Severe Sepsis in Neutropenic Haematological Patients
97
SARI HÄMÄLÄINEN Severe Sepsis in Neutropenic Haematological Patients KUOPION YLIOPISTON JULKAISUJA D. LÄÄKETIEDE 472 KUOPIO UNIVERSITY PUBLICATIONS D. MEDICAL SCIENCES 472
Transcript of Severe Sepsis in Neutropenic Haematological Patients

SARI HÄMÄLÄINEN
Severe Sepsis in Neutropenic
Haematological Patients
ISBN 978-951-27-1372-1ISBN 978-951-27-1389-9 (PDF)ISSN 1235-0303
D 472 • SA
RI H
ÄM
ÄLÄ
INEN
• Severe Sepsis in Neutro
penic Haem
atolo
gical Patients
KUOPION YLIOPISTON JULKAISUJA D. LÄÄKETIEDE 472 KUOPIO UNIVERSITY PUBLICATIONS D. MEDICAL SCIENCES 472
KUOPION YLIOPISTON JULKAISUJA D. LÄÄKETIEDE 472KUOPIO UNIVERSITY PUBLICATIONS D. MEDICAL SCIENCES 472
SARI HÄMÄLÄINEN
Severe Sepsis in NeutropenicHaematological Patients
Doctoral dissertation
To be presented by permission of the Faculty of Medicine of the University of Kuopio for public examination in Conference Hall, Olavinlinna Castle, Savonlinna
on Monday 21st December 2009, at 12 noon
Department of MedicineKuopio University Hospital and
University of Kuopio
KUOPIO 2009

Distributor: Kuopio University Library P.O. Box 1627 FI-70211 KUOPIO Tel. +358 40 355 3430 Fax +358 17 163 410 http://www.uku.fi /kirjasto/julkaisutoiminta/julkmyyn.shtml
Series Editors: Professor Raimo Sulkava, M.D., Ph.D. School of Public Health and Clinical Nutrition
Professor Markku Tammi, M.D., Ph.D. Institute of Biomedicine, Department of Anatomy
Author´s address: Department of Medicine Kuopio University Hospital P.O.Box 1777 FI-70211 KUOPIO Tel. +358 17 173 311 Fax +358 17 173 931
Supervisors: Docent Esa Jantunen, M.D., Ph.D. Department of Medicine University of Kuopio and Kuopio University Hospital
Auni Juutilainen, M.D., Ph.D. Department of Medicine University of Kuopio and Kuopio University Hospital
Irma Koivula, M.D., Ph.D. Department of Medicine Kuopio University Hospital
Taru Kuittinen, M.D., Ph.D. Department of Medicine Helsinki University Central Hospital
Reviewers: Docent Esa Rintala, M.D., Ph.D. Department of Medicine Satakunta Central Hospital
Sari Karlsson, M.D., Ph.D. Department of Medicine Tampere University Hospital
Opponent: Docent Veli-Jukka Anttila, M.D., Ph.D. Department of Medicine Helsinki University Central Hospital
ISBN 978-951-27-1372-1 ISBN 978-951-27-1389-9 (PDF)ISSN 1235-0303
Suomen Graafi set Palvelut Oy LtdKuopio 2009Finland
Hämäläinen, Sari. Severe Sepsis in Neutropenic Haematological Patients.Kuopio University Publications D. Medical Sciences 472. 2009. 99 p.ISBN 978-951-27-1372-1ISBN 978-951-27-1389-9 (PDF)ISSN 1235-0303
ABSTRACT
Neutropenic fever and septic infections are common in patients with acute myeloidleukaemia (AML) and in autologous stem cell transplant (ASCT) recipients. Severe sepsis isimportant cause of treatment-related morbidity and mortality in both patient groups. Readilyavailable circulatory markers for severe sepsis could be useful.
This study evaluated epidemiology, microbiology and outcome of neutropenic fever andsevere sepsis in haematological patients with special reference to the kinetics of C-reactiveprotein (CRP), vascular endothelial growth factor (VEGF) and amino-terminal pro-brainnatriuretic peptide (NT-proBNP).
Retrospective series included 84 AML patients and 319 ASCT recipients. In theprospective series of 70 patients with the same diagnoses CRP, VEGF and NT-proBNP weredetermined at the beginning of the neutropenic fever and then daily.
In retrospective series, severe sepsis was found in 13% of AML patients and in 5% ofASCT recipients. In the prospective study, severe sepsis was found in 14% of febrile periods.Severe sepsis was associated with 27% mortality in AML patients and 53% in ASCTrecipients. In the prospective study including careful supportive care, the mortality rate forsevere sepsis was 15%. Gram-positive microbes were more common in blood cultures than gram-negative ones.During 1996-2006 Pseudomonas spp. bacteraemia was found in 30% of neutropenic periodswith severe sepsis in ASCT recipients. VEGF concentrations were generally low. Less than 24 hours after the start of neutropenicfever the VEGF concentrations were higher in patients with severe sepsis than those without.Neither serial NT-proBNP nor CRP showed early predictive value for development of severesepsis.
Despite of intensive interventions, mortality remained high in haematological patients whodeveloped severe sepsis. Higher CRP values coincided with severe sepsis but could notpredict it. VEGF was a more rapid indicator for severe sepsis than CRP. Neither serial NT-proBNP nor CRP showed early predictive value for development of severe sepsis. Severe sepsis is frequent in neutropenic haematological patients and is associated withsignificant mortality. Careful patient monitoring and supportive care are needed to improvethe outcome of severe sepsis in haematological patients.
National Library of Medicine Classification: WC 240, WH 120, WH 250, QU 325, QZ 350Medical Subjects Headings: Sepsis; Bacteremia; Neutropenia; Fever; Epidemiology;Microbiology; Hematologic Diseases; Leukemia, Myeloid, Acute; Stem Cell Transplantation;Transplantation, Autologous; C-Reactive Protein; Vascular Endothelial Growth Factor A;Natriuretic Peptide, Brain; Mortality; Gram-Positive Bacteria; Pseudomonas; Monitoring,Physiologic.

Pieni ja hento ote ihmisestä kiinni Aivan sama tunne kuin koskettava tuuli Pieni ja hento ote - siinä kaikki
Dave Lindholm

ACKNOWLEDGEMENTS
This thesis was carried out in the Department of Medicine at Kuopio University Hospitalbetween 2006 and 2009. I owe my sincere thanks to Professor Leo Niskanen and DocentSeppo Lehto, Chief Physician of the Department of Medicine, Kuopio University Hospital forarranging me facilities to perform this study. I also wish to express my warmest thanks toMatti Huttunen, Chief Physician of the Department of Medicine, Savonlinna Central Hospitalfor providing me with the opportunity to carry out this study.
I am most grateful to the supervisors of this thesis.
Docent Esa Jantunen who considered his task in coordinating these studies with unfailingexpertise and enthusiasm. He has taught me the fundamentals of scientific writing, and,subsequently, has spent numerous hours revising my manuscript. I admire him for hispositive attitude and availability in all phases of writing this thesis. These qualities and hisunfaltering support have been invaluable throughout this process.
Taru Kuittinen, M.D., PhD., who guided me through the very first steps in statistical andscientific analysing. As a mentor and a supervisor, Taru has been demanding yet alwayskind and friendly. Without her bright attitude, endless support and encouragement when it ismost needed, this work would never have been completed.
Auni Juutilainen, M.D., PhD., who took the responsibility for statistical analyses during theprospective phase of this study. Her intelligent and analytical guidance has been preciousand simply indispensable in writing of this thesis. I admire her unfailing logic, and, at thesame time, her sophisticated and academic approach. In many ways Auni has been the soulof this thesis, and a loyal mentor regardless of time of day.
Irma Koivula, M.D., PhD., who has been my principal teacher in infectious diseases. I greatlyadmire her unbeatable logic and sharp scientific thinking. Irma has provided me with thefacilities to continue this study in the middle of clinical whirl, and without her continuoussupport, this study would have never been made.
Yet more than challenging moments, we have enjoyed laughter, long lasting dinners andsome sparkling wine together. Dear friends, this has been a privilege
I wish to express my warmest thanks to co-authors Professor Esko Ruokonen and DocentTapio Nousiainen, M.D. My thanks go especially to Professor Kari Pulkki and Docent IrmaMatinlauri for their persistency and kindly offered guidance in matters of clinical chemistryand laboratory techniques.
I wish to express my gratitude to the official reviewers of this dissertation, Docent EsaRintala, M.D., and Sari Karlsson, M.D., PhD., for their strict criticism, constructive commentsand valuable advice during the final phase of this thesis. This thesis has substantiallyimproved thanks to their contribution. My warmest thanks to Docent David Laaksonen, M.D.,for proof-reading this thesis.
I am most grateful to the nursing staff at the haematology ward of Kuopio University Hospitalfor their accurate patient monitoring and tireless updating of the patient records. I admiretheir strenuous work in nursing of critically ill patients, especially when there is very little hopeleft. I owe much to Ms Tuulikki Pelkonen and Ms Tuija Nenonen for their administrativesupport always offered with patience. I warmly thank Ms Seija Laitinen, RN, chief medical
laboratory technologist, for performing the VEGF analyses, and our unofficial study nurse MsRaija Isomäki for her unfailing help and support.
I want to express my deepest gratitude to all our study patients. Your willingness toparticipate in this study during a very difficult period in your lives has been simply admirable.
I am privileged to have had this opportunity to work and study medicine in several Finnishhospitals. I want to thank all friends and colleagues at Jyväskylä Central Hospital, at KuopioUniversity Hospital, at Helsinki University Hospital and at Oulu University Hospital for sharingthis journey with me. Especially I want to thank colleagues at Savonlinna Central Hospital formany unforgettable moments in clinical practise and, in particular, around the lunch table.Jaana and Mika, this is for you.
I want to thank my friends for being there for me when I was writing this thesis, and I hopeyou will be there in future, too. To Eija for being a truthful friend and a teacher in practise ofinfectious disease. To Ulla-Maija and her family for their ex tempore dinner parties and theendless conversations we shared. To Merja for early mornings in the swimming pool andsupportive coffee breaks. To Marjut and her family for many exhilarating moments atTaiteiden yö happening in Helsinki, and for being a friend in truly difficult times. To Tarja andall her boys for their tales and laughter as well as for speedy and dangerous situations! ToHelena for being a colleague and a teacher during the very first steps in my career as adoctor as well as for all the heavy metal concerts and horseback riding in Ireland! To all myfriends at the stables and yards, especially to Saila and her family for raising a foal togetherbetween spinning lessons. To Salla and her family for having being both a riding instructorand a loyal friend for over a decade now. To Selina and her family for being there both for thepony, Juulia and myself.
Above all, my warmest thoughts belong to my family. To my mother Ritva and my step-fatherPaavo for helping out in everyday crisis, always having the coffee ready and keeping thepugs fat. For my brother Janne and his family for practical guiding in everyday life. Andspecial thanks to my nephew Juuso for helping out with the typing, and being the bestgodson ever. To my niece Juulia for ceaselessly bringing sunshine and laughter into my life.And last but not least, to my sarcastic sister Sanna for splendid holidays and priceless cross-border caring of my pugs.
The study was financially supported by grants from the Finnish Society of Haematology,Blood Research Foundation, Finnish Cultural Foundation and EVO funding of KuopioUniversity Hospital.
Kuopio, December 2009.

ABBREVIATIONS
AML acute myeloid leukaemiaASCT autologous stem cell transplantationAUC area under curveBEAC carmustine, etoposide, cytarabine and cyclophosphamideBEAM carmustine, etoposide, cytarabine and melphalanBNP brain natriuretic peptideCD4 helper T-cellCD8 cytotoxic T-lymphocyteCI confidence intervalCLL chronic lymphocytic leukaemiaCRP C-reactive proteinEBMT the European Group of Blood and Marrow TransplantationESBL extended-spectrum betalactamaseELISA enzyme-linked immunosorbent assayHDT high-dose chemotherapyHL Hodgkin lymphomaIL interleukinICU intensive care unitIDSA Infectious Diseases Society of AmericaMM multiple myelomaMOF multiorgan failureMRSA methicillin-resistant Staphylococcus aureusNHL non-Hodgkin lymphomaNT-proBNP amino-terminal pro-brain natriuretic peptidePaC02 arterial partial pressure of C02
PAMPs pathogen-associated molecular patternsPCR polymerase chain reactionPCT procalcitoninROC receiver operating characteristic curveSIRS systemic inflammatory response syndromeSOFA sepsis-related organ failure assessmentTh1 type-1 helper T-cellTh2 type-2 helper T-cellTLRs toll-like receptorsSPSS statistical package for the social sciencesS-TnT serum cardiac troponin TTNF- tumor necrosis factor-alphaVEGF vascular endothelial growth factorVRE vancomycin-resistant enterococci

LIST OF ORIGINAL PUBLICATIONS
This thesis is based on the following papers, which will be referred to by their Roman
numerals.
I. Hämäläinen S, Kuittinen T, Matinlauri I, Nousiainen T, Koivula I, Jantunen E.
Neutropenic fever and severe sepsis in adult AML patients receiving intensive
chemotherapy: causes and consequences. Leuk Lymphoma. 49:495-501, 2008
II. Hämäläinen S, Kuittinen T, Matinlauri I, Nousiainen T, Koivula I, Jantunen E.
Severe sepsis in autologous stem cell transplant recipients: microbiological
aetiology, risk factors and outcome. Scand J Infect Dis. 41:14-20, 2009
III. Hämäläinen S, Juutilainen A, Matinlauri I, Kuittinen T, Ruokonen E, Koivula I,
Jantunen E. Serum vascular endothelial growth factor in adult haematological
patients with neutropenic fever: a comparison with C-reactive protein. Eur J
Haematol. 83;251-257, 2009
IV. Hämäläinen S, Juutilainen A, Kuittinen T, Nousiainen T, Matinlauri I, Pulkki K,
Koivula I, Jantunen E. Serum amino-terminal pro-brain natriuretic peptide in
haematological patients with neutropenic fever: a prospective comparison with
C-reactive protein [Submitted]
CONTENTS
1. INTRODUCTION ....................................................................................................................15
2. REVIEW OF THE LITERATURE .............................................................................................16
2.1. Infections in neutropenic haematological patients ..........................................................152.1.1. Bloodstream infections in patients with neutropenic sepsis .............................172.1.2. Infectious complications in patients with acute myeloid leukaemia ..................192.1.3. Infectious complications in autologous stem cell transplant recipients .............20
2.2. Sepsis and severe sepsis..............................................................................................212.2.1. Pathophysiology of sepsis ..............................................................................23
2.2.1.1. Innate immunity response................................................................232.2.1.2. Adaptive immunity response............................................................242.2.1.3. Complement system, coagulation and inflammation.........................252.2.1.4. Endothelium and inflammation.........................................................262.2.1.5. Multiorgan failure.............................................................................26
2.2.2. Epidemiology of sepsis...................................................................................272.2.3. Microbiological aetiology of sepsis..................................................................28
2.3. Markers for severe sepsis .............................................................................................292.3.1. C-reactive protein...........................................................................................302.3.2. Vascular endothelial growth factor..................................................................332.3.3. Amino-terminal pro-brain natriuretic peptide....................................................342.3.4. Other markers ................................................................................................35
2.3.4.1. Lactate ............................................................................................35 2.3.4.2. Procalcitonin....................................................................................36 2.3.4.3. Interleukins......................................................................................37
3. AIMS OF THE STUDY .......................................................................................................38
4. PATIENTS AND METHODS.…………………………………………………………………………. 39
4.1. Patients.........................................................................................................................394.1.1 Patients in retrospective studies (I–II) .............................................................39
4.1.1.1. Characteristics of patients with acute myeloid leukaemia (I).............394.1.1.2. Characteristics of autologous stem cell transplant recipients (II).......39
4.1.2. Patients in prospective studies (III–IV) ............................................................39
4.2. Methods........................................................................................................................434.2.1. Definitions ......................................................................................................434.2.2. Clinical management and supportive care measures (I-IV)…………………….. 43
4.2.2.1. Chemotherapy..................................................................................454.2.2.2. Antimicrobial therapy.......................................................................48
4.2.3. Laboratory methods .......................................................................................484.2.3.1. Blood cultures .................................................................................504.2.3.2. Serum C-reactive protein.................................................................504.2.3.3. Serum vascular endothelial growth factor.........................................524.2.3.4. Plasma amino-terminal pro-brain natriuretic peptide.........................52
4.2.4. Statistical methods .........................................................................................53
4.3. Approval of the Ethics Committee..................................................................................53
5. RESULTS..................................................................................................................................54.
5.1. Retrospective studies (I-II).............................................................................................545.1.1. Epidemiological features of severe sepsis.........................................................54

5.1.2. Microbiological findings and site of infection....................................................555.1.3. Factors associated with severe sepsis............................................................565.1.4. Serum C-reactive protein in relation to severe sepsis......................................60
5.2. Serum vascular endothelial growth factor in patients with neutropenic fever: acomparison with C-reactive protein (III)..........................................................................605.2.1. Epidemiological features of severe sepsis ......................................................605.2.2. Microbiological findings and site of infection....................................................605.2.3. C-reactive protein...........................................................................................615.2.4. Serum vascular endothelial growth factor .......................................................63
5.3. Serum amino-terminal pro-brain natriuretic peptide in patients with neutropenicfever: a comparison with C-reactive protein (IV).............................................................645.3.1. Epidemiological features of severe sepsis ......................................................645.3.2. Microbiological findings and site of infection....................................................685.3.3. Factors associated with severe sepsis............................................................685.3.4. C-reactive protein...........................................................................................685.3.5. Amino-terminal pro-brain natriuretic peptide....................................................695.3.6. Association of amino-terminal pro-brain natriuretic peptide with fluid
intake and previous cardiovascular disease....................................................69
6. DISCUSSION .........................................................................................................................75
6.1. Patients and methods....................................................................................................75
6.2. Epidemiological features and outcome of severe sepsis ................................................766.2.1. Patients with acute myeloid leukaemia ...........................................................766.2.2. Autologous stem cell transplant recipients ......................................................776.2.3. Prospective study...........................................................................................78
6.3. Microbiological findings .................................................................................................78
6.4. Kinetics of C-reactive protein in patients with neutropenic fever (Studies I-II) .................80
6.5. Comparison of serum vascular endothelial growth factor and C-reactive proteinin patients with neutropenic fever (Study III) ..................................................................80
6.6. Comparison of serum amino-terminal pro-brain natriuretic peptide and C-reactiveprotein in patients with neutropenic fever (Study IV) ......................................................82
6.7. Study limitations.... .......................................................................................................83
6.8. Concluding remarks ......................................................................................................846.8.1. Implications for further research .....................................................................85
7. CONCLUSIONS......................................................................................................................87
8. REFERENCES .......................................................................................................................88
ORIGINAL PUBLICATIONS I – IV

15
1. INTRODUCTION
Treatment of haematological malignancies has improved during recent decades. This is due
to modern effective drugs and regimens but also due to improvements in supportive care.
About 40% of younger patients with acute myeloid leukaemia (AML) are cured with intensive
chemotherapy (1, 2). Relatively high percentage of patients with relapsed non-Hodgkin
lymphoma (NHL) (3) or Hodgkin lymphoma (HL) (4) are cured by high-dose therapy supported
by autologous stem cell transplantation (ASCT).
Intensive chemotherapy has certain disadvantages. Chemotherapy induces breakdown of
mucosal barriers, usually leading to high risk of neutropenic fever, which is associated with
development of severe sepsis and high mortality. Thus, early initiation of antimicrobial therapy
(5-7) and other supportive measures are vital in the management of haematological patients
receiving intensive chemotherapy. In spite of some obvious advances, the need for
improvement remains.
Several studies have evaluated the epidemiology and prognostic factors of septic patients
admitted to intensive care units (ICU) (8-10). However, only a minority of these patients has
had haematological malignancies. Therefore, the risk factors for severe sepsis and outcome of
sepsis in these ICU-based studies are not necessarily applicable for patients with neutropenic
sepsis. In fact, there are very limited data available on the incidence, risk factors and outcome
of severe sepsis in neutropenic haematological patients receiving intensive chemotherapy.
C-reactive protein (CRP) has traditionally been used to evaluate the severity of infection and
also the response to antimicrobial therapy in patients with febrile neutropenia, even though its
predictive value has been controversial (11-14). Other markers of septic infections that are
also used to predict outcome in the ICU, like serum vascular endothelial growth factor (VEGF)
(15) or amino-terminal pro-brain natriuretic peptide (NT-proBNP) (16) have not been
prospectively evaluated in a haematological ward setting. Even though marked improvements
have been observed in the treatment of severe sepsis in ICUs (8), there are only limited data
available on careful patient monitoring and vigilant supportive care in haematological wards of
patients with severe sepsis.
The aim of this study was to evaluate the epidemiological features, microbiological aetiology
and outcome of severe sepsis in neutropenic haematological patients. Early prognostic
markers for the development of severe sepsis were also evaluated. These markers included
VEGF and NT-proBNP, with special reference to the kinetics of CRP. In addition, the purpose
of the prospective treatment protocol was to improve the clinical management of septic
neutropenic patients in haematological ward.
16
2. REVIEW OF THE LITERATURE
2.1. Infections in neutropenic haematological patients
Unfortunately, as long as patients are neutropenic it is likely that some of them will develop
infectious complications
GP Bodey (17)
The mechanisms and pathophysiology of sepsis in neutropenic patients is similar to that in
patients without neutropenia but with the exception of pancytopenia. Neutropenia enables the
infection to progress in a more insidious and aggressive way. The role of neutrophils in septic
infections is controversial. They are thought to be essential for the eradication of pathogens
but at the same time, excessive release of oxidants and proteases by neutrophils might be
responsible for tissue injury (18). In studies carried out with granulocyte colony-stimulating
factor in patients with pneumonia the markedly increased neutrophil count was not deleterious
but did not have obvious clinical benefits, either (19). Neutropenic patients with septic
infections have higher mortality rates emphasizing the protective role of an appropriate acute
inflammatory response (20).
Infections have been recognised as complications of leukaemia for the first time as early as
in 1845 (21). Until 1948, there was no specific treatment for acute leukaemia (22). When very
little was to do for the natural course of the disease, there were no major interest to study or
understand the possibility of infectious complications. Although neutropenia is a common
consequence of acute leukaemia, its role in infection was not fully recognised until the early
1960´s (17).
Patients with haematological malignancies are immunocompromised because of both the
underlying malignancy and the therapy employed to manage it. Therapeutic interventions such
as corticosteroids, stem cell transplant and radiotherapy also produce deficiencies in host
defenses. Normal human skin and mucosal colonisation change during chemotherapy and
hospitalisation. Within all this, neutropenia acts as a common risk factor for severe bacterial
infections. It is estimated that at least 30-60% of neutropenic patients develop an infection, of
whom 13-37% develop bacteraemia (23-26). During the last three decades the overall
mortality rate due to septic infections in neutropenic patients has decreased from 21% to 7%
(27), but febrile neutropenia still remains a major reason for significant morbidity and mortality
in this patient group (28). The depth and duration of neutropenia is directly related to incidence
17
of serious bacterial infections. The risk of severe infection is significantly greater at low
neutrophil counts (absolute neutrophil count <0.1x109/l) (29).
Neutropenia alters the host’s inflammatory response and makes the infection difficult to
detect because the classic signs and symptoms of infection are often missing (30, 31). The
endogenous pyrogen (IL-1) is produced by mononuclear cells, not by granulocytes, and these
mononuclear cells include also fixed-tissue macrophages that persist after chemotherapy. This
explains the presence of fever despite the otherwise poor inflammatory response in
neutropenic patients (32). Fever is the principal sign of infection, and it is often the only
evidence of infection in neutropenic patients. In clinical practice, careful history of possible
symptoms and physical examination to seek for subtle signs of infection remain essential. The
prompt initiation of empirical antibiotics has been the most important advance in the treatment
of febrile neutropenic patients (33) – prior to this policy the mortality from gram-negative
infections was as high as 80% (29, 34). The importance of early antimicrobial treatment for
febrile neutropenia was for the first time demonstrated in the study of Schimpff et al (35).
Today the overall survival rate for febrile neutropenic patients is over 90%.
In Finland empirical antimicrobial treatment in febrile neutropenic patients includes usually a
combination of a third generation cephalosporin and an aminoglycoside. If Pseudomonas
aeruginosa bacteraemia is suspected, antimicrobial treatment should be initiated with
antipseudomonal penicillin together with an aminoglycoside. Vancomycin is only rarely used
empirically (36).
2.1.1. Bloodstream infections in patients with neutropenic sepsis
Over the last three decades, several studies have demonstrated a shift in the aetiology of
bacteraemic infections from predominance of gram-negative rods to gram-positive cocci (37,
38). Prior to the availability of methicillin, penicillin-resistant Staphylococcus aureus was the
main threat to neutropenic patients and mortality rate from Staphylococcus aureus infections
exceeded 50%. Methicillin became available during the 1960s, curing most neutropenic
infections caused by Staphylococcus aureus (17). During the subsequent two decades gram-
negative bacteria emerged as the main causative agents (39). Infections with Pseudomonas
aeruginosa were common and were associated with a high mortality rate (40).
By the end of the 1980s and lately during 1990s, gram-positive microbes re-emerged (41,
42). The most common infective agent was coagulase-negative staphylococci, mainly
Staphylococcus epidermidis. The cause for this change has not been clearly identified.
Possible factors responsible for this process include widespread use of indwelling central
18
venous catheters, a higher incidence of severe oropharyngeal mucositis and bowel damage
with the use of more intensive chemotherapy regimens and more profound and prolonged
neutropenia. In addition, use of quinolone-based prophylactic antibiotics suppressing aerobic
gram-negative microbes colonizing the gastrointestinal tract but failing to suppress sufficiently
gram-positive flora and use of other antibiotics with selective pressure may be potential
factors. Furthermore, administration of histamine H2 receptor blockers or proton-pump
inhibitors may promote infections by reducing gastric pH and promoting overgrowth of
oropharyngeal gram-positive flora (43-45).
Mucositis, which is a well-known consequence of cytotoxic chemotherapy (46), predisposes
patients to infections arising from patient’s own flora – primarily of oropharyngeal and
gastrointestinal origin. Mainly because of this, clinically important gram-positive microbes
include also viridans group streptococci (e.g. Streptococcus milleri or Streptococcus mitis),
which belong to the normal flora of the oropharynx and gastrointestinal tract. Among
neutropenic patients both the morbidity and mortality to streptococcal bacteraemia remains
high (6, 47). Other new gram-positive microorganism include species belonging to Enterococci,
Stomatococci, Leuconostoc, Lactobacillus and Corynebacterium species – microbes that were
traditionally considered contaminants in blood cultures.
There is also an interesting difference in the incidence of gram-negative bacteraemias
between developed and developing countries (48-51). In developing countries, the amount of
gram-negative bacteraemias remains high, probably due to the less frequent use of central
lines and prophylactic antibiotics (52, 53). This distribution may nevertheless be reversing
since in some western centers the gram-negative microbes are making a comeback (48, 52,
54). Even though the general incidence of gram-negative microbes as a cause of bacteraemic
infections in developed countries has declined, they are nonetheless still a problem. This is
primarily because of their traditional association with high mortality rates and also the alarming
rise of multidrug-resistant strains (49, 55). In recent study the distribution of bacteraemias in
neutropenic cancer patients was gram-positive in 57%, gram-negative in 34% and
polymicrobial in 10% (56). The mortality rates were 5%, 18% and 13%, respectively. The most
common causative agents of gram-negative rods are Klebsiella and Enterobacter species as
well as Stenotrophomonas maltophilia and Burkholderia cepacia, not forgetting Pseudomonas
species (44, 57).

