Session 47 PD, Accelerated Underwriting and … 47 PD, Accelerated Underwriting and Simplified Issue...
46
Session 47 PD, Accelerated Underwriting and Simplified Issue/New Underwriting Moderator: Richard J. Tucker, FSA, MAAA Presenters: Gregory A. Brandner, FSA, MAAA Michael David Hoyer, FSA, MAAA Mark Andrew Sayre, ASA, CERA, MAAA
Transcript of Session 47 PD, Accelerated Underwriting and … 47 PD, Accelerated Underwriting and Simplified Issue...

Session 47 PD, Accelerated Underwriting and Simplified Issue/New Underwriting
Moderator:
Richard J. Tucker, FSA, MAAA
Presenters: Gregory A. Brandner, FSA, MAAA Michael David Hoyer, FSA, MAAA
Mark Andrew Sayre, ASA, CERA, MAAA

Accelerated Underwriting - Where we started- Where we are today- Where we’re going
Society of Actuaries Life & Annuity Symposium - May, 2016
Gregory Brandner, FSA, MAAAAssistant Vice President & Actuary
A Few Broad Observations
The market is evolving, and the pace of change is accelerating
We continue to move closer to fully underwritten mortality (progress, not perfection)
Use of BIG DATA may be a game-changer
2
How do we measure progress?
Customer experience (UW requirements, processing time, premium rates, . . .)
Target market
Issue Ages
Face Amounts
Preferred Classes
Automation
Products
Mortality
3
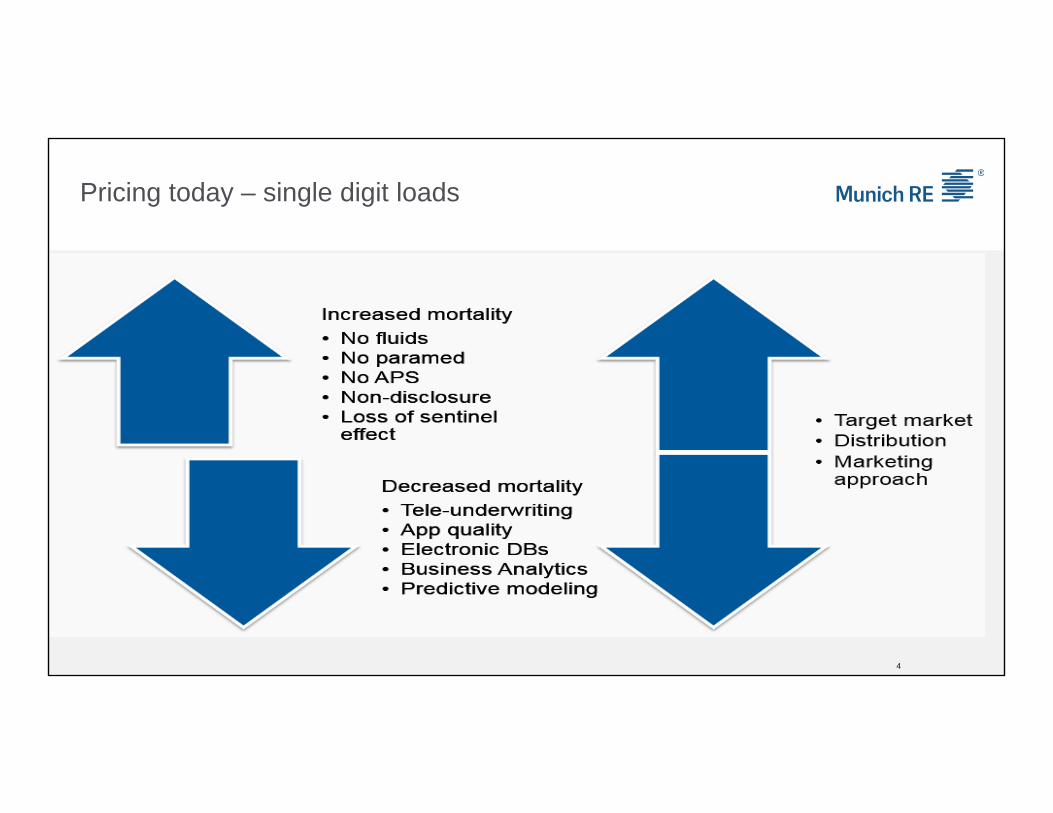
Pricing today – single digit loads
4

