SERVICE SPECIFICATION Service Commissioner … Us/Tenders... · • Protocol, standardised...
18
1 SERVICE SPECIFICATION Service Long Term Conditions Contract Commissioner Lead Charlotte Painter Provider City and Hackney GP Confederation Provider Lead Laura Sharpe Period 01.04.2018 – 31.03.2019 Date of Review 1 Population Needs Core Long Term Conditions Contract There are approximately 80,000 people in City and Hackney with a long term condition. This service offers these patients enhanced primary care via additional reviews, extended appointments, care-planning and treatment targets. The Long Term Conditions (LTCs) Contract rewards City and Hackney GP practices for delivering higher quality care over and above what is in their core GP contracts, which are held with NHS England. The City and Hackney Clinical Commissioning Group (CCG) must improve the quality of care for its patients with LTCs if it is to see any reduction in its high premature mortality rates from cardiovascular disease (CVD) and respiratory disease, and any increase in the proportion of its patients who have an LTC feeling supported to manage their own condition, all of which are key CCG strategic aims, and all of which feature in the CCG Outcome Indicator set. The aim of the contract is to increase standards and reduce variability in access to high quality care between GP practices. The contract is being delivered to an incredibly high standard, the evidence for which comes from the contract’s performance dashboard, which charts at a GP practice level achievement against all of the prevalence targets, clinical process targets and intermediate clinical outcomes targets that are part of the contract (intermediate clinical outcomes are measures of therapeutic effect that are considered reasonably likely to predict changes to morbidity and mortality – for example blood pressure control is an intermediate clinical outcome, the end point clinical outcome being the rate of heart attacks and strokes over time). The added value of the contract regarding existing services can be quantified in terms of performance in the Quality and Outcomes Framework for England and Wales (QOF). The contract has succeeded in moving the CCG into the upper quintile of QOF for many of its indictors and into the best performing CCG for several indicators. This contract will assist in both maintaining and further improving on these gains. Time to talk Patients with LTCs have reported that they would like more time to discuss concerns with their GP. The aim is to give patients the opportunity to discuss worries, depression, lifestyle, family issues, difficulties managing their illnesses, etc. Cancer Improving our cancer care for our patients in City and Hackney is a priority for the CCG. Every hour, three more Londoners are diagnosed with cancer. On average, one of them will die within 12 months, one will live with their cancer for the rest of their life, and only one will beat it. Despite all the advances in successfully treating the disease, Londoners still have a poorer chance of beating their cancer than elsewhere in the country and we need to close that gap. Tackling the reasons behind late diagnosis of cancer is key to making improvement, as well as addressing the unacceptable variations across in screening rates and access to treatment. Children A CCG priority is the focus on Early Years, identifying needs as early as possible, and providing integrated support to meet these needs and reduce further risks. To give each child the “Best Start in Life”, we want to facilitate joint
Transcript of SERVICE SPECIFICATION Service Commissioner … Us/Tenders... · • Protocol, standardised...
1
SERVICE SPECIFICATION
Service Long Term Conditions Contract
Commissioner Lead Charlotte Painter
Provider City and Hackney GP Confederation
Provider Lead Laura Sharpe
Period 01.04.2018 – 31.03.2019
Date of Review
1 Population Needs
Core Long Term Conditions Contract There are approximately 80,000 people in City and Hackney with a long term condition. This service offers these patients enhanced primary care via additional reviews, extended appointments, care-planning and treatment targets.
The Long Term Conditions (LTCs) Contract rewards City and Hackney GP practices for delivering higher quality care over and above what is in their core GP contracts, which are held with NHS England. The City and Hackney Clinical Commissioning Group (CCG) must improve the quality of care for its patients with LTCs if it is to see any reduction in its high premature mortality rates from cardiovascular disease (CVD) and respiratory disease, and any increase in the proportion of its patients who have an LTC feeling supported to manage their own condition, all of which are key CCG strategic aims, and all of which feature in the CCG Outcome Indicator set.
The aim of the contract is to increase standards and reduce variability in access to high quality care between GP practices. The contract is being delivered to an incredibly high standard, the evidence for which comes from the contract’s performance dashboard, which charts at a GP practice level achievement against all of the prevalence targets, clinical process targets and intermediate clinical outcomes targets that are part of the contract (intermediate clinical outcomes are measures of therapeutic effect that are considered reasonably likely to predict changes to morbidity and mortality – for example blood pressure control is an intermediate clinical outcome, the end point clinical outcome being the rate of heart attacks and strokes over time). The added value of the contract regarding existing services can be quantified in terms of performance in the Quality and Outcomes Framework for England and Wales (QOF). The contract has succeeded in moving the CCG into the upper quintile of QOF for many of its indictors and into the best performing CCG for several indicators. This contract will assist in both maintaining and further improving on these gains. Time to talk Patients with LTCs have reported that they would like more time to discuss concerns with their GP. The aim is to give patients the opportunity to discuss worries, depression, lifestyle, family issues, difficulties managing their illnesses, etc. Cancer Improving our cancer care for our patients in City and Hackney is a priority for the CCG. Every hour, three more Londoners are diagnosed with cancer. On average, one of them will die within 12 months, one will live with their cancer for the rest of their life, and only one will beat it. Despite all the advances in successfully treating the disease, Londoners still have a poorer chance of beating their cancer than elsewhere in the country and we need to close that gap. Tackling the reasons behind late diagnosis of cancer is key to making improvement, as well as addressing the unacceptable variations across in screening rates and access to treatment. Children A CCG priority is the focus on Early Years, identifying needs as early as possible, and providing integrated support to meet these needs and reduce further risks. To give each child the “Best Start in Life”, we want to facilitate joint
2
working between the many professionals involved with children with LTCs, to ensure that no child slips through the gaps, and that, through primary care, there is oversight of children and their families’ needs and experience of care.