19
2.1.2. Infectious complications in patients with acute myeloid leukaemia
In patients with acute myeloid leukaemia (AML) intensive chemotherapy regimens enable
complete remission in 80-85% of patients below 65 years of age. About 40% of patients are
cured with intensive consolidation courses (2, 58).
Infections are the major cause of morbidity and mortality in patients with AML. The treatment
protocol of AML induces long lasting periods of neutropenia, which predisposes patients to
recurring infections. These arise mainly during the first course of induction chemotherapy. This
may cause delays in consolidation therapy and increase the risk of leukaemia relapse. Also
consolidation courses are associated with long periods of neutropenia and the risk of fatal
infections both in adults and children (59, 60).
The infectious mortality during AML treatment ranges between 5.5 -13% (60-64). The initial
source of infection often remains unknown and therefore the first antimicrobial therapy choice
is empirical. Therapy is directed primarily against gram-negative microbes. Like in other septic
neutropenic infections, the spectrum of causative pathogens has changed over the past
decades. Coverage of coagulase-negative staphylococci is not necessary for the initial
antimicrobial therapy. Coverage of oropharyngeal streptococci is sufficient when combination
therapy or monotherapy with highly active third-generation cephalosporins or carbapenems are
used (43).
In recent studies the amount of bloodstream infections among neutropenic AML patients has
varied between 34% and 38% (24, 59, 65). In the study of Madani (24) the frequency of
isolation of gram-positive cocci was 74.2% and gram-negative bacilli 12.1%. The most
common pathogens in the gram-positive group were coagulase-negative staphylococci
(34.8%) followed by Streptococcus viridans (22.7%) and in the gram-negative group Klebsiella
pneumoniae (3%) followed by Enterobacter cloacae (1.5%). Ciprofloxacin prophylaxis was
used during the neutropenic period. In spite of this there were still gram-negative
bacteraemias. The amount of resistant microbes was not discussed. In this study, the site of
infection was identified in 81% of all febrile episodes. Mucositis (21.7%), pneumonia (13.2%)
and central venous catheter infection (12.4%) were the most common sites of infection.
Bloodstream infections (37.9%) were commonly associated with cellulitis, mucositis and
central venous catheter infection.
In a study analysing the infections occurring in newly diagnosed AML patients under 65
years of age the amount of bloodstream infections was 34% (59). During induction phase 13%
of neutropenic patients had bloodstream infection caused by gram-negative rods and 21% by
gram-positive cocci. The case fatality rates for gram-negative and gram-positive bacteraemias

20
were 10% and 8%, respectively. When the potential age-related differences in nosocomial
infections between younger (<60 years old) and older leukaemia patients with neutropenic
fever were evaluated, no significant age-related differences were found in the overall incidence
of infections, nosocomial pattern, or overall outcome(66) .
2.1.3. Infectious complications in autologous stem cell transplant recipients
High-dose chemotherapy (HDT) supported by ASCT is a commonly applied treatment for
haematological malignancies, mainly lymphomas and multiple myeloma (MM) (67, 68).
Annually more than 15 000 procedures are performed in Europe (69). The procedure is
considered to be relatively safe with a low incidence of severe complications and transplant-
related mortality. However, approximately 1-5% of neutropenic periods after HDT are
complicated by fatal infections (70-74).
After ASCT, there is an unavoidable period of neutropenia, where the risk for infections is
high. The conditioning regimen causes neutropenia and defects in mucosal and cutaneous
barriers. Neutropenic periods are shorter than in AML treatment, but the intensity of treatment
in ASCT recipients is greater and the mucosal damage may thus become more serious.
Hence, mucositis and indwelling central venous catheters commonly lead to bacterial and
fungal bloodstream infections. During the first 4 weeks after haematopoietic stem cell
transplant, bacterial infections and invasive fungal infections predominate. Between 30 and
100 days after transplant, impaired cellular immunity increases the risk of viral infections (75).
The percentage of bloodstream infections varies between 12% and 20% in ASCT recipients
(72-74, 76). As in all other neutropenic bacteraemias, gram-positive microbes cause at least
half of the bloodstream infections occurring after ASCT. In a recent study 60.3% of the positive
blood cultures were gram-positive cocci and 28.9% gram-negative rods (70). The most
common isolates in the gram-positive group were coagulase-negative staphylococci (43.4%)
followed by Streptococcus viridans (5.7%) and in the gram-negative group Stenotrophomonas
maltophilia (10.1%), followed by Acinetobacter baumannii (6.9%). Of the 314 study patients 12
(3.8%) died because of infectious complications – 6/12 patients because of gram-negative
bacteraemia (Stenotrophomonas maltophilia, Acinetobacter baumannii and Pseudomonas
aeruginosa). In that study norfloxacin was used as a prophylactic antibiotic. During the study
period (1994-2005) Pseudomonas aeruginosa was resistant to ceftazidime and
aminoglycosides in half of the cases and to fluoroquinolones in 25-50% of the cases.
Fluoroquinolone resistance seemed to diminish during the study period. The patients who died
due to infection had markedly longer median time of severe neutropenia (70).
21
2.2. Sepsis and severe sepsis
Inflammation is a reactive state of the organism against disturbances of homeostasis with the
goal of healing and repair of the injured tissue
JB Cone (77)
In 1991 the American College of Chest Physicians/Society of Critical Care Medicine
Consensus Conference (ACCP/SCCM) compiled the current definition of sepsis as a systemic
inflammatory syndrome in response to infection. When this was associated with hypotension,
hypoperfusion or acute organ dysfunction sepsis was considered to be severe (78, 79). Before
these definitions the terms sepsis, septicemia, sepsis syndrome and bacteraemia were used
without precise characterisation.
When the ACCP/SCCM consensus conference released these definitions they also
proposed a new term to describe inflammatory processes that occur in parallel with systemic
infection (78). Systemic inflammatory response syndrome (SIRS) has several clinical
manifestations, including abnormalities in body temperature, respiratory and heart rate.
The definition of SIRS has been noted to be controversial and challenging for clinical use.
American and European critical care societies reconsidered the definitions of ACCP/SCCM in
2001. The decision was that although the concepts based on SIRS were too sensitive and
indefinite, these were useful as a baseline construction for the diagnosis of sepsis (79).
Subsequently, these definitions have been used widely both in clinical practice and in research
worldwide (Table 1).

22
Table 1. Criteria for the systemic inflammatory response syndrome, sepsis and severe sepsisaccording to the Consensus Conference of the ACCP/SCCM (79)_________________________________________________________________________Term Definition_________________________________________________________________________
SIRS Systemic inflammatory response syndrome.
The systemic inflammatory response is manifested bytwo or more of the following criteria:
Fever (body temperature > 38°C) or hypothermia(<36°C)
Tachycardia (heart rate > 90 beats/min)
Tachypnea (>20 breaths/min) or PaC02 < 4.3 kPa
Leucocytosis or leucopenia (white blood cell count >12,000 or < 4000/mm3 or > 10% immature forms
SEPSIS Presence of SIRS in response to infection. SIRS ismanifested by two or more of the criteria mentionedabove
SEVERE SEPSIS Sepsis associated with organ dysfunction,hypoperfusion or hypotension. Organ dysfunction andhypoperfusion abnormalities may include, but are notlimited to lactatic acidosis, oliguria or alteration inmental status
Septic hypotension is defined as a systolic bloodpressure < 90 mmHg or a decrease in systolic bloodpressure by 40 mmHg or more from the baseline
_________________________________________________________________________Abbreviations: PaC02, arterial partial pressure of C02; kPa, kiloPascal.

23
2.2.1. Pathophysiology of sepsis
The microorganisms that seem to have it in for us…turn out…to be rather more like
bystanders…It is our response to their presence that makes the disease. Our arsenal for
fighting off bacteria are so powerful…that we are more in danger from them than the invaders
Lewis Thomas (80)
The English word sepsis is derived from the Greek term ptik s for rotten or “to make
putrid”. Sepsis, defined as the systemic host response to microorganisms in previously sterile
tissue, is a syndrome related to severe infections. In its severe form, sepsis is characterised
by end-organ dysfunction often far away from the primary site of infection.
The pathophysiology of sepsis is understood as a continuum. The normal response of host
to infection is both to identify pathogen invasion and to start tissue repair. The immune
response consists of innate immunity and adaptive immunity responses. The innate immunity
response embodies front-line reaction towards invading pathogens. It includes recognition of
microbial components, activation of local phagocytosis (e.g. neutrophils, eosinophils,
monocytes and macrophages), complement system and coagulation as well as production of
acute phase proteins. Adaptive immunity comprises responses of cell-mediated and humoral
immunity. These phenomena progress in parallel and are contingent on each other. These
both give rise to anti-inflammatory and proinflammatory responses (81). If this continuum is
disturbed, a chain of events occurs in which the promotion and liberation of mediators leads
inevitably to sepsis (82).
2.2.1.1. Innate immunity response
The natural physical barriers to host invasion are formed externally by the skin and internally
by mucous membranes lining the gastrointestinal, genitourinary and respiratory tracts. These
form a mechanical barrier towards invading pathogens in co-operation with local normal flora.
In the hospital environment patients’ indwelling catheters, intravenous cannulas and urinary
catheters must be noted as possible sources of infection (83). Sepsis may be caused by
numerous invasive pathogens, including bacteria, yeasts, viruses and parasites.
The structural components of the microbe responsible for triggering the septic process are
important not only for understanding the mechanisms of infection and inflammation, but also
for identifying potential therapeutic targets. Endotoxin is a lipopolysaccharide present in the
outer portion of gram-negative bacteria. Exposure to endotoxins, exotoxins produced by gram-
24
positive bacteria, or other types of microbial components triggers intracellular events in
immune cells and the epithelium, endothelium and neuroendocrine system through microbial-
associated molecular patterns (84).
The initiation of the response involves pattern of recognition receptors which recognise
specific structures of microbes (85). Part of this family are toll-like receptors (TLRs), which are
transmembrane proteins on the surface of immune cells. These are capable of sensing
invading microbes. Microbes have unique cell-wall molecules known as pathogen-associated
molecular patterns (PAMPs). PAMPs bind to TLRs on the surface of immune cells. This
binding activates, in turn, intracellular signaling pathways. At the end of this pathway,
proinflammatory cytokines are released. Also macrophages and monocytes participate in the
secretion of proinflammatory cytokines. Neutrophils and endothelial cells are activated to
produce adhesion molecules, which help to kill pathogens, but also cause damage to the
endothelium (85). Macrophages release VEGF-like mediators, which increase vascular
permeability and vascular proliferation, contributing to coagulation and inflammatory processes
(86).
2.2.1.2. Adaptive immunity response
Following the initial host-microbe interaction there is a widespread activation of adaptive
immune response, which coordinates defence response involving both humoral and cellular
immune systems.
The humoral immune response is mediated by secreted antibodies (immunoglobulins)
produced in the cells of B lymphocyte lineage (plasma cells). Secreted antibodies bind to
antigens on the surfaces of invading microbes, marking them for destruction by components of
innate immune system (87, 88). Pathogens are destroyed by phagocytic cells (e.g. neutrophils,
macrophages or natural killer cells) with the help of complement activation or recognition by
antibodies (89, 90).
Cellular immunity is an immune response mediated by T-cells. It involves activation of
macrophages, natural killer cells, antigen-specific cytotoxic T-lymphocytes and the release of
various cytokines in response to an antigen. Cytotoxic T-lymphocytes (CD8) are able to
destroy cells infected by viruses or cells with intracellular bacteria. Helper T cells (CD4)
secrete cytokines by differentiating into type 1 helper T-cells (Th1) and type 2 helper T-cells
(Th2) (or other subsets). Th1 secretes pro-inflammatory cytokines and Th2 anti-inflammatory
cytokines. Proinflammatory mediators (e.g. interleukin-1 (IL-1), interleukin-6 (IL-6) and tumor
necrosis factor-alpha (TNF- )) contribute to eradication of invading pathogens and anti-

25
inflammatory mediators (e.g. interleukin-4 (IL-4) and interleukin-10 (IL-10)) to control this
response (91, 92). This proinflammatory response leads inevitably to damage of the host
tissues, whereas the anti-inflammatory response causes leukocyte reprogramming and
changes immune status (93). During this time sequence, circulatory abnormalities (e.g. intra-
vascular volume depletion, peripheral vasodilatation and myocardial depression) lead to an
imbalance between systemic oxygen delivery and demand.
2.2.1.3. Complement system, coagulation and inflammation
The complement system and coagulation are the major components of plasma cascades.
They are closely related and are activated in a contiguous manner by common stimuli (e.g.
infection, trauma). They both contribute to inflammation and mutually interact at several stages
(94, 95).
Complement is not only a part of the innate immune system, but also an effector of antibody-
mediated immunity. The major functions are the defence against pyogenic bacterial infections
bridging innate and adaptive immunity, and clearance of immune complexes and products of
inflammatory injury. Circulating components of the complement are activated via three
pathways: 1) the classical pathway initiated by the binding of component C1q to antigen-
antibody complex, 2) the lectin pathway initiated by binding of mannose-binding lectin to
sugars present in the bacterial wall, and 3) an alternative pathway initiated after exposure to
surface molecules of invading pathogens. At the end of these pathways several convertases
(e.g. C3, C5) are released and they in turn facilitate the phagocytosis of opsonised pathogens
by macrophages and neutrophils, act as inflammatory mediators and, further, participate in the
lysis of bacterial cell membranes. The regulatory mechanisms of the complement system are
sensitively balanced. The aim is to focus the activation of complement on the surface of
invading pathogens, while on limiting deposition on normal cells and tissues (94, 96).
A delicate balance of pro- and anticoagulant factors maintains haemostasis. In normal
conditions three anticoagulant pathways prevent systemic activation of coagulation:
antithrombin, activated protein C and tissue factor pathway inhibitor. During inflammation-
induced activation of coagulation all three functions are impaired; IL-6 release triggers tissue
factor upregulation, initiating the coagulation cascade, and TNF- mediates the suppression of
natural anticoagulants. The latter can lead to disseminated intravascular coagulation, which
has been thought to be central in the pathogenesis of multiorgan failure (MOF) in sepsis
patients. Thus, sepsis is a chaotic environment associated with exacerbated coagulation,
decreased anticoagulation and impaired fibrin removal (95, 97, 98).
26
Complement and coagulation cascades are intended to act locally. If they are activated
systemically as a result of a failure of the relevant control mechanisms, the effect of this broad
reaction can be irreversible.
2.2.1.4. Endothelium and inflammation
Vascular endothelial cells play an active role in the regulation of blood vessel tone,
permeability, coagulation, angiogenesis and both leukocyte and platelet activation. Endothelial
cells synthesise several pro- and anti-inflammatory molecules. They also synthesise proteins
which increase vascular permeability to fluid and large molecules (e.g. antibodies and
components of complement) (95, 99).
Several microbes can adhere to the endothelium, causing localised inflammation and
recruitment of neutrophils and monocytes. Increased vascular permeability allows leukocyte
migration into surrounding tissue as a response to chemotactic factors generated at the site of
injury. Bacterial endotoxins or other foreign particles induce neutrophil activation and release
of pro-inflammatory cytokines. Strong adhesion initiates the coagulation cascade (97, 99). The
endothelium is one of the key organs involved in the pathogenesis of sepsis. Endothelial
damage may result in global tissue hypoxia or shock (99). Worsening tissue hypoxia may
ultimately lead to MOF and death.
2.2.1.5. Multiorgan failure
The ultimate cause of death in patients with severe sepsis is multiorgan failure. The exact
mechanisms for MOF are unknown. Earlier observations indicate that the number of failing
organs or organs with dysfunction correlates with mortality, with an increase of 20% for each
additional organ failure (100, 101). In-hospital mortality with the failure of at least two organ is
four-hold compared with patients who have only a single organ failure (102).
Mechanisms of multiorgan failure include widespread microvascular occlusion, development
of tissue exudates that further compromise tissue oxygenation and disorders in microvascular
homeostasis, which all result from elaboration of vasoactive substances (e.g. histamine).
Cellular infiltrates (mainly neutrophils) damage tissue directly by releasing lysosomal
enzymes. Proinflammatory cytokines (mainly TNF- ) mediate increased production of nitric
oxide, causing further vascular instability. This may also contribute to the direct myocardial
depression that occurs commonly in sepsis (82) .

27
Ongoing tissue hypoxia acts as an indicator for progressive MOF. The extent of oxygen
debt, i.e. the amount by which oxygen requirements exceed oxygen delivery, is related to the
outcome of sepsis. Also impaired endocrine responses to sepsis may result due to cytokines
and metabolic and ischaemic derangements in hypothalamic-pituitary axis and adrenal
glands. Deficiencies in adrenal gland function and vasopressin production contribute to
hypotension and eventual death (103, 104).
2.2.2. Epidemiology of sepsis
Despite extensive study and new therapeutic modalities, sepsis is still a challenge in clinical
medicine. Severe sepsis and septic shock are both relatively common and represent an
important cause of morbidity and mortality.
Both the incidence and mortality in severe sepsis varies in different studies. In Scandinavia,
there are only a few nationwide studies, the most important of which are the Norwegian study
in 1999 and the FINNSEPSIS study in 2004-2005. The national health database in Norway
was retrospectively screened for cases of severe sepsis. The incidence of severe sepsis was
1.5/1000 of the population. Severe sepsis was diagnosed in 31.8% of sepsis patients, and the
hospital mortality for severe sepsis was 27% (9). The FINNSEPSIS study was a prospective
study in the ICUs of 21 hospitals in Finland. Severe sepsis was diagnosed in 470 of 4500
patients (10.5%) admitted to ICUs. The incidence of ICU-treated severe sepsis in Finland was
0.38/1000 of the adult population. The ICU mortality rate was 15.5% and the number of organ
failures affected the mortality rate. In patients with a single organ failure the mortality was
11.5% but in patients with three organ failures mortality increased up to 34% (10).
In the EPISEPSIS study sepsis was prospectively evaluated among all admissions of 206
adult ICUs of public hospitals in France (8). The incidence of severe sepsis was 0.95/1000.
Altogether 14.6% of patients had severe sepsis or septic shock. The in-hospital mortality rate
was 35% at 30 days. This study was a reappraisal for an earlier study (105) in which 8.4% of
patients were found to have severe sepsis or septic shock and 56% of them died at hospital.
Although the admission rate of severe sepsis in French ICUs appears to have increased,
hospital mortality has decreased suggesting improved management (105). In a large
retrospective British study, the incidence of severe sepsis was 0.46-0.66/1000 of population.
Of adult patients admitted to ICU, 27% met criteria for severe sepsis during the first 24 hours
(in-hospital mortality 47%). In the multicentre prospective European SOAP-study the
corresponding percentage was 25% (total in-hospital mortality 36%) (106). Authors found a
considerable variation among the European countries, with a strong correlation between the

28
frequency of sepsis and the intensive care unit mortality rates. In two large retrospective
epidemiological studies, the incidence of severe sepsis was 0.76/1000 of the population and
in-hospital mortality 31% in Australia. In the United States, the incidence of severe sepsis was
3/1000 in population and overall hospital mortality rate 29% (100, 107).
With the exception of the FINNSEPSIS-study, the occurrence and mortality rates of severe
sepsis seem to be rather similar. Most studies were made in ICUs and in adult population,
considering all patient groups admitted to intensive care (surgical and non-surgical). The
different classifications of intensive care units between countries should also be noted – ICU
and lighter step-up/ step-down units might have been classified together in these studies. The
amount of malignancies among study patients varied between 4.6% and 11.6%, but the
number of haematological patients with neutropenia was not mentioned (10, 108, 109).
An important finding in FINNSEPSIS study was that even though there were national
guidelines for the treatment of severe sepsis in adults (110) the compliance to the guidelines
was noted to be poor. This was also the case in the international setting (111, 112), even
though relative simple therapeutic interventions might save a significant number of lives (113).
It is well known that the time window for interventions in the evolution of sepsis is short. The
transition from a mild to serious situation occurs during the critical “golden hours” when
recognition and aggressive treatment provide maximal benefit in terms of outcome (114).
2.2.3. Microbiological aetiology of sepsis
Blood cultures have been positive in 30-60% of the patients (9, 10, 115) in ICU- based
sepsis studies. In most studies the percentage of positive blood cultures was less than 60% -
underlining the fact that severe sepsis must primarily be a clinical diagnosis.
Among the ICU studies including both community- and hospital-acquired infections the
respiratory tract has been the most common site of infection, followed by the abdomen, urinary
tract and skin or soft tissue infections (5, 8, 100, 109, 115, 116). In the recent FINNSEPSIS
study (10) blood cultures were positive in 40% of patients with severe sepsis. Of these, the
proportion of gram-positive bacteria was 59% and gram-negative bacteria 33%, respectively.
The most common site of infection was the respiratory system (43%) followed by intra-
abdominal (32%) and skin or soft tissue (10%) infections. In patients older than 65 years the
urinary tract has been observed to be a common site of infection (117).
Since the late 1980s, gram-positive organisms have slowly replaced gram-negative bacteria
as a cause of sepsis (116, 118). This was demonstrable in most studies during this decade (8,
107, 115) with some exceptions. In a large Chinese study (108) gram-negative microbes were
29
the most common isolates in blood cultures. This was also the situation in the study by Valles
et al (119). In that study 339 patients were admitted to ICU with community-acquired
bacteraemia (25% with sepsis, 20% with severe sepsis and 55% with septic shock). The most
common pathogens were Escherichia coli (25%), Streptococcus pneumoniae (16%) and
Staphylococcus aureus (14%).
It has been showed that initiation of effective antimicrobial therapy within the first hour
following the onset of septic shock-related hypotension is associated with an 80% survival.
Every additional hour of delay in the initiation of antimicrobial therapy decreased survival by an
average of 7.6% (5). The importance of broad coverage in the initial treatment was illustrated
by the poor prognosis of patients in whom the first line antibiotics were found to be ineffective
in sensitivity assays (120).
At presentation both the source of infection and the microbial nature of the disease are often
unknown. Antibiotic treatment should be therefore guided by symptoms and signs, bedside
clinical findings and knowledge of local bacterial resistance. The epidemiological change of
nosocomial bloodstream infections can be insidious, which was observed recently in Taiwan
and the Republic of Korea (121-123). This was characterised by the notable predominance of
gram-negative microbes with increasing antimicrobial resistance.
2.3. Markers for severe sepsis
In severe sepsis and other serious infections, the circulating levels of biomarkers depend on
the origin and extent of the infection. In addition, microbes may induce a distinct response in
various organs, resulting in a variable diversity of circulating biomarkers and mediators. It is
obvious that any infection is far too complex to be reduced to a single cutoff of any biomarker.
Nevertheless, the dynamics of biomarker levels have prognostic implications, and increasing
levels are associated with an unfavourable outcome. On the contrary, decreasing levels
suggest favourable outcome (124). Biomarkers may be valuable and helpful tools in the
diagnostic dilemma of severe sepsis, especially in distinguishing severe sepsis from less
severe forms of infections in early phase of the disease.
Various treatment strategies are effective in septic infections, but the disease should be
diagnosed early to be effectively treated. Early diagnosis with an unknown microbiological
aetiology, but early initiation of sepsis therapy is more effective than specific, but lately initiated
sepsis therapy (125). This is especially true in neutropenic sepsis, where symptoms and
clinical findings of infection may be obscure or even absent. Thus, early prognostic markers of
bacterial infections are warranted in the treatment of neutropenic patients.

30
These markers should be released and regulated independently of neutrophil cell counts and
activity of the underlying disease. An ideal prognostic marker should be also able to distinguish
septic infections from several other causes of the systemic inflammatory response syndrome.
It should also reflect the severity of the infection and distinguish periods with high risk of
complications from those with low risk (126).
Leukocyte count and leukocyte differentiation are among the oldest markers of infection, but
are useless in patients with severe neutropenia. CRP, procalcitonin (PCT) and
proinflammatory cytokines (IL-6 and IL-8) are all useful markers of inflammation. In addition,
VEGF, natriuretic peptides, lactate and procalcitonin have been a persistent interest of study.
Among other potential future candidates are lactoferrin, neopterin and prostaglandins (126).
2.3.1. C-reactive protein
CRP is a member of the acute-phase reactants, because its level rises rapidly in response
to inflammatory processes. CRP is produced by hepatocytes, predominantly under
transcriptional control by IL-6 (Table 2). About 90% of healthy population has CRP
concentrations < 3 mg/l (127). Synthesis after the inciting stimulus starts rapidly, and serum
concentrations of CRP rise above 5 mg/l by about 6 hours. The peak values are achieved in
around 48 hours. The sole determinant of circulating CRP concentration is the synthesis rate,
and it reflects directly the intensity of the pathological process stimulating CRP production
(128). When the stimulus terminates, the concentration of circulating CRP falls rapidly.
CRP production is part of the nonspecific acute-phase response to most forms of
inflammation, infection and tissue damage. Persistent increases in CRP can also occur in
chronic inflammatory disorders, including autoimmune diseases and malignancy. It has been
shown that CRP has an important role in host defence by complement action, opsonization
and by inducing phagocytosis (129, 130). CRP has been used clinically for monitoring
infections and autoimmune disorders. CRP concentrations are most useful clinically when
combined with full knowledge of all other clinical and pathological results (126, 131). Of note,
in severe liver diseases CRP is generated at a markedly lower pace than in patients without
liver pathology (132).
The use of CRP is common in many European countries, mainly because of its low costs
and easy availability in everyday clinical practise. In many studies, CRP has usually been used
as a comparator for other markers of inflammation, mainly because its well-known kinetics and
broad use in various infectious diseases (133).

31
The time from suspicion to diagnosis in septic infections is critical because uncontrolled
infections can rapidly lead to severe sepsis, with a mortality rate of 20-52% (81, 82, 141). In
many recent sepsis studies, the initial slow kinetics of CRP has diminished its value as an
early marker of septic infection. In the study by Rintala et al (142) CRP peaked 24h later than
procalcitonin (PCT) in bacteraemic patients. The finding was similar in another study (143),
where the PCT concentrations reacted more quickly than CRP to the severity of sepsis in ICU
patients. The diagnostic utility of CRP and other inflammation markers was studied in cancer
patients with suspected infection (144). Only PCT seemed to be a good marker to discriminate
bacteraemic patients from other patients.
In studies with neutropenic patients, the results are in line with the studies in sepsis patients
without known neutropenia. CRP identifies patients with infection, but when the time interval is
short (<12 hours), predictive capacity of CRP declines significantly. When CRP kinetics during
infections in leukaemia patients was evaluated, it was concluded that CRP-level over 100 mg/l
was predictive for infection (145). Manian (12) found that an increase in CRP level of > 40 mg/l
over 2 or 3 days may suggest infection. A CRP level > 200 mg/l for over 5 days during
neutropenia was associated with a mortality rate of 50%. In another study CRP levels were
significantly higher in bacteraemic haematological patients and in patients whose infection
focus was identified than in those with fever of unknown origin (11). On the other hand,
Yonemori and colleagues (13) found no predictive value for serial measurement of CRP in
their study of 47 neutropenic patients. In these studies, CRP kinetics was not compared
between periods with severe sepsis and those without.
Persson et al (14) studied prospectively the predictive value of systemic inflammation
markers to determine the clinical course of febrile neutropenic patients. CRP did not differ at
any time point between patients with and those without complications. Another study from the
same group evaluated the ability of CRP and other inflammatory markers to predict
bacteraemia during the first 48 hours of fever in neutropenic patients (146). During the first 10
hours, CRP had sensitivity of 42% and specificity of 76% for bacteraemia. The positive
predictive value was 33%. CRP reached the highest levels after 20 to 30 hours of neutropenic
fever in patients with bacteraemia. In another study there were no differences in early CRP
concentrations between bacteraemic and non-bacteraemic neutropenic patients (147).The
result was similar in the study of Sandri and colleagues (148), where PCT concentrations
increased early only in bacteraemic patients with the highest levels at day +1 after the onset of
fever. CRP reached its peak level also at day +1 after the onset of fever but could not
distinguish bacteraemic patients from non-bacteraemic patients. Based on these studies, CRP
is useless from a predictive point of view.

32
Table 2. Markers for severe sepsis discussed in this thesis (90, 95, 128, 133-140).Marker Main source T½ Nature Major activities
CRP Liver (hepatocytes) 19 hours Acute phasereactantBoth anti- andproinflammatoryproperties
Ability to bindphosphocholineand recogniseforeign pathogensActivation ofcomplementsystemInduction ofinflammatorycytokines andtissue factor inmonocytes
Procalcitonin MonocytesParenchymal cells
25-30 hours Precursor ofcalcitonin
Mediator insystemicinfections, exactfunction unknown
IL-4 Helper T cells (Th2)B cellsMast cellsBasophilsEosinophilsStromal cells
Few minutes(NA)
Anti-inflammatory Activation oflymphocytes andmonocytes
IL-6 Helper T cells (Th2)MonocytesMacrophagesEndothelial cells
< 60 minutes ProinflammatoryAnti-inflammatory
Activation oflymphocytes,differentiation of B-cells, stimulation ofthe production ofacute-phaseproteins
IL-8 T cellsMonocytesMacrophagesEndothelial cells
< 10 hours ProinflammatoryAnti-inflammatory
Chemotaxis ofneutrophils,basophils and T-cells
IL-10 MonocytesLymphocytesMacrophages
Approximately2 minutes
Anti-inflammatory Inhibits productionof proinflammatorycytokinesRegulates T- andB cell proliferationStimulates Th2-mediated immunity
VEGFs(VEGF-A,-B,-C,-D,-E,-Fand placentalgrowth factorPIGF)
LymphocytesMacrophagesPlateletsVascular smoothmuscle cellsLung epithelium
Approximately3 minutes
Hypoxia inducedmediators
AngiogenesisMediator ofvascularpermeability
NT-proBNP Inactive metaboliteof BNP, which inturn is secreted bycardiomyocytes
120 minutes Inactive metaboliteof BNP
Maintaincardiovascularhomeostasis
Abbreviations: CRP, C-reactive protein; IL, interleukine; VEGF, vascular endothelial growth factor; NT-pro-BNP, amino terminal pro-brain natriuretic peptide; BNP, brain natriuretic peptide; T½, half-life.