Current Medical Underwriting
5
Distribution by risk class
Super Preferred 30.0%Preferred 40.0%Standard 20.0%
Substandard 7.0%Decline 3.0%Overall 100.0%
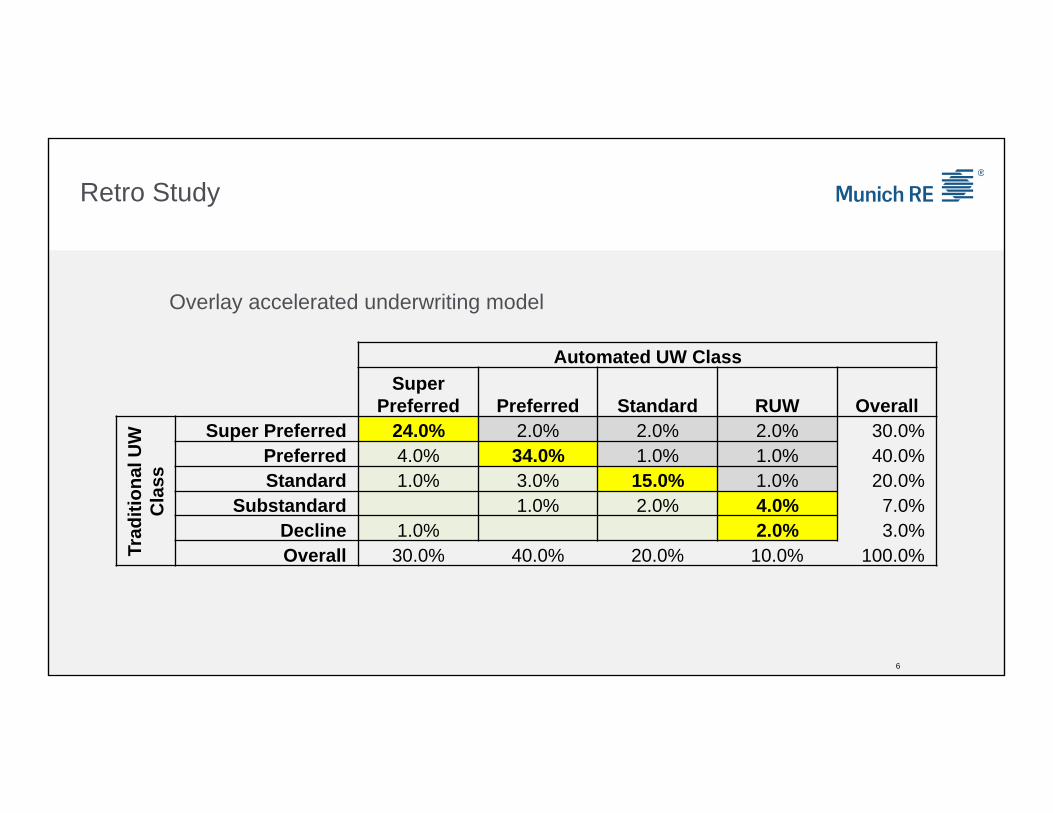
Retro Study
6
Overlay accelerated underwriting model
Automated UW ClassSuper
Preferred Preferred Standard RUW Overall
Trad
ition
al U
W
Cla
ss
Super Preferred 24.0% 2.0% 2.0% 2.0% 30.0%Preferred 4.0% 34.0% 1.0% 1.0% 40.0%Standard 1.0% 3.0% 15.0% 1.0% 20.0%
Substandard 1.0% 2.0% 4.0% 7.0%Decline 1.0% 2.0% 3.0%Overall 30.0% 40.0% 20.0% 10.0% 100.0%

Retro Study
7
Normalized to exclude “defectors”
Automated UW ClassSuper
Preferred Preferred Standard RUW Overall
Trad
ition
al U
W
Cla
ss
Super Preferred 26.4% 26.4%Preferred 4.4% 37.4% 41.8%Standard 1.1% 3.3% 16.5% 20.9%
Substandard 1.1% 2.2% 4.4% 7.7%Decline 1.1% 2.2% 3.3%Overall 33.0% 41.8% 18.7% 6.6% 100.0%

Retro Study
8
Relative Mortality
Automated UW ClassSuper
Preferred Preferred Standard RUW Overall
Trad
ition
al U
W
Cla
ss
Super Preferred 100.0% 80.0%Preferred 115.0% 100.0% 92.0%Standard 150.0% 130.4% 100.0% 120.0%
Substandard 218.8% 190.2% 145.8% 100.0% 175.0%Decline 1000.0% 100.0% 800.0%Overall 133.7% 104.8% 105.4% 100.0% 114.1%
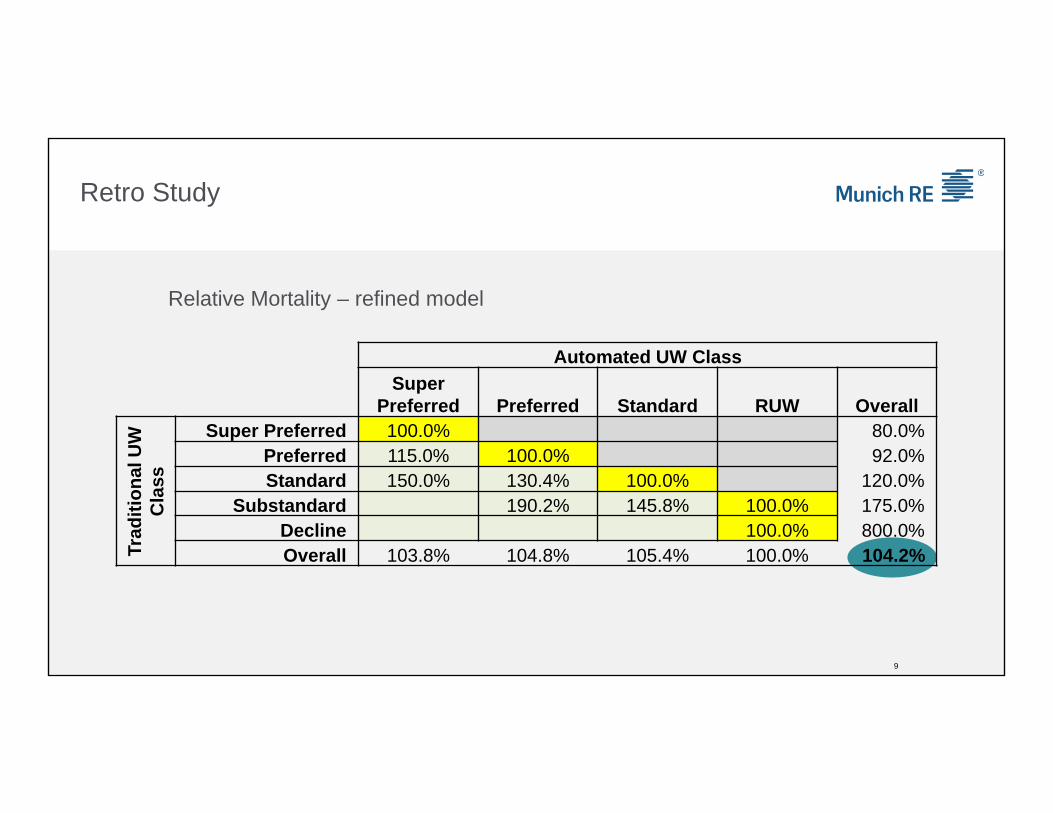
Automated UW ClassSuper
Preferred Preferred Standard RUW Overall
Trad
ition
al U
W
Cla
ss
Super Preferred 100.0% 80.0%Preferred 115.0% 100.0% 92.0%Standard 150.0% 130.4% 100.0% 120.0%
Substandard 190.2% 145.8% 100.0% 175.0%Decline 100.0% 800.0%Overall 103.8% 104.8% 105.4% 100.0% 104.2%
Retro Study
9
Relative Mortality – refined model