2 Outcomes
1 Preventing people from dying prematurely
2 Enhancing quality of life for people with Long term conditions
3 Helping people recover from episodes of ill health or following injury -
4 Ensuring people have a positive experience of care
5 Treating and caring for people in safe environment and protecting them from avoidable harm
-
Core LTC contract
A detailed list of outcomes and indicators is appended at the end of the specification.
The service will contribute towards the CCG outcomes of reducing premature mortality and helping people with long term conditions feel supported to manage their condition.
Time to Talk
The aim is to give patients the opportunity to discuss worries, depression, lifestyle, family issues, etc. Research shows that the use of a patient “prompt” sheet acts as an aide-memoire; provides a focus for the consultation; gives patients “permission” to discuss certain things and helps provide greater tailoring for the patient.
Cancer
The Planned Care Workstream wishes to drive more quality improvements in patient care and experience. Formal commissioning of primary care to support the CRUK programme is in line with the national agenda and additional time to support a diagnosis of cancer seeks to provide extra capacity in primary care for GPs to have the opportunity to support their patients in a more meaningful way.
Children This contract facilitates personalised, structured management of LTCs for children, embedding the established approach to managing adults’ LTCs. Children under the care of out of borough Trusts have local support and information to support their access to local services, and children and their families are supported to manage their long term conditions. It is intended that unnecessary hospital attendances are reduced through improved local oversight and management of children, there is integrated transition support for children as they move to adults’ services, and GPs contribute to joint planning for young people with special educational needs and disabilities.
3 Scope of Service
3.1 Service model
3
LTC core contract
This service is available to all patients registered with a City and Hackney GP and is delivered by local GP practices supported by the GP confederation.
The service includes case-finding; prevalence targets for some conditions; annual reviews; care planning; extended consultations and treatment targets.
The Confederation is required to achieve population coverage; performance to minimum standards at CCG level and practices must meet minimum standards at a practice level.
Time to Talk
Eligible patients: adult patients registered with a C&H GP with 2 or more of the following LTCs: 1. Asthma 2. Atrial fibrillation 3. Chronic kidney disease 4. Chronic obstructive pulmonary disease 5. Coronary heart disease 6. Dementia 7. Diabetes 8. Heart failure 9. Hypertension 10. Learning disabilities 11. Severe mental illness 12. Stroke/transient ischaemic attack 13. Peripheral arterial disease
Other LTCs such as hypothyroidism, epilepsy, rheumatoid arthritis, osteoporosis, multiple sclerosis, MUS, etc., can be included at the discretion of the clinician. Patients on the Proactive care home visiting and proactive care practice-based contracts are excluded. Patients with sickle cell disease are eligible for a Time to talk consultation irrespective of whether they have any other condition.
Cancer
This service will be available to adult patients registered with a City and Hackney GP and who have a diagnosis of cancer or who are eligible for bowel cancer screening.
Children This service supports primary care identification of children with asthma (and at risk of asthma), diabetes, epilepsy and sickle cell disease. Personalised asthma action plans which are consistently used across primary and secondary care, with prompt follow up after unplanned hospital attendances, are intended to support improved management of asthma. Annual care contacts and oversight of secondary /tertiary management of children with diabetes, epilepsy and sickle cell are intended to integrate care locally for children and their families, with personalised support during transition. Young people (18 to 25 years) with special educational needs and disabilities (SEND) will be supported in their education and health care plan (EHCP) process, recognising the gap in lead health professional for this cohort of young people.
3.2 Care Pathways
LTC Core Contract
4
Patients with relevant long term conditions will be offered services under the contract and this will be coded by the GP practice. The service is supported by searches created by CEG and EMIS templates to prompt and record activity.
The service will need to link with:
Clinical Effectiveness Group; peer educators; services referred on to e.g. exercise on referral, National Diabetes Prevention Programme; community specialist nurses; other services commissioned by public health e.g. health checks; smoking cessation.
