representreactive hyperplasia
927
-
7/27/2019 Sham Berger
6/6
and operating rooms, hypothermia has been associatedwith adverse effects such as cardiac arrhythmias andalterations in hemostasis [10]. Thus, rather than induc-ing hypothermia prospectively, it might be preferable toobserve the patient closely and have cooling blankets orice packs available if hyperthermia ensues. Alternatively,some have used a Bair-Hugger temperature management
unit (Arizant Healthcare, Eden Prairie, Minn., USA) tomaintain the proper core temperature in childrenundergoing RFA (Fred Hoffer, MD, verbal communi-cation).
No biopsy was performed prior to the decision toundertake ablation in this case. The necessity of biopsyprior to treating bilateral Wilms tumor or diffusenephroblastomatosis is controversial [3]. Biopsy prior tothe decision to undertake ablation in this patient wouldhave required a separate procedure under anesthesia.Instead, an FNA immediately prior to the ablation wasperformed, although no quick stain or frozen sectionwas obtained. The FNA can have difficulty distin-
guishing hyperplastic nephrogenic rests from Wilms tu-mor [11]. Based on the imaging characteristics andclinical behavior of the mass, it would not have changedmanagement. A core biopsy, in our opinion, might haveincreased the risk of bleeding without clearly addingbenefit, as the decision to treat had already been agreedto unanimously.
In summary, we successfully performed RFA of aWilms tumor in a solitary kidney that provided short-term palliation in a child for whom partial or totalnephrectomy carried high risk and low likelihood ofsuccess. Although it might only be useful ultimately as atemporizing measure, oncologists and surgeons mightwish to consider RFA as an option in children whowould otherwise require dialysis and renal transplanta-tion or who are poor surgical candidates. Various spe-cific technical issues differentiate pediatric from adulttumor ablation, including the amount of intra-abdomi-nal fat, need for smaller grounding pads, and potentialsystemic effects of tissue-heating.
References
1. Wood BJ, Ramkaransingh JR, Fojo T,et al (2002) Percutaneous tumor abla-tion with radiofrequency. Cancer94:443451
2. Shiels WE, Brown SD (2005) Radio-frequency tumor ablation in children.In: vanSonnenberg E, McMullen W,Solbiati L (eds) Tumor ablation: prin-ciples and practice. Springer, New York
3. Hoffer FA (2005) Interventional radi-ology in pediatric oncology. Eur JRadiol 53:313
4. Gervais DA, McGovern FJ, ArellanoRS, et al (2003) Renal cell carcinoma:clinical experience and technical successwith radio-frequency ablation of 42 tu-mors. Radiology 226:417424
5. Mahnken AH, Gunther RW, Tacke J(2004) Radiofrequency ablation of renaltumors. Eur Radiol 14:14491455
6. Farrell MA, Charboneau JW, Call-strom MR, et al (2003) Paranephricwater instillation: a technique to preventbowel injury during percutaneous renalradiofrequency ablation. AJR181:13151317
7. Pavlovich CP, Walther MM, ChoykePL, et al (2002) Percutaneous radiofrequency ablation of small renal tu-mors: initial results. J Urol 167:1015
8. Kam AW, Littrup PJ, Walther MM,et al (2004) Thermal protection duringpercutaneous thermal ablation of renalcell carcinoma. J Vasc Interv Radiol15:753758
9. Schultze D, Morris CS, Bhave AD, et al(2003) Radiofrequency ablation of renaltransitional cell carcinoma with protec-tive cold saline infusion. J Vasc IntervRadiol 14:489492
10. Polderman KH (2004) Application oftherapeutic hypothermia in the intensivecare unit. Opportunities and pitfalls of apromising treatment modality. 2. Prac-tical aspects and side effects. IntensiveCare Med 30:757769
11. Beckwith JB (1993) Precursor lesions ofWilms tumor: clinical and biologicalimplications. Med Pediatr Oncol21:158168
928