33
There are no prospective studies evaluating predictive capacity of CRP kinetics in relation to
development of severe sepsis in haematological patients with neutropenic fever.
2.3.2. Vascular endothelial growth factor
Vascular endothelial growth factors (VEGFs) are important signaling proteins involved in
both vasculogenesis (de novo formation of the embryonic circulatory system) and
angiogenesis (growth of blood vessels from pre-existing vasculature). VEGF is one of the most
potent factors regulating angiogenesis and microvascular permeability (149-151). VEGF
production is induced in hypoxaemic cells. When a cell is deficient in oxygen, it produces
hypoxia-inducible factor (HIF). HIF in turn stimulates the release of VEGF (152). The role of
VEGF as a mediator of vascular permeability is important in severe infections. VEGF has been
found to cause vasodilatation influenced by endothelial nitric oxidase synthase in patients with
sepsis (153). In the study of Yano and colleagues (154), experimental septic infections were
associated with time-dependent increase in circulating levels of VEGF. They also showed that
peak VEGF concentration occurred during the first 24 hours after the onset of experimental
sepsis, and the concentration of VEGF remained elevated for several days.
Two groups have reported that VEGF levels increase in patients with severe sepsis. Pickkers
and colleagues (155) studied meningococcal septic shock in children as a prototype of gram-
negative septic shock. VEGF plasma concentrations were measured during the first 48 hours
and were highest in the presence of septic shock. VEGF concentrations at admission also
correlated with the severity of infection. Van der Flier and colleagues (156) measured plasma
VEGF levels in patients with severe sepsis in the adult ICU. They found that VEGF levels were
significantly elevated in patients with severe sepsis compared with healthy controls. Moreover,
VEGF levels in non-survivors were higher than in survivors. Increased VEGF levels at study
entry also correlated with the severity of MOF during the course of disease. Karlsson and
colleagues (15) evaluated serum VEGF values in ICU patients with severe sepsis in order to
predict organ dysfunction and mortality. They found that VEGF values were elevated in
patients with severe sepsis compared with healthy controls. Low circulating VEGF levels were
associated with haematological and renal dysfunction, suggesting possible disturbed
production of VEGF in severe sepsis. Furthermore, very low concentrations of VEGF were
associated with more severe forms of organ dysfunction and mortality, possibly because of
endothelial injury.
There are no previous prospective studies available on VEGF in patients with neutropenic
fever. Kraft and colleagues (157) analysed the VEGF values of 212 patients with various

34
malignant tumours without known neutropenia and compared the results with the VEGF values
of both healthy controls and patients with non-malignant disease. Elevated levels of VEGF
were detectable in 0-20% of patients with localised cancer but in 11-69% of patients with
metastatic cancer. VEGF levels in acute infection (non-severe sepsis) were elevated
compared with levels in healthy individuals.
The pathogenesis of sepsis, including the production of VEGF, is congruent in patients with
and without neutropenia. It has been shown that in cancer patients VEGF production
correlated with platelet count after chemotherapy-induced thrombocytopenia (158).
Furthermore, a peak in VEGF production followed platelet recovery. Several other studies
have shown that circulating VEGF resides not only in platelets but also in granulocytes, mainly
in neutrophils (159-162). This might influence VEGF production in patients with neutropenic
fever.
2.3.3. Amino-terminal pro-brain natriuretic peptide
Brain natriuretic peptide (BNP) is a prohormone secreted by cardiomyocytes. Secretion is
primarily a response to the increased myocardial wall stress and is aimed to maintain
cardiovascular homeostasis through its natriuretic, diuretic and vasodilatory properties (163).
NT-proBNP is an inactive metabolite of BNP. NT-proBNP has markedly longer plasma half-life
and better stability than BNP, which makes it better applicable for clinical use (164) (Table 2).
Increased levels of both BNP and NT-proBNP have been identified as early markers of
myocardial dysfunction and increased mortality in the ICU setting (165-167). Elevated levels of
natriuretic peptides have been found to be markers of unfavourable prognosis in patients with
severe sepsis and septic shock (16, 168, 169). Varpula and colleagues (138) found that the
NT-proBNP values were frequently increased in severe sepsis and septic shock in patients
admitted to the ICU. Of note, NT-proBNP values were higher in non-survivors than survivors.
Also patients with less severe infections seem to have elevated levels of natriuretic peptides
(170).
A correlation between increased plasma levels of BNP and IL-6 in patients with septic shock
has been shown earlier and in recent studies both BNP and NT-pro-BNP secretion have been
linked to general inflammation (171). Rudiger and colleagues (172) showed a correlation
between NT-pro-BNP and CRP levels in a small group of haemodynamically unstable patients.
NT-pro-BNP or BNP levels did not differ significantly between patients with acute cardiac
failure and those with septic shock. The result was similar in a study by Shor and colleagues
(173), in which BNP levels correlated positively with CRP in septic patients without systolic
35
myocardial dysfunction. In another study the focus was in cancer patients with multiple co-
morbidities (174). The BNP-levels of these patients were elevated but without association with
volume overload or left ventricular dysfunction. Nonetheless, there was a significant
association with both sepsis and 30-day mortality in patients with markedly elevated BNP-
values. Nikolaou and colleagues (170) showed that BNP levels were elevated also in the acute
phase of community-acquired microbial infections without severe sepsis or septic shock.
There are no earlier studies of the kinetics or predictive use of NT-pro-BNP in patients with
neutropenic fever.
2.3.4. Other markers
2.3.4.1. Lactate
Plasma lactate is a result of the balance between lactate production and consumption.
Hyperlactataemia is typically present in patients with severe sepsis or septic shock. In these
patients not only high lactate but also poor lactate clearance has been recognized as an early
marker of mortality (175). Hyperlactatemia may be secondary to anaerobic metabolism due to
tissue hypoperfusion. The prognostic value of raised serum lactate levels has been well
established in patients with septic shock, especially if the high levels persist (176, 177). Serial
lactate measurements have been considered to be better markers for mortality and organ
failure than a single lactate determination (178). Evaluation of serum lactate levels is essential
to identify tissue hypoperfusion in patients who are not yet hypotensive, but who are at high
risk for septic shock.
The estimation of lactate levels in septic patients is not always straightforward. For example,
elevated lactate levels may result from decreased clearance by the liver or lactate acidosis
rather than from global hypoperfusion. In the study by Ramzi and colleagues (179) elevated
lactate (>3 mmol/l) and low serum bicarbonate (<17 mmol/l) at the onset of bacteraemia were
useful biomarkers in predicting septic shock and mortality in neutropenic patients. In a
multivariate analysis, especially two variables, pulmonary infection and serum lactate >3
mmol/l, were associated strongly with septic shock.
There are only limited data available on the kinetics or prognostic usefulness of lactate in
haematological patients with neutropenic fever. In a recent study elevated plasma lactate level
at start of neutropenic fever was not common, and did not distinguish severe sepsis. In
contrast, a high lactate level and impaired lactate decrease signified a fatal course of
neutropenic fever (180).

36
2.3.4.2. Procalcitonin
Calcitonin and its precursor procalcitonin (PCT) were initially used as a serum marker for
detection and follow-up of therapy for neuroendocrine tumours. Later on PCT levels were
found to be increased in patients with severe systemic inflammation (e.g. trauma, systemic
bacterial infection and sepsis). Levels of procalcitonin are undetectable in healthy individuals
(181).
The production and biological function of PCT involves a complex and time-dependent
mechanism. Significant production of PCT has been observed in adherent monocytes, but not
in circulating leukocytes. Monocytes produce PTC only for a limited time. Parenchymal cells
start to produce PTC after interaction with adherent monocytes. Local or systemic
inflammations affecting the parenchyma and monocyte adhesion are the preconditions for PCT
production. This explains also why PCT is induced by not only local or systemic inflammation,
but also after tissue trauma (182). In neutropenic patients, monocytes and other leukocytes are
absent, leaving tissue-based mechanisms of host defence (124). PCT elevates rapidly (within
2-4 hours) in severe forms of systemic inflammation or bacterial infections. It has been shown
in many settings that PTC serum concentrations react more rapidly than CRP concentrations
in sepsis patients (142, 147).
In Switzerland PCT has been used to guide antibiotic therapy in non-neutropenic community-
acquired pneumonia with success (183). The results have been similar when decrease in
serial PCT concentrations was used to predict favourable outcome of febrile episodes in
neutropenic haematological patients (184). In recent review by Sakr and colleagues (185) PCT
was shown to discriminate fever due to systemic forms of infection from fever of non-infectious
origin. It had only a minimal role in discriminating gram-negative from gram-positive infections.
Of note, PCT was not superior to interleukin-6 or CRP concentrations in outcome prediction in
patients with febrile neutropenia. In a large meta-analysis the results were in line with the
findings of Sakr and colleagues: although high PCT occured commonly in infection, it was also
elevated in many non-infectious conditions (186). There were also observations of febrile
septic patients with documented bacteraemia having PCT values within normal range.
Accordingly, PCT is not a specific indicator of either infection or sepsis and publications
concerning its prognostic utility have been contradictory (187-189). The authors point out that
the most commonly applied assay is not sensitive enough to detect potentially important mild
elevations or trends and that clinical studies with a more sensitive PCT assay are needed
(125, 183).

37
2.3.4.3. Interleukins
Interleukins 6 (IL-6) and 8 (IL-8) are proinflammatory cytokines, mainly produced by
monocytes. They are an important part of the cytokine cascade, together with inhibitory
cytokines (126). The kinetics of these cytokines are very fast (releasing within less than 1-2
hours), but concentrations may also decline within a short time (Table 2). IL-6 is a
multifunctional cytokine that regulates B- and T-cell function and acute-phase response such
as secretion of CRP. IL-8 is an inflammatory cytokine that mainly functions as a neutrophil
chemo-attractant and activating factor (190).
Both IL-6 and IL-8 have been demonstrated to be reliable predictors of sepsis in patients with
neutropenic fever (190). Engel and colleagues (191) showed that both IL-6 and IL-8 had
predictive value in neutropenic patients with bacteraemia. Especially IL-8 might have predictive
capacity in this respect.
Anti-inflammatory cytokines, mainly interleukin 4 (IL-4) and 10 (IL-10), are produced to down-
regulate the systemic inflammatory response in sepsis. The value of anti-inflammatory
cytokines in different studies is rather obscure. Loisa and colleagues (192) studied the anti-
infammatory response in the development of MOF in the ICU setting, but overproduction of IL-
10 was not observed. In another study the simultaneus detection of 17 different cytokines
demonstrated that both pro- and anti-inflammatory cytokines were significantly higher in
patients with septic shock than in patients with severe sepsis (193). Thus, higher cytokine
concentrations were associated with severity and evolution of organ dysfunction, but anti-
inflammatory cytokines had no specific role in this setting. In adult patients the measurement of
IL-10 was of limited value in predicting the outcome of febrile neutropenia (194).
38
3. AIMS OF THE STUDY
The aim of this study was to examine the nature of severe sepsis and possible predictive
factors of severe sepsis in neutropenic haematological patients. The specific study questions
were:
1. What are the epidemiological features, microbiological aetiology and outcome of severe
sepsis patients with AML and ASCT? (I, II)
2. Are the kinetics of CRP associated with severe sepsis in neutropenic patients with AML
and ASCT? (I, II)
3. Does serum VEGF have predictive value in severe neutropenic sepsis compared with
CRP? (III)
4. Does serum NT-proBNP have predictive value in severe neutropenic sepsis when
compared with CRP? (IV)

39
4. PATIENTS AND METHODS
4.1. Patients
4.1.1. Patients in retrospective studies (I-II)
4.1.1.1. Characteristics of patients with acute myeloid leukaemia (I)
The study included altogether 84 patients aged 70 years with AML treated with intensive
chemotherapy in the Department of Medicine, Kuopio University Hospital in 1996-2005. There
were 44 males and 40 females with a median age of 50 years at diagnosis (range 18-69
years).
4.1.1.2. Characteristics of autologous stem cell recipients (II)
The study population consisted of 319 adult patients who received ASCT at the Department
of Medicine, Kuopio University Hospital in 1996-2006. There were 189 males and 130 females,
with a median age of 55 years (range 16-73). The most common diagnosis was NHL (n=160,
50%) followed by MM (n=113, 35%). The patient and transplant characteristics are presented
in Table 3.
4.1.2. Patients in prospective studies (III-IV)
From first of December 2006 to 30th of November 2008 adult patients ( 70 years of age)
treated in the haematology ward of Kuopio University Hospital were enrolled in the prospective
part of the study. Patients were eligible if they had either AML or received high-dose
chemotherapy supported by ASCT and if they had neutropenic fever after chemotherapy.
Study III included all eligible patients treated during the first 12 months (n=42) and study IV all
eligible patients during a 24-month period (n=70). Patient characteristics and chemotherapy
given for study III are presented in Table 4 and for study IV patients in Table 5.
In study III, only the first episode of neutropenic fever was included in the study. In study IV,
fourteen patients with AML had more than one period of neutropenic fever after induction and
consolidation chemotherapy. Thus, the number of periods with neutropenic fever was 94 in 70
patients.
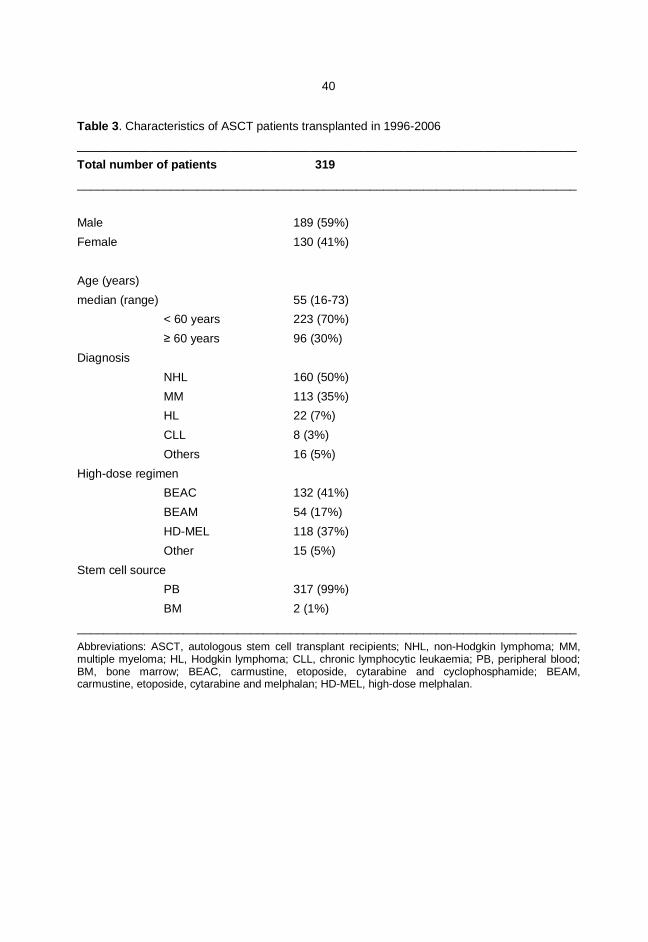
40
Table 3. Characteristics of ASCT patients transplanted in 1996-2006___________________________________________________________________________Total number of patients 319___________________________________________________________________________
Male 189 (59%)Female 130 (41%)
Age (years)median (range) 55 (16-73)
< 60 years 223 (70%) 60 years 96 (30%)Diagnosis NHL 160 (50%) MM 113 (35%) HL 22 (7%) CLL 8 (3%) Others 16 (5%)High-dose regimen BEAC 132 (41%) BEAM 54 (17%) HD-MEL 118 (37%) Other 15 (5%)Stem cell source PB 317 (99%) BM 2 (1%)___________________________________________________________________________Abbreviations: ASCT, autologous stem cell transplant recipients; NHL, non-Hodgkin lymphoma; MM,multiple myeloma; HL, Hodgkin lymphoma; CLL, chronic lymphocytic leukaemia; PB, peripheral blood;BM, bone marrow; BEAC, carmustine, etoposide, cytarabine and cyclophosphamide; BEAM,carmustine, etoposide, cytarabine and melphalan; HD-MEL, high-dose melphalan.

41
Table 4. Characteristics of patients in study III.
Number of patients 42
MaleFemale
26 (62%)16 (38%)
Age: median, range 57, 18-70
> 60 years, number (%) 16 (38%)
Diagnosis, number (%)
AML 15 (36%)
NHL 13 (31%)
MM 7 (17%)
HL 6 (14%)
CLL 1 (2%)
High-dose regimen,number (%)
BEAC 15 (36%)
BEAM 5 (12%)
HD-MEL 9 (21%)
IAT 6 (14%)
HD-AraC-Ida 5 (12%)
Mito-HDAraC 2 (5%)
Abbreviations:AML, acute myeloid leukaemia;NHL, non-Hodgkin lymphoma;MM, multiple myeloma; HL,Hodgkin lymphoma;CLL, chronic lymphocytic leukaemia;BEAC, carmustine, etoposide, cytarabine andcyclophosphamide; BEAM: carmustine, etoposide, cytarabine and melphalan; HD-MEL, high-dosemelphalan; IAT, idarubicin, cytarabine, thioguanine; HD-AraC-Ida, high-dose cytarabine, idarubicin;Mito-HDAraC, mitoxantrone, high-dose cytarabine.

42
Table 5. Characteristics of patients in study IV._________________________________________________________________________Number of patients 70Male 44 (63%)Female 26 (37%)Age: median, range 56, 18-70
60 years, number (%) 23 (33%)
Diagnosis, number (%) AML 19 (27%) NHL 25 (36%) MM 14 (20%) HL 9 (13%) Other 3 (4%)
Previous cardiovascular disease, number (%) 10 (14%)Hypertension and coronary heart disease 2Hypertension and chronic atrial fibrillation 2Previous coronary by-pass 2Cardiomyopathy (anthracycline) 2Mixed type cardiomyopathy 1Hypertension and aortic valve sclerosis 1
High-dose regimen during first period of neutropenic fever, number (%) BEAM 20 (29%) BEAC 15 (21%) HD-MEL 16 (23%) IAT 8 (11%) HDAraC-Ida 6 (9%) IdAraC-Ida 3 (4%) Mito-HDAraC 2 (3%)
Prior anthracycline therapy, number (%) 60 (86%) Doxorubicin 41 (59%) Idarubicin 19 (27%)_________________________________________________________________________
Abbreviations: NHL, non-Hodgkin lymphoma; AML, acute myeloid leukaemia; MM, multiple myeloma;HL, Hodgkin lymphoma; BEAM, carmustine, etoposide, cytarabine and melphalan; BEAC, carmustine,etoposide, cytarabine and cyclophosphamide; HD-MEL, high-dose melphalan; IAT, idarubicin,cytarabine, thioguanine; HD-AraC-Ida, high-dose cytarabine, idarubicin; IdAraC-Ida, intermediate-dosecytarabine, idarubicin; Mito-HDAraC, mitoxantrone, high-dose cytarabine.
43
4.2. Methods
4.2.1. Definitions
Neutropenic fever was defined using the criteria from the Infectious Diseases Society of
America (IDSA) for the definition of neutropenia and neutropenic fever (6). Neutropenia was
defined as a neutrophil count of <0.5 x 109/l, or a count of <1 x 109/l with a predicted decrease
to <0.5 x 109/l. Fever was defined as a single oral temperature of 38.3°C or a temperature of
38.0°C for 1 h.
Sepsis was defined as a clinical syndrome in which a systemic inflammatory response was
present with infection. Severe sepsis was present if sepsis was complicated by organ
dysfunction, hypoperfusion or hypotension. The definiton for septic hypotension included
systolic arterial pressure <90 mmHg, a mean arterial pressure <60 mmHg or a reduction in
systolic blood pressure of >40 mmHg from baseline despite adequate volume resuscitation, in
the absence of other causes of hypotension (78, 79).
4.2.2. Clinical management and supportive care measures (I-IV)
In retrospective studies (I-II) the information of chemotherapy regimen used, number of days
with neutropenia, number of febrile days (>38°C) and blood culture findings were collected
from individual patient charts for each febrile neutropenic period (Figure 1). Haematological
wards are accustomed to taking care of critically ill patients and individual monitoring charts
are familiar. These are also commonly used, which makes the collection of data much easier.
In retrospective part of the study each patient’s temperature, blood pressure and heart rate
were observed twice a day after chemotherapy by the nursing staff of the haematological ward
as a part of the normal treatment routine. In case of neutropenic fever bed-side monitoring
continued at a two or three hour interval. In case of severe sepsis, the monitoring was
constinuous. A potential localisation of infection was searched for during each neutropenic
period. In addition, re-induction chemotherapy cycles and intensive consolidation cycles were
taken into account in patients with AML.
In the prospective part of the study (studies III-IV) the clinical aim was to improve
management of haematological patients with neutropenic fever with close monitoring and
vigilant supportive care in the haematology ward setting. The start of prospective study was
preceeded by careful education of the whole nursing staff.
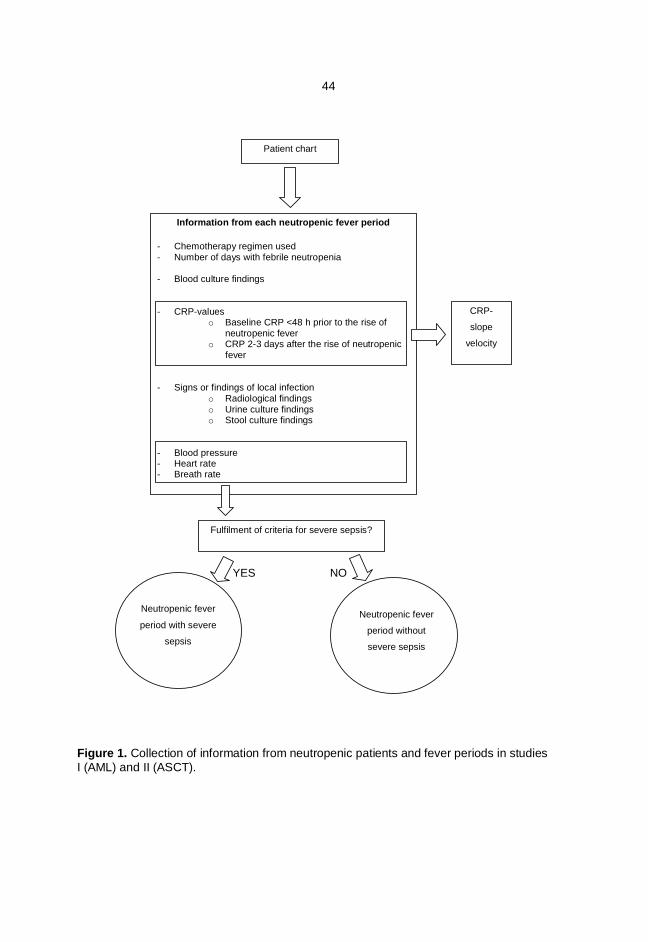
44
Information from each neutropenic fever period
- Chemotherapy regimen used- Number of days with febrile neutropenia
- Blood culture findings
- CRP-valueso Baseline CRP <48 h prior to the rise of
neutropenic fevero CRP 2-3 days after the rise of neutropenic
fever
- Signs or findings of local infectiono Radiological findingso Urine culture findingso Stool culture findings
- Blood pressure- Heart rate- Breath rate
CRP-
slope
velocity
Patient chart
Fulfilment of criteria for severe sepsis?
Neutropenic fever
period with severe
sepsis
Neutropenic fever
period without
severe sepsis
YES NO
Figure 1. Collection of information from neutropenic patients and fever periods in studiesI (AML) and II (ASCT).

45
Each patient was examined daily for signs and possible sources of infections. Special
attention was paid to features indicating the development of severe sepsis. When a patient
became neutropenic, monitoring (body temperature, blood pressure, heart rate, breath rate
and peripheral blood oxygen saturation) began bedside twice a day. From the beginning of
neutropenic fever monitoring was either hourly or continual – depending on the individual
patient situation (Table 6). Daily fluid intake (intravenous and per os) and urine output were
registered every 12 hours during the first three days of neutropenic fever by haematological
ward nursing staff. The patient’s weight was monitored once a day. The chemotherapy used,
number of days with neutropenia (<0.5 x 109/l), number of febrile days (>38°C) and blood
culture findings were also noted for each febrile neutropenic period (Figure 2). In case of fever
during neutropenia, fluid resuscitation using saline infusion was used.
Indwelling central venous catheters were used during the study period in all AML patients.
Central venous catheters were used in about 80% of ASCT recipients. Granulocyte colony-
stimulating factor (filgrastim or peg-filgrastim) was routinely used in ASCT recipients, whereas
only a minority of neutropenic AML patients received growth factors as a part of supportive
care, on an individual basis. Red blood cell concentrates were used to keep haemoglobin >80
g/l, and platelet concentrates were given routinely if the morning platelet count was less than
20 x109/l.
4.2.2.1. Chemotherapy
During the retrospective study period, patients with AML were treated with intensive
induction and consolidation chemotherapy courses according to the Finnish Leukaemia Group
prospective protocols. The chemotherapy for AML is given in the haematological wards of
university hospitals. The intensive induction course takes weeks, with long lasting neutropenia
until the bone marrow recovers. After this AML patients may leave hospital for a few days
before consolidation courses begin. Peripheral blood samples are monitored on a regular
basis. When cytopenia or neutropenic fever developes, patients return to the hospital. The
AML-92 protocol (2) (Table 7) was used for 65 patients and the AML-2003 protocol for 19
patients. In the AML-2003 trial, the induction course is according to randomisation idarubicin,
low-dose cytarabine and thioguanine (IAT) or intermediate-dose cytosine arabinoside plus
idarubicin.
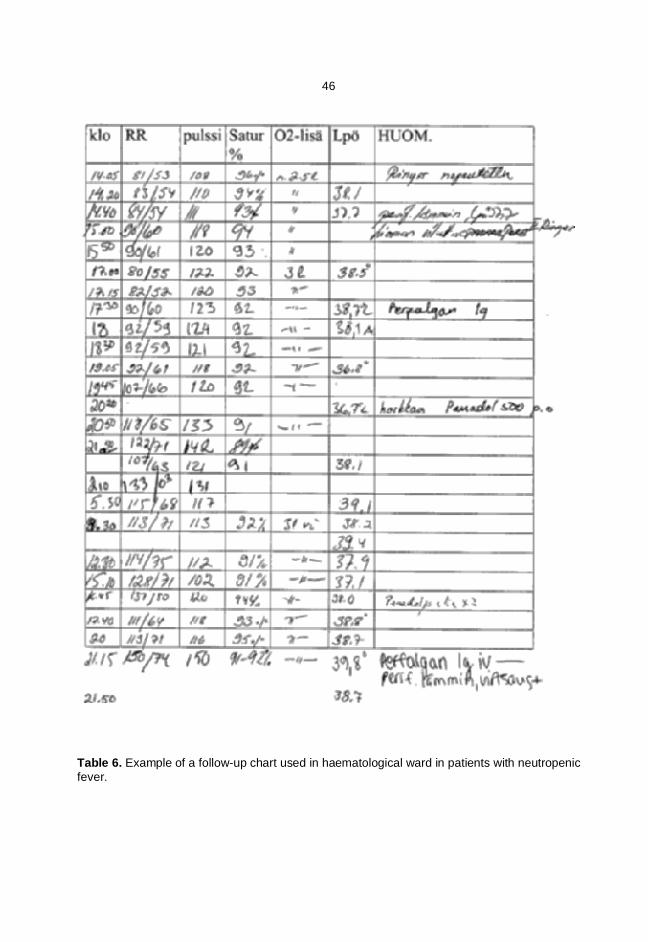
46
Table 6. Example of a follow-up chart used in haematological ward in patients with neutropenicfever.