Time to Talk
Practice will offer an extended consultation with either the practice nurse or GP (this should be the patient’s usual GP where possible)
Practices will proactively identify patients
Practices will give the patient a “prompt” sheet in advance of the extended consultation – the aim of the prompt sheet is to help the patient focus on what they want to raise in the consultation
Patients should be informed that they can bring someone else along (spouse, carer, friend, advocate, etc) The extended consultation can be added onto a CDM annual review
The extended consultation could be written up as a care plan The average length of an extended consultation is expected to be 30 minutes (longer for patients who have
communication problems or whose first language isn’t English)
Coded as offered/declined/done
Cancer
Increase uptake of bowel screening through outreach and endorsement All practices will instigate the systems and participate with the promotion of patient participation in national bowel screening programme. • All practices to receive electronic results of bowel screening via lablinks • Check bowel cancer screening participation opportunistically at consultations with people aged 59 to 75 (pop-
up reminder to be included in EMIS); endorse and support screening uptake • Use CEG search to identify people due for screening invitations (60th birthday pending) or DNA result in last 4
weeks • Practices to write to, telephone and provide standardised GP endorsement and information to:
People aged 60 due to be invited (1,600 p.a.) for bowel screening for the first time People aged 61 – 74 who were invited and failed to participate in bowel screening (11,500 pa)
• Contact to non-returners of the bowel screening kit to offer an explanation and support complete the test • Practices to consider and make additional efforts for patients with difficulties that could include language,
literacy, physical disabilities, learning difficulties or who are profoundly deaf • Protocol, standardised endorsement letters and health promotion script for calling can be provided to
practices by the CCG Cancer Clinical Lead • Engage through PPI groups to support work to develop patient literature and other communication materials
to encourage bowel screening uptake
Work with community groups to discuss ways of increasing uptake in the local population and produce a plan for implementation in 2019/20 for example via community pharmacy cancer champions
Referral “safety-netting” With continued support from the CCG Cancer Lead and the CRUK Primary Care Engagement Facilitator, the GP Confederation will ensure that all practices will: • Have a system to ensure the dispatch of all 2 week wait referrals within 24 hours of the patient consultation; • Have a system to make all diagnostic referrals where cancer is suspected within 24 hours of the patient
consultation; • Ensure that all 2 week wait referrals are routinely coded;
5
• Ensure that the practice has a safety net process for follow-up of all 2 week wait referrals • Practices will be provided with a template for routine recording of this information • Ensure that information on 2 week wait referral pathways, diagnostic testing and local pathways is available
to locums and new registrars
Include patients practices have referred straight for diagnostic tests e.g. test (OGD, CT, MRI) rather than fast track outpatient appointment; use London Cancer safety-netting template.
Time to talk for cancer patients via extended practice consultations. This service will be primarily focused on patients diagnosed with cancer, some of which may need more than one consultation because of more complex existing health conditions which have been further complicated by a diagnosis of cancer. Ten minute consultations already exist within QOF therefore the CCG will commission the GP Confederation to ensure that all patients on the QOF Cancer register are offered an additional 20 minutes consultation time. The extended consultation of up to 30 minutes with the patient’s GP (usual GP where possible) will • Cover issues of multi-morbidity, multiple medications, their interactions and possible side-effects • Discuss the cancer diagnosis in context of existing illness both psychological and physical Consultations will be offered to appropriate patients in any of the following circumstances: Once a City and Hackney registered patient has a confirmed diagnosis of cancer notified by secondary care: • The practice will identify the named GP for the patient who will provide continuity of care to the patient; • The practice will offer the patient an extended consultation to come in to see their GP (usual GP where
possible) on receipt of the diagnosis; Once a City and Hackney registered patient has had one of the following: • A planned inpatient episode (e.g. surgery) for management of cancer; • The first of a planned programme of radiotherapy or chemotherapy; • An unplanned emergency hospital admission; • Completed a course of radiotherapy/chemotherapy; • Been discharged from hospital care (including patients discharged in line with risk stratified pathways – breast
pathway will be the initial patient group) The GP will keep an overview of each patient’s care and referrals and, where clinically appropriate, proactively organise a consultation to review or discuss the care plan. The extended consultations could cover: • Reviewing the patient’s condition, current health status and recent history; • Reviewing the patient’s care plan and ensuring that this reflects their wishes; • Discussing the diagnosis, tests and treatment options that have been suggested including potential side effects
and what the NHS will provide; • Ensuring that the patient and their carers have access to emotional support and other local voluntary sector
support groups, access to patient information and information about local resources; • Reviewing any lifestyle issues as appropriate • Arranging annual immunisations and the relevance of involvement in future screening programme activity
(and where necessary making arrangements for the patient to be excluded); • Undertaking a medication review; • Assessment of the carer and their needs; For patients finishing treatment and moving onto self-management: • Ensuring they have been offered an individualised Health and Wellbeing event by their cancer care provider
as part of the Recovery Package • Ensuring they understand warning signs which necessitate representation to secondary care
Cleaning of registers
6
Practices should undertake a review of cancer registers in year to clean up prevalence data and ensure they are up to date with a view to increasing capacity next year to incorporate people with a past diagnosis of cancer
Prostate Cancer - Primary Care Prostate Follow Up Service for stable prostate cancer patients (stratified follow up)
Aim: To provide enhanced support for men with stable prostate cancer in the community, including annual holistic needs assessment and ongoing PSA monitoring The primary care provider will be required to:
Conduct a quarterly search for patients with prostate cancer (READ code B46 or B834) who are not under secondary care and maintain a register
Offer a 30 minute welcome appointment to all newly transferred patients within four weeks of notification transfer from secondary care under the Time to Talk Cancer scheme above (expected numbers for City and Hackney <100 per annum). N.B. Barts Health will be running a nurse led follow up model which will manage the majority of patients on BH pathway.
Organise PSA testing as per the instructions on the patient's Treatment Summary, review the results and organise follow up testing or re-referral to secondary care as appropriate.
Children
Patients with relevant long term conditions will be offered services under the contract and this will be coded by the GP practice. The service is supported by searches created by CEG and EMIS templates to prompt and record activity.
The service will need to link with the Trusts under whom their children receive their care, where there are clinical concerns.
The GP Confederation (GPC) will liaise with the Commissioner regarding trends in poor communication between Trusts and GPs, to inform commissioning requirements.
The GPC and CCG will continue to review and develop necessary information sharing arrangements, where they are required, to enable integrated delivery of care to relevant children.
3.3 Structural Support
LTC core contract The C&H GP Confederation (GPC) is contracted to ensure that all practices meet all minimum prevalences and standards.