Self-reporting Full disclosure
Height and weight
Cryptic smokers
Avocations
Family history
Medical history
10
“Survey Shows Many Americans Fine with Lying to the IRS, or Their Insurer”
One-in-five people surveyed said it is acceptable to lie about the number of miles driven each year to receive lower auto insurance rates
16 percent of Americans believe it’s acceptable to lie about smoking marijuana to receive lower life insurance rates
Eleven percent of respondents say it is acceptable to lie about tobacco smoking habits to receive lower life insurance rates
P.S. 24 percent of people are OK with withholding information about extra income from the IRS
11
February 2016 survey conducted by NerdWallet

Smoking Prevalence - Nondisclosure
2013 study published in the Journal of Insurance Medicine:19.3% of life insurance applicants who tested positive for cotinine self-reported as non-tobacco users
Impact on Mortality (example)
Fully Underwritten program: 80% non-tobacco; 20% tobacco
Accelerated Underwriting program:
• 1 out of 5 tobacco users does not disclose their tobacco use
• 84% “non-tobacco”; 16% tobacco
• Assume tobacco mortality is 200% of non-tobacco
“Non-Tobacco” mortality will increase by 4.8% due to nondisclosure
12
And… questions everywhere
What’s the value of labs? What’s the impact of Rx, MVR, and MIB? Is there value in a tele-interview? How do I blend requirements to achieve pricing metrics and the desired customer experience? What’s the protective value of a new data source?
I’m being approached by a startup telling me that shoe size and choice of footwear predicts mortality. How do I assess?
Can I use it this new data source in making an underwriting decision?
How far can I go in using data in my target marketing?
How do I quantify the impact of a predictive model? Will Electronic Health Records solve all my problems?
13

The future of accelerated underwriting:A few thoughts, observations, and predictions
Easy to hypothesize on how it should be done; not nearly so easy to do
New data sources will help
• Wearable devices
• The Internet of Things
• Electronic Health Records
Predictive modeling
Effective use of Business Analytics is essential
Some distribution channels work better than others
Be prepared to make adjustments – you won’t get it right the first time
14

The future of accelerated underwriting:A few thoughts, observations, and predictions
Predictions:
As an industry we will get to fully underwritten pricing using accelerated underwriting
If we don’t figure it out, somebody else will
(i.e. watch out for Google and Amazon)
15

Thank you for your attention

1
Proprietary and Confidential.
Prescription for Success in Accelerated Underwriting
SOA Life & Annuity Symposium Session 47May 17, 2016
Mike Hoyer, FSA, MAAA
2
Proprietary and Confidential.
Agenda
How does Rx work
Mortality implications
Rx rules engines and predictive models
Assessing protective value
3
Proprietary and Confidential.
The future of underwriting
Increasing:• Electronic requirements (Rx, MIB, Medical, Credit …)
• Decision engines driven by data
• Predictive Models
Decreasing:• APS, Labs
• Cycle times
• Costs
Better Customer Experience
4
Proprietary and Confidential.
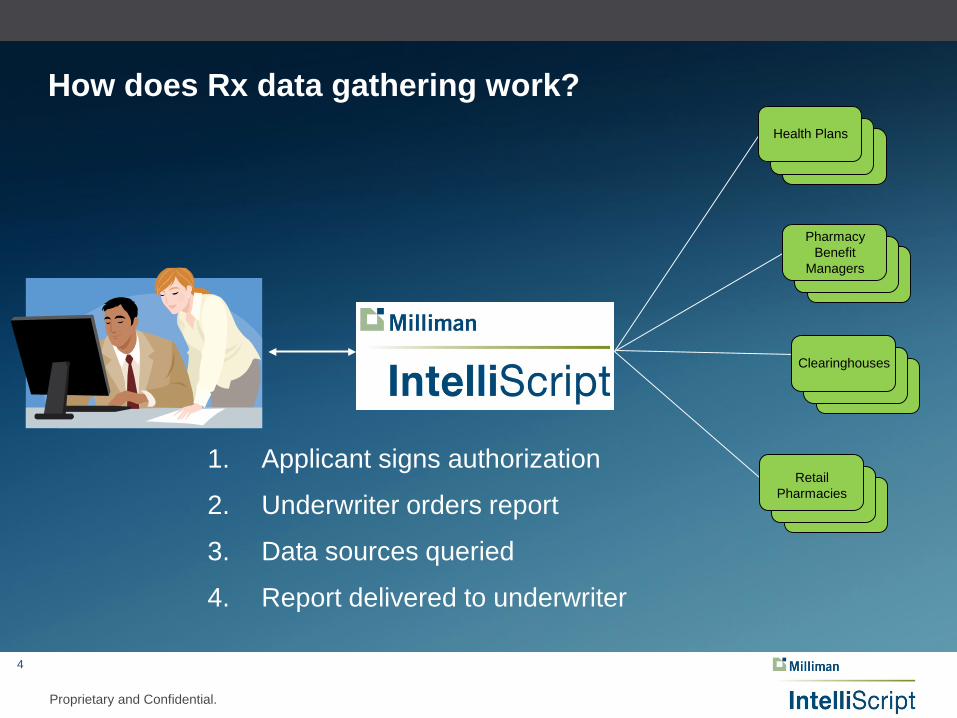
How does Rx data gathering work?
Pharmacy Benefit
Managers
Clearinghouses
Retail Pharmacies
Health Plans
1. Applicant signs authorization
2. Underwriter orders report
3. Data sources queried
4. Report delivered to underwriter

