
Severe Acute Respiratory Syndrome ( SARS )home.sums.ac.ir/~shafieian/files/SARS.pdf · Clinical...
33
Transcript of Severe Acute Respiratory Syndrome ( SARS )home.sums.ac.ir/~shafieian/files/SARS.pdf · Clinical...


Severe Acute Respiratory Syndrome
( SARS )
Severe Acute Respiratory Syndrome
( SARS )
Dr. Mohammad Rahim KadivarPediatrics Infections Specialist
Shiraz University of Medical Sciences
Slides Designer:
Dr. Ramin Shafieian
R. Dadrast

What is SARS ?• A severe acute respiratory illness that has recently been reported in some countries.
• A new mutation of Coronavirusis suspected as the cause .
• Majority of patients are adults.
What is SARS ?• A severe acute respiratory illness that has recently been reported in some countries.
• A new mutation of Coronavirusis suspected as the cause .
• Majority of patients are adults.

Coronavirae FamilyCoronavirae Family

nCoronavirus family also has the property of surviving in dry air/surfaces for up to 3 hours.n In these conditions, the virus crystallizes,
and can float in the air like dust.n It is suspected that the SARS
virus can be transmitted in this manner.
nnCoronavirusCoronavirus family also has the property family also has the property of surviving in dry air/surfaces for up to 3 of surviving in dry air/surfaces for up to 3 hours.hours.nn In these conditions, the virus crystallizes, In these conditions, the virus crystallizes,
and can float in the air like dust.and can float in the air like dust.nn It is suspected that the SARSIt is suspected that the SARS
virus can be transmitted in this manner.virus can be transmitted in this manner.
Schematic view of a crystallized virus particleSchematic view of a Schematic view of a crystallized virus particlecrystallized virus particle