The GP Confederation supports practices to deliver the service and oversees quality and governance (e.g. via audit).
All minimum prevalences and standards apply to all practices.
Where a minimum prevalence or standard has not been met (recorded prevalence measured 31st Mar 2019) the GPC is asked to produce a report, calling on the assistance of CEG if needed, outlining what action has been taken to get the practice to the minimum prevalence or standard. The GPC is asked to provide a report on each missed prevalence or standard to be submitted to the CCG’s LTC Board. Practices will need to be able to show that they have looked at and acted upon the CEG suite of searches. The GPC is asked to monitor exception reporting levels at an individual practice level and to take action where levels are found to be excessive (e.g. higher than similar practices; higher than the national average). The GPC is asked to provide a report on any action taken to be submitted to the CCG’s LTC Board after year end. There is no payment associated with this requirement nor are other payments dependent upon having done this. The CCG will also commission CEG to provide reports on exception reporting use by practice.
7
Children
The C&H GP Confederation (GPC) is contracted to ensure that all practices meet all minimum prevalences and standards.
The GP Confederation supports practices to deliver the service and oversees quality and governance (e.g. via audit).
All minimum prevalences and standards apply to all practices.
Where a minimum prevalence or standard has not been met (recorded prevalence measured 31st Mar 2019) the GPC is asked to produce a report, calling on the assistance of CEG if needed, outlining what action has been taken to get the practice to the minimum prevalence or standard. The GPC is asked to provide a report on each missed prevalence or standard to be submitted to the CCG’s LTC Board. Practices will need to be able to show that they have looked at and acted upon the CEG suit of searches. The GPC is asked to monitor exception reporting levels at an individual practice level and to take action where levels are found to be excessive (e.g. higher than similar practices; higher than the national average). The GPC is asked to provide a report on any action taken to be submitted to the CCG’s LTC Board after year end. There is no payment associated with this requirement nor are other payments dependent upon having done this. The CCG will also commission CEG to provide reports on exception reporting use by practice. Cancer Work with CEG during 2018/19 to develop proxy outcomes demonstrating improved uptake of screening , sourcing
best practice sourcing best practice to increase screening
Link to referral forms and education materials:
https://www.healthylondon.org/our-work/cancer/suspected-cancer-referrals/
5 Key Performance Indicators
Core LTC contract
The full list of outcomes and indicators is appended. Final targets will be agreed in May 2018.
Maintaining performance: GPC level: GPC to meet minimum average prevalence. As a general principle the final targets associated with the minimum prevalence and standards will be set at the lower end of one standard deviation of the 2017/18 results. However, these can be set higher at the discretion of the CCG. GPC to meet minimum average standards
As a general principle the final targets associated with the minimum prevalence and standards will be set at the median of the 2017/18 results. However, these can be set higher at the discretion of the CCG.
Time to talk
Delivery of up to 12,420 extended consultations in-line with the specification.
Cancer
Key performance indicators and outcomes: Bowel screening – quarterly reports • % of men and women contacted around their 60th birthday by telephone and offered health promotion to
encourage uptake of bowel screening
8
• % of men and women in the above group sent endorsement letter by practice if not reached by telephone • % of men and women aged 61 – 70 who have not participated in bowel screening in the last 3 months
contacted by telephone and offered health promotion to encourage uptake of bowel screening • % of men and women in the above group sent endorsement letter by practice if not reached by telephone • Increase in bowel screening uptake across City and Hackney practices 2 week waits – quarterly reports • Numbers made by practice • Numbers of DNAs/delays where the practice took action
Follow up of 62 day wait patients – supporting secondary care if requested
Report patient outcomes on recovery and management of consequences of cancer treatment – measures to be agreed during 2018/19
Report on patient experience
Time to talk – quarterly reports • % of appointments offered by practice • % of appointments taken up by practice • Annual patient experience survey/questionnaire Children
The full list of KPIs is appended. Final targets will be agreed in May 2018.
Maintaining performance: GPC level: GPC to meet minimum average prevalence. As a general principle the final targets associated with the minimum prevalence and standards have been set at the lower end of one standard deviation of the 2016/17 results. However, these can be set higher at the discretion of the CCG. GPC to meet minimum average standards
As a general principle the final targets associated with the minimum prevalence and standards have been set at the median of the 2017/18 results. However, these can be set higher at the discretion of the CCG.
6 Reporting Requirements
Core LTC Contract
Maintaining performance at practice level: GPC to ensure individual practice prevalences are maintained to at least their 2017/18 levels. GPC to ensure individual practice denominators are maintained to at least their 2017/18 levels, having taken account of any changes in practices registers or indicator definitions. Where a prevalence and/or denominator at year end is below its 2017/18 level the GPC is asked to produce a report, calling on the assistance of CEG if needed, outlining what action has been taken and any mitigating factors. The GPC’s performance will be assessed at the end of the year (31st Mar 2019) on the following:
CEG LTC Contract Dashboard GPC end of year report detailing:
a) Minimum prevalences and standards at practice and GPC level b) Exception reporting levels c) Denominator levels
9
The full suite of reports will be considered at the next available prevention workstream (with input from the Children’s workstream and the Planned Care workstream).
The prevention workstream will then make its recommendation to the GP Contracts Committee who will in turn make a recommendation for payment to the CCG Governing Body / Integrated Commissioning Board.