47
Figure 2. Collection of information from neutropenic patients and fever periods in studies III(VEGF) and IV (NT-proBNP).
Information from the first
neutropenic fever period
(Study III)
Patient chart
Information from each
neutropenic fever period
(Study IV)
Neutropenic fever
with
severe sepsis
Neutropenic fever
without
severe sepsis
Neutropenic fever
with
severe sepsis
Neutropenic fever
without
severe sepsis
Information from each neutropenic fever period
Chemotherapy regimen used
Number of days with febrile neutropenia
Blood culture findings
Signs or findings of local infection
- Radiological findings
- Urine culture findings
- Stool culture findings
- Blood pressure
- Heart rate
- Breath rate
- Peripheral oxygen saturation
- Daily fluid intake and diuresis (every 12 hours)
NT-proBNP values
CRP values
VEGF values
CRP values
in case of neutropenic
fever either every one
hour or constantly
48
The second course is high-dose cytosine arabinoside plus idarubicin. Responding patients
receive risk-adapted consolidation courses all including high-dose cytosine arabinoside with an
anthracycline or mitoxantrone.
HDT supported by ASCT is given in university hospitals. Chemoterapy characteristics for
studies II-IV are presented in Tables 3-5. Additionally, in study IV, sixty patients (86%) had a
history of anthracycline treatment. Nineteen of these patients (27%) received idarubicin
(median dose 36, range 24-60 mg/m2) and 41 (59%) received doxorubicin or epirubicin
(median dose 300, range 100-500 mg/m2).
4.2.2.2. Antimicrobial therapy
In case of neutropenic fever, 2-3 blood culture sets were drawn from cubital veins at a one-
hour interval by laboratory technicians. Empirical antibiotic treatment was started immediately
after blood cultures were obtained. A combination of a broad-spectrum betalactam and an
aminoglycoside was used. Antimicrobial treatment was changed when needed, according to
the microbiological findings, radiological or clinical findings. If the fever persisted for 3-5 days,
new blood cultures were drawn, and the initial antimicrobial therapy was re-considered. In case
of mucosal symptoms during neutropenia, oral fluconazole (200 mg/d) was started. In case of
persistent fever, amphotericin B deoxycholate was given as empirical antifungal therapy. More
recently caspofungin has been used for empirical antifungal therapy. Vancomycin was
considered only if there were signs of infection in central venous catheter or if simultaneus
blood cultures revealed coagulase-negative staphylococci. No systematic antibacterial
prophylaxis was used until January 2008, when oral ciprofloxacin (500mg b.i.d) was given to
neutropenic NHL patients receiving ASCT as a part of clinical protocol.
General infection control measures (e.g. isolation policies, hospital hygiene including
cleaning and hand-washing policies) remained constant during the whole study period.
4.2.3. Laboratory methods
In the retrospective part of the study (I-II) serum concentrations of C-reactive protein (CRP)
were collected from the individual patient charts. CRP was routinely determined three times
per week during neutropenia. During clinically significant infection, CRP measurements were
performed at 1-2 day intervals.

49
Table 7. Chemotherapy protocol in the AML-92 study of the Finnish Leukaemia Group (2)
_________________________________________________________________________
Therapy Dosage Administration Days administered_________________________________________________________________________
First course (IAT)
Idarubicin 12 mg/m2 i.v., 10–15 min 1, 3, 5
Cytarabine 50 mg/m2 i.v., bolus 1
100 mg/m2 i.v., continuously 1(–7)–9
Thioguanine 75 mg/m2 p.o., twice daily 1(–7)–9
Second course (HDAraC-Ida)
Cytarabine 1500 mg (1.0 g)/m2 i.v., 3 h, twice daily 1–5
Idarubicin 8 mg/m2 i.v., 30 min 6–8
Third course (MEA)
Etoposide 100 mg/m2 i.v., 1 h 1–4
Cytarabine 1000 mg (0.5 g)/m2 i.v., 2 h, twice daily 1–4
Mitoxantrone 12 mg (8 mg)/m2 i.v., 30 min 2–5
Fourth course (Amsa-HDAraC)
Amsacrine 115 mg/m2 i.v., 2 h 1–5
Cytarabine 3000 mg/m2 i.v., 3 h, twice daily 1–2
Fifth course (HDAraC-Ida)
Cytarabine 1500 mg (1.0 g)/m2 i.v., 3 h, twice daily 1–5
Idarubicin 8 mg/m2 i.v., 10–15 min 6–8
_________________________________________________________________________
Dosage and days administered in parenthesis indicate patients 56 years old.Abbreviations: i.v, intravenously; p.o, orally.
For the prospective part of the study (III-IV), the first blood samples for the measurement of
CRP, vascular endothelial growth factor (VEGF) and amino-terminal pro-brain natriuretic
peptide (NT-proBNP) serum concentrations were drawn at the beginning of neutropenic fever
concomitantly with samples taken for blood cultures. Further samples were collected next
morning and then every 24 hours up to three or five days (Figure 3). Platelet and leukocyte
counts were routinely examined daily throughout the neutropenic period.
50
Blood samples for VEGF and NT-proBNP were centrifuged (2200 G 10 minutes) by
laboratory technicians. VEGF samples were then stored at -20°C for later analysis and NT-
proBNP samples were analysed within 12 hours.
4.2.3.1. Blood cultures
In case of neutropenic fever (neutropenia and a single oral measurement of 38.3°C or
>38°C for one hour) 2-3 blood cultures were drawn from cubital veins at 1 hour interval by
laboratory technicians. Blood cultures were processed using the automated
blood culture system Bactec 9240 (Becton Dickinson, Sparks, USA). Incubation period for both
aerobic and anaerobic bottles were 7 days and for MYCO F / Lytic bottles 42 days.
A single positive blood culture was considered significant if the microbe was a clinically
relevant cause of infection. Common skin contaminants (e.g. coagulase-negative
staphylococci) were considered significant only if they were found in two consecutive blood
cultures or if there was a concurrent skin or catheter infection.
4.2.3.2. Serum C-reactive protein
The concentration of serum CRP was measured with an immunoturbidometric method
(Otsuji, 1982, Clin Chem) using a multichannel Hitachi 717 Automatic Analyzer (Hitachi Ltd,
Tokyo, Japan) until the year 2000 and then with a Konelab60i Clinical Chemistry Analyzer (Lab
systems CLD, Konelab, Helsinki, Finland). The reference value for serum CRP in healthy
persons was <10 mg/l.
In the retrospective studies (I-II) also CRP slope velocity was analysed. For all febrile
neutropenic periods following intensive chemotherapy, baseline CRP (< 48 h prior to rise of
fever, CRP0) and the CRP level 2-3 days after the onset of fever (CRP2-3) was registered. Peak
CRP and the time from the rise of fever to the highest CRP value of a given neutropenic period
was also registered. CRP slope velocity was defined as the difference between CRP2-3 and
CRP0, divided by the number of days and expressed as mg/l/d.
CRP2-3 – CRP0CRP slope velocity = -------------------------------------- Number of days (2 or 3)
In the prospective studies (III-IV), CRP was measured at the start of neutropenic fever and
then every morning during the study period (Figure 3).
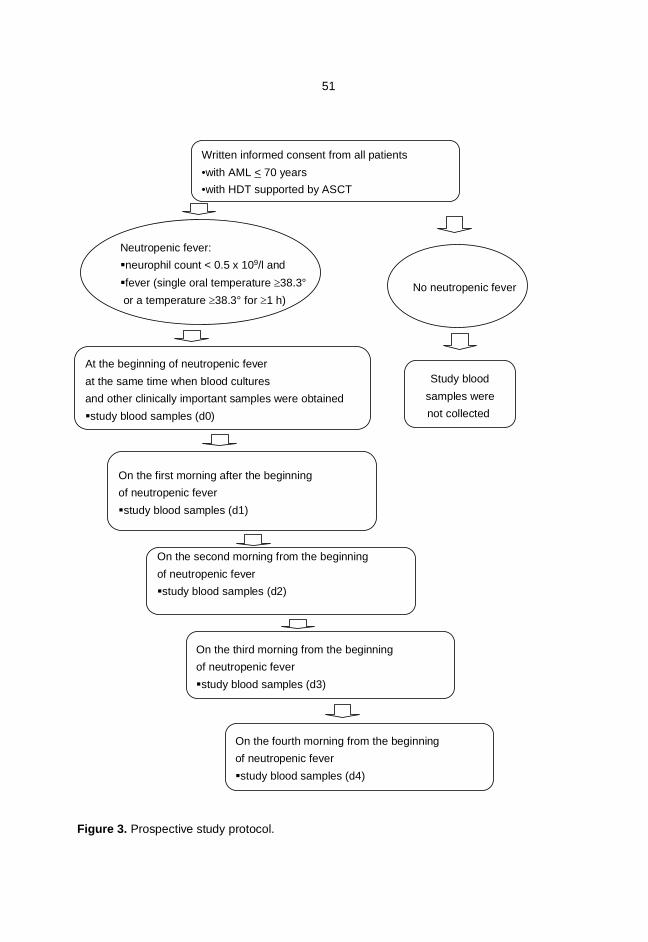
51
Figure 3. Prospective study protocol.
Written informed consent from all patients•with AML < 70 years•with HDT supported by ASCT
On the first morning after the beginningof neutropenic feverstudy blood samples (d1)
Neutropenic fever:neurophil count < 0.5 x 109/l andfever (single oral temperature 38.3°or a temperature 38.3° for 1 h)
No neutropenic fever
On the second morning from the beginningof neutropenic feverstudy blood samples (d2)
On the third morning from the beginningof neutropenic feverstudy blood samples (d3)
On the fourth morning from the beginningof neutropenic feverstudy blood samples (d4)
Study bloodsamples werenot collected
At the beginning of neutropenic feverat the same time when blood culturesand other clinically important samples were obtainedstudy blood samples (d0)
52
4.2.3.3. Serum vascular endothelial growth factor
Serum VEGF concentrations were measured using a commercial enzyme-linked
immunosorbent assay (ELISA) kit (Quantikine ®, R&D Systems; Minneapolis, MN), which
recognises the soluble isoforms (VEGF121 and VEGF165). The same VEGF ELISA method was
used and described in detail in a recent Finnish study called FINNSEPSIS (15). In brief, the
optical density at 450 nm was measured with wavelength correction at 540 nm (Multiscan RC
plate reader; Thermolabsystems, Helsinki, Finland) and serum VEGF concentration was
determined with Genesis (Life Sciences, UK) computer software capable of generating a four
parameter logistic curve fit.
The intra-assay coefficient variation (CV) for a control sample (mean concentration 345
pg/ml) was 5.7% (n=10) and for pooled serum (mean concentration 96 pg/ml) 6.5% (n=10).
The inter-assay CV for two control samples (mean concentration 167 pg/ml and 1002 pg/ml)
was 8.9% and 4.3% (n=12). For pooled serum the inter-assay CV was 8.5% (n=12). In the
FINNSEPSIS study, the samples of 30 healthy adult controls were collected. The mean age of
these controls was 36±7 years. The number of males and females was equal (M/F 15/15). The
median concentration of VEGF in the control group was 260 (IQR 126-459, range 63-809)
pg/ml, which was used as the control value in the FINNSEPSIS study (15).
4.2.3.4. Plasma amino-terminal pro-brain natriuretic peptide
Samples for the measurement of serum NT-proBNP were drawn by venipuncture into Li
heparin-containing tubes from patients lying in the supine position. Plasma was separated and
NT-proBNP was determined within 24 hours using an electrochemiluminescence
immunoassay (ECLIA, Roche Diagnostics) on a Cobas e 601 analyzer (Hitachi High
Technology Co, Tokyo, Japan). The measuring range, defined by the lower detection limit and
the maximum of the master curve provided by the manufacturer was 0.6-35 000 ng/l. The
reference values were given according to age and gender of the patients: for males under 50
years of age 0-84 ng/l, 50-65 years of age 0-194 ng/l and over 65 years of age 0-229 ng/l. For
females under 50 years of age 0-155 ng/l, 50-65 years of age 0-222 ng/l and over 65 years of
age 0-352 ng/l.

53
4.2.4. Statistical methods
Statistical analysis was performed with SPSS version 14.0 for Windows (SPSS, Inc.,
Chicago, IL, USA). For the analysis of nominal data, the Chi-square test was employed.
Continuous variables were expressed as medians with ranges (interquartile ranges or ranges
from minimum to maximum). Categorical variables were expressed as absolute numbers
(percentages).
The correlation between continuous variables was evaluated by the non-parametric
Spearman’s correlation. For single measurements, differences between subgroups were
evaluated by the Mann-Whitney U-test, and by Student’s t-test for log-transformed variables. In
study III the time period from the beginning of neutropenic fever to achieve maximal VEGF
concentration was compared to the respective time to achieve maximal CRP concentration
using Wilcoxon signed ranks test. The Youden index (sensitivity + specificity –1) (195), a
summary measure of receiver-operating-characteristics curve analysis, was used to evaluate
the goodness of CRP vs. VEGF on the first days of neutropenic fever to predict the
development of severe sepsis (a high Youden index indicates good test performance).
Repeated measures ANOVA was used to assess the impact of severe vs. non-severe sepsis
(defined as between-subjects factor) on the VEGF and CRP concentrations. The within-
subjects factor was defined as the VEGF concentration on day 0, 1, 2, and 3. The receiver-
operating characteristic (ROC) curve analysis was used to evaluate the predictive
discrimination of VEGF and CRP for severe sepsis on day 0 and day 1 of neutropenic fever.
In the study IV a logarithmic transformation was used to correct the skewed distribution of
NT-proBNP and CRP. After logarithmic transformation, a near-normal distribution was
achieved. When patient-related variables were evaluated, only the first episode of neutropenic
fever for each patient was included in the analyses. When fever period-related variables were
evaluated, all fever periods were included. ANOVA for repeated measurements was used to
evaluate possible differences between subgroups in NT-proBNP and CRP levels during days
0-3. A p-value < 0.05 was considered significant.
4.3. Approval of the Ethics Committee
The study was approved by the Ethic Committee of the Kuopio University Hospital. All study
patients gave their written informed consent.
54
5. RESULTS
5.1. Retrospective studies (I-II)
5.1.1 Epidemiological features of severe sepsis
In study I, there were altogether 290 neutropenic periods in 84 AML patients (median 3,
range 1-7). In 280 periods (97%) neutropenic fever was present. Severe sepsis was observed
in 35 periods (13%) and in 13 periods (5% of all neutropenic fever periods) severe sepsis led
to ICU admission (Table 8). In 17 periods (49%) the criteria for severe sepsis was hypotension
despite of fluid resuscitation. In 11 periods (31%) the criteria for severe sepsis was septic
shock and in 3 periods (8%) respiratory failure. In 3 periods (8%) septic shock developed into
MOF. One patient (3%) died due to septic shock on the way to the hospital (Table 9).
The median time from the onset of the fever to the point where criteria for severe sepsis
were met was 2 days (range 0-39). Thirteen patients were treated in the ICU due to severe
sepsis, with a median stay of 3 days (1-42). Five patients (38%) recovered and eight patients
died due to irreversible septic shock a median of 2 days (1-7) after admission to the ICU.
After the first induction course in study I, neutropenic fever was found in 80 out of 84 patients
(95%). Severe sepsis was observed in 10 patients (13%) and 7 patients (8%) were admitted to
the ICU. Four patients (5%) died after the first induction course due to infectious complications.
In study II there were 319 ASCT recipients with 265 (83%) febrile neutropenic periods.
Because of the treatment protocol, only one period of neutropenic fever was included for each
patient. Severe sepsis was observed in 17 patients (5%). In 5 patients (29%) the criteria for
severe sepsis was hypotension despite fluid resuscitation. In 12 patients (71%) the criteria for
severe sepsis was septic shock (Table 10). In nine occasions (3%) severe sepsis led to ICU
admission.
The median time from the onset of fever to the point, where criteria for severe sepsis were
met was 3 days (range 1-10). The median time to ICU admission was 7 days after the start of
fever (range 2-25), and the median treatment time at ICU was 3 days (1-17). Seven patients
(78%) died due to irreversible septic shock a median of 2.5 days (1-12) after the admission to
ICU. Only two patients treated in the ICU (22%) recovered.
Severe sepsis was the most common severe early (<30 d) complication in ASCT recipients
(17/20 patients, 85%). Other severe early complications included pneumonia (n=1), severe
cardiotoxicity (n=1) and a combination of liver and cardiac failure (n=1).

55
Table 8. Studies I-IV
Study I Study II Study III Study IV
_________________________________________________________________________Number of patients 84 319 42 70
Number of patients with severe sepsis 30 (36%) 17 (5%) 5 (12%) 13 (19%)
Number of neutropenic feverperiods 280 265 42 94
Number of periods with severe sepsis 35 (13%) 17 (5%) 5 (12%) 13 (14%)
Length of neutropenia, daysmedian (range)
Periods with severe sepsis 23 (7-85) 11 (6-25) 9 (3-25) 12 (3-25) Periods without severe sepsis 24 (5-227) 9 (3-63) 10 (4-23) 10 (4-30)
Mortality associatedwith severe sepsis 9/84 (11%) 9/319 (2%) 1/42 (2%) 2/70 (3%)
Case fatality rate for periodswith severe sepsis 9/35 (27%) 9/17 (53%) 1/5 (20%) 2/13 (15%)________________________________________________________________________
In study I neutropenic septic infection was the cause of death in 9 patients. Thus mortality
due to neutropenic sepsis was 11% (9/84). Neutropenic sepsis was suspected cause of death
also in 2 other patients: one patient (number 27 in table 9) died due to a septic shock outside
hospital (paramedic care) and one patient (number 26 in table 9) with refractory leukaemia
died without ICU admission in the hematology ward. The case fatality rate for periods with
severe sepsis was 27% (9/35). In study II neutropenic sepsis was the cause of death in 9
patients and mortality due to neutropenic sepsis was 2% (9/319). The case fatality rate for
periods with severe sepsis was 53% (9/17). The mortality due to severe sepsis was higher in
NHL patients when compared to other patient groups (6% vs. 0%, p=0.003).
5.1.2 Microbiological findings and site of infection
In study I clinically significant microbiological findings were found by blood cultures in 165 out
of 280 episodes with neutropenic fever (59%) (Table 11). Gram-positive cocci were the most
commonly identified causes of neutropenic fever (94 episodes, 57%), followed by gram-

56
negative rods (70 episodes, 43%). Only one fungal sepsis was observed during this time. In
cases of severe sepsis, gram-negative rods were found in 15/35 of periods (43%).
In study II clinically significant microbiological growth in blood cultures was seen in 68 out of
265 periods with neutropenic fever (26%) (Table 11). Gram-positive cocci (44 episodes, 65%)
were the most common identified cause of neutropenic fever, followed by gram-negative rods
(23 episodes, 34%). Only one fungal bloodstream infection was found, concomitantly with
gram-positive bacteraemia. In cases of severe sepsis, gram-positive cocci were found in 7 out
of 17 periods (41%). Gram- negative rods were found in six periods (35%). Pseudomonas
aeruginosa was the most common (5 episodes, 30%).
The lungs and upper respiratory airways were the most common site of infection (48
episodes, 17%) in study I. The number of catheter-related infections was 45 (16%) and skin
(including perineal region) infections 17 (6%). In study II, the localisation of infection remained
in most cases unknown. The percentage of catheter-related infections was 11%.
5.1.3. Factors associated with severe sepsis
In both studies, the neutropenic febrile periods were divided into those with and those
without severe sepsis. In study I there were no differences in the median length of neutropenia,
but in study II the median length of neutropenia was longer in ASCT recipients with severe
sepsis (11 vs. 9, p=0.05).
In study I gram-negative bacteria were found more often in blood cultures (43% vs. 22%,
p=0.03) and blood culture findings were more often positive (66% vs. 58%, NS) in periods with
severe sepsis than those without. In study II severe sepsis was more common in patients with
NHL than in other patients (9% vs. 3%, NS). Patients with severe sepsis were also older than
those without (59 vs. 55, p=0.007). Blood culture findings were significantly more often positive
(76% vs. 22%, p<0.001) and gram-negative bacteria were found more often (35% vs. 7%,
p=0.001) among patients with severe sepsis than those without. Of note, Pseudomonas
aeruginosa was found in 30% (n=5) of patients with severe sepsis and only in 1% (n=3) of
those without severe sepsis (p<0.001).
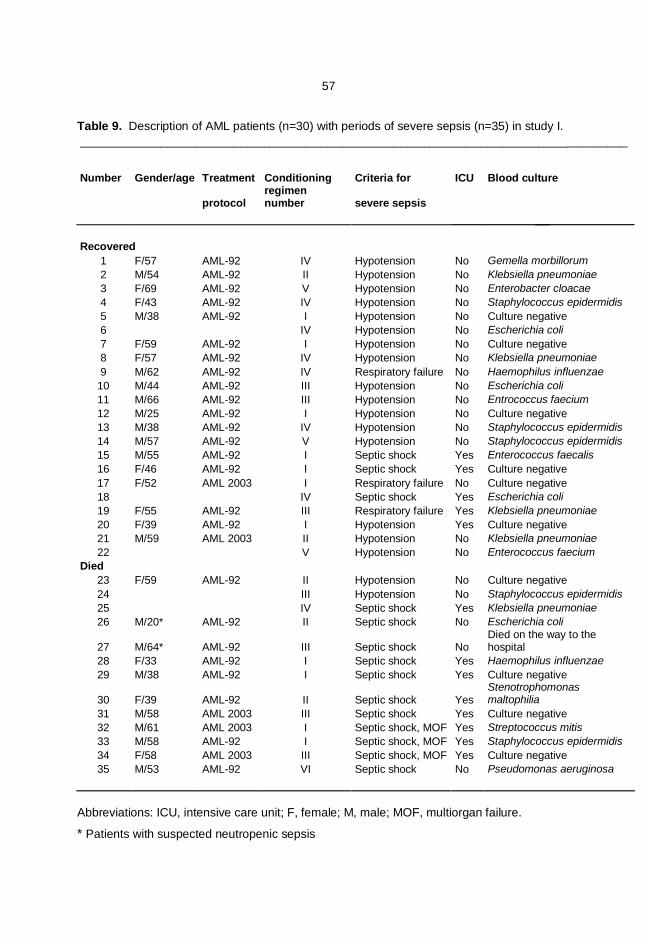
57
Table 9. Description of AML patients (n=30) with periods of severe sepsis (n=35) in study I.____________________________________________________________________________
Number Gender/age Treatment Conditioning Criteria for ICU Blood culture
protocolregimennumber severe sepsis
Recovered1 F/57 AML-92 IV Hypotension No Gemella morbillorum2 M/54 AML-92 II Hypotension No Klebsiella pneumoniae3 F/69 AML-92 V Hypotension No Enterobacter cloacae4 F/43 AML-92 IV Hypotension No Staphylococcus epidermidis5 M/38 AML-92 I Hypotension No Culture negative6 IV Hypotension No Escherichia coli7 F/59 AML-92 I Hypotension No Culture negative8 F/57 AML-92 IV Hypotension No Klebsiella pneumoniae9 M/62 AML-92 IV Respiratory failure No Haemophilus influenzae
10 M/44 AML-92 III Hypotension No Escherichia coli11 M/66 AML-92 III Hypotension No Entrococcus faecium12 M/25 AML-92 I Hypotension No Culture negative13 M/38 AML-92 IV Hypotension No Staphylococcus epidermidis14 M/57 AML-92 V Hypotension No Staphylococcus epidermidis15 M/55 AML-92 I Septic shock Yes Enterococcus faecalis16 F/46 AML-92 I Septic shock Yes Culture negative17 F/52 AML 2003 I Respiratory failure No Culture negative18 IV Septic shock Yes Escherichia coli19 F/55 AML-92 III Respiratory failure Yes Klebsiella pneumoniae20 F/39 AML-92 I Hypotension Yes Culture negative21 M/59 AML 2003 II Hypotension No Klebsiella pneumoniae22 V Hypotension No Enterococcus faecium
Died23 F/59 AML-92 II Hypotension No Culture negative24 III Hypotension No Staphylococcus epidermidis25 IV Septic shock Yes Klebsiella pneumoniae26 M/20* AML-92 II Septic shock No Escherichia coli
27 M/64* AML-92 III Septic shock NoDied on the way to thehospital
28 F/33 AML-92 I Septic shock Yes Haemophilus influenzae29 M/38 AML-92 I Septic shock Yes Culture negative
30 F/39 AML-92 II Septic shock YesStenotrophomonasmaltophilia
31 M/58 AML 2003 III Septic shock Yes Culture negative32 M/61 AML 2003 I Septic shock, MOF Yes Streptococcus mitis33 M/58 AML-92 I Septic shock, MOF Yes Staphylococcus epidermidis34 F/58 AML 2003 III Septic shock, MOF Yes Culture negative35 M/53 AML-92 VI Septic shock No Pseudomonas aeruginosa
Abbreviations: ICU, intensive care unit; F, female; M, male; MOF, multiorgan failure.
* Patients with suspected neutropenic sepsis
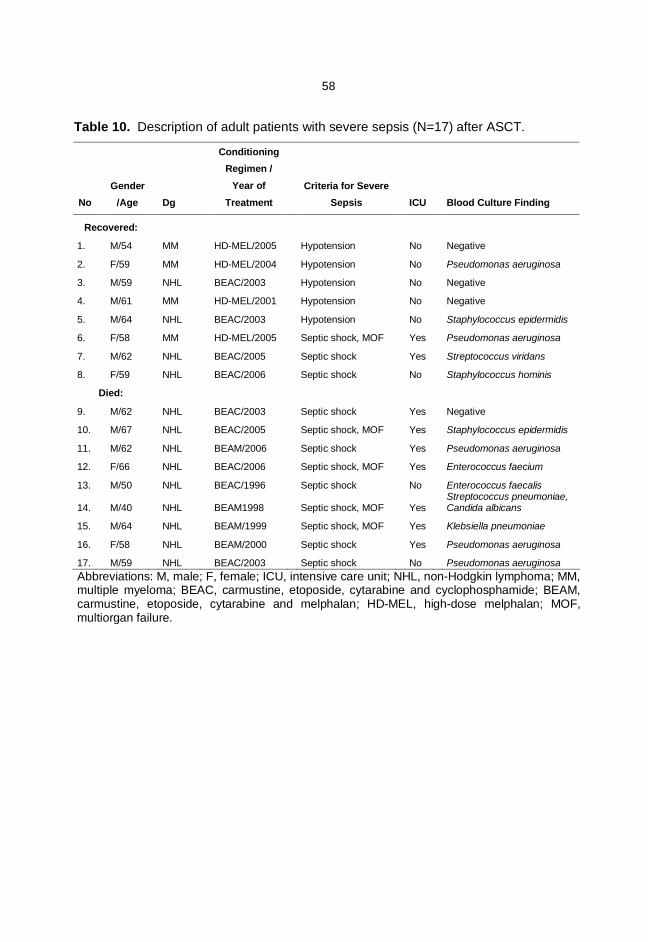
58
Table 10. Description of adult patients with severe sepsis (N=17) after ASCT.
NoGender
/Age Dg
ConditioningRegimen /
Year ofTreatment
Criteria for SevereSepsis ICU Blood Culture Finding
Recovered:
1. M/54 MM HD-MEL/2005 Hypotension No Negative
2. F/59 MM HD-MEL/2004 Hypotension No Pseudomonas aeruginosa
3. M/59 NHL BEAC/2003 Hypotension No Negative
4. M/61 MM HD-MEL/2001 Hypotension No Negative
5. M/64 NHL BEAC/2003 Hypotension No Staphylococcus epidermidis
6. F/58 MM HD-MEL/2005 Septic shock, MOF Yes Pseudomonas aeruginosa
7. M/62 NHL BEAC/2005 Septic shock Yes Streptococcus viridans
8. F/59 NHL BEAC/2006 Septic shock No Staphylococcus hominis
Died:
9. M/62 NHL BEAC/2003 Septic shock Yes Negative
10. M/67 NHL BEAC/2005 Septic shock, MOF Yes Staphylococcus epidermidis
11. M/62 NHL BEAM/2006 Septic shock Yes Pseudomonas aeruginosa
12. F/66 NHL BEAC/2006 Septic shock, MOF Yes Enterococcus faecium
13. M/50 NHL BEAC/1996 Septic shock No Enterococcus faecalis
14. M/40 NHL BEAM1998 Septic shock, MOF YesStreptococcus pneumoniae,Candida albicans
15. M/64 NHL BEAM/1999 Septic shock, MOF Yes Klebsiella pneumoniae
16. F/58 NHL BEAM/2000 Septic shock Yes Pseudomonas aeruginosa
17. M/59 NHL BEAC/2003 Septic shock No Pseudomonas aeruginosaAbbreviations: M, male; F, female; ICU, intensive care unit; NHL, non-Hodgkin lymphoma; MM,multiple myeloma; BEAC, carmustine, etoposide, cytarabine and cyclophosphamide; BEAM,carmustine, etoposide, cytarabine and melphalan; HD-MEL, high-dose melphalan; MOF,multiorgan failure.
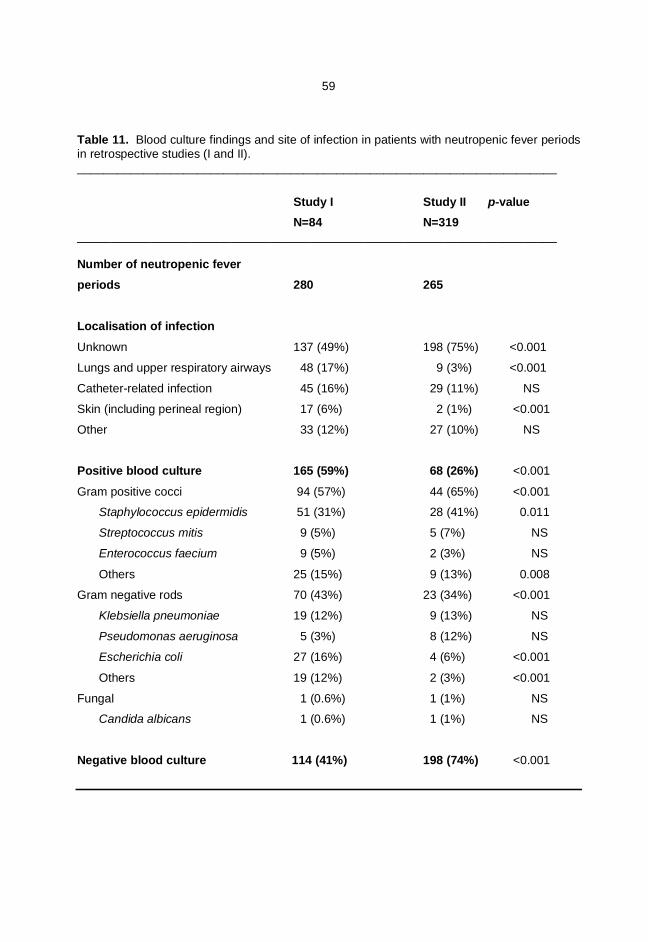
59
Table 11. Blood culture findings and site of infection in patients with neutropenic fever periodsin retrospective studies (I and II).________________________________________________________________________
Study I Study II p-value N=84 N=319________________________________________________________________________
Number of neutropenic feverperiods 280 265
Localisation of infection
Unknown 137 (49%) 198 (75%) <0.001
Lungs and upper respiratory airways 48 (17%) 9 (3%) <0.001
Catheter-related infection 45 (16%) 29 (11%) NS
Skin (including perineal region) 17 (6%) 2 (1%) <0.001
Other 33 (12%) 27 (10%) NS
Positive blood culture 165 (59%) 68 (26%) <0.001
Gram positive cocci 94 (57%) 44 (65%) <0.001
Staphylococcus epidermidis 51 (31%) 28 (41%) 0.011
Streptococcus mitis 9 (5%) 5 (7%) NS
Enterococcus faecium 9 (5%) 2 (3%) NS
Others 25 (15%) 9 (13%) 0.008
Gram negative rods 70 (43%) 23 (34%) <0.001
Klebsiella pneumoniae 19 (12%) 9 (13%) NS
Pseudomonas aeruginosa 5 (3%) 8 (12%) NS
Escherichia coli 27 (16%) 4 (6%) <0.001
Others 19 (12%) 2 (3%) <0.001
Fungal 1 (0.6%) 1 (1%) NS
Candida albicans 1 (0.6%) 1 (1%) NS
Negative blood culture 114 (41%) 198 (74%) <0.001
60
5.1.4. Serum C-reactive protein in relation to severe sepsis
In study I the median time from the onset of the fever to peak CRP value was 4 days (range
1-39). The median peak CRP value was higher in patients with severe sepsis (261 mg/l vs.
153 mg/l, p<0.001). CRP2-3 was higher in patients with severe sepsis (190 mg/l vs. 96 mg/l,
p<0.001) than those without. In this study the CRP slope velocity was steeper in patients with
severe sepsis (48 vs. 34 mg/l/d, p= 0.02) (Table 12).
In study II the median time from the onset of fever to the peak CRP value was 3 days (range
1-7). CRP2-3 was higher in patients with severe sepsis (148 mg/l vs. 90 mg/l, p<0.001) as well
as the median peak CRP value (217 mg/l vs. 111 mg/l, p<0.001). The CRP slope velocity was
again found to be steeper in patients with severe sepsis (54 vs. 30 mg/l/d, p= 0.007) (Table
12).
5.2. Serum vascular endothelial growth factor in patients with neutropenic
fever: a comparison with C-reactive protein (III)
5.2.1. Epidemiological features of severe sepsis
All patients with severe sepsis had received ASCT for NHL. The median time after the onset
of fever to the fulfillment of the criteria for severe sepsis was 1 day (range 1-3). The diagnostic
criteria for severe sepsis were fulfilled in five out of 42 patients (12%) (Table 8): one of them
had septic shock requiring vasopressor support in the ICU, one patient had septic respiratory
failure requiring CPAP ventilation and three patients had fluid-responsive hypotension. One
patient (2%) died due to septic shock in the ICU during the first day after admission (Table 13).
5.2.2. Microbiological findings and site of infection
Blood cultures remained negative in the majority of the patients (36/42, 85%). Positive
findings in blood cultures included Staphylococcus epidermidis (n=3) and Staphylococcus
haemolyticus, Enterobacter cloacae and Escherichia coli, one each. The lungs were the most
common site of infection (n=10, 24%), followed by skin infections (including perineal region)
(n=8, 19%). The percentage of catheter related infections was 10%. In 18 periods (43%), the
site of infection remained unknown.