How does SARS spread?How does SARS spread?How does SARS spread?nNOT likely airborne
(recent concern?)nDroplets
- Via close contact with an infected personnContaminated working
surfaces (e.g. fomites, stainless steel, doorknobs)~ survival up to 6 hours
nnNOT likely airborne NOT likely airborne (recent concern?)(recent concern?)nnDropletsDroplets
-- Via close contact with Via close contact with an infected personan infected personnnContaminated working Contaminated working
surfaces (e.g. surfaces (e.g. fomitesfomites, , stainless steel, doorknobs)stainless steel, doorknobs)~ survival up to 6 hours~ survival up to 6 hours
Methods of TransmissionMethods of TransmissionMethods of Transmission
n Most frequent method of transmission of coronavirus from person to person is droplet transmission.n If the sick person coughs or sneezes, the
virus can be carried in saliva droplets to people nearby, infecting them.
nn Most frequent method of transmission of Most frequent method of transmission of coronaviruscoronavirus from person to person is from person to person is droplet transmission.droplet transmission.nn If the sick person coughs or sneezes, the If the sick person coughs or sneezes, the
virus can be carried in saliva droplets to virus can be carried in saliva droplets to people nearby, infecting them.people nearby, infecting them.
Incubation period is typically 2 - 7 days, may
be up to 10 days.
Incubation period is typically 2 - 7 days, may
be up to 10 days.
Symptoms and Signs of SARS• Fever
• Chills
• Headache
• General feeling of discomfort
• Body aches
• Dry non-productive cough
• Breathing difficulty
• Hypoxia
Symptoms and Signs of SARS• Fever
• Chills
• Headache
• General feeling of discomfort
• Body aches
• Dry non-productive cough
• Breathing difficulty
• Hypoxia
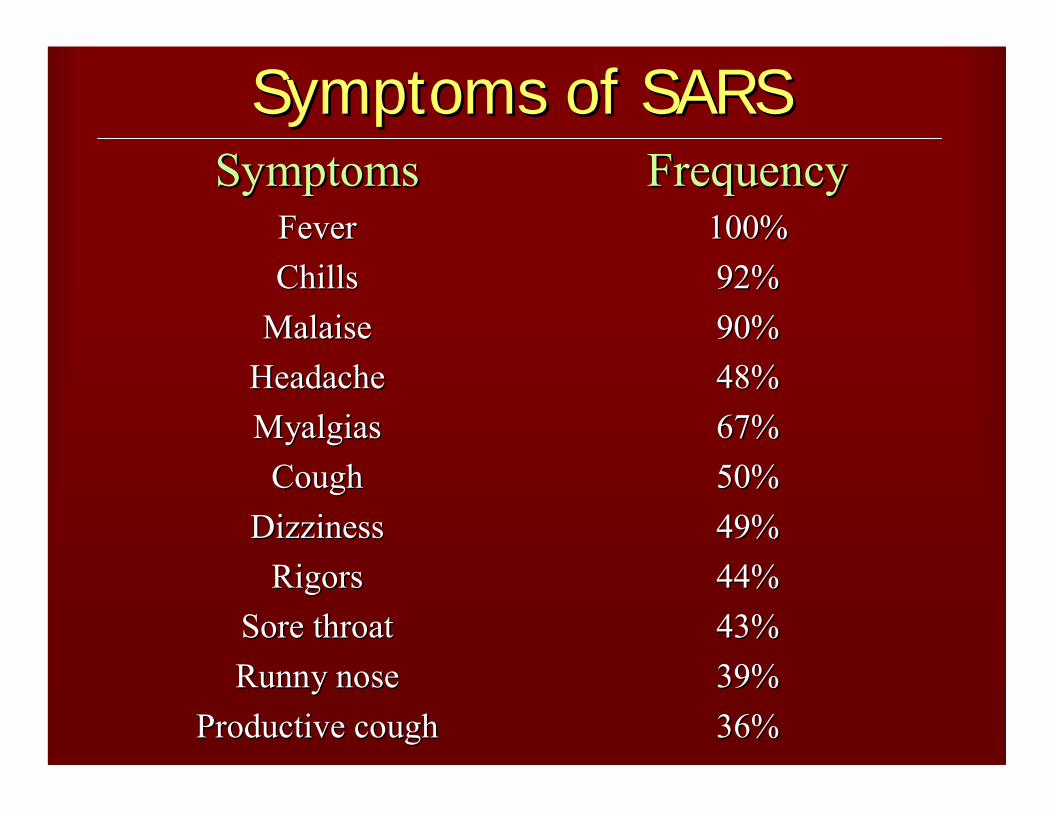
Symptoms of SARSSymptoms of SARSSymptoms of SARSFrequencyFrequency
100%100%92%92%90%90%48%48%67%67%50%50%49%49%44%44%43%43%39%39%36%36%
SymptomsSymptomsFeverFeverChillsChills
MalaiseMalaiseHeadacheHeadacheMyalgiasMyalgias
CoughCoughDizzinessDizziness
RigorsRigorsSore throatSore throatRunny noseRunny nose
Productive coughProductive cough

Clinical Course of SARSClinical Course of SARSClinical Course of SARSn Most patients adults aged 25-70 years , has occurred in
children.n Begins with fever > 38 °C , often with chills and
shaking , sometimes headache , malaise , muscle aches.
n May initially have only mild respiratory symptomsn After 3-5 days , lower respiratory phase begins with
dry cough.n 80 – 90 % begin to recover slowly by day 6 or 7 .n 10 – 20 % have severe respiratory illness which might
require mechanical ventilation (ARDS).n Case fatality rate 3.5%
nn Most patients adults aged Most patients adults aged 2525--7070 years , has occurred in years , has occurred in children.children.
nn Begins with Begins with feverfever > 38 > 38 °°CC , often with , often with chillschills and and shakingshaking , sometimes , sometimes headacheheadache , , malaisemalaise , , muscle muscle achesaches..
nn May initially have only mild respiratory symptomsMay initially have only mild respiratory symptomsnn After After 33--55 days , lower respiratory phase begins with days , lower respiratory phase begins with
dry cough.dry cough.nn 80 80 –– 90 %90 % begin to recover slowly by begin to recover slowly by dayday 66 or or 7 7 ..nn 10 10 –– 20 %20 % have severe respiratory illness which might have severe respiratory illness which might
require mechanical ventilation (ARDS).require mechanical ventilation (ARDS).nn Case fatality rate 3.5%Case fatality rate 3.5%