Time to Talk
The GPC is asked to provide a report along the following lines: Equity of access report analysed by all nine protected characteristics, where available, and by number of conditions, across all activity variables (consultation offered, patient choice of GP or nurse where offered, consultation declined, uptake of consultation with nurse, uptake of consultation with GP), and at an individual practice level. The report should include the number of eligible patients identified per practice and uptake per practice.
The GPC will produce a report detailing the patient experience of at least 200 patients who have had an extended consultation.
Cancer
Annual / quarterly report (see finance section).
Children
Maintaining performance at practice level: GPC to ensure individual practice prevalences are maintained to at least their 2016/17 levels. GPC to ensure individual practice denominators are maintained to at least their 2017/18 levels, having taken account of any changes in practices registers or indicator definitions. Where a prevalence and/or denominator at year end is below its 2017/18 level the GPC is asked to produce a report, calling on the assistance of CEG if needed, outlining what action has been taken and any mitigating factors. The GPC’s performance will be assessed at the end of the year (31st Mar 2019) on the following:
CEG LTC Children’s Dashboard
GPC end of year report detailing: d) Minimum prevalences and standards at practice and GPC level e) Exception reporting levels f) Denominator levels
The full suite of reports will be considered at the Children’s workstream meeting, and in coordination with the prevention workstream recommendations will be made to the Transformation Board who in turn will make payment recommendation to the Integrated Commissioning Board.
The Confederation are required to provide qualitative feedback to the Children’s workstream on a quarterly basis, regarding the effectiveness of joint / shared care planning and communication between practices and Trusts. This supports the work of the programme board in improving these pathways in year. Payments for the three schedules are fully independent of each other. Budget:
Core (adults): £2,461,699
Children: 100,000 Time to Talk: £622,000
Cancer: £136,894
10
Overheads: £107,011 Total: £3,427,604
Core LTC contract
The recurrent budget for this service is £2,461,699
The CCG will award the GPC 100% of the total contract value (£2,461,699), if all practices achieve all minimum standards and the GPC achieves all minimum standards (this includes practices’ prevalences and standards that have not been met but where the CCG’s LTC Board agrees that there is sufficient evidence from the Confederation that the standard cannot be achieved).
If these conditions are not met then the following financial penalties will apply:
For each missed Confederation level standard: 2% penalty (£49,233.98) (capped at £300,000) For each missed Practice level standard: 0.5% penalty (£12,308.50) (capped at £50,000 per practice) [No penalties for Greenhouse as unique and challenging population] Indicator L12 Standard 0.5% penalty (£12,308.50) per practice for missing Q4 improvement target. Penalty calculated at practice level but aggregated to Confederation level
Maximum penalty (including L12) capped at £500,000. There are no penalties in relation to exception reporting or denominators. The Confederation is to be paid £1,961,699 in monthly instalments of £163,474.92 for delivery of the core contract. Over time we expect this contract to move towards a more outcomes based contract. Further discussions to be held in 2018/19 with the Prevention workstream to explore this in more detail.
Time to Talk The available budget is £622,000. The GPC is commissioned to deliver up to 12,420 extended consultations in-line with the specification (see above). For each consultation the GPC will be paid £50. Each practice needs to provide a certain minimum number of extended consultations (in order to demonstrate equity). This number will be established for each practice based on its respective share of the total number of people with LTCs registered with all C&H Practices – and the minimum of 20% of its respective share. Worked example There are 75000 people with LTCs across all 43 C&H practices – Sandringham has 1800 pts with LTCs – their respective share of the 75000 is 2.4% (1200/75000*100) – 2.4% of 12,420 is 298- the minimum number of consultations required is 20% of a practice’s relative share so Sandringham need to have provided 20% of 298 (i.e. 60 consultations). 3% of the GPC’s total earnings under this Contract (no. of consultation delivered x £50) will be deducted for each practice that does not meet its minimum target. Example: The Confederation delivers 10,000 consultations and consequently stands to earn £500,000. However Sandringham only delivers 20 of the 60 it needed to deliver to meet its minimum therefore the Confederation earns a 3% penalty (3% of £500k i.e., £15k). Cancer The available budget is £136,895 non-recurrent. Bowel screening
11
A payment of £57,500 will be available on a yearly basis to the GP confederation. 75% (£43,125) of this budget will be paid to the confederation for demonstrating that all pract ices have implemented the processes associated with the bowel screening elements of the contract. These include a system for identifying eligible patients and a method of recording contacts made by the practice to the patient and the date of screening undertaken. Practices will also need to have a system to search for patients identified to the practice as a DNA for bowel screening. The confederation should include a report on the numbers of patients actively contacted by practices to take up bowel screening. A further 25% (£14,375 divided equally across the four targets) will be paid to the GP Confederation will be on achievement each of the following targets:
60% of eligible men and women contacted around their 60th birthday by telephone and offered health promotion to encourage uptake of bowel screening.
90% of men and women in the above group sent endorsement letter by practice if not reached by telephone 60% of eligible men and women aged 6 – 70 who have not taken up their bowel screening (DNA notifications
are sent direct to the practices) in the last 3 months are contacted by telephone and offered health promotion advice and support to encourage uptake of bowel screening
90% of men and women in the above DNA group sent endorsement letter by practice if not reached by telephone
Outcomes The service aims to increase bowel screening uptake across all practices in City and Hackney.
On publication of the National Bowel Screening data a further payment of £6250 will be made to the Confederation if a 5% improvement is achieved across all City and Hackney practices.
An additional payment of £6,250 will be made if a 10% increase in bowel screening uptake is achieved.