5
Proprietary and Confidential.
Rx history query information Prescription
• Brand and generic name• Dosage and quantity• Date of fill
Physician• Specialty• Contact information
Pharmacy• Contact information
Dates of eligibility
With or without prescriptions
Underwriting significance indicator (risk score)
6
Proprietary and Confidential.
Mortality studies
RGA study (using Milliman data) - 2009
• 1M exposure years
• 2,500 deaths
Milliman study – 2012
• 21M exposure years
• 45,000 deaths
Milliman study – 2015
• 53M exposure years
• 231,000 deaths
• Created Milliman risk score
7
Proprietary and Confidential.
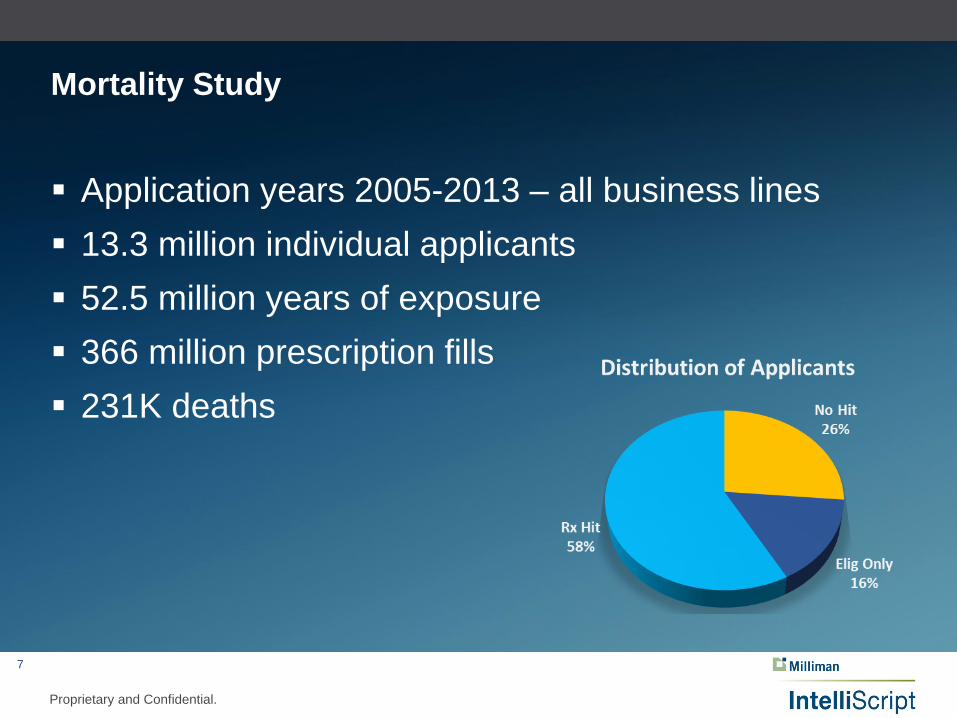
Mortality Study
Application years 2005-2013 – all business lines 13.3 million individual applicants 52.5 million years of exposure 366 million prescription fills 231K deaths