61
Table 12. Comparison of CRP in neutropenic fever periods with or without severesepsis in studies I and II.
Study I Study II
With
severe sepsis
Without
severe
sepsis
p
With
severe
sepsis
Without
severe
sepsis
P
N=35 N=245 N=17 N=248
Baseline CRP (mg/l)
median (range)17 (5-194) 24 (5-227) NS 27 (5-127) 15 (5-118) NS
CRP (mg/l) 2 to 3
days median (range)190 (26-379) 96 (3-359) <0.001 148 (76-375) 90 (5-253) <0.001
Peak CRP (mg/l)
median (range)261 (57-563) 153 (22-492) <0.001 217 (76-545) 111 (5-304) <0.001
Time to peak CRP
(d) median (range)4 (1-39) 5 (1-59) NS 3 (1-7) 3 (0-13) NS
CRP slope velocity
(mg/l/day) median
(range)
48 (8-167) 34 (0-162) 0.02 54 (4-120) 30 (0-125) 0.007
Abbreviations: CRP, C-reactive protein.
5.2.3. C-reactive protein
The median CRP concentration was 35 mg/l (range 5-253 mg/l) at the beginning of the fever
(d0), 65 mg/l (range 11-234 mg/l) on day 1 (d1), 83 mg/l (range 7-257 mg/l) on day 2 (d2) and
82 mg/l (range 12-241 mg/l) on day 3 (d3) in the whole group of patients.
The peak concentration of CRP was achieved on d0 in 10%, on d1 in 19%, on d2 in 40% and
on d3 in 31% of the patients. There were no statistically significant differences in CRP values
on any day between the groups with severe and non-severe sepsis (Table 14). In the analysis
of variance of repeated measures the overall difference in CRP between patients with and
without severe sepsis was not statistically significant either (p=0.344).
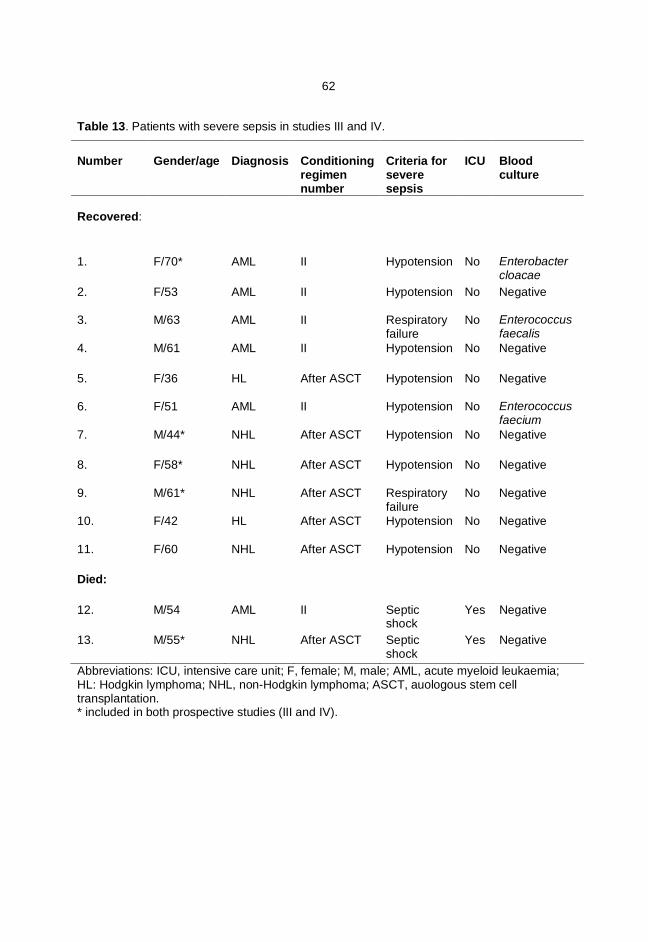
62
Table 13. Patients with severe sepsis in studies III and IV.
Number Gender/age Diagnosis Conditioningregimennumber
Criteria forseveresepsis
ICU Bloodculture
Recovered:
1. F/70* AML II Hypotension No Enterobactercloacae
2. F/53 AML II Hypotension No Negative
3. M/63 AML II Respiratoryfailure
No Enterococcusfaecalis
4. M/61 AML II Hypotension No Negative
5. F/36 HL After ASCT Hypotension No Negative
6. F/51 AML II Hypotension No Enterococcusfaecium
7. M/44* NHL After ASCT Hypotension No Negative
8. F/58* NHL After ASCT Hypotension No Negative
9. M/61* NHL After ASCT Respiratoryfailure
No Negative
10. F/42 HL After ASCT Hypotension No Negative
11. F/60 NHL After ASCT Hypotension No Negative
Died:
12. M/54 AML II Septicshock
Yes Negative
13. M/55* NHL After ASCT Septicshock
Yes Negative
Abbreviations: ICU, intensive care unit; F, female; M, male; AML, acute myeloid leukaemia;HL: Hodgkin lymphoma; NHL, non-Hodgkin lymphoma; ASCT, auologous stem celltransplantation.* included in both prospective studies (III and IV).
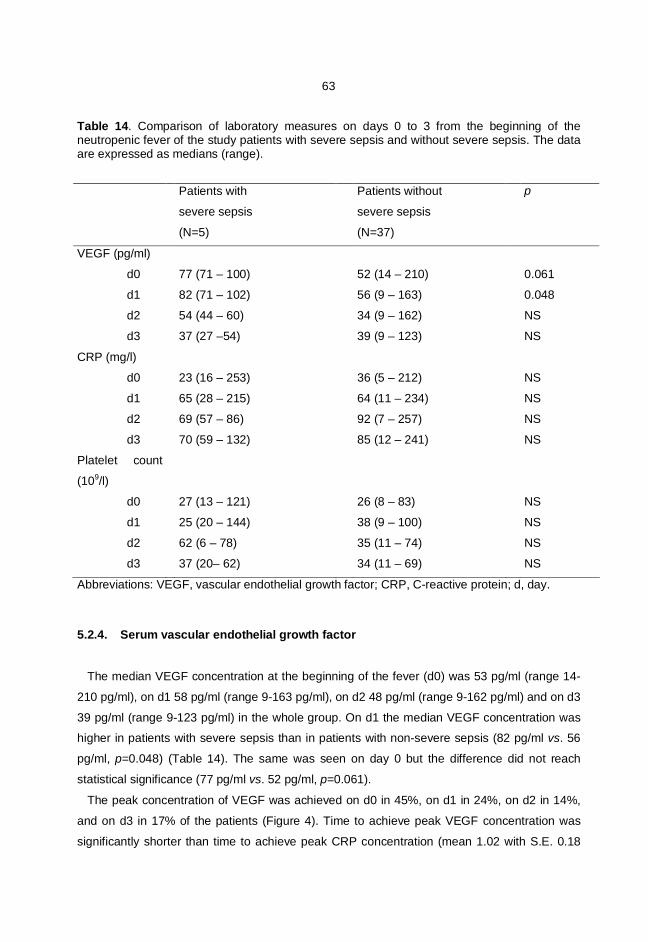
63
Table 14. Comparison of laboratory measures on days 0 to 3 from the beginning of theneutropenic fever of the study patients with severe sepsis and without severe sepsis. The dataare expressed as medians (range).
Patients with
severe sepsis
(N=5)
Patients without
severe sepsis
(N=37)
p
VEGF (pg/ml)
d0 77 (71 – 100) 52 (14 – 210) 0.061
d1 82 (71 – 102) 56 (9 – 163) 0.048
d2 54 (44 – 60) 34 (9 – 162) NS
d3 37 (27 –54) 39 (9 – 123) NS
CRP (mg/l)
d0 23 (16 – 253) 36 (5 – 212) NS
d1 65 (28 – 215) 64 (11 – 234) NS
d2 69 (57 – 86) 92 (7 – 257) NS
d3 70 (59 – 132) 85 (12 – 241) NS
Platelet count
(109/l)
d0 27 (13 – 121) 26 (8 – 83) NS
d1 25 (20 – 144) 38 (9 – 100) NS
d2 62 (6 – 78) 35 (11 – 74) NS
d3 37 (20– 62) 34 (11 – 69) NS
Abbreviations: VEGF, vascular endothelial growth factor; CRP, C-reactive protein; d, day.
5.2.4. Serum vascular endothelial growth factor
The median VEGF concentration at the beginning of the fever (d0) was 53 pg/ml (range 14-
210 pg/ml), on d1 58 pg/ml (range 9-163 pg/ml), on d2 48 pg/ml (range 9-162 pg/ml) and on d3
39 pg/ml (range 9-123 pg/ml) in the whole group. On d1 the median VEGF concentration was
higher in patients with severe sepsis than in patients with non-severe sepsis (82 pg/ml vs. 56
pg/ml, p=0.048) (Table 14). The same was seen on day 0 but the difference did not reach
statistical significance (77 pg/ml vs. 52 pg/ml, p=0.061).
The peak concentration of VEGF was achieved on d0 in 45%, on d1 in 24%, on d2 in 14%,
and on d3 in 17% of the patients (Figure 4). Time to achieve peak VEGF concentration was
significantly shorter than time to achieve peak CRP concentration (mean 1.02 with S.E. 0.18

64
days vs. mean 1.93 days with S.E. 0.15 days, p=0.002). On d0 and d1 VEGF seems to
distinguish the groups with severe and without severe sepsis better than CRP (Table 14,
Figure 5). There was no significant correlation between VEGF and platelet levels at any time
point. There were no statistically significant correlations between CRP and VEGF levels,
either. In the analysis of variance of repeated measures the overall difference in VEGF
between patients with and without severe sepsis was not statistically significant (p=0.310).
The advantage of CRP compared to VEGF in the prediction of severe sepsis was evaluated
based on receiver operating characteristics curve analysis (ROC) and the Youden index. In the
ROC curve analysis, the AUC for CRP was 0.56 (95% CI 0.40-0.72, p=0.480) on day 0 and
0.49 (95% CI 0.33-0.64, p=0.880) on day 1. AUC for VEGF on day 0 was 0.76 (95% CI 0.62-
0.90, p=0.060) and 0.80 (0.67-0.94 p=0.048) on day 1 (Figure 6). The predictive capacity of
VEGF was better for severe sepsis during the first 24 hours after the beginning of neutropenic
fever.
5.3. Serum amino-terminal pro-brain natriuretic peptide in patients withneutropenic fever: a comparison with C-reactive protein (IV)
5.3.1. Epidemiological features of severe sepsis
There were altogether 70 patients with 94 episodes of neutropenic fever when all
neutropenic fever periods were included (fourteen patients with AML had more than one period
of neutropenic fever). The diagnostic criteria for severe sepsis were fulfilled in 13/94
neutropenic fever periods (14%) (Table 8). As it is shown in table 13 there were only one
neutropenic fever period with severe sepsis for each patient. In 9 patients (69%, 9/13) the
criteria for severe sepsis was hypotension despite of fluid resuscitation. In 2 patients (15%,
2/13) the criteria for severe sepsis was septic shock and in 2 patients (15%, 2/13) respiratory
failure. Two patients (15% of the patients with severe sepsis) died due to septic shock in
intensive care unit; one ASCT recipient one day after admission and one after second
laparotomy because of appendicitis while still neutropenic following the second induction
course for AML. The median time after the onset of fever to the point when the criteria for
severe sepsis were fulfilled was 1 day (range 1-7).
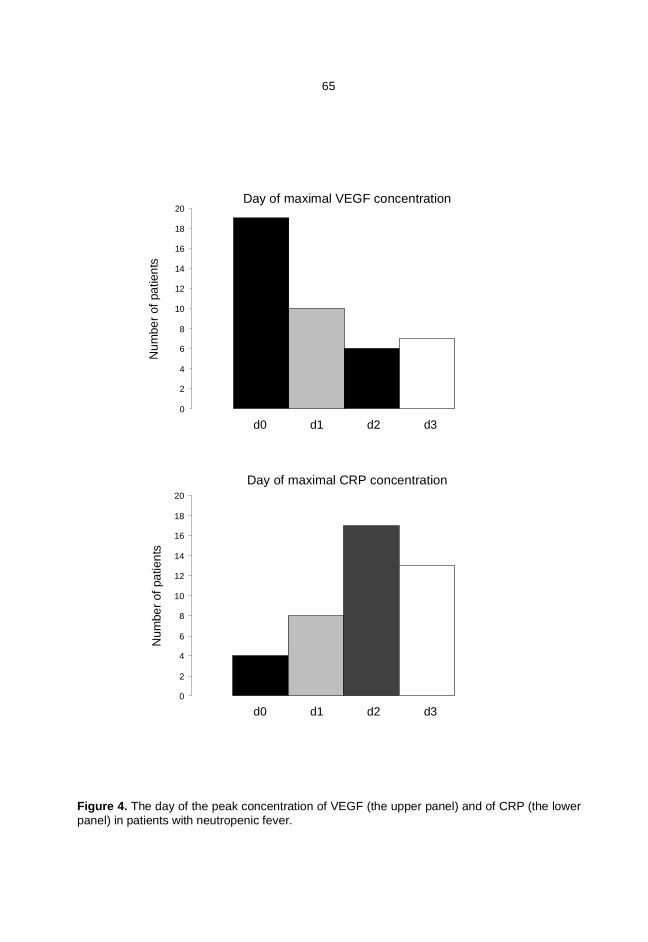
65
Figure 4. The day of the peak concentration of VEGF (the upper panel) and of CRP (the lowerpanel) in patients with neutropenic fever.
0
2
4
6
8
10
12
14
16
18
20
0
2
4
6
8
10
12
14
16
18
20
Num
ber o
f pat
ient
sN
umbe
r of p
atie
nts
d0 d1 d2 d3
d0 d1 d2 d3
Day of Maximal CRP concentration
Day of Maximal VEGF concentrationDay of maximal VEGF concentration
Day of maximal CRP concentration
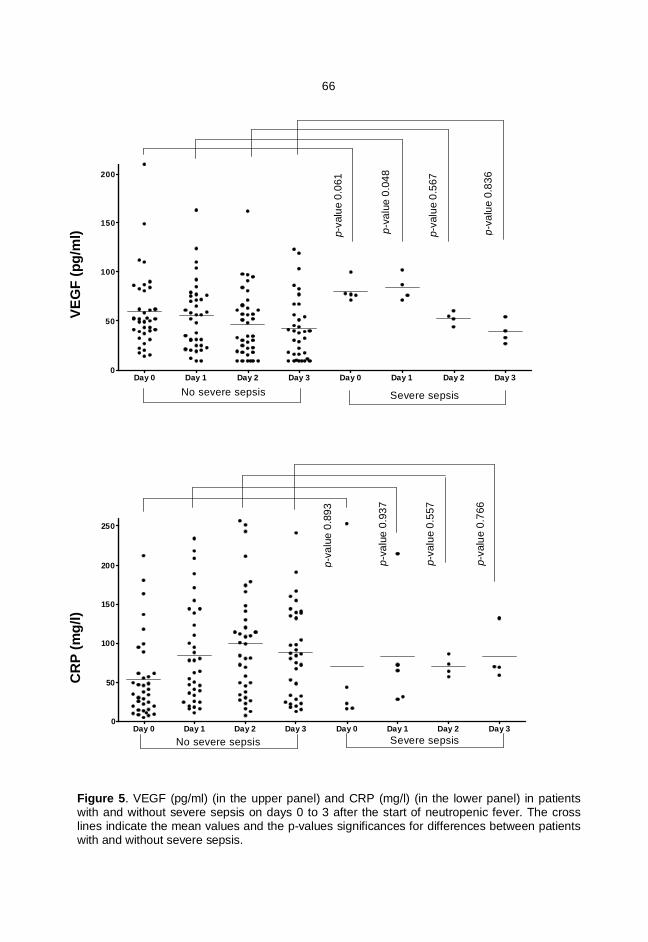
66
Figure 5. VEGF (pg/ml) (in the upper panel) and CRP (mg/l) (in the lower panel) in patientswith and without severe sepsis on days 0 to 3 after the start of neutropenic fever. The crosslines indicate the mean values and the p-values significances for differences between patientswith and without severe sepsis.
VEGF
Day 0 Day 1 Day 2 Day 3 Day 0 Day 1 Day 2 Day 30
50
100
150
200
VEG
F(pg
/ml)
CRP
Day 0 Day 1 Day 2 Day 3 Day 0 Day 1 Day 2 Day 30
50
100
150
200
250
CRP
(mg/
l)
VEGF No severe sepsis Severe sepsis
CRP No severe sepsis Severe sepsis
p = 0.310
p = 0.344
p-va
lue
0.06
1
p-va
lue
0.04
8
p-va
lue
0.56
7
p-va
lue
0.83
6
p-va
lue
0.89
3
p-va
lue
0.93
7
p-va
lue
0.55
7
p-va
lue
0.76
6
No severe sepsis
Severe sepsisNo severe sepsis
Severe sepsis
CR
P (m
g/l)
VE
GF
(pg/
ml)

67
Figure 6. In the ROC curve analysis for VEGF, AUC was 0.80 (0.67-0.94), p=0.048 on day1 to discriminate between severe and non-severe sepsis among neutropenic fever periods.The diagonal line (with dashes) represents results no better than chance.

68
5.3.2. Microbiological findings and site of infection
Blood cultures were positive in 22 (23%) of the periods with neutropenic fever. Positive
findings included Staphylococcus epidermidis (n=4), Escherichia coli (n=3), Klebsiella
pneumoniae (n=2), Enterobacter cloacae (n=2), Rothia mucilaginosa (n=2) and
Staphylococcus haemolyticus, Staphylococcus aureus, Streptococcus pneumoniae,
Streptococcus mitis, Enterococcus faecalis, Enterococcus faecium, Pseudomonas aeruginosa,
Stenotrophomonas maltophilia and Morganella morganii, one each.
In about half of the neutropenic febrile periods the site of infection remained unknown. The
lungs and upper respiratory airways were the most common known sites of infection (19
episodes, 20%), followed by skin infections (including the perineal region) (16 episodes, 16%)
and catheter-related infections (8 episodes, 9%).
5.3.3. Factors associated with severe sepsis
The median age of patients in the subgroups with and without severe sepsis was similar. The
median length of neutropenia was 10 days (range 3-30) without statistically significant
difference between periods with and without severe sepsis.
The frequency of severe sepsis was similar in patients with and without previous
cardiovascular disease. The incidence of severe sepsis was 14% (6/43) in AML patients and
14% (7/51) in ASCT recipients of all episodes of neutropenic fever.
5.3.4. C-reactive protein
The peak CRP level was achieved on d2 (Figure 7). The median CRP was 35 (17-61) mg/l
on d0, 79 (38-79) mg/l on d1, 109 (56-109) mg/l on d2, 90 (54-160) mg/l on d3, and 84 (44-
141) mg/l.
There were no differences between the subgroups with and without severe sepsis in the
levels of CRP on d0 to d2 but the difference was found in CRP values between the subgroups
on d3 (147 mg/l vs. 86 mg/l, p=0.052) and on d4 (179 mg/l vs. 79 mg/l, p=0.015) (Table 15,
Figure 8). Even though in the repeated measures ANOVA from day 0 to 3 no difference was
found in the levels of CRP (p=0.454) between subgroups, the differences of CRP were
significant between d0-d1 and between d1-d2 with p-values of < 0.001 and < 0.001,
respectively.