The GP Confederation should link with NEL vanguard schemes and endeavour to ensure that any proposed schemes for increasing uptake do not overlap with NHSE or Vanguard site initiatives
2 week waits A £300 payment will be made to each practice per quarter (£51,600) on delivery of the following:
Compliance with and maintenance of new systems Numbers made by practice
Numbers of DNAs/delays where the practice took action In the following year (2019/20) the outcomes will move to reducing variation between practices on 2ww
referrals (with the aim of increasing 2ww referrals per 1,000 population) and reducing emergency presentations at hospital – this may include review of relevant referrals to direct access services
Time to talk (cancer) Payments will be made on the basis of a quarterly activity report from the confederation of the number of extended sessions of 20 minutes per patient on QOF register at the rate of £35 per patient (up to available budget of £15,295).
Children
The recurrent budget for this service is £100,000.
The CCG will award the GPC 90% of the total contract value (£90,000), if all practice level minimum standards are achieved.
If the asthma personalised plan and annual review standard is not achieved, there will be a Confederation penalty of £9,000
The Confederation is to be paid £90,000 in quarterly instalments of £22,500 for delivery of the children’s contract. The CCG will award the GPC 10% of the total contract value (£9,000) if the prescribed standards (referral to epilepsy nurse and EHCP pathway) are met.

12
Overheads Available budget £107,011 will be paid in quarterly instalments, no financial penalties will be associated with this element of the contract.
13
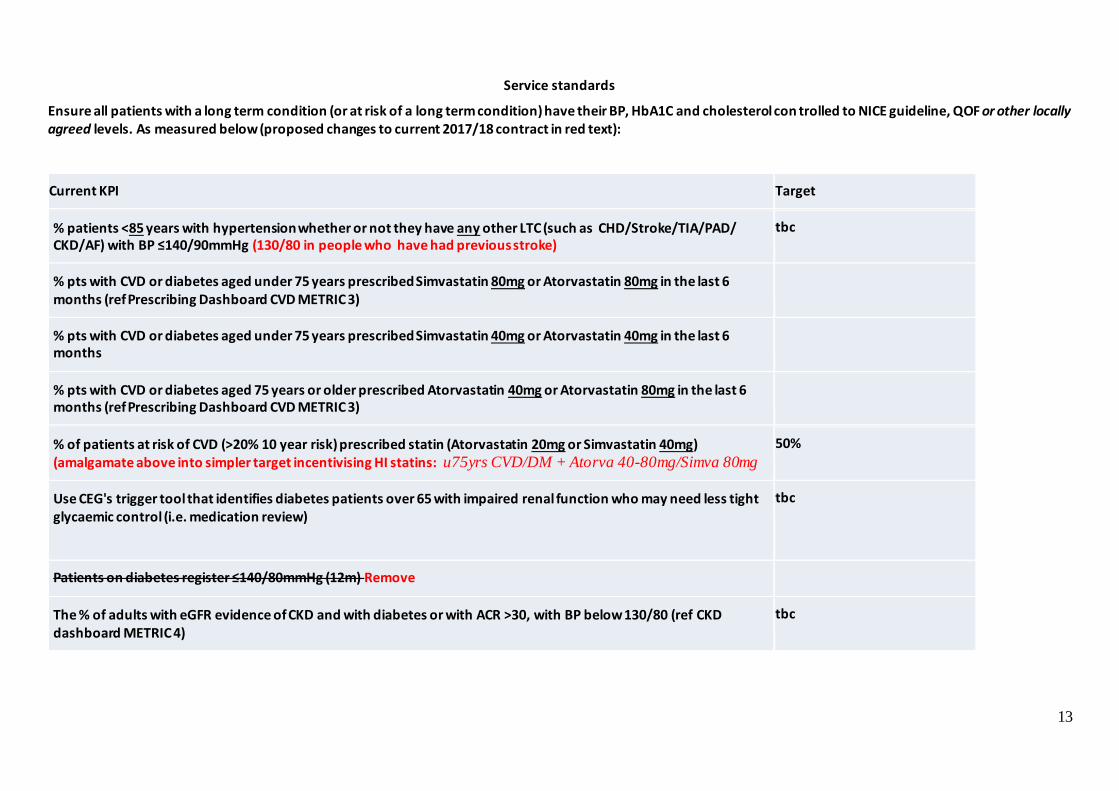