8
Proprietary and Confidential.
Relative mortality - hit status

9
Proprietary and Confidential.
Relative mortality – hit status by age

10
Proprietary and Confidential.
Relative mortality by red fill count
11
Proprietary and Confidential.
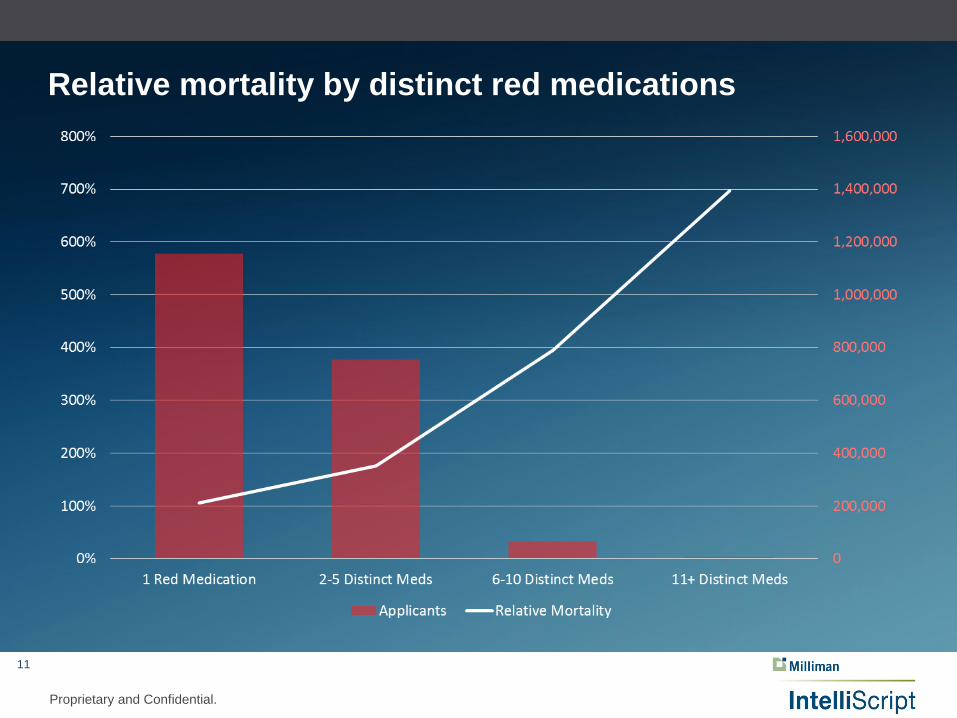
Relative mortality by distinct red medications
12
Proprietary and Confidential.
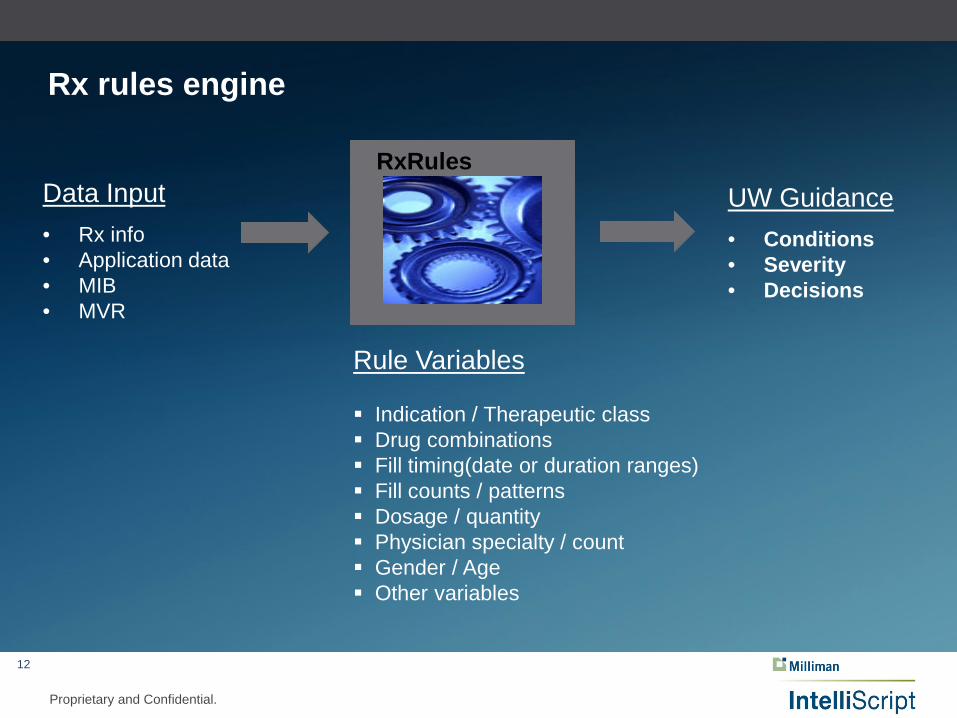
Rx rules engine
UW Guidance• Conditions• Severity• Decisions
Data Input• Rx info• Application data• MIB • MVR
RxRules
Rule Variables
Indication / Therapeutic class Drug combinations Fill timing(date or duration ranges) Fill counts / patterns Dosage / quantity Physician specialty / count Gender / Age Other variables

13
Proprietary and Confidential.
Benefits of Rx rules engine
Consistency
Efficiency
Decisions
Evidence

14
Proprietary and Confidential.
RxRules – timing and duration matters.
Corticosteroids105% relative mortality
Low frequency/duration99%
High frequency/duration201%
Corticosteroids are very common among insurance applicants
15
Proprietary and Confidential.
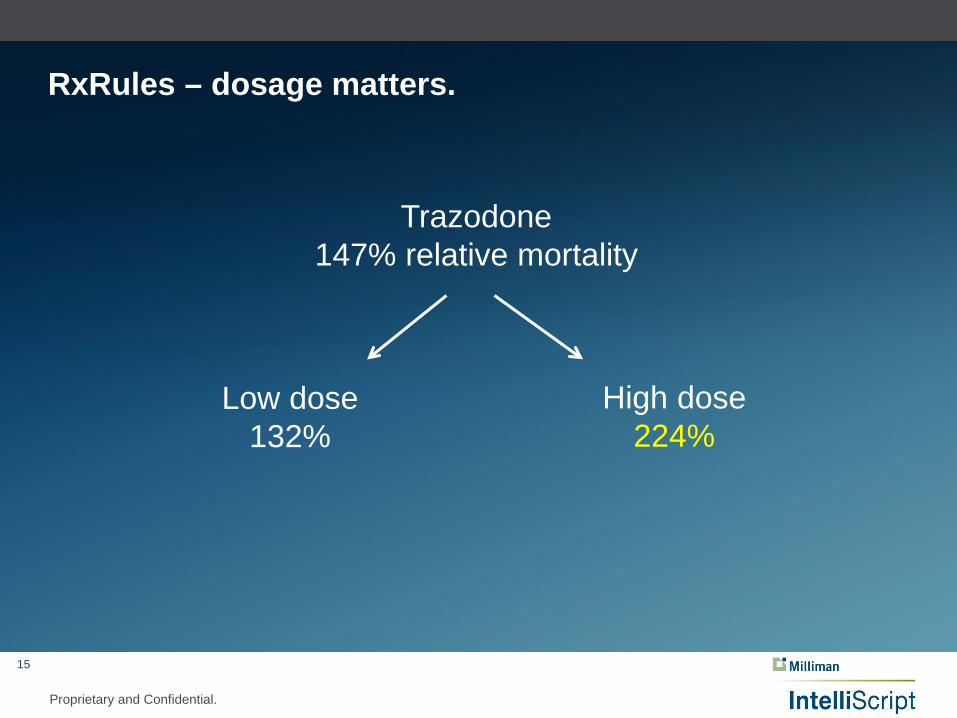
RxRules – dosage matters.
Trazodone147% relative mortality
Low dose132%
High dose224%