69
5.3.5. Amino-terminal pro-brain natriuretic peptide
The peak median NT-proBNP concentration was achieved on d4. The median NT-proBNP
was 127 (57-393) ng/l on d0, 236 (78-752) ng/l on d1, 318 (126-734) ng/l on d2, 351 (134-
1023) ng/l on d3, and 542 (194-1385) ng/l on d4 (Figure 7).
There were no statistically significant differences between the subgroups with and without
severe sepsis in the level of NT-proBNP at any time point (Table 15, Figure 8). After excluding
subjects with previous cardiovascular disease, the findings remained similar. In the repeated
measures ANOVA from day 0 to 3 no difference was found in the levels of NT-proBNP
(p=0.474) between subgroups with and without severe sepsis, but the differences between d0-
d1 and between d1-d2 NT-proBNP levels were significant (p= 0.001 and 0.011, respectively).
There was no correlation between NT-proBNP and the level of the same day CRP on the
first three days of neutropenic fever. However, NT-proBNP on d3 correlated slightly with CRP
on d4 (r=0.24, p=0.050), and NT-proBNP on d4 correlated with CRP on d3 (r=0.35, p=0.010)
and on d4 (r=0.33, p=0.015).
5.3.6. Association of amino-terminal pro-brain natriuretic peptide with fluidintake and previous cardiovascular disease
There was a slight negative correlation between NT-proBNP and the level of the fluid intake
on the same day for d0 and d1 of neutropenic fever (d0: r=-0.24, p=0.038; d1: r=-0.25,
p=0.021). Day 0 fluid intake correlated negatively with d4 NT-proBNP (r=-0.35, p=0.020).
The levels of NT-proBNP were higher in the subgroup of patients with previous
cardiovascular disease than those without throughout the course of the neutropenic fever
(Table 16, Figure 9). In the repeated measures ANOVA from d0 to d3 a significant difference
was found in the levels of NT-proBNP (p<0.001) between subgroups with and without previous
cardiovascular disease.
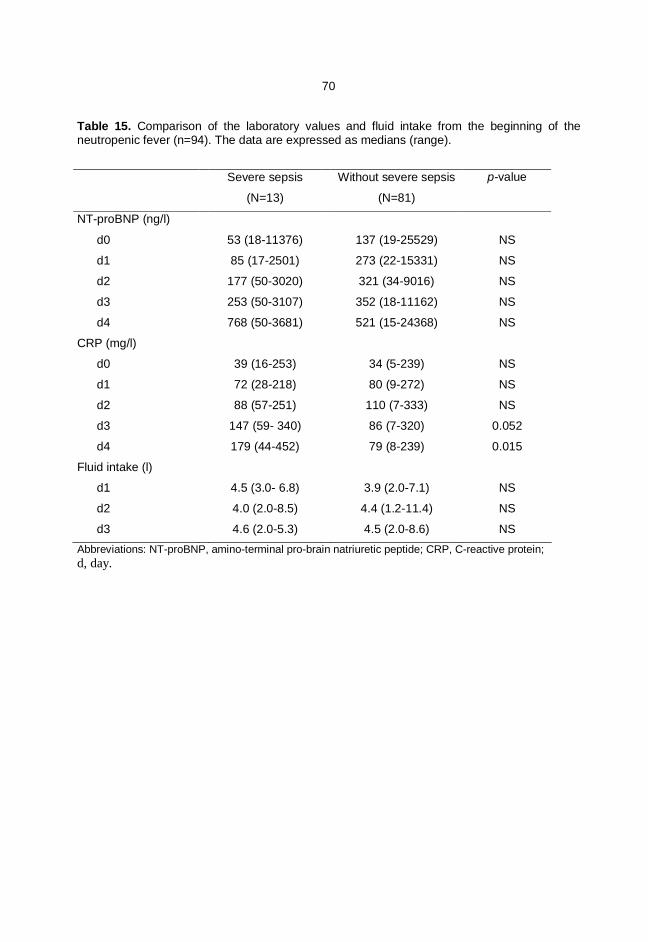
70
Table 15. Comparison of the laboratory values and fluid intake from the beginning of theneutropenic fever (n=94). The data are expressed as medians (range).
Severe sepsis
(N=13)
Without severe sepsis
(N=81)
p-value
NT-proBNP (ng/l)
d0 53 (18-11376) 137 (19-25529) NS
d1 85 (17-2501) 273 (22-15331) NS
d2 177 (50-3020) 321 (34-9016) NS
d3 253 (50-3107) 352 (18-11162) NS
d4 768 (50-3681) 521 (15-24368) NS
CRP (mg/l)
d0 39 (16-253) 34 (5-239) NS
d1 72 (28-218) 80 (9-272) NS
d2 88 (57-251) 110 (7-333) NS
d3 147 (59- 340) 86 (7-320) 0.052
d4 179 (44-452) 79 (8-239) 0.015
Fluid intake (l)
d1 4.5 (3.0- 6.8) 3.9 (2.0-7.1) NS
d2 4.0 (2.0-8.5) 4.4 (1.2-11.4) NS
d3 4.6 (2.0-5.3) 4.5 (2.0-8.6) NSAbbreviations: NT-proBNP, amino-terminal pro-brain natriuretic peptide; CRP, C-reactive protein;d, day.
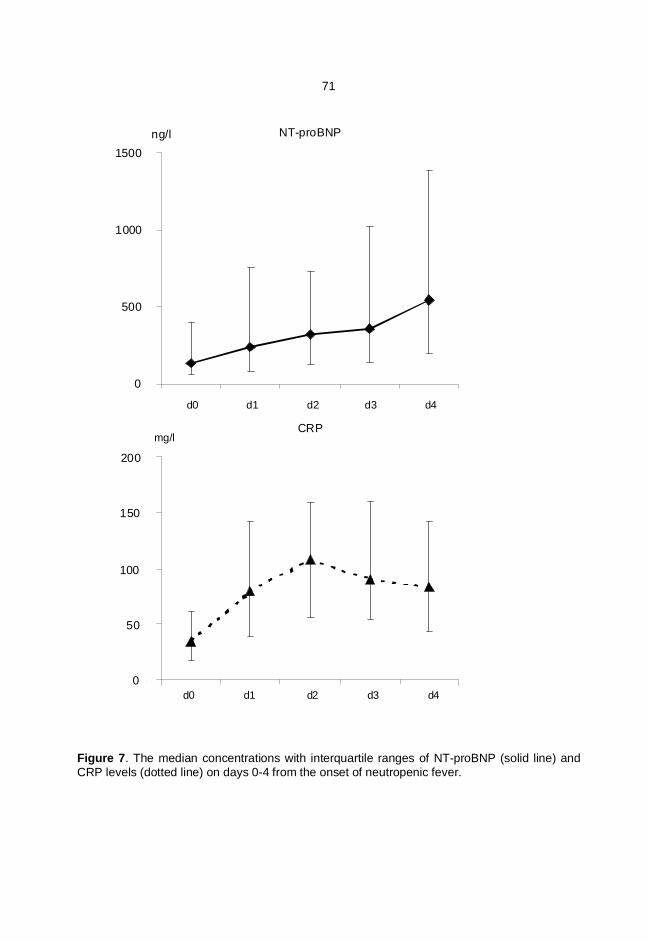
71
Figure 7. The median concentrations with interquartile ranges of NT-proBNP (solid line) andCRP levels (dotted line) on days 0-4 from the onset of neutropenic fever.
0
500
1000
1500
0
50
100
150
200
NT-proBNP
d0 d1 d2 d3 d4
d0 d1 d2 d3 d4
CRPmg/l
ng/l
d0 d1 d2 d3 d4
d0 d1 d2 d3 d4
NT-proBNP
CRP
d0 d1 d2 d3 d4
d0 d1 d2 d3 d4
ng/l
mg/l
1500
1000
500
0
200
150
100
50
0

72
Figure 8. The median concentrations with interquartile ranges of NT-proBNP and CRP ondays 0-4 from the onset of neutropenic fever in periods with (dotted lines) and without (solidlines) severe sepsis.
10
100
1000
10000
10
100
1000
NT-proBNP
CRP
d0 d1 d2 d3 d4
ng/l
mg/l
d0 d1 d2 d3 d4
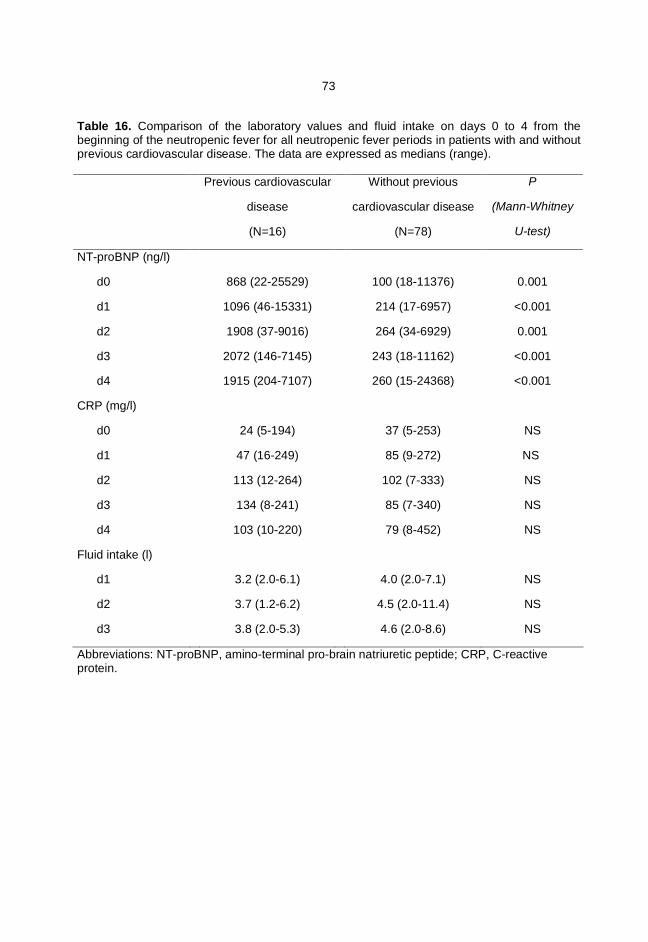
73
Table 16. Comparison of the laboratory values and fluid intake on days 0 to 4 from thebeginning of the neutropenic fever for all neutropenic fever periods in patients with and withoutprevious cardiovascular disease. The data are expressed as medians (range).
Previous cardiovascular
disease
(N=16)
Without previous
cardiovascular disease
(N=78)
P
(Mann-Whitney
U-test)
NT-proBNP (ng/l)
d0 868 (22-25529) 100 (18-11376) 0.001
d1 1096 (46-15331) 214 (17-6957) <0.001
d2 1908 (37-9016) 264 (34-6929) 0.001
d3 2072 (146-7145) 243 (18-11162) <0.001
d4 1915 (204-7107) 260 (15-24368) <0.001
CRP (mg/l)
d0 24 (5-194) 37 (5-253) NS
d1 47 (16-249) 85 (9-272) NS
d2 113 (12-264) 102 (7-333) NS
d3 134 (8-241) 85 (7-340) NS
d4 103 (10-220) 79 (8-452) NS
Fluid intake (l)
d1 3.2 (2.0-6.1) 4.0 (2.0-7.1) NS
d2 3.7 (1.2-6.2) 4.5 (2.0-11.4) NS
d3 3.8 (2.0-5.3) 4.6 (2.0-8.6) NS
Abbreviations: NT-proBNP, amino-terminal pro-brain natriuretic peptide; CRP, C-reactiveprotein.

74
Figure 9. The median concentrations with interquartile ranges of NT-proBNP and CRP ondays 0-4 from the onset of fever in neutropenic fever periods in patients with (dotted lines) andwithout (solid lines) previous cardiovascular disease.
10
100
1000
10000
10
100
1000
NT-proBNP
CRP
d0 d1 d2 d3 d4
ng/l
mg/l
d0 d1 d2 d3 d4
75
6 DISCUSSION
6.1 Patients and methods
The present series of studies are based on two retrospective studies (I-II) and a prospective
still ongoing study (III-IV). The intention of the study was to evaluate the various aspects of
severe sepsis in haematological patients, especially in patients with a high risk of neutropenic
fever. Therefore, only patients with AML and those receiving ASCT were included.
Chemotherapy regimens used in the treatment of AML cause a markedly longer period of
neutropenia than HDT supported by ASCT (Table 8). The intensity of the HDT in ASCT
recipients, on the other hand, causes more severe mucosal damage in the patients. These
patient groups present different sides of high-risk neutropenic fever and were analysed
separately in the retrospective part of the present series. For prospective study, these patient
groups were combined because interest was focused on clinical management of
haematological patients with severe sepsis.
The definitions for neutropenia, neutropenic fever and severe sepsis were based on
internationally used definition criteria of both the Infectious Diseases Society of America (6)
and 2001 International Sepsis Definitions Conference (79). Even though the definition of SIRS
and severe sepsis have been available for almost two decades (78), these have not been
systematically applied in haematological patients receiving intensive therapy. The definition of
SIRS includes leukocytosis or leucopenia, fever, tachypnea and tachycardia (Table 1), and two
of these criteria must be manifested to fulfill the criteria of SIRS. All of the study patients met at
least two of these other criteria than leucopenia. Thus, leucopenia is a consequence of the
treatment, and this has also been taken into account in this study.
Despite the criteria for neutropenic fever and severe sepsis are definitive, the backgrounds
for both entities are often heterogeneous. The treatment strategies for septic infections in
haematological wards may differ, but the amount of supportive care remains crucial. Vigorous
volume resuscitation as used in the prospective study might thus prevent or shorten the
duration of severe sepsis - with obvious clinical benefits. Severe sepsis that responds quickly
to supportive therapy may be different from the situation where hypotension responds more
slowly and eventually necessitates ICU admission.
Based on retrospective studies it was evident that hard endpoints (ICU admission, death)
were rather infrequent in this patient cohort. Because of this, severe sepsis was used as an
endpoint in prospective studies and as a model to evaluate prognostic utility of various
76
laboratory markers. Therefore, the findings of the present studies do not as such apply to the
ICU setting although the kinetics of various markers are likely to be the same.
During the study period, the empirical antimicrobial treatment practice and hospital infection
control measures (e.g. isolation policies and hospital hygiene, including cleaning and hand-
washing policies) remained constant. Systematic antibiotic prophylaxis was not used, except
during the last study year in NHL patients receiving ASCT. In the prospective studies, each
patient was daily carefully monitored for clinical signs and possible sources of infections.
Special attention was paid to features indicating the development of severe sepsis. In addition,
supportive care was provided including aggressive volume resuscitation when needed.
In regard to laboratory methods, serum CRP measurements have been routine for more than
two decades, and the method is standard. Also serum NT-proBNP measurements have been
in clinical use in ISLAB (Eastern Finland Laboratory Centre, Kuopio, Finland) for several years.
NT-proBNP was preferred to BNP because of its markedly longer plasma life and better
stability (164). VEGF was determined from serum samples instead of plasma. This was
because it was the only method used by the laboratory (ISLAB) and because reference values
were available only for serum VEGF based on the FINNSEPSIS study.
6.2. Epidemiological features and outcome of severe sepsis
The available data of incidence of severe sepsis in neutropenic patients is limited. One
reason for this might be that most of the studies regarding incidence of severe sepsis or septic
shock are made in patients treated at ICUs. The policy among admission practice of patients
with malignant diseases to ICUs varies between centres (196, 197). In present studies the
admission of patients with neutropenia and severe sepsis to ICU has had a relatively low
threshold. The admission criteria to ICU may have had slight changes during the study period,
and this naturally may influence the outcome of patients.
6.2.1. Patients with acute myeloid leukaemia
In AML patients, the criteria for severe sepsis were fulfilled in 13% of periods with
neutropenic fever after intensive induction or consolidation courses. Nine out of 84 AML
patients (11%) died due to severe sepsis. This underlines the importance of severe sepsis as a
cause of death in AML patients treated with modern intensive chemotherapy. In other studies,
the infection mortality rate has ranged between 5-13% (2, 60-64). In elderly patients, the risks
may be even higher (198).
77
Even though the induction course may be the most dangerous in relation to severe or fatal
infections, also the consolidation courses are associated with high risk of neutropenic fever (2,
62). Therefore, it is obvious that all measures aiming to decrease mortality due to severe
sepsis might improve overall outcome of AML patients. Unfortunately, in the present study only
38% of patients treated in ICU recovered. At least in some patients the late referral to ICU
might be a possible reason for this. During the study period (1996-2005) the practises of
admission to ICU have changed: life-sustaining treatments are begun outside ICUs in different
step-up/ step-down units. Moreover, the threshold admission to the ICU has become lower for
patients with malignancies and severe co-morbidities. In AML patients, the goal of the
intensive treatment is curative, and early ICU admission in severe sepsis may improve
prognosis. Close clinical monitoring of these patients is therefore mandatory in the
haematology ward.
6.2.2. Autologous stem cell transplant recipients
In ASCT recipients the incidence of severe sepsis was much lower (5%) than in AML
patients, but patients receiving a transplant for NHL were at a higher risk than the rest of ASCT
recipients. In earlier studies the percentage of septic bloodstream infections in ASCT recipients
has varied between 12% and 20% (72-74, 76).
The case fatality rate in patients with severe sepsis was, however, high (9/17, 53%) and all
patients who died due to severe sepsis after ASCT had NHL. Only 18% of patients admitted to
ICU recovered. This figure is clearly inferior than in some ICU- based studies of
haematological patients (199), but the reason for admission may effect ICU outcome in an
important way (e.g. septic hypotension in young neutropenic patients vs. neutropenic septic
shock in patients with co-morbidies).
The mortality for severe sepsis was 6% in patients with NHL. This is a high figure compared
with other series where an early mortality of 2-4% has been observed (70-72, 74). One
potential reason for the high mortality rate in this study may be the relatively high number of
elderly NHL patients receiving ASCT. In an EBMT (European Group of Blood and Marrow
Transplantation) study, the risk of early treatment-related mortality in older NHL patients (>60
years of age) was significantly higher (4.4%) than in younger patients (2.8%) (200). Other
reasons for higher mortality of NHL patients due to severe sepsis might be the combination of
longer neutropenia together with the known cardiotoxicity of prior anthracycline treatment
(201). Therefore, a prospective treatment protocol for NHL patients receiving ASCT was
initiated in January 2008. This includes oral ciprofloxacin prophylaxis during neutropenia,
78
cardiac pre-evaluation with radio-cardiography, ACE-inhibitor treatment in patients with
decreased left ventricular ejection fraction and use of BEAM chemotherapy instead of earlier
BEAC. The latter is known to be associated with early cardiotoxicity (201).
6.2.3. Prospective study
In the prospective series the incidence of severe sepsis was 14% without a difference
between AML patients and ASCT recipients. Even though the incidence of severe sepsis was
not lower than in retrospective series, the case fatality rate for periods with severe sepsis
seemed to be lower (15%). There are many possible reasons for this. Improved supportive
care during the prospective treatment protocol and thus possibly earlier detection of severe
sepsis may be important factors. This includes starting effective treatment by the trained
nursing personnel earlier. However the number of periods with severe sepsis is still relatively
low in the prospective series and more experience is needed before drawing firm conclusions.
Haematological patients themselves may today be better informed and aware of the risk of
septic infections during chemotherapy. This in turn helps them to recognise symptoms of
septic infections and contact hospitals earlier than other patients with community-acquired
sepsis.
6.3. Microbiological findings
In general, the incidence of microbiologically documented bloodstream infections has been
between 7.7% and 19% in patients with neutropenic fever (23, 25, 26). In the present studies,
the percentage varied between 23 and 59%. In AML patients (study I) the amount of
bloodstream infections was 59%, which is higher than in earlier studies (24, 66).
There are some obvious reasons for the high percentage of bloodstream infections in AML
patients. The duration of neutropenia in AML patients during intensive induction and
consolidation chemotherapy is markedly longer than in any other treatment protocol for
malignancies. During the long-lasting treatment period, the use of long-term indwelling
catheters (up to six months) is common. This predisposes patients to catheter-related
infections. In addition, intensive chemotherapy itself causes mucosal damage. This in turn
increases the risk of infections caused by microbes from the normal oro-pharyngeal and
gastrointestinal flora. Long-lasting febrile neutropenia increases the number of blood cultures
taken and hence, also the number of positive culture results.
79
As expected, gram-positive microbes caused the majority of bloodstream infections. This
finding is in accord with other recent studies (24, 37, 74). The proportion of gram-negative
microbes in blood cultures was high (9-25%) and especially as a cause of severe sepsis (35-
41%). The presumable reason for this is the lack of prophylactic antibiotics in present series –
the situation is similar in other centres where antibiotic prophylaxis has not been used (202-
204).
Among gram-positive microbes causing bloodstream infections the most common finding
was Staphylococcus epidermidis, which is in line with earlier observations (59, 205, 206). The
amount of bloodstream infections arising from central venous catheters varied between 9%
and 16%, with the highest percentage in AML patients. The plausible explanation for this was
the long-term use of indwelling catheters in this patient group. The lungs and upper respiratory
airways were the most common known localisation of infection in febrile neutropenic patients,
as observed in other studies (66, 70).
Candida albicans was found in 1% of febrile neutropenic periods in both AML patients and
ASCT recipients. The apparent reason for the small amount of fungaemia was the use of
fluconazole prophylaxis during prolonged neutropenia and mucosal symptoms (207). In the
Finnish nationwide series the risk of invasive Candida-infections was also <1% among 1188
ASCT recipients (208). In addition, the lack of systematic antibacterial prophylaxis may have
had an impact.
In contrast to some other recent series (38, 209), there were not a single case of
multiresistant bacteria like MRSA, VRE, extended-spectrum -lactamase (ESBL) -producing
gram-negative rods or multi-drug resistant gram-negative microbes. The explanation for this
might be our treatment practice in Finland – antibacterial prophylaxis is not commonly used.
Furthermore, empirical use of vancomycin has been restricted during the whole study period
and the overall use of wide spectrum antibiotics has been under control.
In the beginning of 2008 the use of oral ciprofloxacin was started for NHL patients receiving
ASCT. This was mainly because of the fatal Pseudomonas aeruginosa-bloodstream infections
in NHL patients during years 1996-2006 (study II). The mortality with Pseudomonas
aeruginosa bloodstream infections was high and this finding is in line with earlier studies (210-
213). The present prophylaxis practice is experimental and is part of a prospective clinical
protocol. Although preliminary, the early impression seems to be promising, because there has
not been a single case of severe sepsis among fourteen consecutive patients treated within
this protocol (214). The amount of patients who received ciprofloxacin prophylaxis during the
present study time was low and probably does not have a major influence on the study
findings.

80
6.4. Kinetics of serum C-reactive protein in patients with neutropenic fever(Studies I-II)
In the retrospective studies (I-II) the median time from the onset of neutropenic fever to the
point where criteria for severe sepsis were met was 2 (study I) and 3 days (study II). CRP
concentrations elevated in paralle with this but the peak CRP was achieved later than the
criteria for severe sepsis. Neither CRP slope velocity nor CRP on days 2-3 reliably distinguish
periods with severe sepsis from those without in advance. In the study of Persson and
colleagues (14) the CRP concentrations on days 2 and 3 of febrile neutropenia were lower in
those patients who did not develop complications (e.g. pneumonia). This is in line with our
findings.
Although several parameters of CRP kinetics were statistically associated with severe
sepsis, in most instances CRP parameters evaluated coincided or even followed the diagnosis
of severe sepsis. This was observed also in earlier studies both in patients with febrile
neutropenia (146) and those without (142, 143). CRP identifies patients with infection but when
the time interval is short, the predictive capacity of CRP declines markedly. This is mostly
explained by the biochemistry of CRP – the peak values are reached 48 hours after the
beginning of secretion independently of the reason for secretion (128).
6.5. Comparison of serum vascular endothelial growth factor and C-reactiveprotein in patients with neutropenic fever (Study III)
The peak serum VEGF level was reached during the first 24 hours and the peak CRP values
on day 2 after the onset of neutropenic fever in patients with severe sepsis. Serum VEGF
levels were continuously low, but slightly higher in patients who developed severe sepsis than
in those who did not. The difference reached statistical significance for VEGF after the first 24
hours but there were no statistically significant differences in CRP values on any day between
the groups with severe and non-severe sepsis.
The serum VEGF values on d0 in study III were notably lower than in patients with severe
sepsis in FINNSEPSIS study (median 423 pg/ml) or in healthy controls (median 260 pg/ml)
(Figure 10) (15). However, during the first 24 hours the VEGF levels in neutropenic patients
with severe sepsis were higher than in those without. This latter finding is in line with earlier
studies (215-217), although those studies included patients without known neutropenia or
thrombocytopenia.
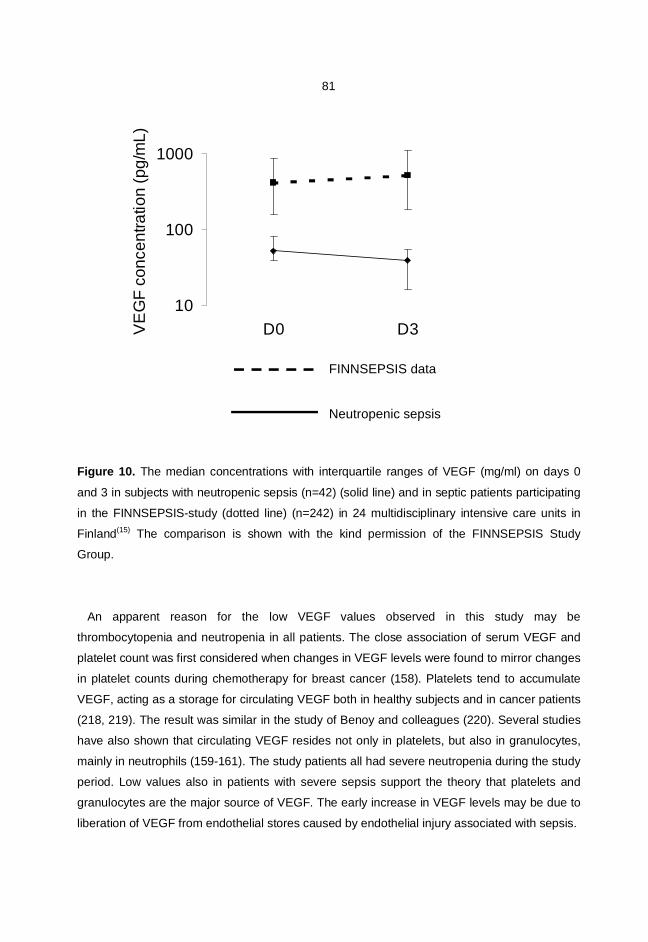
81
Figure 10. The median concentrations with interquartile ranges of VEGF (mg/ml) on days 0
and 3 in subjects with neutropenic sepsis (n=42) (solid line) and in septic patients participating
in the FINNSEPSIS-study (dotted line) (n=242) in 24 multidisciplinary intensive care units in
Finland(15) The comparison is shown with the kind permission of the FINNSEPSIS Study
Group.
An apparent reason for the low VEGF values observed in this study may be
thrombocytopenia and neutropenia in all patients. The close association of serum VEGF and
platelet count was first considered when changes in VEGF levels were found to mirror changes
in platelet counts during chemotherapy for breast cancer (158). Platelets tend to accumulate
VEGF, acting as a storage for circulating VEGF both in healthy subjects and in cancer patients
(218, 219). The result was similar in the study of Benoy and colleagues (220). Several studies
have also shown that circulating VEGF resides not only in platelets, but also in granulocytes,
mainly in neutrophils (159-161). The study patients all had severe neutropenia during the study
period. Low values also in patients with severe sepsis support the theory that platelets and
granulocytes are the major source of VEGF. The early increase in VEGF levels may be due to
liberation of VEGF from endothelial stores caused by endothelial injury associated with sepsis.
10
100
1000
D0 D3VE
GF
conc
entra
tion
(pg/
mL)
Neutropenic sepsis Sepsis (Finsepsis data)FINNSEPSIS data
Neutropenic sepsis
82
In patients with neutropenic fever, there are no previous studies available on the kinetics and
prognostic utility of serum VEGF. In the present study, it was demonstrated that also
thrombocytopenic and neutropenic patients are capable of producing VEGF during fever.
Although haematological patients had low VEGF concentrations during sepsis, the VEGF
concentrations in severely septic patients were higher than in other febrile patients, especially
on the first days after the start of fever. This implies that VEGF is a more rapid indicator than
CRP in haematological patients with neutropenic fever, which deserves further study.
6.6. Comparison of serum amino-terminal pro-brain natriuretic peptide and C-reactive protein in patients with neutropenic fever (Study IV)
There were no statistically significant differences in the level of NT-proBNP between patients
with and without severe sepsis at any time point analysed. CRP concentrations did not show
any predictive utility either; the median level of CRP was significantly higher in the subgroup
with severe sepsis only on day 3 and day 4. Taking into account that the median time to the
fulfilment of criteria for severe sepsis was only one day in this prospective study, it is obvious
that these markers are unsuitable for clinical use to predict severe sepsis.
Previous myocardial infarction, acute coronary syndrome, valvular disease, ventricular
hypertrophy and cardiomyopathy are known cardiological reasons for increased values of
natriuretic peptides. Non-cardiac factors include age, female gender, renal failure,
glucocorticoid use and acute pulmonary embolism (138, 221, 222). In the present study,
patients with a history of previous cardiovascular disease had significantly higher levels of NT-
proBNP than those without, even though none of the study patients had clinically severe
cardiovascular disease. Significant release of NT-proBNP continued during the entire study
period. Of note, the amount of daily fluid intake did not show any significant association with
NT-proBNP levels.
There are some previous studies showing a significant association with sepsis and ICU
mortality in patients with markedly elevated BNP- and NT-proBNP values (16, 138, 168, 169).
Nikolau and his colleagues showed that BNP levels were elevated also in the acute phase of
community-acquired microbial infections without severe sepsis or septic shock (170). It was
therefore reasonable to assume that natriuretic peptides would serve as prognostic markers
also in the haematology ward setting. This was, however, not the case in the present study
where NT-proBNP was used.
Neither serial NT-proBNP nor CRP showed any early predictive value in neutropenic periods
with severe sepsis compared to those without. NT-proBNP seemed to reflect cardiac distress

83
more than the inflammatory response in this patient population. It might thus serve as a useful
adjunct to optimise management of patients with previous cardiovascular disease during
sepsis.
6.7. Study limitations
Because of the retrospective nature, studies I-II have several unavoidable limitations. The
criteria for severe sepsis were well applicable for all study subjects, although the retrospective
classification of patients with severe sepsis was challenging. All periods regarded to represent
severe sepsis were confirmed by consultation between the clinical haematologist (EJ) and
infectious disease specialist (SH), but uncertainties remain in patients who were not treated in
the ICU.
CRP values on the first day of the fever and particularly 12-24 hours from the onset of fever
were often missing. For this reason the values 2 or 3 days after the onset of fever were used.
Further, in patients with clinical signs of severe infection CRP values were evaluated
apparently more often than febrile neutropenic patients without these signs. The observers
were not blinded to CRP values when evaluating febrile neutropenic periods.
In studies I and IV all febrile neutropenic periods in study patients were included. This is
common practice in haematological studies, but it also causes a situation where the same
patient is analysed repeteadly during new periods of neutropenic fever. It is unknown how
inflammatory markers behave in repeating periods of febrile neutropenia in the same
individual. However, in present series only four patients (study I) (Table 9) had more than one
episode of severe sepsis. As with these patients and with all other study patients, it was
impossible to predict the febrile period that will be complicated with severe sepsis. For this
reason, all periods with neutropenic fever are included.
The site of infection remained unknown in most of the febrile neutropenic periods.
Neutropenia alters the host’s inflammatory response and makes the infection difficult to detect
because the classic signs and symptoms of infection are usually missing. This is mainly
because of an almost total lack of neutrophils. In this respect traditional laboratory methods are
also useless. Fever is often the only sign of infection in accordance with criteria of severe
sepsis (e.g. hypotension). Sometimes medications like corticosteroids can obscure especially
fever. Only patients with both neutropenia and fever ( 38.3°C or 38.0°C for 1 h) were
included into the present studies. It is possible that there have been also patients with
neutropenic infection but without fever. In septic infections, however, this is unlikely. Patients