Suspect case :1. A person presenting after 1 November 2002 with history of :Ø High fever (> 38
oC)
And Ø Cough or breathing difficultyAndone or more of the following exposures during the 10 days
period to onset of symptoms:Ø Close contact with a person who is a suspect or probable case
of SARS;Ø History of travel, to an affected areaØ Residing in an affected area
Suspect case :1. A person presenting after 1 November 2002 with history of :Ø High fever (> 38
oC)
And Ø Cough or breathing difficultyAndone or more of the following exposures during the 10 days
period to onset of symptoms:Ø Close contact with a person who is a suspect or probable case
of SARS;Ø History of travel, to an affected areaØ Residing in an affected area

Suspect case: (continue)
2. A person with an unexplained acute respiratory illness resulting in death after 1 November 2002, but on whom no autopsy has been performed .
And
one or more of the following exposures during to 10 days prior to onset of symptoms:
ü Close contact, with a person who is suspect or probable case of SARS;
ü History of travel to an affected areaü Residing in area an affected .
Suspect case: (continue)
2. A person with an unexplained acute respiratory illness resulting in death after 1 November 2002, but on whom no autopsy has been performed .
And
one or more of the following exposures during to 10 days prior to onset of symptoms:
ü Close contact, with a person who is suspect or probable case of SARS;
ü History of travel to an affected areaü Residing in area an affected .

Probable case:1. A suspect case with radiographic evidence of infiltrates consistent with pneumonia or respiratory distress syndrome (RDS) on chest X-ray (CXR).
2. A suspect case with autopsy findings consistent with the pathology of RDS without an identifiable cause.
Probable case:1. A suspect case with radiographic evidence of infiltrates consistent with pneumonia or respiratory distress syndrome (RDS) on chest X-ray (CXR).
2. A suspect case with autopsy findings consistent with the pathology of RDS without an identifiable cause.

EXCLUSION criteria:A case should be excluded if an alternative
diagnosis can fully explain the illness.
EXCLUSION criteria:A case should be excluded if an alternative
diagnosis can fully explain the illness.

1) Close Contact : having cared for, lived with, or had direct contact with respiratory secretions or body fluids of a suspect or probable case of SARS.
2) Affected area : an area in which local chain(s) of transmission of SARS is/are occurring as reported by the national public health authorities.
1) Close Contact : having cared for, lived with, or had direct contact with respiratory secretions or body fluids of a suspect or probable case of SARS.
2) Affected area : an area in which local chain(s) of transmission of SARS is/are occurring as reported by the national public health authorities.

Diagnostic Testing :Initial diagnostic Testing should include:
• CBC - Platelets
• Creatinine Phosphokinase Levels
• Transaminases Levels
• Plasma Sodium
• Chest Radiograph
• Pulse Oximetry
• Blood Cultures
• Sputum Gram’s Stains and Cultures
• Testing for Viral Respiratory Pathogens
Diagnostic Testing :Initial diagnostic Testing should include:
• CBC - Platelets
• Creatinine Phosphokinase Levels
• Transaminases Levels
• Plasma Sodium
• Chest Radiograph
• Pulse Oximetry
• Blood Cultures
• Sputum Gram’s Stains and Cultures
• Testing for Viral Respiratory Pathogens

Chest X-ray :ü Chest radiograph might be normal during the febrile prodrome and throughout the course of the illness.
ü In a substantial proportion of the patients the respiratory phase is characterized by early focal interstitial infiltrates progressing to more generalized, patchy and interstitial infiltrates.
ü Some chest radiographs from patients in late stages of SARS also have shown areas of consolidation.
Chest X-ray :ü Chest radiograph might be normal during the febrile prodrome and throughout the course of the illness.
ü In a substantial proportion of the patients the respiratory phase is characterized by early focal interstitial infiltrates progressing to more generalized, patchy and interstitial infiltrates.
ü Some chest radiographs from patients in late stages of SARS also have shown areas of consolidation.