16
Proprietary and Confidential.
RxRules – drug combinations matter.
Spironolactone 209% relative mortality
With 2 out of 3 of:
Thiazide Diuretics (102%)Ace / Angio II (ARBS) (116%)Beta Blocker (122%)
328%
Without 2 out of 3 of:
Thiazide Diuretics (102%)Ace / Angio II (ARBS) (116%)Beta Blocker (122%)
166%
17
Proprietary and Confidential.
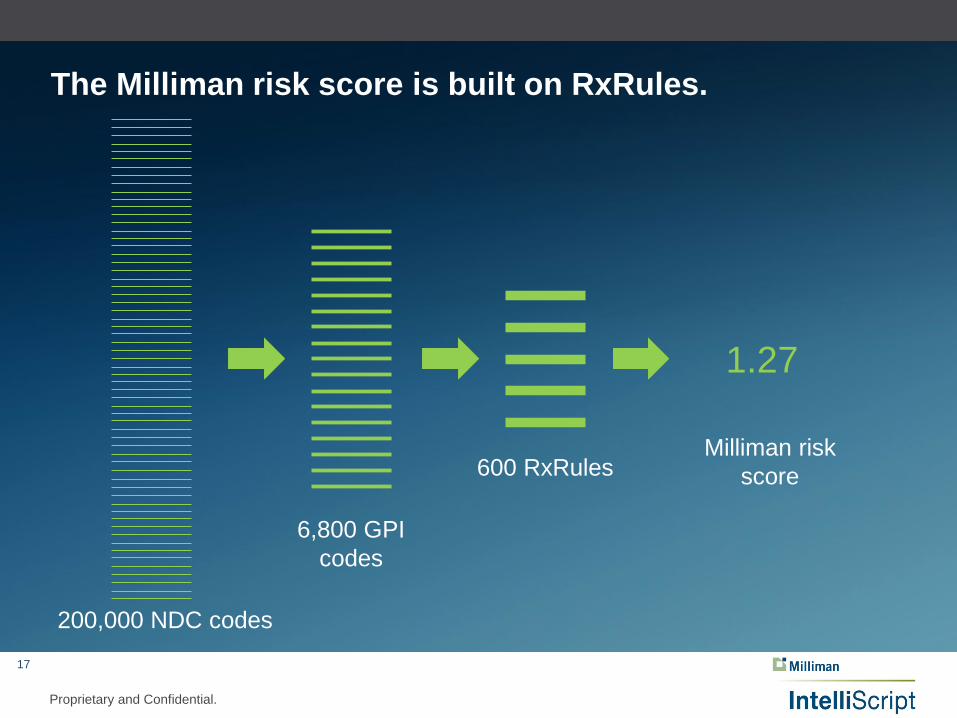
The Milliman risk score is built on RxRules.
Milliman risk score
200,000 NDC codes
6,800 GPI codes
600 RxRules
1.27

18
Proprietary and Confidential.
Milliman’s risk score predicts mortality.
19
Proprietary and Confidential.
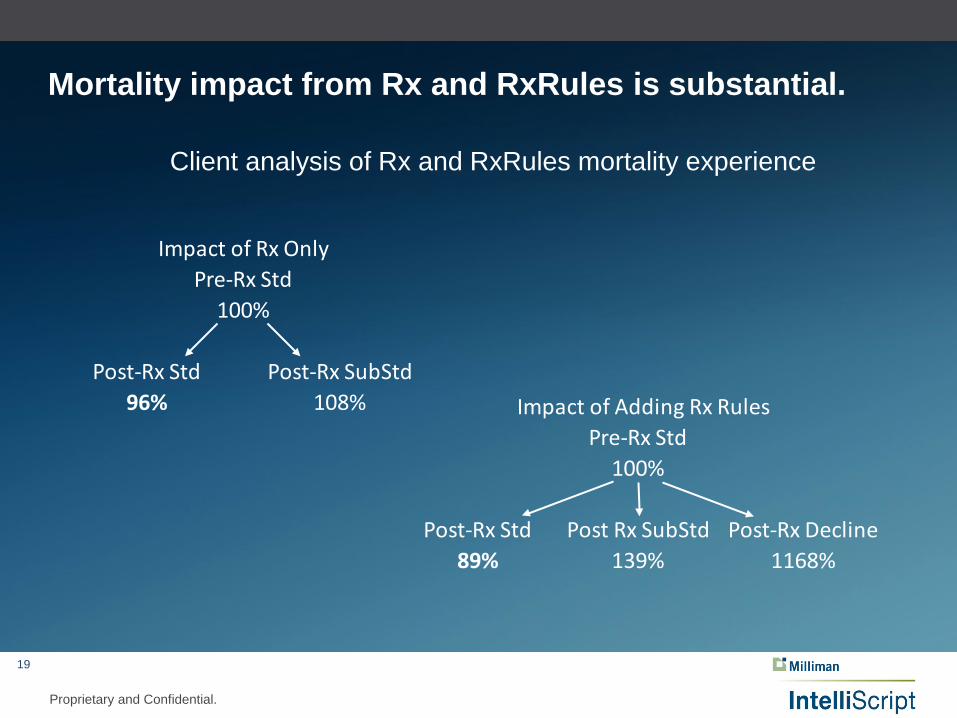
Mortality impact from Rx and RxRules is substantial.
Client analysis of Rx and RxRules mortality experience
Pre-Rx Std100%
Post-Rx Std Post-Rx SubStd96% 108%
Impact of Rx Only
Pre-Rx Std100%
Post-Rx Std Post Rx SubStd Post-Rx Decline89% 139% 1168%
Impact of Adding Rx Rules
20
Proprietary and Confidential.
The future of underwriting
Increasing:• Electronic requirements (Rx, MIB, Medical, Credit …)
• Decision engines driven by data
• Predictive Models
Decreasing:• APS, Labs
• Cycle times
• Costs
Better Customer Experience