Service standards
Ensure all patients with a long term condition (or at risk of a long term condition) have their BP, HbA1C and cholesterol con trolled to NICE guideline, QOF or other locally agreed levels. As measured below (proposed changes to current 2017/18 contract in red text):
Current KPI Target
% patients <85 years with hypertension whether or not they have any other LTC (such as CHD/Stroke/TIA/PAD/ CKD/AF) with BP ≤140/90mmHg (130/80 in people who have had previous stroke)
tbc
% pts with CVD or diabetes aged under 75 years prescribed Simvastatin 80mg or Atorvastatin 80mg in the last 6 months (ref Prescribing Dashboard CVD METRIC 3)
% pts with CVD or diabetes aged under 75 years prescribed Simvastatin 40mg or Atorvastatin 40mg in the last 6 months
% pts with CVD or diabetes aged 75 years or older prescribed Atorvastatin 40mg or Atorvastatin 80mg in the last 6 months (ref Prescribing Dashboard CVD METRIC 3)
% of patients at risk of CVD (>20% 10 year risk) prescribed statin (Atorvastatin 20mg or Simvastatin 40mg) (amalgamate above into simpler target incentivising HI statins: u75yrs CVD/DM + Atorva 40-80mg/Simva 80mg
50%
Use CEG's trigger tool that identifies diabetes patients over 65 with impaired renal function who may need less tight glycaemic control (i.e. medication review)
tbc
Patients on diabetes register ≤140/80mmHg (12m) Remove
The % of adults with eGFR evidence of CKD and with diabetes or with ACR >30, with BP below 130/80 (ref CKD dashboard METRIC 4)
tbc
14
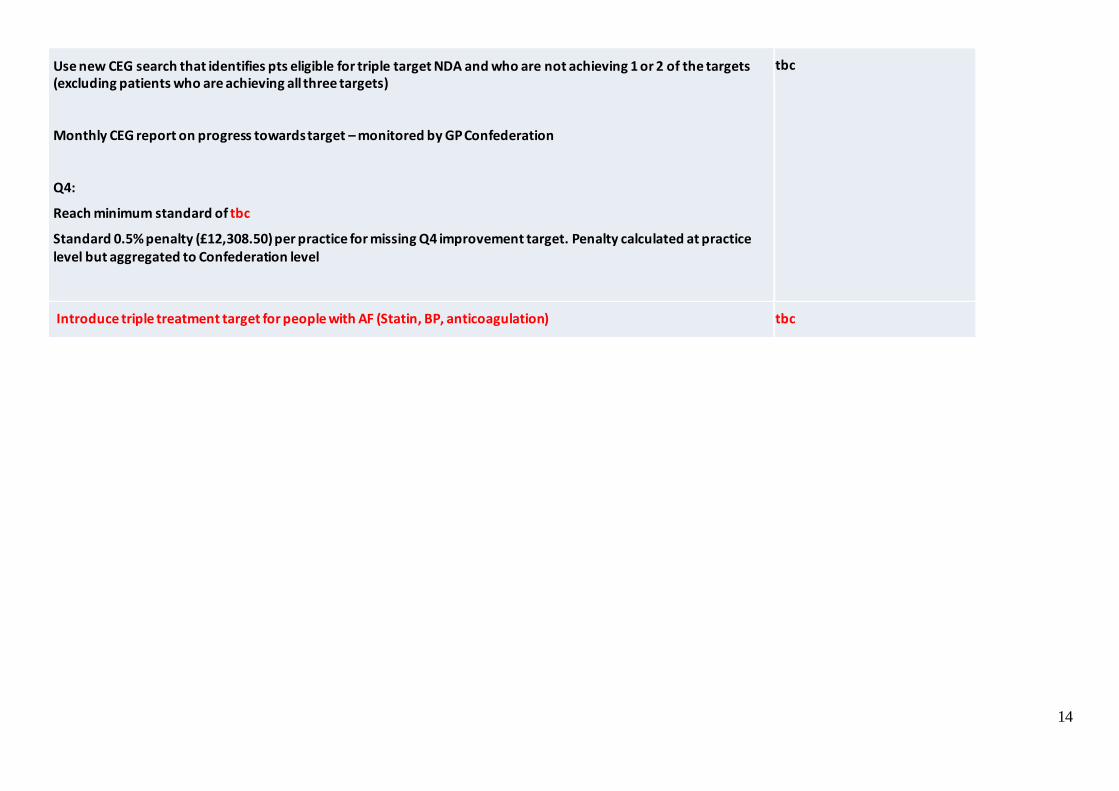
Use new CEG search that identifies pts eligible for triple target NDA and who are not achieving 1 or 2 of the targets (excluding patients who are achieving all three targets)