84
are closely monitored during the treatment period. Even without fever, the other signs of
severe infection (e.g. hypotension, dyspnoea) would have been noted.
Study III was the first prospective study published evaluating VEGF kinetics in cytopenic
haematological patients. The number of patients was relatively small. Consequently, the
number of patients who had severe sepsis was also small. The number of endpoints (severe
sepsis, septic shock or death) was low in both prospective studies, but in line with the
incidences observed in retrospective studies.
Sepsis-related Organ Failure Assesment (SOFA) or another comparable method would have
been useful in patient monitoring. Classification of neutropenic patients with SOFA in
haematological wards has some inevitable limitations. Patients have a low number of platelets
because of chemotherapy even in the absence of infection, and platelet count is one of the
main criteria for SOFA. A more important reason for not using SOFA is that usage of invasive
monitoring is not routine outside ICUs.
More frequent early measurements (e.g. between 2-6 hour intervals after the beginning of
fever) of both NT-proBNP and CRP might have been more informative in prospective studies.
However, such a frequent sampling may not be applicable in clinical practice outside intensive
care units. Considering the kinetics of these measures, it is also unlikely that more frequent
sampling would have led to different conclusions.
6.8. Concluding remarks
The frequency of severe sepsis was lowest among ASCT recipients (study II) (5%) and
highest in study IV (14%), where both AML patients and ASCT recipients were prospectively
included. The outcome of severe sepsis was rather poor in the retrospective studies with a
mortality of 11% in AML patients and 2% in ASCT recipients during intensive therapy. The
case fatality rate for periods with severe sepsis were 27% and 53%, respectively. In the
prospective study with close patient monitoring and supportive care, the mortality during
intensive therapy was 3% and the case fatality rate for periods with severe sepsis 15%.
Altough the incidence of severe sepsis seems to remain the same, the outcome seems to have
been better in the prospective part of the study.
The microbial aetiology of severe sepsis in neutropenic patients did not change during the
study period (1995-2008). Gram-positive microbes were the predominant findings in blood
cultures, which is well in line with other studies (37, 38, 223). Because antibacterial prophylaxis
was not used, the proportion of gram-negative microbes in bloodstream infections was
considerable compared with studies where prophylactic antibiotics were used. The incidence

85
of Pseudomonas aeruginosa was nevertheless alarming, and changed the policy concerning
prophylactic antimicrobial use in patients with greatest risk of fatal septic infections. During the
study period, not a single strain of MRSA, VRE or ESBL were found, which is an important
finding concerning the hospital hygiene policies in our hospital.
CRP was one of the infection markers chosen for this study protocol. It is easily available
and familiar as a reference marker for sepsis. Other chosen markers were compared with
CRP. As demonstrated in the earlier studies (14, 142, 146), CRP was slow to change in the
early phase (< 24 hours) of severe sepsis. The situation was similar with the NT-proBNP
(study IV). The peak values came far too late for predictive purposes in patients with
neutropenic sepsis.
The results with serum VEGF showed some promise. Study III was the first study published
evaluating VEGF kinetics in haematological patients with neutropenic fever. It was
demonstrated that also thrombocytopenic and neutropenic patients can produce VEGF during
fever. Although the VEGF concentrations were in general low, the VEGF concentrations in
severely septic patients were higher than in other febrile patients. The difference was obvious
during the first critical hours from the start of neutropenic fever. This implies that VEGF might
be a rapid indicator for severe sepsis in haematological patients with neutropenic fever. The
problem with VEGF is the current lack of an appropriate methodology in clinical laboratories
that can provide results within 12-24 hours. The definition of practical cut-off values with
evaluation of positive and negative predictive capacity in neutropenic and thrombocytopenic
patients is also needed.
6.8.1. Implications for further research
The major focus of this series of studies was on febrile neutropenic patients treated in a
haematological ward. In these circumstances, the conditions and equipment are inferior to
those in ICUs. Furthermore, the possibilities for respiratory and circulatory support are limited.
In retrospective studies only 38% of the AML patients and 22% of the ASCT recipients
admitted to the ICU recovered. This contrasts with the results of the FINNSEPSIS study (10),
where 86% of the patients admitted for sepsis to ICU recovered. In recent years, intensive care
treatment with step-down units has become more available, and admission criteria have
probably changed. In addition, the treatment strategies in haematological wards have
changed. Although the supportive care in haematological ward has been rather efficient also in
the near past, the need for improvement is obvious. The possibilities in the ward are, however,