21
Proprietary and Confidential.
Contact Info
Mike Hoyer, FSA, MAAA Life [email protected] (262) 923-3636

PROPRIETARY & CONFIDENTIAL
Accelerated Underwriting
SOA Life & Annuity Symposium - May 17, 2016Nashville, TNMark A. Sayre, FSA, CERA, MAAA
❏ A Digital, Customer-Centric Process■ 43 States as of January 2016■ Ages 18-45■ Fully Digital End-to-End Experience, Direct-to-Consumer
❏ Simple Product■ Fully-Underwritten Level Term (3 Non-Tob classes, 2 Tob classes)■ 10, 15, 20 and 30-year versions■ 4-month Temporary Coverage■ No conversions and no commissions■ ACH only, monthly
❏ An Algorithmic Foundation■ Real-time Underwriting inputs■ Evolving modeling expertise■ Immediate Feedback (and temporary coverage)
❏ ....But Sales are Below Plan
Background
PROPRIETARY & CONFIDENTIAL
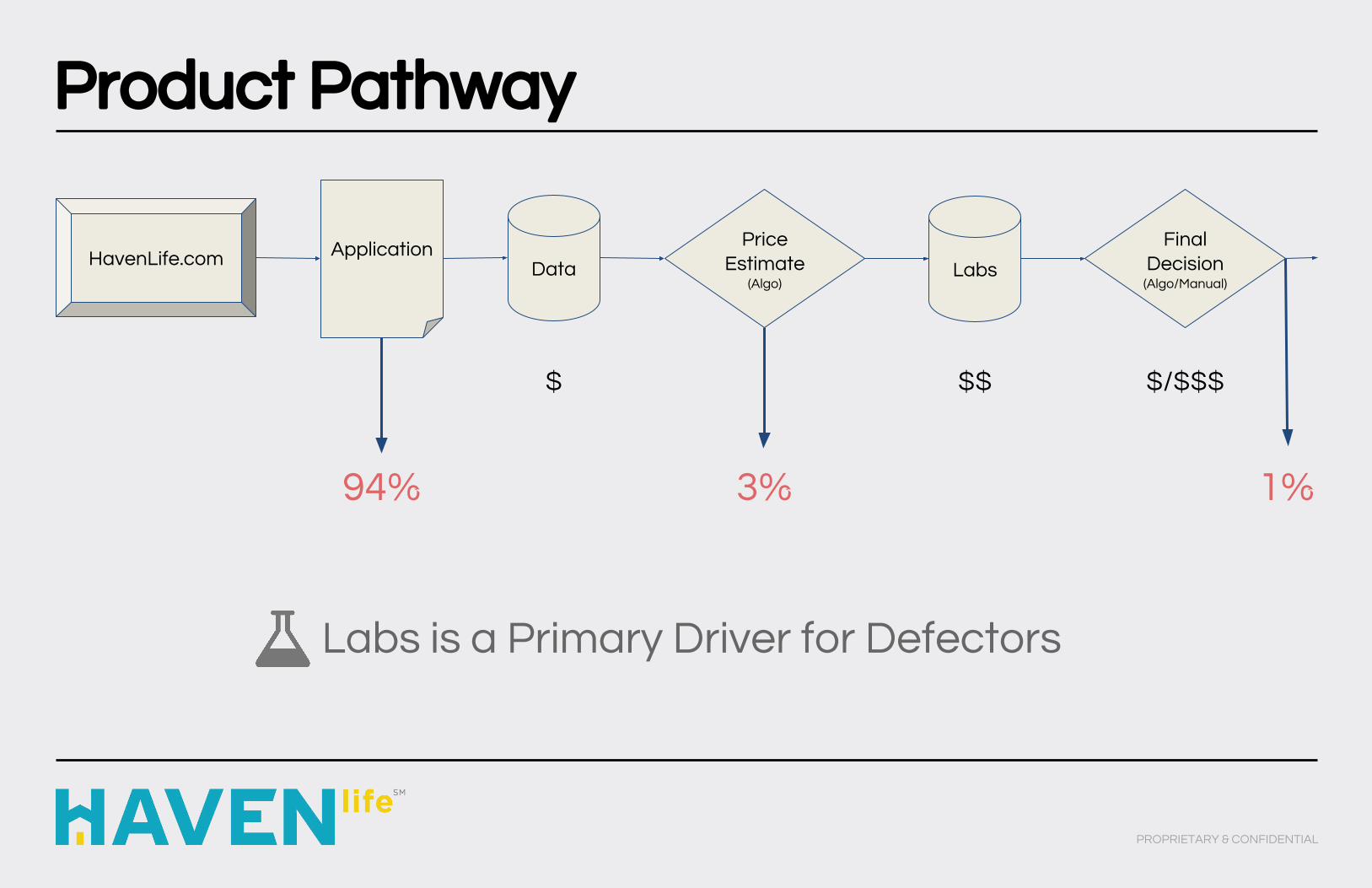
Product Pathway
PROPRIETARY & CONFIDENTIAL
HavenLife.com Application Price Estimate
(Algo)LabsData
Final Decision
(Algo/Manual)
$ $$ $/$$$
94% 3% 1%
Labs is a Primary Driver for Defectors
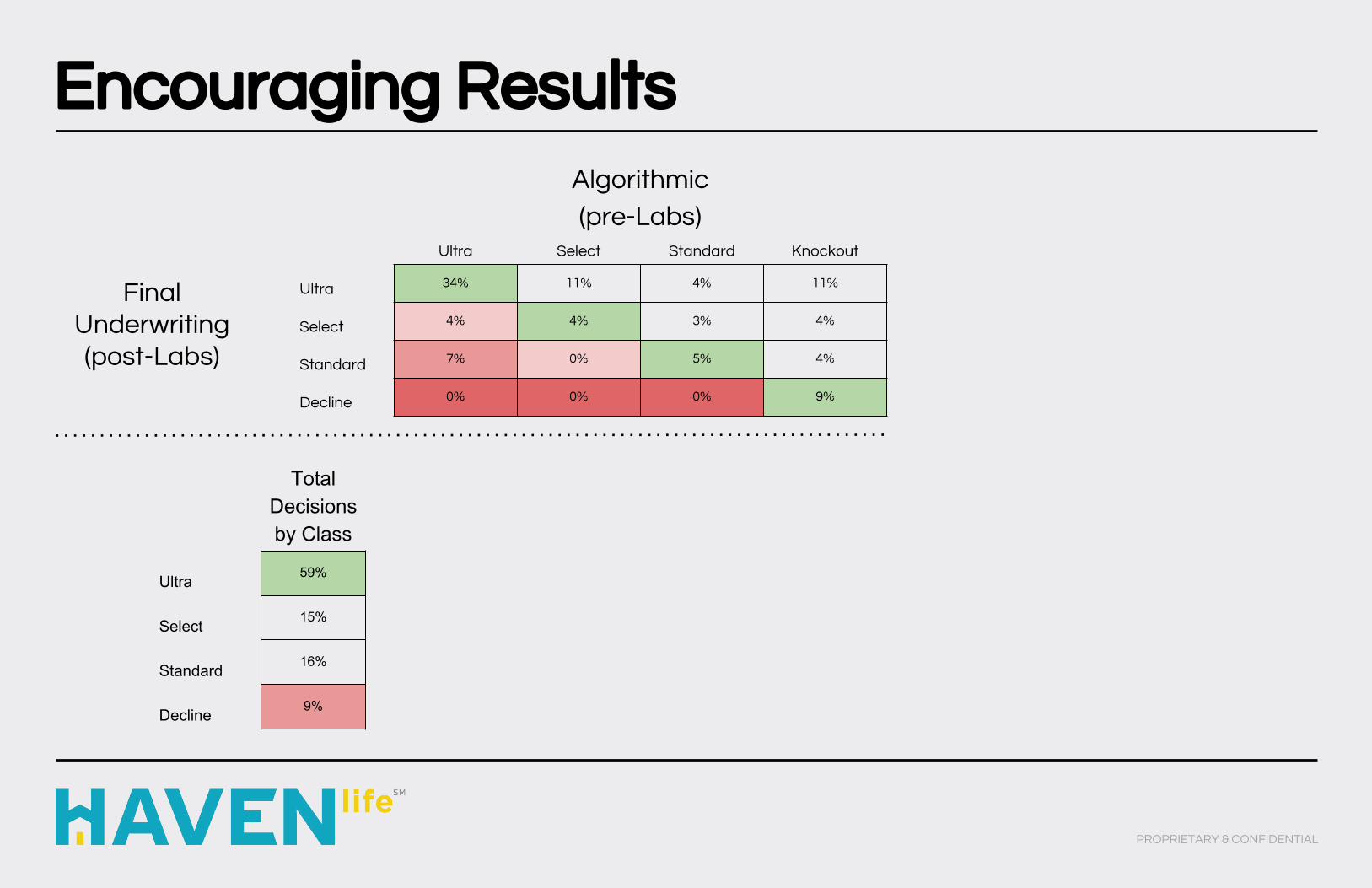
Encouraging Results
PROPRIETARY & CONFIDENTIAL
Algorithmic
(pre-Labs)Ultra Select Standard Knockout
Ultra 34% 11% 4% 11%
Select 4% 4% 3% 4%
Standard 7% 0% 5% 4%