Monthly CEG report on progress towards target – monitored by GP Confederation
Q4:
Reach minimum standard of tbc
Standard 0.5% penalty (£12,308.50) per practice for missing Q4 improvement target. Penalty calculated at practice level but aggregated to Confederation level
tbc
Introduce triple treatment target for people with AF (Statin, BP, anticoagulation) tbc
15
16
17
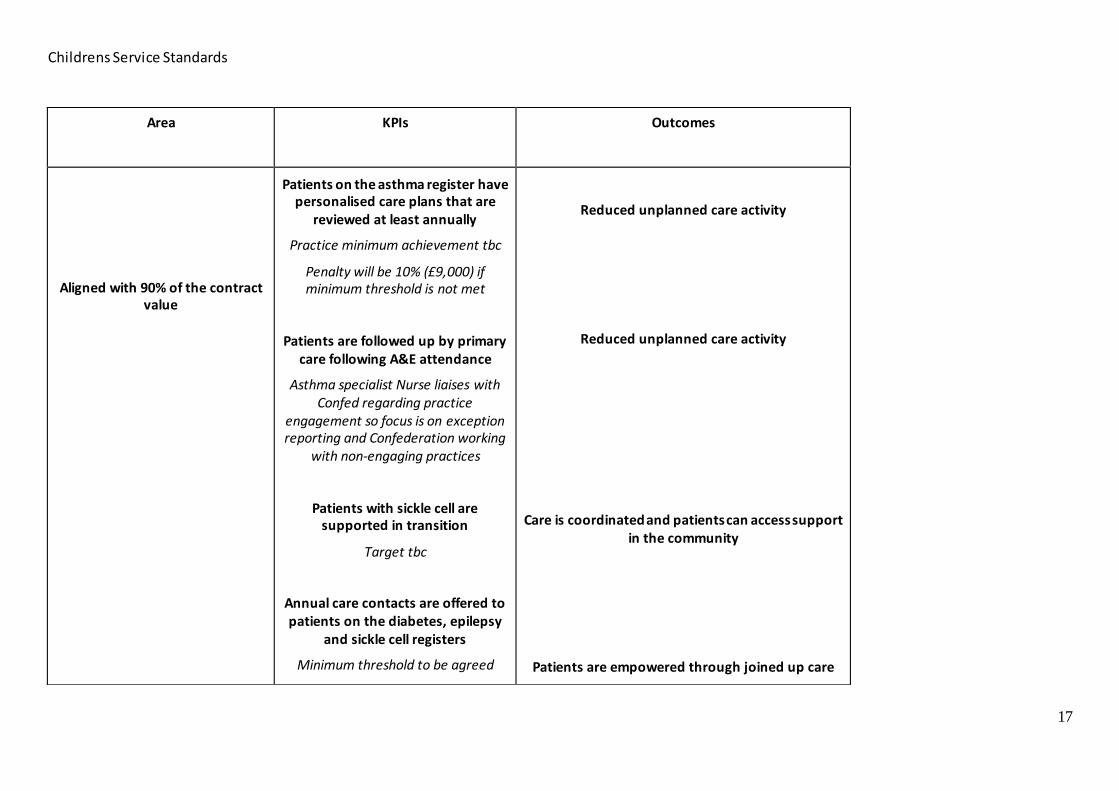
Childrens Service Standards
Area
KPIs Outcomes
Aligned with 90% of the contract value
Patients on the asthma register have personalised care plans that are
reviewed at least annually
Practice minimum achievement tbc
Penalty will be 10% (£9,000) if minimum threshold is not met
Patients are followed up by primary care following A&E attendance
Asthma specialist Nurse liaises with Confed regarding practice
engagement so focus is on exception reporting and Confederation working
with non-engaging practices
Patients with sickle cell are supported in transition
Target tbc
Annual care contacts are offered to patients on the diabetes, epilepsy
and sickle cell registers
Minimum threshold to be agreed
Reduced unplanned care activity
Reduced unplanned care activity
Care is coordinated and patients can access support in the community
Patients are empowered through joined up care
18
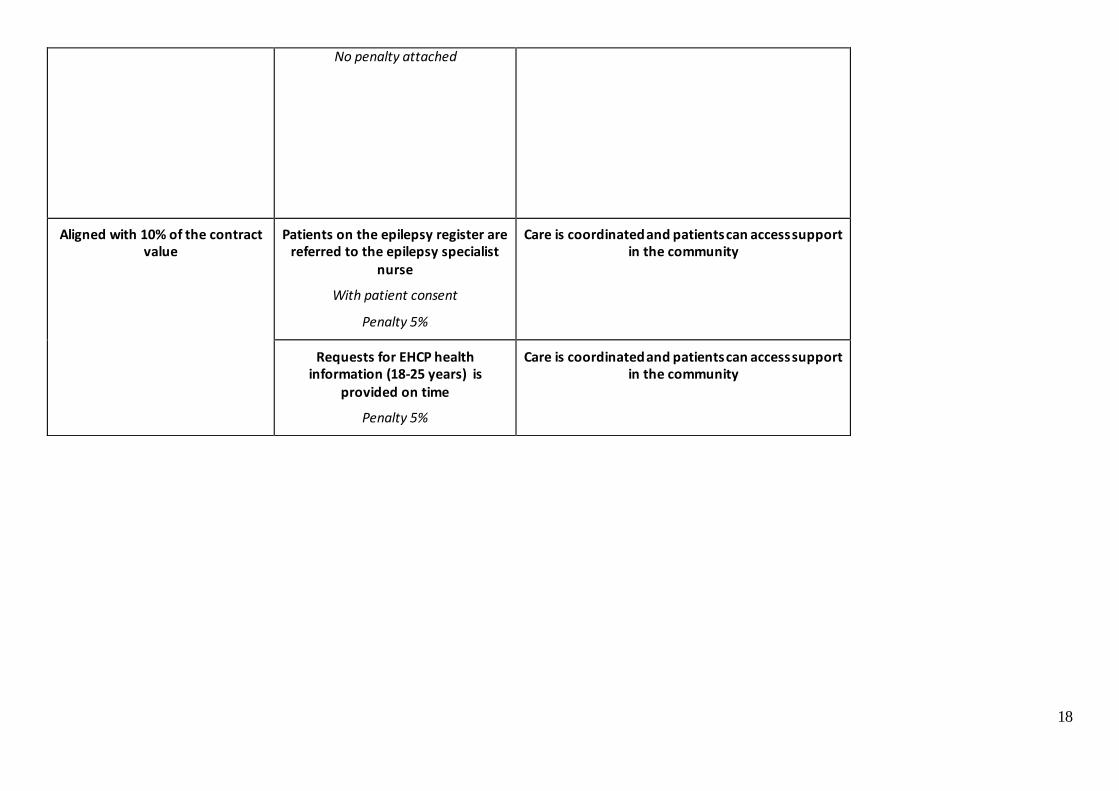
No penalty attached
Aligned with 10% of the contract value
Patients on the epilepsy register are referred to the epilepsy specialist
nurse
With patient consent
Penalty 5%
Care is coordinated and patients can access support in the community
Requests for EHCP health information (18-25 years) is
provided on time
Penalty 5%
Care is coordinated and patients can access support in the community


