86
limited and a flexible consultation system is essential to get these patients early into step-up-
step-down units or the ICU when needed.
The question of antibiotic prophylaxis in neutropenic haematological patients needs to be
reconsidered. Based on the findings in study II a new prospective protocol was started in the
beginning of January 2008. One of its main principles is to determine the benefits and possible
disadvantages of fluoroquinolone prophylaxis in high-risk ASCT recipients. Mucositis caused
by intensive chemotherapy is in closely associated with this – if the incidence of mucositis
could be reduced (224, 225), the amount of neutropenic infections and of course, septic
infections would diminish. There are interesting possibilities for the development of locally
administered nonpharmacological measures and pharmacotherapeutics to restore mucosal
barriers in the future (226).
Readily available early circulatory markers for severe sepsis could be helpful in clinical
practice, especially in haematological wards. Severe sepsis proceeds rapidly. Commonly used
laboratory methods recognise this phenomenon too late and too slowly. Serum VEGF might be
one option for further research. At present, the lack of an appropriate methodology applicable
in clinical laboratories to get the result within 12-24 hours and the lack of practical cut-off
values with known positive and negative prediction capacity are problems. Many other early
markers are of potential interest in relation to the pathogenesis of sepsis in neutropenic
haematological patients as well as polymerase chain reaction (PCR) based assays for fast
microbial recognition (135, 227).
While continuing the search for clinically useful laboratory markers, it is of utmost importance
that febrile neutropenic patients be carefully monitored for vital functions with optimised
supportive care. In haematological wards, severe sepsis is still primarily a clinical diagnosis,
and the experience of caregiving physicians is vitally important. Close co-operation with
colleagues in ICUs and other supportive care units is crucial in the treatment of patients with
severe neutropenic sepsis.
87
7. CONCLUSION
I Severe sepsis was observed in 13 % of periods with neutropenic fever in AML patients
and 5% of periods in ASCT recipients. Gram-negative rods were more commonly
found in blood cultures of periods with severe sepsis in both patient groups. In ASCT
recipients, 30% of blood stream infections were caused by Pseudomonas sp. The
case fatality rate of severe sepsis was 28 % in patients with AML and 53 % in ASCT
recipients.
II Peak CRP values were higher and CRP slope velocity steeper in periods with severe
sepsis in both patient groups. CRP kinetic merely coincided than preceded the
development of severe sepsis.
III VEGF concentrations were in general low but < 24 hours after the start of neutropenic
fever VEGF levels were higher in patients with severe sepsis. VEGF seems to be a
more rapid indicator of severe sepsis than CRP in haematological patients with
neutropenic fever.
IV Neither serial NT-proBNP nor CRP showed any early predictive value for the
development of severe sepsis in haematological patients with neutropenic fever. NT-
proBNP values were significantly higher in patients with previous cardiovascular
disease.
88
8. REFERENCES
1. Burnett AK. The treatment of AML: current status and novel approaches. Hematology 2005;10Suppl 1:50-3.
2. Koistinen P, Räty R, Itälä M, Jantunen E, Koivunen E, Nousiainen T, et al. Long-term outcome ofintensive chemotherapy for adults with de novo acute myeloid leukaemia (AML): the nationwideAML-92 study by the Finnish Leukaemia Group. Eur J Haematol 2007;78(6):477-86.
3. Wrench D, Gribben JG. Stem cell transplantation for non-Hodgkin's lymphoma. Hematol Oncol ClinNorth Am 2008;22(5):1051-79.
4. Sureda A. Autologous and allogeneic stem cell transplantation in Hodgkin's lymphoma. HematolOncol Clin North Am 2007;21(5):943-60.
5. Kumar A, Roberts D, Wood KE, Light B, Parrillo JE, Sharma S, et al. Duration of hypotension beforeinitiation of effective antimicrobial therapy is the critical determinant of survival in human septicshock. Crit Care Med 2006;34(6):1589-96.
6. Hughes WT, Armstrong D, Bodey GP, Bow EJ, Brown AE, Calandra T, et al. 2002 guidelines for theuse of antimicrobial agents in neutropenic patients with cancer. Clin Infect Dis 2002;34(6):730-51.
7. Bodey GP, Rolston KV. Management of fever in neutropenic patients. J Infect Chemother2001;7(1):1-9.
8. Brun-Buisson C, Meshaka P, Pinton P, Vallet B. EPISEPSIS: a reappraisal of the epidemiology andoutcome of severe sepsis in French intensive care units. Intensive Care Med 2004;30(4):580-8.
9. Flaatten H. Epidemiology of sepsis in Norway in 1999. Crit Care 2004;8(4):R180-4.
10. Karlsson S, Varpula M, Ruokonen E, Pettilä V, Parviainen I, Ala-Kokko TI, et al. Incidence,treatment, and outcome of severe sepsis in ICU-treated adults in Finland: the Finnsepsis study.Intensive Care Med 2007;33(3):435-43.
11. Rintala E, Irjala K, Nikoskelainen J. Value of measurement of C-reactive protein in febrile patientswith hematological malignancies. Eur J Clin Microbiol Infect Dis 1992;11(11):973-8.
12. Manian FA. A prospective study of daily measurement of C-reactive protein in serum of adults withneutropenia. Clin Infect Dis 1995;21(1):114-21.
13. Yonemori K, Kanda Y, Yamamoto R, Hamaki T, Suguro M, Chizuka A, et al. Clinical value of serialmeasurement of serum C-reactive protein level in neutropenic patients. Leuk Lymphoma 2001;41(5-6):607-14.
14. Persson L, Söderquist B, Engervall P, Vikerfors T, Hansson LO, Tidefelt U. Assessment of systemicinflammation markers to differentiate a stable from a deteriorating clinical course in patients withfebrile neutropenia. Eur J Haematol 2005;74(4):297-303.
15. Karlsson S, Pettilä V, Tenhunen J, Lund V, Hovilehto S, Ruokonen E. Vascular endothelial growthfactor in severe sepsis and septic shock. Anesth Analg 2008;106(6):1820-6.
16. Brueckmann M, Huhle G, Lang S, Haase KK, Bertsch T, Weiss C, et al. Prognostic value of plasmaN-terminal pro-brain natriuretic peptide in patients with severe sepsis. Circulation 2005;112(4):527-34.
17. Bodey GP. The changing face of febrile neutropenia - from monotherapy to moulds to mucositis.Fever and neutropenia: the early years. J Antimicrob Chemother 2009;63 Suppl 1:i3-13.
18. Hotchkiss RS, Karl IE. The pathophysiology and treatment of sepsis. N Engl J Med2003;348(2):138-50.
19. Root RK, Lodato RF, Patrick W, Cade JF, Fotheringham N, Milwee S, et al. Multicenter, double-blind, placebo-controlled study of the use of filgrastim in patients hospitalized with pneumonia andsevere sepsis. Crit Care Med 2003;31(2):367-73.
89
20. Pettilä V, Pentti J, Pettilä M, Takkunen O, Jousela I. Predictive value of antithrombin III and serumC-reactive protein concentration in critically ill patients with suspected sepsis. Crit Care Med2002;30(2):271-5.
21. Craigie D. Case of disease of the spleen in which death took place in consequences of thepresence of purulent matter in the blood. Edinb Med Surg J 1845;64:400.
22. Farber S, Diamond LK. Temporary remissions in acute leukemia in children produced by folic acidantagonist, 4-aminopteroyl-glutamic acid. N Engl J Med 1948;238(23):787-93.
23. Rintala E. Incidence and clinical significance of positive blood cultures in febrile episodes of patientswith hematological malignancies. Scand J Infect Dis 1994;26(1):77-84.
24. Madani TA. Clinical infections and bloodstream isolates associated with fever in patientsundergoing chemotherapy for acute myeloid leukemia. Infection 2000;28(6):367-73.
25. Perola O, Nousiainen T, Pentikäinen J, Laatikainen A, Katila ML. Infections and bacterialcolonization during cytotoxic therapy in patients with acute leukemia. Eur J Clin Microbiol Infect Dis2005;24(11):766-8.
26. Gencer S, Salepci T, Ozer S. Evaluation of infectious etiology and prognostic risk factors of febrileepisodes in neutropenic cancer patients. J Infect 2003;47(1):65-72.
27. Viscoli C, Castagnola E. Planned progressive antimicrobial therapy in neutropenic patients. Br JHaematol 1998;102(4):879-88.
28. Gafter-Gvili A, Paul M, Fraser A, Leibovici L. Antibiotic prophylaxis in neutropenic patients. Isr MedAssoc J 2007;9(6):460-2.
29. De Pauw BE, Verweij PE. Infections in patients with hematologic malignancies. In: Mandell GL,Bennett JE, Dolin R, editors. Mandell, Douglas, and Bennett's Principles and Practice of InfectiousDiseases. 6th ed. Philadelphia: Elsevier Churchill Livingstone; 2005.
30. Sickles EA, Greene WH, Wiernik PH. Clinical presentation of infection in granulocytopenic patients.Arch Intern Med 1975;135(5):715-9.
31. Valdivieso M, Gil-Extremera B, Zornoza J, Rodriquez V, Bodey GP. Gram-negative bacillarypneumonia in the compromised host. Medicine (Baltimore) 1977;56(3):241-54.
32. Klastersky J. Empiric treatment of infections in neutropenic patients with cancer. Rev Infect Dis1983;5 Suppl 1:S21-31.
33. Klastersky J. The changing face of febrile neutropenia-from monotherapy to moulds to mucositis.Why empirical therapy? J Antimicrob Chemother 2009;63 Suppl 1:i14-5.
34. Chang HY, Rodriguez V, Narboni G, Bodey GP, Luna MA, Freireich EJ. Causes of death in adultswith acute leukemia. Medicine (Baltimore) 1976;55(3):259-68.
35. Schimpff S, Satterlee W, Young VM, Serpick A. Empiric therapy with carbenicillin and gentamicinfor febrile patients with cancer and granulocytopenia. N Engl J Med 1971;284(19):1061-5.
36. Anttila VJ, Ruotsalainen E. [Empirical antimicrobial therapy in a patient with neutropenia].Neutropeenisen potilaan empiirinen mikrobilääkehoito. Duodecim 2002;118(21):2241-7.
37. Ramphal R. Changes in the etiology of bacteremia in febrile neutropenic patients and thesusceptibilities of the currently isolated pathogens. Clin Infect Dis 2004;39 Suppl 1:S25-31.
38. Kanamaru A, Tatsumi Y. Microbiological data for patients with febrile neutropenia. Clin Infect Dis2004;39 Suppl 1:S7-S10.
39. Günther G, Björkholm M, Björklind A, Engervall P, Stiernstedt G. Septicemia in patients withhematological disorders and neutropenia. A retrospective study of causative agents and theirresistance profile. Scand J Infect Dis 1991;23(5):589-98.
40. Hersh EM, Bodey GP, Nies BA, Freireich EJ. Causes of death in acute leukemia: a ten-year studyof 414 patients from 1954-1963. JAMA 1965;193:105-9.
90
41. Rubio M, Palau L, Vivas JR, del Potro E, Diaz-Mediavilla J, Alvarez A, et al. Predominance of gram-positive microorganisms as a cause of septicemia in patients with hematological malignancies.Infect Control Hosp Epidemiol 1994;15(2):101-4.
42. Viscoli C, Bruzzi P, Castagnola E, Boni L, Calandra T, Gaya H, et al. Factors associated withbacteraemia in febrile, granulocytopenic cancer patients. The International Antimicrobial TherapyCooperative Group (IATCG) of the European Organization for Research and Treatment of Cancer(EORTC). Eur J Cancer 1994;30A(4):430-7.
43. Sharma A, Lokeshwar N. Febrile neutropenia in haematological malignancies. J Postgrad Med2005;51 Suppl 1:S42-8.
44. Picazo JJ. Management of the febrile neutropenic patient: a consensus conference. Clin Infect Dis2004;39 Suppl 1:S1-6.
45. Costa SF, Miceli MH, Anaissie EJ. Mucosa or skin as source of coagulase-negative staphylococcalbacteraemia? Lancet Infect Dis 2004;4(5):278-86.
46. Sonis ST, Oster G, Fuchs H, Bellm L, Bradford WZ, Edelsberg J, et al. Oral mucositis and theclinical and economic outcomes of hematopoietic stem-cell transplantation. J Clin Oncol2001;19(8):2201-5.
47. Klastersky J. Science and pragmatism in the treatment and prevention of neutropenic infection. JAntimicrob Chemother 1998;41 Suppl D:13-24.
48. Gaytan-Martinez J, Mateos-Garcia E, Sanchez-Cortes E, Gonzalez-Llaven J, Casanova-Cardiel LJ,Fuentes-Allen JL. Microbiological findings in febrile neutropenia. Arch Med Res 2000;31(4):388-92.
49. Oliveira AL, de Souza M, Carvalho-Dias VM, Ruiz MA, Silla L, Tanaka PY, et al. Epidemiology ofbacteremia and factors associated with multi-drug-resistant gram-negative bacteremia inhematopoietic stem cell transplant recipients. Bone Marrow Transplant 2007;39(12):775-81.
50. Kanafani ZA, Dakdouki GK, El-Chammas KI, Eid S, Araj GF, Kanj SS. Bloodstream infections infebrile neutropenic patients at a tertiary care center in Lebanon: a view of the past decade. Int JInfect Dis 2007;11(5):450-3.
51. Baskaran ND, Gan GG, Adeeba K, Sam IC. Bacteremia in patients with febrile neutropenia afterchemotherapy at a university medical center in Malaysia. Int J Infect Dis 2007;11(6):513-7.
52. Feld R. Bloodstream infections in cancer patients with febrile neutropenia. Int J Antimicrob Agents2008;32 Suppl 1:S30-3.
53. Pizzo PA. Fever in immunocompromised patients. N Engl J Med 1999;341(12):893-900.
54. Picazo JJ. Management of the febrile neutropenic patient. Int J Antimicrob Agents 2005;26 Suppl2:S120-2.
55. Tumbarello M, Spanu T, Caira M, Trecarichi EM, Laurenti L, Montuori E, et al. Factors associatedwith mortality in bacteremic patients with hematologic malignancies. Diagn Microbiol Infect Dis2009, April 2nd. [Epub ahead of print]; doi:10.1016/j.diagmicrobio.2009.02.008.
56. Klastersky J, Ameye L, Maertens J, Georgala A, Muanza F, Aoun M, et al. Bacteraemia in febrileneutropenic cancer patients. Int J Antimicrob Agents 2007;30 Suppl 1:S51-9.
57. Chatzinikolaou I, Abi-Said D, Bodey GP, Rolston KV, Tarrand JJ, Samonis G. Recent experiencewith Pseudomonas aeruginosa bacteremia in patients with cancer. Retrospective analysis of 245episodes. Arch Intern Med 2000;160(4):501-9.
58. Burnett AK. Acute myeloid leukemia: treatment of adults under 60 years. Rev Clin Exp Hematol2002;6(1):26-45; discussion 86-7.
59. Malagola M, Peli A, Damiani D, Candoni A, Tiribelli M, Martinelli G, et al. Incidence of bacterial andfungal infections in newly diagnosed acute myeloid leukaemia patients younger than 65 yr treatedwith induction regimens including fludarabine: retrospective analysis of 224 cases. Eur J Haematol2008;81(5):354-63.
91
60. Sung L, Gamis A, Alonzo TA, Buxton A, Britton K, Deswarte-Wallace J, et al. Infections andassociation with different intensity of chemotherapy in children with acute myeloid leukemia. Cancer2009;115(5):1100-8.
61. Cassileth PA, Lee SJ, Litzow MR, Miller KB, Stadtmauer EA, Tallman MS, et al. Intensifiedinduction chemotherapy in adult acute myeloid leukemia followed by high-dose chemotherapy andautologous peripheral blood stem cell transplantation: an Eastern Cooperative Oncology Group trial(E4995). Leuk Lymphoma 2005;46(1):55-61.
62. Elonen E, Almqvist A, Hänninen A, Jansson SE, Järventie G, Koistinen P, et al. Comparisonbetween four and eight cycles of intensive chemotherapy in adult acute myeloid leukemia: arandomized trial of the Finnish Leukemia Group. Leukemia 1998;12(7):1041-8.
63. Castaigne S, Chevret S, Archimbaud E, Fenaux P, Bordessoule D, Tilly H, et al. Randomizedcomparison of double induction and timed-sequential induction to a "3 + 7" induction in adults withAML: long-term analysis of the Acute Leukemia French Association (ALFA) 9000 study. Blood2004;104(8):2467-74.
64. Matsouka P, Pagoni M, Zikos P, Giannakoulas N, Apostolidis I, Asprogeraka T, et al. Addition ofcyclosporin-A to chemotherapy in secondary (post-MDS) AML in the elderly. A multicenterrandomized trial of the Leukemia Working Group of the Hellenic Society of Hematology. AnnHematol 2006;85(4):250-6.
65. Kinnunen U, Koistinen P, Ohtonen P, Koskela M, Syrjälä H. Influence of chemotherapy courses onthe rate of bloodstream infections during neutropenia in adult acute myeloid leukaemia. Scand JInfect Dis 2008;40(8):642-7.
66. Fanci R, Leoni F, Longo G. Nosocomial infections in acute leukemia: comparison between youngerand elderly patients. New Microbiol 2008;31(1):89-96.
67. Gratwohl A. Activity survey and historical perspective of autologous stem cell transplantation inEurope. Semin Hematol 2007;44(4):220-6.
68. Nivison-Smith I, Bradstock KF, Dodds AJ, Hawkins PA, Ma DD, Moore JJ, et al. Hematopoieticstem cell transplantation in Australia and New Zealand, 1992-2004. Biol Blood Marrow Transplant2007;13(8):905-12.
69. Gratwohl A, Baldomero H, Frauendorfer K, Rocha V, Apperley J, Niederwieser D. The EBMTactivity survey 2006 on hematopoietic stem cell transplantation: focus on the use of cord bloodproducts. Bone Marrow Transplant 2008;41(8):687-705.
70. Gil L, Styczynski J, Komarnicki M. Infectious complication in 314 patients after high-dose therapyand autologous hematopoietic stem cell transplantation: risk factors analysis and outcome. Infection2007;35(6):421-7.
71. Jantunen E, Itälä M, Lehtinen T, Kuittinen O, Koivunen E, Leppä S, et al. Early treatment-relatedmortality in adult autologous stem cell transplant recipients: a nation-wide survey of 1482transplanted patients. Eur J Haematol 2006;76(3):245-50.
72. Krüger W, Rüssmann B, Kröger N, Salomon C, Ekopf N, Elsner HA, et al. Early infections inpatients undergoing bone marrow or blood stem cell transplantation--a 7 year single centreinvestigation of 409 cases. Bone Marrow Transplant 1999;23(6):589-97.
73. Reich G, Mapara MY, Reichardt P, Dörken B, Maschmeyer G. Infectious complications after high-dose chemotherapy and autologous stem cell transplantation: comparison between patients withlymphoma or multiple myeloma and patients with solid tumors. Bone Marrow Transplant2001;27(5):525-9.
74. Puig N, de la Rubia J, Jarque I, Salavert M, Montesinos P, Sanz J, et al. A study of incidence andcharacteristics of infections in 476 patients from a single center undergoing autologous blood stemcell transplantation. Int J Hematol 2007;86(2):186-92.
75. Pallera AM, Schwartzberg LS. Managing the toxicity of hematopoietic stem cell transplant. JSupport Oncol 2004;2(3):223-37.
92
76. Ketterer N, Espinouse D, Chomarat M, Dumontet C, Moullet I, Rieux C, et al. Infections followingperipheral blood progenitor cell transplantation for lymphoproliferative malignancies: etiology andpotential risk factors. Am J Med 1999;106(2):191-7.
77. Cone JB. Inflammation. Am J Surg 2001;182(6):558-62.
78. Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, et al. Definitions for sepsis andorgan failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCMConsensus Conference Committee. American College of Chest Physicians/Society of Critical CareMedicine. Chest 1992;101(6):1644-55.
79. Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, et al. 2001SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med2003;31(4):1250-6.
80. Thomas L. Germs. N Engl J Med 1972;287(11):553-5.
81. Rangel-Frausto MS, Pittet D, Costigan M, Hwang T, Davis CS, Wenzel RP. The natural history ofthe systemic inflammatory response syndrome (SIRS). A prospective study. JAMA1995;273(2):117-23.
82. Silva E, Passos Rda H, Ferri MB, de Figueiredo LF. Sepsis: from bench to bedside. Clinics2008;63(1):109-20.
83. Lever A, Mackenzie I. Sepsis: definition, epidemiology, and diagnosis. BMJ 2007;335(7625):879-83.
84. Astiz ME, Rackow EC. Septic shock. Lancet 1998;351(9114):1501-5.
85. Cinel I, Dellinger RP. Advances in pathogenesis and management of sepsis. Curr Opin Infect Dis2007;20(4):345-52.
86. Kim I, Moon SO, Kim SH, Kim HJ, Koh YS, Koh GY. Vascular endothelial growth factor expressionof intercellular adhesion molecule 1 (ICAM-1), vascular cell adhesion molecule 1 (VCAM-1), and E-selectin through nuclear factor-kappa B activation in endothelial cells. J Biol Chem2001;276(10):7614-20.
87. Pier GB, Lyczak JB, Wetzler LM. Immunology, infection, and immunity. pp. 718. In. Washington:ASM Press; 2004. p. pp.718.
88. Martins PS, Brunialti MK, da Luz Fernandes M, Martos LS, Gomes NE, Rigato O, et al. Bacterialrecognition and induced cell activation in sepsis. Endocr Metab Immune Disord Drug Targets2006;6(2):183-91.
89. Delves PJ, Roitt IM. The immune system. First of two parts. N Engl J Med 2000;343(1):37-49.
90. Delves PJ, Roitt IM. The immune system. Second of two parts. N Engl J Med 2000;343(2):108-17.
91. Opal SM, DePalo VA. Anti-inflammatory cytokines. Chest 2000;117(4):1162-72.
92. Abbas AK, Murphy KM, Sher A. Functional diversity of helper T lymphocytes. Nature1996;383(6603):787-93.
93. Annane D, Bellissant E, Cavaillon JM. Septic shock. Lancet 2005;365(9453):63-78.
94. Markiewski MM, Nilsson B, Ekdahl KN, Mollnes TE, Lambris JD. Complement and coagulation:strangers or partners in crime? Trends Immunol 2007;28(4):184-92.
95. Castellheim A, Brekke OL, Espevik T, Harboe M, Mollnes TE. Innate immune responses to dangersignals in systemic inflammatory response syndrome and sepsis. Scand J Immunol 2009;69(6):479-91.
96. Walport MJ. Complement. First of two parts. N Engl J Med 2001;344(14):1058-66.
97. Cunneen J, Cartwright M. The puzzle of sepsis: fitting the pieces of the inflammatory response withtreatment. AACN Clin Issues 2004;15(1):18-44.
98. Dellinger RP. Inflammation and coagulation: implications for the septic patient. Clin Infect Dis2003;36(10):1259-65.
93
99. Hack CE, Zeerleder S. The endothelium in sepsis: source of and a target for inflammation. Crit CareMed 2001;29(7 Suppl):S21-7.
100. Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology ofsevere sepsis in the United States: analysis of incidence, outcome, and associated costs of care.Crit Care Med 2001;29(7):1303-10.
101. Vincent JL, de Mendonca A, Cantraine F, Moreno R, Takala J, Suter PM, et al. Use of the SOFAscore to assess the incidence of organ dysfunction/failure in intensive care units: results of amulticenter, prospective study. Working group on "sepsis-related problems" of the EuropeanSociety of Intensive Care Medicine. Crit Care Med 1998;26(11):1793-800.
102. Guidet B, Aegerter P, Gauzit R, Meshaka P, Dreyfuss D. Incidence and impact of organdysfunctions associated with sepsis. Chest 2005;127(3):942-51.
103. Cavaillon JM, Adib-Conquy M, Fitting C, Adrie C, Payen D. Cytokine cascade in sepsis. Scand JInfect Dis 2003;35(9):535-44.
104. Singer M, De Santis V, Vitale D, Jeffcoate W. Multiorgan failure is an adaptive, endocrine-mediated,metabolic response to overwhelming systemic inflammation. Lancet 2004;364(9433):545-8.
105. Brun-Buisson C, Doyon F, Carlet J, Dellamonica P, Gouin F, Lepoutre A, et al. Incidence, riskfactors, and outcome of severe sepsis and septic shock in adults. A multicenter prospective study inintensive care units. French ICU Group for Severe Sepsis. JAMA 1995;274(12):968-74.
106. Padkin A, Goldfrad C, Brady AR, Young D, Black N, Rowan K. Epidemiology of severe sepsisoccurring in the first 24 hrs in intensive care units in England, Wales, and Northern Ireland. CritCare Med 2003;31(9):2332-8.
107. Sundararajan V, MacIsaac CM, Presneill JJ, Cade JF, Visvanathan K. Epidemiology of sepsis inVictoria, Australia. Crit Care Med 2005;33(1):71-80.
108. Cheng B, Xie G, Yao S, Wu X, Guo Q, Gu M, et al. Epidemiology of severe sepsis in critically illsurgical patients in ten university hospitals in China. Crit Care Med 2007;35(11):2538-46.
109. Blanco J, Muriel-Bombin A, Sagredo V, Taboada F, Gandia F, Tamayo L, et al. Incidence, organdysfunction and mortality in severe sepsis: a Spanish multicentre study. Crit Care 2008;12(6):R158.
110. Ruokonen E, Hovilehto S, Kuoppala J, Loisa P, Malmivaara A, Perttilä J, et al. [Care of sepsis inadults]. Aikuisten vaikean sepsiksen hoito. Duodecim 2005;121(15):1662-9.
111. Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud PA, et al. Why don't physiciansfollow clinical practice guidelines? A framework for improvement. JAMA 1999;282(15):1458-65.
112. Kortgen A, Niederprum P, Bauer M. Implementation of an evidence-based "standard operatingprocedure" and outcome in septic shock. Crit Care Med 2006;34(4):943-9.
113. Dellinger RP, Levy MM, Carlet JM, Bion J, Parker MM, Jaeschke R, et al. Surviving SepsisCampaign: international guidelines for management of severe sepsis and septic shock: 2008.Intensive Care Med 2008;34(1):17-60.
114. Rivers E, Nguyen B, Havstad S, Ressler J, Muzzin A, Knoblich B, et al. Early goal-directed therapyin the treatment of severe sepsis and septic shock. N Engl J Med 2001;345(19):1368-77.
115. Vincent JL, Sakr Y, Sprung CL, Ranieri VM, Reinhart K, Gerlach H, et al. Sepsis in Europeanintensive care units: results of the SOAP study. Crit Care Med 2006;34(2):344-53.
116. Nguyen HB, Rivers EP, Abrahamian FM, Moran GJ, Abraham E, Trzeciak S, et al. Severe sepsisand septic shock: review of the literature and emergency department management guidelines. AnnEmerg Med 2006;48(1):28-54.
117. Meyers BR, Sherman E, Mendelson MH, Velasquez G, Srulevitch-Chin E, Hubbard M, et al.Bloodstream infections in the elderly. Am J Med 1989;86(4):379-84.
118. Mackenzie I, Lever A. Management of sepsis. BMJ 2007;335(7626):929-32.
94
119. Valles J, Rello J, Ochagavia A, Garnacho J, Alcala MA. Community-acquired bloodstream infectionin critically ill adult patients: impact of shock and inappropriate antibiotic therapy on survival. Chest2003;123(5):1615-24.
120. Harbarth S, Garbino J, Pugin J, Romand JA, Lew D, Pittet D. Inappropriate initial antimicrobialtherapy and its effect on survival in a clinical trial of immunomodulating therapy for severe sepsis.Am J Med 2003;115(7):529-35.
121. Wu CJ, Lee HC, Lee NY, Shih HI, Ko NY, Wang LR, et al. Predominance of Gram-negative bacilliand increasing antimicrobial resistance in nosocomial bloodstream infections at a university hospitalin southern Taiwan, 1996-2003. J Microbiol Immunol Infect 2006;39(2):135-43.
122. Hsueh PR, Chen WH, Luh KT. Relationships between antimicrobial use and antimicrobialresistance in Gram-negative bacteria causing nosocomial infections from 1991-2003 at a universityhospital in Taiwan. Int J Antimicrob Agents 2005;26(6):463-72.
123. Kang CI, Kim SH, Park WB, Lee KD, Kim HB, Kim EC, et al. Bloodstream infections caused byantibiotic-resistant gram-negative bacilli: risk factors for mortality and impact of inappropriate initialantimicrobial therapy on outcome. Antimicrob Agents Chemother 2005;49(2):760-6.
124. Schuetz P, Christ-Crain M, Muller B. Biomarkers to improve diagnostic and prognostic accuracy insystemic infections. Curr Opin Crit Care 2007;13(5):578-85.
125. Meisner M. Biomarkers of sepsis: clinically useful? Curr Opin Crit Care 2005;11(5):473-80.
126. Pfafflin A, Schleicher E. Inflammation markers in point-of-care testing (POCT). Anal Bioanal Chem2009;393(5):1473-80.
127. Shine B, de Beer FC, Pepys MB. Solid phase radioimmunoassays for human C-reactive protein.Clin Chim Acta 1981;117(1):13-23.
128. Vigushin DM, Pepys MB, Hawkins PN. Metabolic and scintigraphic studies of radioiodinated humanC-reactive protein in health and disease. J Clin Invest 1993;91(4):1351-7.
129. Szalai AJ. The biological functions of C-reactive protein. Vascul Pharmacol 2002;39(3):105-7.
130. Foglar C, Lindsey RW. C-reactive protein in orthopedics. Orthopedics 1998;21(6):687-91.
131. Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Invest 2003;111(12):1805-12.
132. Mackenzie I, Woodhouse J. C-reactive protein concentrations during bacteraemia: a comparisonbetween patients with and without liver dysfunction. Intensive Care Med 2006;32(9):1344-51.
133. Gabay C, Kushner I. Acute-phase proteins and other systemic responses to inflammation. N Engl JMed 1999;340(6):448-54.
134. George ML, Eccles SA, Tutton MG, Abulafi AM, Swift RI. Correlation of plasma and serum vascularendothelial growth factor levels with platelet count in colorectal cancer: clinical evidence of plateletscavenging? Clin Cancer Res 2000;6(8):3147-52.
135. Herzum I, Renz H. Inflammatory markers in SIRS, sepsis and septic shock. Curr Med Chem2008;15(6):581-7.
136. Oberholzer A, Oberholzer C, Moldawer LL. Cytokine signaling--regulation of the immune responsein normal and critically ill states. Crit Care Med 2000;28(4 Suppl):N3-12.
137. Oczenski W, Fitzgerald RD, Schwarz S. Procalcitonin: a new parameter for the diagnosis ofbacterial infection in the peri-operative period. Eur J Anaesthesiol 1998;15(2):202-9.
138. Varpula M, Pulkki K, Karlsson S, Ruokonen E, Pettilä V. Predictive value of N-terminal pro-brainnatriuretic peptide in severe sepsis and septic shock. Crit Care Med 2007;35(5):1277-83.
139. Villarete LH, Remick DG. Transcriptional and post-transcriptional regulation of interleukin-8. Am JPathol 1996;149(5):1685-93.
140. Waage A, Brandtzaeg P, Halstensen A, Kierulf P, Espevik T. The complex pattern of cytokines inserum from patients with meningococcal septic shock. Association between interleukin 6, interleukin1, and fatal outcome. J Exp Med 1989;169(1):333-8.
95
141. van Gestel A, Bakker J, Veraart CP, van Hout BA. Prevalence and incidence of severe sepsis inDutch intensive care units. Crit Care 2004;8(4):R153-62.
142. Rintala EM, Aittoniemi J, Laine S, Nevalainen TJ, Nikoskelainen J. Early identification of bacteremiaby biochemical markers of systemic inflammation. Scand J Clin Lab Invest 2001;61(7):523-30.
143. Castelli GP, Pognani C, Meisner M, Stuani A, Bellomi D, Sgarbi L. Procalcitonin and C-reactiveprotein during systemic inflammatory response syndrome, sepsis and organ dysfunction. Crit Care2004;8(4):R234-42.
144. Kallio R, Surcel HM, Bloigu A, Syrjälä H. C-reactive protein, procalcitonin and interleukin-8 in theprimary diagnosis of infections in cancer patients. Eur J Cancer 2000;36(7):889-94.
145. Rose PE, Johnson SA, Meakin M, Mackie PH, Stuart J. Serial study of C-reactive protein duringinfection in leukaemia. J Clin Pathol 1981;34(3):263-6.
146. Persson L, Engervall P, Magnuson A, Vikerfors T, Söderquist B, Hansson LO, et al. Use ofinflammatory markers for early detection of bacteraemia in patients with febrile neutropenia. ScandJ Infect Dis 2004;36(5):365-71.
147. von Lilienfeld-Toal M, Dietrich MP, Glasmacher A, Lehmann L, Breig P, Hahn C, et al. Markers ofbacteremia in febrile neutropenic patients with hematological malignancies: procalcitonin and IL-6are more reliable than C-reactive protein. Eur J Clin Microbiol Infect Dis 2004;23(7):539-44.
148. Sandri MT, Passerini R, Leon ME, Peccatori FA, Zorzino L, Salvatici M, et al. Procalcitonin as auseful marker of infection in hemato-oncological patients with fever. Anticancer Res2008;28(5B):3061-5.
149. Roy H, Bhardwaj S, Ylä-Herttuala S. Biology of vascular endothelial growth factors. FEBS Lett2006;580(12):2879-87.
150. Ferrara N, Gerber HP, LeCouter J. The biology of VEGF and its receptors. Nat Med 2003;9(6):669-76.
151. Senger DR, Galli SJ, Dvorak AM, Perruzzi CA, Harvey VS, Dvorak HF. Tumor cells secrete avascular permeability factor that promotes accumulation of ascites fluid. Science1983;219(4587):983-5.
152. Pugh CW, Ratcliffe PJ. Regulation of angiogenesis by hypoxia: role of the HIF system. Nat Med2003;9(6):677-84.
153. Kroll J, Waltenberger J. A novel function of VEGF receptor-2 (KDR): rapid release of nitric oxide inresponse to VEGF-A stimulation in endothelial cells. Biochem Biophys Res Commun1999;265(3):636-9.
154. Yano K, Liaw PC, Mullington JM, Shih SC, Okada H, Bodyak N, et al. Vascular endothelial growthfactor is an important determinant of sepsis morbidity and mortality. J Exp Med 2006;203(6):1447-58.
155. Pickkers P, Sprong T, Eijk L, Hoeven H, Smits P, Deuren M. Vascular endothelial growth factor isincreased during the first 48 hours of human septic shock and correlates with vascular permeability.Shock 2005;24(6):508-12.
156. van der Flier M, van Leeuwen HJ, van Kessel KP, Kimpen JL, Hoepelman AI, Geelen SP. Plasmavascular endothelial growth factor in severe sepsis. Shock 2005;23(1):35-8.
157. Kraft A, Weindel K, Ochs A, Marth C, Zmija J, Schumacher P, et al. Vascular endothelial growthfactor in the sera and effusions of patients with malignant and nonmalignant disease. Cancer1999;85(1):178-87.
158. Verheul HM, Hoekman K, Luykx-de Bakker S, Eekman CA, Folman CC, Broxterman HJ, et al.Platelet: transporter of vascular endothelial growth factor. Clin Cancer Res 1997;3(12 Pt 1):2187-90.
159. Choi JH, Kim HC, Lim HY, Nam DK, Kim HS, Yi JW, et al. Vascular endothelial growth factor in theserum of patients with non-small cell lung cancer: correlation with platelet and leukocyte counts.Lung Cancer 2001;33(2-3):171-9.
96
160. Gaudry M, Brégerie O, Andrieu V, El Benna J, Pocidalo MA, Hakim J. Intracellular pool of vascularendothelial growth factor in human neutrophils. Blood 1997;90(10):4153-61.
161. Kusumanto YH, Dam WA, Hospers GA, Meijer C, Mulder NH. Platelets and granulocytes, inparticular the neutrophils, form important compartments for circulating vascular endothelial growthfactor. Angiogenesis 2003;6(4):283-7.
162. Salven P, Orpana A, Joensuu H. Leukocytes and platelets of patients with cancer contain highlevels of vascular endothelial growth factor. Clin Cancer Res 1999;5(3):487-91.
163. Levin ER, Gardner DG, Samson WK. Natriuretic peptides. N Engl J Med 1998;339(5):321-8.
164. Pfister R, Scholz M, Wielckens K, Erdmann E, Schneider CA. Use of NT-proBNP in routine testingand comparison to BNP. Eur J Heart Fail 2004;6(3):289-93.
165. Kotanidou A, Karsaliakos P, Tzanela M, Mavrou I, Kopterides P, Papadomichelakis E, et al.Prognostic importance of increased plasma amino-terminal pro-brain natriuretic peptide levels in alarge noncardiac, general intensive care unit population. Shock 2009;31(4):342-7.
166. Meyer B, Huelsmann M, Wexberg P, Delle Karth G, Berger R, Moertl D, et al. N-terminal pro-B-typenatriuretic peptide is an independent predictor of outcome in an unselected cohort of critically illpatients. Crit Care Med 2007;35(10):2268-73.
167. Zakynthinos E, Kiropoulos T, Gourgoulianis K, Filippatos G. Diagnostic and prognostic impact ofbrain natriuretic peptide in cardiac and noncardiac diseases. Heart Lung 2008;37(4):275-85.
168. Ueda S, Nishio K, Akai Y, Fukushima H, Ueyama T, Kawai Y, et al. Prognostic value of increasedplasma levels of brain natriuretic peptide in patients with septic shock. Shock 2006;26(2):134-9.
169. Rivers EP, McCord J, Otero R, Jacobsen G, Loomba M. Clinical utility of B-type natriuretic peptidein early severe sepsis and septic shock. J Intensive Care Med 2007;22(6):363-73.
170. Nikolaou NI, Goritsas C, Dede M, Paissios NP, Papavasileiou M, Rombola AT, et al. Brainnatriuretic peptide increases in septic patients without severe sepsis or shock. Eur J Intern Med2007;18(7):535-41.
171. Witthaut R, Busch C, Fraunberger P, Walli A, Seidel D, Pilz G, et al. Plasma atrial natriureticpeptide and brain natriuretic peptide are increased in septic shock: impact of interleukin-6 andsepsis-associated left ventricular dysfunction. Intensive Care Med 2003;29(10):1696-702.
172. Rudiger A, Fischler M, Harpes P, Gasser S, Hornemann T, von Eckardstein A, et al. In critically illpatients, B-type natriuretic peptide (BNP) and N-terminal pro-BNP levels correlate with C-reactiveprotein values and leukocyte counts. Int J Cardiol 2008;126(1):28-31.
173. Shor R, Rozenman Y, Bolshinsky A, Harpaz D, Tilis Y, Matas Z, et al. BNP in septic patients withoutsystolic myocardial dysfunction. Eur J Intern Med 2006;17(8):536-40.
174. Burjonroppa SC, Tong AT, Xiao LC, Johnson MM, Yusuf SW, Lenihan DJ. Cancer patients withmarkedly elevated B-type natriuretic peptide may not have volume overload. Am J Clin Oncol2007;30(3):287-93.
175. Billeter A, Turina M, Seifert B, Mica L, Stocker R, Keel M. Early serum procalcitonin, interleukin-6,and 24-hour lactate clearance: useful indicators of septic infections in severely traumatized patients.World J Surg 2009;33(3):558-66.
176. Friedman G, Berlot G, Kahn RJ, Vincent JL. Combined measurements of blood lactateconcentrations and gastric intramucosal pH in patients with severe sepsis. Crit Care Med1995;23(7):1184-93.
177. Mikkelsen ME, Miltiades AN, Gaieski DF, Goyal M, Fuchs BD, Shah CV, et al. Serum lactate isassociated with mortality in severe sepsis independent of organ failure and shock. Crit Care Med2009;37(5):1670-7.
178. Kobayashi S, Gando S, Morimoto Y, Nanzaki S, Kemmotsu O. Serial measurement of arteriallactate concentrations as a prognostic indicator in relation to the incidence of disseminatedintravascular coagulation in patients with systemic inflammatory response syndrome. Surg Today2001;31(10):853-9.
97
179. Ramzi J, Mohamed Z, Yosr B, Karima K, Raihane B, Lamia A, et al. Predictive factors of septicshock and mortality in neutropenic patients. Hematology 2007;12(6):543-8.
180. Juutilainen A, Hämäläinen S, Matinlauri I, Kuittinen T, Nousiainen T, Pulkki K, et al. Serial plasmalactate measurements in haematological patients with neutropenic fever. Accepted for publication.Scand J Infect Dis 2009.
181. Hambach L, Eder M, Dammann E, Schrauder A, Sykora KW, Dieterich C, et al. Diagnostic value ofprocalcitonin serum levels in comparison with C-reactive protein in allogeneic stem celltransplantation. Haematologica 2002;87(6):643-51.
182. Linscheid P, Seboek D, Schaer DJ, Zulewski H, Keller U, Müller B. Expression and secretion ofprocalcitonin and calcitonin gene-related peptide by adherent monocytes and by macrophage-activated adipocytes. Crit Care Med 2004;32(8):1715-21.
183. Christ-Crain M, Stolz D, Bingisser R, Müller C, Miedinger D, Huber PR, et al. Procalcitonin guidanceof antibiotic therapy in community-acquired pneumonia: a randomized trial. Am J Respir Crit CareMed 2006;174(1):84-93.
184. von Lilienfeld-Toal M, Schneider A, Orlopp K, Hahn-Ast C, Glasmacher A, Stüber F. Change ofprocalcitonin predicts clinical outcome of febrile episodes in patients with hematologicalmalignancies. Support Care Cancer 2006;14(12):1241-5.
185. Sakr Y, Sponholz C, Tuche F, Brunkhorst F, Reinhart K. The role of procalcitonin in febrileneutropenic patients: review of the literature. Infection 2008;36(5):396-407.
186. Becker KL, Snider R, Nylen ES. Procalcitonin assay in systemic inflammation, infection, and sepsis:clinical utility and limitations. Crit Care Med 2008;36(3):941-52.
187. Svaldi M, Hirber J, Lanthaler AI, Mayr O, Faes S, Peer E, et al. Procalcitonin-reduced sensitivityand specificity in heavily leucopenic and immunosuppressed patients. Br J Haematol2001;115(1):53-7.
188. Blijlevens NM, Donnelly JP, Meis JF, De Keizer MH, De Pauw BE. Procalcitonin does notdiscriminate infection from inflammation after allogeneic bone marrow transplantation. Clin DiagnLab Immunol 2000;7(6):889-92.
189. Jimeno A, Garcia-Velasco A, del Val O, Gonzalez-Billalabeitia E, Hernando S, Hernandez R, et al.Assessment of procalcitonin as a diagnostic and prognostic marker in patients with solid tumors andfebrile neutropenia. Cancer 2004;100(11):2462-9.
190. de Bont ES, Vellenga E, Swaanenburg JC, Fidler V, Visser-van Brummen PJ, Kamps WA. PlasmaIL-8 and IL-6 levels can be used to define a group with low risk of septicaemia among cancerpatients with fever and neutropenia. Br J Haematol 1999;107(2):375-80.
191. Engel A, Mack E, Kern P, Kern WV. An analysis of interleukin-8, interleukin-6 and C-reactive proteinserum concentrations to predict fever, gram-negative bacteremia and complicated infection inneutropenic cancer patients. Infection 1998;26(4):213-21.
192. Loisa P, Rinne T, Laine S, Hurme M, Kaukinen S. Anti-inflammatory cytokine response and thedevelopment of multiple organ failure in severe sepsis. Acta Anaesthesiol Scand 2003;47(3):319-25.
193. Bozza FA, Salluh JI, Japiassu AM, Soares M, Assis EF, Gomes RN, et al. Cytokine profiles asmarkers of disease severity in sepsis: a multiplex analysis. Crit Care 2007;11(2):R49.
194. Uys A, Rapoport BL, Fickl H, Meyer PW, Anderson R. Prediction of outcome in cancer patients withfebrile neutropenia: comparison of the Multinational Association of Supportive Care in Cancer risk-index score with procalcitonin, C-reactive protein, serum amyloid A, and interleukins-1beta, -6, -8and -10. Eur J Cancer Care (Engl) 2007;16(6):475-83.
195. Youden WJ. Index for rating diagnostic tests. Cancer 1950;3(1):32-5.
196. Markou N, Demopoulou E, Myrianthefs P. The critically ill patient with cancer - indications forIntensive Care Unit admission and outcomes. J Buon 2008;13(4):469-78.
98
197. Taccone FS, Artigas AA, Sprung CL, Moreno R, Sakr Y, Vincent JL. Characteristics and outcomesof cancer patients in European ICUs. Crit Care 2009;13(1):R15.
198. Estey EH. Advances in the management of AML in the elderly. Clin Adv Hematol Oncol2007;5(3):185-7.
199. Silfvast T, Pettilä V, Ihalainen A, Elonen E. Multiple organ failure and outcome of critically ill patientswith haematological malignancy. Acta Anaesthesiol Scand 2003;47(3):301-6.
200. Jantunen E, Canals C, Rambaldi A, Ossenkoppele G, Allione B, Blaise D, et al. Autologous stemcell transplantation in elderly patients (>60 years) with diffuse large B-cell lymphoma: an analysisbased on data in the European Blood and Marrow Transplantation registry. Haematologica2008;93(12):1837-42.
201. Kuittinen T, Husso-Saastamoinen M, Sipola P, Vuolteenaho O, Ala-Kopsala M, Nousiainen T, et al.Very acute cardiac toxicity during BEAC chemotherapy in non-Hodgkin's lymphoma patientsundergoing autologous stem cell transplantation. Bone Marrow Transplant 2005;36(12):1077-82.
202. Cherif H, Kronvall G, Bjorkholm M, Kalin M. Bacteraemia in hospitalised patients with malignantblood disorders: a retrospective study of causative agents and their resistance profiles during a 14-year period without antibacterial prophylaxis. Hematol J 2003;4(6):420-6.
203. Salazar R, Sola C, Maroto P, Tabernero JM, Brunet J, Verger G, et al. Infectious complications in126 patients treated with high-dose chemotherapy and autologous peripheral blood stem celltransplantation. Bone Marrow Transplant 1999;23(1):27-33.
204. Sigurdardottir K, Digranes A, Harthug S, Nesthus I, Tangen JM, Dybdahl B, et al. A multi-centreprospective study of febrile neutropenia in Norway: microbiological findings and antimicrobialsusceptibility. Scand J Infect Dis 2005;37(6-7):455-64.
205. Auner HW, Sill H, Mulabecirovic A, Linkesch W, Krause R. Infectious complications after autologoushematopoietic stem cell transplantation: comparison of patients with acute myeloid leukemia,malignant lymphoma, and multiple myeloma. Ann Hematol 2002;81(7):374-7.
206. Slavin MA, Grigg AP, Schwarer AP, Szer J, Spencer A, Sainani A, et al. A randomized comparisonof empiric or pre-emptive antibiotic therapy after hematopoietic stem cell transplantation. BoneMarrow Transplant 2007;40(2):157-63.
207. Nihtinen A, Anttila VJ, Elonen E, Juvonen E, Volin L, Ruutu T. Effect of fluconazole prophylaxis onthe incidence of invasive candida infections and bacteraemias in patients with acute leukaemia. EurJ Haematol 2008;80(5):391-6.
208. Jantunen E, Salonen J, Juvonen E, Koivunen E, Siitonen T, Lehtinen T, et al. Invasive fungalinfections in autologous stem cell transplant recipients: a nation-wide study of 1188 transplantedpatients. Eur J Haematol 2004;73(3):174-8.
209. Craig M, Cumpston AD, Hobbs GR, Devetten MP, Sarwari AR, Ericson SG. The clinical impact ofantibacterial prophylaxis and cycling antibiotics for febrile neutropenia in a hematologicalmalignancy and transplantation unit. Bone Marrow Transplant 2007;39(8):477-82.
210. Cheong HS, Kang CI, Wi YM, Kim ES, Lee JS, Ko KS, et al. Clinical significance and predictors ofcommunity-onset Pseudomonas aeruginosa bacteremia. Am J Med 2008;121(8):709-14.
211. Hakki M, Limaye AP, Kim HW, Kirby KA, Corey L, Boeckh M. Invasive Pseudomonas aeruginosainfections: high rate of recurrence and mortality after hematopoietic cell transplantation. BoneMarrow Transplant 2007;39(11):687-93.
212. Maschmeyer G, Braveny I. Review of the incidence and prognosis of Pseudomonas aeruginosainfections in cancer patients in the 1990s. Eur J Clin Microbiol Infect Dis 2000;19(12):915-25.
213. Scheetz MH, Hoffman M, Bolon MK, Schulert G, Estrellado W, Baraboutis IG, et al. Morbidityassociated with Pseudomonas aeruginosa bloodstream infections. Diagn Microbiol Infect Dis2009;64(3):311-9.
214. Jantunen E, Hämäläinen S, Kuittinen T, Penttilä K, Pyörälä M, Juutilainen A, et al. Towards saferautotransplants in patients with non-Hodgkin's lymphoma: cardiac pre-evaluation, angiotensin-
99
converting enzyme inhibition in patients with decreased left ventricular function, antimicrobialprophylaxis and vigilant supportive care. Bone Marrow Transplant 2009;43 (Suppl. 1):S386(abstract).
215. Rafat N, Hanusch C, Brinkkoetter PT, Schulte J, Brade J, Zijlstra JG, et al. Increased circulatingendothelial progenitor cells in septic patients: correlation with survival. Crit Care Med2007;35(7):1677-84.
216. van der Heijden M, van Nieuw Amerongen GP, Koolwijk P, van Hinsbergh VW, Groeneveld AB.Angiopoietin-2, permeability oedema, occurrence and severity of ALI/ARDS in septic and non-septiccritically ill patients. Thorax 2008;63(10):903-9.
217. Shapiro NI, Yano K, Okada H, Fischer C, Howell M, Spokes KC, et al. A prospective, observationalstudy of soluble FLT-1 and vascular endothelial growth factor in sepsis. Shock 2008;29(4):452-7.
218. Salgado R, Vermeulen PB, Benoy I, Weytjens R, Huget P, Van Marck E, et al. Platelet number andinterleukin-6 correlate with VEGF but not with bFGF serum levels of advanced cancer patients. Br JCancer 1999;80(5-6):892-7.
219. Salgado R, Benoy I, Bogers J, Weytjens R, Vermeulen P, Dirix L, et al. Platelets and vascularendothelial growth factor (VEGF): a morphological and functional study. Angiogenesis 2001;4(1):37-43.
220. Benoy I, Salgado R, Colpaert C, Weytjens R, Vermeulen PB, Dirix LY. Serum interleukin 6, plasmaVEGF, serum VEGF, and VEGF platelet load in breast cancer patients. Clin Breast Cancer2002;2(4):311-5.
221. Ruskoaho H. Cardiac hormones as diagnostic tools in heart failure. Endocr Rev 2003;24(3):341-56.
222. Bettencourt PM. Clinical usefulness of B-type natriuretic peptide measurement: present and futureperspectives. Heart 2005;91(11):1489-94.
223. Kibbler CC, Prentice HG. Pathogen 'shift' in febrile neutropenia. Curr Opin Infect Dis1999;12(4):351-4.
224. Spielberger R, Stiff P, Bensinger W, Gentile T, Weisdorf D, Kewalramani T, et al. Palifermin for oralmucositis after intensive therapy for hematologic cancers. N Engl J Med 2004;351(25):2590-8.
225. Johansson JE, Hasseus B, Johansson P, Eklöf C, Ohman D, Stockelberg D. Gut protection bypalifermin during autologous haematopoietic SCT. Bone Marrow Transplant 2009;43(10):807-11.
226. Köstler WJ, Hejna M, Wenzel C, Zielinski CC. Oral mucositis complicating chemotherapy and/orradiotherapy: options for prevention and treatment. CA Cancer J Clin 2001;51(5):290-315.
227. Tissari P, Zumla A, Tarkka E, Mero S, Savolainen L, Vaara M, et al. Accurate and rapid speciationof bacteria from positive blood cultures using a novel DNA-based microarray platform. Lancet 2009,accepted.

SARI HÄMÄLÄINEN
Severe Sepsis in Neutropenic
Haematological Patients
ISBN 978-951-27-1372-1ISBN 978-951-27-1389-9 (PDF)ISSN 1235-0303
D 472 • SA
RI H
ÄM
ÄLÄ
INEN
• Severe Sepsis in Neutro
penic Haem
atolo
gical Patients
KUOPION YLIOPISTON JULKAISUJA D. LÄÄKETIEDE 472 KUOPIO UNIVERSITY PUBLICATIONS D. MEDICAL SCIENCES 472