Treatment :Because the etiology of SARS has not been determined definitely, treatment is empirical and includes:
Ø Variety of antibiotics to presumptively treat known bacterial agents of atypical pneumonia.
ØAntiviral agents such as Oseltamivir or Ribavirin.
Ø Steroids have also been suggested.
Treatment :Because the etiology of SARS has not been determined definitely, treatment is empirical and includes:
Ø Variety of antibiotics to presumptively treat known bacterial agents of atypical pneumonia.
ØAntiviral agents such as Oseltamivir or Ribavirin.
Ø Steroids have also been suggested.

Convalescent cases of SARS:We advise that the following criteria are considered prior to making a decision regarding a convalescent case:Clinical symptoms/findings:
• Afebrile for 48 hours• Resolving Cough
Laboratory Tests (If previously abnormal):• White cell count returning to normal• Platelet count returning to normal• Creatine Phosphokinase returning to normal• Plasma Sodium returning to normal• C Reactive Protein returning to normal
Radiological Findings:• Improving Chest X-ray changes
Convalescent cases of SARS:We advise that the following criteria are considered prior to making a decision regarding a convalescent case:Clinical symptoms/findings:
• Afebrile for 48 hours• Resolving Cough
Laboratory Tests (If previously abnormal):• White cell count returning to normal• Platelet count returning to normal• Creatine Phosphokinase returning to normal• Plasma Sodium returning to normal• C Reactive Protein returning to normal
Radiological Findings:• Improving Chest X-ray changes
SARS is less infective than Influenza.
Each year more than 35000 people die in the United States alone from
influenza and 114000 need to be admitted in hospitals.
SARS is less infective than Influenza.SARS is less infective than Influenza.
Each year more than Each year more than 3500035000 people die people die in the United States alone from in the United States alone from
influenza and influenza and 114000114000 need to be need to be admitted in hospitals.admitted in hospitals.

Preventionv Infection control precautions should be continued for SARS patients for 10 days after respiratory symptoms and fever are gone.
v During this 10 days period all members of household with SARS patients should carefully follow recommendations for hand hygiene.
v Each patient with SARS should cover his/her mouth and nose with a tissue before sneezing or coughing.
Preventionv Infection control precautions should be continued for SARS patients for 10 days after respiratory symptoms and fever are gone.
v During this 10 days period all members of household with SARS patients should carefully follow recommendations for hand hygiene.
v Each patient with SARS should cover his/her mouth and nose with a tissue before sneezing or coughing.

Prevention (continue)
vDisposable gloves should be considered for any contact with body fluids from a SARS patient.
v SARS patients should avoid sharing eating utensils, towels and bedding with other members of the household.
v Common household cleaners are sufficient for disinfection.
v Other members of household need not restrict their outside activities unless they develop symptoms of SARS, such as a fever or respiratory illness.
Prevention (continue)
vDisposable gloves should be considered for any contact with body fluids from a SARS patient.
v SARS patients should avoid sharing eating utensils, towels and bedding with other members of the household.
v Common household cleaners are sufficient for disinfection.
v Other members of household need not restrict their outside activities unless they develop symptoms of SARS, such as a fever or respiratory illness.

Clinicians evaluating suspected cases should use standard precautions
together with airborne and contact precautions.
Clinicians evaluating suspected cases should use standard precautions
together with airborne and contact precautions.