Decline 0% 0% 0% 9%
Final Underwriting (post-Labs)
Total Decisions by Class
Ultra 59%
Select 15%
Standard 16%
Decline 9%
Gaining and Losing
PROPRIETARY & CONFIDENTIAL
❏ Labs Provide Significant Value■ Diabetes, HIV, Kidney Disease,
Drug/Alcohol Abuse
❏ Rx Closes Gaps - Not All■ Undisclosed, Undiagnosed, Untreated
❏ New Data Sources Help■ Ideally uncorrelated (Credit, Social) -
Diversification is Key■ Focus on Frequency, Value and Cost
Process Multiplier = ( Protective Value * Frequency ) / Cost

A New Approach
PROPRIETARY & CONFIDENTIAL
Algorithmic Underwriting
❏ Reflexive Application❏ Identity Verification❏ Driving History❏ Prescription History❏ Rx Interpretation
Accelerated Underwriting
❏ Reflexive Application❏ Identity Verification❏ Driving History❏ Prescription History❏ Rx Interpretation✓ Credit Data✓ Inspection Reports✓ Credit/MVR Scoring

What Comes Next
PROPRIETARY & CONFIDENTIAL
❏ Lifestyle Risk ■ Foreign Travel■ Avocation (Skydiving, Scuba Diving)■ Thrill-Seeking■ Binge-Drinking / Party Drugs
❏ Real-Time Medical Information■ Historical Labs■ Diagnoses and Treatments■ Clarity and Context for Rx
❏ Advanced Algorithms■ Dimensionality Reduction■ Clustering■ Complex Rules

Thank You!
PROPRIETARY & CONFIDENTIAL