Precautions To Take When Visiting ICUsPrecautions To Take When Visiting ICUsPrecautions To Take When Visiting ICUsn Leave all personal belongings, not relevant to the visit,
in the office.n Take a N95 or FFP-1grade mask from the office.n Before entering the unit, put on the mask as per
instructions, and check for leakage.n After entering the unit, ask for a pair of surgical gloves
before handling equipment.n Do not place belongings, tools etc on the floor or on
exposed surfaces. Request a paper towel from the staff to spread on the surface.
n If you need to bring equipment/parts back to the office, have them sterilized according to hospital procedure by a member of the ICU staff.
nn Leave all personal belongings, not relevant to the visit, Leave all personal belongings, not relevant to the visit, in the office.in the office.
nn Take a N95 or FFPTake a N95 or FFP--1grade mask from the office.1grade mask from the office.nn Before entering the unit, put on the mask as per Before entering the unit, put on the mask as per
instructions, and check for leakage.instructions, and check for leakage.nn After entering the unit, ask for a pair of surgical gloves After entering the unit, ask for a pair of surgical gloves
before handling equipment.before handling equipment.nn Do not place belongings, tools etc on the floor or on Do not place belongings, tools etc on the floor or on
exposed surfaces. Request a paper towel from the staff exposed surfaces. Request a paper towel from the staff to spread on the surface.to spread on the surface.
nn If you need to bring equipment/parts back to the office, If you need to bring equipment/parts back to the office, have them sterilized according to hospital procedure by have them sterilized according to hospital procedure by a member of the ICU staff.a member of the ICU staff.

When Leaving The ICU…When Leaving The ICUWhen Leaving The ICU……n After exiting the unit, remove the
mask first and discard it, then remove the gloves.
nWash hands thoroughly with chlorhexidine scrub solution.
n Do not re-use a mask.n Do not touch a used mask without
wearing gloves.
nn After exiting the unit, remove the After exiting the unit, remove the mask first and discard it, then mask first and discard it, then remove the gloves.remove the gloves.
nn Wash hands thoroughly with Wash hands thoroughly with chlorhexidinechlorhexidine scrub solution.scrub solution.
nn Do not reDo not re--use a mask.use a mask.nn Do not touch a used mask without Do not touch a used mask without
wearing gloves.wearing gloves.

Prevention of Respiratory Tract Infection – DON’Ts
Prevention of Respiratory Tract Prevention of Respiratory Tract Infection Infection –– DONDON’’TsTs
1. Cough or sneeze into your hands2. Share food, cups, straws, cigarettes, hand
towels3. Chew Pens, pencils, etc.4. Put your chopsticks, forks, spoons into
communal dishes5. Visit friends if you or they have flu-like
symptoms
1.1. Cough or sneeze into your handsCough or sneeze into your hands2.2. Share food, cups, straws, cigarettes, hand Share food, cups, straws, cigarettes, hand
towelstowels3.3. Chew Pens, pencils, etc.Chew Pens, pencils, etc.4.4. Put your chopsticks, forks, spoons into Put your chopsticks, forks, spoons into
communal dishescommunal dishes5.5. Visit friends if you or they have fluVisit friends if you or they have flu--like like
symptomssymptoms
Who is at the most risk of the contracting SARS ?
Primarily those people who have had direct close contact with an infected
person.
WhoWho is at the most risk of the is at the most risk of the contracting SARS ?contracting SARS ?
Primarily those people who have had direct close contact with an infected
person.
Travel restrictions
At this time it is advised to postpone non-essential travel to
affected areas (China, Hong Kong, Vietnam, Singapore and Canada).
Travel restrictionsTravel restrictions
At this time it is advised to postpone non-essential travel to
affected areas (China, Hong Kong, Vietnam, Singapore and Canada).

Until 12 April 2003 a cumulative total of 2960 SARScases and 119 deaths have been reported from 21 countries of all
5 continents.
Until 12 April 2003 a cumulative total of 2960 SARScases and 119 deaths have been reported from 21 countries of all
5 continents.

How about our country?How about our country?How about our country?



















